37
A glance at: Bronchopulmonary Dysplasia Mohammad Rezaei Pediatric Pulmonologist
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | mohammad-rezaei |
| View: | 247 times |
| Download: | 3 times |

A glance at:
Bronchopulmonary Dysplasia
Mohammad Rezaei
Pediatric Pulmonologist
The 2010 NICHD Neonatal Research Network estimated that as many as 68% of VLBW infants can be diagnosed with BPD.

BPD First described by Northway & colleagues in 1967
Prematures with RDS:
Died in first week
or
Survived without Respiratory morbidity
improved survival
But
new chronic lung disease in a group of premature infants who had RDS and had received prolonged ventilation with high FiO2
resulted in dramatic changes in the clinical course and outcomes of premature newborns with RDS.
the overall incidence of BPD has not declined over the past decade
But
its severity has been clearly modulated by changes in clinical practice.
Before
1960
1960Introduction
of mechanical ventilation
prenatal steroid usesurfactant therapy
management of PDA new ventilator strategy
improved nutritionAnd …..
DEFINITION
In 1979, Bancalari and colleague offered the first alterationto Northway’s original definition:
• supplemental oxygen requirement at 28 days
• chronic changes on chest radiograph
• tachypnea with crackles or retractions.
in 1988: a criterion for BPD was then defined as oxygensupplementation at 36 weeks’ postmenstrual age (PMA).
At June 2000: New definition by NIH consensus conference
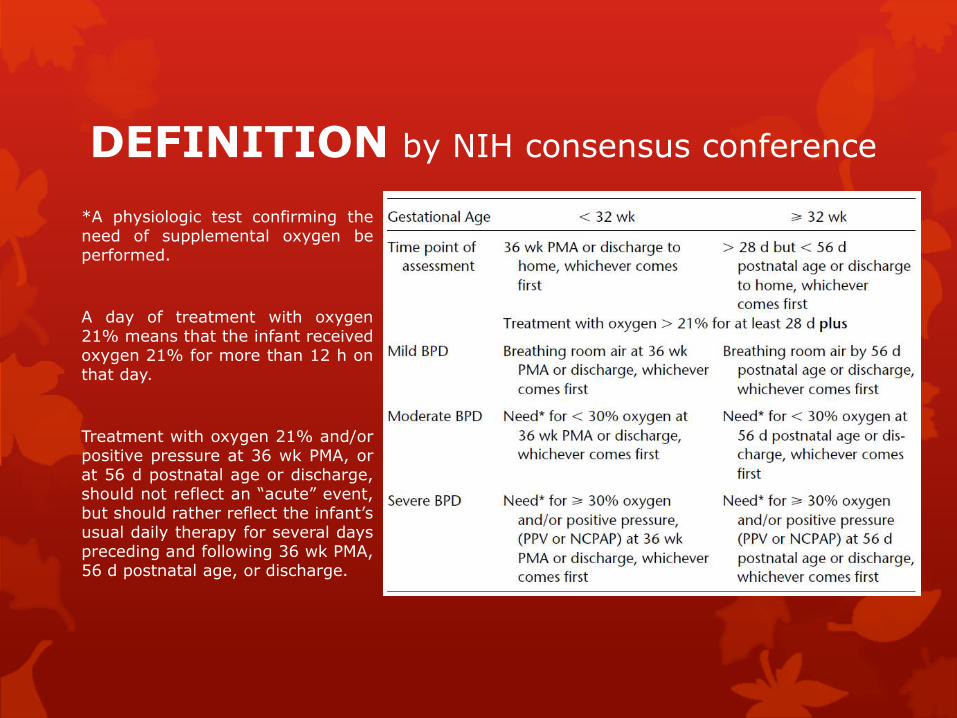
DEFINITION by NIH consensus conference
*A physiologic test confirming theneed of supplemental oxygen beperformed.
A day of treatment with oxygen21% means that the infant receivedoxygen 21% for more than 12 h onthat day.
Treatment with oxygen 21% and/orpositive pressure at 36 wk PMA, orat 56 d postnatal age or discharge,should not reflect an “acute” event,but should rather reflect the infant’susual daily therapy for several dayspreceding and following 36 wk PMA,56 d postnatal age, or discharge.
EPIDEMIOLOGY
Pulmonary immaturity is the primary risk factor for BPD
Risk of BPD is inversely related to both birthweight and gestational age at birth.
• (85% in neonates between 500-699 g)
• (5% in infants with birth weights >1500 g)
Currently, most infants who develop BPD are born with extreme prematurity, and 75% of cases have birth weights <1000 g
Factors that modify BPD risk :
gestational immaturity
lower birth weight
male sex
white or nonblack race
family history of asthma
SGA
absence of maternal glucocorticoid treatment
lower Apgar scores
perinatal asphyxia
respiratory distress syndrome.
Smoking
pre-eclampsia
Chorioamnionitis
intrauterine growth restriction
Early respiratory support
greater severity of initial pulmonary disease ( pneumothorax, pulmonary interstitial emphysema, and severe atelectasis)
patent ductus arteriosus
pulmonary edema
higher weight-adjusted fluid intake
earlier use of parenteral lipid
light-exposed parenteral nutrition
duration of oxygen therapy.
duration and approach to mechanical ventilation (High FiO2/ High PIP/ High RR/ Low PEEP)
Colonization or infection with Ureaplasmaurealyticum
postnatal sepsis
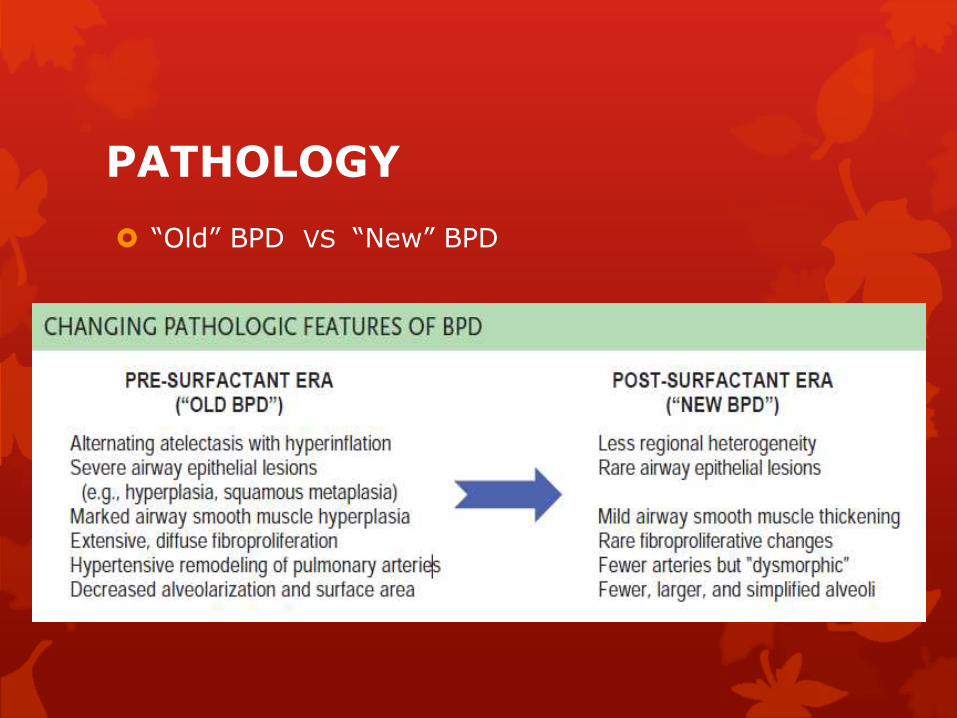
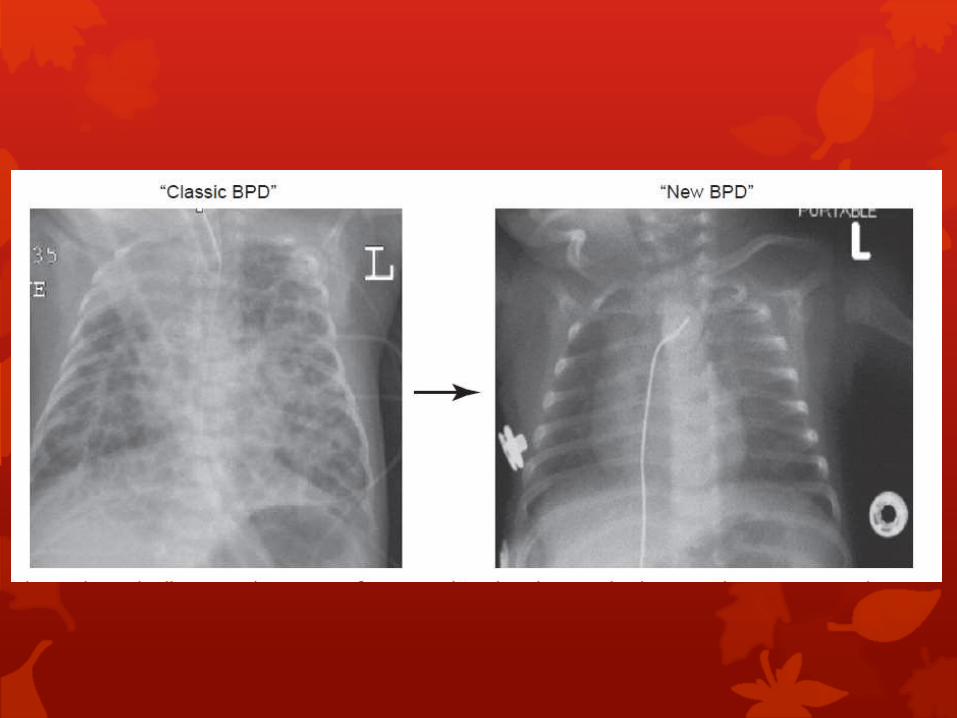
PATHOLOGY
“Old” BPD VS “New” BPD

PATHOLOGY

“New” BPD: disruption of distal Lung growth
Decreased, large and simplified alveoli
(alveolar hypoplasia, decreased acinar complexity)
Decreased, dysmorphic capillaries
Variable interstitial fibroproliferation
Less severe arterial/arteriolar vascular lesions
Negligible airway epithelial lesions
Variable airway smooth muscle hyperplasia
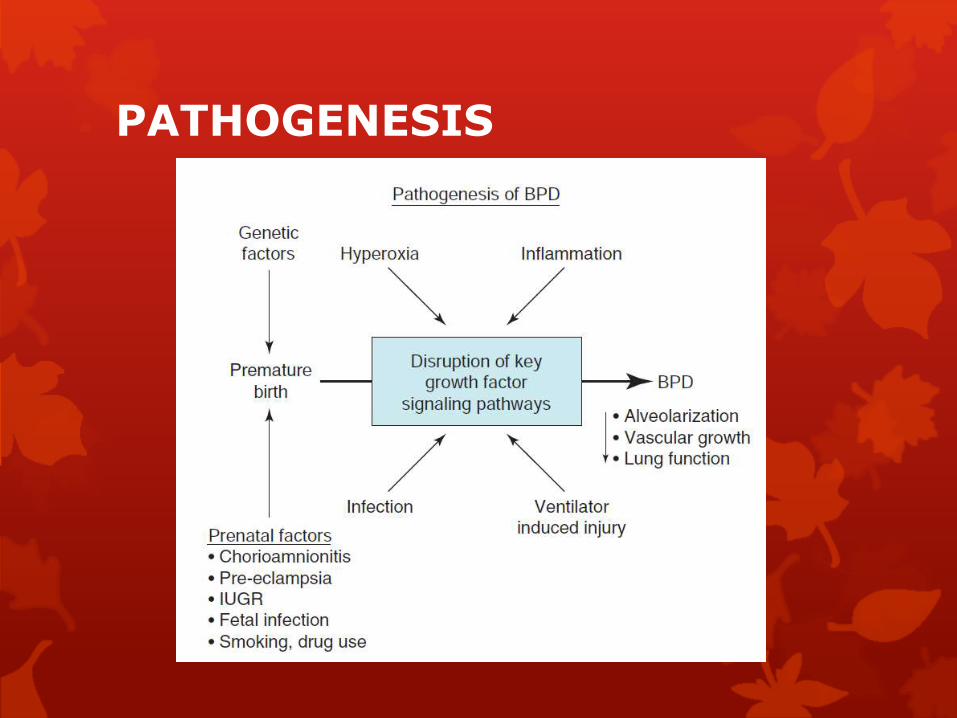
PATHOGENESIS

Oxygen Toxicity
Lungs of premature infants are relatively
deficient in antioxidant
enzyme system
High O2:Increases theproduction of
ROS
BPD
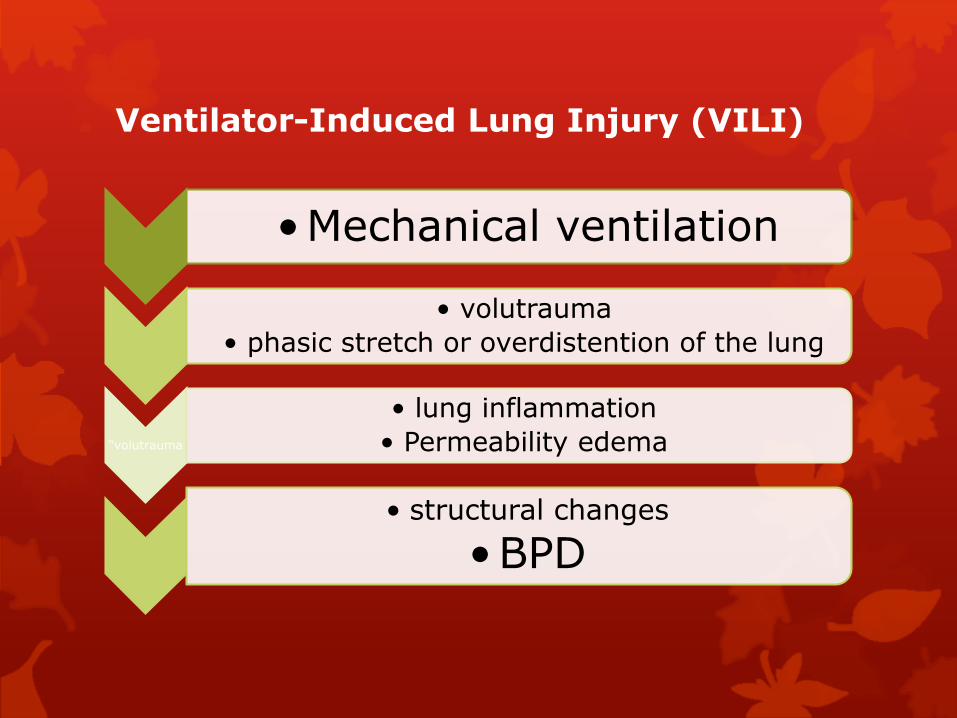
Ventilator-Induced Lung Injury (VILI)
•Mechanical ventilation
• volutrauma
• phasic stretch or overdistention of the lung
“volutrauma
• lung inflammation
• Permeability edema
• structural changes
•BPD

Inflammation
plays a central role in the pathobiology of BPD
Oxygen toxicity, volutrauma, and infection can induce early and sustained inflammatory responses that promote the recruitment and activation of neutrophils, which persists in infants who develop BPD.

Genetic Susceptibility
risk for developing BPD is markedly influenced by complex interactions between genetic and environmental risk factors.
as strong a role for genetic factors in BPD as observed in such complex diseases in adults as:
systemic hypertension (30%)
cancer (42%)
psychiatric disorders (> 60%)

PATHOGENESIS
Infection
PDA

PATHOPHYSIOLOGY

PATHOPHYSIOLOGY
Respiratory Function

Pulmonary Circulation
Endothelial cells are particularly susceptible to oxidant injury due to hyperoxiaor inflammation.
smooth muscle cell proliferation, precocious maturation of immature pericytes into mature smooth muscle cells, and incorporation of fibroblasts into the vessel wall and surrounding adventitia
Structural changes in the lung vasculature contribute to high pulmonary vascular resistance (PVR) due to narrowing
Decreased angiogenesis may limit vascular surface area, causing further elevations of PVR
a marked vasoconstrictor response to acute hypoxia
Early injury to the lung circulation leads to the rapid development of PH
In severe BPD, decreased vascular growth occurs in conjunction with marked reductions in alveolar formation impairs gas exchange causes marked hypoxemia

Cardiovascular Abnormalities
In addition to pulmonary vascular disease and right ventricular hypertrophy, other cardiovascular abnormalities associated with BPD include:
left ventricular hypertrophy (LVH)
systemic hypertension
development of prominent systemic-to-pulmonary collateral vessels.

PATHOPHYSIOLOGY
Respiratory Function
Pulmonary Circulation
Cardiovascular Abnormalities

LONG-TERM OUTCOME
Approximately 50% of infants with BPD will require hospital re-admission during early childhood
rate of hospitalization generally declines during the second and third year of life
but lung function studies often show limited reserve even in patients with minimal overt respiratory signs

LONG-TERM OUTCOME
Infants with severe BPD often develop COPD.
In the majority of BPD infants, lung growth and remodeling during infancy results in progressive improvement of gas exchange, lung function, and level of oxygen therapy.
few BPD patients remain oxygen dependent beyond 2 years of age.
Lung function is usually in the low-normal range by 2 to 3 years of age, but air flow abnormalities may remain.

LONG-TERM OUTCOME
Although pulmonary function in most survivors with BPD improves over time and permits normal activity, abnormalities detected by PFT often persist through adolescence, including increased airway resistance and reactivity.
LONG-TERM OUTCOME
Chest x-ray findings during follow-up are generally nonspecific (typically including hyperinflation with peribronchial
cuffing and scattered interstitial infiltrates consistent with fibrosis,
edema, or atelectasis.)
These findings tend to clear with age and are very insensitive markers of changes in lung function.
CT scans ??

PREVENTION
there is no single therapy or prevention strategy except for the prevention of premature birth.

PREVENTION
Antenatal Steroids
NIV
Strategy of mechanical vetilation
Fluid restreiction ??
Treatment of PDA ?
Nutritional support
Vit A ?
Corticosteroids ?
Caffeine (reduce the risk of BPD by 50%)
iNO ?

TREATMENT
Supplemental oxygen
Diuretics
Bronchodilators
Steroids
Antiviral Immunization
Pulmonary Hypertension
TREATMENT
Supplemental oxygen
remains a mainstay of therapy for infants with BPD
(most appropriate target for oxygen saturation levels ??)

TREATMENT
Diuretics
improve pulmonary compliance and airway resistance by reducing lung edema
furosemide
thiazides and spironolactone
TREATMENT
Bronchodilators
Infants with BPD have airway smooth muscle hypertrophy and often have signs of bronchial hyperreactivity that acutely improve with bronchodilator therapy; but response rates are variable.
β-agonists and anticholinergics
Methylxanthines ,aminophylline and caffeine
TREATMENT
Steroids
Overall, glucocorticoid treatment improves lung mechanics and gas exchange, facilitating earlier extubation.
one study showed that inhaled steroids can improve the rate of successful extubation and reduce the need for systemic steroids.

TREATMENT
Antiviral Immunization
Infants with BPD are at increased risk of recurrent respiratory tract infections, especially those due to RSV
The American Academy of Pediatrics recommendations include the use of Palivizumab or RSV-IVIG prophylaxis for infants and children <2 years of age with BPD who required oxygen therapy for their lung disease prior to RSV season. Older infants with more severe BPD may benefit from prophylaxis for two RSV seasons.
TREATMENT
Pulmonary Hypertension
initial clinical strategy for the management of PH in infants with BPD begins with treating the underlying lung disease.
(extensive evaluation for chronic reflux and aspiration, structural airway abnormalities (e.g., tonsillar and adenoidal hypertrophy, vocal cord paralysis, subglottic stenosis, and tracheomalacia), assessments of bronchial reactivity, improving lung edema and airway function, and other pulmonary considerations.)
Periods of acute hypoxia, whether intermittent or prolonged, can often contribute to late PH in BPD ----> sleep study
strongly encourage cardiac catheterization prior to the initiation of chronic therapy
Current therapies : NO, sildenafil, endothelin-receptor antagonists (ETRAs), and calcium channel blockers
sildenafil or bosentan

When you stop learning, You stop growing

















