20
HOSPITALS. An architect's perspective 2010 Book 8.2 Royal Prince Alfred Hospital, Sydney Its architecture, growth & change 1993-2014 William Miller
| Date post: | 08-Aug-2015 |
| Category: |
Healthcare |
| Upload: | william-miller |
| View: | 91 times |
| Download: | 2 times |

HOSPITALS.An architect's perspective
2010
Book 8.2 Royal Prince Alfred Hospital, Sydney
Its architecture, growth & change 1993-2014
William Miller
BLANK

Hospitals. An Architect's Perspective
Book 8.2 Royal Prince Alfred Hospital, SydneyIts architecture, growth and change 1993-2014
William Miller
20/02/15
BLANK

PrefaceThis notebook 8.2 is one of a series about the architecture of hospitals across the centuries:
1. The Modern Hospital
2. Synopsis. 2500 BCE to the present
3. Sumer and Egypt. 4000 to 500 BCE
4. Greece and Rome. 500 BCE to 500 CE.
5. Medieval period 500 to 1450 CE
6. Renaissance 1400 to 1650
7. Pre-modern 1650 to 1850
8. Modern 1850 to 1950
8.1 Royal Prince Alfred Hospital 1873 to 1910
8.2 Royal Prince Alfred Hospital. Its growth and change 1993-2014
9. Late modern 1950 – present
Hospitals are one of society's most enduring institutions; they tend to remain in place, evolving and regenerating their services and organisation to care for us over many generations, indeed, centuries; subject of course, to political interference.
Since WWII and especially since the 1960s, the pace of change has been such that, by the time a new hospital or facility within an established hospital is built, it is out of date and typically, too often because of architectural rigidities and inertia in the process of capital acquisition, it will be between a few and several years before any of its facilities are remodelledto meet contemporaneous need.
Thus while hospitals deliver services of time present, they must operate through an inherited architecture of times past.And while an inherited architecture enables service delivery it also inhibits and frustrates adaptability to emerging needs. In this regard, some architectures perform better than others. Identifying those architectures which outperform others is a central objective of this work. And wherever possible reference will be made context and the development process.
This Book 8.2. tells the story of RPA's redevelopment between 1993 and 2014. The development strategy arose from a commission to upgrade the Hospital's Emergency Centre; normally it would be the other way round. Nonetheless the processyielded a very successful strategy which added value beyond expectation. Thus it seemed to me that the story should be told.
Like their subject, this Book is subject to growth and change. Thus if you find any part informative, return to check the date on the document's file name and inside Fly.
Finally, I welcome comment and advice.
Bill Miller,20/02/[email protected]
Contents
Preface
Introduction
A&E Centre at RPA as found 1993
Architectural appraisal
A&E's facility needs
Hospital services, facility needs and infrastructure design
Opportunities for A&E
Opportunities for consolidation hospital services
Economic appraisal
Benefits of A&E Option 1b
A&E design
Consolidation 1993-2004
Post consolidation opportunities realised 2004-2014
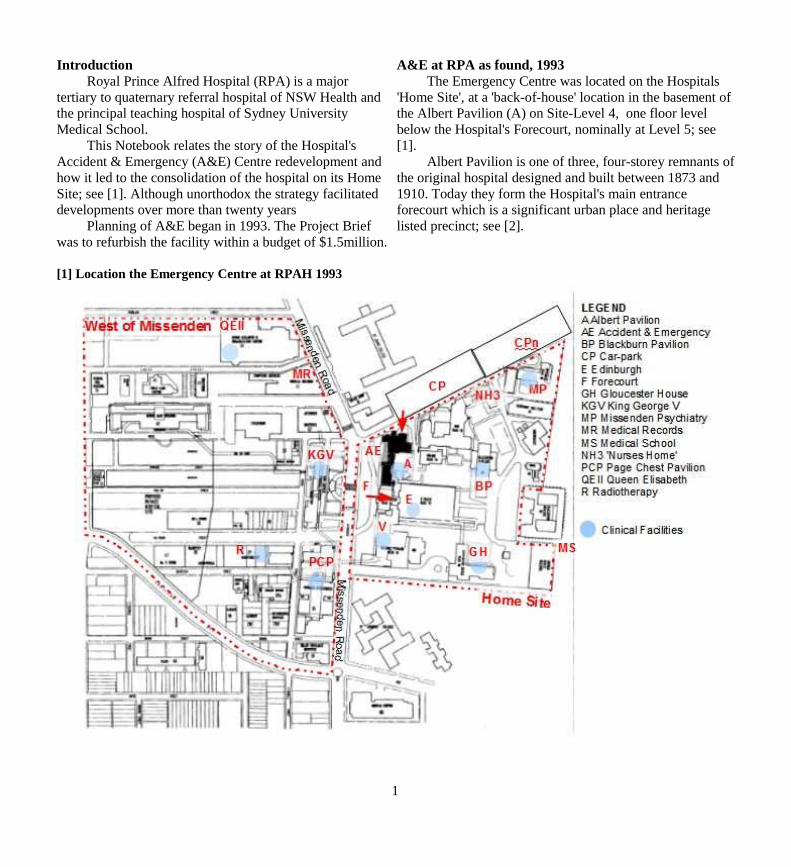
IntroductionRoyal Prince Alfred Hospital (RPA) is a major
tertiary to quaternary referral hospital of NSW Health and the principal teaching hospital of Sydney University Medical School.
This Notebook relates the story of the Hospital's Accident & Emergency (A&E) Centre redevelopment and how it led to the consolidation of the hospital on its Home Site; see [1]. Although unorthodox the strategy facilitated developments over more than twenty years
Planning of A&E began in 1993. The Project Brief was to refurbish the facility within a budget of $1.5million.
[1] Location the Emergency Centre at RPAH 1993
A&E at RPA as found, 1993The Emergency Centre was located on the Hospitals
'Home Site', at a 'back-of-house' location in the basement of the Albert Pavilion (A) on Site-Level 4, one floor level below the Hospital's Forecourt, nominally at Level 5; see [1].
Albert Pavilion is one of three, four-storey remnants ofthe original hospital designed and built between 1873 and 1910. Today they form the Hospital's main entrance forecourt which is a significant urban place and heritage listed precinct; see [2].
1
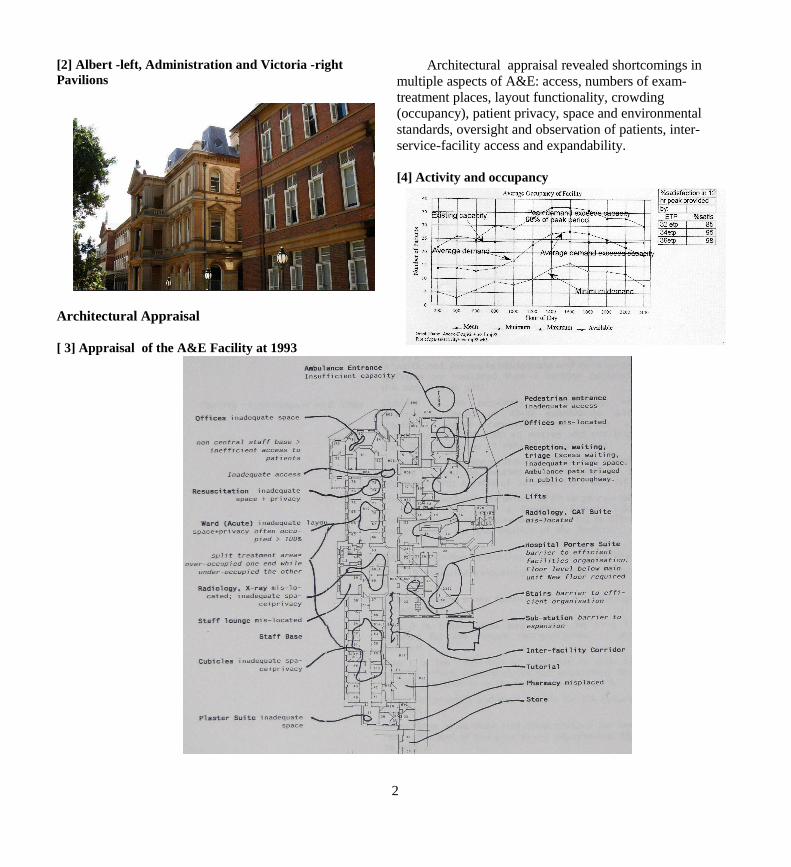
[2] Albert -left, Administration and Victoria -righ t Pavilions
Architectural Appraisal
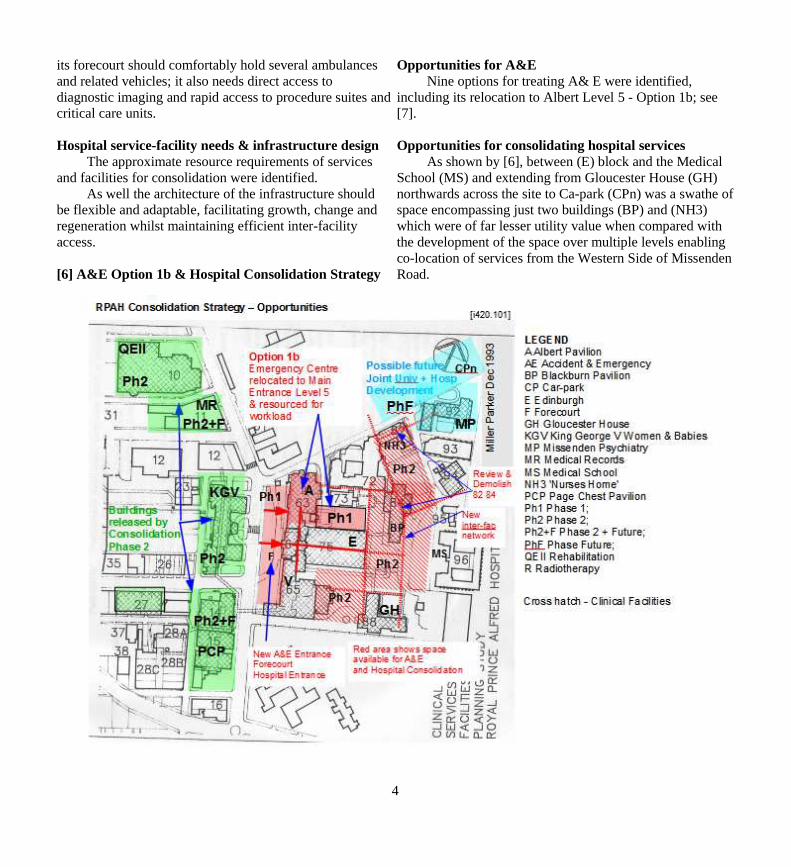
[ 3] Appraisal of the A&E Facility at 1993
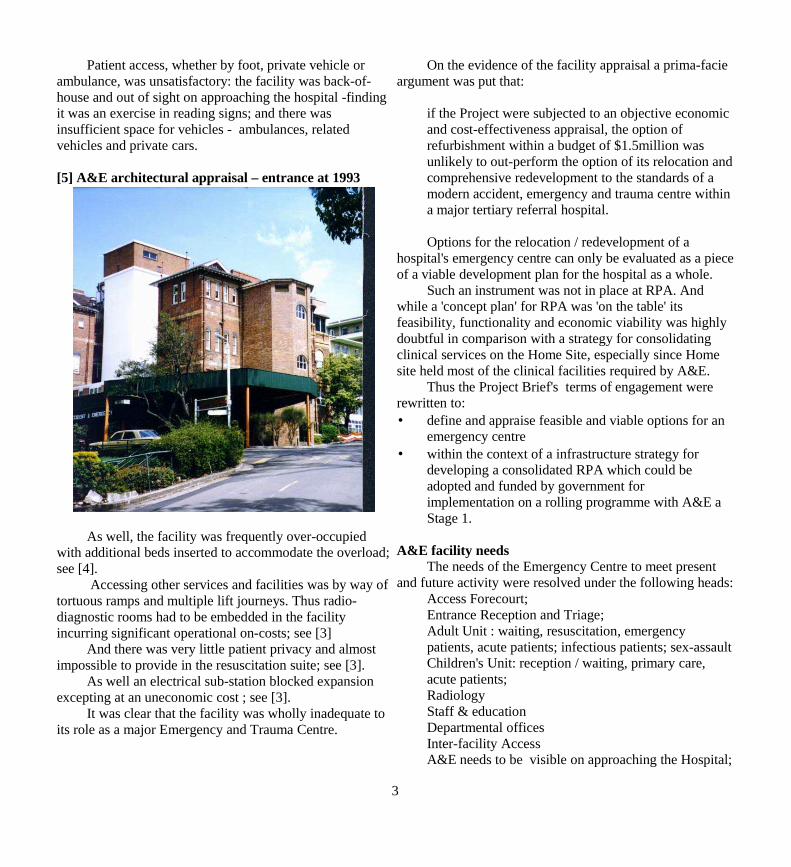
Architectural appraisal revealed shortcomings in multiple aspects of A&E: access, numbers of exam-treatment places, layout functionality, crowding (occupancy), patient privacy, space and environmental standards, oversight and observation of patients, inter-service-facility access and expandability.
[4] Activity and occupancy
2
Patient access, whether by foot, private vehicle or ambulance, was unsatisfactory: the facility was back-of-house and out of sight on approaching the hospital -finding it was an exercise in reading signs; and there was insufficient space for vehicles - ambulances, related vehicles and private cars.
[5] A&E architectural appraisal – entrance at 1993
As well, the facility was frequently over-occupied with additional beds inserted to accommodate the overload;see [4].
Accessing other services and facilities was by way oftortuous ramps and multiple lift journeys. Thus radio-diagnostic rooms had to be embedded in the facility incurring significant operational on-costs; see [3]
And there was very little patient privacy and almost impossible to provide in the resuscitation suite; see [3].
As well an electrical sub-station blocked expansion excepting at an uneconomic cost ; see [3].
It was clear that the facility was wholly inadequate to its role as a major Emergency and Trauma Centre.
On the evidence of the facility appraisal a prima-facie argument was put that:
if the Project were subjected to an objective economic and cost-effectiveness appraisal, the option of refurbishment within a budget of $1.5million was unlikely to out-perform the option of its relocation andcomprehensive redevelopment to the standards of a modern accident, emergency and trauma centre within a major tertiary referral hospital.
Options for the relocation / redevelopment of a hospital's emergency centre can only be evaluated as a pieceof a viable development plan for the hospital as a whole.
Such an instrument was not in place at RPA. And while a 'concept plan' for RPA was 'on the table' its feasibility, functionality and economic viability was highly doubtful in comparison with a strategy for consolidating clinical services on the Home Site, especially since Home site held most of the clinical facilities required by A&E.
Thus the Project Brief's terms of engagement were rewritten to:• define and appraise feasible and viable options for an
emergency centre • within the context of a infrastructure strategy for
developing a consolidated RPA which could be adopted and funded by government for implementation on a rolling programme with A&E a Stage 1.
A&E facility needsThe needs of the Emergency Centre to meet present
and future activity were resolved under the following heads:Access Forecourt; Entrance Reception and Triage; Adult Unit : waiting, resuscitation, emergencypatients, acute patients; infectious patients; sex-assaultChildren's Unit: reception / waiting, primary care,acute patients;Radiology Staff & education Departmental officesInter-facility AccessA&E needs to be visible on approaching the Hospital;
3
its forecourt should comfortably hold several ambulances and related vehicles; it also needs direct access to diagnostic imaging and rapid access to procedure suites andcritical care units.
Hospital service-facility needs & infrastructure design The approximate resource requirements of services
and facilities for consolidation were identified.As well the architecture of the infrastructure should
be flexible and adaptable, facilitating growth, change and regeneration whilst maintaining efficient inter-facility access.
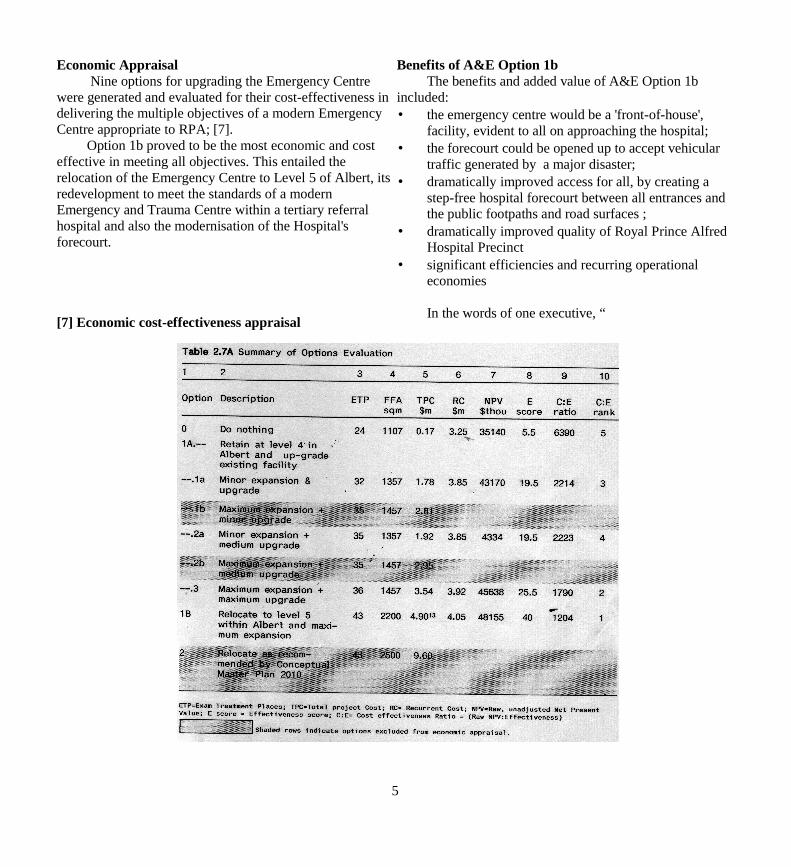
[6] A&E Option 1b & Hospital Consolidation Strategy
Opportunities for A&ENine options for treating A& E were identified,
including its relocation to Albert Level 5 - Option 1b; see [7].
Opportunities for consolidating hospital servicesAs shown by [6], between (E) block and the Medical
School (MS) and extending from Gloucester House (GH) northwards across the site to Ca-park (CPn) was a swathe ofspace encompassing just two buildings (BP) and (NH3) which were of far lesser utility value when compared with the development of the space over multiple levels enabling co-location of services from the Western Side of Missenden Road.
4
Economic Appraisal Nine options for upgrading the Emergency Centre
were generated and evaluated for their cost-effectiveness indelivering the multiple objectives of a modern Emergency Centre appropriate to RPA; [7].
Option 1b proved to be the most economic and cost effective in meeting all objectives. This entailed the relocation of the Emergency Centre to Level 5 of Albert, itsredevelopment to meet the standards of a modern Emergency and Trauma Centre within a tertiary referral hospital and also the modernisation of the Hospital's forecourt.
[7] Economic cost-effectiveness appraisal
Benefits of A&E Option 1bThe benefits and added value of A&E Option 1b
included:• the emergency centre would be a 'front-of-house',
facility, evident to all on approaching the hospital;• the forecourt could be opened up to accept vehicular
traffic generated by a major disaster; • dramatically improved access for all, by creating a
step-free hospital forecourt between all entrances and the public footpaths and road surfaces ;
• dramatically improved quality of Royal Prince Alfred Hospital Precinct
• significant efficiencies and recurring operational economies
In the words of one executive, “
5
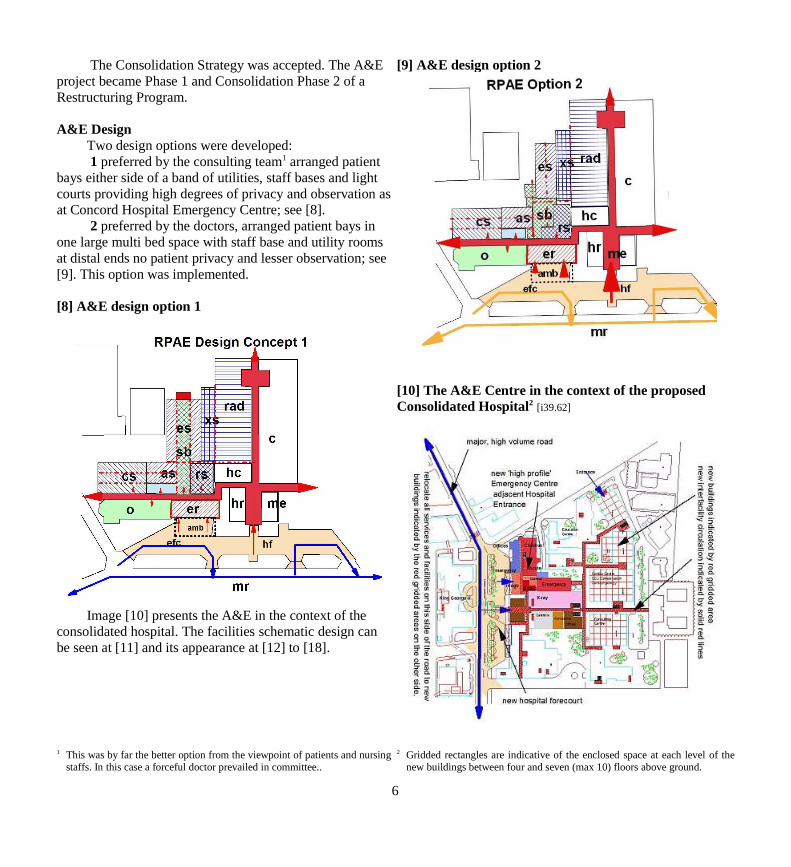
The Consolidation Strategy was accepted. The A&E project became Phase 1 and Consolidation Phase 2 of a Restructuring Program.
A&E Design Two design options were developed: 1 preferred by the consulting team1 arranged patient
bays either side of a band of utilities, staff bases and light courts providing high degrees of privacy and observation asat Concord Hospital Emergency Centre; see [8].
2 preferred by the doctors, arranged patient bays in one large multi bed space with staff base and utility rooms at distal ends no patient privacy and lesser observation; see [9]. This option was implemented.
[8] A&E design option 1
Image [10] presents the A&E in the context of the consolidated hospital. The facilities schematic design can be seen at [11] and its appearance at [12] to [18].
1 This was by far the better option from the viewpoint of patients and nursingstaffs. In this case a forceful doctor prevailed in committee..
[9] A&E design option 2
[10] The A&E Centre in the context of the proposed Consolidated Hospital2 [i39.62]
2 Gridded rectangles are indicative of the enclosed space at each level of thenew buildings between four and seven (max 10) floors above ground.
6

[11] RPA A&E Design – Floor Plan 1993
7

[12] A&E Entrance at 1993
[13] A&E Entrance as designed 1994 Forecourt design
[14] Emergency Forecourt – entrance at 1998
[15] Emergency forecourt 1998
8

[15] A&E in Consolidated Hospital 1993
[i420.102]g
[16] RPA Consolidated ca 2004 cf [10]
[17] RPA Entrance forecourt 1993
[18] RPA Entrance forecourt at 1998
9
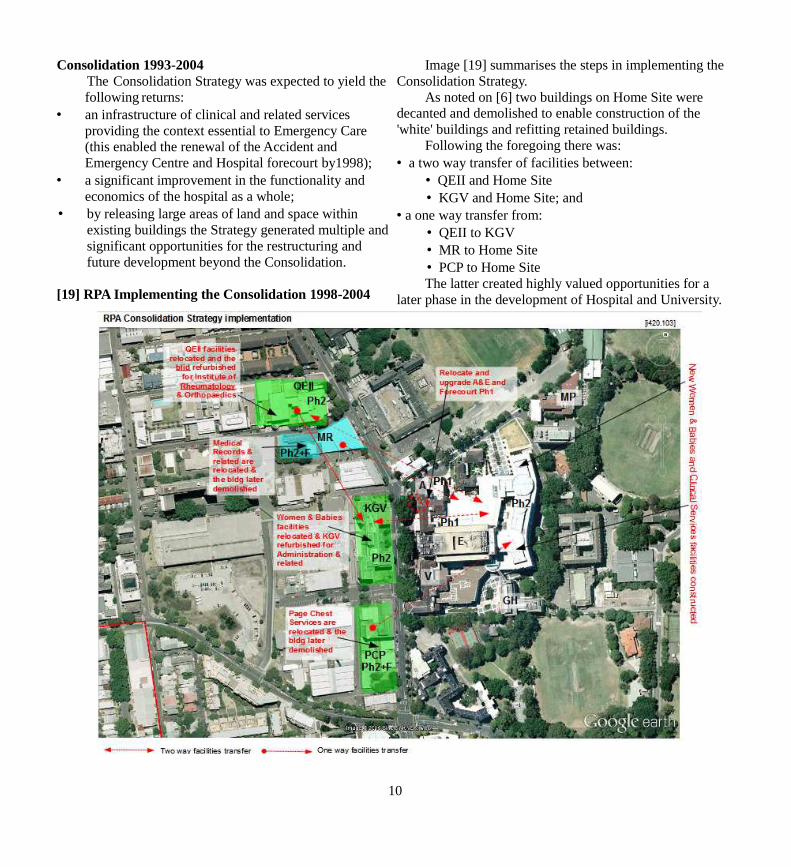
Consolidation 1993-2004The Consolidation Strategy was expected to yield the following returns:
• an infrastructure of clinical and related services providing the context essential to Emergency Care (this enabled the renewal of the Accident and Emergency Centre and Hospital forecourt by1998);
• a significant improvement in the functionality and economics of the hospital as a whole;
• by releasing large areas of land and space within existing buildings the Strategy generated multiple andsignificant opportunities for the restructuring and future development beyond the Consolidation.
[19] RPA Implementing the Consolidation 1998-2004
Image [19] summarises the steps in implementing the Consolidation Strategy.
As noted on [6] two buildings on Home Site were decanted and demolished to enable construction of the 'white' buildings and refitting retained buildings.
Following the foregoing there was:• a two way transfer of facilities between:
• QEII and Home Site• KGV and Home Site; and
• a one way transfer from:• QEII to KGV • MR to Home Site • PCP to Home SiteThe latter created highly valued opportunities for a
later phase in the development of Hospital and University.
10
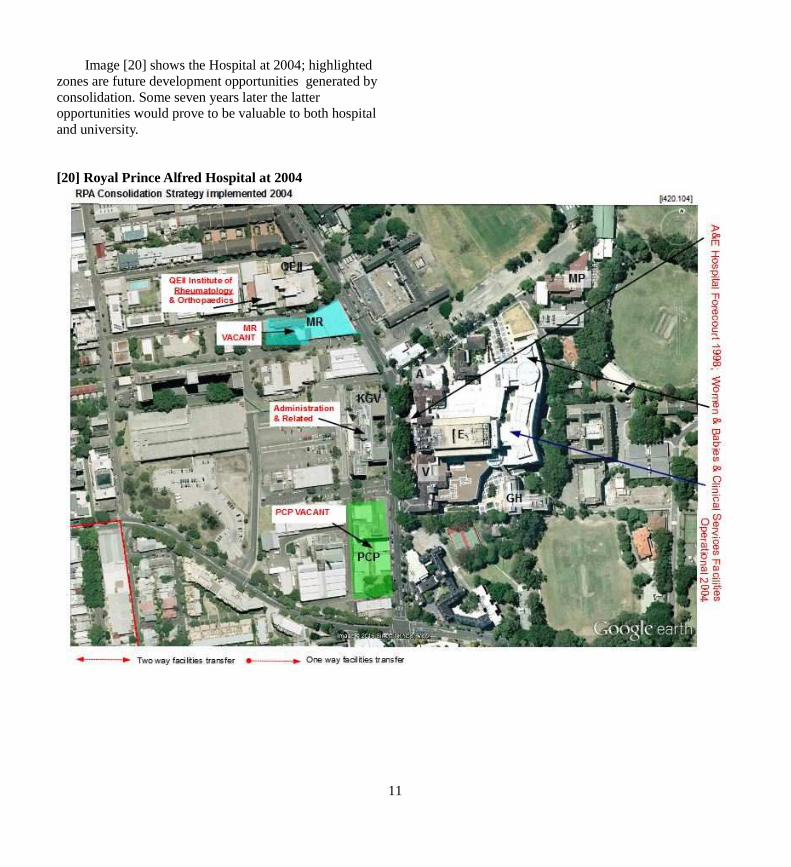
Image [20] shows the Hospital at 2004; highlighted zones are future development opportunities generated by consolidation. Some seven years later the latter opportunities would prove to be valuable to both hospital and university.
[20] Royal Prince Alfred Hospital at 2004
11
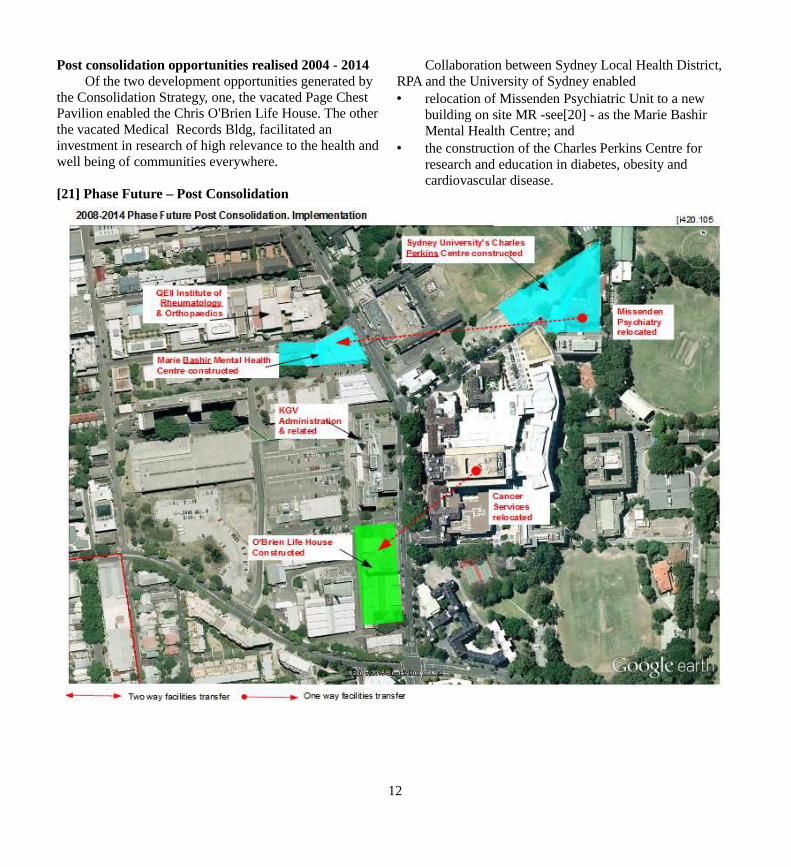
Post consolidation opportunities realised 2004 - 2014Of the two development opportunities generated by
the Consolidation Strategy, one, the vacated Page Chest Pavilion enabled the Chris O'Brien Life House. The other the vacated Medical Records Bldg, facilitated an investment in research of high relevance to the health and well being of communities everywhere.
[21] Phase Future – Post Consolidation
Collaboration between Sydney Local Health District, RPA and the University of Sydney enabled • relocation of Missenden Psychiatric Unit to a new
building on site MR -see[20] - as the Marie Bashir Mental Health Centre; and
• the construction of the Charles Perkins Centre for research and education in diabetes, obesity and cardiovascular disease.
12

Thus by 2014 the 'future opportunities' generated by the consolidation of the Hospital were taken up:
• PCP (Page Chest Pavilion) was demolished and replaced by the Chris O'Brien Life House, an interdisciplinary Cancer Care Centre [22];
https://www.mylifehouse.org.au/About_Lifehouse/
22] Chris O'Brien Life House
• MP (Missenden Psychiatric Unit) was relocated to MRto become RPA's Marie Bashir Centre for Community Mental Health [23];
[23] Marie Bashir Community Mental Health Centre
• the adjacent car-park and MP site were conjoined to realise Sydney University's Charles Perkins Centre for interdisciplinary research into diabetes, and obesity and cardiovascular disease [24]
http://sydney.edu.au/perkins/about/our-approach.shtml•
[24] Charles Perkins Centre
13
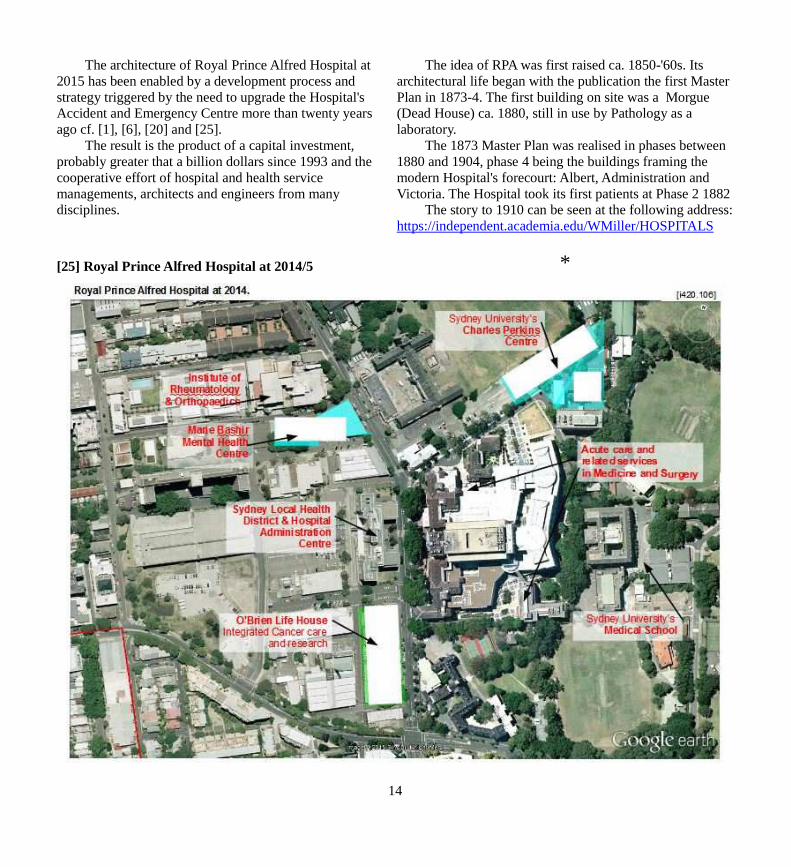
The architecture of Royal Prince Alfred Hospital at 2015 has been enabled by a development process and strategy triggered by the need to upgrade the Hospital's Accident and Emergency Centre more than twenty years ago cf. [1], [6], [20] and [25].
The result is the product of a capital investment, probably greater that a billion dollars since 1993 and the cooperative effort of hospital and health service managements, architects and engineers from many disciplines.
[25] Royal Prince Alfred Hospital at 2014/5
The idea of RPA was first raised ca. 1850-'60s. Its architectural life began with the publication the first Master Plan in 1873-4. The first building on site was a Morgue (Dead House) ca. 1880, still in use by Pathology as a laboratory.
The 1873 Master Plan was realised in phases between 1880 and 1904, phase 4 being the buildings framing the modern Hospital's forecourt: Albert, Administration and Victoria. The Hospital took its first patients at Phase 2 1882
The story to 1910 can be seen at the following address:https://independent.academia.edu/WMiller/HOSPITALS
*
14

















