International Psychogeriatrics (2007), 19:5, 874–891 C 2007 International Psychogeriatric Association doi:10.1017/S1041610206004790 Printed in the United Kingdom A controlled trial of a predominantly psychosocial approach to BPSD: treating causality .............................................................................................................................................................................................................................................................................. Michael Bird, 1 Robert H. Llewellyn Jones, 2,3 Ailsa Korten 1, † and Heather Smithers 3 1 Australian National University and NSW Greater Southern Area Health Service, Australia 2 Northern Sydney Central Coast Area Health Service, Australia 3 Discipline of Psychological Medicine, University of Sydney, Australia †Sadly died during the preparation of this paper. ABSTRACT Background: The adverse effects of behavioral and psychological symptoms of dementia (BPSD) are well described but treatment remains problematical, including overuse of psychotropic medication. This study aims to compare the outcome of two approaches to BPSD, one focusing on causality and using predominantly psychosocial interventions, the other relying predominantly on psychotropic medication. Methods: Thirty-three residential care clients manifesting BPSD who had been referred to a community psychogeriatric service (intervention group) were assessed and treated, with the focus placed on the causes of the behavior and why it was perceived as a problem by nursing staff. Cases were managed primarily by psychosocial means with psychopharmacology as an adjunct. A control group was made up of 22 referrals to an adjacent service, which used primarily psychopharmacology with psychosocial methods as an occasional adjunct. Results: Measures of behavior and staff response showed significant improvement in both groups at two- and five-months’ follow-up. Antipsychotic use in the intervention group decreased over time while in the control group it increased. Service measures showed both groups required approximately the same number of clinical visits but the intervention group experienced fewer medication changes, fewer drug side effects, and all but one case could be treated in situ. Five control group participants spent extended periods as inpatients in a psychogeriatric unit. Minor sampling differences did not affect the results, and neither they nor the nature of the behavior explained the difference in clinical approach. Correspondence should be addressed to: Michael Bird, NSW Greater Southern Area Health Service, PO Box 1845, Queanbeyan, NSW 2620, Australia. Phone +61 2 6124 9874; Fax +61 6299 6363. Email: [email protected]. nsw.gov.au. Received 26 Apr 2006; revision requested 10 Jul 2006; revised version received 5 Dec 2006; accepted 7 Dec 2006. First published online 19 January 2007. 874
1Australian National University and NSW Greater Southern Area Health Service, Australia2Northern Sydney Central Coast Area Health Service, Australia3Discipline of Psychological Medicine, University of Sydney, Australia†Sadly died during the preparation of this paper.
ABSTRACT
Background: The adverse effects of behavioral and psychological symptoms ofdementia (BPSD) are well described but treatment remains problematical,including overuse of psychotropic medication. This study aims to compare theoutcome of two approaches to BPSD, one focusing on causality and usingpredominantly psychosocial interventions, the other relying predominantly onpsychotropic medication.
Methods: Thirty-three residential care clients manifesting BPSD who had beenreferred to a community psychogeriatric service (intervention group) wereassessed and treated, with the focus placed on the causes of the behavior and whyit was perceived as a problem by nursing staff. Cases were managed primarilyby psychosocial means with psychopharmacology as an adjunct. A controlgroup was made up of 22 referrals to an adjacent service, which used primarilypsychopharmacology with psychosocial methods as an occasional adjunct.
Results: Measures of behavior and staff response showed significant improvementin both groups at two- and five-months’ follow-up. Antipsychotic use inthe intervention group decreased over time while in the control group itincreased. Service measures showed both groups required approximately thesame number of clinical visits but the intervention group experienced fewermedication changes, fewer drug side effects, and all but one case could be treatedin situ. Five control group participants spent extended periods as inpatients in apsychogeriatric unit. Minor sampling differences did not affect the results, andneither they nor the nature of the behavior explained the difference in clinicalapproach.
Correspondence should be addressed to: Michael Bird, NSW Greater Southern Area Health Service, PO Box 1845,Queanbeyan, NSW 2620, Australia. Phone +61 2 6124 9874; Fax +61 6299 6363. Email: [email protected]. Received 26 Apr 2006; revision requested 10 Jul 2006; revised version received 5 Dec 2006; accepted 7 Dec2006. First published online 19 January 2007.
874
A predominantly psychosocial approach to BPSD 875
Conclusion: The causality-focused approach appears to be as effective as the morecommon predominantly pharmacological approach, and appears to involvelower human and financial costs.
The effects of behavioral and psychological symptoms of dementia (BPSD)include distress both for the person with dementia and their family carers, and,in cases of early institutionalization (Balestreri et al., 2000), for residential carestaff (Evers et al., 2002; Wood et al., 1999). There is also evidence showing anover-reliance on psychotropic medication to reduce unwanted behavior, despitemodest efficacy and frequent side effects (Herrmann, 2001; Margallo-Lanaet al., 2001; Deberdt et al., 2005). Atypical neuroleptics are the treatment ofchoice for most BPSD among Australian and New Zealand psychogeriatricians(Greve and O’Connor, 2005).
The conceptualization underpinning the approach evaluated in this study isthat there are usually multiple interacting causes of the behavior and differentreasons why it is seen as a problem, which are particular to each case. This meansthat the same behavior will have different causes in different patients, and will beperceived differently by different carers. For example, many interacting factorscan contribute to vocal disruption in dementia, including pain or depression(Cohen-Mansfield and Werner, 1999), overstimulation (Meares and Draper,1999), loneliness (Hallberg et al., 1993), or premorbid characteristics andhistory (Bird, 2005). There is also evidence suggesting that carer/nursing staff orinstitution variables are more important than resident behavior in determiningwhether behavior is seen as a problem (Cole et al., 2000; Moniz-Cook et al.,2000).
This study evaluated an approach in which treatment, whether pharma-cological or psychosocial or both, was tailored to and targeted at causes ofthe problem, including causes of why the behavior was perceived as a problem.This was compared with the outcome of what can be characterized as usual care,i.e. care that relies predominantly on psychotropic medication.
Method
EthicsThe study was approved by the Hornsby Ku-ring-gai Hospital Human ResearchEthics Committee, Sydney.
DesignThis was a naturalistic controlled trial with repeated measures. Participantsreceiving the causality-focused approach (hereafter the intervention group) and
876 M. Bird et al.
participants receiving usual care (the control group) were assessed at baseline,after two months (Time 2) and after five months (Time 3), and comparedaccording to behavior and care staff measures. In addition, data on servicevariables for both groups were compared for a period of nine months, from twomonths before baseline to two months after Time 3.
ParticipantsThe definition of BPSD adopted for this study was “any behavior associatedwith dementia which causes distress or danger to the patient and/or others”(Birdet al., 1998). Participants were required to meet all of the following criteria:
(a) evidence of dementia and/or significant stroke-related cognitiveimpairment based on medical notes in the facility and confirmed bystudy measures;
(b) behaviors of at least one month’s duration (to eliminate acute deliriumas far as possible), which caused significant distress or danger to theresident and/or others;
(c) behaviors which required significant clinical input (individuals withbehaviors which could be resolved by simple interventions in a singlevisit were not included);
(d) a minimum of two months’ residence at their current location (tocontrol for behavior related to recent relocation, which often settlesspontaneously);
(e) informed consent; and,(f) carers/informants.
Because carer and facility variables rather than resident and behaviorvariables frequently determine whether behavior is perceived as “challenging”(Cole et al., 2000; Moniz-Cook et al., 2000), naturalistic referrals were used toensure that facility staff were genuinely concerned and needed help. To minimizebias, consecutive referrals which fitted the above criteria were used, with neitheractive recruitment of cases nor selective exclusion.
The intervention group comprised referrals from residential care to thecommunity psychogeriatric team servicing the Hornsby Ku-ring-gai sector ofthe Northern Sydney Central Coast Area Health Service (NSCCAHS). Thecontrol group consisted of consecutive referrals to two psychogeriatric teamswhich serviced the adjacent Lower North Shore/Ryde sector of NSCCAHS.The staffing, resources and clinical approach were similar for both the controlgroup teams. The catchment populations of all teams were broadly similar interms of socioeconomic status, availability of general practitioners (GPs) andthe types of facilities serviced. Both control group teams had access to thesame psychogeriatric inpatient unit whereas the intervention group had accessto beds in an adult psychiatric unit. Baseline differences between control andintervention groups were controlled for in outcome analyses.
Because this was a trial not of a specific treatment but of a clinical approachwhich, dependent upon causality, would vary case to case, the control condition
A predominantly psychosocial approach to BPSD 877
was defined as usual care. No effort was made to influence the clinical approachof control group clinicians which, consistent with the literature (Deberdt et al.,2005; Greve and O’Connor, 2005) and common practice, was mainly psycho-pharmacological.
Written informed consent was obtained on behalf of all participants withdementia from the responsible family member or guardian. Written consent wasobtained from all staff who completed research measures and, where feasible,from the participants with dementia.
MeasuresInstruments assessing resident and care staff status, the referred behavior, staffresponse to the resident and to the behavior, and psychotropic medicationsprescribed were administered to both groups at baseline, and at two-month(Time 2) and five-month (Time 3) follow-up. It was expected that interventionswould be taking effect by Time 2; Time 3 measurements were undertaken todetermine whether the effects were maintained.
Level of dementia was measured using the Mini-mental State Examination(MMSE) (Folstein et al., 1975), the Clinical Dementia Rating (CDR) (Morris,1993), and an activities of daily living (ADL) measure – the DependenceScale (Stern et al., 1994). Type and dose of psychotropic medications takenby participants over a seven-day period at each time point was recorded.
For between-group comparisons of behavior at all three time points, twomeasures were used. First, the Dementia Behavior Disturbance Scale (DBDS)(Baumgarten et al., 1990) was administered to both groups at all threetime points. Secondly, direct care staff used a seven-point scale at Time 2(Retrospective Perception of Behavior) to record whether they felt the referredbehavior had deteriorated or improved (4 = no change). This measure proved tohave adequate reliability (ICC – intra-class correlation = 0.39) when recoded as“better,” “unchanged,” and “worse,” and using direct behavior monitoring asthe gold standard (Bird et al., 2002).
Staff satisfaction and morale was assessed at baseline using the Satisfaction inNursing Care and Work Scale (Hansson et al., 1995). At all three time points,emotional response to the main referred behavior was assessed on a seven-point scale (Carer Stress Scale) by asking three direct care staff how muchstress it caused them, and senior staff assessed its disruption to the facilityon a five-point scale (Problem Severity). Separate validation studies for thesemeasures, which were created for the study (Bird et al., 2002), showed thatboth had excellent test–retest reliability after an interval of two months: (ICCfor Stress = 0.52; for Severity = 0.66). Consistent with one of the conceptualunderpinnings of the approach evaluated in this study (namely, that caregivervariables impact on whether a given behavior is viewed as a problem), bothscales had only a low to moderate inter-rater reliability (ICC for Stress = 0.29;for Severity = 0.33). Accordingly, for each case, the Stress and Severity scaleswere used with the same staff members rating the same resident at all three timepoints.
878 M. Bird et al.
Attitude to the resident at all three time points was assessed using anAustralianized version of the Strains in Nursing Care Scale (Hallberg andNorberg, 1995; Bird et al., 2002). Principal component analysis with varimaxrotation produced three factors explaining 45% of the variance (Bird et al.,2002). The first factor loaded heavily on items which showed empathy for theresident (e.g. “is lonely,” “is anxious”). The other two factors were negative:one best summarized as regarding the resident as hostile (e.g. “is resistive,” “isaggressive”); the other loading on attributions of selfishness (e.g. “is attentionseeking,” “is ungrateful”).
To minimize respondent bias, all staff measures had full instructions for self-completion of forms so that they could be filled out in private, and then sealedand sent in stamped addressed envelopes for data entry.
For both groups, psychogeriatric service records and residential facilityprogress and doctors’ notes for each participant provided: (a) frequency ofGP and psychogeriatric service or geriatrician visits to the facility to dealwith disturbed behavior; (b) frequency of changes to medication prescribedbecause of the behavior; (c) drug side effects; and (d) hospitalizations becauseof the behavior. These data covered a period of nine months, from twomonths before baseline to two months after Time 3. Pre-baseline data werecollected to enable valid comparisons of the approach to be made betweenthe groups because control group clinicians sometimes adjusted psychotropicmedication on the first visit, before the case was assessed as eligible for thestudy and therefore before consent could be obtained and baseline measuresundertaken. The data after Time 3 were collected as a proxy measure of theeffectiveness of interventions after withdrawal of the intervention group clinicalteam.
Clinical approachFor the intervention group, all cases were assessed and interventions undertakenby 1.2 full time equivalent (FTE) community registered nurses and a 0.5 FTEclinical psychologist. Access was available to a geriatrician or psychogeriatricianwhen medication adjustment was required. The core assumption was thatthe behavior occurred, or occurred at intolerable intensity, for identifiablephysical or medical or psychosocial reasons, and/or was seen as “challenging”by staff exposed to it for identifiable reasons. The role of the interventiongroup clinicians was to work with facility staff to identify and determine whichof these causes of behavior and staff distress were amenable to adjustmentand, collectively, devise an intervention package to address them. Care wastaken to ensure that the package could be implemented realistically giventhe constraints of the situation, including level of impairment of the resident,staffing levels, skills and motivation, and facility resources. Interventions werediverse and usually multifaceted, and might include treating pain or depressionpharmacologically, changing the way staff carried out showering, changing theway staff perceived the resident’s behavior, or a host of other modalities. Byfar the commonest interventions were changing care practices and supportingand educating staff about the resident and causes of the behavior. After Time 3
A predominantly psychosocial approach to BPSD 879
the intervention group specialist clinicians ceased their involvement. Twenty-six(79%) of intervention group cases were treated either entirely or mainly withpsychosocial methods, in nine (27.3%) the approach used was entirely psycho-social.
Although control group services were multi-disciplinary and causality wasaddressed in some cases (e.g. depression), a specific causality-focused approachwas not used. All control cases were treated with psychotropic medicationwhich was prescribed either by the GP or psychogeriatric consultant orregistrar. Psychosocial interventions were provided in addition to medicationfor 18% of control cases but none was entirely managed using psychosocialmethods. Intervention group clinicians took no part in any control groupcases.
In both groups, after the five-month data collection period, the main clinicianresponsible for treatment in each case provided a summary of pharmacologicaland/or psychosocial methods used, supplemented and validated by a searchof psychogeriatric service and residential facility notes. These interventionsummaries, including information about psychotropic medications prescribedbefore baseline and after Time 3, were rated for pharmacological/psychosocialbalance on a five-point scale (1 = “entirely psychosocial intervention” throughto 5 = “entirely pharmacological intervention”) by independent aged-careclinicians (two medical, two nursing, and one allied health) who were blindto the participants’ group status. See Bird et al. (2002) for a more detaileddescription of the clinical procedure, complete case studies for both groups,and a classified list of all psychosocial methods used in the interventiongroup.
Results
Participant flow and follow-upThere were 38 intervention group participants for whom baseline data wereavailable. By Time 2, 13% had been lost to death, relocation or loss ofinformants, leaving 33 with useable data (i.e. with at least one set of outcomemeasures). The attrition rate for the control group sample (n = 29) from baselineto Time 2 was 24%, leaving 22 with useable data. By Time 3 the survivingsample was 29 for the intervention group (attrition from baseline 24%), and 16for the control group (attrition from baseline = 45%). The difference in attritionrates between groups represents a greater proportion of control participantsdying or being moved to a specialist psychogeriatric in-patient unit (PGU) formanagement of the behavior after baseline, and then moved elsewhere and lostto follow-up. Participants admitted post-baseline but discharged back to theiroriginal accommodation at follow-up remained in the sample. In the interventiongroup only one participant was hospitalized (for two days); all others were treatedin situ. High drop-out rates are common in intervention studies with fragilepopulations (e.g. Teri et al., 2000).
880 M. Bird et al.
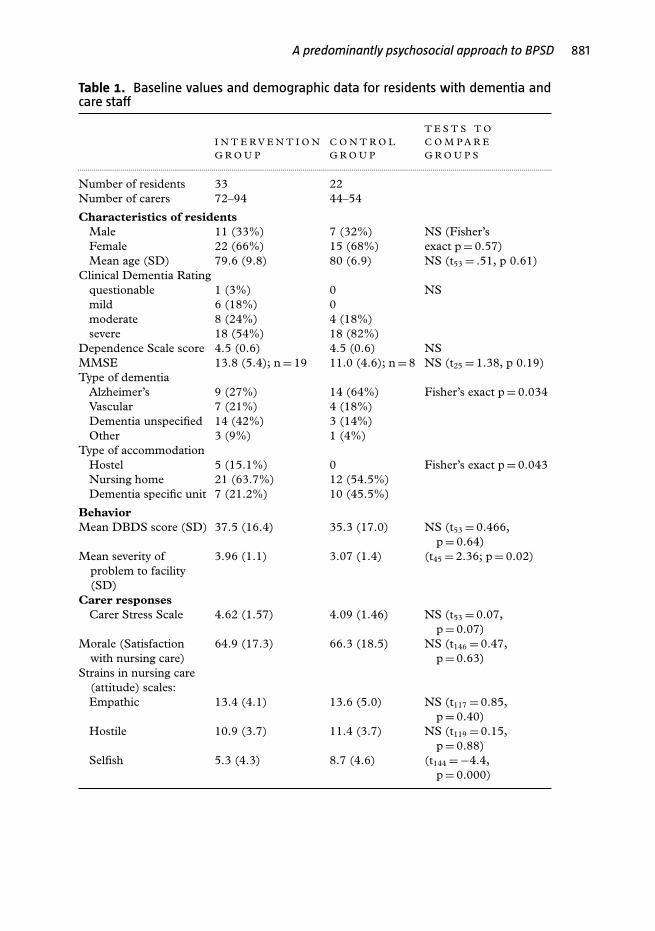
Baseline sample characteristicsThere were no significant differences between groups in participant age, gender,level of impairment, ADL functioning, staff morale/working environment, anddegree of stress caused by the behavior (Table 1). Intervention group residentswere less likely to be in dementia specific units and more likely to have a genericdementia diagnosis.
Table 1 also shows that there was no significant difference between groupsin scores on the Dementia Behavior Disturbance Scale (DBDS), but thatbehaviors in the intervention group were perceived as more disruptive (ProblemSeverity Scale) by senior nursing staff at baseline. For each case we alsocollected descriptions of the main behavior that staff perceived as “challenging.”These behaviors were grouped into broad types and are presented in Table S1(available as supplementary material online attached to the electronic versionof this paper at www.journals.cambridge.org/jid_IPG). Both groups had similarproportions of people with aggressive behavior, including violent resistance inpersonal care. The intervention group had a greater proportion of residentswho screamed or yelled or made repetitive demands whereas the control grouphad more wanderers and cases where the behavior was less clearly defined (e.g.“agitation”). In both groups, the main referred behavior had been present insome form for between two months and more than three years (interventiongroup 2–40 months; control group 2–48 months), with a mean of about oneyear.
At baseline, there was no significant difference between the groups inthe proportion of participants being given antipsychotic, antidepressant, andanxiolytic medications and in the mean dose of each class converted respectivelyinto Chlorpromazine, Amitriptyline, and Diazepam equivalents, using formulasfrom the Victorian Drug Use Advisory Committee’s “Psychotropic TherapeuticGuidelines” (Victorian Drug Usage Advisory Committee, 1996/1997; 2000).There was no difference between groups in the proportion of participants takinganticonvulsants.
Difference in clinical approach: control versus intervention groupTable 2 summarizes the ratings by five independent clinicians of thepsychopharmacological or psychosocial balance of interventions for each group.The difference in approach is significant: intervention group participants weremanaged using primarily psychosocial methods with psychopharmacology asan adjunct, whereas controls were managed using medication with psychosocialmethods as an occasional adjunct. Because there were such striking differences intreatment approach, multiple logistic regression was used to determine whetherthis was due to the four baseline sampling differences (type of dementia, type ofaccommodation, problem severity/degree of disruption, and type of behavior).These variables were entered into the equation together with group status. Theonly predictor was group (OR = 9.6; 95% CI, 2.7–33.8, p = 0.000). These dataconfirm that the clinical approach of each team and not sampling differencespredicted treatment choice.
A predominantly psychosocial approach to BPSD 881
Table 1. Baseline values and demographic data for residents with dementia andcare staff
p = 0.88)Selfish 5.3 (4.3) 8.7 (4.6) (t144 = −4.4,
p = 0.000)
882 M. Bird et al.
Table 2. Comparison of treatment approach between the groups
PRIMARY T REAT MENT MODA LITY
ENTIRELY
PSYCHOSOCIAL
MAINLY
PSYCHOSOCIAL
PSYCHOSOCIAL
A N D DR U G
MAINLY
D R U G
ENTIRELY
D R U G TOTA L....................................................................................................................................................................................................................................................................................
Control group 0 2 2 3 15 220% 9.1% 9.1% 13.6% 68.2% 100%
Fisher’s exact p = 0.000.
0
5
10
15
20
25
30
35
40
Time 1 Time 2 Time 3
DB
DS
Intervention
Control
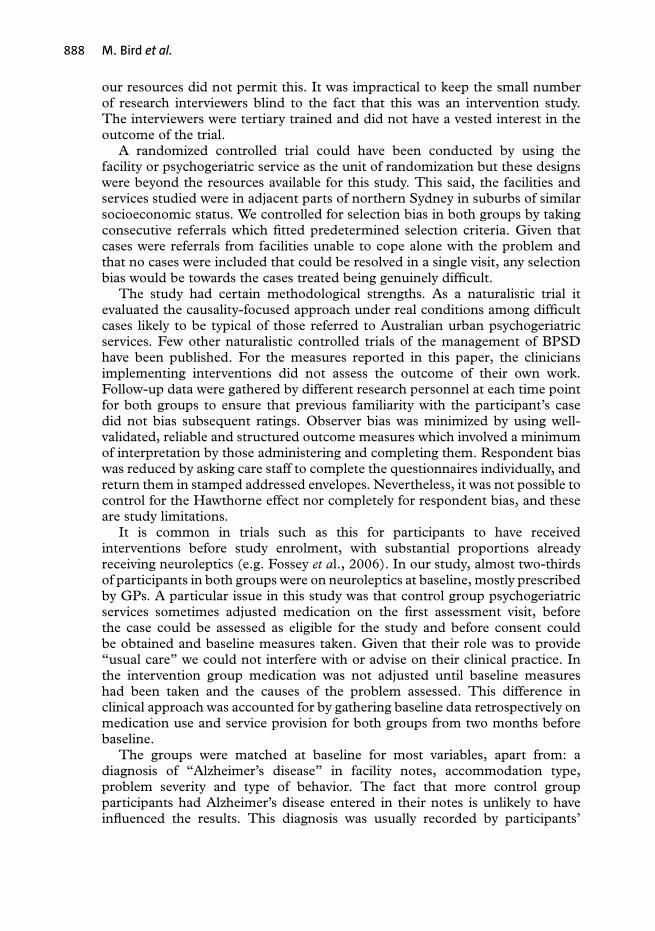
Figure 1 DBDS mean scores with SE bars over time, showing main within-subject effect.
Overall within-subject change: F(2,90) = 14.589, p = 0.000; Time 1–Time 2: F(1,45) = 14.175,
p = 0.000 (no group effect: F(1,45) = 2.25, p =0.141; no change/group interaction: F(2,90)= 1.035,
p = 0.360)
Change in behavior over timeRepeated measures analysis of variance (Figure 1) shows significantimprovement in behavior as measured on the Dementia Behavior DisturbanceScale from baseline to Time 2, and maintained three months later. There wasno difference between the groups. Figure 2 shows significant and maintainedimprovement in disruptiveness (Problem Severity Scale) for both groupswith no difference between them. Direct care staff perceptions match thesefindings. Scores on the Retrospective Perception of Behavior showed perceivedimprovement for both groups, but no difference between them in the proportionendorsing “worse,” “unchanged,” or “better” (χ2 = 0.58, d.f. = 2, p = 0.97).
A predominantly psychosocial approach to BPSD 883
0
1
2
3
4
5
6
7
Time 1 Time 2 Time 3
Pro
blem
sev
erity
and
car
er s
tres
sCarer stress - Intervention
Carer stress - Control
Problem severity - Intervention
Problem severity - Control
Figure 2 Carer response mean scores with SE bars over time showing main effects.
Problem severity, within-subject change: F(2,48) = 14.055, p = 0.000; Time 1–2: F(1,24) = 19.487,
p = 0.000 (no group effect: F(1,24) = 3.996, p = 0.057; No change/group interaction: F(2,48) =0.607, p = 0.549)
Carer stress, within-subject change: F2192 = 11.105, p = 0.000; Time –2: F1,96 = 5.012, p = 0.027 (no
group effect: F(1,96) = 1.399, p = 0.240; no change/group interaction: F(2192) = 1.463, p = 0.234)
For all three outcome variables, the small sample size made it statisticallyquestionable to enter baseline differences as covariates in the analysis ofvariance. Accordingly, regression was used to control for the two most importantsampling differences at baseline: degree of disruption (Problem Severity) andbehavior type. Small sample size prohibited controlling for dementia subtypeand type of accommodation. Because the change in all measures occurredduring the intervention period between Time 1 and Time 2, we maximizedsample size by making Time 2 the dependent variable and minimized thenumber of cells by collapsing categories in both dependent and independentvariables. Neither degree of disruption nor behavior type at Time 1 norgroup significantly predicted Time 2 scores for DBDS, Problem Severity, orRetrospective Perception of Behavior. Figure 2 also shows that, in the fullrepeated analysis of variance model, there was no significant difference betweenthe groups for Problem Severity, and no group by change interaction.
Change in staff responseFigure 2 shows significant and maintained improvement in staff stress relatedto the main referred behavior with no significant difference between groups.Controlling for the baseline sampling differences as described in the previousparagraph does not affect these conclusions. There was some improvementin staff attitude (Strains in Nursing Care Scale) for both groups. Repeated
884 M. Bird et al.
Table 3. Service delivery variables for both groups including medication changes,drug side effects and hospitalisations
T W OM O N T H SP R E -B A S E L I N E T I M E 1 – 2 T I M E 2 – 3
Mean GP visits per case where psychotropic medication changedIntervention group 1.19 1.06 0.81 0.35 3.41Control group 3.45 2.09 2.00 1.13 8.67
Patients for whom drug side effects reported (n)Intervention group 7 (23%) 2 (6%) 0 3 (12%)Control group 11 (50%) 10 (45%) 6 (35%) 5 (31%)
Hospitalizations (n, mean stay in days)Intervention group 1 (3%); 7 days 1 (3%); 2
days0 0
Control group 0 1 (5%); 28days
3 (18%); 43days
1 (6%); 22days
∗Project clinicians only worked on cases between Times 1 and 3: mean clinician hours per case Time 1to Time 2 = 6.69; Time 2–Time 3 = 0.80. Hours per case not collected for any other clinician.
measures analysis of variance showed a main within-subject effect for the“hostile” factor, with no group effect. The intervention group score improvedfrom 11.01 (3.74) to 11.91 (3.18); the control group from 11.24 (3.67) to11.70 (3.48): F(1101) = 4.659, p = 0.033. There was no within-subject changefor the “selfish” factor but the difference between groups at baseline remained(F(1119) = 10.330, p = 0.002). That is, control group staff were already lesslikely to attribute selfishness to residents at baseline, and remained so inclined.
Service and cost variablesClinical hours on site per case were recorded for the intervention group cliniciansonly (see Table 3), so the number of clinical visits provides the only availablecomparison of costs in time per case. Accordingly, for both groups, Table 3 showsmean frequency of visits per case to deal with disturbed behavior by GP and
A predominantly psychosocial approach to BPSD 885
aged medical specialist services (mainly psychogeriatricians or a psychogeriatricregistrar) for both groups over a nine-month period, plus clinical visits for theintervention group from baseline to Time 3 by the specialist project clinicians(registered nurse (RN) and/or clinical psychologist). As noted, data from twomonths prior to baseline were assessed because control group pharmacologicalinterventions sometimes occurred at the first visit by the psychogeriatric service,before the case was assessed as eligible for the study and therefore before consentcould be obtained and baseline measures taken. This is shown in Table 3 andmeans that data from two months before baseline must be included in thesecomparisons. The total number of visits is comparable, though it is likely thatintervention group specialist clinicians spent more time on site.
In relation to medication costs, there were no significant differences in useof antidepressants or anxiolytics (low in both groups) at follow-up. Almost twothirds of participants were on antipsychotics at baseline; 22/33 in the interventiongroup and 14/22 among controls. By Time 2, the proportion was reduced in theintervention group to 17/33 (51%) and had increased among controls to 16/22(73%), including three residents who had not previously been on antipsychotics.This is a significant difference (p = 0.048). Table 3 shows that medication costswere potentially exacerbated by wastage in the control group, where there weremore than twice the number of changes of medication between baseline andTime 2. Table 3 also shows that the control group experienced higher humancosts in drug side-effects that were serious enough to be noted in residentialfacility notes and/or doctors’ notes. More control participants were admitted toa specialist psychogeriatric unit, and for substantial periods of time, for treatmentof the behavior. In the intervention group, all but one resident (admitted for twodays) was treated in situ.
Discussion
Clinical and service measuresA clinical approach addressing causality of the behavior and/or causes ofwhy the behavior was “challenging” enabled a series of cases of BPSD tobe treated using a predominantly psychosocial approach, with psychotropicmedication as an adjunct where required. It was compared with what ischaracterized as usual care, with predominantly psychopharmacology being used.Both approaches produced equivalent improvements in measures of behaviorfrequency, disruptiveness, staff-perceived behavior change, staff stress, andattitude to the referred residents. The differences were mainly in human andfinancial costs. Focusing on causality may be time-intensive for a short period –in this study, a mean of just over six visits per case between baseline and Time2, each visit lasting a mean of just over an hour (total clinician hours 6.69),but this approach took no more clinical visits overall than the comparison usualcare sample. It may even be less costly since control cases had twice as manyGP visits and most control cases were ultimately treated by specialist medicalpractitioners on at least twice the salary of the RN or clinical psychologist
886 M. Bird et al.
who provided most of the services for the intervention group. The causality-focused approach had less wastage of medications, fewer drug side effects,and fewer hospitalizations. There is also evidence that it resolved more cases –after the five-month follow-up, there were more GP and psychogeriatric servicevisits and more psychotropic medication changes in the control group (seeTable 3).
The finding that more control participants were admitted and for much longerperiods may be related to the fact the control group had access to a specialistpsychogeriatric inpatient unit, whereas the intervention group only had accessto an adult inpatient psychiatric unit, less suitable for this population. This said,the intervention group approach enabled all cases to be treated in the aged carefacility where they lived – apart from one participant briefly hospitalized to givestaff respite. Hospitalization for treatment of disturbed behavior is costly becausebed days cost more in hospitals than in aged care facilities and also because, inAustralia, the nursing home bed must be kept open for a defined period whilethe resident is in hospital.
Sampling differences between the groups at baseline did not explain thedifference in clinical approach. These included the type of accommodation,whether or not a diagnosis of Alzheimer’s disease was entered in the participants’file and, in particular, the nature of the behavior and degree of disruptiveness –which was perceived at baseline by senior staff as greater in the interventiongroup. Group status was the only predictor of whether a predominantlypsychosocial or psychopharmacological approach was used. Clinical approachwas determined by service variables, not variables associated with the participant,behavior, facility, or staff.
Comment on the intervention group approachThe aim of the approach trialed here was to determine which combination ofpsychosocial or/and pharmacological methods best fitted the individual profilesof a series of BPSD cases. Each profile was based on a thorough investigationof what caused or exacerbated the behavior and/or what caused the behaviorto be perceived as a problem. Variability of perception was well illustrated inour validation studies of the Carer Stress and Problem Severity scales. After twomonths there was high within-subject consistency of staff stress levels in responseto the same behavior by the same resident, and degree of disruption perceived bysenior staff. However, there was low agreement between these informants aboutstress and disruption.
In the intervention group, the causes of the problem were variable andcase specific. Three of these cases, each involving the same behavior (physicalaggression), were reported in Bird (2005). In the first, contributory factorswere the resident’s history of obsessive compulsive disorder which interactedwith staff ignorance of this fact, and low confidence and skill. In the secondcase the primary cause was escalating pain which interacted with the busypremorbid personality of the resident. In the third case, multiple causes includedpremorbid character, cultural expectations, pain, frustration at being bed-bound, and family guilt affecting their behavior towards facility staff. These
A predominantly psychosocial approach to BPSD 887
factors interacted with staff being unaware of their rights, low morale andhigh distress, lack of knowledge and understanding of the resident’s past,and failure to grasp her degree of physical discomfort. Addressing the causesameliorated all three cases although in Case 1 there was no change in frequencyof behavior because the intervention addressed staff distress, skill and confidenceassociated with managing a resident whose behavior was never likely tochange.
By design this was not a trial of one discrete therapy compared withanother. Rather, a naturalistic study design was chosen in order to evaluate theeffectiveness of focusing on causality in BPSD under real life conditions. Thisdesign was used to capture the variability of causality at the individual case level,and to illustrate the consequent variability of treatment in the intervention group.Using this approach, psychosocial and psychopharmacological approacheswere seen as complementary rather than in opposition. For the interventiongroup, what determined the psychosocial/pharmacological balance, and theprecise nature of the interventions used in each case, were clinical decisionsabout what would address most effectively the causes of the behaviorand/or why it was seen by staff as a problem. Ultimately, psychotropicmedication was used in only a minority of cases, and the use of neurolepticsreduced.
For the control group, while this study does not provide evidence ofunnecessary psychotropic medication use, the results from the interventiongroup and the fact that neither sampling differences nor the nature of thebehavior predicted the clinical approach suggest that a stronger focus on causalitycould have reduced its use. Fossey et al. (2006), using case-specific individualizedinterventions for BPSD, as well as “whole of home” interventions in residentialcare, also produced reductions in neuroleptic use.
An increasing number of instruments have been published in the pastfive years which highlight the importance of assessing causal factors at theindividual case level to help treatment choice (e.g. Howard et al., 2001; McMinnand Draper, 2005). Despite this, a survey of Australian and New Zealandpsychogeriatricians found that neuroleptics were “favored overwhelmingly formost symptoms of BPSD” (Greve and O’Connor, 2005, p. 202). If furthertrials of case-specific as opposed to generic interventions produce similarresults to this study, it will suggest that focusing on causal factors is away to reduce the predominant reliance on neuroleptic medication to treatBPSD.
Study methodology: strengths and limitationsThe study design was dictated by the clinical approach in the intervention groupand the resources available. It was not a randomized controlled trial and ablinding procedure was not used. Double-blinding is only possible in studiesof drug interventions. It is impossible for clinicians undertaking complex case-specific psychosocial interventions and for the staff involved to be blind to thenature of the intervention. Complete single blinding would have been possiblehad completely independent assessment teams gathered all outcome data, but
888 M. Bird et al.
our resources did not permit this. It was impractical to keep the small numberof research interviewers blind to the fact that this was an intervention study.The interviewers were tertiary trained and did not have a vested interest in theoutcome of the trial.
A randomized controlled trial could have been conducted by using thefacility or psychogeriatric service as the unit of randomization but these designswere beyond the resources available for this study. This said, the facilities andservices studied were in adjacent parts of northern Sydney in suburbs of similarsocioeconomic status. We controlled for selection bias in both groups by takingconsecutive referrals which fitted predetermined selection criteria. Given thatcases were referrals from facilities unable to cope alone with the problem andthat no cases were included that could be resolved in a single visit, any selectionbias would be towards the cases treated being genuinely difficult.
The study had certain methodological strengths. As a naturalistic trial itevaluated the causality-focused approach under real conditions among difficultcases likely to be typical of those referred to Australian urban psychogeriatricservices. Few other naturalistic controlled trials of the management of BPSDhave been published. For the measures reported in this paper, the cliniciansimplementing interventions did not assess the outcome of their own work.Follow-up data were gathered by different research personnel at each time pointfor both groups to ensure that previous familiarity with the participant’s casedid not bias subsequent ratings. Observer bias was minimized by using well-validated, reliable and structured outcome measures which involved a minimumof interpretation by those administering and completing them. Respondent biaswas reduced by asking care staff to complete the questionnaires individually, andreturn them in stamped addressed envelopes. Nevertheless, it was not possible tocontrol for the Hawthorne effect nor completely for respondent bias, and theseare study limitations.
It is common in trials such as this for participants to have receivedinterventions before study enrolment, with substantial proportions alreadyreceiving neuroleptics (e.g. Fossey et al., 2006). In our study, almost two-thirdsof participants in both groups were on neuroleptics at baseline, mostly prescribedby GPs. A particular issue in this study was that control group psychogeriatricservices sometimes adjusted medication on the first assessment visit, beforethe case could be assessed as eligible for the study and before consent couldbe obtained and baseline measures taken. Given that their role was to provide“usual care” we could not interfere with or advise on their clinical practice. Inthe intervention group medication was not adjusted until baseline measureshad been taken and the causes of the problem assessed. This difference inclinical approach was accounted for by gathering baseline data retrospectively onmedication use and service provision for both groups from two months beforebaseline.
The groups were matched at baseline for most variables, apart from: adiagnosis of “Alzheimer’s disease” in facility notes, accommodation type,problem severity and type of behavior. The fact that more control groupparticipants had Alzheimer’s disease entered in their notes is unlikely to haveinfluenced the results. This diagnosis was usually recorded by participants’
A predominantly psychosocial approach to BPSD 889
GPs. Given uncertainty regarding the accuracy of GPs’ diagnoses of dementiasubtypes (Olafsdottir et al., 2000) the difference may be more apparent thanreal. BPSD occurs in all subtypes of dementia and multiple measures confirmedthat study participants had dementia. Considerable overlap is likely betweenAlzheimer’s disease and other dementias (Zekry et al., 2002) and the groups werematched for age, gender, cognitive status and level of dependence – commonpredictors of BPSD severity (Beck et al., 1998).
It is unclear whether having more control group residents living in facilitiesdescribed as “dementia-specific” at baseline would have influenced the results.This difference could not be controlled for in outcome analyses and this is alimitation of the study. Type of accommodation had no effect on whether caseswere managed predominantly using pharmacological means or psychosocialmeans. All four baseline differences were controlled for by analyzing thisdifference. It was the clinical approach of each team – not the variables associatedwith the participant, behavior, facility, or staff – that predicted treatmentchoice.
Conclusion
The majority of participants in the intervention group were managed usingpsychosocial interventions while the majority of control participants weremanaged with psychotropic medication. This study was not a comparison ofunimodal treatments. The intervention group received multifaceted treatmentpackages whereas only a minority of controls received such care. The causality-focused approach was as effective as the predominantly pharmacologicalapproach and involved lower human and financial costs. Despite the limitationsof this study, our results provide encouragement for further research intoapproaches which look in greater depth at causality and individualizedinterventions.
Conflict of interest
None.
Description of authors’ roles
Michael Bird and Robert Llewellyn-Jones initiated and designed the studyand obtained study funding. Michael Bird designed and implemented manyof the intervention group interventions and supervised the other interventiongroup clinicians, assisted with data interpretation and analysis, and draftedthe manuscript. Robert Llewellyn-Jones oversaw the study, jointly drafted themanuscript and contributed to data interpretation, editing and revising themanuscript, and was the treating psychogeriatrician on intervention groupcases where psychotropic medication was required. Ailsa Korten analyzed andinterpreted study data, prepared the graphs and tables, and wrote much of the
890 M. Bird et al.
Results section. Heather Smithers contributed to the study planning, collecteddata and coordinated data collection by others, and checked data entry.
Acknowledgments
We express our profound gratitude to the residents and staff who took partin this study, and to the Australian Government Department of Health andAgeing, whose funding made the study possible. We also wish to acknowledgethe clinicians from both groups and the research support staff. Dr. Bob Russelland Dr. Ruth Foster led the control group clinical teams and we gratefullyacknowledge their input and cooperation throughout the study. They have readand approved the publication of this manuscript. Additional intervention groupclinicians included Maureen Stronach and Karen Cohen, who were assistedby Kris Revson and Lucy O’Neill on a few cases. Dr. Sue Kurrle and Dr.Ian Cameron provided geriatrician input where required for the interventiongroup. Sandra Faase assisted with study administration and data collection,Jasmine Cohen entered the data, and Karen Baikie provided general assistancethroughout. Special thanks go to Tanya Caldwell, who provided statistical adviceduring revision of this manuscript, and to Annaliese Blair, who produced thegraphs. Dedicated in grateful memory to Ailsa Korten.
References
Balestreri, L., Grossberg, A. and Grossberg, G. T. (2000). Behavioral and psychologicalsymptoms of dementia as a risk factor for nursing home placement. InternationalPsychogeriatrics, 12, 59–62.
Baumgarten, M., Becker, R. and Gauthier, S. (1990). Validity and reliability of theDementia Behavior Disturbance Scale. Journal of the American Geriatrics Society, 38, 221–226.
Beck, C. et al. (1998). Correlates of disruptive behavior in severely cognitively impaired nursinghome residents. The Gerontologist, 38, 187–198.
Bird, M. (2005). A predominantly psychosocial approach to behaviour problems in dementia:treating causality. In A. Burns, J. O’Brien and D. Ames (eds.), Dementia. 3rd edn. London:Hodder Arnold.
Bird, M. et al. (1998). Challenging behaviours in dementia: a project at Hornsby/Ku-ring-gaiHospital. Australian Journal on Ageing, 17, 10–15.
Bird, M., Llewellyn-Jones, R., Smithers, H. and Korten, A. (2002). PsychosocialApproaches to Challenging Behaviour in Dementia: A Controlled Trial. Canberra: CommonwealthDepartment of Health and Ageing. (http://www.health.gov.au/internet/wcms/publishing.nsf/Content/ageing-publicat-psychsoc.htm)
Cohen-Mansfield, J. and Werner, P. (1999). Longitudinal predictors of non-aggressiveagitated behaviors in the elderly. International Journal of Geriatric Psychiatry, 14,831–844.
Cole, R. P., Scott, S. and Skelton-Robinson, M. (2000). The effect of challengingbehaviour, and staff support, on the psychological wellbeing of staff working with older adults.Aging and Mental Health, 4, 359–365.
Deberdt, W. et al. (2005). Comparison of Olanzapine and Risperidone in the treatment ofpsychosis and associated behavioural disturbances in patients with dementia. American Journalof Geriatric Psychiatry, 13, 722–730.
A predominantly psychosocial approach to BPSD 891
Evers, W., Tomic, W. and Brouwers, A. (2002). Aggressive behaviour and burnout amongstaff of homes for the elderly. International Journal of Mental Health Nursing, 11, 2–9.
Folstein, M., Folstein, S. and McHugh, P. (1975). Mini-mental state: a practical method forgrading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12,189–198.
Fossey, J. et al. (2006). Effect of enhanced psychosocial care on antipsychotic use in nursinghome residents with severe dementia: cluster randomised trial. BMJ, 332, 756–761.
Greve, M. and O’Connor, D. (2005). A survey of Australian and New Zealand old agepsychiatrists’ preferred medications to treat behavioral and psychological symptoms ofdementia (BPSD). International Psychogeriatrics, 17, 195–205.
Hallberg, I. R., Edberg, A.-K., Nordmark, A. and Johnsson, K. (1993). Daytime vocalactivity in institutionalised severely demented patients identified as vocally disruptive bynurses. International Journal of Geriatric Psychiatry, 8, 155–164.
Hallberg, I. R. and Norberg, A. (1995). Nurses’ experiences of strain and their reactions inthe care of severely demented patients. International Journal of Geriatric Psychiatry, 10,757–766.
Hansson, U. W., Hallberg, I. R. and Axelsson, K. (1995). Nurses’ satisfaction with nursingcare and work at three care units for severely demented people. Journal of Psychiatric andMental Health Nursing, 2, 151–158.
Herrmann, N. (2001). Recommendations for the management of behavioural and psychologicalsymptoms of dementia. Canadian Journal of Neurological Science, 28, S96–S107.
Howard, R., Ballard, C., O’Brien, J. and Burns, A. (2001). Guidelines for themanagement of agitation in dementia. International Journal of Geriatric Psychiatry, 16,714–717.
McMinn, B. and Draper, B. (2005). Vocally disruptive behaviour in dementia: developmentof an evidence-based practice guideline. Aging and Mental Health, 9, 16–24.
Margallo-Lana, M. et al. (2001). Prevalence and pharmacological management of behaviouraland psychological symptoms amongst dementia sufferers living in care environments.International Journal of Geriatric Psychiatry, 16, 39–44.
Meares, S. and Draper, B. (1999). Treatment of vocally disruptive behaviour ofmulti-factorial aetiology. International Journal of Geriatric Psychiatry, 14, 285–290.
Moniz-Cook, E., Woods, R. and Gardiner, E. (2000). Staff factors associated withperception of behaviour as ‘challenging’ in residential and nursing homes. Aging and MentalHealth, 4, 48–55.
Morris, J. (1993). The Clinical Dementia Rating (CDR): current version and scoring rules.Neurology, 43, 2412–2414.
Olafsdottir, M., Skoog, I. and Marcusson, J. (2000). Detection of dementia in primarycare. Dementia and Geriatric Cognitive Disorders, 11, 223–229.
Stern, Y. et al. (1994). Assessing patient dependence in Alzheimer’s disease. Journals ofGerontology: Medical Sciences, 49, M216–M222.
Teri, L. et al. (2000). Treatment of agitation in AD: a randomized, placebo-controlled clinicaltrial. Neurology, 55, 1271–1278.
Victorian Drug Usage Advisory Committee (1996/1997). Psychotropic Drug Guidelines. 3rdedn. Melbourne: Jenkin Buxton.
Victorian Drug Usage Advisory Committee (2000). Psychotropic Drug Guidelines. 4th edn.Melbourne: Jenkin Buxton.
Wood, S. A., Cummings, J. L., Barclay, T., Hsu, M.-A., Allahyar, M. and Schnelle,J. F. (1999). Assessing the impact of neuropsychiatric symptoms on distress in professionalcaregivers. Aging and Mental Health, 3, 241–245.
Zekry, D., Hauw, J-J. and Gold, G. (2002). Mixed dementia: epidemiology, diagnosis, andtreatment. Journal of the American Geriatrics Society, 50, 1431–1438