34
A gastroenterologist’s view of post-surgical complications George Triadafilopoulos, MD Clinical Professor of Medicine Stanford University School of Medicine MISS, Salt Lake, UT, 2.21.2012
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | ashlyn-terry |
| View: | 221 times |
| Download: | 1 times |

A gastroenterologist’s view of post-surgical complications
George Triadafilopoulos, MDClinical Professor of Medicine
Stanford University School of Medicine
MISS, Salt Lake, UT, 2.21.2012

Outline
• What can happen
• How do we find out
• What can we do about it

What can happen…



Reasons for revisional surgery
Dysphagia Reflux Herniation Atypical0
10
20
30
40
50
60
48
33
15
4
%
N=109 pts
Lamb et al. Br J Surg. 2009;96(4):391-7

Esophagus – Diagnostic Steps

Barium studies

Intra-thoracic wrap migration
Revisional surgery


Endoscopy: Intact fundoplication
Snug scope upon retroflexion
Elongated intra-abdominal sphincter
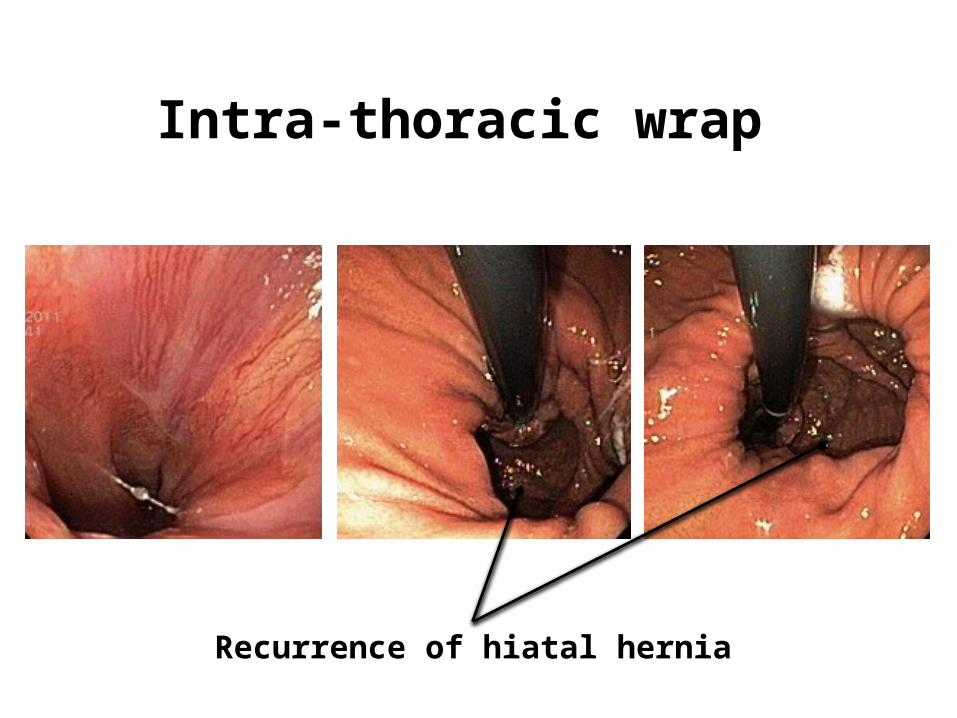
Intra-thoracic wrap
Recurrence of hiatal hernia

Lax fundoplication with GERD and Barrett’s esophagus
LaxityFree reflux and Barrett’sesophagus
Barrett’s esophagus
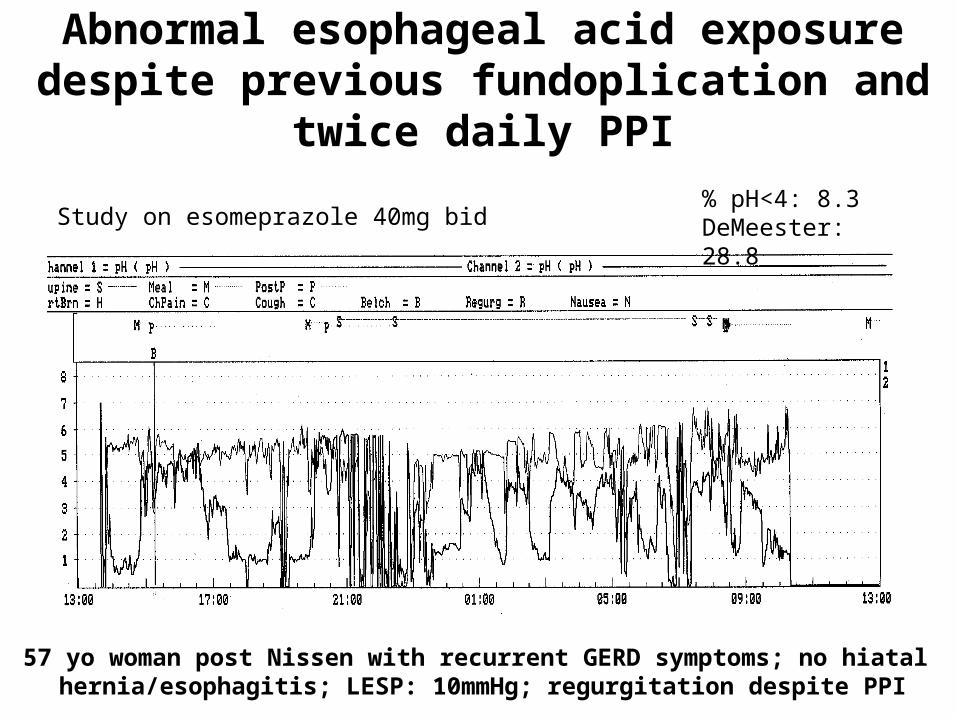
Abnormal esophageal acid exposure despite previous fundoplication and
twice daily PPI
57 yo woman post Nissen with recurrent GERD symptoms; no hiatal hernia/esophagitis; LESP: 10mmHg; regurgitation despite PPI
% pH<4: 8.3DeMeester: 28.8Study on esomeprazole 40mg bid
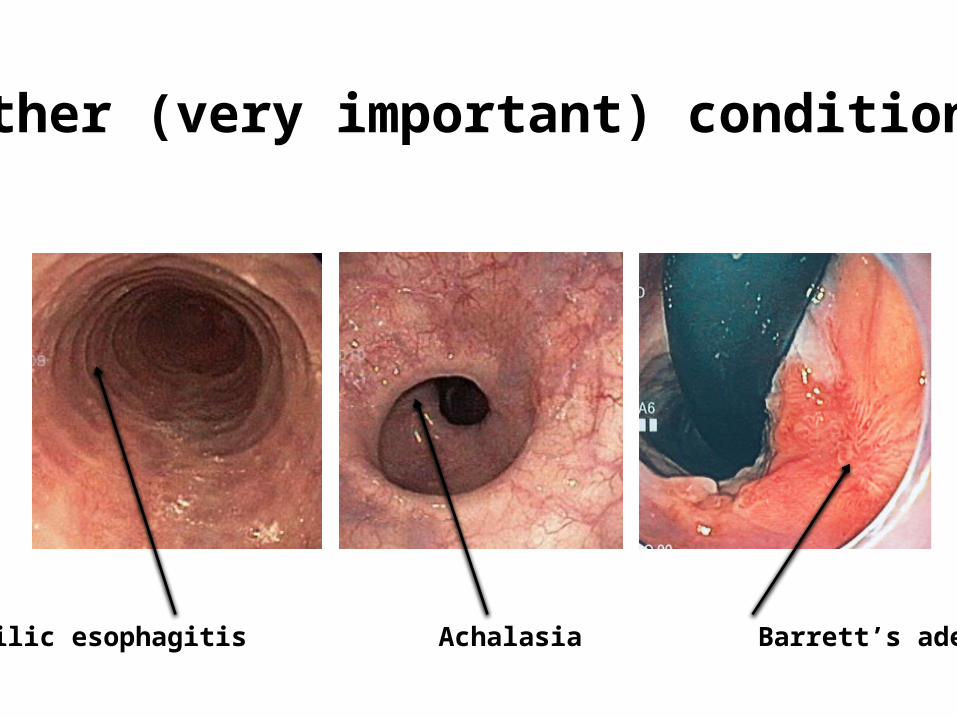
Other (very important) conditions
Eosinophilic esophagitis Achalasia Barrett’s adenocarcinoma
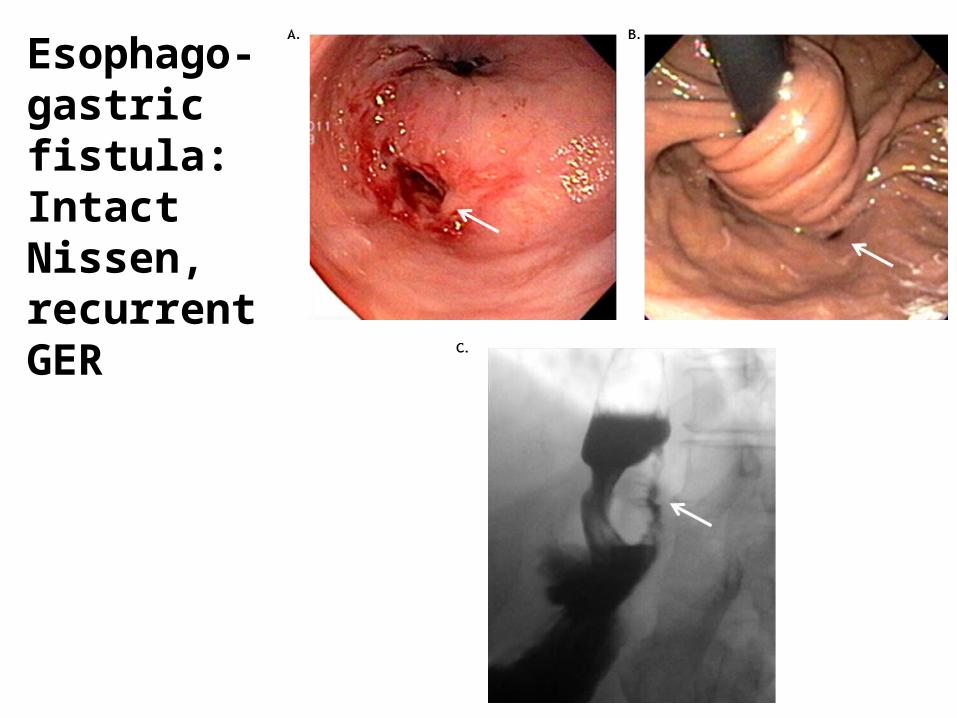
Esophago-gastric fistula: Intact Nissen, recurrentGER

Multichannel intraluminal impedance assesses esophageal
clearance

Recurrent, persistent, or new onset of dysphagia after
antireflux surgery
3 possibilities:
• Patients with signs of obstruction at or above the GEJ suspicious of “crural stenosis” (40%).
• Patients with signs of total or partial migration of the wrap intra-thoracically (50%).
• Patients in whom the hiatal closure is radiologically assessed to be correct with a supposed “stenosis of the wrap” (10%).

Pneumatic dilation for crural stenosis: 85% successful


Stomach/Intestine – Diagnostic Steps

Gastric emptying study in gastroparesis
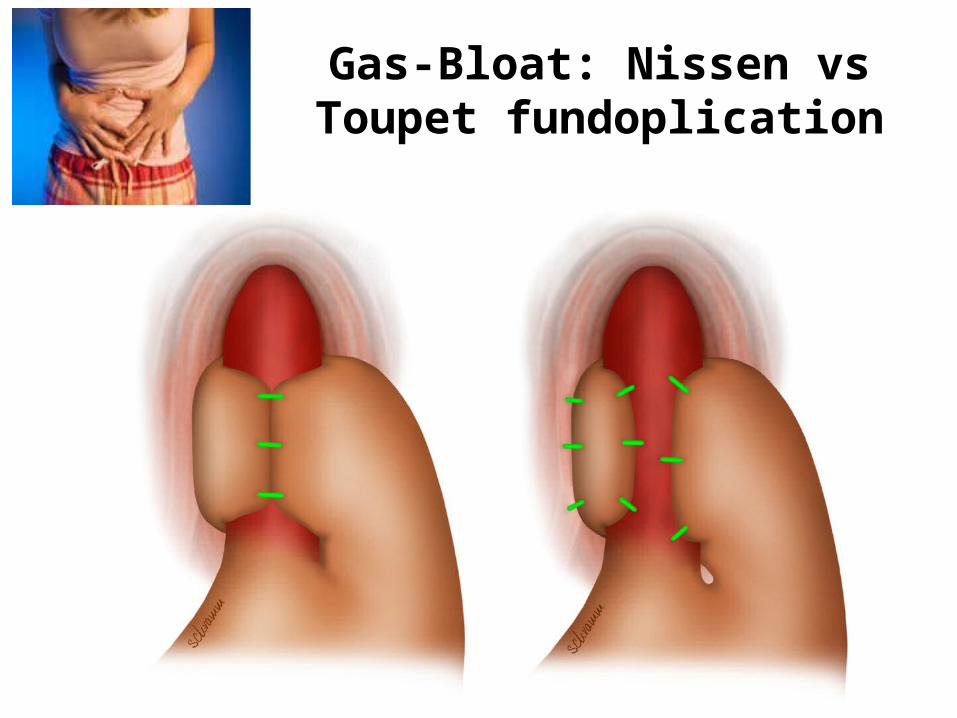
Gas-Bloat: Nissen vs Toupet fundoplication

Gas-bloat symptoms post NissenDigestive and Liver Disease 39 (2007) 312–318
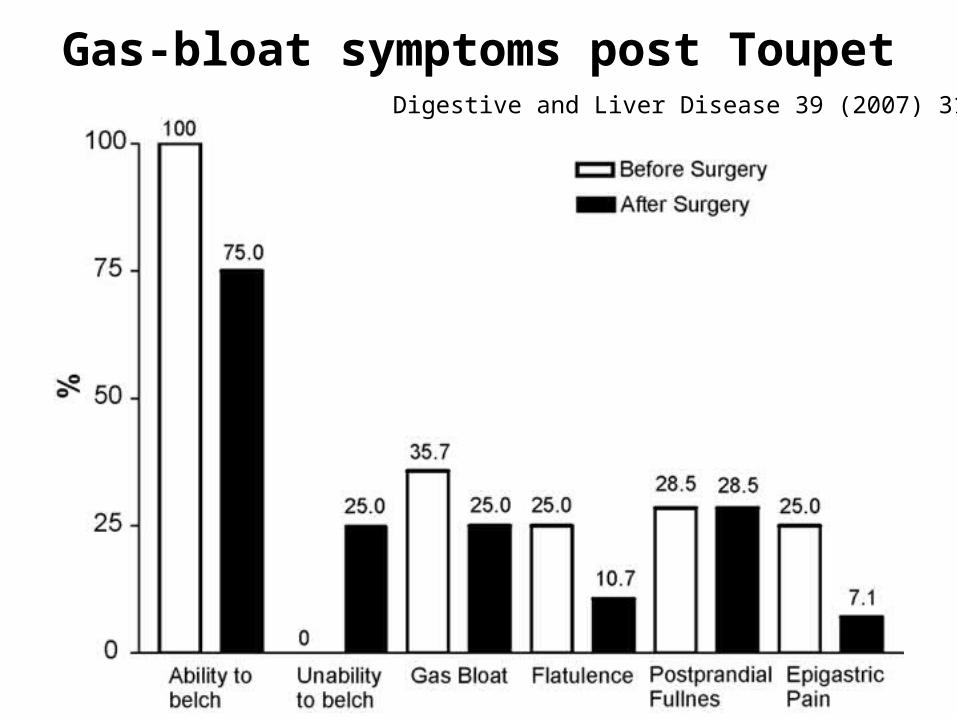
Gas-bloat symptoms post ToupetDigestive and Liver Disease 39 (2007) 312–318

Bloating before and after fundoplication +/- pyloroplasty
World J Surg. 2007;31(2):332-6
*
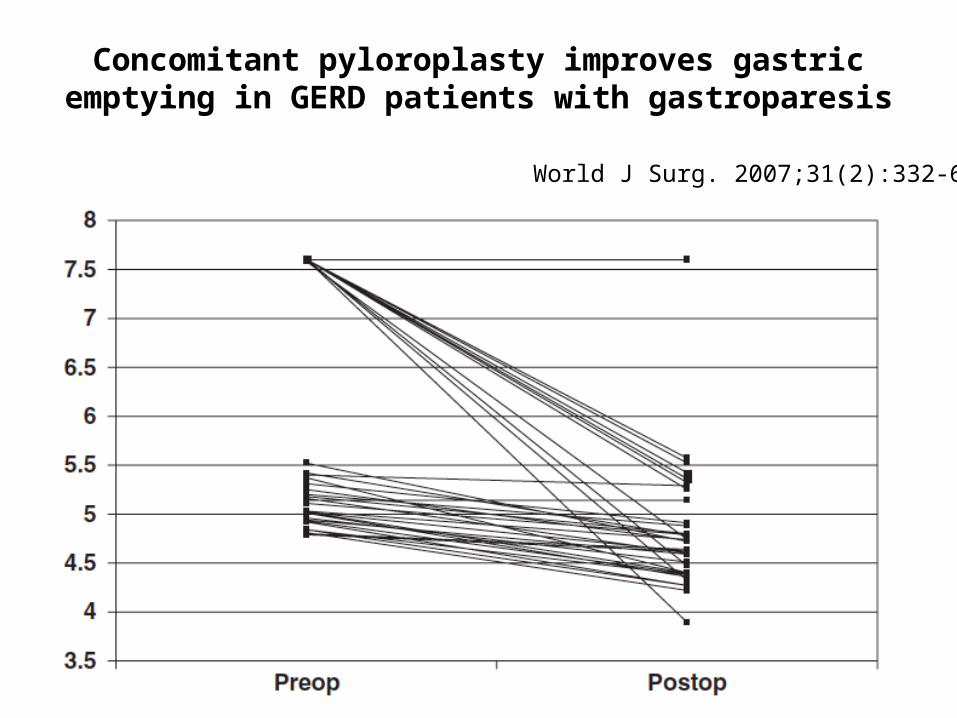
Concomitant pyloroplasty improves gastric emptying in GERD patients with gastroparesis
World J Surg. 2007;31(2):332-6

Medical therapy of mild to moderate gastroparesis
• Dietary modification• Liquid supplements• Metoclopramide• Domperidone• Erythromycin• Antiemetics• PPI
Camilleri, M. N Engl J Med 2007; 356:820

Medical therapy of severe gastroparesis
• Pyloric BoTox injection• Enterra• Venting PEG & feeding PEJ• Subtotal gastrectomy & Roux-en-Y gastro-
jejunostomy
Camilleri, M. N Engl J Med 2007; 356:820

Pyloric motility and BoTox injection for gastroparesis

Pyloric BoTox for gastroparesis
GES Symptoms0
10
20
30
40
50
60
5255
% improvement at 2 months, n=6
Ezzedine et al. GIE. 2002;55:920-3

Enterra® for refractory post-surgical gastroparesis
GES Symptoms0
10
20
30
40
50
60
4853
% improvement at 60 months n=31
McCallum et al .CGH 2011

Small bowel bacterial overgrowth
• Diagnosed by lactulose breath test (early rise in hydrogen production)
• Treatment with antibiotics– Rifaximin– Augmentin plus metronidazole– Septra plus metronidazole– Norfloxacin

Conclusions
• Post-fundoplication syndromes are multifaceted and require thorough evaluation
• Revisional surgery may be needed
• Medical therapy for gas bloat and gastroparesis is complex and suboptimal




![1877.] Medicine. 241 MEDICINE.](https://static.documents.pub/doc/80x56/6248decce7f255195063a334/1877-medicine-241-medicine.jpg)












