No. 1994. NOVEMBER 16, 1861. A Course of Lectures ON P A I N, AND THE THERAPEUTIC INFLUENCE OF MECHANICAL AND PHYSIOLOGICAL REST IN ACCIDENTS & SURGICAL DISEASES. Delivered in the Theatre of the Royal College of Surgeons, BY JOHN HILTON, ESQ., F.R.S., SURGEON TO GUY’S HOSPITAL, PROFESSOR OF ANATOMY AND SURGERY TO THE ROYAL COLLEGE OF SURGEONS. LECTURE V.-PART III. ON looking at the late Mr. Bransby Cooper’s description of a Chinese lady’s feet, I find that no mention is made of any dis- ease of the structures forming the articulations. The joints are distorted, and the whole foot dwarfed by rest and pressure; yet, as far as I can see on examining the dried preparation, no bony anchylosis has occurred in any of the articulations. ’, It so happens that this College is rich at this time in Chinese ladies’ feet, and I place before you a very good specimen, which I shall employ for the purpose of sustaining the view that I entertain regarding the non-deteriorating influence of rest in healthy joints. Here is a large drawing of the preparation which FIG. 33. This sketch represents a vertical section of the foot of a Chinese lady. The specimen belongs to the College of Surgeons, and has been preserved in spirits of wine. The bones are num- bered. 1, Tibia. 2, Astragalus. 3, 3, Os calcis. 4, Scaphoid. 5, Cu- neiform. 6, Metatarsal bone, with phalanges appended. It will be noted that all the joints between the different bones remain perfect, although the shapes and directions of the articular surfaces have been rendered very abnormal by rest and long-continued mechanical pressure upon the foot. is in the bottle. I do not know how old the lady was, but we may fairly presume, looking to the appearance of the bones, that she had arrived at, or beyond, the age of puberty. Now these joints have been compressed upon each other during twenty or thirty years, and yet these same articular surfaces are in a perfect condition; the articular structures are not in the slightest degree deteriorated by it. If one were asked to produce a notable instance where pressure and constrained position are exerted upon joints by the strong competition car- ried on for many years between the efforts of nature from within and the application of brute human force from without, and no injury to them, this is surely the one. Yet there never was a case in which the conclusion could be more manifest than in this, for the articular surfaces are perfectly entire and healthy. In a note that I had from Dr. Barder, one of the curators of the College Museum, on the 23rd of January, 1861, he says, " The articular cartilages from the articulation of the Chinese foot are microscopically perfectly healthy." This illustration ought, I think, to displace the illegitimate fear and apprehen- sion, that continued mechanical rest to joints leads to their irre- parable deterioration. Then take another instance. If you strap up a foot firmly in order to cure disease of one of the tarsal joints, do the other tarsal joints become anchylosed? Certainly not necessarily. Here is a beautiful illustration of this fact. It is the foot of a FIG 34- This drawing from nature represents a longitudinal section of the foot, so made as to display the complete bony consolidation or anchylosis of the head of the astragalus with the concave arti- cular surface of the scaphoid bone, whilst the joints between the scaphoid and cuneiform bones remain in a distinctly healthy condition. a, Astragalus and scaphoid bones consolidated. b, Internal cuneiform bone. c, Middle cuneiform bone. This section was made obliquely, so as to show parts of two of the cuneiform articulations, with the scaphoid bone. young man whose limb I removed for disease of the knee-joint. Upon the inner side of the foot there may be seen a well-marked specimen of anchylosis between the scaphoid bone and the astragalus, yet the joints nearest to it are not in any way in- volved in that mischief; there is no anchylosis ; they are per- fectly healthy. The anchylosis had taken place about two years previous to the amputation of the limb. It is a very typical instance of anchylosis, and I employ it for the purpose to which I am now referring-namely, to show that, although pressure by strapping the foot, quiet, and rest were resorted to during a long period, in order to cure the disease between the astragalus and scaphoid, yet the only two bones which be- came anchylosed were those between which the joint was in an unhealthy condition. Again, is the larynx in a case of severe cut throat voiceless after a rest of six, seven, eight, or ten weeks ? or is an unfed stomach after six or eight weeks incompetent to resume its duties of digestion, if provided carefully with food and a small amount of necessary exercise ? Certainly not. In cases of cataract, either congenital or of recent date, is the retina in- capacitated to receive or appreciate the rays of light carefully introduced into the organ ? Certainly not. Then, I say, if all this be true, what right have we to expect that a joint should present different pathological and physiological phenomena? I think I have advanced facts enough to induce those gentle- men who entertain these opinions, as to scrofula being very constantly the cause of mischief in diseased joints, to admit that other causes, such as a chronic inflammatory condition, and slight local injury are by far the most frequent; and, further, that rest to healthy joints does not induce disease leading to anchylosis. Here I might say that, in teaching on this subject at Guy’s Hospital during many years, I have taken occasion to point out to those whom I have had the honour of instructing that the generally received impression as to scro- fula being, as a rule, at the foundation of joint diseases is really not true. This was taught publicly at Guy’s before the profes- sional existence of those who now publish such views as new. It is not stating too much to say that the diseases of joints are modified by age, in one or two respects especially. In the adult period of life we see disease of the individual articular structures, whether of synovial membrane, articular cartilage, or bone, and we observe that not only is the progress of the dis- ease usually slow, but the progress of repair at that period is
Transcript
No. 1994.
NOVEMBER 16, 1861.
A Course of LecturesON
P A I N,AND THE
THERAPEUTIC INFLUENCE OF MECHANICALAND PHYSIOLOGICAL REST
IN
ACCIDENTS & SURGICAL DISEASES.
Delivered in the Theatre of the Royal College of Surgeons,
BY JOHN HILTON, ESQ., F.R.S.,SURGEON TO GUY’S HOSPITAL,
PROFESSOR OF ANATOMY AND SURGERY TO THE ROYAL COLLEGE OF SURGEONS.
LECTURE V.-PART III.ON looking at the late Mr. Bransby Cooper’s description of a
Chinese lady’s feet, I find that no mention is made of any dis-ease of the structures forming the articulations. The joints aredistorted, and the whole foot dwarfed by rest and pressure;yet, as far as I can see on examining the dried preparation, nobony anchylosis has occurred in any of the articulations. ’,
It so happens that this College is rich at this time in Chineseladies’ feet, and I place before you a very good specimen, whichI shall employ for the purpose of sustaining the view that Ientertain regarding the non-deteriorating influence of rest inhealthy joints. Here is a large drawing of the preparation which
FIG. 33.
This sketch represents a vertical section of the foot of a Chineselady. The specimen belongs to the College of Surgeons, andhas been preserved in spirits of wine. The bones are num-bered.
1, Tibia. 2, Astragalus. 3, 3, Os calcis. 4, Scaphoid. 5, Cu-neiform. 6, Metatarsal bone, with phalanges appended.
It will be noted that all the joints between the different bonesremain perfect, although the shapes and directions of thearticular surfaces have been rendered very abnormal by restand long-continued mechanical pressure upon the foot.
is in the bottle. I do not know how old the lady was, but wemay fairly presume, looking to the appearance of the bones,that she had arrived at, or beyond, the age of puberty. Nowthese joints have been compressed upon each other duringtwenty or thirty years, and yet these same articular surfacesare in a perfect condition; the articular structures are not inthe slightest degree deteriorated by it. If one were asked to
produce a notable instance where pressure and constrainedposition are exerted upon joints by the strong competition car-ried on for many years between the efforts of nature from
within and the application of brute human force from without,
and no injury to them, this is surely the one. Yet there neverwas a case in which the conclusion could be more manifest thanin this, for the articular surfaces are perfectly entire and healthy.In a note that I had from Dr. Barder, one of the curators ofthe College Museum, on the 23rd of January, 1861, he says," The articular cartilages from the articulation of the Chinesefoot are microscopically perfectly healthy." This illustrationought, I think, to displace the illegitimate fear and apprehen-sion, that continued mechanical rest to joints leads to their irre-parable deterioration.Then take another instance. If you strap up a foot firmly
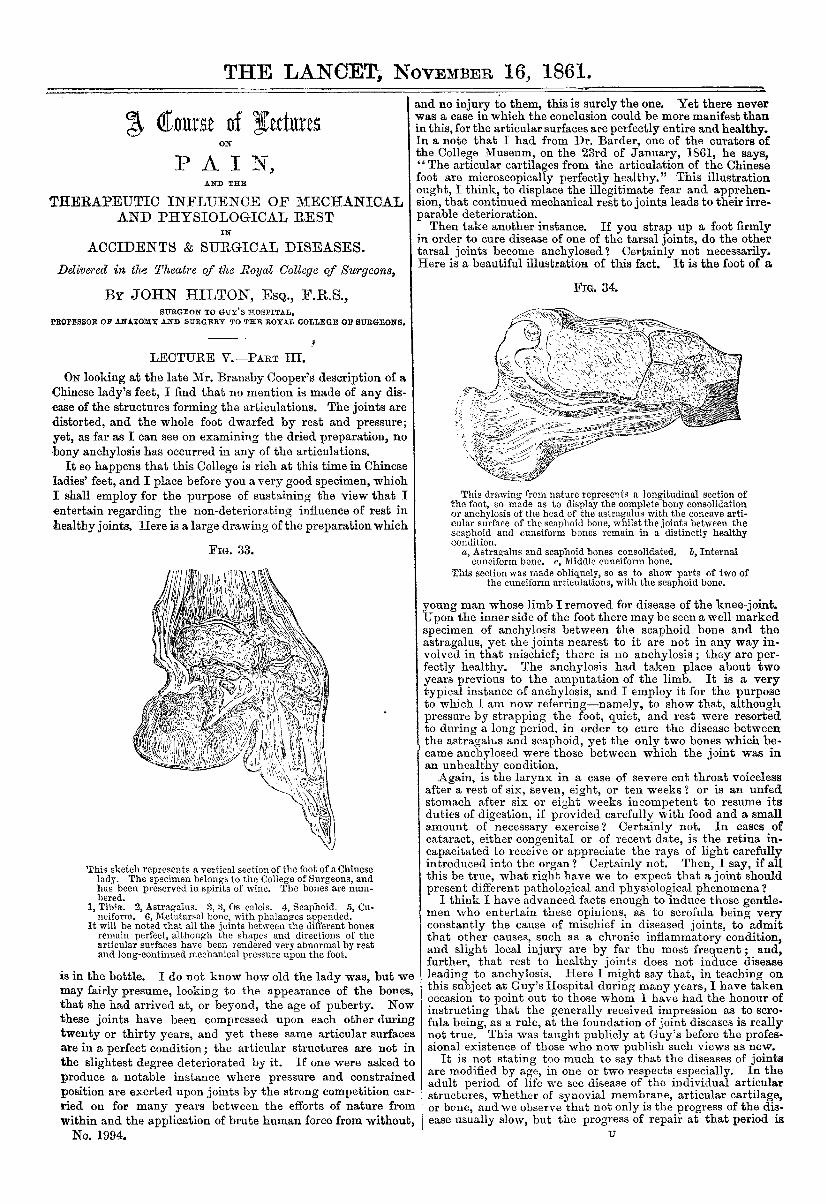
in order to cure disease of one of the tarsal joints, do the othertarsal joints become anchylosed? Certainly not necessarily.Here is a beautiful illustration of this fact. It is the foot of a
FIG 34-
This drawing from nature represents a longitudinal section ofthe foot, so made as to display the complete bony consolidationor anchylosis of the head of the astragalus with the concave arti-cular surface of the scaphoid bone, whilst the joints between thescaphoid and cuneiform bones remain in a distinctly healthycondition.
a, Astragalus and scaphoid bones consolidated. b, Internalcuneiform bone. c, Middle cuneiform bone.
This section was made obliquely, so as to show parts of two ofthe cuneiform articulations, with the scaphoid bone.
young man whose limb I removed for disease of the knee-joint.Upon the inner side of the foot there may be seen a well-markedspecimen of anchylosis between the scaphoid bone and theastragalus, yet the joints nearest to it are not in any way in-volved in that mischief; there is no anchylosis ; they are per-fectly healthy. The anchylosis had taken place about twoyears previous to the amputation of the limb. It is a verytypical instance of anchylosis, and I employ it for the purposeto which I am now referring-namely, to show that, althoughpressure by strapping the foot, quiet, and rest were resortedto during a long period, in order to cure the disease betweenthe astragalus and scaphoid, yet the only two bones which be-came anchylosed were those between which the joint was inan unhealthy condition.
Again, is the larynx in a case of severe cut throat voicelessafter a rest of six, seven, eight, or ten weeks ? or is an unfedstomach after six or eight weeks incompetent to resume itsduties of digestion, if provided carefully with food and a smallamount of necessary exercise ? Certainly not. In cases ofcataract, either congenital or of recent date, is the retina in-capacitated to receive or appreciate the rays of light carefullyintroduced into the organ ? Certainly not. Then, I say, if allthis be true, what right have we to expect that a joint shouldpresent different pathological and physiological phenomena?
I think I have advanced facts enough to induce those gentle-men who entertain these opinions, as to scrofula being veryconstantly the cause of mischief in diseased joints, to admitthat other causes, such as a chronic inflammatory condition,and slight local injury are by far the most frequent; and,further, that rest to healthy joints does not induce diseaseleading to anchylosis. Here I might say that, in teaching onthis subject at Guy’s Hospital during many years, I have takenoccasion to point out to those whom I have had the honour ofinstructing that the generally received impression as to scro-fula being, as a rule, at the foundation of joint diseases is reallynot true. This was taught publicly at Guy’s before the profes-sional existence of those who now publish such views as new.
It is not stating too much to say that the diseases of jointsare modified by age, in one or two respects especially. In theadult period of life we see disease of the individual articularstructures, whether of synovial membrane, articular cartilage,or bone, and we observe that not only is the progress of the dis-ease usually slow, but the progress of repair at that period is
468
slow also. In children, however, we note a very quick implica-tion, if we may so term it, of all the articular structures indisease, and quick destruction of the parts, and subsequentlyvery speedy repair. In young children this progress is veryrapid in acute disease. Here I have the outline of a cast of an
anchylosed knee-joint. It does not perhaps represent a speci-Fia. 35.
men of perfect surgery, but it indicates the rapidity of repairin a young person. The boy was three and a half years old,when he fell from a window, and damaged his knee. The injuryled to suppuration within the joint, and enormous swellingaround it; absorption of all the true articular structures, andultimately to complete bony anchylosis. The whole of thiswas accomplished in a very few months.But I advance this case in reference to another and very im-
portant point. It is a very common thing for surgeons to con-clude that a joint is irreparably damaged when they hear orfeel the articular ends of the bones grating upon each other.Now, I had a good opportunity of testing the value of thatpoint in this child when he was very ill, and the joint was verymuch swollen and suppuration going on in it. My dresser saidto me, " When dressing this leg, I can hear and feel the bonesgrating upon each other;" and he rather looked upon thissymptom as fatal to any probability of the repair of the joint. Iremarked to him, " Before we amputate this limb we will lookinto the interior of the joint." I made a free incision into thejoint, on its inner side, and washed out all the purulent fluid;and then I saw the dense articular laminæ of bone still uponthe femur and upon the tibia, and, on rubbing them together,the harsh, grating sound was produced. The internal soft
parts of the joint were all destroyed. I saw that the articularlaminae on the bones presented a worm-eaten, or minutely cri-briform, appearance, indicating that interstitial absorption ofthe laminae was going on; and I came to the conclusion that itwould be completely absorbed. I therefore secured the bonesin as easy and as accurate apposition as I could. I wished todivide the tendons of the ilexors; but it was determined bythe father that as the child was so ill he would not permit himto be touched any more in the way of operation ; therefore wedid the best we could with mechanical appliances to preventflexion of the knee-joint, and ultimately the boy got well, andcan now walk a mile or a mile and a half with facilitv. In thiscase I touched the interior of the joint with my linger, and Isaw distinctly what was the cause of the grating sensationwhen the surfaces were moved upon each other. It arose
clearly from the persistence, for a time, of the articular laminaebetween the cancellated structure of the bones and the arti-cular cartilage. You may observe here, in this diagram, thearticular lamin2 interposed between the articular cartilage andthe interior of the bone. It is, as we all know, a very dense,compact structure; and it is intelligible how it occurs thatwhen these surfaces were brought together they would createthe hard, rubbing, grating sensation which we so frequentlyhear and feel on examining diseased joints.As another practical application of this point, I may say that
the fact of this grating sensation sometimes determines in theminds of surgeons the propriety of excision or amputation.Now it should not be overlooked that there must be a periodin every joint disease which is to be cured by anchylosis whenthis grating sensation is to be experienced, and that is beforethe articular lamina is actually removed by absorption. Whenthe articular lamina is removed, consolidation can take place,but just anterior to that period it is plain that the friction orrubbing of two layers of compact bone upon each other mayproduce a rough grating, and might lead unjustly to theconclusion, that those portions of the bone which ought tobe in a. healthy condition in order to secure subsequent an-chylosis, are irreparably diseased. I have repeatedly heardand felt this grating noise in the fingers, ankle, hip, and otherarticulations, and yet the patient’s joints have done well byanchylosis. This practical point appeared to me to be wellworthy of a passing remark, especially as I had met with an
opportunity of having the explanation of the facts and thesymptoms actually demonstrated.
I purpose placing before you this fact, that diseases of thejoints in children follow a peculiar course, and not perfectly incorrespondence with that which obtains with respect to adults.In adults the individual structures of a joint may be diseased,and each may present its own local indications, or special localsymptoms. Thus, we may meet with isolated inflammationof the synovial membranes or ligaments, inflammation anddeterioration of the articular cartilage, or a disease of thearticular ends of the bones in the adult. Now, althoughthese numerous structures are at all periods of life necessarilycontinuous with each other and closely allied in function,yet it is at the adult period-after the completion of theircognate and harmonious development-that each separate struc-ture seems to have acquired, and thenceforward to manifestboth in health and disease, a structural independence, whichgives a character of individuality and isolation to the diseasesof the different structures of the joint.
In children all the structures of the joint must be formed,built up, and nourished in concert and in due relation to eachother, under the excitation of extreme vital energy or epi-genesis. There must be a great and intimate sympathy exist.ing between the different parts of a joint during childhood, orduring the period of growth, through the medium of an organicor vital power impressed upon those parts by Nature. It isthis formative or constructive power affixed by Nature mutuallyto the different articular structures which engenders in theirpathological conditions a tendency to diffuse disease cotem-poraneously in all the articular structures. Hence we see inour practice the quick propagation of inflammation from onearticular structure to another, and a rapidity of implication ofthe various structures of the joint in childhood and youth whichwe do not observe at a later period of life.
It is true, I believe, that in childhood the separate anddistinct disease of the articular structures can seldom be reco-
gnised with any useful precision during life. In cases of inflam-matory condition the results of severe local injury, or of slightinjury with strongly-developed constitutional tendencies, allthe various structures (including the bone, ligaments, cartilage,and synovial membrane) tributary to the formation of thejoint, become at this period of childhood soon more or less in-volved. It is, therefore, to my mind-and this is no new idea,for I have taught it publicly these last flfteen years or more-an unsubstantiated refinement in most cases of joint disease inchildhood to attempt to depict the symptoms indicating dis-tinct or separate pathological states of the individual structurescomposing a joint. It is certainly not in accordance withclinical experience, and surely it is not a sound basis uponwhich to fix and determine the plan of treatment.
This active principle of epigenesis and pathogenesis is notpeculiar to the joints alone in children ; it is the great feature,it is the pathological type, which this young period of life con-stantly displays in other parts of the body. Some of those gen-tlemen whom I now address know better than myself, and Itake it upon the statement of those in whom I have confidence,that in adults you meet with pneumonia, as a separate disease;you may see pleurisy as a separate disease, or bronchitis as aseparate disease, each recognised by distinct symptoms, andtreated in reference to the structural implication. But not so inchildhood ; at that period of life you scarcely ever meet withpleurisy, pneumonia, and bronchitis as distinct inflammations.They all appear together, or there is a general and rapid im-plication of all these structures nearly at the same time.
So it is in diseases of the brain. It is a common thing to seedisease of the membranes or disease of individual parts of thebrain in the adult; yet it is rare to see these in the same distinctand isolated manner during childhood. So, as I remarked be-fore, with regard to the larynx. In disease of the larynx inchildren all the soft parts become equally involved ; whilst inadult life, when the laryngeal structures seem to have acquireda normal independence, which they had not previously, theypossess also the pathological tendency towards the same kindand degree of independence.
Thus, I think, we mark by analogy a feature of high physio-logical and pathological importance, and very suggestive as aguide to treatment in Practice—viz., the difference between therelative progress and implication of the various structures ofdiseased joints in childhood and in manhood, showing that inchildren vigour and rapidity as to the diffusion and progress ofinflammatory conditions, as well as rapidity of repair, standin very strong and distinct antagonism to the like diseased con-ditions (in all other respects alike) which may attack the samestructures, but at a more advanced period of life.