29
9310-TC-PBM Hot Topic: Reassessing the Role of Plasma October 24, 2011 10:30 AM - 12:00 PM

9310-TC-PBM Hot Topic: Reassessing the Role of Plasma October 24, 2011 10:30 AM - 12:00 PM

Event Outline
Event Title: 9310-TC-PBM Hot Topic: Reassessing the Role of Plasma
Event Date: Monday, October 24, 2011
Event Time: 10:30 AM to 12:00 PM
Presenters: Bryan Cotton, Lawrence Goodnough, Ravi Sarode
Speaker Presentation
Bryan Cotton Role of Plasma in Trauma
Lawrence Goodnough Emergency Management of Warfarin-Associated Coagulopathy in Patients
Ravi Sarode A Randomized Clinical Trial Comparing Beriplex with FFP

Event Faculty List
Event Title: 9310-TC-PBM Hot Topic: Reassessing the Role of Plasma
Event Date: Monday, October 24, 2011
Event Time: 10:30 AM to 12:00 PM
Director Pampee Young MD, PhD Vanderbilt University Medical Center 1161 21st Avenue, South C3321 MCN Nashville, TN 37232 [email protected] Disclosures: Yes
Speaker Bryan Cotton MD, MPH Center for Translational Injury Research-University of Texas 6410 Fannin Street 1100 UPB Houston, TX 77494 [email protected] Disclosures: Nothing to Disclose
Speaker Lawrence Goodnough MD Stanford University Medical Center 300 Pasteur Drive Rm. H-1402 MC 5626 Stanford, CA 94305 [email protected] Disclosures: Yes
Speaker Ravi Sarode MD UT Southwestern Medical Center 5323 Harry Hines Boulevard Dallas, TX 75390 [email protected] Disclosures: Yes

2011-09-28
1
Emergency management of warfarin-associated coagulopathy in patients
Lawrence Tim Goodnough, MDProfessor of Pathology and Medicine Stanford UniversityDirector, Transfusion Service Stanford University Medical Center Stanford, CA
How we treat warfarin-associated coagulopathy in patients with
intracerebral hemorrhage.
Goodnough LT, Shander AS. Blood 2011;117(23):6091-9
The effect of plasma transfusion on morbidity and mortality: a systematic
review and meta-analysis
• Very-low quality evidence suggests that plasma infusion in the setting of massive transfusion for trauma patients may be associated with a reduction in the risk of death and multiorgan failure.
• A survival benefit was not demonstrated in most other transfusion populations.
Murad et al. Transfusion 2010; 50:1370-1383

2011-09-28
2
A. B.
Fig. 4. Should plasma transfusion (vs. no plasma) be used for patients with warfarin anticoagulation–related intracranial hemorrhage? (A) Percentage of panel recommending for or against this intervention. (B) Quality of evidence supporting this intervention, as rated by the panel.
Evidence-Based Practice Guidelines for Plasma Transfusion
• ‘Efficacy of plasma to reduce mortality outweighed its potential risks (e.g. TRALI, inventory) in warfarin-treated patients with ICH.’*
* However, the level of recommendation and grading of evidence as ‘low’ may be attributed to ‘too little too late’ (type II error)
Roback JD, et al. Transfusion 2010;50:1227-1239
Variability in Treatment of Patients on Oral Anticoagulants with Spontaneous ICH
1 Hospital 4 Other Hospitals
Plasma 4 of 7 (60%) 2 of 34 (6%)
PCC 19 of 26 (73%) 1 of 37 (3%)
No Action Taken 2 of 26 (8%) 23 of 40 (57%)
Sjoblom et al Stroke 2001;32:2567

2011-09-28
3
ED Management and INR Reversal in Warfarin-Associated Coagulopathy
INR Reversed at 24 h
No (n=12) Yes (n=57)Median Median P
Characteristic (25% to 75%) (25% to 75%) ValueDoor to CT time 65 (30 to 90) min. 40 (25 to 85) min. 0.5CT to FFP time* 210 (100 to 375) min. 90 (60 to 205) min. 0.02Dose of FFP 2 (1 to 5) units 4 (2 to 6) units 0.1CT to Vit. K time 245 (37 to 361) min. 87 (25 to 210) min. 0.2Any Vit. K given 58% 81% 0.1
*First Dose
Goldstein, et al Stroke 2006;37:151-5.
Plasma Therapy in Successful Reversal of Warfarin Anticoagulation in Patients with ICH
Barrier Estimated Time Needed
Patient blood type must be determined Up to 60 minutes
Plasma units must be thawed 30-45 minutes
Plasma volume requires careful management
to avoid circulatory overload 30 minutes per unit
Plasma dosing is underestimated
Liquid AB plasma available? 5 minutes
Thawed A plasma available? 5 minutes
Physiologic basis for transfusion therapy in hemorrhagic disorders
“As an initial infusion, 1000mL of normal plasma to an average sized adult is usually required to produce minimum hemostatic levels.”
Paul Aggler
Transfusion 1961;1:71-86
2011-09-28
4
Care of patients receiving long-term anticoagulant therapy
“Volume of plasma required for reversal is almost invariably too large to be infused safely”
Sam Schulman
N Engl J Med 2003;349:675-683.
Use of Factor IX complex in Warfarin-Related ICH
• PT greater than 17 sec. patients (n=13) with:• Randomized to FFP alone (n=8) vs. FFP + PCC
(n=5)• PT, INR Q 2H x 7. Target INR 1.3• Vitamin K 10mg sq• Plasma infusion, maximum rate tolerated
CVP monitoring 2-3 liters
Boulis et al. Neurosurgery. 1999;45(5):1113-8.

2011-09-28
5
Toward rational fresh frozen plasma transfusion: The effect of plasma transfusion
on coagulation test results.
• Based on the assumption that 30% factor level is adequate, an INR of 1.8 represents minimally acceptable level of coagulation
Holland LL, Brooks JP. Am J Clin Pathol. 2006 Jul;126:133-9.
Predicted FFP transfusion volume, dose, and expected Factor increment for various
target INR values
Holland LL, et al. Am J Clin Pathol 2006;126:137

2011-09-28
6
Efficacy of standard dose and 30 ml/kg fresh frozen plasma in correcting laboratory parameters
of haemostasis in critically ill patients
• Current guidelines on the use of FFP result in predictably small increments in coagulation factors in critically ill patients and should be reviewed.
• 12.5 ml/kg of FFP lead to relatively small, inadequate increments in factor levels and 30 ml/kg of FFP adequately corrected all factors levels.
• FFP is standardized only for fibrinogen and Factor VIII content.
Chowdhury et al. Br J Haematol 2004;125:69-73
Urgent reversal of warfarin with prothrobmin complex concentrate:
where are the evidence-based data (Editorial)?
• No PCC has received approval from FDA for reversal of elevated INR’s or warfarin-related bleeding
• No 4 Factor PCC currently available in USProplex-T (Baxter) removed 2005.
• Does reversal of warfarin-effect require repletion of all four (II,VII, IX, X) or selected Vitamin K-dependent factors?
• INR correction after rVIIa administration probably occurs independently of its hemostatic activity: generation of thrombin ‘burst’ on surface of activated platelets.
CM Kessler. J Thromb Haemostas 2006;4:963-966
Role of Prothrombin Complex Concentrates in Reversing Warfarin Anticoagulation: A
Review of the Literature
• In the US, FFP is considered the standard of care for warfarin reversal
• PCC’s offer an alternative to FFP
• However, few prospective trials
• In comparison studies, PCC’s found more effective for INR correction
• Evidence-based treatment guidelines needed
Leissinger CA, et al. Am J Hematol 2008; 83:137-143.
2011-09-28
7
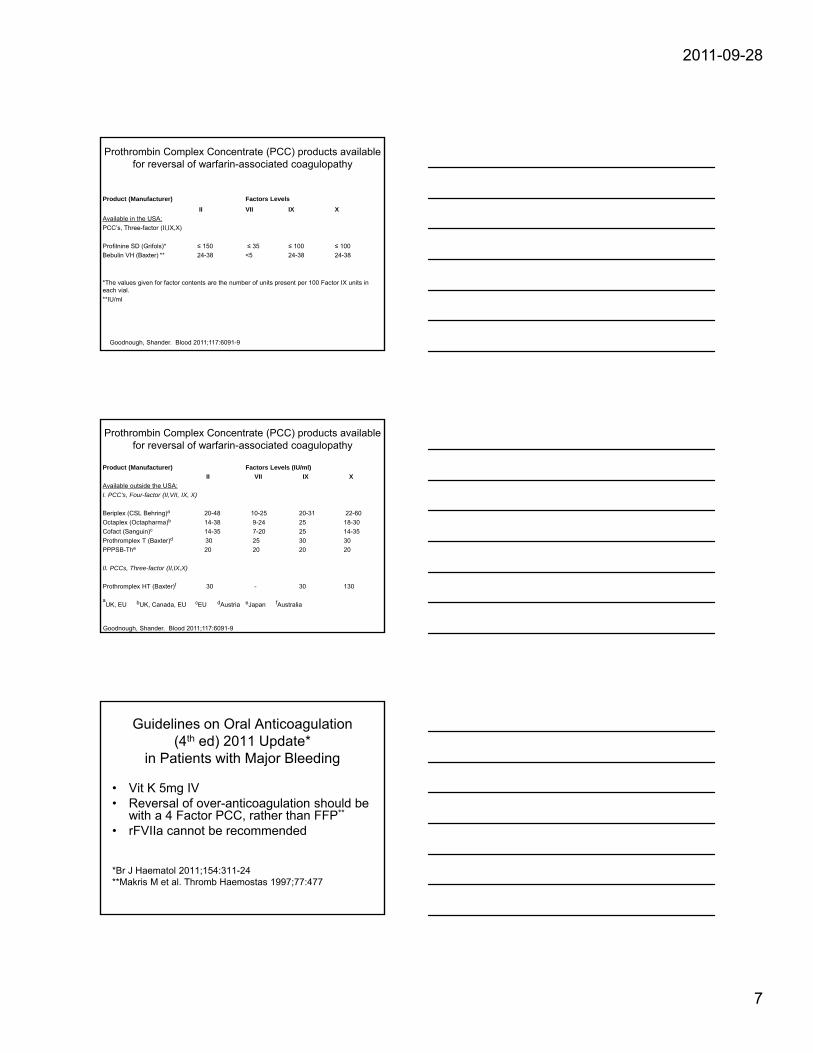
Prothrombin Complex Concentrate (PCC) products available for reversal of warfarin-associated coagulopathy
Product (Manufacturer) Factors Levels
II VII IX X
Available in the USA:
PCC’s, Three-factor (II,IX,X)
Profilnine SD (Grifols)* ≤ 150 ≤ 35 ≤ 100 ≤ 100
Bebulin VH (Baxter) ** 24-38 <5 24-38 24-38
*The values given for factor contents are the number of units present per 100 Factor IX units in each vial.
**IU/ml
Goodnough, Shander. Blood 2011;117:6091-9
Prothrombin Complex Concentrate (PCC) products available for reversal of warfarin-associated coagulopathy
Product (Manufacturer) Factors Levels (IU/ml)
II VII IX X
Available outside the USA:
I. PCC’s, Four-factor (II,VII, IX, X)
Beriplex (CSL Behring)a 20-48 10-25 20-31 22-60
Octaplex (Octapharma)b 14-38 9-24 25 18-30
Cofact (Sanguin)c 14-35 7-20 25 14-35
Prothromplex T (Baxter)d 30 25 30 30
PPPSB-The 20 20 20 20
II. PCCs, Three-factor (II,IX,X)
Prothromplex HT (Baxter)f 30 - 30 130
aUK, EU bUK, Canada, EU cEU dAustria eJapan fAustralia
Goodnough, Shander. Blood 2011;117:6091-9
Guidelines on Oral Anticoagulation (4th ed) 2011 Update*
in Patients with Major Bleeding
• Vit K 5mg IV• Reversal of over-anticoagulation should be
with a 4 Factor PCC, rather than FFP**
• rFVIIa cannot be recommended
*Br J Haematol 2011;154:311-24**Makris M et al. Thromb Haemostas 1997;77:477
2011-09-28
8
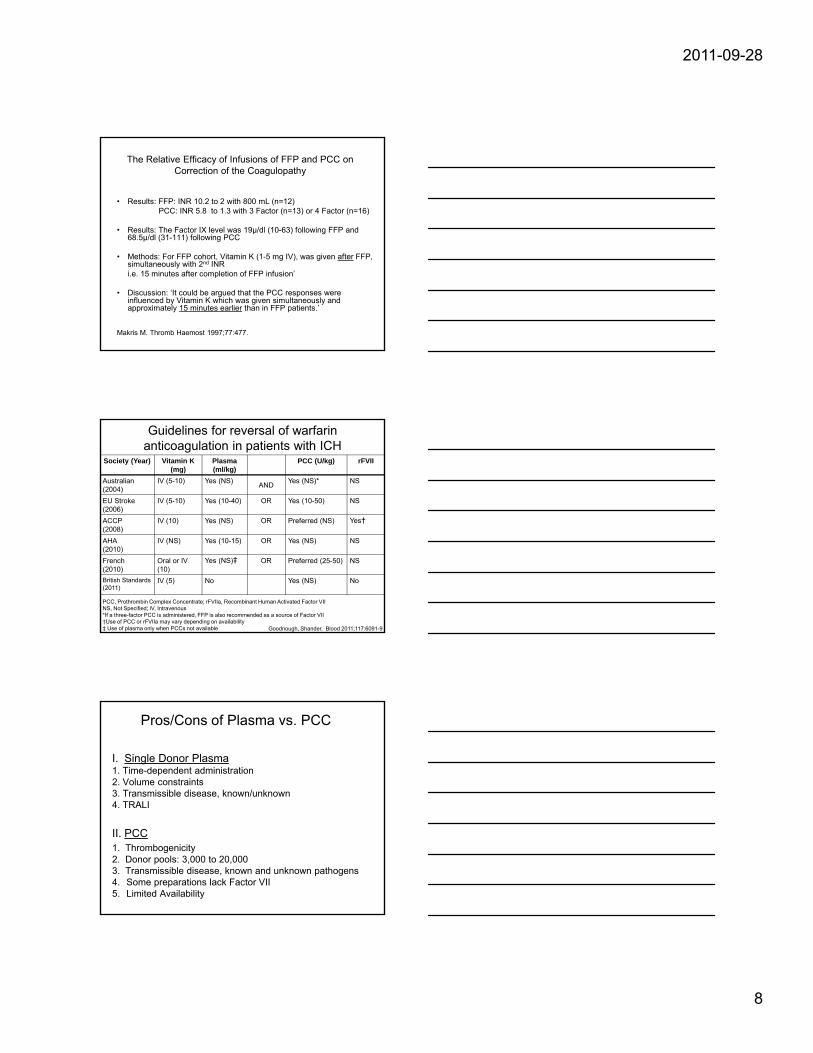
The Relative Efficacy of Infusions of FFP and PCC on Correction of the Coagulopathy
• Results: FFP: INR 10.2 to 2 with 800 mL (n=12)PCC: INR 5.8 to 1.3 with 3 Factor (n=13) or 4 Factor (n=16)
• Results: The Factor IX level was 19µ/dl (10-63) following FFP and 68.5µ/dl (31-111) following PCC
• Methods: For FFP cohort, Vitamin K (1-5 mg IV), was given after FFP, simultaneously with 2nd INR i.e. 15 minutes after completion of FFP infusion’
• Discussion: ‘It could be argued that the PCC responses were influenced by Vitamin K which was given simultaneously and approximately 15 minutes earlier than in FFP patients.’
Makris M. Thromb Haemost 1997;77:477.
Guidelines for reversal of warfarin anticoagulation in patients with ICH
Society (Year) Vitamin K (mg)
Plasma (ml/kg)
PCC (U/kg) rFVII
Australian(2004)
IV (5-10) Yes (NS)AND
Yes (NS)* NS
EU Stroke (2006)
IV (5-10) Yes (10-40) OR Yes (10-50) NS
ACCP (2008)
IV (10) Yes (NS) OR Preferred (NS) Yes†
AHA(2010)
IV (NS) Yes (10-15) OR Yes (NS) NS
French(2010)
Oral or IV (10)
Yes (NS)‡ OR Preferred (25-50) NS
British Standards (2011)
IV (5) No Yes (NS) No
PCC, Prothrombin Complex Concentrate; rFVIIa, Recombinant Human Activated Factor VIINS, Not Specified; IV, Intravenous*If a three-factor PCC is administered, FFP is also recommended as a source of Factor VII†Use of PCC or rFVIIa may vary depending on availability‡ Use of plasma only when PCCs not available Goodnough, Shander. Blood 2011;117:6091-9
Pros/Cons of Plasma vs. PCC
I. Single Donor Plasma1. Time-dependent administration2. Volume constraints3. Transmissible disease, known/unknown4. TRALI
II. PCC1. Thrombogenicity2. Donor pools: 3,000 to 20,0003. Transmissible disease, known and unknown pathogens4. Some preparations lack Factor VII5. Limited Availability

2011-09-28
9
How We Treat Warfarin-Associated Coagulopathy in Patients with ICH
• Blood type and screen • Vitamin K 10mg IV over 30 min, Q12h• Plasma therapy: 15-30 mL/kg, or 4-8 units. First
units should be thawed ‘A’ plasma or liquid AB plasma
• INR goal: less than 1.7• 3 factor PCC is off-label, approved only for
replenishment of Factor IX.
How We Treat Warfarin-Associated Coagulopathy in Patients with ICH
• In some countries, 4 Factor PCC is available/approved.
Doses 25 IU/kg in therapeutic range (TR)
Doses 35-50 IU/kg greater than TR
• rFVIIa not approved in this setting. 2 mg IV provides 20-40 microgm/kg for 100 kg to 50 kg patients
• rFVIIa: risks of arterial thrombosis

1
Ravi Sarode, MD
Coordinating PI
Director, Transfusion Medicine and
Reference Hemostasis Laboratory
UT Southwestern Medical Center,
Dallas, TX
Warfarin Use and Bleeding Complications in the US
2-3 million patients on warfarin for hypercoagulablestates, stroke and cardiac conditions
Major side effect is bleeding
15-20% per year 1
1-3% life-threatening and fatal2
Upto 2% suffer ICH/SDH with up to 79% mortality3
1.5% (conservative estimate) suggest ~ 45,000 major bleeds per year requiring rapid reversal
Another 0.3% require urgent reversal for surgery
1. Beyth et al, Am J med, 1998, 2. Wintzen et al, Ann Neuro 1984, 3. Mathiesen et al Acta Neuro Scan, 1995

2
INR Above Therapeutic Range But <5.0 With No Significant Bleeding
2008
Lower or omit dose
Frequent monitoring
Resume warfarin at lower dose
If minimally above therapeutic range – no dose reduction
(Grade 1C)
INR >5.0 - <9.0 But No Significant Bleeding
2008 2004
Omit one or two doses Same
More frequent monitoring Same
Resume warfarin at lower dose Same
If increased risk of bleeding omit dose and give VK1 1-2.5 mg Oral
VK1: <5 mg oral
Rapid reversal (<24 hrs) for urgent surgery – VK1 <5 mg oral.
If still high, give additional VK1 1-2 mg oral
VK1 2.5-5– if still high 1-2 mg oral
(Grade 1C) (Grade 2C)
INR >9.0 But No Significant Bleeding
2008 2004
Hold warfarin Same
VK1 higher dose 2.5-5.0 mg oral with expectation that it will reduce
substantially within 24-48 hrsVK1 5-10 mg oral
More frequent monitoring Same
If necessary give additional VK1 Same
Resume VKA at lower dose Same
(Grade 1 B) (Grade 2C)
3
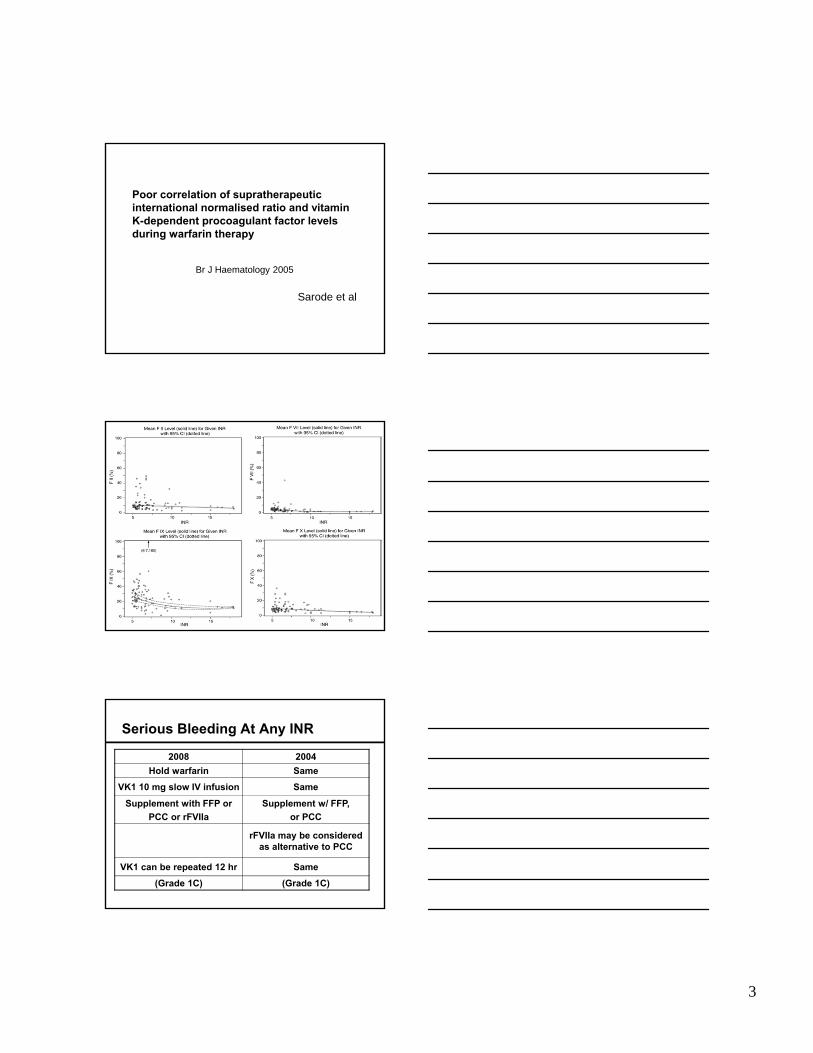
Poor correlation of supratherapeutic international normalised ratio and vitamin K-dependent procoagulant factor levels during warfarin therapy
Sarode et al
Br J Haematology 2005
Serious Bleeding At Any INR
2008 2004
Hold warfarin Same
VK1 10 mg slow IV infusion Same
Supplement with FFP or
PCC or rFVIIa
Supplement w/ FFP,
or PCC
rFVIIa may be considered as alternative to PCC
VK1 can be repeated 12 hr Same
(Grade 1C) (Grade 1C)
4
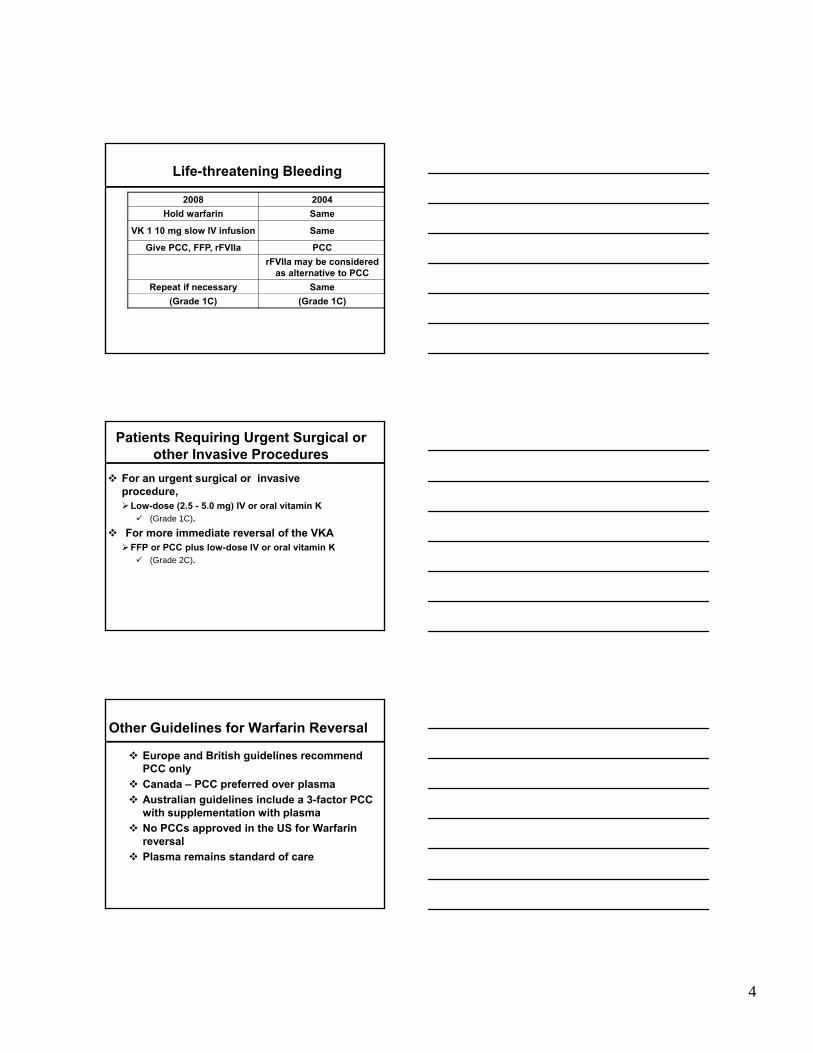
Life-threatening Bleeding
2008 2004
Hold warfarin Same
VK 1 10 mg slow IV infusion Same
Give PCC, FFP, rFVIIa PCC
rFVIIa may be considered as alternative to PCC
Repeat if necessary Same
(Grade 1C) (Grade 1C)
Patients Requiring Urgent Surgical or other Invasive Procedures
For an urgent surgical or invasive procedure,Low-dose (2.5 - 5.0 mg) IV or oral vitamin K (Grade 1C).
For more immediate reversal of the VKA FFP or PCC plus low-dose IV or oral vitamin K (Grade 2C).
Other Guidelines for Warfarin Reversal
Europe and British guidelines recommend PCC only
Canada – PCC preferred over plasma
Australian guidelines include a 3-factor PCC with supplementation with plasma
No PCCs approved in the US for Warfarin reversal
Plasma remains standard of care

5
Rapid Reversal Critical
Retrospective study of warfarin related ICH in 69 patients
Multivariate analysis showed shorter time to plasma transfusion was the most important determinant of INR correction
Every 30 minutes delay for the first dose of plasma was associated with 20% decreased odds of INR correction within 24 hours (OR 0.8;95% CI 0.63-0.99)
Goldstein, Stroke 2006
Other Studies
INR correction was 4.6 times faster (p=<0.001) and extent of INR correction was greater (p=<0.05) with PCC than FFP in ICH. PCC patients had less clinical deterioration. (1)
Rapid reversal with PCC associated with lower incidence of intracerebral hematoma enlargement as compared with FFP. (2)
1. Fredriksson et al, Stroke, 1992; 2. Yasaka et al, Thromb Hemost, 2003
Comparison Between Plasma and PCC
Plasma PCC
Specificity of therapy
Contains all clotting factors (and other plasma proteins not required for warfarin reversal).
Contains specific VKDF (II, VII, IX and X) including PC and PS.
Volume infused At 10-15 cc/kg for 100 kg patient, 1000-1500 cc (4-6 units of Plasma)
At 25-50 U/kg for 100 kg patient 2500-5000U; max. volume 100-200 cc
Time required 2 - 8 hours < 5 minutes to prepare and less than 10 minutes to infuse
Onset of action (INR reduction)
Hours from the time of infusion
Less than 15 minutes

6
Side Effects
Plasma PCCTACO 1:100-1000, especially in
elderly patients with cardiac problems
None, well tolerated
TRALI 1:5,000 to 1:10,000
The commonest cause of transfusion related death
Purified clotting factors,
no Ig - no risk of TRALI
Allergic reactions
Very common: 5-20% Uncommon, since there are no other proteins
Risk of disease transmission
Relatively higher, because plasma is not treated to eliminate any potential viruses
Extremely low, due to heat treatment & nanofiltration to remove known and unknown viruses
Types of PCCs
Activated (aPCC)FEIBA
Non-activated PCC4-factor PCC – all VKDF including PC and PS
(Beriplex and Octaplex)
3-factor PCC – poor FVII content and probably no PC and PS
PCC in the US
Only 3-factor PCCs availableProfilnine (Grifols)
Bebulin VH (Baxter)
Both have very low FVII (<35 U/100 U of FIX) and contain no protein C and S

7
Thrombosis and PCC
Non-activated PCC originally used for hemophilia B
Given daily for days
FII/X long half lives-cumulative effects
aPCC used in Hemophilia A and B with inhibitorscontain FVIIa and Xa
continued use for days prothrombotic
PCC for warfarin reversal one or two doses
Suboptimal effect of a three-factor PCC(Profilnine-D) In correcting supratherapeutic
INR due to warfarin overdose
Holland, Warkentin, Refaai, Crowther, Johnston and Sarode
Transfusion 2009
Correction of ST- INRs
After PCC After TP
Therapy Initial INR INR
% pts with INR
<3.0INR
% pts with INR
<3.0 pValue
TP alone controls
(n = 42)
9.4 (5.1-9.4)
NA N/A 2.3 (1.2-5.0)
62
PCC Low Dose ( n=23) PCC Highdose (n=17)
9.0 (5.2-15.0)
4.6(1.4-15.0)
55 2.1 (1.6-3.3)
89 0.01
8.6 (5.3-15.0)
4.7(1.4-15.0)
43 2.0 (1.3-3.2)
93 <0.01
Difference NS NS NS NS p ≤ 0.01

8
Mean Pre/post-therapy Factor Levels
U/mL FII FVII F IX FX
Pre/Post Pre/Post Pre/Post Pre/Post
PCC (n=8)
0.05 / 0.53 0.05 / 0.10 0.09 / 0.26 0.06 / 0.33
PCC+TP(n=5)
0.07 / 0.58 0.02 / 0.24 0.16 / 0.50 0.05 / 0.53
p Value 0.41 0.001 0.15 0.47
Holland et al Transfusion 2009;49:1171-77
Absolute Factor Increment
N = 13 FII (U/mL)Factor
Increment
FVII (U/mL)Factor
Increment
FIX (U/mL)Factor
Increment
FX (U/mL)Factor
Increment
PCC
(n=8)
0.48 0.05 0.16 0.26
PCC + TP
(n=5)
0.51 0.22 0.34 0.41
P value = 0.41 0.001 0.15 0.47
Holland et al Transfusion 2009;49:1171-77
An open-label, randomized multicenter Phase IIIb study to assess the efficacy, safety and tolerance of BERIPLEX®
P/N compared with plasma for rapid reversal of coagulopathy induced by coumarin derivatives in
subjects with acute major bleeding
Coordinating Investigator: Ravi Sarode, MD
9
Protocol Overview
Primary Objective: To compare the hemostatic efficacy of Beriplex®
P/N and plasma in ceasing spontaneous or
traumatically-induced major bleeding in
subjects who have a deficiency of vitamin K-
dependent coagulation factors II, VII, IX and X,
as well as the proteins C and S, acquired from
oral anticoagulation therapy.
Protocol Overview
Co-Primary Objective To compare the efficacy of Beriplex® P/N and
plasma in rapidly reducing the INR (≤1.3) values between the 2 treatment groups at 30 minutes after end of infusion.
Primary Efficacy Variable:
Hemostatic efficacy with respect to the adequacy of stopping an ongoing major bleed.
Assessed for the entire period of 24 hours from start of the infusion at 3,6 and 24 hours
Include: clinical condition, laboratory values such as Hb, and INR and any additional hemostatic treatments
The primary endpoint, adequacy of cessation of a bleed, will be assessed by a blinded independent Endpoint Adjudication Board as excellent, good, or poor/none, based on pre-specified definitions.

10
To compare the levels of FII, FVII, FIX, FX and PC and PS between the two treatment groups
To compare the hemostatic efficacy of Beriplex®P/N and plasma at 1 and 4 hours after end of infusion
To document the time from the start of infusion until INR correction both in treatment groups
To document the time from randomization until INR correction for both treatment groups
Secondary Efficacy Variables
Secondary Efficacy Variables –contd…
To compare the total number of RBC transfusions and the proportion of subjects with 1 or more transfusions
To compare the use of non-study-prescribed blood products and/or hemostatic agents in both treatment groups,
All cause mortality at 45 days after treatment,
To determine the safety and tolerability of Beriplex®P/N compared to that of plasma.
Other Objectives
To compare INR values between the 2 treatment groups at 30 minutes from the start of infusion.
To evaluate the neurological outcome as assessed by mRS for ICH subjects at discharge.
To compare Investigator assessment of hemostatic efficacy.

11
Study Population
Subjects who have any acquired deficiency of factors II, VII, IX, and X and proteins C and S from oral vitamin K-antagonist therapy and who present with acute major bleeding.
At least 166 subjects (83 per group) who have a non-missing value for the primary endpoint
Approximately 40 sites inside the US and approximately 40 sites outside the US.
Study Population (cont.)
Subjects who have acute major bleeding, defined as one of the following:
Life-threatening or potentially life-threatening
Acute bleeding with Hb fall ≥ 2g/dL
Bleeding requiring blood product transfusion (plasma, red blood cells and other coagulation factor products)
Study Population (cont.)
Bleeding could occur in one of the following locations/manifestations:
Intracranical
Intra-\ retro-peritoneal
Thorax
Joint
Muscle
Gastrointestinal
Genitourinary
12
Inclusion Criteria for Enrollment
Subjects 18 years and older. Received oral vitamin K-antagonist therapy. Have acute major bleeding, defined as one of the following:
Life-threatening or potentially life-threatening Acute bleeding associated with a fall in HB level ≥ 2g/dL Bleeding requiring blood product transfusion
INR 2 within 3 hours before start of study treatment Subjects with acute major bleeding requiring minimal invasive
procedures (e.g. endoscopy, bronchoscopy, central lines) indicated for diagnostic or therapeutic reasons, as long as plasma is intended to be given for treatment of major bleeding
Informed consent has been obtained
Exclusion Criteria
Expected survival < 3 days or surgery in <1 day
Acute trauma for which reversal of VKA alone would not be expected to control or resolve the acute bleeding event.
For patients with ICH: Glasgow coma score < 7 ICH volume > 30cc assessed by ABC/2 SDH : max thickness ≥10mm, midline shift ≥ 5mm SAH : any evidence of hydrocephalus Infratentorial ICH location Epidural hematomas Intraventricular extension of hemorrhage Modified Rankin score of > 3 prior to ICH
Exclusion Criteria (cont.)
History of thrombolytic event, MI, DIC, CVA, TIA, unstable angina pectoris, severe PVD within 3 months of enrollment
Known history APLS Suspected or confirmed sepsis at time of enrollment Use for UFH or LMWH 24 hours prior to enrollment
or expected need 24 hours after start of infusion. Administration of whole blood, plasma or plasma
fractions within two weeks before study entry Note: administration of packed red blood cells
is not an exclusion criterion

13
Exclusion criteria (cont.)
Large blood vessel rupture (e.g. in advanced Ca) Pre-existing progressive fatal disease with life
expectancy of less than two months Known inhibitors to coagulation factors II, VII, IX or X;
hereditary protein C or S deficiency; or HIT Treatment with any other investigational medicinal
product in the last 30 days before study entry Presence or history of hypersensitivity to the study
medication Pregnant women or women who are breast-feeding or
who intend to breast-feed Prior inclusion in this study or any other CSL Behring
sponsored Beriplex study.
Investigator Rating- Excellent (effective)Secondary rating of hemostatic efficacy for
visible and non-visible muscular/skeletal bleeding
Visible bleeding: Cessation of bleeding 3 hours after end of infusion; and no additional coagulation intervention
Non Visible Bleeding: Muscular /skeletal bleeding: Pain relief, no increase in swelling and/ or unequivocal improvement in objective signs of bleeding 3 hour; condition has not deteriorated during 24 h period.
For all types of bleeding: no additional plasma, blood products and/or coagulation factor products required after initial treatment with study drug.
Notes: Any additional diagnostic data for a particular bleeding site, e.g.
nasogastric tube, ultrasound, GI endoscope, or CT scan, will also be taken into account for the overall assessment.
Pain, swelling and signs of bleeding are considered to be typical symptoms in case of muscular/skeletal bleeding and are expected to be present at baseline.
Investigator Rating- Good (effective)
Visible bleeding: Cessation of bleeding between >3 and 6 hours
after start of infusion and no additional coagulation intervention required.
Non Visible Bleeding: Muscular /skeletal bleeding: pain relief or no
increase in swelling or unequivocal improvement in signs of bleeding between >3 and ≤6 hrs; and the condition has not deteriorated during the 24 hr period.
For all type of bleeding: no more than 2 units of additional plasma or blood products and/or coagulation factor products required after
initial treatment with study drug

14
Visible bleeding: Cessation of bleeding > 6 hours after start
of infusion and/or additional intervention required.
Non Visible Bleeding: Muscular /skeletal bleeding: No
improvement by 4 hrs after the end of infusion and/or the condition has deteriorated during the 24 h period.
Investigator Rating- Poor (non-effective)
Investigator Assessment
1 h, 3h, 4h & 6h assessment will be completed for muscular & visual bleeding only
Rating completed at the 24h assessment - Primary Endpoint
Based on clinical condition, additional products given, tarry stool, additional diagnostic data for a particular bleeding site (i.e., nasogastric tube, ultrasound, GI endoscopy, CT scans etc.) will also take into account for the overall assessment.
Uncontrolled bleeding that did not respond to Beriplex or plasma and is related to the underlying disease will be taken into account for the overall assessment
Efficacy Adjudication Board
Chair and 10 members (Trauma surgeon, hematologists, cardiologist and GI)
Charter: Independently and blindly evaluate the
hemostatic efficacy at 24 hours Based on pre-specified variables Effective = excellent and good hemostasis Not-effective = poor or no hemostatic response

15
DSMB
Chair and 3 members including a biostatistician
Charter Protecting safety and well being of pts ensuring ethical conduct evaluation of risk/benefit ratio Review SAEs, deaths and withdrawals in details When appropriate to confirm investigator
assessment of severity and relationship of SAEs
Safety Adjudication Board
One non-voting moderator, and 3 voting members with expertise in hemostasis and cardiology
Since the DSMB was unblinded to the study, SAB was established to independently adjudicate certain SAEs – late bleeding and thrombotic events and deaths
Time windows for virus safety follow-up
Day 10 Calendar day 7 - 11
Day 45 Calendar day 43 – 51
Day 90 Calendar 86 – 96
* where calendar day 1 is the calendar day of the start of the infusion

16
Study Administration Plasma
The dose of plasma will be based on baseline INR, according to the following guideline:
The dose calculation should be based on 100 kg b.w. for subjects weighing more than 100 kg.
Baseline INR Dosage PlasmamL/Kg
2 - <4 10
4 – 6 12
>6 15
Vitamin K1
All subjects will receive vitamin K1* by slow intravenous infusion.
Dose based on the ACCP guidelines or local clinical practice if different (e.g., 2 to 10 mg)
Further doses of vitamin K1 may be required and should be administered according to local clinical practice, e.g., every 12 to 24 hours.
If IV K1 was administered for this bleeding event prior to enrolment, an additional dose will not be needed unless indicated by local clinical practice or the above guidelines.
Beriplex® P/N: Active Ingredients
Beriplex P/N is a lyophilized plasma protein preparation
One box of Beriplex containts: 1 vacuum vial with dried substance & 1 vial with 20 mL water for injection Each Vial Contains
Factor II 640 IU
Factor VII 340 IU
Factor IX 500 IU
Factor X 760 IU
Protein C + Protein S

17
Study Drug AdministrationBeriplex® P/N
The dose of Beriplex® P/N will be calculated based on the factor IX IU/kg and the baseline INR
The dose calculation should be based on 100 kg b.w. for subjects weighing more than 100 kg.
Beriplex® P/N will be administered once. (approx. 3 IU/kg/min, max 210 IU/min or 8.5 mL/min)
Baseline INR
Dosage of Beriplex® P/N
Plasma Ml/kg
2 - <4 25 10
4 – 6 35 12
>6 50 15
Summary
Bleeding study completed
Data being analyzed for FDA submission
Results will be published soon
Stay tuned

















