24
A case of inappropriate ICD shock causing cardiac arrest Dr Darragh Moran, Dr Niall Mahon
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | shannon-briggs |
| View: | 220 times |
| Download: | 0 times |
A case of inappropriate ICD shock causing cardiac arrest
Dr Darragh Moran, Dr Niall Mahon
• 2003 ED MMUH• 16 year old male• Chest discomfort• Abnormal ECG• Normal coronaries
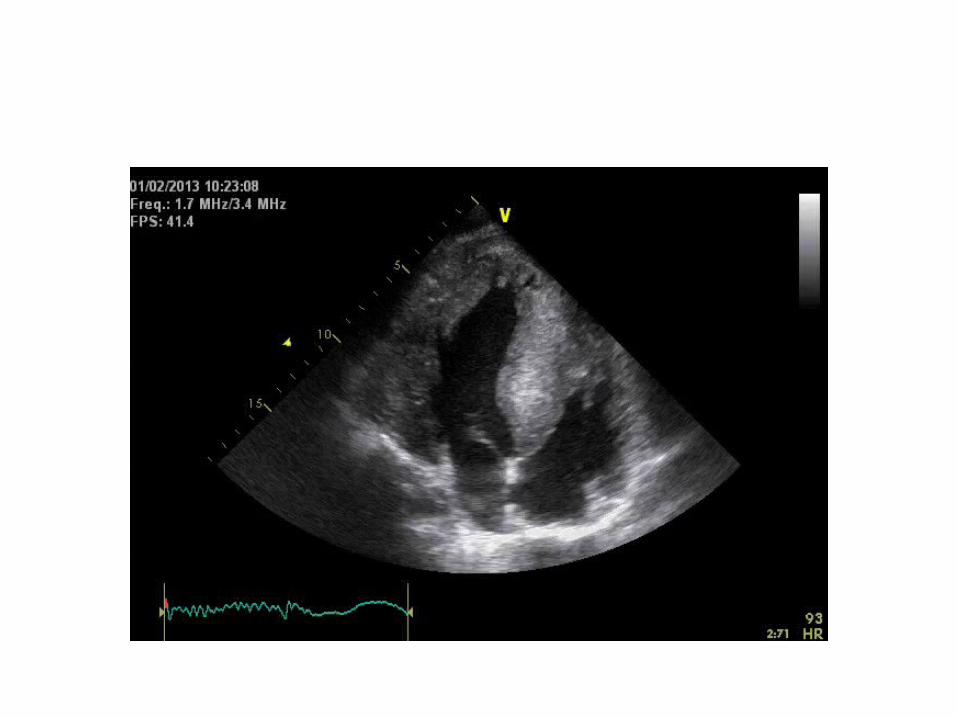
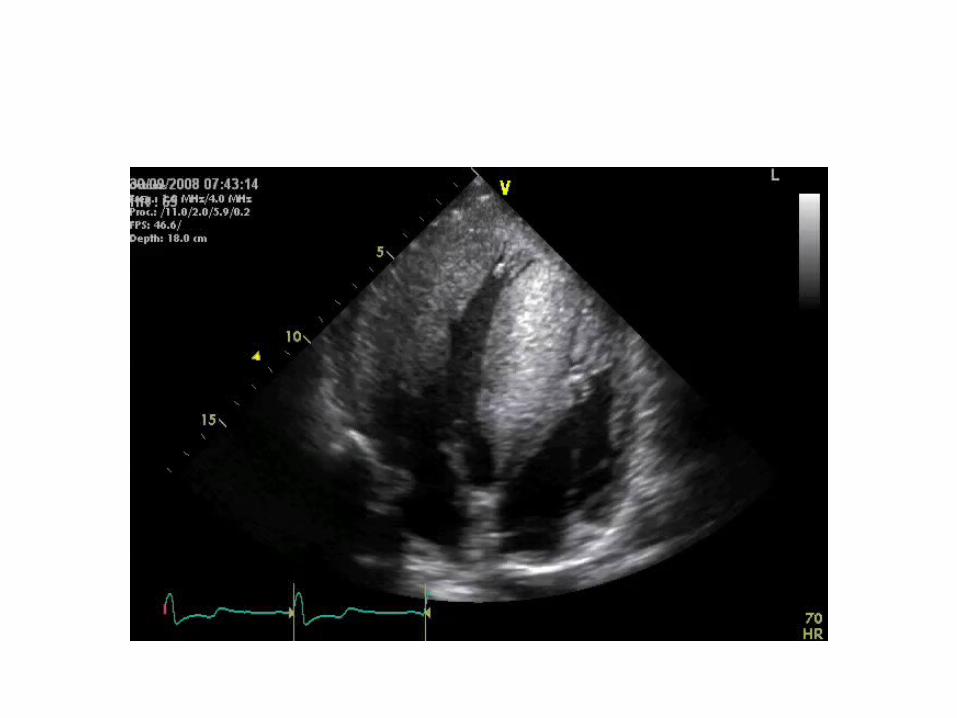
• IVDd of 22mm• No LVOT gradient noted • Satisfactory TMET• Rx betablockade• Normal 24 holter• Episodic left-sided chest discomfort persisted• No family history of SCD
• May 2007, aged 20• ED MMUH – collapse following game of soccer


• No arrhythmia seen during inpatient monitoring
• TMET – drop in blood pressure at peak exertion
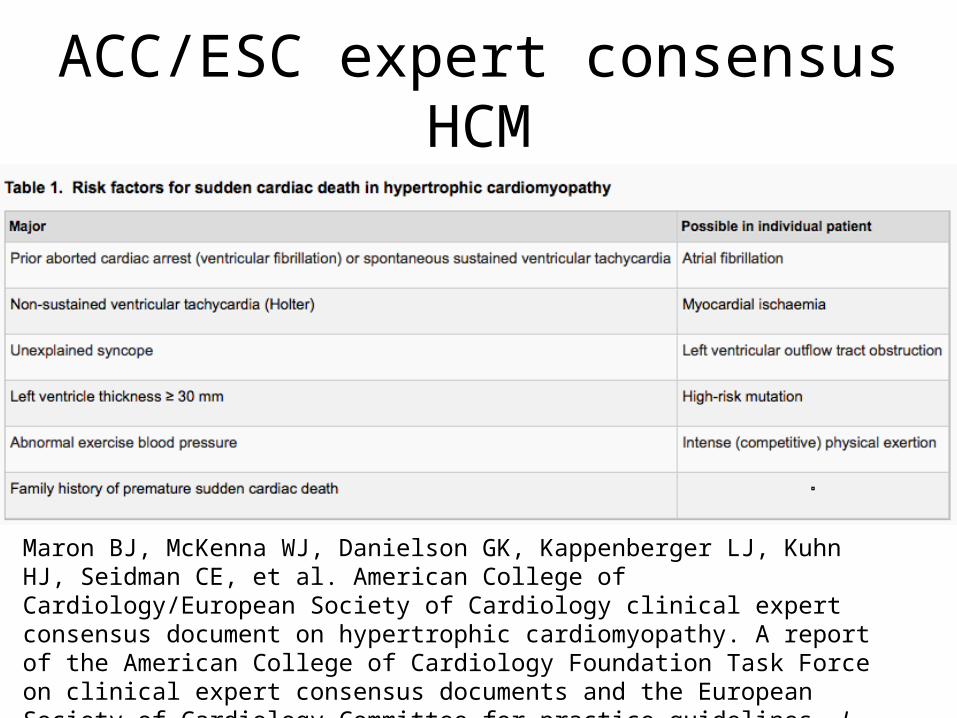
ACC/ESC expert consensus HCM
Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, et al. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on clinical expert consensus documents and the European Society of Cardiology Committee for practice guidelines. J Am Coll Cardiol 2003;42:1687–713.
• 18 days later – ED MMUH• OHCA whilst cycling• Prolonged CPR, external DCCV for VF at scene• GCS 3, intubation and ventilation with inotropic
support• GCS 11 day 2, GCS 15 day 4• Aspiration pnemonia• Post-traumatic amnesia, poor concentration,
attention deficit

• RV lead repositioning• DFT testing – failed 25J and 35J shocks
requiring 200J external rescue shock
• Defibrillation testing was repeated 1 week later. No further T wave oversensing was detected during this interrogation. VF was appropriately sensed by the ICD, both a 20J and 25J shock were unsuccesful, with a 30J rescue shock being required to restore sinus rhythm. The patient was discharged home in the days that followed.
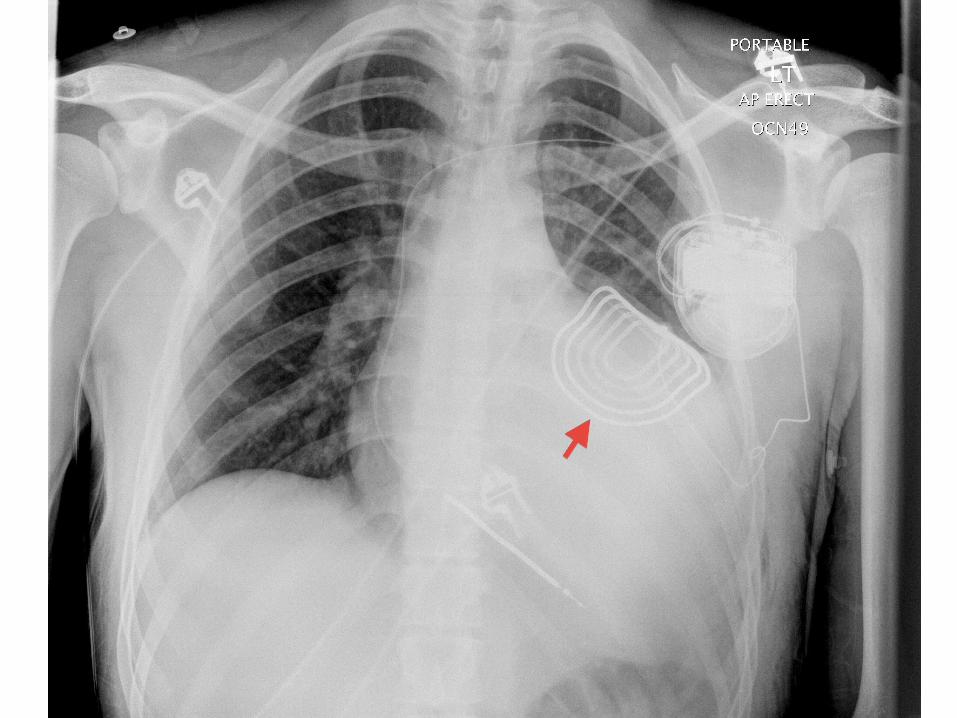
2/12 later, patient returned to hospital as SC array had dislodged whilst swimming
• 2 years of uneventful follow-up• 2009 – threatened pocket erosion of device• Deep submuscular repositioning• Device check April 2010, high impedance
values, >200J, sensitivity of 0.6mV• Admitted for revision and testing of leads and
epicardial patch
• 3/7 later patient returned for DFT testing• 1st 35J shock was unsuccessful, 2nd successfully
restored SR• Long discussion with patient regarding risks
and benefits of further intervention• Discharged home, albeit with unsatisfactory
DFT
• Few months later…• Pain and swelling around device insertion site• Chronic pocket infection• Device explanted

• 7 years of device complications• No ventricular events in that time• High risk of SCD• SC implantable defibrillator offered• AEDs located at workplace and also at the
gym patient attends to reduce risk of SCD• No further symptoms/adverse events to date

















