Metabolic Surgery Philip R. Schauer, MD Professor of Surgery, Cleveland Clinic Lerner College of Medicine The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file again. If the red x still appears, you may have to delete the image and then insert it again. The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file again. If the red x still appears, you may have to delete the image and then insert it again.
Transcript
Metabolic Surgery
Philip R. Schauer, MD Professor of Surgery, Cleveland Clinic Lerner College of Medicine
The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file again. If the red x still appears, you may have to delete the image and then insert it again.
The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file again. If the red x still appears, you may have to delete the image and then insert it again.
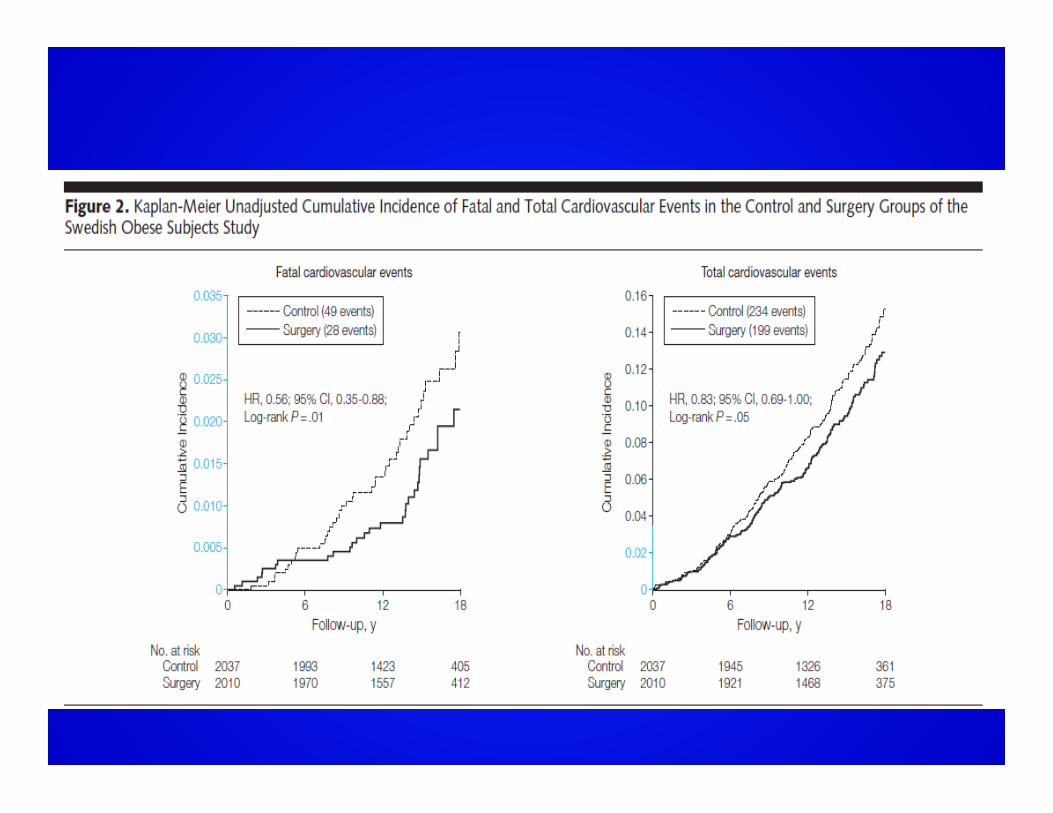
• Many surgical patients were able to reduce the number of CV medications.
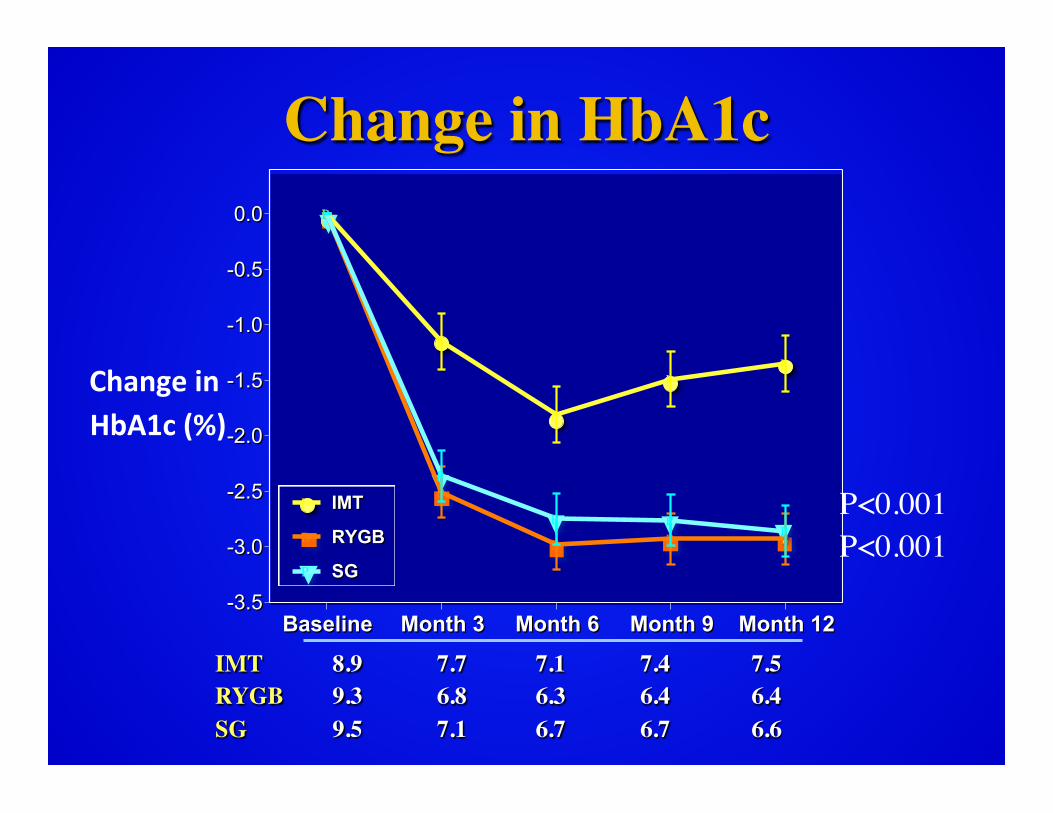
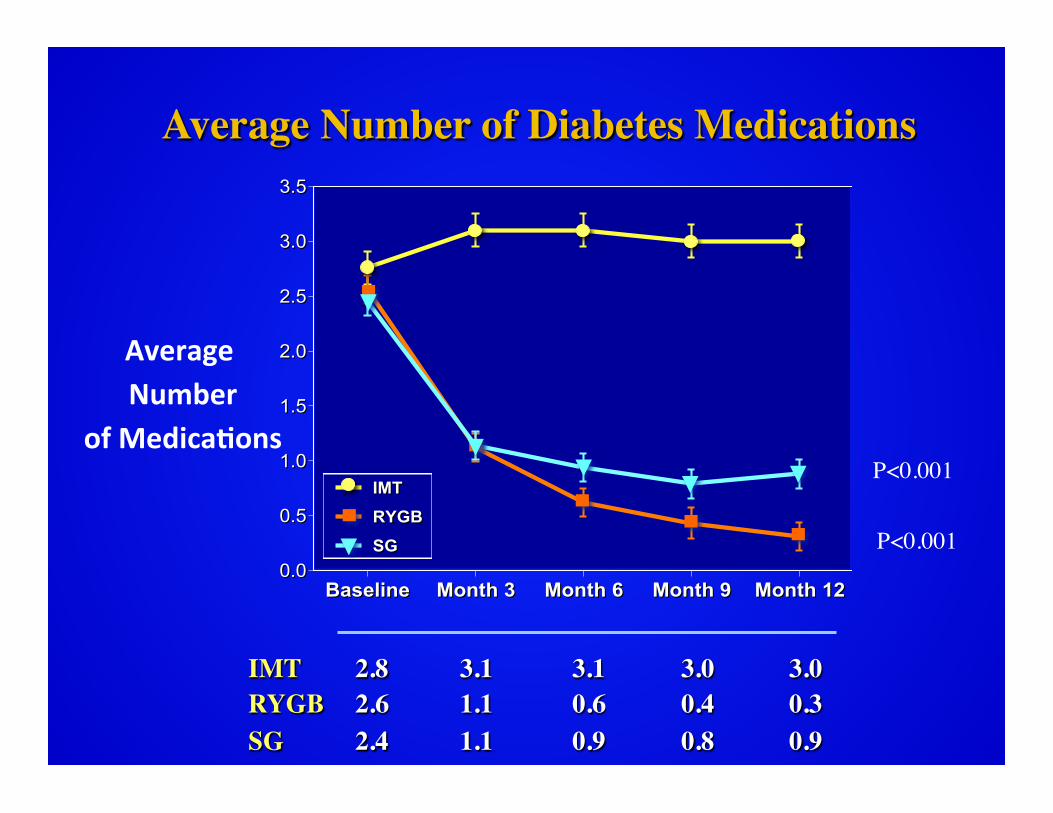
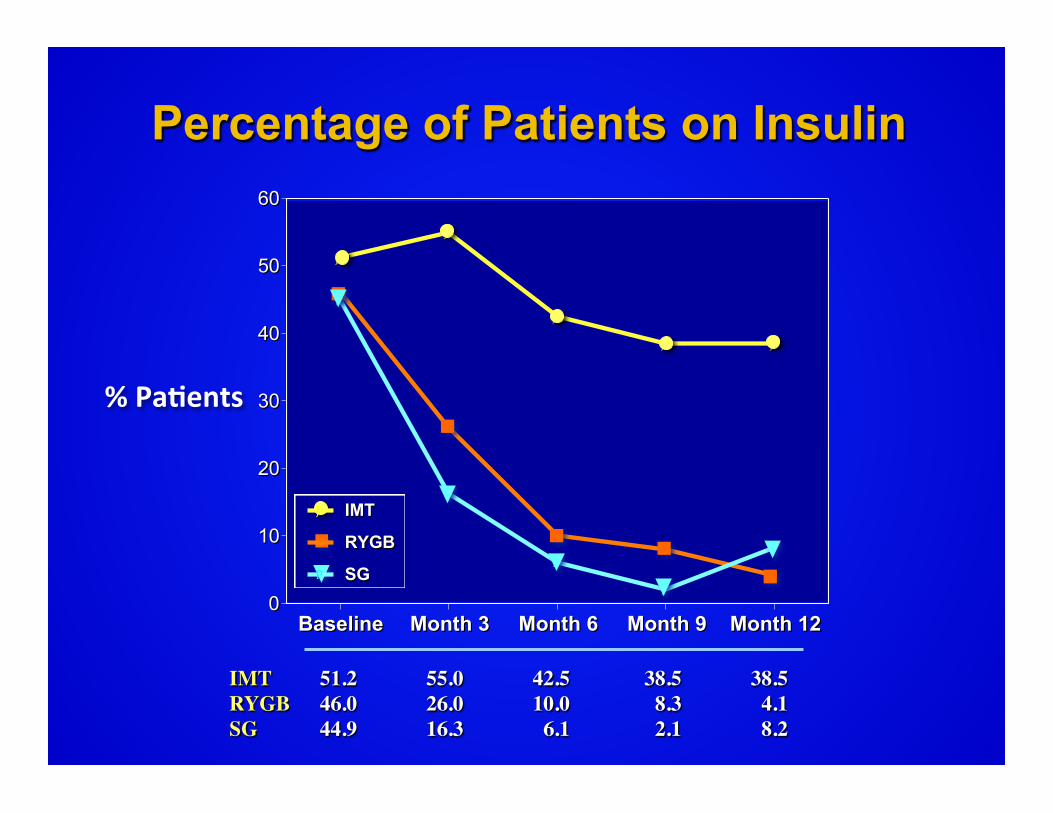
Schauer et al. NEJM 2012
Conclusion Bariatric surgery (gastric bypass or sleeve
gastrectomy) may be considered as a treatment option for patients with uncontrolled T2DM and moderate to severe obesity (BMI > 30 Kg/M2)
Schauer et al. NEJM 2012
Mingrone et al. NEJM 2012
Results: Primary Endpoint, HA1c
2012: The Year of Metabolic Surgery���Recent Relevant Publications
SOS JAMA 2012
A
5
6
7
8
9
10
11
0 6 12 24 48 60 72
Months After Surgery
Hemoglobin
A1c
(%)
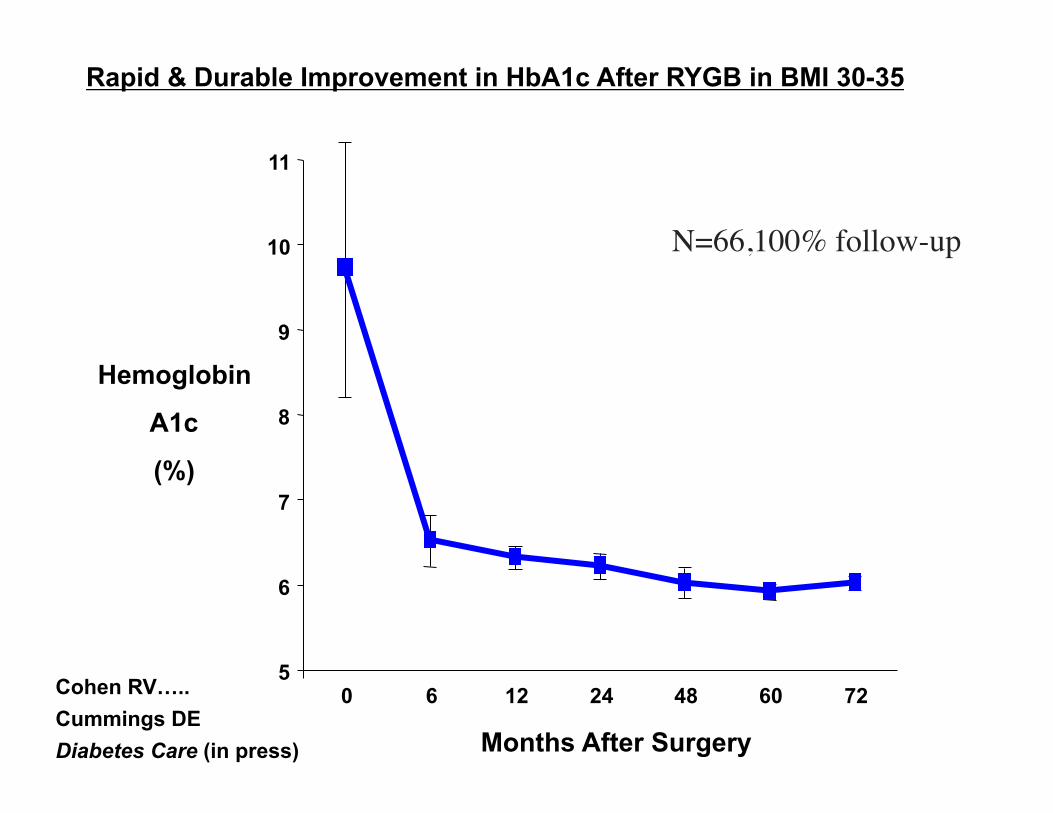
Cohen RV….. Cummings DE Diabetes Care (in press)
Rapid & Durable Improvement in HbA1c After RYGB in BMI 30-35
N=66,100% follow-up
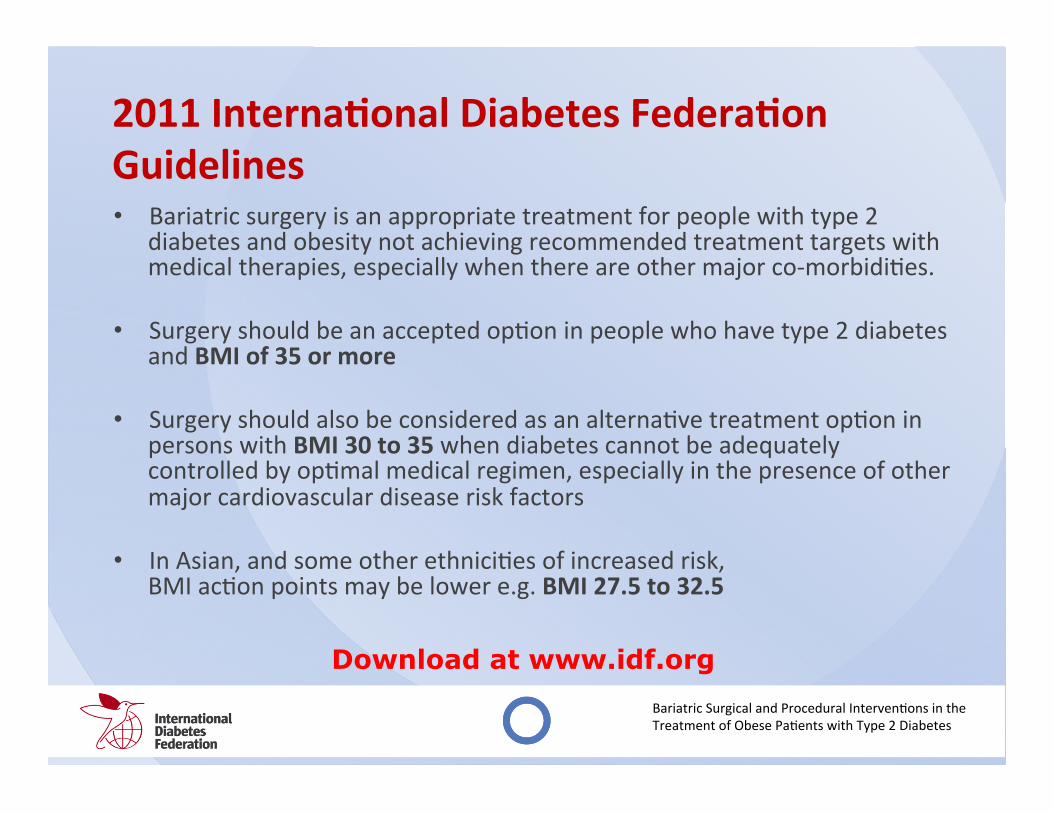
2011 Interna>onal Diabetes Federa>on Guidelines • Bariatric surgery is an appropriate treatment for people with type 2
diabetes and obesity not achieving recommended treatment targets with medical therapies, especially when there are other major co-‐morbidi<es.
• Surgery should be an accepted op<on in people who have type 2 diabetes
and BMI of 35 or more
• Surgery should also be considered as an alterna<ve treatment op<on in persons with BMI 30 to 35 when diabetes cannot be adequately controlled by op<mal medical regimen, especially in the presence of other major cardiovascular disease risk factors
• In Asian, and some other ethnici<es of increased risk,
BMI ac<on points may be lower e.g. BMI 27.5 to 32.5
Bariatric Surgical and Procedural Interven<ons in the Treatment of Obese Pa<ents with Type 2 Diabetes
Download at www.idf.org
Conclusion • 3 RCT’s show surgery results in superior
glycemic control compared to medical Rx • CV risk factors improved with surgery • Weight loss is a major driver of
improvement • Patients with uncontrolled T2DM (HbA1c
>7.0%) and Obesity (BMI > 30) and should be considered for bariatric surgery