A G8 plan that works: Reducing maternal, newborn and child mortality Dr. André Lalonde, FRCSC SOGC Executive Vice President FIGO Executive Board Member PMNCH Executive Board Member Dr. Heather MacDonnell, FRCPC, FAAP, DTMH(UK) Co-Head International Adoption Clinic Division of Pediatric Medicine, CHEO Assistant Professor of Pediatrics, U Ottawa Dr. Mark Walker, FRCSC Associate Professor University of Ottawa Senior Scientist OHRI Scientific Director BORN Ontario
Transcript
A G8 plan that works: Reducing maternal, newborn and child
mortality
Dr. André Lalonde, FRCSCSOGC Executive Vice PresidentFIGO Executive Board MemberPMNCH Executive Board Member
Dr. Heather MacDonnell, FRCPC, FAAP, DTMH(UK)
Co-Head International Adoption ClinicDivision of Pediatric Medicine, CHEO
Assistant Professor of Pediatrics, U Ottawa
Dr. Mark Walker, FRCSCAssociate Professor University of OttawaSenior Scientist OHRI
Scientific Director BORN Ontario
Canada to host the 2010 G8 Summit
This year, Canada is presented with an important opportunity to reaffirm itself as a global
humanitarian leader, as we welcome world leaders to the 2010 G8 and G20 Summits.
G8 to focus on Maternal and Child Health
Prime Minister Harper’s announcement is a step in the right direction.
But what exactly is included in the mother and child initiative?
And will promises be met?
Millennium Development Goals
Millennium Development Goals4. Reduce Child Mortality
• 180-210 million pregnancies every year• 80 million unwanted pregnancies• 50 million induced abortions• 20 million unsafe abortions • 68,000 deaths from unsafe abortion• 20 million women suffer from maternal morbidity• Estimated 536,000 maternal deaths• 3 million babies are born dead • Almost 10 million children under 5 die • Of which 3 million newborns die within the first week of life• 500,000 infants are infected with HIV
Progress toward MDG 4:
Source: Progress for children. A world fit for children. Statistical tables on MDG4. Available at http://www.unicef.org/progressforchildren/2007n6/index_41854.htm
• 12 of 13 countries with highest Maternal Mortality Ratios are in sub-Saharan Africa
• Pattern of contextual factors differs from that of MDG4.
High HIV prevalence (>5%, 1/13)
Conflict (8/13)
Coverage failures across the continuum of care
Coverage estimates for interventions across the continuum of care in the 68 priority countries (2000-2006). Vertical bars indicate the range in coverage across countries.
For some interventions:
• Family planning
• Exclusive breastfeeding
• Clinical care for newborn and child illnesses
In some countries:
• Wide gaps in coverage across countries
Key strategies to reduce maternal mortality
Skilled attendance at birth saves mothers and babies
Skilled attendance at childbirth is the most effective interventionWorld Health Organization
April 05
1. Political leadership and community engagement and mobilization
2. Delivering high quality services
3. Removing financial, social, and cultural barriers to access
4. Ensuring skilled and motivated health workers
5. Accountability at all levels for credible results
The Global Consensus for Maternal, Newborn and Child Health:
Simple strategies prevent deaths and are not necessarily expensive!
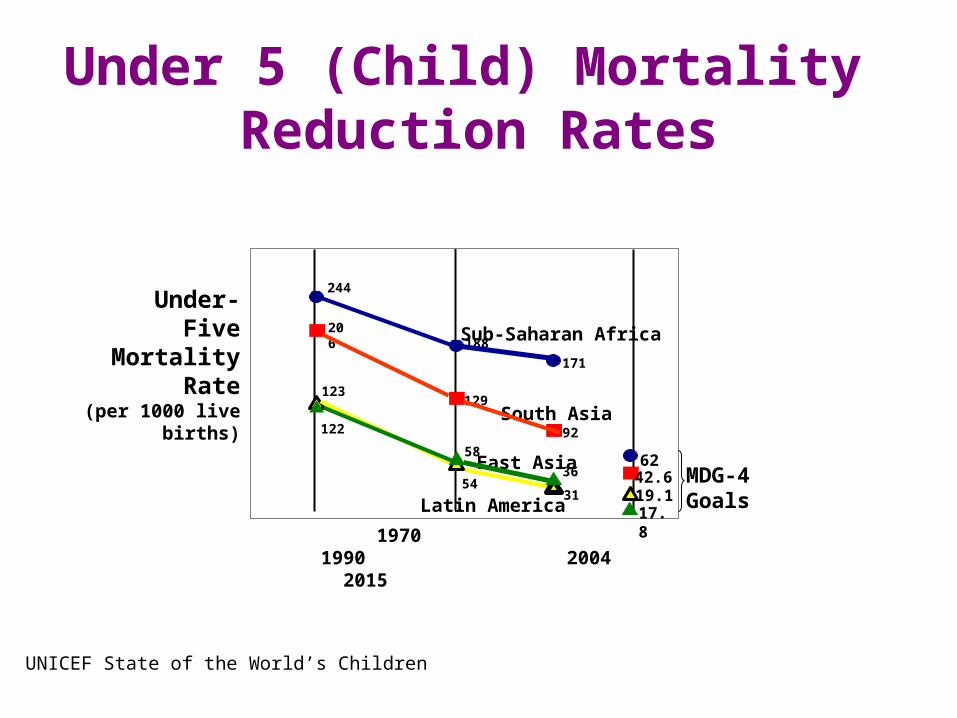
Sub-Saharan Africa
South Asia
Latin America
East Asia
Under-Five
MortalityRate
(per 1000 live births)
244
188
171
62
206
129
92
42.6
122
5431
17.8
123
58
36
19.1
1970 1990 2004 2015
MDG-4Goals
Under 5 (Child) Mortality Reduction Rates
UNICEF State of the World’s Children
Child Mortality Rate/1000 live births 6 130
Infant Mortality Rate/1000 live births 5 84
Stillbirth Rate
/1000 total births 3 32UNICEF State of the World’s Children
Preventable Conditions Cause Most Child Deaths
Infection 36%
Prematurity 27%
Asphyxia 23%}
Malnutrition
55%
WHO data
What can be done to save the children?
Postpartum
• Clean cord care• Skin to skin with mother (kangaroo care)• Antibiotics for suspected sepsis • Early breastfeeding, exclusive x 6 months
.
.
Early Infancy and Beyond
• Routine immunizations• Regular growth measurements• Health education to mothers
– Hygiene, clean water, sanitation• Antibiotics for pneumonia• Iron, Zinc, Vitamin A supplementation• Insecticide treated bed nets
What can be done to save the children?
Save a child’s life for a pittance
Estimated cost of interventions:
Insecticide-treated bed net $6Full WHO EPI immunizations (Africa) $14Oral rehydration solution (ORS) < $1
Total cost $887 per life saved
Save 800,000 African newborns at $1.39 per person per year
Recommendations• Focus on essential interventions that will prevent or
reduce maternal, newborn and child mortality and morbidity
• Increase capacity with training of skilled birth attendants and health care providers at all levels
• Improve and strengthen physical infrastructure of health care facilities and supply of commodities
• Embed surveillance into programs to drive process with measureable outcomes and send feedback on progress made back to the community
3 + 3 + 3
Maternal Health
-Post partum hemorrhage
-Eclampsia
-Dystocia
Maternal Health
-Post partum hemorrhage
-Eclampsia
-Dystocia
Newborn Health
-Infection
-Prematurity
-Asphyxia
Newborn Health
-Infection
-Prematurity
-Asphyxia
Child Health
-Acute respiratory illness
-Diarrhea
-Malaria
Child Health
-Acute respiratory illness
-Diarrhea
-Malaria
By focusing efforts on the 3 main causes of death, we can make real progress to improve the health of women, newborns and children
The way forward for Canada to lead in the area of Maternal and
Child Health • Increased funding for maternal and child health programs• Focus on the main causes of mortality and morbidity• Capitalize on Canada’s expertise in the field of maternal and child
health to strengthen programs and improve health outcomes• Use a rights-based approach• Ensure family planning• Upgrade the skills of health professionals, especially in the area of
Emergency Obstetric Care• Ensure programs are directed at all levels of service delivery
(local, regional, national)• Use the three delays model to influence program design and fund
allocation• Allocate funding in a way that addresses gaps along the
continuum of care
ConclusionConclusion• Maternal survival and health is essential for the
economic development of nations
• Survival and health of the world’s newborns and children depends on their mothers
• Parliamentarians need to play their part for Canada to assume a leadership role
There is no better time to raise your voice for women and children worldwide