Brief Report Joint WHO and Ministry of Public Health Evaluation Mission on Integrated Management for Emergency and Essential Surgical Care (IMEESC) 31 August-5 September 2006 Kabul, Maimana and Mazar-e-Sharif, Afghanistan 1
Transcript
Brief Report
Joint WHO and Ministry of Public Health Evaluation Mission on
Integrated Management for Emergency and Essential Surgical Care (IMEESC)
1. Executive summary The key issues facing the hospitals in Afghanistan are: a relatively low number of hospitals and hospital beds compared to other countries with a comparable level of income; the uneven distribution of hospital facilities and services with large parts of the population unable to access referral facilities. A Joint WHO and Ministry of Public Health (MoPH) evaluation mission was taken to follow-up on the Letter of Intent agreed upon by the WHO, MoPH Afghanistan and Norwegian Deployable Hospital (NDH) for strengthening surgical and anesthesia capacities in Northern Afghanistan. It was agreed by the MoPH and WHO Afghanistan that the health service delivery in Maimana (Faryab Province) and Mazar (Mazar-e Sharif in Balkh province) hospitals should be evaluated by a joint team representing members from the WHO, MoPH and NDH. The meetings resulted in agreement by the MoPH and WHO country office for training through incorporation of a locally adapted WHO Integrated Management for Emergency and Essential Surgical Care (IMEESC) toolkit in the Essential Health Package of Afghanistan for regional and provincial hospitals.
3
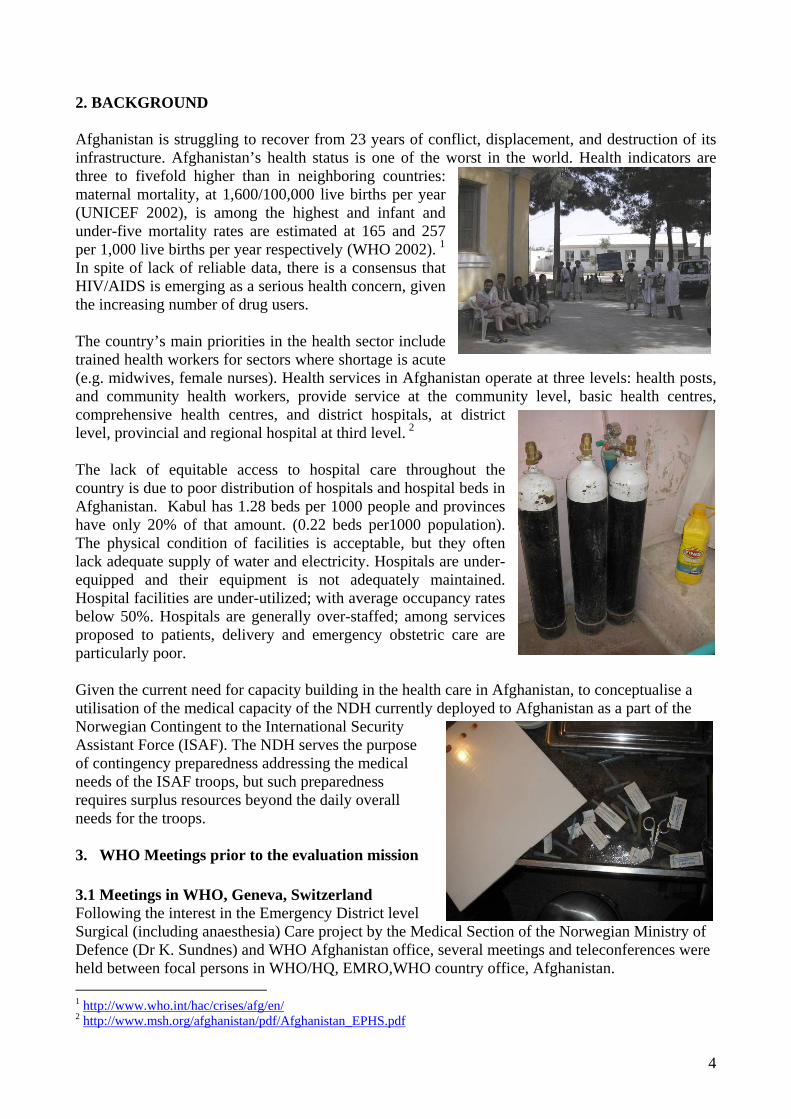
2. BACKGROUND Afghanistan is struggling to recover from 23 years of conflict, displacement, and destruction of its infrastructure. Afghanistan’s health status is one of the worst in the world. Health indicators are three to fivefold higher than in neighboring countries: maternal mortality, at 1,600/100,000 live births per year (UNICEF 2002), is among the highest and infant and under-five mortality rates are estimated at 165 and 257 per 1,000 live births per year respectively (WHO 2002). 1 In spite of lack of reliable data, there is a consensus that HIV/AIDS is emerging as a serious health concern, given the increasing number of drug users. The country’s main priorities in the health sector include trained health workers for sectors where shortage is acute (e.g. midwives, female nurses). Health services in Afghanistan operate at three levels: health posts, and community health workers, provide service at the community level, basic health centres, comprehensive health centres, and district hospitals, at district level, provincial and regional hospital at third level. 2 The lack of equitable access to hospital care throughout the country is due to poor distribution of hospitals and hospital beds in Afghanistan. Kabul has 1.28 beds per 1000 people and provinces have only 20% of that amount. (0.22 beds per1000 population). The physical condition of facilities is acceptable, but they often lack adequate supply of water and electricity. Hospitals are under- equipped and their equipment is not adequately maintained. Hospital facilities are under-utilized; with average occupancy rates below 50%. Hospitals are generally over-staffed; among services proposed to patients, delivery and emergency obstetric care are particularly poor.
Given the current need for capacity building in the health care in Afghanistan, to conceptualise a utilisation of the medical capacity of the NDH currently deployed to Afghanistan as a part of the Norwegian Contingent to the International Security Assistant Force (ISAF). The NDH serves the purpose of contingency preparedness addressing the medical needs of the ISAF troops, but such preparedness requires surplus resources beyond the daily overall needs for the troops. 3. WHO Meetings prior to the evaluation mission 3.1 Meetings in WHO, Geneva, Switzerland Following the interest in the Emergency District level Surgical (including anaesthesia) Care project by the Medical Section of the Norwegian Ministry of Defence (Dr K. Sundnes) and WHO Afghanistan office, several meetings and teleconferences were held between focal persons in WHO/HQ, EMRO,WHO country office, Afghanistan. 1 http://www.who.int/hac/crises/afg/en/2 http://www.msh.org/afghanistan/pdf/Afghanistan_EPHS.pdf
3.2 Meetings in Oslo, Norway In agreement with EHT/CPR, EIP/HDS, HAC departments in WHO/HQ, EMRO, WHO Country Office and MoPH Afghanistan, meetings were held in Oslo, Norway, with the members of the NDH, the Ministry of Defence and the Ministry of Foreign Affaires. The objective of the meeting was to seek agreement on the focus of the project with due attention to sustainability for strengthening capacities in emergency and essential surgical care in northern Afghanistan and expand it to national level. Discussions included:
• Brainstorming on the existing situation of the operation of the public and private health services with regard to access to emergency surgical and anesthesia procedures and equipment in Northern Afghanistan
• Focusing the project to improve equality of surgical care at district level. • Norwegian forces are the main supporter for Provincial Reconstruction Team (PRT) in
Maimana together with some small number of Letvanian military forces. Medical staff of NDH located in Mazar-e-Sharif has the capability to support Mazar provincial hospital in the field of anaesthesia and surgery. Norwegian forces already donated one machine of anaesthesia to Maimana hospital and trained 3 staff of the hospital in anaesthesia.
• Adaptation and distribution of the WHO manual "Surgical Care at the District Hospital" for the whole country.
• Provision of some equipment (surgery and anaesthetics) in Northern Afghanistan. • Practical demonstration of relevant equipment
(anesthesia and surgery) at the War Surgery Training Center in Oslo, Norway
• Training programme to be developed and applied, based on existing collaborations between the Norwegian Army Medical Services (Surgical) and provincial hospitals in Northern Afghanistan (Mazar-e-sharif and Maimana) ready for nationwide implementation.
• Pragmatic and opportunistic engagement of the Norwegian military medical services with local health authorities in Afghanistan.
• Drafting of a project document • Editing the draft of the Memorandum of
Understanding. 4. Objectives of the evaluation mission
• To evaluate health service delivery in Maimana and Mazar-e-Sharif and Kabul hospitals
• To introduce WHO IMEESC toolkit towards building
5
and strengthening capacities in basic emergency and essential surgical skills training with an integrated approach at resource-limited health care facilities in Afghanistan
5. Field visits to the Teaching, Tertiary, Provincial and Regional Hospitals Visits were made to the teaching (Indira Gandhi Institute of Child Health, Kabul, Maimana provincial hospital and Mazar-e-Sharif regional hospitals for a situation analysis of provision of life saving emergency surgical and anaesthesia procedures and equipment. 5.1 Situation analysis at Maimana hospital • The hospital staff (surgeons and anaesthetists) were
satisfied with the collaboration and support provided by Norwegian medical team.
• The anaesthesia machine donated by Norwegian government was in good functional conditions. The donated anaesthesia machine functions even when the electrical power goes off, meets the needs of the current situation in Afghanistan.
• The Norwegian military medical team has trained 3 staff of Maimana hospital in anaesthesia.
• For the sustainability of the anaesthesia machines the Norwegian medical team agreed to train the hospital staff to fix and repair some minor technical problems of the machine. Meanwhile they are providing some spare parts of the machine to the hospital.
• Norwegian medical team have protection by their military forces when moving around the hospital premises.
• Turkish International Cooperation Agency (TIKA) is supporting the hospital on regular basis in terms of provision of medicine, medical equipments and incentive salaries for the hospital staff.
• The situation in emergency room and operation theatre of obstetrics and gynaecology was not satisfactory and needs improvement.
• The Provincial Public Health Director (PHD) was appointed recently and started his job one day before the visit of the evaluation mission, which provided an opportunity to have a detailed evaluation of the health facility
5.2 Situation analysis at Balkh/Mazar provincial hospital • Mazar Hospital although a provincial hospital is working as the main regional hospital in the
north including referred cases from other provinces of the region. • This hospital serves as academic and research centre
in affiliation with Mazar Medical College. • A medical team of Indian doctors (supported by the
India Ministry of Foreign Affaires) are working with Afghan doctors in surgical care and anaesthesia since last 3.5 years. The Indian medical team were expected to train Afghan doctors, but partly due to language constraints they were unable to go beyond the provision of services.
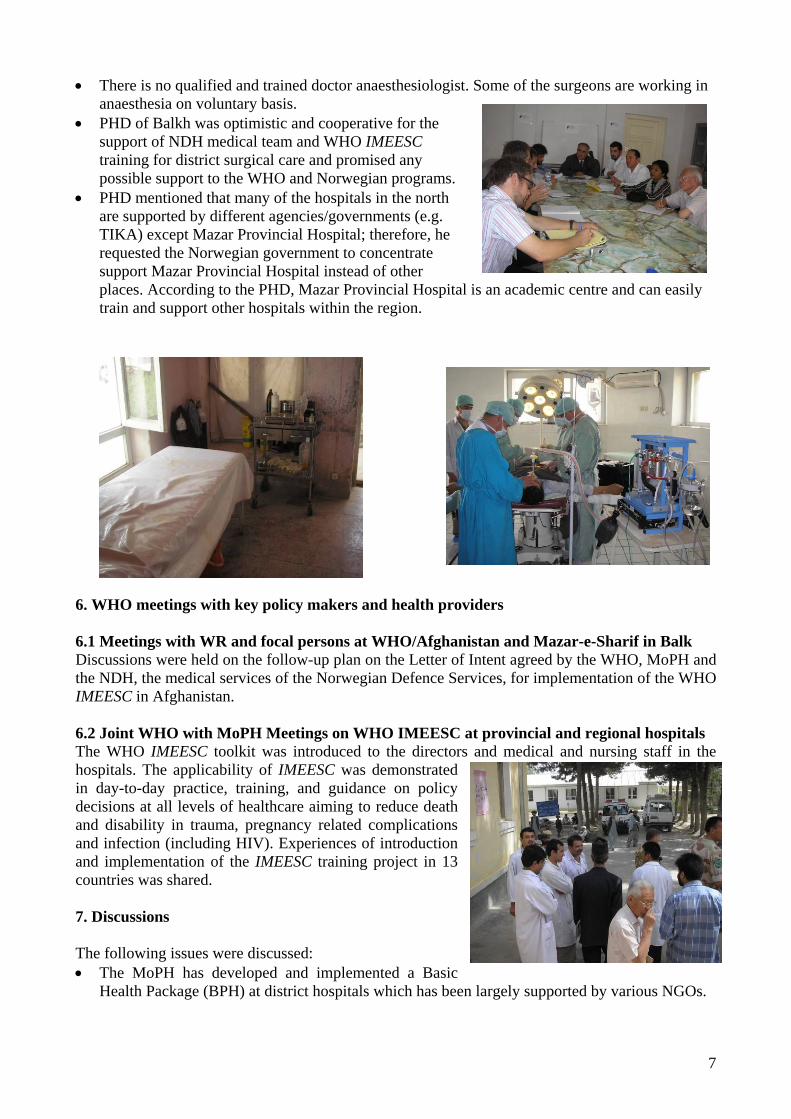
• There were different types of anaesthesia machines in various operation theatres of the Mazar Provincial Hospital and in one of the operation theatre there was no suction machine.
6
• There is no qualified and trained doctor anaesthesiologist. Some of the surgeons are working in anaesthesia on voluntary basis.
• PHD of Balkh was optimistic and cooperative for the support of NDH medical team and WHO IMEESC training for district surgical care and promised any possible support to the WHO and Norwegian programs.
• PHD mentioned that many of the hospitals in the north are supported by different agencies/governments (e.g. TIKA) except Mazar Provincial Hospital; therefore, he requested the Norwegian government to concentrate support Mazar Provincial Hospital instead of other places. According to the PHD, Mazar Provincial Hospital is an academic centre and can easily train and support other hospitals within the region.
6. WHO meetings with key policy makers and health providers
6.1 Meetings with WR and focal persons at WHO/Afghanistan and Mazar-e-Sharif in Balk Discussions were held on the follow-up plan on the Letter of Intent agreed by the WHO, MoPH and the NDH, the medical services of the Norwegian Defence Services, for implementation of the WHO IMEESC in Afghanistan.
6.2 Joint WHO with MoPH Meetings on WHO IMEESC at provincial and regional hospitals The WHO IMEESC toolkit was introduced to the directors and medical and nursing staff in the hospitals. The applicability of IMEESC was demonstrated in day-to-day practice, training, and guidance on policy decisions at all levels of healthcare aiming to reduce death and disability in trauma, pregnancy related complications and infection (including HIV). Experiences of introduction and implementation of the IMEESC training project in 13 countries was shared. 7. Discussions The following issues were discussed: • The MoPH has developed and implemented a Basic
Health Package (BPH) at district hospitals which has been largely supported by various NGOs.
7
• The MoPH, supported by various NGOs, has also developed an Essential Package of hospital services which will be implemented at the tertiary, provincial and regional health facilities. Incorporation of the WHO IMEESC in both the BPH and Essential Package of hospital services will add value towards strengthening anesthesia services at regional and provincial hospitals, in parallel with surgical training programs.
• Action plan to strengthen anesthesia and surgical services in Northern Afghanistan in the Letter of Intent.
• There is an urgent need for strengthening emergency surgical and anesthesia interventions (procedures and equipment) to reduce death and disability in pregnancy related complications and trauma
• Collaborations with international and local partners to support local adaptation, equipment and training in emergency surgical and anesthesia skills in identified health facilities by the MoPH and WHO Country Office.
• The WHO manual Surgical Care at the District Hospital and the WHO IMEESC training toolkit could be incorporated towards a standard training curriculum of the medical and nursing training programs
• Local translation of the WHO IMEESC toolkit into Farsi and Pushto for strengthening capacities at provincial and regional health facilities.
• WHO IMEESC tools will add value to the Provincial Reconstruction Reform developed by the MoPH
• Provincial Public Health Director (Maimana) emphasized on increasing support to the hospital instead of only donating one anaesthesia machine or training their staff in anaesthesia.
• Medical doctors/surgeons have their own responsibilities and they can not give anaesthesia for the patients operated by other doctors. To guarantee the sustainability of anaesthesia we should identify and train anaesthetists according to the MoPH organigram.
8. Recommendations and Action Plan • Incorporation of WHO IMEESC within the essential package of hospital services for
Afghanistan towards standardized training in emergency and essential surgical and anesthesia procedures with linked equipment at regional and provincial hospitals
• Local translation into Farsi and Pushto, production and dissemination of the WHO IMEESC toolkit by the WHO and MoPH.
• Strengthening anesthesia services for identified regional and provincial hospitals with the provision of surgical training programs by the Norwegian partners
• Coordinate for a Training of Trainers workshop with locally adapted IMEESC tool for Afghanistan
• MoPH will follow-up on the policy issue for strengthening emergency surgical and anesthesia services and prevention of infection towards both patient and health personnel safety
8
• Since surgical care and anaesthesia does not have standardized guidelines like other public health programs, the idea of translation/adaptation of the WHO district surgical care guidelines have been welcomed by the PHDs of Maimana and Balkh.
• The Norwegian team will continue their support in Maimana and provide one more anaesthesia machine to Maimana hospital to be used in operation theatre and another anaesthesia machine to Mazar Provincial Hospital.
9. Conclusions There was a consensus for a local adaptation of the WHO IMEESC tool, production, dissemination and training of trainers, towards strengthening capacities at rural health facilities in emergency and essential surgical and anesthesia procedures with linked equipment. There is an urgent need to support anesthesia training at regional and provincial hospitals to improve the quality of surgical and obstetrical procedures. Acknowledgements were made for the Norwegians and WHO support and WHO recommended its expansion to the other parts of the region.
Members of the Joint WHO and Ministry of Public Health Evaluation Mission:
• Dr Riyad M. F. Musa Ahmad, WR, Afghanistan • Dr. Haseeb Niayesh, MoPH Afghanistan • Dr Asadullah Taqdeer WHO Afghanistan • Dr Gafhari Ahmed, WHO, Mazar-e-Sharif • Dr. Meena Cherian, WHO Geneva • Mr Baard Vandvik, Political /Development adviser,
Norwegian PRT Maimana • Mr Rune Jacobsen, Norwegian Contingent Command • Dr Knut O Sundnes, Norvegian military forces • Mr Andreas Loevold, Second secretary, Royal
Norwegian embassy in Kabul
10. Acknowledgements
• Afghan Ministry of Public Health • World Health Organization WHO HQ, Country office, Sub-office Mazar-e-Sharif • Norwegian Ministry of Defence • Norwegian Embassy • Norwegian Deployable Hospitals (NDH) • TIKA-Turkish International Cooperation Agency
9
Annexe 1. Participants of the Meetings Dr. Haseeb Niayesh, MoPH Afghanistan
Ms Elizabeth Benedetti, Senior External relation Officer Mine action centre for Afghanistan, United Nations Ms Mary L Vitelli Senior energy advisor Ministry of Mines and Industries Afghanistan Mr Espen Barth Eide, Deputy Minister of Defence Head of the Medical Section,Norway Mr. Shivaji R Salunke USAID, Afghanistan Mr. Andreas Loevold Second Secretary, Political Affairs Royal Norwegian embassy in Kabul Afghanistan Dr. Abdi M. Ahmed, Medical officer, WHO Country office Afghanistan Mr Torbjørn Urfjell Ministry of Foreign Affaires Political Adviser for Minister for Development Cooperation., Norway Major General Harald Sunde Head of Military Section Ministry of Defence, Norway Dr. Knut O Sundnes Head of Anaesthesia Norwegian Defence Forces, Norway Lt. Col. Olsson, Incoming Commander Norwegian Deployable Hospital. Afghanistan Dr. Mirwais Rabi Balkh Provincial Public Health Director Mazar-Sharif Public Hospital Afghanistan Mr Jan Arne Flølo, MFA, Adviser, Humanitarian Section, Norway Ms Anja Paajanen Development Adviser Meymaneh provincial Reconstruction Team
Faryab Province, Afghanistan Lt. Col. Geir Anders Fagerheim, Legal adviser, Norway Mr Kim Traavik, Norwegian Ambassador to NATO delegation Brussels Mr Baard Vandvik, Political /Development advisor, Norwegian PRT, Maimana Afghanistan Mr Rune Jacobsen, Norwegian Contingent Command Norway WHO Dr Riyad M.F. Musa Al Ahmad, WR Afghanistan WHO/ Kabul, Afghanistán Dr Ghaffary Mir AhmadWHO/ Mazar-e-Sharif, Afghanistán Dr Asadullah Taqdeer Technical officer, WHO/Kabul, Afghanistan. Dr Momin Abdi Ahmed WHO/Kabul, Afghanistan. Dr N. Metwalli, Regional Advisor WHO/EMRO/Cairo, Egypt Dr Meena Nathan Cherian Project: Emergency & Essential Surgical Care Clinical Procedures Unit (CPR) Department of Essential Health Technologies WHO HQ, Geneva, Switzerland tel:0041 22 791 4011; fax: 0041 22 791 4836 [email protected], www.who.int/surgery Dr A.D. Alwan, Representative of Director-General for Health Action in Crises WHO HQ, Geneva, Switzerland Dr D.Lopez Acuna DIR/HAC WHO HQ, Geneva, Switzerland Dr O.F. Nielsen, Public Health Officer, HDS/EIP WHO HQ, Geneva, Switzerland
10
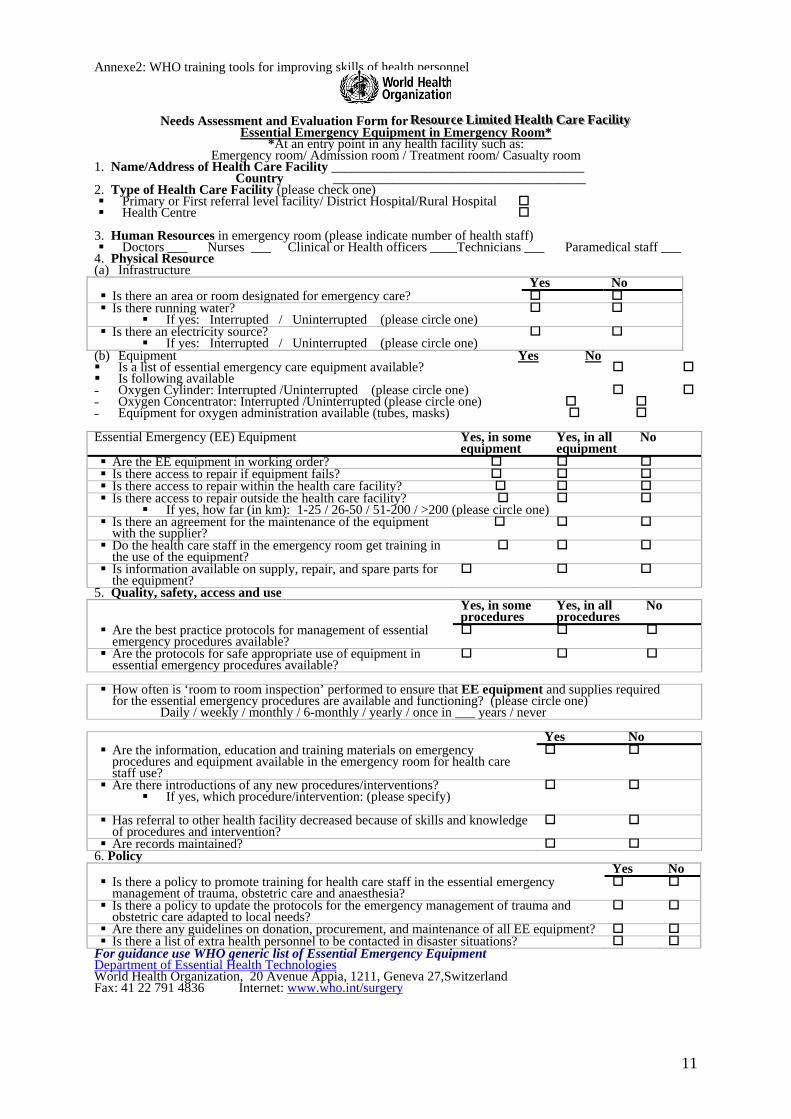
Annexe2: WHO training tools for improving skills of health personnel
Needs Assessment and Evaluation Form for RRReeesssooouuurrrccceee LLLiiimmmiiittteeeddd HHHeeeaaalll ttthhh C CCaaarrreee FFFaaaccciii lll iii tttyyy Essential Emergency Equipment in Emergency Room*
*At an entry point in any health facility such as: Emergency room/ Admission room / Treatment room/ Casualty room
1. Name/Address of Health Care Facility ______________________________________ Country ______________________________________ 2. Type of Health Care Facility (please check one)
Primary or First referral level facility/ District Hospital/Rural Hospital Health Centre
3. Human Resources in emergency room (please indicate number of health staff)
Doctors ___ Nurses ___ Clinical or Health officers ____Technicians ___ Paramedical staff ___ 4. Physical Resource (a) Infrastructure Yes No
Is there an area or room designated for emergency care? Is there running water?
If yes: Interrupted / Uninterrupted (please circle one) Is there an electricity source?
If yes: Interrupted / Uninterrupted (please circle one) (b) Equipment Yes No Is a list of essential emergency care equipment available? Is following available - Oxygen Cylinder: Interrupted /Uninterrupted (please circle one) - Oxygen Concentrator: Interrupted /Uninterrupted (please circle one) - Equipment for oxygen administration available (tubes, masks) Essential Emergency (EE) Equipment Yes, in some
equipment Yes, in all equipment
No
Are the EE equipment in working order? Is there access to repair if equipment fails? Is there access to repair within the health care facility? Is there access to repair outside the health care facility?
If yes, how far (in km): 1-25 / 26-50 / 51-200 / >200 (please circle one) Is there an agreement for the maintenance of the equipment with the supplier?
Do the health care staff in the emergency room get training in the use of the equipment?
Is information available on supply, repair, and spare parts for the equipment?
5. Quality, safety, access and use Yes, in some
procedures Yes, in all procedures
No
Are the best practice protocols for management of essential emergency procedures available?
Are the protocols for safe appropriate use of equipment in essential emergency procedures available?
How often is ‘room to room inspection’ performed to ensure that EE equipment and supplies required for the essential emergency procedures are available and functioning? (please circle one)
Daily / weekly / monthly / 6-monthly / yearly / once in ___ years / never
Yes No
Are the information, education and training materials on emergency procedures and equipment available in the emergency room for health care staff use?
Are there introductions of any new procedures/interventions? If yes, which procedure/intervention: (please specify)
Has referral to other health facility decreased because of skills and knowledge of procedures and intervention?
Are records maintained? 6. Policy Yes No
Is there a policy to promote training for health care staff in the essential emergency management of trauma, obstetric care and anaesthesia?
Is there a policy to update the protocols for the emergency management of trauma and obstetric care adapted to local needs?
Are there any guidelines on donation, procurement, and maintenance of all EE equipment? Is there a list of extra health personnel to be contacted in disaster situations?
For guidance use WHO generic list of Essential Emergency Equipment Department of Essential Health TechnologiesWorld Health Organization, 20 Avenue Appia, 1211, Geneva 27,Switzerland Fax: 41 22 791 4836 Internet: www.who.int/surgery
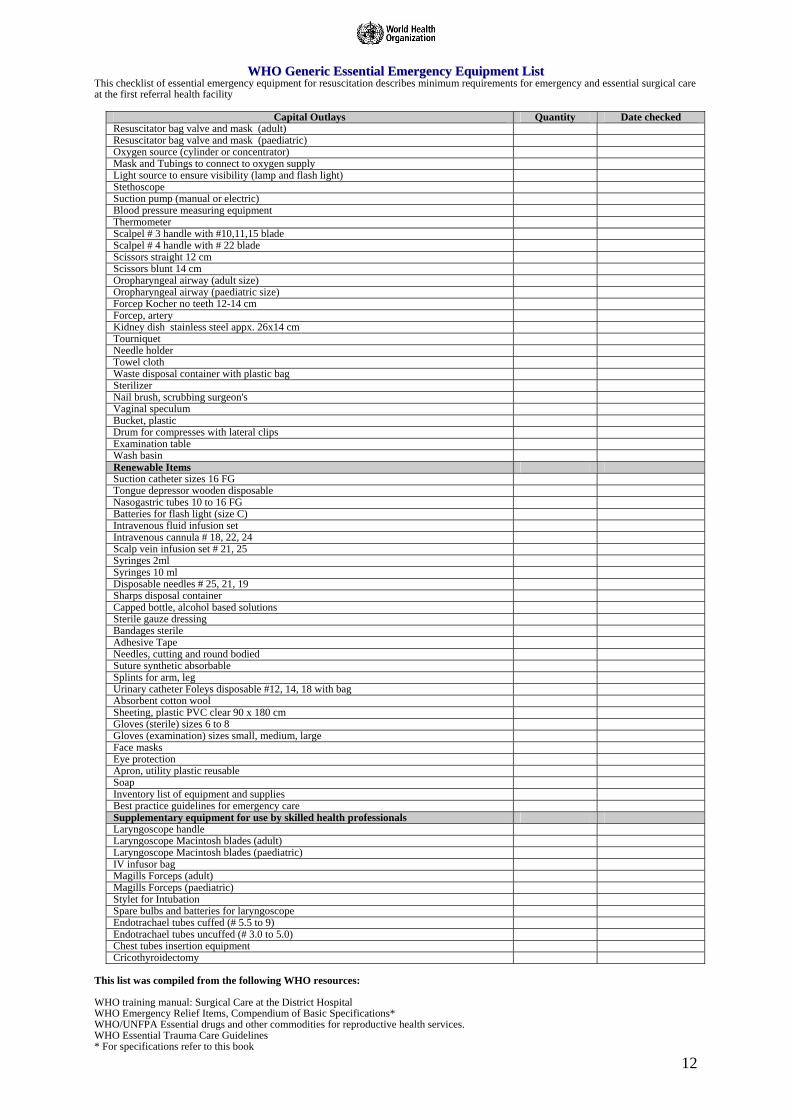
WWHHOO GGeenneerriicc EEsssseennttiiaall EEmmeerrggeennccyy EEqquuiippmmeenntt LLiisstt This checklist of essential emergency equipment for resuscitation describes minimum requirements for emergency and essential surgical care at the first referral health facility
Capital Outlays Quantity Date checked Resuscitator bag valve and mask (adult) Resuscitator bag valve and mask (paediatric) Oxygen source (cylinder or concentrator) Mask and Tubings to connect to oxygen supply Light source to ensure visibility (lamp and flash light) Stethoscope Suction pump (manual or electric) Blood pressure measuring equipment Thermometer Scalpel # 3 handle with #10,11,15 blade Scalpel # 4 handle with # 22 blade Scissors straight 12 cm Scissors blunt 14 cm Oropharyngeal airway (adult size) Oropharyngeal airway (paediatric size) Forcep Kocher no teeth 12-14 cm Forcep, artery Kidney dish stainless steel appx. 26x14 cm Tourniquet Needle holder Towel cloth Waste disposal container with plastic bag Sterilizer Nail brush, scrubbing surgeon's Vaginal speculum Bucket, plastic Drum for compresses with lateral clips Examination table Wash basin Renewable Items Suction catheter sizes 16 FG Tongue depressor wooden disposable Nasogastric tubes 10 to 16 FG Batteries for flash light (size C) Intravenous fluid infusion set Intravenous cannula # 18, 22, 24 Scalp vein infusion set # 21, 25 Syringes 2ml Syringes 10 ml Disposable needles # 25, 21, 19 Sharps disposal container Capped bottle, alcohol based solutions Sterile gauze dressing Bandages sterile Adhesive Tape Needles, cutting and round bodied Suture synthetic absorbable Splints for arm, leg Urinary catheter Foleys disposable #12, 14, 18 with bag Absorbent cotton wool Sheeting, plastic PVC clear 90 x 180 cm Gloves (sterile) sizes 6 to 8 Gloves (examination) sizes small, medium, large Face masks Eye protection Apron, utility plastic reusable Soap Inventory list of equipment and supplies Best practice guidelines for emergency care Supplementary equipment for use by skilled health professionals Laryngoscope handle Laryngoscope Macintosh blades (adult) Laryngoscope Macintosh blades (paediatric) IV infusor bag Magills Forceps (adult) Magills Forceps (paediatric) Stylet for Intubation Spare bulbs and batteries for laryngoscope Endotrachael tubes cuffed (# 5.5 to 9) Endotrachael tubes uncuffed (# 3.0 to 5.0) Chest tubes insertion equipment Cricothyroidectomy
This list was compiled from the following WHO resources: WHO training manual: Surgical Care at the District Hospital WHO Emergency Relief Items, Compendium of Basic Specifications* WHO/UNFPA Essential drugs and other commodities for reproductive health services. WHO Essential Trauma Care Guidelines * For specifications refer to this book