Page 1
1
63rd
Political Studies Association Conference
25 - 27 March 2013
City Hall Cardiff
Participation and Deliberation in Brazil: a comparative analysis of the Public
Policy Conferences
Cláudia F. Faria
Professor of Political Science Department – Federal University of Minas Gerais- Brazil
[email protected]
Alfredo Ramos Pérez
PhD student of Political Science of Universidad Complutense de Madrid.
[email protected]
Abstract
The Brazilian Public Policy Conferences change the pattern of social
participation in Brazil, since they introduce a combination of local, regional
and national levels of participation. This article analyses the key elements of
this process that integrates participatory and deliberative systems. Two cases
are the focus of a comparative analysis: the Health Conferences and the
Conferences on Policies for Women.
Key Word: Deliberative Democracy, Participatory Democracy, Brazil.
Public Conferences on Policies for Women, Public Conferences on Health
Page 2
2
Introduction
The aim of this paper is to portray the main elements of a Participative
Institution of contemporary Brazil, the Public Policies Conferences.
They will herein be analysed as constitutive elements of an integrated
participatory and deliberative system.
The idea of a plurality of spaces with a diversity of discourses that can
foster the development of deliberative capacities in different degrees is
an important analytical contribution of the proposal of an integrated
participatory and deliberative system. In order to consider the Public
Policies Conferences under this prism one must, therefore, understand
how the different actors participate, discuss and deliberate in a context
with multiple spheres. The local, state, regional and national spheres
involve different patterns of action oriented to the same goal: putting
forward a public agenda to influence the public power as regards the
real and symbolic needs of those who participate in these spaces.
In order to achieve our goal, we will present the key aspects of the
conference process and of the idea of integrated systems, which
underpins the proposed analysis. We will then perform a comparative
analysis of the XIV National Health Conference (XIV Conferência
Nacional de Saúde) and the III National Conference on Policies for
Women (III Conferência Nacional de Política para as Mulheres), both
Page 3
3
of which occurred in 2011. We will cover their preliminary stages,
which took place in the city of Belo Horizonte and in the state of
Minas Gerais, and its final moment in Brasília. This analysis allows us
to explain to which extent and for what reasons the analysed
conferences accord or not to the idea of an integrated system.
1. Definition and analysis of the mobilisation process of the
Policies for Women and the Health Conferences
We define the Public Policies Conferences as institutional spaces of
participation, representation and deliberation. They require diverse
efforts of social mobilisation as well as of building political
representation and of defining an agenda for public policies (Faria et
al, 2012). Although each one presents its own dynamics, they have all
got public assemblies in which the participants discuss and decide the
policy proposals and elect delegates for the various levels of the
federation, from the local to the national. The process ends in Brasília
with the reunion of all delegates elected in the former stages, held in
numerous municipalities and in the 27 Brazilian states. The
conferences are summoned by law, decree, ministerial or joint
ministerial ordinance or by an edict of the relevant Council, and they
intend to define the guidelines for the Public Policy Plans of the
various levels of the federation. These plans are expected to guide the
actions of both the executive and the legislative of each of these
levels.
Page 4
4
The conference process establishes, in Brazil, a new scenario for
participatory practices, since these no longer are limited to the local
level but, rather, assume a national dimension. The political
mobilisation pattern in Brazil is undergoing changes since the
promulgation of the Federal Constitution of 1988, which allowed for
the creation of numerous participatory mechanisms, spaces and
institutions, such as the Participatory Budget (Orçamento
Participativo), Public Hearings, the Public Policies and Rights
Management Councils and the City Plans (Planos Diretores). These,
amongst others, promoted participation primarily at the local level.
From Lula’s government (2003-2010) onwards, on the other hand, we
observe the development and increase in number of a group of
national participatory institutions, amongst which the analysed
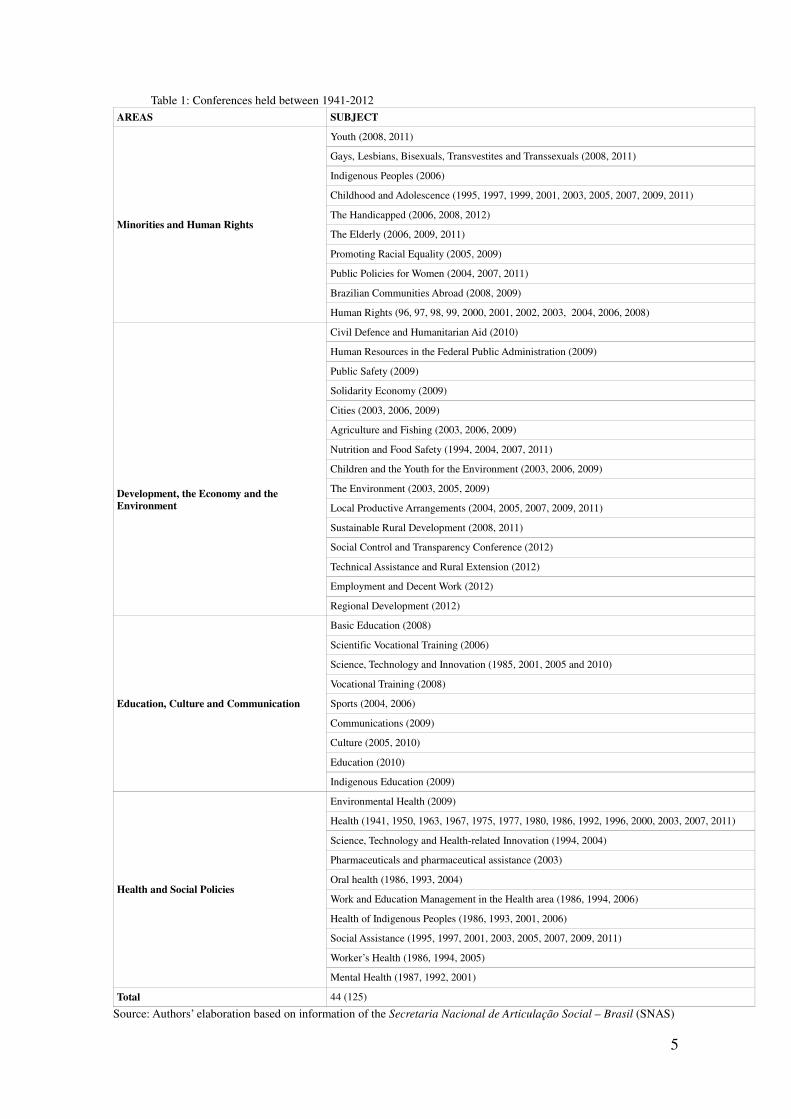
Conferences are of practical and analytical significance. From 1941,
when the first Health Conference was held, to the end 2012, there
have been 126 National Conferences concerning 45 different subject
areas. There were held, moreover, hundreds of State and Municipal
Conferences that assembled, according to official data, over seven
million people. The table below shows the kinds of Conferences that
have been held, as well as the number and the public policy subject
areas that have included this participatory mechanism since the
beginning of Lula’s government.
Page 5
5
Table 1: Conferences held between 1941-2012
AREAS SUBJECT
Minorities and Human Rights
Youth (2008, 2011)
Gays, Lesbians, Bisexuals, Transvestites and Transsexuals (2008, 2011)
Indigenous Peoples (2006)
Childhood and Adolescence (1995, 1997, 1999, 2001, 2003, 2005, 2007, 2009, 2011)
The Handicapped (2006, 2008, 2012)
The Elderly (2006, 2009, 2011)
Promoting Racial Equality (2005, 2009)
Public Policies for Women (2004, 2007, 2011)
Brazilian Communities Abroad (2008, 2009)
Human Rights (96, 97, 98, 99, 2000, 2001, 2002, 2003, 2004, 2006, 2008)
Development, the Economy and the
Environment
Civil Defence and Humanitarian Aid (2010)
Human Resources in the Federal Public Administration (2009)
Public Safety (2009)
Solidarity Economy (2009)
Cities (2003, 2006, 2009)
Agriculture and Fishing (2003, 2006, 2009)
Nutrition and Food Safety (1994, 2004, 2007, 2011)
Children and the Youth for the Environment (2003, 2006, 2009)
The Environment (2003, 2005, 2009)
Local Productive Arrangements (2004, 2005, 2007, 2009, 2011)
Sustainable Rural Development (2008, 2011)
Social Control and Transparency Conference (2012)
Technical Assistance and Rural Extension (2012)
Employment and Decent Work (2012)
Regional Development (2012)
Education, Culture and Communication
Basic Education (2008)
Scientific Vocational Training (2006)
Science, Technology and Innovation (1985, 2001, 2005 and 2010)
Vocational Training (2008)
Sports (2004, 2006)
Communications (2009)
Culture (2005, 2010)
Education (2010)
Indigenous Education (2009)
Health and Social Policies
Environmental Health (2009)
Health (1941, 1950, 1963, 1967, 1975, 1977, 1980, 1986, 1992, 1996, 2000, 2003, 2007, 2011)
Science, Technology and Health-related Innovation (1994, 2004)
Pharmaceuticals and pharmaceutical assistance (2003)
Oral health (1986, 1993, 2004)
Work and Education Management in the Health area (1986, 1994, 2006)
Health of Indigenous Peoples (1986, 1993, 2001, 2006)
Social Assistance (1995, 1997, 2001, 2003, 2005, 2007, 2009, 2011)
Worker’s Health (1986, 1994, 2005)
Mental Health (1987, 1992, 2001)
Total 44 (125)
Source: Authors’ elaboration based on information of the Secretaria Nacional de Articulação Social – Brasil (SNAS)
Page 6
6
Although not all conferences follow the same pattern, as they have got
their specificities, it is possible to identify common phases in the three
levels (municipal, state and national):
� Accreditation: the participants inscribe themselves for the
conference process and receive the material that will give support to
the discussions – such as the Programme, the Conference Procedures ,
the Proposals and other information.
� Opening Plenary Session: the directing board is designated and the
authorities and organising committees present the process and the
tasks to be done. Many presentations are made aiming at preparing the
participants for the deliberative process. The Conference Procedures,
made beforehand by the organising committees and/or by the councils,
are then debated and modified in a negotiation process.
� Work groups (hereafter WGs): delegates and invitees (the latter
without the right to vote) assess, debate and decide about the
proposals conceived in former stages. They may modify or eliminate
them, and, in some (but not all) cases, present new proposals.
� Final plenary session: the proposals approved in the WGs are
presented and submitted to a new round of discussion. Their special
requests are presented and debated, and the original proposal is then
approved or modified.
� Election of Delegates: the organising committees define the criteria
for this process, taking into account the population of the territory
and/or the degree of mobilisation and participation. The participants
thereby elect their representatives for the next phase of the
Page 7
7
Conferences, until the national one (which is the last stage of the
process).
The two Conferences analysed in this paper display different patterns,
which we believe are influenced by their different degrees of political
institutionalisation and by the mobilisation of the civil society.
Whereas Health is one of the most consolidated policy areas in terms
of political-administrative decentralisation and participation (Arretche,
2002), actually functioning as a health system in the whole country, it
is otherwise with Policies for Women, as this area has only recently
been thought as a set of public policies of national scope. We hold that
this difference in their institutional and participatory path determines
the quality of the conference process under analysis1.
The first Health Conference occurred 71 years ago, in 1941, during
Vargas’s government. From then to 2011 there were held 14 National
Conferences (and hundreds of local, municipal and state Conferences).
The first Conference on Policies for Women was held in 2004, with a
second edition in 2007. Table 2 below shows various other differences
between both processes, considering variables such as the
mobilisation level, the number of participants, their organisation and
representative procedures. The comparison of these variables allows
for the conclusion that the Health Conferences are more decentralised,
mobilise more people and are more institutionalised.
1 We share the views that hold that, besides the institutional design of the participatory institutions, the
constellation of social forces is a determinant of their success or failure, and actually even define the
design they come to possess (Fung and Wright, 2003; Avritzer, 2009).
Page 8
8
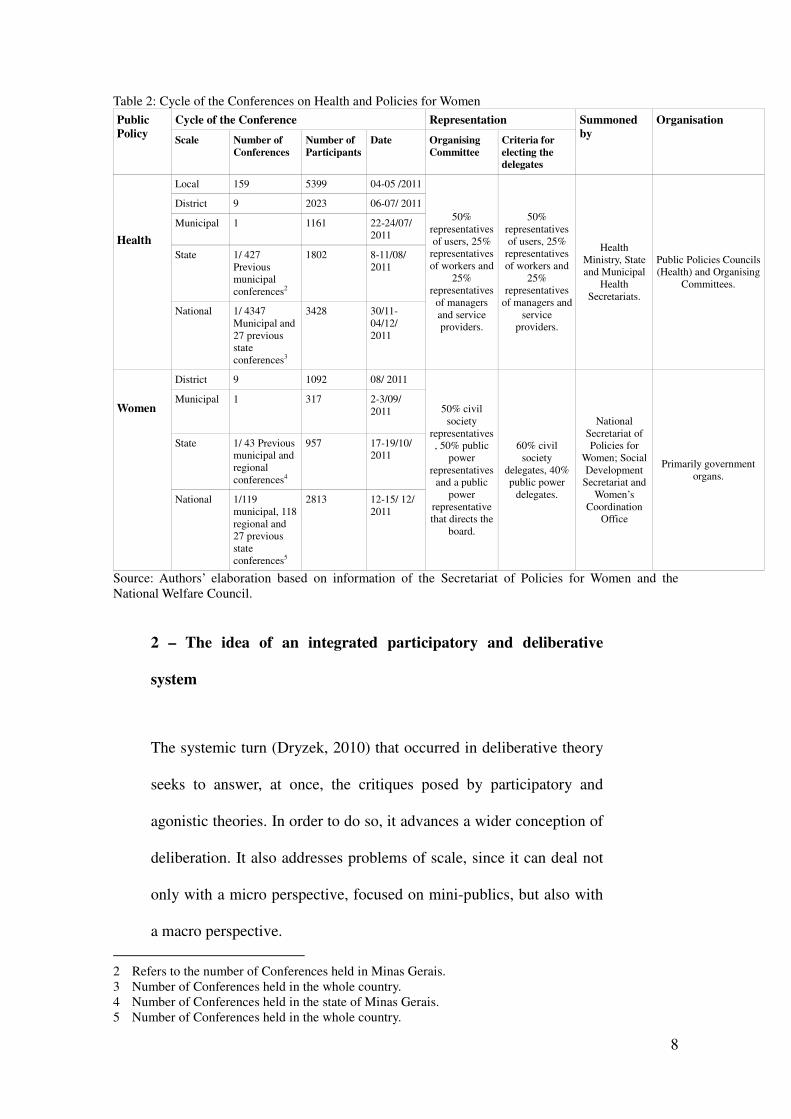
Table 2: Cycle of the Conferences on Health and Policies for Women
Public
Policy
Cycle of the Conference Representation Summoned
by
Organisation
Scale Number of
Conferences
Number of
Participants
Date Organising
Committee
Criteria for
electing the
delegates
Health
Local 159 5399 04-05 /2011
50%
representatives
of users, 25%
representatives
of workers and
25%
representatives
of managers
and service
providers.
50%
representatives
of users, 25%
representatives
of workers and
25%
representatives
of managers and
service
providers.
Health
Ministry, State
and Municipal
Health
Secretariats.
Public Policies Councils
(Health) and Organising
Committees.
District 9 2023 06-07/ 2011
Municipal 1 1161 22-24/07/
2011
State 1/ 427
Previous
municipal
conferences2
1802 8-11/08/
2011
National 1/ 4347
Municipal and
27 previous
state
conferences3
3428 30/11-
04/12/
2011
Women
District 9 1092 08/ 2011
50% civil
society
representatives
, 50% public
power
representatives
and a public
power
representative
that directs the
board.
60% civil
society
delegates, 40%
public power
delegates.
National
Secretariat of
Policies for
Women; Social
Development
Secretariat and
Women’s
Coordination
Office
Primarily government
organs.
Municipal 1 317 2-3/09/
2011
State 1/ 43 Previous
municipal and
regional
conferences4
957 17-19/10/
2011
National 1/119
municipal, 118
regional and
27 previous
state
conferences5
2813 12-15/ 12/
2011
Source: Authors’ elaboration based on information of the Secretariat of Policies for Women and the
National Welfare Council.
2 – The idea of an integrated participatory and deliberative
system
The systemic turn (Dryzek, 2010) that occurred in deliberative theory
seeks to answer, at once, the critiques posed by participatory and
agonistic theories. In order to do so, it advances a wider conception of
deliberation. It also addresses problems of scale, since it can deal not
only with a micro perspective, focused on mini-publics, but also with
a macro perspective.
2 Refers to the number of Conferences held in Minas Gerais.
3 Number of Conferences held in the whole country.
4 Number of Conferences held in the state of Minas Gerais.
5 Number of Conferences held in the whole country.
Page 9
9
Although participation and deliberation are actions oriented to
improving the quality of public life, they work through different
channels. This leads to the fact that “mass participation and quality
deliberation are two concepts in dispute” (Sintomer, 2001: 239). Both
share an interest in the principles of discussion, inclusion and
publicity; nevertheless, whilst participation presumes direct and ample
involvement, deliberation seeks to provide a qualified reflection on
preferences and the actors’ political choice, which may lead to a
curtailment of the process of inclusion (Cohen and Fung, 2004;
Papadopoulos and Warrin, 2007, Blondiaux, 2008).
The potential inclusionary limits that the deliberative practice brings
about are criticised by those who see deliberation as a form of
“dispassionate, reasoned, and logical” communication (Dryzek,
2000: 64) oriented towards consent. This is especially true when forms
of argumentation that grant advantages to certain actors are promoted
(Blondiaux, 2008), (potentially) advancing inequalities (Della Porta,
2011: 89). Mouffe ascertains that the deliberative perspectives “deny
the central role in politics of the conflictual dimension and its crucial
role in the formation of collective identities” (1999: 752).
Faced with a certain deliberative tradition that “unnecessarily restricts
the reasons or the legitimate forms of argumentation in the
deliberative process to those which are strictly rational or logical”
(Jorba, 2009: 28), Sander (1997) argues for the equality of the
epistemic authority of the various discourses. Other authors also
Page 10
10
defend the fostering of negotiation processes through which are
sought recognition and the interaction between forms of knowledge in
unequal conditions. They hence include other forms of
communication, such as protests, testimonies, rhetoric etc. (Chambers,
2009, Streich, 2002, Young, 2002, Blondiaux and Sintomer, 2004). All
of this is particularly important “when [one notices that] the public
that deliberates is increasingly less homogeneous” (Jorba, 2009: 30).
The idea of a “deliberative system” seeks to establish a dialogue with
these critiques, linking different kinds of actions performed in
different spheres that will comprise the system. This analytical
perspective posits that forms of action closer to participation, such as
public manifestations, bargaining etc., can and must coexist with
forms of action more oriented towards the public solution of conflicts,
such as deliberation (Goodin, 2005; Mansbridge, 1999, 2007;
Hendriks 2006). It thus seeks to render compatible different forms of
action that play distinct roles inside a complex socio-institutional web.
Different spaces with variegated repertoires and divergent
inclusionary degrees come to work as inputs for one another, thus
allowing for the promotion of a bottom-up public judgement (Faria et
al, 2012).
According to Dryzek (2010: 10-12), a system is deliberative only
insofar as it engenders an authentic, inclusive and consequential
deliberation. It is authentic to the extent that it promotes coercion-free
deliberation, through which the different arguments and points of view
Page 11
11
are taken into account. It is inclusive when it permits the participation
of all affected by the decision (or their representatives). And it is
consequential if the deliberation determines or influences the
decisions.
In his proposal, the deliberative system must possess certain elements.
These are: the public space, where free, unrestricted communication
takes place; the “empowered” space, which comprises formal or
informal spaces capable of exerting influence, and is thus qualified for
the deliberation of actors oriented to the collective decision-making
process; a transmission mechanism, or instruments through which a
wider public sphere may communicate with the empowered space;
accountability between the deliberative spheres and the public space;
meta-deliberation, a specific deliberative field that assesses how the
“deliberative system” may be organised; and, at last, decision-making
capacity, that involves various articulations between the mentioned
components and influences the decision-making process as a whole
(Dryzek, 2010: 10-12).
In light of this perspective, Mansbridge et al (2012) identify a system
as a “set of distinguishable, differentiated, but to some degree
interdependent parts, often with distributed functions and a division of
labour, connected in such a way as to form a complex whole” (ibid: 6).
The system must display differentiation, integration, a division of
labour and interdependence, dealing with conflict and problem-
solving via different forms of communication. The parts of the system
Page 12
12
must be analysed as a whole, i.e., considering the contribution of each
one to the deliberative quality of the entire system – hence building a
deliberative ecology. Such a strategy “allows us to see more clearly
where a system might be improved, and recommend institutions or
other innovations that could supplement the system in areas of
weakness” (ibid: 4-5). Decisions will be democratically legitimate
when they are taken in a context of mutual respect, following an
inclusive decision-making process not devoid of conflict.
The system possesses three main functions. The first is the Epistemic
one, which regards its contribution to the production of opinions,
preferences and decisions informed by facts and the argumentative
logic. The second is the Ethical function, based on its contribution to
promoting mutual respect and recognition between actors, in a context
characterised by the absence of domination and by equal treatment
amongst peers. The last is the Democratic function, which values the
inclusion of actors and interests, recognising “different forms of
action, ranging from protest to cooperative negotiation” (ibid: 9).
By limiting the deliberative or participative processes to the local
scale, the idea of a “deliberative system”, according to its advocates,
aims at expanding deliberation beyond a specific forum, conceiving
them as many forums through time (ibid: 2).
Page 13
13
3. The process of the Health and Policies for Women Conferences
In order to analyse to which extent the Public Policies Conferences
can be seen as an integrated system, as was herein presented, we shall
depict the different stages of their cycles, as well as the multiple
interactions between the elements that comprise them.
3.1 The Local Health Conferences (LHC), District Health Conferences
(DHC) and the District Conference on Policies for Women (DCPW):
differences and similarities in the beginning of the conference process.
One of the core differences between the two conference processes in
the city of Belo Horizonte regards, as previously mentioned, their
level of decentralisation. Only the Health Conference had a local stage
before the Pre-Conferences – the district stage, held in the city’s nine
regional administrative districts (see table 2).
Neither the LHCs nor the DCPWs debate their Conference Procedures
– an important mechanism that normatively governs the whole
process. In this sense, they display a similar degree of informality.
They both share some characteristics, such as: neither the LHCs nor
the DCPWs debate their internal rules; they make use of direct
participation, without the mediation of representatives (delegates);
they represent the first moment of contact and learning that many
participants have regarding the procedures and the content of the
conference process; and they are the stage in which are elaborated the
Page 14
14
proposals to underpin the other stages.
All stages of the conference process begin with the accreditation of
the participants, who receive the badges and the documents necessary
for the debate. In the DHCs, the participants receive a report with the
proposals approved in the former stage, as well as the Conference
Procedures, which are debated and modified in the opening plenary
session.
In the health area, some LHCs and most DHCs included the formation
of Work Groups (WGs), divided according to the subjects of the
conference guidelines. In the WGs the proposals directed to the
various government branches are made. In the first stage, the number
of participants in the WGs varied according to the number of
assembled participants, while in the second stage this number
oscillated between fifteen and twenty-five. In the DHCs the
deliberative process is more complex, for the participants are allowed
to modify proposals by special requests and via argumentative
negotiations. Changes in their text, inclusion of ideas and partial or
total elimination of proposals are allowed. The proposals are
prioritised either by a consensus of the group or by voting. In the final
plenary sessions of both stages the proposals made in each WG are
publicly presented, and the group of participants submits them to a
new round of discussion, special requests , argumentative negotiation,
voting and/or approving without voting.
Page 15
15
Not every Conference of the DCPWs had WGs. In these cases, the
discussions were held in the plenary sessions. This is due to the fact
that the number of participants was not sufficient in all cases for
performing these group activities. As to what regards the debating
mechanism, the Health and Policies for Women Conferences are
similar, despite the fact that the proposals were not voted in the WGs
in most groups of the DCPWs. In both cases, the transmission of the
proposals from the WGs to the final plenary session, when the latter
existed, was deficient. In but few cases the final plenary sessions
constituted a space for debate and the approval of proposals.
In both the WGs and the plenary sessions of these stages, the
discussions, when conducted, were mostly centred on accounts of
personal experiences related to the subject. Based upon these, and
with the help of professionals and activists of the area, the proposals
were made. The interventions of the activists were of more technical
and politicised character, given the professional and militant
knowledge they had of the matter at hand.
After making the proposals, the delegates are elected. In the DCPWs
there can be elected at most twenty regular delegates, regardless of the
resident population of each district. This quantity is defined in the
Conference Procedures of the III Municipal Conference. In some
regional administrative districts the elections for delegates of the civil
society and of the public power occurred separately. This separation
by segment also occurred in all the elections for delegates of the
Page 16
16
health policy. Each LHC had autonomy to decide how many delegates
it should elect in this stage, even if they all accepted the
proportionality established by law of having 50% of users, 25% of
workers and 25% of managers/service providers. The DHCs observed
the proportionality criteria, but the Municipal Health Council defined
the number of delegates based on multiple criteria, including the size
of the population and the management experience of the regional
administrative district.
3.2 Municipal Health Conference (MHC) and Municipal Conference
on Policies for Women (MCPW) in Belo Horizonte.
Both the MHC and the MCPW started with the accreditation of the
delegates. In this moment everyone receives their identification
badges, which allows for voting in the WGs and in the Final Plenary
Sessions, and the rest of the documents necessary for the discussions.
These include the matrix of proposals defined in former stages,
divided by government branch, as well as the Conference Procedures.
The matrix of proposals is a key document in the whole process, and
clear evidence of the fact that the Conferences internally constitute an
integrated participatory and deliberative system. The proposals
discussed in former scales undergo, in this stage, a new round of
debates, and those considered most relevant are selected.
After the accreditation there are the initial plenary sessions, with
speeches on the various public policies. Only in the case of Policies
Page 17
17
for Women, however, was there a speech on the assessment of the
conference process (meta-deliberation). The Conference Procedures
were debated in both, but while there were no significant
modifications in the MHC, in the MCPW there was great debate and
changes to the proposals for the percentage of elected delegates. The
public sector workers, who were not managers, got to be counted as
part of the civil society. With this modification, the division of
delegates of this segment changed from 60% civil society and 40%
government to, respectively, 80% and 20%.
The number of WGs was significantly larger in the MHC, with 30 of
them (six for each area), while the MCPW had but five. The number
of participants in each WG was similar in both, on average 35 to 40
people. The proposals were read and debated separately for each
competence area (municipal, state and federal). Their decision process
was significantly varied. In some WGs the text of the proposals could
be altered, by merging some of them and altering their quality and
impact. On the other hand, in other WGs the selected proposals were
only discussed and voted, with no modifications being allowed. In
neither policy was there the possibility of creating new proposals in
this stage.
In this second stage, the circulation of knowledge and the learning,
both stemming from the previous phases and the interactive process,
were much larger. This enabled the participants to build a better-
informed stance on the issues being discussed. Regarding the health
Page 18
18
policy, it stood out how the arguments no longer referred to local or
district matters, but, rather, assumed a municipal dimension and were
justified in more technically and politically sophisticated manners.
The Final Plenary Sessions also displayed significant differences. In
the MCPW all proposals were read and there was only one special
request, without any significant debate surrounding the remaining
ones. In contradistinction to this, in the MHS the debate on the
proposals the rapporteurs presented led to 54 special requests that
generated further discussion. The final decision was reached by
contrasting votes in favour and against.
The election of the delegates for the State Conference occurred in
specific forums for each segment, as in previous stages. In the MHC
the State Health Council defined the electoral criteria, according to the
population of the municipalities. Contrary to the previous stages, in
which women were overrepresented in both segments, in the MHC
male delegates had more representatives in the segment of users. In
the MCPW more than 95% of the delegates were women. In the civil
society segment, after much discussion surrounding the electoral
criteria, they opted for a territorial representation in which all districts
presented delegates who met separately to elect their representatives.
3.3 – The State Health Conference (SHC) and the State Conference on
Policies for Women (SCPW) of Minas Gerais: consolidating the
representative and deliberative processes
Page 19
19
As regards the actors, both analysed State Conferences differed from
previous stages in respect to the number and the plurality of
participants and to the greater presence of institutional representatives.
Both enjoyed many presentations on the issues at hand and, once
more, only the SCPW included an assessment of the policies debated
in the former conferences.
In both cases the debate on, and the voting of, the Conference
Procedures led to significant modifications in the process. Two facts
stood out. In the SHC the delegates decided, by majority vote, to
discuss all the proposals in the plenary, and not in the WGs. This
decision was reached after an intense and conflict-ridden debate on the
rule that vetoed changes in the proposals, allowing only for their
approval or disapproval. The plenary voted for modifying the
regulation of the Conference Procedures and of the SHC resolution,
thus altering the methodology of the process. In the SCPW the
participants altered the criteria for electing the delegates. Based on
territorial and mobilisation criteria, each of the state’s regions should
elect their delegates according to their own criteria, while observing
this general rule. The change enacted in the plenary also inverted the
formerly established weights for the criteria, attaching higher
importance to the each region’s level of mobilisation. This led to
changes in the distribution of delegates in fourteen of the twenty
regions.
Given the absence of WGs in the SHC, the delegates read and debated
Page 20
20
in the plenary the 535 proposals. This impacted the whole process,
which became less deliberative and more plebiscitary. If, on the one
hand, this change demonstrates the autonomy of the delegates, who
could modify the proposals as they saw fit, it also presents problems
for the representativeness and legitimacy of the whole process, since
the delegates did not respect what had been accorded in the former
stages, which had a much smaller plurality of actors.
The participants of the SCPW divided themselves in six WGs on the
various axes of the II National Plan for Policies for Women. The
groups were supposed to debate and choose proposals for the state and
national level. The general process consisted in suppressing some
proposals and working on the approved ones by merging many of
them and correcting, suppressing or altering their text. New proposals
could also be presented. The size of the groups was much larger than
in previous stages – they had between 70 and 90 participants. This was
more demanding for the mediators, who intermediated discursive
interactions more diversified in their arguments and strategies. The
mechanisms for approving the proposals varied from public
acclamation to voting, in order to solve conflicts or corroborate the
consensus that had been reached.
The final plenary session of the SCPW aimed at approving the
proposals made in the WGs. In this plenary, as opposed to the plenary
sessions of the previous stages, the consolidation of the proposals
occurred after a debate that allowed for the modification and
Page 21
21
suppression of the proposals. Of the 63 proposals approved in the
WGs, 43 were subjected to special requests. As in the WGs, the
reasons presented to maintain or alter the proposals combined legal
and political references, as well as personal and local experiences. In
many cases the proposals showed clearer and more objective writing.
New proposals could also be made in this stage. The plenary session
was marked by conflict, as that surrounding the legalisation of
abortion – the most polemical issue in the SCPW. As such, it was the
proposal with the most special requests. The result was to maintain the
legalisation proposal, reached in a tight voting.
In both cases the election for delegates occurred in specific spaces for
each segment. The criterion for distributing the delegates of the SHC
to each region of the state was defined by the National Health
Council, according to their population. As in the municipal stage,
there were more male delegates in the segment of users, the same
happening, in this stage, in the segment of managers/service providers.
This tendency did not prevail only the segment of workers. As a
consequence of the modifications of the Conference Procedures, a
great part of the debate in the SCPW consisted in establishing the
electoral criteria for each region. This led, on the one hand, to a debate
on what the group considered that should be represented (age,
ethnicity, entities etc.), and, on the other, to a marked conflict
surrounding the legitimacy of the representation of the delegates –
which made clear both the power relations and the tensions within the
representatives of each region.
Page 22
22
3.4 The National Health Conference (NHC) and the National
Conference on Policies for Women (NCPW): the ending of the
conference process
The last stage of both cycles maintained the four earlier analysed
phases of the process. After the accreditation, there was the
distribution of the consolidated book of proposals and the Conference
Procedures. The opening speeches were made and the Conference
Procedures were debated. It is worth mentioning that the NCPW was
the only conference in which the President of the Republic, Dilma
Roussef, participated. In her opening speech, she stressed the
importance of the Conference to ensure another form of governability,
founded on the social participation of all affected.
The discussion of the Conference Procedures in the NCPW was not
marked by much polemic, except only when deciding the number of
proposals the WGs could prioritise. In the NHC, in contrast, the
opposite occurred, notwithstanding the virtual debate held before the
NHC in order to build previous agreements6. Of its 29 articles, 24
were subjected to special requests, and the greatest polemic regarded
the use of secret electronic means to vote for the proposals. The
delegates argued that the secret voting with electronic ballot boxes
would distort the “public character” of the process and, based on this
argument, electronic voting was discarded.
6 The debate was organised by the Collective Health and Nutrition Nucleus (Núcleo de Saúde Coletiva e
Nutrição), in partnership with the Participative Democracy Project (Projeto Democracia
Participativa), both of the Federal University of Minas Gerais.
Page 23
23
Both Conferences had many speeches on the issues under discussion
and also had some innovations in the formation of the actors. The
NCPW had “debate circles” on subjects such as racism and
lesbophobia, economic and social autonomy, amongst others. The
NHC included “thematic dialogues”, in which specialists and
researches of the area debated with government technicians, health
workers and users.
Social movements played a central role in this stage. In the NCPW the
meetings organized by Women’s Entities are worth mentioning. They
were nationally articulated and promoted previous in-person debates
on some proposals to be presented in the WGs. Meanwhile, in the
NHC there were public manifestations of social movements and
unions of the area, against the Ministry of Health’s proposal of
establishing public-private partnerships for service provision in the
whole country. The defence of a national public health policy marked
many debates.
The NHC had 17 WGs, each with approximately 200 participants. The
NCPW, in its stead, had 24 WGs in the first day to discuss and
deliberate on the issue of economic autonomy, and 24 more WGs in
the second day to debate the issues of personal, political and cultural
autonomy (eight for each subject). The number of participants in these
groups varied from 50 to 100 delegates. There was more autonomy in
the NCPW, for the delegates could alter the proposals as well as
include new ones. Besides having a large number of participants per
Page 24
24
WG, an electronic system was used in the NHC that did not permit
increasing the debate time or including new proposals, but only
accepting or rejecting them.
Regarding both Health and Policies for Women, the justifications
presented based themselves in technical and political arguments,
aiming at solving national problems. The argumentative exchange led
to a change of preferences in many subjects, with the exception of the
most polemical ones – as the public-private partnerships, in the NHC,
and the legalisation of abortion, in the NCPW. It also made evident
that many participants possessed participative experiences that they
used in the negotiation process, both inside and outside the plenary
sessions. A great part of the participants adopted an informed stance,
built during the learning process the Conference cycles provide. In the
NCPW, the discursive diversity and the personal appeals grew less
numerous, hence leading to a more qualified flow of knowledge –
albeit also more professionalised and derived from previous
participative experiences than in the former stages.
In the final plenary sessions, the proposals that met with acceptance in
70% of the WGs were considered approved. Those with a lower
acceptance level, but still sufficient to be discussed in plenary, were
read and debated. In the NHC only 19 proposals (5% of the discussed)
were submitted to the plenary, and the voting consisted in approving
or eliminating them. In the NCPW most of the proposals presented for
debate in the plenary were approved without the need of voting.
Page 25
25
Contrary to what occurred in the NHC, the plenary of the NCPW
could alter the text of the proposals, modifying or merging them. The
legalisation of abortion, once more, emerged as the most polemical
issue in the III NCPW. In this case, the most explicit proposal for
legalising abortion led to open conflict between several hundred
Women in favour of and against legalisation. Ultimately, the proposal
was submitted to voting and approved in the final plenary session.
4. Conclusions
This article compared two kinds of Public Policy Conferences based
on the idea of an integrated system. This idea, as indicated earlier,
defends the connection and coordination of an ensemble of social
practices performed in different spaces and scales, all with the shared
objective of including different voices in the deliberative construction
of a common public policy agenda.
The analysis of the Conference processes showed that the health and
Policies for Women Conferences differ in their capillarity and in their
mobilisation capacity. This is proven by the decentralisation of their
processes and the number of participants. In both cases, as the stage
changes the organisational complexity increases, as demonstrated by
the presence of a variety of resources such as the Conference
Procedures, the WGs, the speeches and the book of proposals, as well
as by the discursive quality.
Page 26
26
Based on their rules and institutional design, one can say that the
analysed Conferences conform to a vertically integrated process. Their
different scales are connected and serve as inputs for one another. The
participation and deliberation processes in the WGs and in the Plenary
sessions, in the various levels, subsidise the succeeding scales by
means of the participation and the debate on the proposed subjects.
The representative procedure also allows for this connection between
the parts. It does so by electing delegates in the different scales, as
well as by the discursive formulation of the proposals that are debated
and/or modified along the process.
Regarding deliberation, in the case of the Health Conference the
changes of rules, regulations and resolutions that occurred during the
whole process made of the Conferences a more aggregative process,
particularly in the state and national levels. In the Conference on
Policies for Women (CPW), on the other hand, the opposite took
place. As the scale progressed upwards, the debates in the WGs and in
the Final Plenary Sessions gained in quality via the possibility of
modifying, altering and improving the presented proposals.
The state level of the Conference on Policies for Women modified
almost 80% of the proposals that came from previous stages, a figure
that in the national level increased to almost 95% of the proposals
presented for debate. In the Health area this process did not occur in
the same manner. In the national level the rules that were determined
forestalled a more substantive debate and the modification of the
Page 27
27
proposals.
On the argumentative pattern, in the initial stages – local and district –
of both processes a more informal discourse prevailed. It comprised
personal experiences of the civil society representatives, alongside
arguments based on technical knowledge of the professionals of their
respective areas. As the scale increases the first repertoire is overtaken
by more technical and politicised knowledge, mobilised by the social
movements, and/or by the participative knowledge stemming from the
experience of the Conference and of other participative institutions.
Many communicative styles intermesh in the PWC, even if those
closer to participation and social mobilisation predominate.
It is worth highlighting the debates on the Conference Procedures as a
form of meta-deliberation. In both cases these debates, which
modified the conditions of the process, referred to questions such as
the methodology for devising proposals, how to select the latter and
the representation criteria. In both policy areas and in various scales,
the possibility of a democratic discussion on the organisation of the
Conferences substantively altered them, thus showing the influence of
the participants in both processes.
The formation and learning are also conditioned by the change of
scale. In an initial moment, the information transmitted refers to local
particularities or to the very participative process of both Conferences.
Contrarily, in the national stage there is a myriad of panels and
Page 28
28
speeches to subsidise the debates in the WGs and in the plenary
sessions, which positively contributes to the progress of the
discussions. In the WGs the reasons presented for justifying the
proposals and the flow of information on local, municipal or regional
particularities increase the knowledge on the issue under debate. The
very process of the Conference implies a strategic learning on how to
mobilise different elements in the debates and secure support to
certain proposals.
Regarding representation, we can state that, whilst in both areas it
integrates the different stages of the process, it also undergoes a
change of meaning in each of the analysed policies. In the health area
representativeness assumes a marked territorial character,
fundamentally representing the proposals and demands made in the
former stages. It is otherwise in the CPW, whose forms of
representativeness are more linked to the participation in certain
entities and movements or to the association with particular policy
areas. Nevertheless, as the scales increases the representation criteria
become more complex, thus developing new factors of legitimacy.
Each forum for electing the delegates becomes a conflict-ridden arena,
due to the composition of both the civil society and the public power,
which have different projects and legitimate different modalities of
representation.
The NCPW, in contrast to the NHC, presented in various moments of
its many stages – particularly during the initial speeches – an
Page 29
29
accountability of the results of the policies for women, as well as an
assessment of the implementation of the proposals deliberated in
previous Conferences. Besides these and some virtual mechanisms for
controlling the implementation of proposals in experimental stages,
there are no mechanisms, in either process, for controlling the
implementation of the approved proposals – notwithstanding the fact
that the resolutions of the health Conferences and Councils are of law-
like status. This is one of the great problems of these participative
institutions. Councils and Coordination Offices, in the various
government levels, do not assume the task of controlling the approved
proposals, however much they may be spaces whose core function is
precisely this. Thus, the health area, in spite of the mentioned
capillarity it acquired via the mobilising work of the countless existing
councils – local, district, state and national –, does not yet adequately
fulfil this function. This can explain, for example, the repetition of
thousands of proposals from one edition to the other.
These evidences allow us to conclude that, on the one hand, the
Conferences in both policy areas form a vertically integrated system,
successfully linking one stage to the other. On the other hand, by
looking at the integration and coordination between the Conferences
in different areas, as well as with other participative institutions as the
Councils, we realise that, from the horizontal point of view, the
national participatory and deliberative system must still be improved
in order for it to effectively perform the epistemic, ethical and
democratic functions suggested by the theory at hand.
Page 30
30
References
Arretche, Marta. 2000. Estado federativo e políticas sociais:
determinantes da descentralização. Rio de Janeiro, São Paulo: Revan,
FAPESP.
Avritzer, Leonardo. 2009. Participatory institutions in democratic
Brazil. Washington: Woodrow Wilson Center Press.
Blondiaux, Loic. 2008. Le nouvel espirit de la democratie. Paris:
Seuil.
Blondiaux, Loic, y Sintomer, Yves. 2004. “El imperativo
deliberativo”, Revista de Estudios Políticos, 24: 95-114
Chambers, Simone . 2009. “Rethoric and the public sphere: Has
deliberative democracy abandoned mass democracy?” Political
Theory 37: 323-350.
Cohen, Joshua, and Fung, Archon. 2004. “Radical Democracy”, Swiss
Political Science Review 10: 26-46.
Della Porta, Donatella. 2011. Democrazzie. Bologna: Il Mulino.
Dryzek, John. 2000. Deliberative democracy and beyond: Liberals,
Page 31
31
critics, contestations. Oxford: Oxford University Press.
- 2010. Foundations and frontiers of deliberative governance. Oxford:
Oxford University Press.
Faria, Claudia, Petinelli, Viviane e Lourenço, Isabella. 2012.
“Conferências de políticas públicas: Um sistema integrado de
participação e deliberação?”, Revista Brasileira de Ciência Política 7:
249-284.
Fung, Archon and Wright, Erick. 2003. Deepening Democracy:
Institutional Innovations in Empowered Participatory Governance.
London: Verso,
Goodin, Robert. 2005. “Sequencing deliberative moments”, Acta
Politica 40: 182-196
Hendriks, Carolyn. 2006. “Integrated deliberation: Civil Society´s
dual role in deliberative democracy”, Political Studies 54: 486-508
Jorba, Laia. 2009. Deliberación y preferencias ciudadanas: un
enfoque empírico. La experiencia de Cordoba. Madrid: CIS:
Mansbridge, Jane. 1999. “Every day talk in the deliberative system”,
en Stephen Macedo, ed., Deliberative politics: essays on democracy
Page 32
32
and disagreement. New York: Oxford University Press.
- 2007. “Deliberative democracy or democratic deliberation”, en
Shawn Rosenberg, ed., Deliberation, participation and democracy:
Can the people govern?. New York: Palgrave Macmillan.
Mansbridge, Jane, Bohman, James, Chambers, Simone, Christiano,
Thomas, Fung, Archon., Parkinson, John, Thompson, Dennis, and
Warren, Mark. 2012. “A systemic approach to deliberative
democracy”. (mimeo)
Mouffe, Chantall. 1999. “Deliberative Democracy or Agonistic
Pluralism?”, Social Research 66: 745-758
Papadopoulos, Yannis. and Warin, Philippe. 2007. “Are innovative,
participatory and deliberative procedures in policy making democratic
and effective?”, European Journal of Political Research, 46: 445-472.
Sanders, Lynn. 1999 “Against deliberation”, Political Theory 25: 347-
376.
Sintomer, Yves. 2011. “Deliberation et participation: Affinité élective
ou concepts en tension?”, Participations 1: 239-276.
Streich, Gregory. 2002. “Constructing Multiracial Democracy: To
Page 33
33
deliberate or not to deliberate?”, Constellations 9: 127-153.
Young, Iris. 2002. Inclusion and democracy. Oxford: Oxford
University Press.