74
A H Gershlick University Hospital of Leicester UK AA 2008 Who should we rescue ?

A H Gershlick
University Hospital of Leicester UK
A H Gershlick
University Hospital of Leicester UK
AA 2008
Who should we rescue ?Who should we rescue ?
Thrombolysis Tissue Plasminogen activator

150 000 patients
53% early reperfusion
52% thrombolysis
Thrombolysis studied in 45 000 ptThrombolysis studied in 45 000 pt20-30 lives saved / 100020-30 lives saved / 1000
Thrombolysis studied in 45 000 ptThrombolysis studied in 45 000 pt20-30 lives saved / 100020-30 lives saved / 1000

Acute MI Catchments Tertiary PCI Catchments
Is P-PCI deliverable everywhere

While there is still lysis, there will be lytic failure While there is still lysis, there will be lytic failure
Failure ? :
“TIMI 3”
In the real world
? ST segment resolution @ 60/ 90 min
Failure ? :
“TIMI 3”
In the real world
? ST segment resolution @ 60/ 90 min
X
Normal FlowNormal Flow
60% 40%
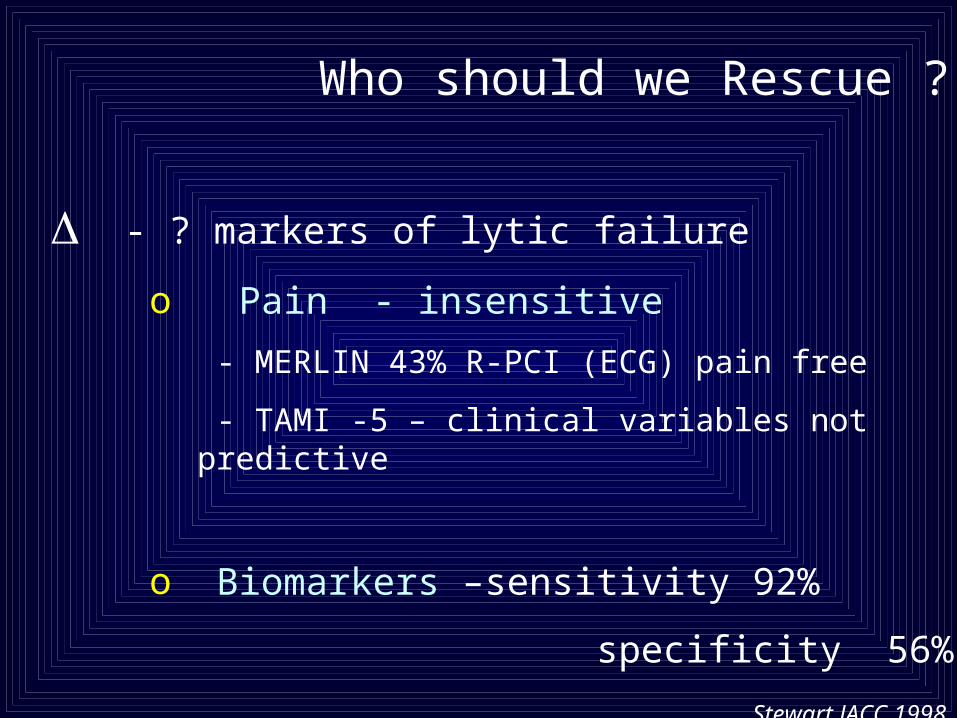
Who should we Rescue ?
- ? markers of lytic failure
o Pain - insensitive
- MERLIN 43% R-PCI (ECG) pain free
- TAMI -5 – clinical variables not predictive
o Biomarkers –sensitivity 92%
specificity 56%
Stewart JACC 1998 31 1499


Schroder R et al. JACC 1995;26:1657-1664
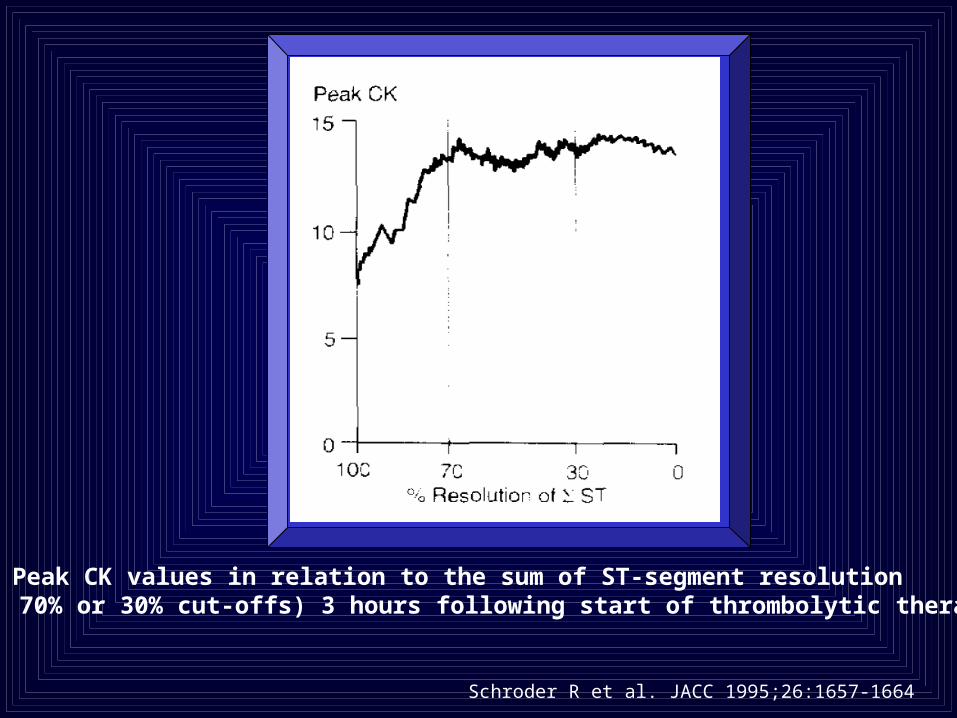
Peak CK values in relation to the sum of ST-segment resolution (100%, 70% or 30% cut-offs) 3 hours following start of thrombolytic therapy
Schroder R et al. JACC 1995;26:1657-1664
The Data :
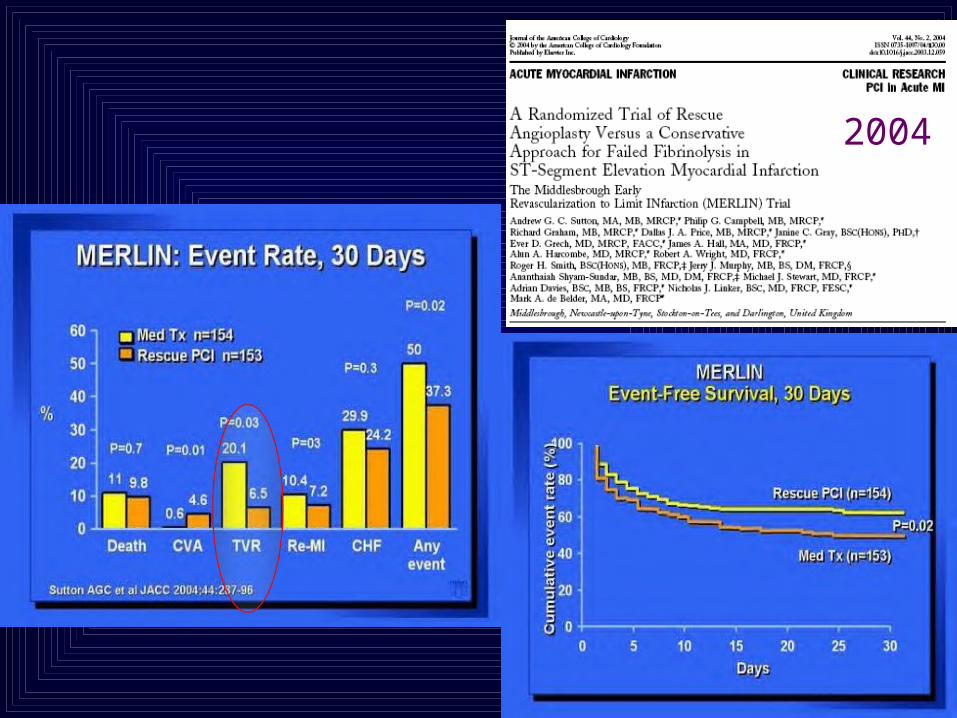
2004



Cumulative Event-free Survival following R-PCI versus Conservative Therapy
REACT MERLIN
Gershlick AH et al NEJM 2005;353:2758-2768 Sutton AGC et al JACC 2004;44:287-296

Differing Methodology: REACT versus MERLIN
Centres 35 5
ST Resolution 50% at 90mins 50% at 60 mins 10% had TIMI III at angios 40% TIMI III at angio
SK 58% 96%
Stents 69% 50%
GP IIb-IIIa use 43% 3%
PCI arm- PCI mandated not mandated completed in 96.5% completed in 66%
PCI within 30 days 2% of conservative group 20% conservative group
Recruitment 3.3 patients /centre/ year 30.7 patients/centre/year
Heart failure “NYHA III or IV” Diuretics

Outcome
MERLIN versus REACT @ 1 year
Outcome
MERLIN versus REACT @ 1 year

12 month
&
Long term
12 month
&
Long term
REACT TrialREACT Trial

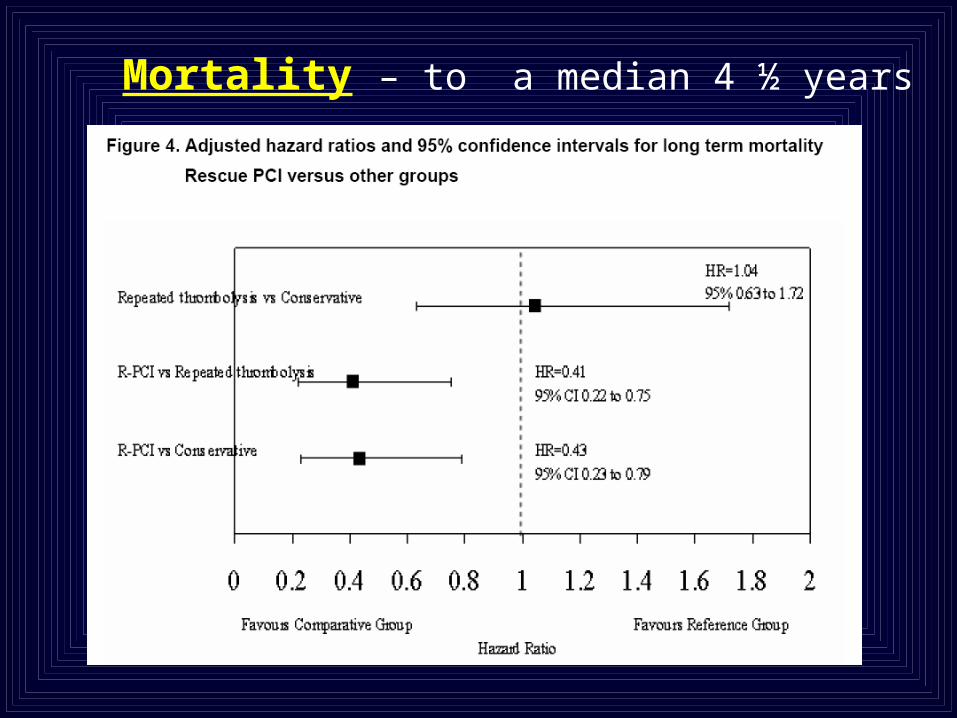
Mortality – to a median 4 ½ years
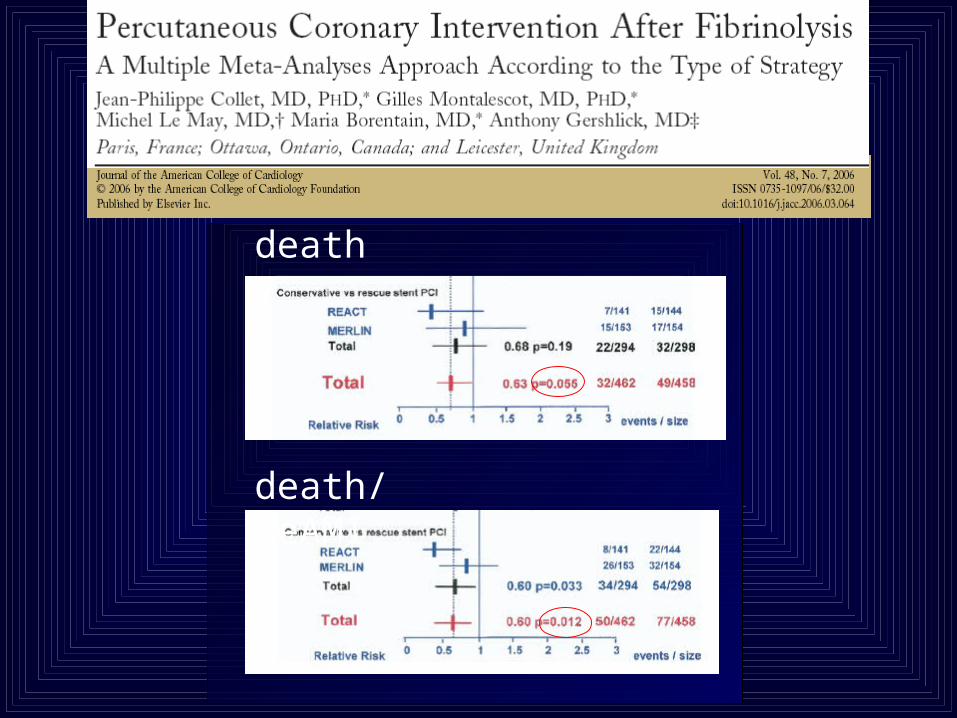
death
death/reAMI
RESCUE PCI – HOW DO THE OUTCOMES FROM ‘REAL-WORLD’ PATIENTS COMPARE
TO THE PUBLISHED TRIALS ?
• 185 Consecutive Rescue PCI patients April 2005-August 2007 @ glenfield
• Clinical follow-up via PCI database, case-note review and ONS, at a mean of 4.5months
• Mean (SD) delay from symptom onset to PCI =501 (229) minutes [8.35 hours], range 145-2240 min
Kelly DJ, Siddiqui N, Holt M, Gershlick AH-Submitted to BCS

2007 R-PCI Registry vs REACT Trial
* Mean 4.5month Follow-up **6/12 Follow-up
7
2.2
0.5
10.3
6.2
2.1
4.9
15.3
0
2
4
6
8
10
12
14
16
%
2007 Registry* REACT Trial**
DeathRe-AMICVAHeart FailureMACE

Local vs Transfer Patientsp=0.322
p=0.42
Mean Delay 438min Mean Delay 525min
3.7
9.38.4
11.5
0
2
4
6
8
10
12
%
Local PCICentre Patients
TransferredPatients
MortalityMACE
7.3 hrs 8.75 hrsMean Delay S-B

When ? : Timing issues
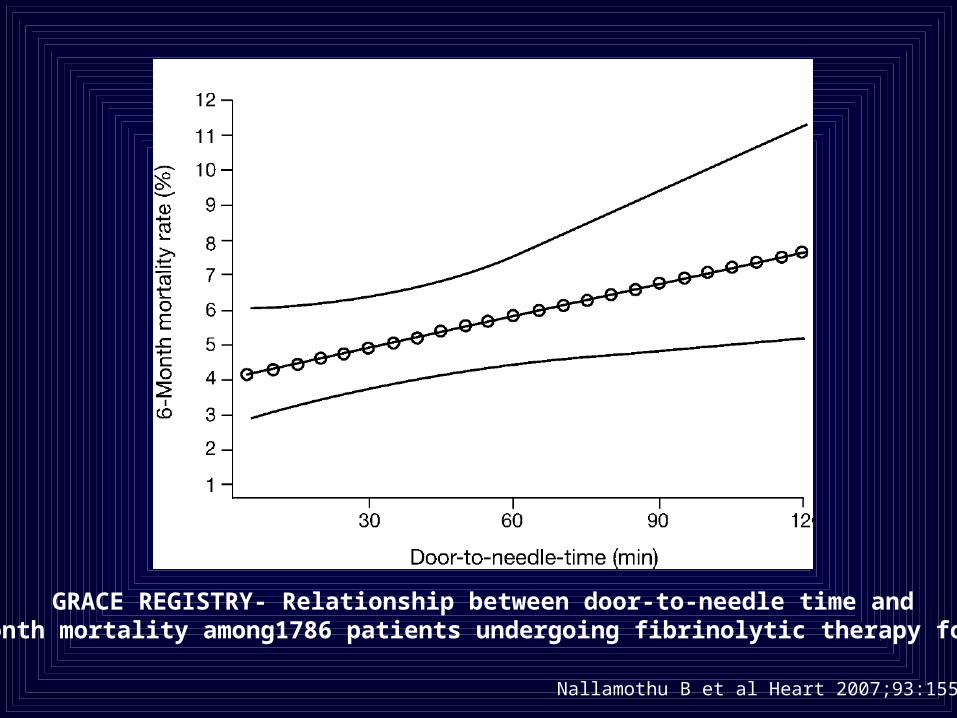
GRACE REGISTRY- Relationship between door-to-needle time and 6-month mortality among1786 patients undergoing fibrinolytic therapy for AMI
Nallamothu B et al Heart 2007;93:1552-5

Time (hrs)
Lytic to R-PCI
Symptom to R-PCI
4.6 hours 6.9 hours
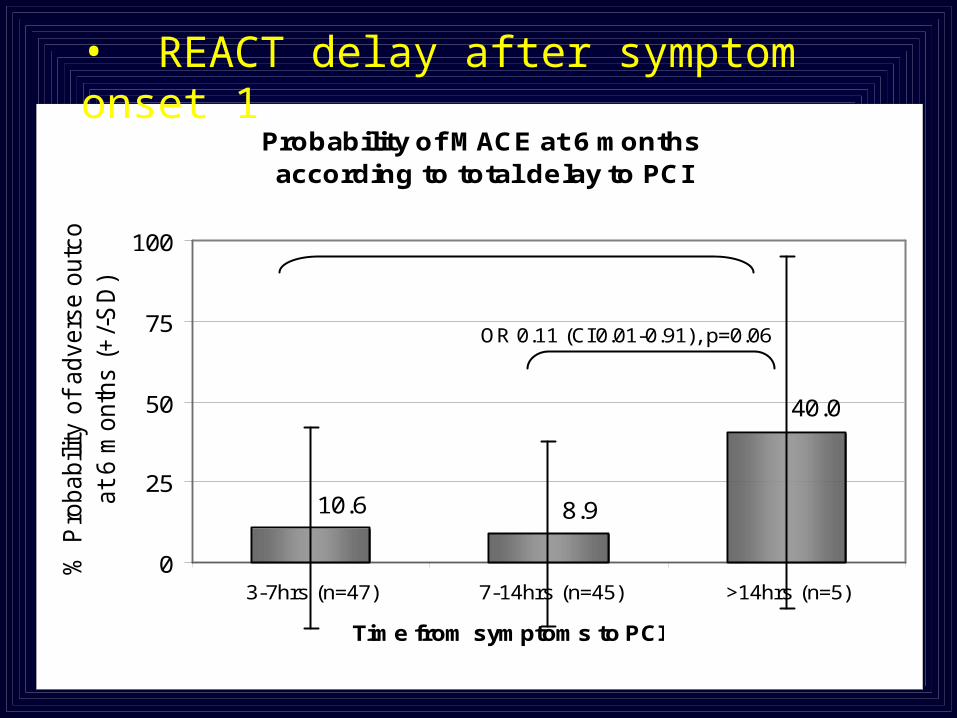
Probability of MACE at 6 months according to total delay to PCI
10.6 8.9
40.0
0
25
50
75
100
3-7hrs (n=47) 7-14hrs (n=45) >14hrs (n=5)
Time from symptoms to PCI
% P
robabili
ty o
f advers
e o
utc
om
e
at
6 m
onth
s (
+/-
SD
)
OR 0.11 (CI 0.01-0.91), p=0.06
OR 0.22 (CI 0.03-1.6), p=0.57
• REACT delay after symptom onset 1

Mortality versus Tertile of Delay (Symptom onset to R-PCI)
*Mean Delay from Symptom Onset to R-PCI (all patients)
p=0.09
3.2
4.8
13.1
0
2
4
6
8
10
12
14
All-cause Mortality
(%)
Shortest 290min*
Mid tertile485 min
Longest 694min
Registry

Rescue PCI :
o All failed lytic (25%-30%)
failure to resolve max St to > 50% at 90 mins
o As soon as possible (Sympt - balloon < 3 hrs)
Who not to “rescue”

1082 PCI 1084 OMT
3–28 days post AMI


“Mm… shall I give repeat thrombolysis ?”
REACT –
Bleeding Outcomes
REACT –
Bleeding Outcomes
5
15
20
10
4.9
2.1
18.7
3.5
8.58.4
%%
MAJOR ( > 3g/dl)
MAJOR ( > 3g/dl)
Lysis C RPCI Lysis C RPCI
OVERT Bld No OVERT Bld OVERT Bld No OVERT Bld
22/27
(82%) sheath
22/27
(82%) sheath
3 HPericard
1 Death
3 HPericard
1 Death 1 H thorax
1 Death
1 H thorax
1 Death
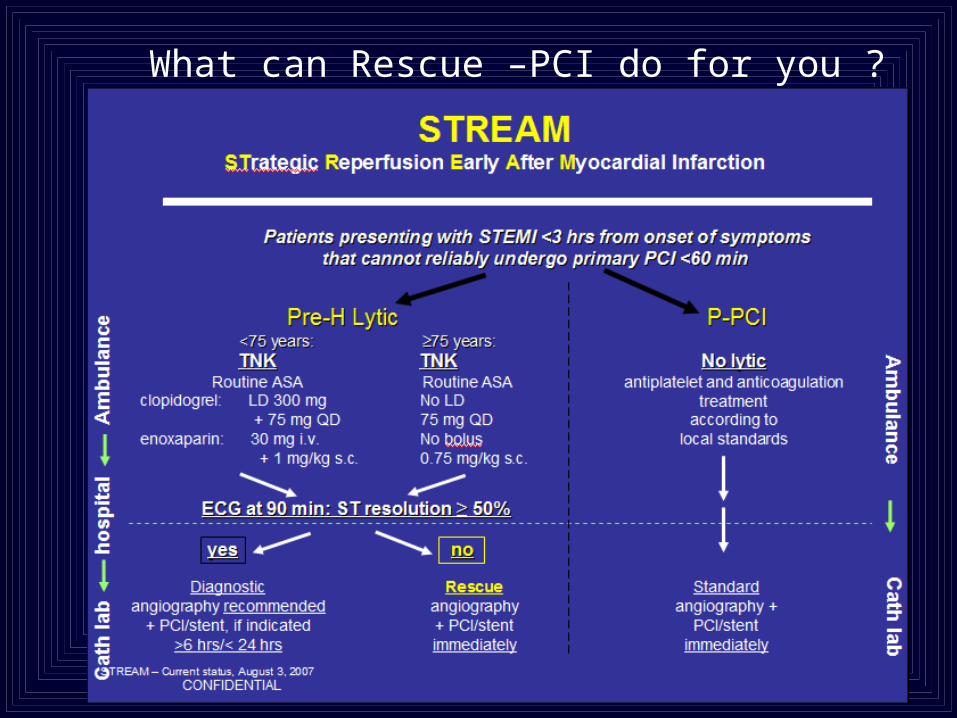
What can Rescue –PCI do for you ?

Pre-Hospital Lysis @ 4.30 am
ECG @ 6 am
Angio @ 6.45
Pre-Hospital Lysis @ 4.30 am
ECG @ 6 am
Angio @ 6.45

RESCUE–PCI should be mandated
& be part of AMI protocols
Repeat lytic may be dangerous
RESCUE–PCI should be mandated
& be part of AMI protocols
Repeat lytic may be dangerous

R-PCI trials

30.7
3.3 2.4
13.99.5
0
5
10
15
20
25
30
35
Recruitment per Centre per Year
MERLIN REACT RESCUE I MERLIN* MERLIN**
RECRUITMENT RATES AMONG RESCUE PCI TRIALS
*1st anterior ‘failed reperfusion’**1st anterior ‘occluded LAD’
Adapted from Kunadian B, et al. J Invasive Cardiol 2007 Sep;19(9):359-68

MERLIN: 30-day Mortality according to ST-segment resolution 6 hours after initiation of fibrinolytic therapy
Sutton et al JACC 2004;44:287-96

Timing of AMI Rx
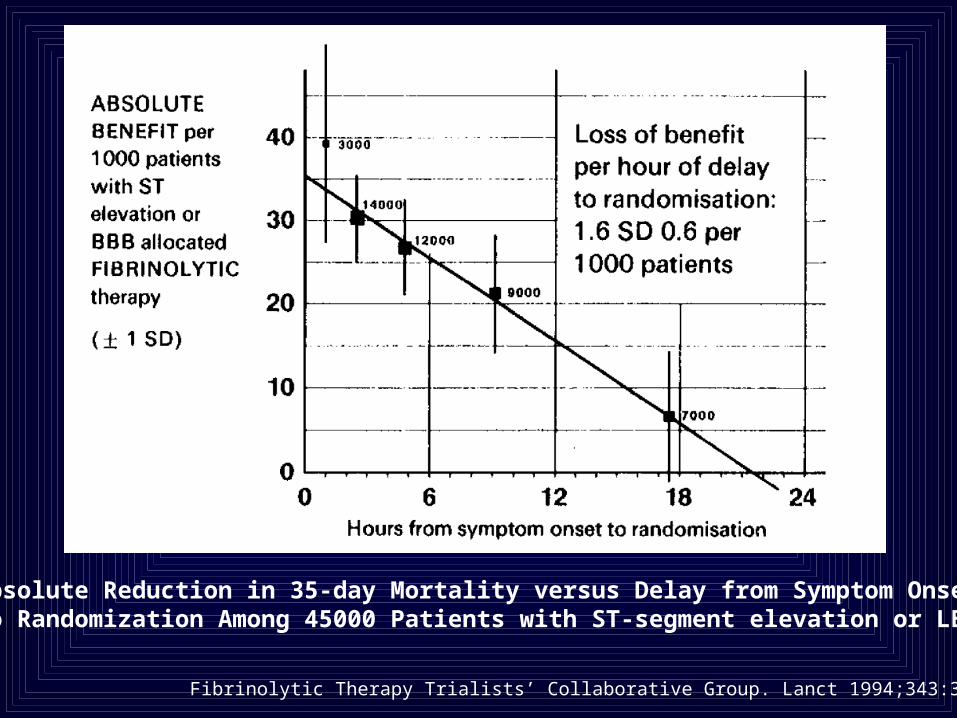
Absolute Reduction in 35-day Mortality versus Delay from Symptom Onset to Randomization Among 45000 Patients with ST-segment elevation or LBBB
Fibrinolytic Therapy Trialists’ Collaborative Group. Lanct 1994;343:311-322

Use of reperfusion therapy in 376,753 patients from NRMI-4 with STEMI or LBBB within 12 hours of symptom onset
Curtis JP et al JACC 2006;47:1544-52

GRACE REGISTRY- Relationship between door-to-needle time and 6-month mortality among 2173 patients undergoing Primary PCI for AMI
Nallamothu B et al Heart 2007;93:1552-5

Wiviott SD et al JACC 2004;44:783-9)
Mortality versus NRMI-4 Risk Index following AMI

Curtis JP et al JACC 2006;47:1544-52

Thrombolysis Primary PCI


Denmark
Czech Republic


REACT (REscue Angioplasty v Conservative treatment or repeat Thrombolysis )
ECGECG 90 min90 min post (post (anyany incl SK) thrombolytic incl SK) thrombolytic
ST < 50 % resolution (with or without pain)
CONSENT & RANDOMISE
Conservative 2 nd thrombolytic Coronary Angio 24 iv heparin Accelerated tPA or +/- PCI Reteplase
primary end point: 6/12 ~death/re-infarction/severe HF/CVA
REACT (REscue Angioplasty v Conservative treatment or repeat Thrombolysis )
ECGECG 90 min90 min post (post (anyany incl SK) thrombolytic incl SK) thrombolytic
ST < 50 % resolution (with or without pain)
CONSENT & RANDOMISE
Conservative 2 nd thrombolytic Coronary Angio 24 iv heparin Accelerated tPA or +/- PCI Reteplase
primary end point: 6/12 ~death/re-infarction/severe HF/CVA
2000
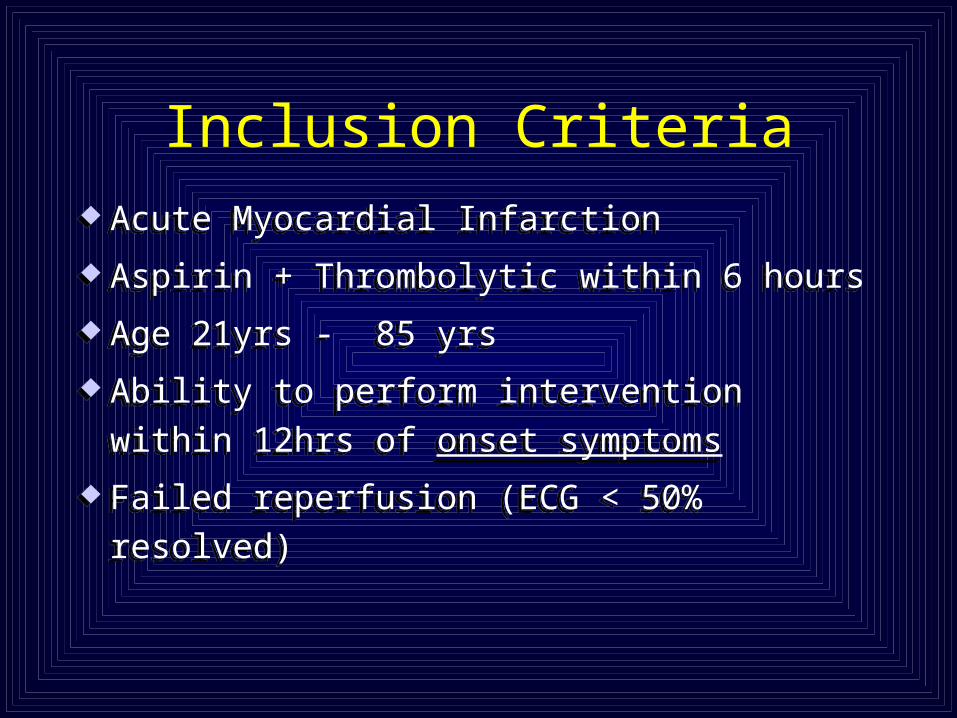
Inclusion Criteria
Acute Myocardial Infarction
Aspirin + Thrombolytic within 6 hours
Age 21yrs - 85 yrs
Ability to perform intervention within 12hrs
of onset symptoms
Failed reperfusion (ECG < 50% resolved)
Acute Myocardial Infarction
Aspirin + Thrombolytic within 6 hours
Age 21yrs - 85 yrs
Ability to perform intervention within 12hrs
of onset symptoms
Failed reperfusion (ECG < 50% resolved)

Exclusion CriteriaExclusion CriteriaExclusion CriteriaExclusion Criteria Safety pre-requisites pre randomisation Safety pre-requisites pre randomisation
(thrombolytic) (thrombolytic)
a. Hb, Hct & platelet count a. Hb, Hct & platelet count
b. Weight (< 65 kg)b. Weight (< 65 kg)
c. Age (> 85 y) c. Age (> 85 y)
d. Any evidence bleedingd. Any evidence bleeding
e. Hypertension during admissione. Hypertension during admission(after administration first lytic; age ) (after administration first lytic; age )
f. CGSf. CGS
{g. LMW heparin}{g. LMW heparin}
Safety pre-requisites pre randomisation Safety pre-requisites pre randomisation (thrombolytic) (thrombolytic)
a. Hb, Hct & platelet count a. Hb, Hct & platelet count
b. Weight (< 65 kg)b. Weight (< 65 kg)
c. Age (> 85 y) c. Age (> 85 y)
d. Any evidence bleedingd. Any evidence bleeding
e. Hypertension during admissione. Hypertension during admission(after administration first lytic; age ) (after administration first lytic; age )
f. CGSf. CGS
{g. LMW heparin}{g. LMW heparin}

6 month data 6 month data
REACT TrialREACT Trial

Primary composite endpoint:(death and non-fatal re-AMI, CVA , Severe HF)
Primary composite endpoint:(death and non-fatal re-AMI, CVA , Severe HF)
RESULTS No. of subjects with a component of the Composite Primary End Point @ any time within 6 months
N=142
R-LYSIS
N=142
R-LYSIS
N=141
Conservative
N=141
Conservative
N=144
R-PCI
N=144
R-PCI
44
(31.0%)44
(31.0%)42
(29.8%)42
(29.8%)22
(15.3%)22
(15.3%)
R-PCI v Repeat lytic p< 0.001
R-PCI v Conservative p< 0.01
Repeat lytic v Conservative NS
R-PCI
R-lysis
C

40036032028024020016012080400
No. of Days
100
80
60
40
20
0
Eve
nt
Fre
e S
urv
ival
(%
)Time to First Event at 12 Months
P=0.004
R-PCI
Rpt Lysis
Conser
91% F-up91% F-up

18 2
18 3
9 2
18 2
14 0
4 1
0-6 months 6-12 months
3 0
4 0
1 0
21 3
22 2
13 1
0-6 months 6-12 months
33 5
29 14
19 5
Re-vasc
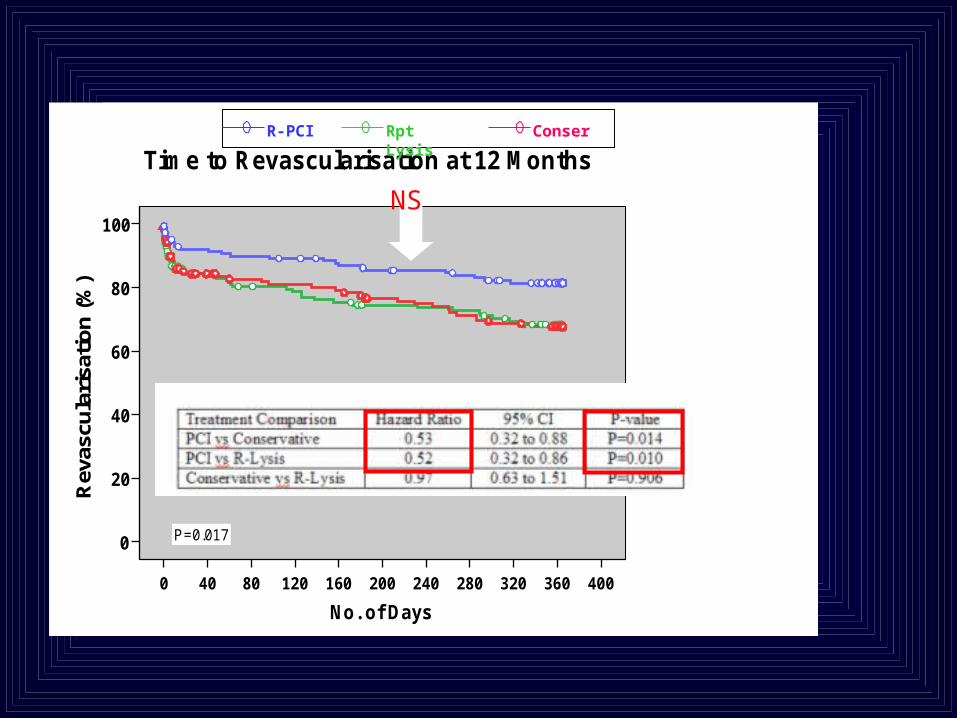
40036032028024020016012080400
No. of Days
100
80
60
40
20
0
Rev
ascu
lari
sati
on
(%
)
Time to Revascularisation at 12 Months
P=0.017
R-PCI Rpt Lysis Conser
NS
Mortality Mortality
REACT TrialREACT Trial

0.13

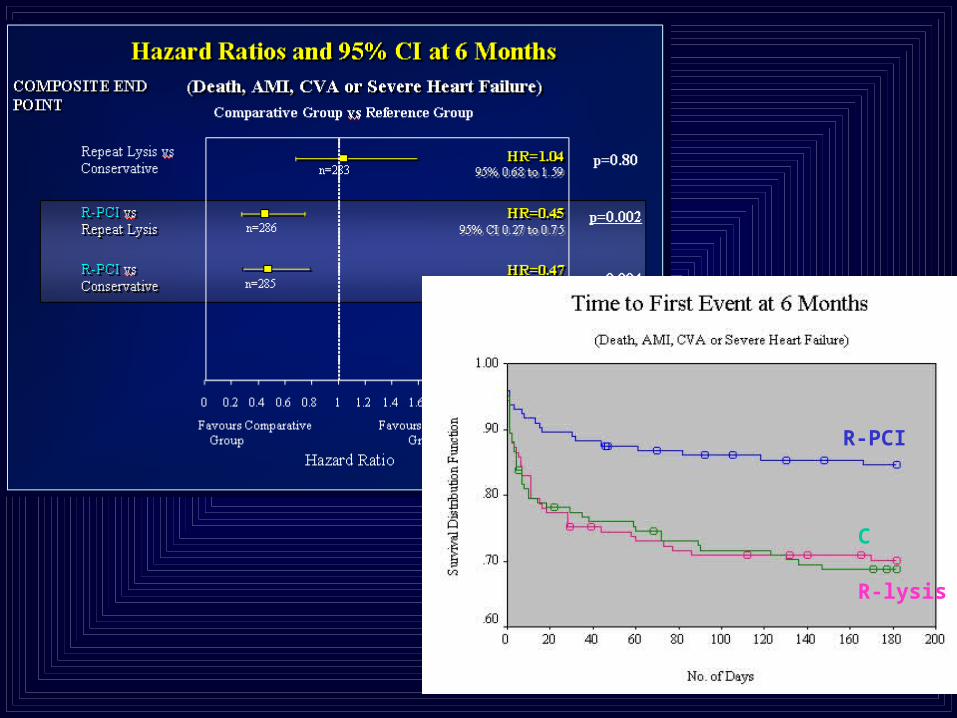
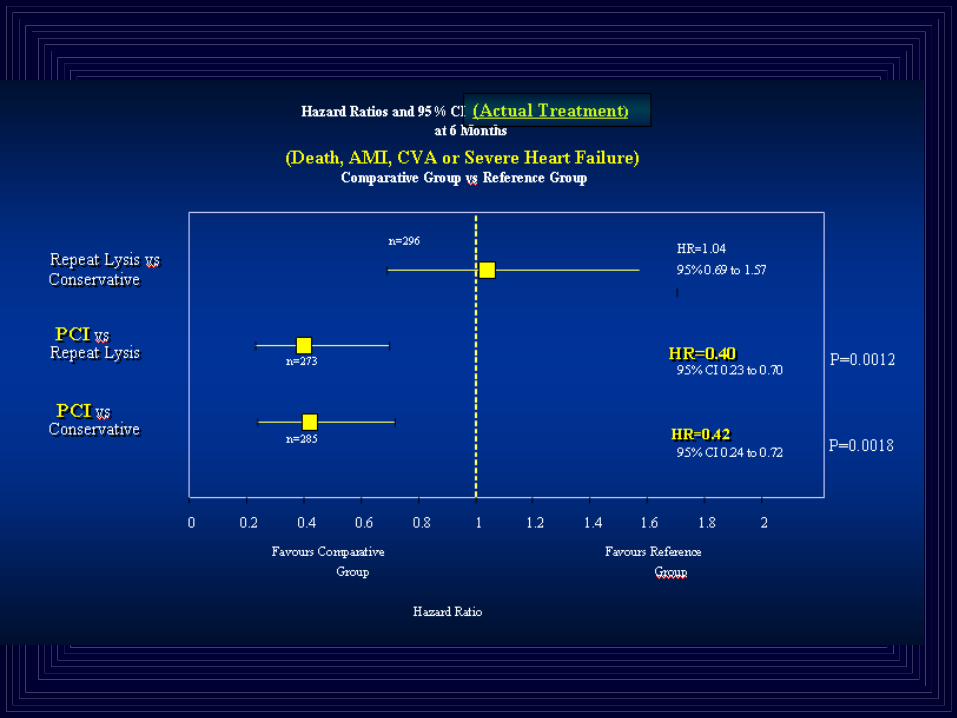
Hazard Ratios and 95% CI of Mortality at 6 Months Hazard Ratios and 95% CI of Mortality at 6 Months
R-PCI vsR-PCI vsConservativeConservative
Repeat Lysis vsConservative
R-PCI vsR-PCI vsRepeat LysisRepeat Lysis
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 2Favours Comparative Favours Reference
Group Group
Hazard Ratio
HR=0.48HR=0.4895% CI 0.21 to 1.0695% CI 0.21 to 1.06
HR=0.48HR=0.4895% CI 0.21 to 1.0695% CI 0.21 to 1.06
HR=1.00HR=1.0095% 0.52 to 1.9295% 0.52 to 1.92
n=285
n=286
n=283
Comparative Group vs Reference Group
p= 0.07p= 0.07
p=0.07p=0.07
Longer term mortality
ONS
Patient specific NHS No.

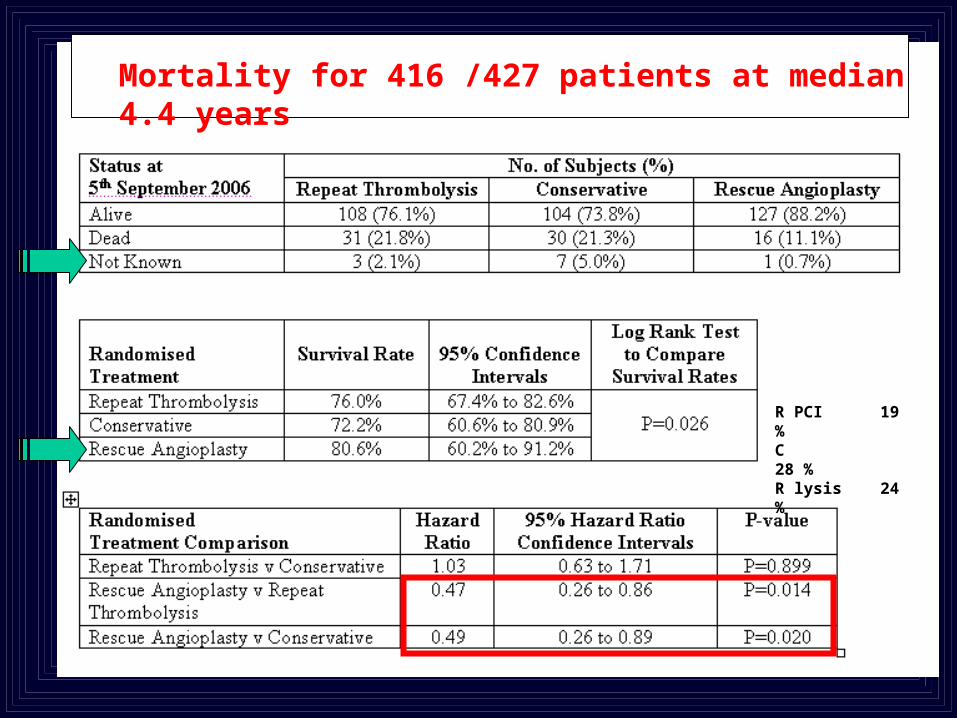
Mortality for 416 /427 patients at median 4.4 years
R PCI 19 %C 28 % R lysis 24 %

REACT trial Longer term outcome
Events and difference in outcome happens early
Benefit is maintained out to 12 months
Late (4.4) year data indicates longer term mortality benefit
In general R-PCI Where lysis is still a reperfusion strategy
• Failed lysis (< 50% ST segment resolution @ 90 mins) should be treated with Rescue – PCI
• R-PCI should be part mandated reperfusion protocols
• timing issues are unresolved ASAP (within 3 hours of ECG )
REACT trial Longer term outcome
Events and difference in outcome happens early
Benefit is maintained out to 12 months
Late (4.4) year data indicates longer term mortality benefit
In general R-PCI Where lysis is still a reperfusion strategy
• Failed lysis (< 50% ST segment resolution @ 90 mins) should be treated with Rescue – PCI
• R-PCI should be part mandated reperfusion protocols
• timing issues are unresolved ASAP (within 3 hours of ECG )
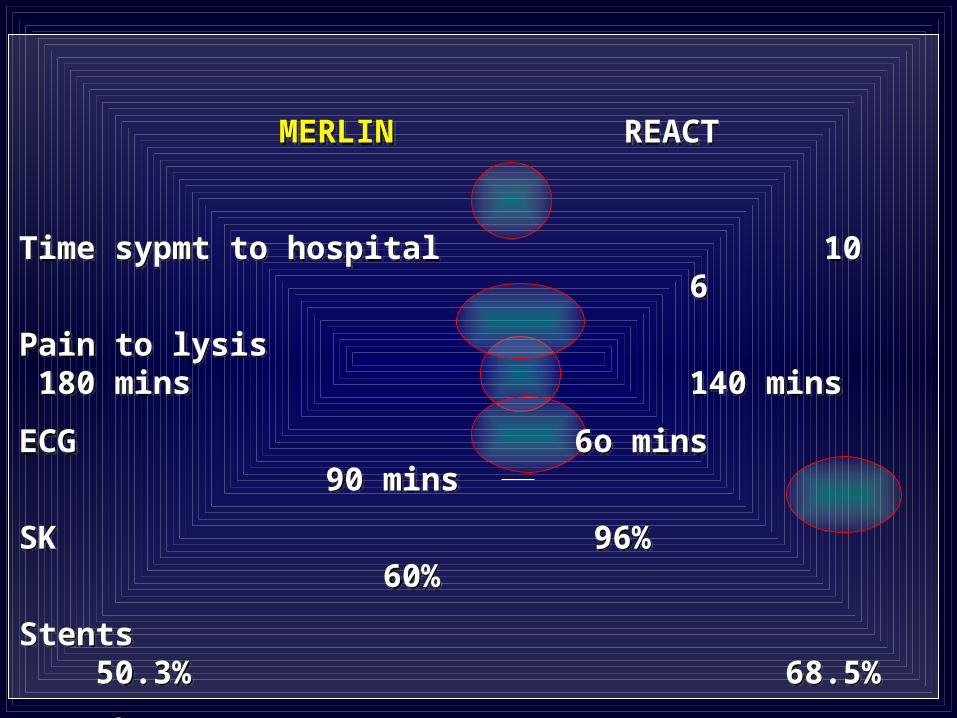
MERLIN REACT
Time sypmt to hospital 10 6
Pain to lysis 180 mins 140 mins
ECG 6o mins 90 mins
SK 96% 60%
Stents 50.3% 68.5%
GP IIbIIIa 3.3% 43.4%
Pain to cath lab 320 mins 420 mins
Local v National
Definitions (HF)
MERLIN REACT
Time sypmt to hospital 10 6
Pain to lysis 180 mins 140 mins
ECG 6o mins 90 mins
SK 96% 60%
Stents 50.3% 68.5%
GP IIbIIIa 3.3% 43.4%
Pain to cath lab 320 mins 420 mins
Local v National
Definitions (HF)

Conservative Rescue p value
(n=154) (n=153)
Death 11.0 9.8 0.7
Re-AMI 10.4 7.2 0.3
Stroke 0.6 4.6 0.03
Heart failure 29.9 24.2 0.3
Re-vasculascularisation 20.1 6.5 < 0.01
COMPOSITE 72 37.3 0.02
MERLIN 30 day JACC 2004,4, 287-96 MERLIN 30 day JACC 2004,4, 287-96
10.6
7.8
2.1
12.1
14.9
47.5
4.9
0.7
1.4
7.6
8.3
22.9
REACT 30 day


Thrombolysis :(+ APT) tested in 100 000 pts
Saves 20-30 lives per thousand
Easy to administer
It is where the patients attend
No extra training
Starting to understand its limitations
Using pharmacology on way to cath lab not appropriate
(ASSENT 4 FINESS)
Thrombolysis :(+ APT) tested in 100 000 pts
Saves 20-30 lives per thousand
Easy to administer
It is where the patients attend
No extra training
Starting to understand its limitations
Using pharmacology on way to cath lab not appropriate
(ASSENT 4 FINESS)
Achieving recommended time lines for P-PCI may be difficult

Schroder R et al. JACC 1995;26:1657-1664

Schroder R et al. JACC 1995;26:1657-1664

Schroder R et al. JACC 1995;26:1657-1664

Admission
Lysis
90 min repeat ECG
Admission
Lysis
90 min repeat ECG
Giving lytic and going to bed is not enough !!!
Primary Strategy

















