236
A Matter of Urgency: Including Children with Special Needs in Child Care in Canada

A Matter ofUrgency:
Including Childrenwith Special Needsin Child Care in Canada


Sharon Hope IrwinSpeciaLink:
The National Centrefor Child Care Inclusion
A Matter ofUrgency:
Including Childrenwith Special Needsin Child Care in Canada
Breton Books
Donna S. LeroDepartment of Family Relations
and Applied NutritionUniversity of Guelph
Kathleen BrophyDepartment of Family Relations
and Applied NutritionUniversity of Guelph

ACKNOWLEDGEMENTS
For their sponsorship and belief in the importance of the research on childcare staff attitudes toward including children with special needs, our thanksto our primary sponsor, Child Care Visions, Social Development Partner-ships Program, Human Resources Development Canada and our project of-ficers, Penny Hammell and Carol Levesque.
Our thanks to the 283 centre directors, early childhood educators, in-houseresource teachers, travelling resource teachers and resource consultants whotook the time to answer our survey questions and to add their insightfulcomments.
Our thanks to Laura Coulman, M.Sc. and to Leo Keating at the University ofGuelph for their assistance with data coding and statistical analysis, and tothe You Bet I Care! principal investigators for sharing data from their repre-sentative sample of Canadian child care centres.
Our thanks to the staff at SpeciaLink, including Natalie White and GailHoldner, office coordinators; Glenda Watt, research assistant; and LisaDorcich, librarian. Our thanks to the staff at Breton Books, especially RonaldCaplan and Bonnie Thompson, for their commitment to this book. Our thanksto James Fader, ArtPlus, for his technological skills and for his untiring in-terest and enthusiasm for the task.
Our thanks to the staff, parents, and children of Town Daycare Centre, inGlace Bay, Cape Breton, Nova Scotia, for their interest in participating in thephoto session that yielded the cover pictures. Our thanks also to OwenFitzgerald, photographer, for taking the cover pictures.
ACKNOWLEDGEMENTS v

TABLE OF CONTENTS vii
TABLE OF CONTENTS
ACKNOWLEDGEMENTS ......................................................................................... V
OVERVIEW ....................................................................................................... XIII
CHAPTER 1 INTRODUCTION AND BACKGROUND ........................................................ 1Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy
1.1 Introduction ................................................................................................................................... 11.2 Background ................................................................................................................................... 31.3 Defining “Inclusion” ..................................................................................................................... 41.4 Our Theoretical Model: The Ecology of Inclusive Child Care ................................................... 61.5 Goals and Objectives of the Present Study ............................................................................... 81.6 Unique Characteristics of This Research Study ........................................................................ 91.7 A “Matter of Language” .............................................................................................................. 101.8 Defining “Children With Special Needs” for the Current Study ............................................. 11
CHAPTER 2 CURRENT UNDERSTANDINGS .............................................................. 13Sharon Hope Irwin, Donna S. Lero, Kathleen Brophy
2.1 The Prevalence of Special Needs and Chronic Health Conditions in Canadian Children ... 132.2 Inclusive Child Care: Opportunities to Support Child Development and Family Well-Being142.3 The Evolution of Inclusive Child Care in Canada .................................................................... 202.4 Appreciating the Context in Which the Study was Conceptualized and Undertaken,
and in which this Report is Being Disseminated ..................................................................... 252.5 The Evolution of Quality Care as a Concept That Encompasses Inclusiveness and
Diversity — Using Assessment Tools as a Benchmark .......................................................... 262.6 The Current Status of Inclusion in Canadian Child Care Programs ...................................... 292.7 Remaining Barriers; Ongoing Challenges ................................................................................ 31
CHAPTER 3 LITERATURE REVIEW: THE ROLES OF STAFF ATTITUDE, EXPERIENCE, ANDTRAINING IN EFFECTIVE INCLUSION IN CHILD CARE ............................................... 35Sharon Hope Irwin, Kathleen Brophy, Donna S. Lero
3.1 Historical Overview of the Literature on Child Care Inclusion .............................................. 353.2 Organization of the Literature Review ...................................................................................... 383.3 The Roles of Staff Attitude, Experience, and Training in Effective Inclusion in Child Care 37
3.31 Nature of the Child’s Special Needs .............................................................................. 373.32 Staff Training ................................................................................................................... 383.33 Experience in Working With Children With Special Needs ......................................... 423.34 Confidence of the Staff ................................................................................................... 433.35 Availability of Resources ............................................................................................... 443.36 Parental Attitudes and Collaboration With Parents ..................................................... 443.37 The Leadership Approach Taken by Early Childhood Program Directors ................ 46
CHAPTER 4 METHODOLOGY ............................................................................... 55Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy
4.1 Introduction ................................................................................................................................. 554.2 Issues That Affected our Sampling Approach ......................................................................... 55

4.3 Sample Selection and Augmentation ........................................................................................ 574.4 Our Obtained Samples ............................................................................................................... 584.5 Questionnaire Development and Descriptions ........................................................................ 60
4.51 The Questionnaire for Directors .................................................................................... 604.52 The Questionnaire for ECEs and In-House RTs ........................................................... 614.53 The Questionnaire for Travelling RTs and RCs............................................................ 62
4.6 Pretesting .................................................................................................................................... 634.7 Data Collection Procedures ....................................................................................................... 634.8 Preparation for Data Analysis .................................................................................................... 64
CHAPTER 5 DESCRIPTIVE INFORMATION ABOUT THE CENTRES, STAFF ANDDIRECTORS IN OUR SAMPLE .............................................................................. 65Donna S. Lero, Kathleen Brophy, Sharon Hope Irwin
5.1 Introduction ................................................................................................................................. 655.2 Our Child Care Centres .............................................................................................................. 65
5.21 Location ........................................................................................................................... 655.22 Centre Type ..................................................................................................................... 655.23 Centre Size, Full/Part Day Programs, Age of Children Served, and Auspice ............ 675.24 A Glimpse of Child Care Inclusion ................................................................................ 675.25 How Our Centres Compare to Available National Profiles .......................................... 68
5.3 Our Sample of Front-Line Child Care Professionals ............................................................... 695.31 ECEs and In-House Resource Teachers ....................................................................... 695.32 Front-Line Professionals’ Experience in Child Care ................................................... 705.33 Front-Line Professionals’ Experience With Children with Special Needs ................. 705.34 Front-Line Professionals’ Educational Background ................................................... 705.35 How Our Front-Line Professionals Compare to Available National Profiles ............. 71
5.4 Our Sample of Directors ............................................................................................................. 715.41 The Roles of Centre Directors ....................................................................................... 725.42 Directors’ Experience in the Child Care Field .............................................................. 725.43 Directors’ Experience With Children With Special Needs ........................................... 725.44 Directors’ Educational Background .............................................................................. 735.45 How Our Directors Compare to a National Profile ....................................................... 73
5.5 Summing Up ................................................................................................................................ 74
CHAPTER 6 THE NATURE AND EXTENT OF INCLUSION — CENTRE PRACTICES ............ 75Donna S. Lero, Sharon Hope Irwin. Kathleen Brophy
6.1 Introduction ................................................................................................................................. 756.2 Including Children With Special Needs: Children in Child Care Programs........................... 75
6.21 The Number of Children With Special Needs Included in Child Care Programs ...... 766.22 The Nature and Severity of Children’s Conditions Among Children Enrolled .......... 776.23 Is Participation Limited to Part-Time Attendance? ...................................................... 78
6.3 To What Extent are Children With Special Needs not Accommodated in Child Care Programs? 796.4 Centre Practices Related to Inclusion ...................................................................................... 81
6.41 Program Planning ........................................................................................................... 816.42 Communication With Parents ........................................................................................ 826.43 Degree of Parents’ Involvement .................................................................................... 826.44 Coordinating Services for Children With Special Needs in the Centre ..................... 83
6.5 The Resources Available to Centres to Support Inclusive Child Care .................................. 836.51 Additional On-Site Staff .................................................................................................. 846.52 Itinerant Staff and Resource Consultants .................................................................... 856.53 The Availability of Both On-Site and Travelling Consultants ..................................... 856.54 The Availability of Other Professionals ........................................................................ 85
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canadaviii
6.55 Support From Parents .................................................................................................... 856.6 Summing Up ................................................................................................................................ 85
CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF ............................. 87Kathleen Brophy, Donna S. Lero, Sharon Hope Irwin
7.1 Introduction ................................................................................................................................. 877.2 Staff Characteristics ................................................................................................................... 88
7.21 Specific Roles of Front-Line Staff ................................................................................. 887.22 Education and Training .................................................................................................. 897.23 Experience in the Child Care Field ................................................................................ 91
7.3 Staff’s Attitudes and Beliefs About Inclusion .......................................................................... 917.31 Staff’s Attitudes Toward Inclusion ................................................................................ 917.32 Staff’s Beliefs About Inclusion ...................................................................................... 94
7.4 Staff’s Experiences in Providing Inclusive Child Care ............................................................ 967.41 Children Who Were Successfully Included .................................................................. 977.42 Areas In Which Child Care Staff Were Most Successful ............................................. 987.43 Resources That Enabled Staff to Be Successful ......................................................... 997.44 Sources of Frustration ................................................................................................. 1007.45 Resources That Would Have Helped........................................................................... 1017.46 Less Successful Experiences ...................................................................................... 103
7.5 Personal Change in Staff’s Values and Feelings ................................................................... 1057.6 Changes in Centres that Impact on Inclusion ........................................................................ 1087.7 Staff’s Confidence in Themselves as Agents of Inclusion ................................................... 1097.8 Future Training Needs to Support Inclusion .......................................................................... 1107.9 Relationships Between Education, Attitudes and Experience ............................................. 1127.10 Summing Up .............................................................................................................................. 114
CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS ........................... 119Donna S. Lero, Kathleen Brophy, Sharon Hope Irwin
8.1 Introduction ............................................................................................................................... 1198.2 Directors’ Education and Experience: A Foundation for Effective Inclusion ...................... 120
8.21 Continued Learning: Courses and Conferences ....................................................... 1218.22 Providing Workshops to Others .................................................................................. 1218.23 Directors’ Interests in Additional Training and Information ..................................... 121
8.3 Directors’ Involvement in Program Planning, Communicating With Parents, andCoordinating Resources .......................................................................................................... 121
8.4 Directors’ Attitudes and Beliefs About Inclusion ................................................................... 1238.41 Directors’ Current Attitudes Towards Including Children With Special Needs inRegular Preschool and Child Care Programs ....................................................................... 1248.42 Differing Perspectives Among Directors .................................................................... 1258.43 Have Directors’ Attitudes Changed? ........................................................................... 1258.44 Directors’ Beliefs About Inclusion .............................................................................. 126
8.5 Personal Change in Directors’ Values and Feelings ............................................................. 1298.51 Commitment to Inclusion ............................................................................................. 1318.52 Accepting of a Broader Range of Children With Special Needs or More Cautious 1328.53 More Comfortable With Children With Special Needs ............................................... 133
8.6 Directors’ Views of Their Centre’s Effectiveness in Integrating Children With Special Needs 1338.61 Markers/Validators of Directors’ Views of Their Centre as More Inclusive or
More Effective ................................................................................................................ 1348.62 Perceived Enablers of Effective Inclusion .................................................................. 1358.63 Factors that Limit or Frustrate Effective Inclusion .................................................... 137
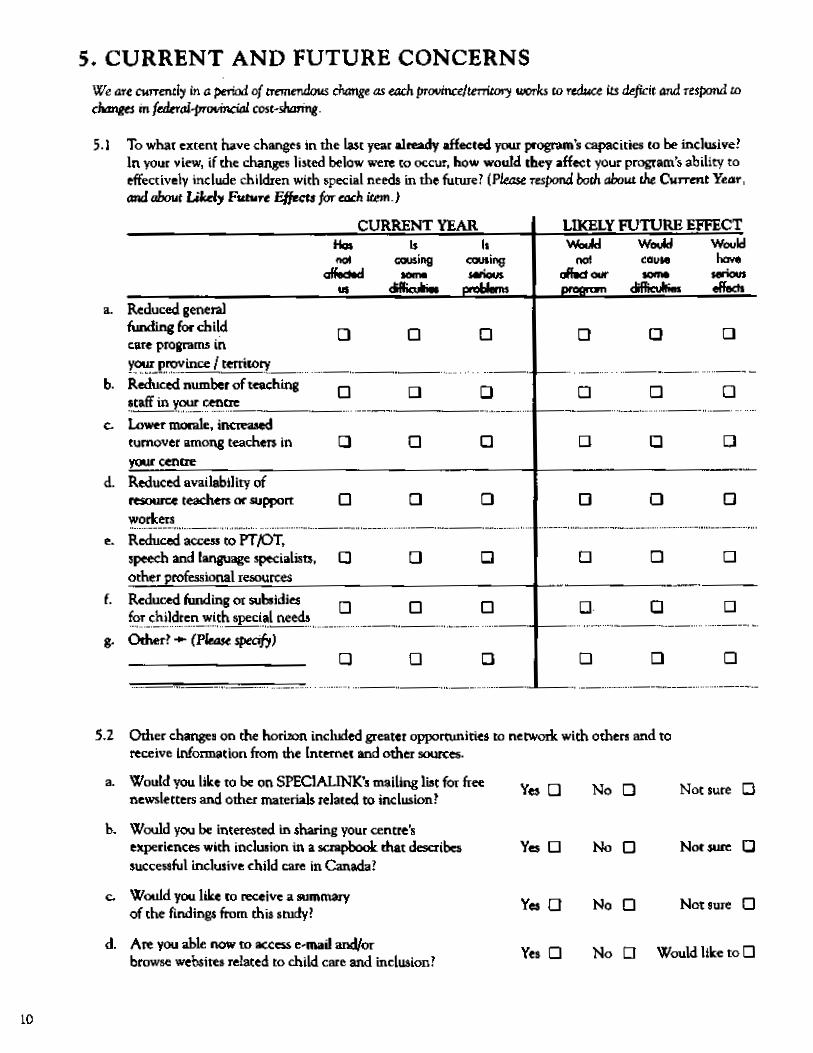
8.7 Current and Future Concerns About Inclusion: The Perceived Impacts of Fiscal Restraint 138
TABLE OF CONTENTS ix

8.8 Summing Up .............................................................................................................................. 140
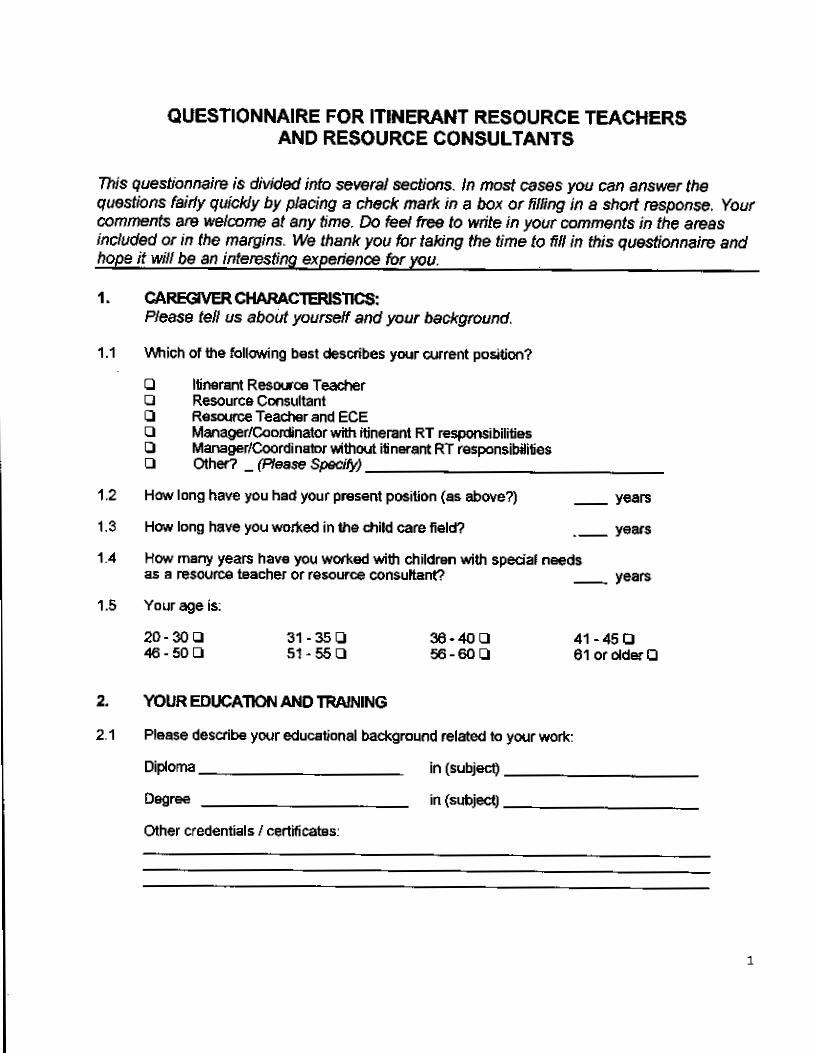
CHAPTER 9 AN EXTERNAL WINDOW: THE VIEWS OF TRAVELLING RESOURCETEACHERS AND RESOURCE CONSULTANTS .......................................................... 143Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy
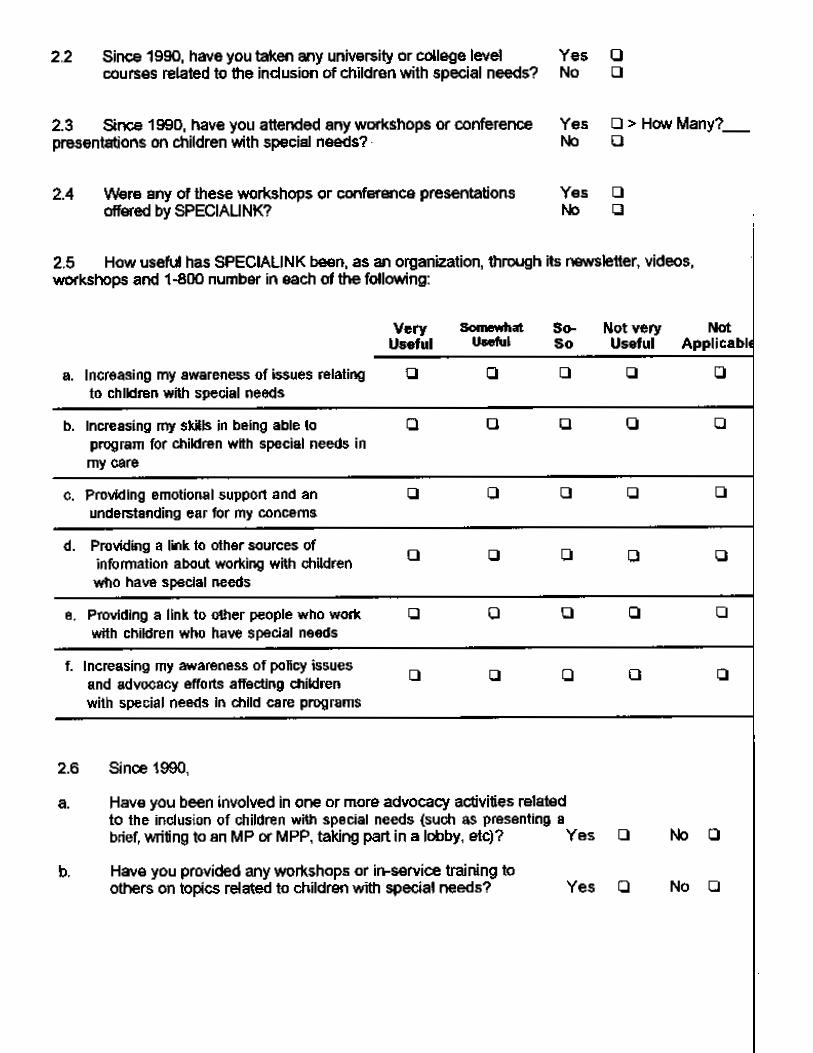
9.1 Introduction ............................................................................................................................... 1439.2 Experience, Education and Training of Travelling Resource Teachers/Resource
Consultants ............................................................................................................................... 1449.21 Experience ..................................................................................................................... 1449.22 Education and Training ................................................................................................ 144
9.3 Roles and Responsibilities of Travelling Resource Teachers/Resource Consultants ....... 1469.4 Views of Resource Teachers/Resource Consultants of Factors That Differentiate
Centres That are Extremely Effective From Those Struggling With Inclusion ................... 1479.5 Summing Up .............................................................................................................................. 150
CHAPTER 10 INTEGRATING WHAT WE HAVE LEARNED ......................................... 153Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy
10.1 Introduction ............................................................................................................................... 15310.2 Necessary Ingredients for Successful Inclusion ................................................................... 15410.3 Specific Findings From Our Research .................................................................................... 156
10.31 Positive Attitudes Toward Inclusion and Staff’s Education and Training ............... 15610.32 Supports Within Child Care Programs ....................................................................... 15810.33 The Role of Program Directors as Leaders ................................................................ 160
10.4 The Effects of Experiences With Inclusion ............................................................................ 16210.5 Conclusions .............................................................................................................................. 164
10.51 Revisiting Our Definition of, and Expectations for, Inclusive Child Care ................ 16410.52 The Relationship Between Effective Inclusion and High Quality Child Care .......... 165
CHAPTER 11 RECOMMENDATIONS ..................................................................... 167Sharon Hope Irwin, Donna S. Lero, Kathleen Brophy
11.1 Introduction ............................................................................................................................... 16711.2 Recommendations .................................................................................................................... 168
11.21 A Focus on Legislation, Policy Development and Funding ...................................... 16811.22 A Focus on Capacity-Building ..................................................................................... 169
REFERENCES ................................................................................................................................... 175
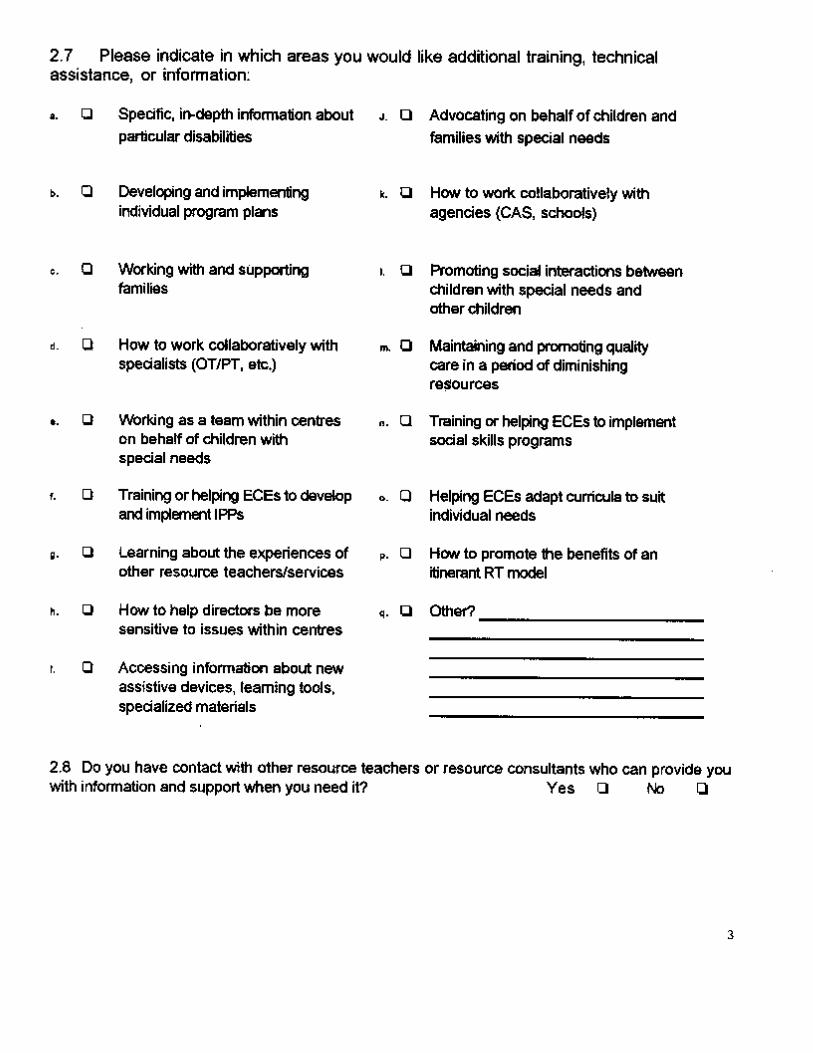
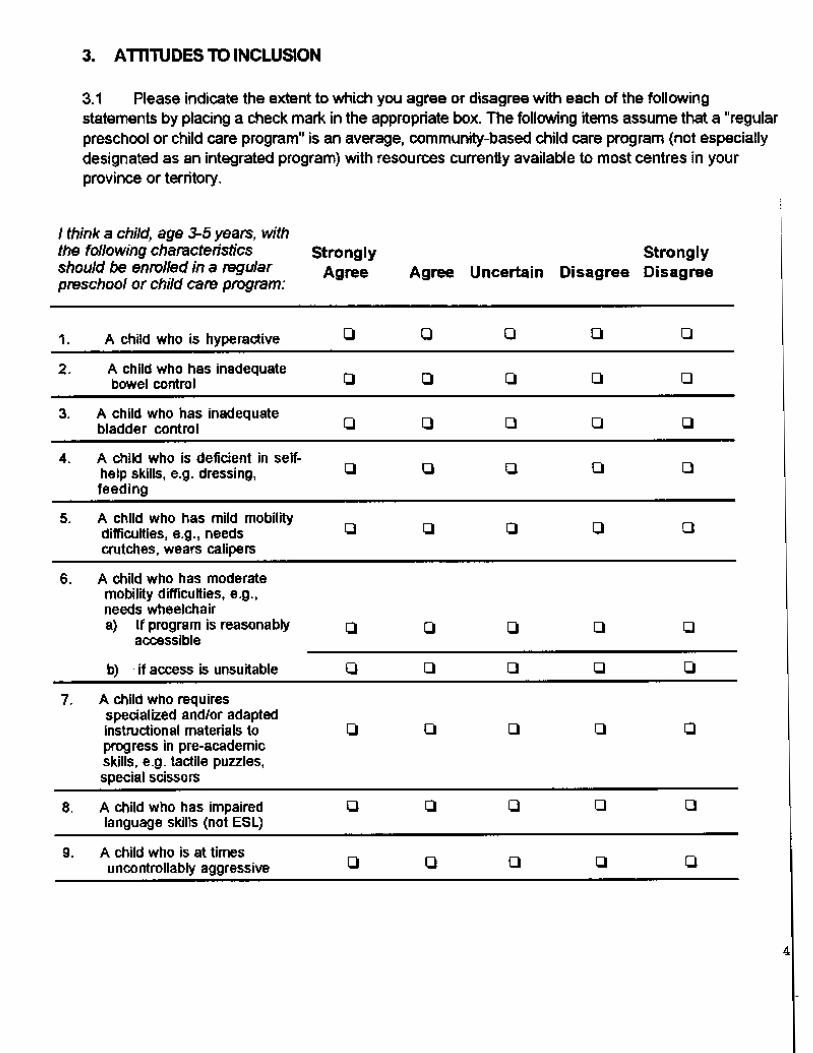
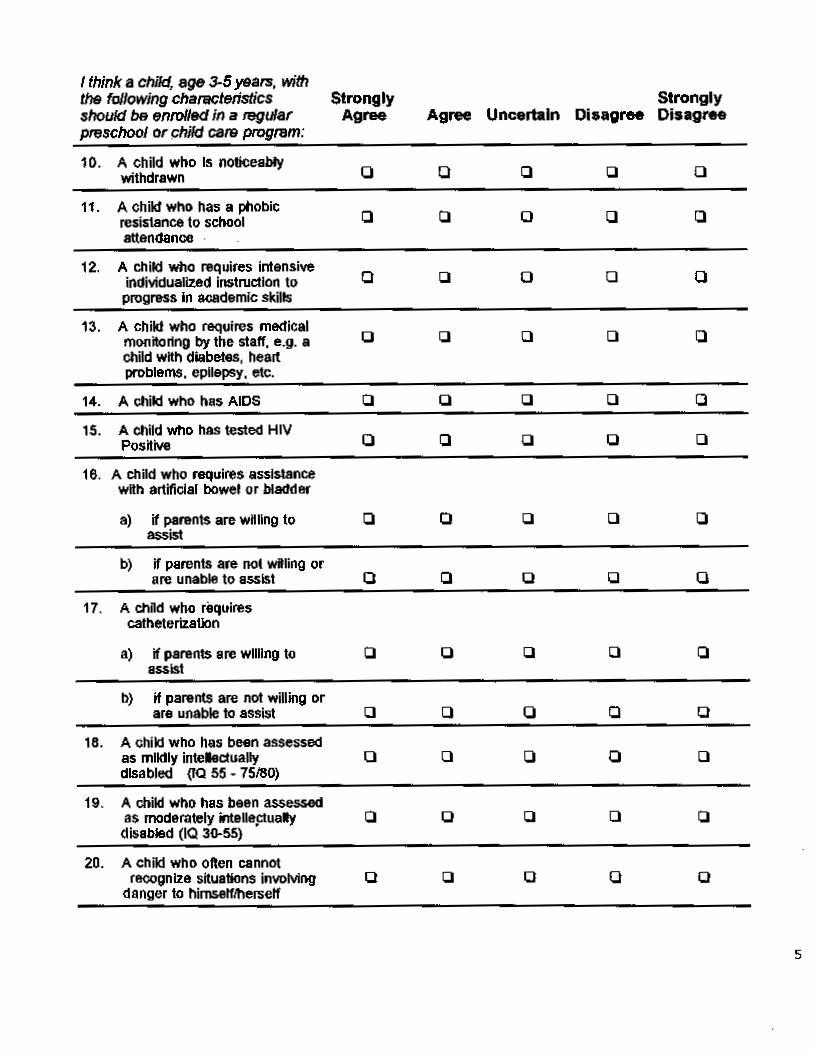
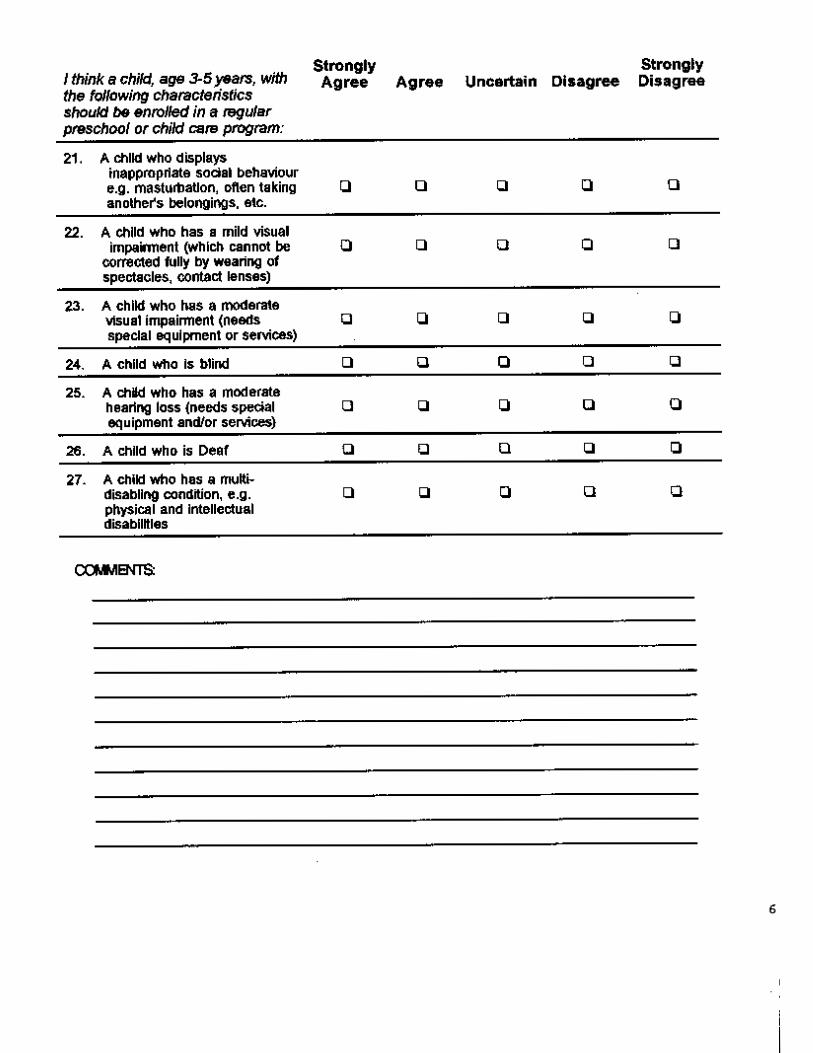
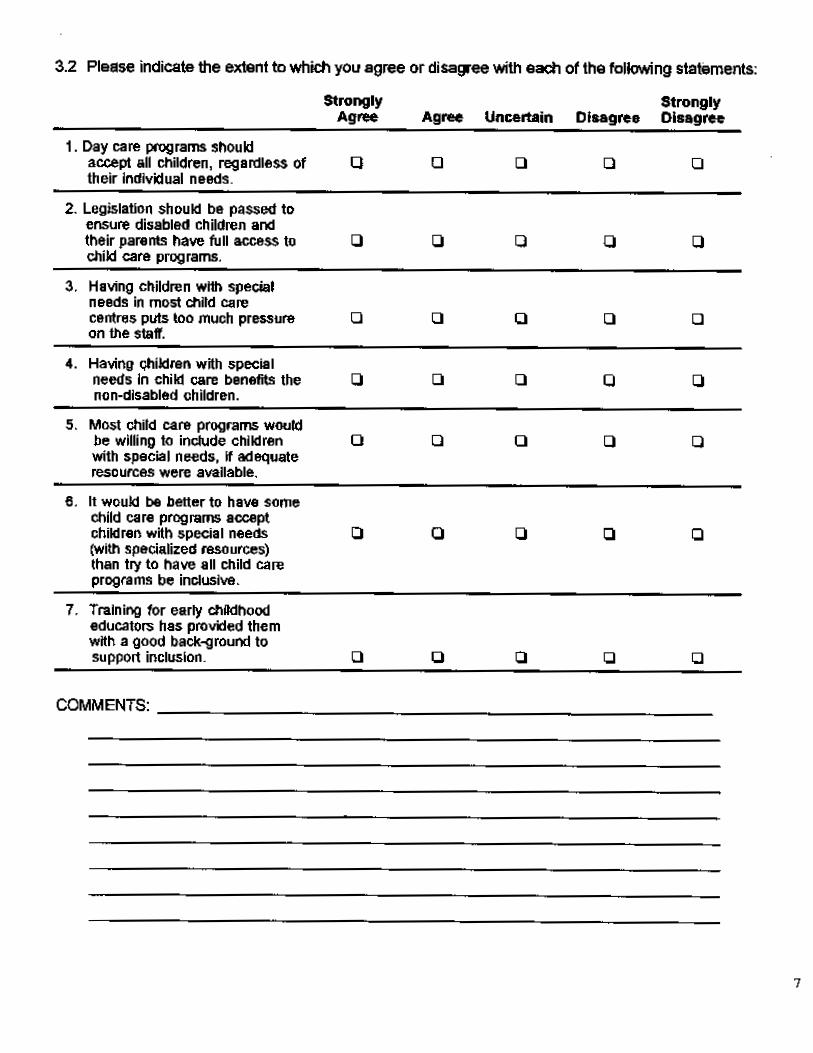
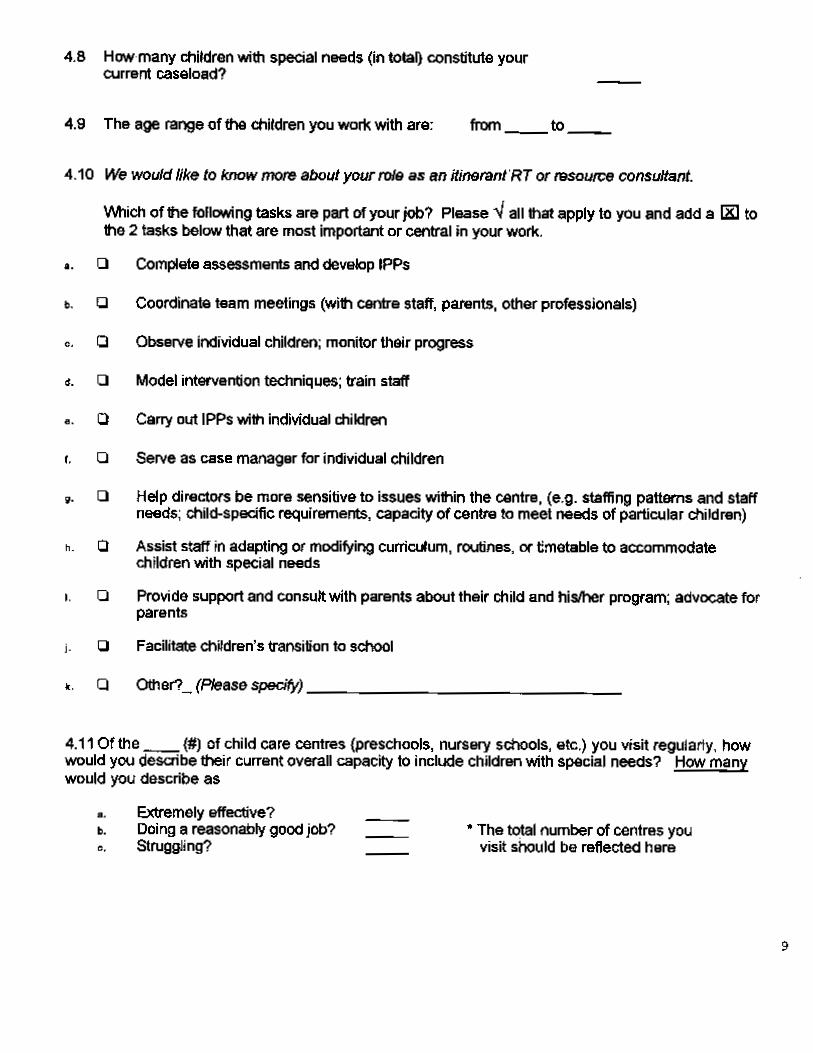
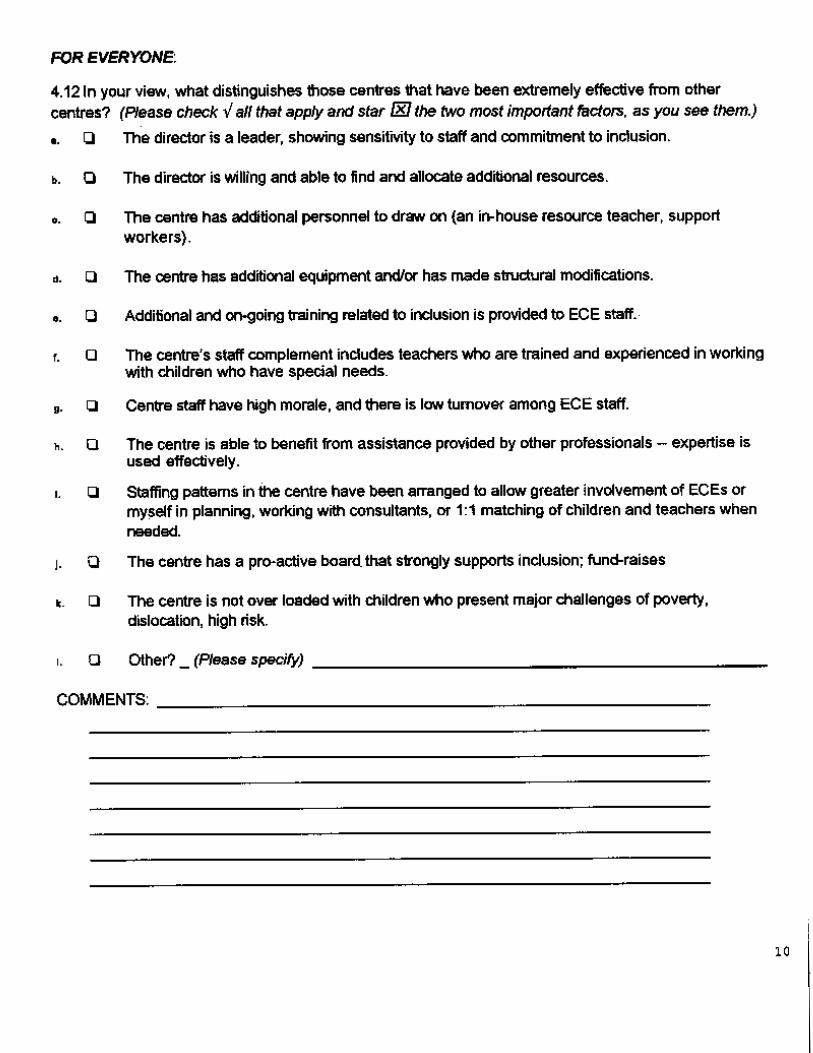
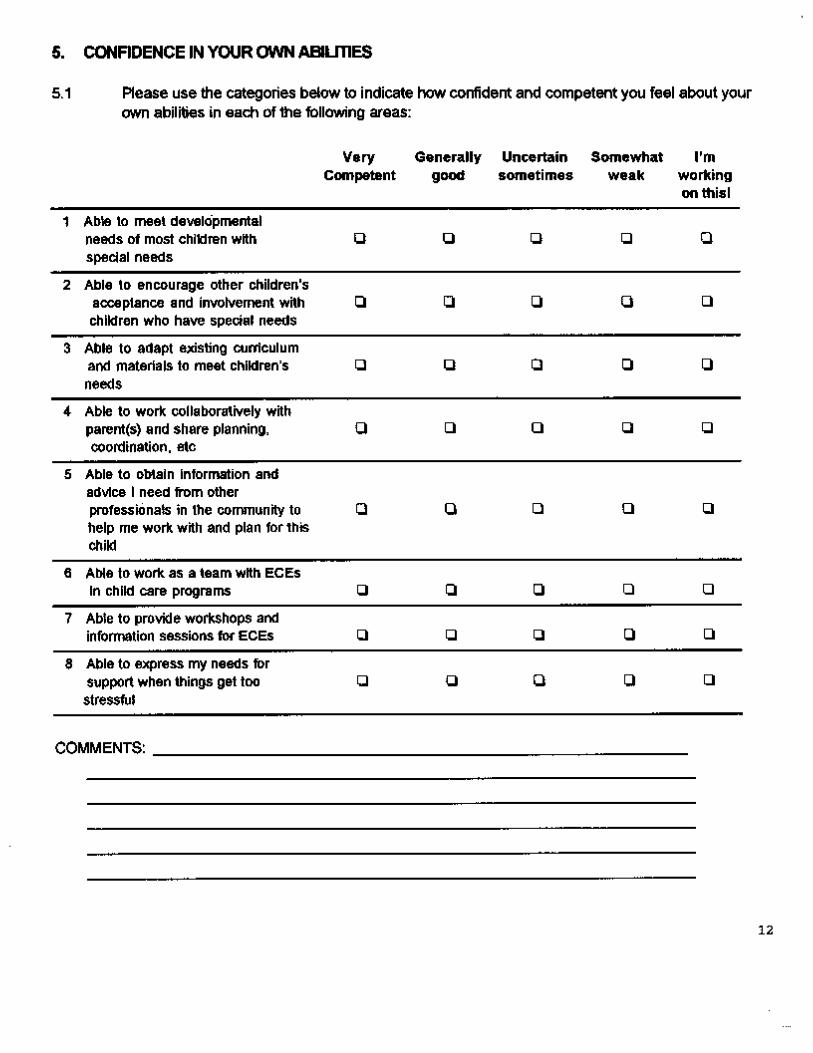
Appendix A: Early Childhood Educator’s and Resource Teacher’s Questionnaire ................. 183Appendix B: Director’s Questionnaire .......................................................................................... 195Appendix C: Itinerant Resource Teacher’s/Consultant’s Questionnaire .................................. 207
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canadax

TABLES
Table 4.1 Response Rates From Directors of Child Care Centres ............................................. 58Table 4.2 Response Rates From ECEs and In-House Teachers ................................................. 59Table 4.3 Response Rates From Travelling Resource Teachers/Resource Consultants ......... 59Table 5.1 Front-Line Professionals’ Educational Background Related to Their Work ............. 70Table 5.2 Directors’ Educational Background Related to Their Work ........................................ 73Table 6.1 The Number of Children With Special Needs Included in All Sample Child
Care Programs ................................................................................................................ 76Table 6.2 The Number of Children With Special Needs Included in Regular and
Integrated Child Care Programs .................................................................................... 77Table 6.3 Reasons Children with Special Needs are Limited to Part-Time Attendance ........... 79Table 6.4 Main Reasons that Caused You to Turn Down a Child (Children) With Special Needs . 80Table 6.5 Extent of Parental Involvement in Centres Including Children With Special Needs 82Table 6.6 Resources Described as “Available” to Support Inclusion by Centre Directors ...... 84Table 7.1 Front-Line Staff’s Current and Recent Involvement With Children Who Have
Special Needs, by Position ............................................................................................ 89Table 7.2 Front-Line Staff’s Education and Training, by Position .............................................. 90Table 7.3 Circumstances in Which Fewer Than 75% of Front-Line Staff Agreed or
Strongly Agreed That Children With Special Needs Should Be Enrolled inRegular Early Childhood Programs .............................................................................. 93
Table 7.4 Front-Line Staff’s Beliefs About Inclusion, by Position .............................................. 95Table 7.5 Nature of Children’s Special Needs Among Those Who Benefited From Inclusion
in the Last Two Years ...................................................................................................... 97Table 7.6 Areas in Which Staff Were Most Successful ................................................................ 98Table 7.7 Factors That Enabled Child Care Staff to Work Successfully, by Severity of
Child’s Condition .......................................................................................................... 100Table 7.8 Factors That Were Frustrating or Problematic in More Successful Situations ...... 102Table 7.9 Resources That Would Have Helped When Problems Arose ................................... 103Table 7.10 Sources of Frustration and Difficulty When Inclusion Was Not Successful ........... 104Table 7.11 Changes in Centre Practices and Resources, as Perceived by Staff ...................... 109Table 7.12 Staff Perceptions of Their Confidence and Competence in Specific Areas ............ 111Table 7.13 Percentage of Staff Wanting Additional Information of Training on a Variety of
Topics, by Position ....................................................................................................... 112Table 8.1 Directors’ Self-Identified Learning Needs ................................................................... 122Table 8.2 Directors Were More Reserved About Including Children in the Following Seven
Circumstances .............................................................................................................. 125Table 8.3 A Comparison of Average Item Scores on Attitudes Towards Inclusion of
Children in Regular Programs Across Three Studies ............................................... 127Table 8.4 Directors’ Beliefs About Inclusion ............................................................................... 128Table 8.5 Changes in Directors’ Personal Beliefs Over Time ................................................... 130Table 8.6 Enablers of Effective Inclusion at the Centre ............................................................. 136Table 8.7 Frustrators of Effective Inclusion at the Centre ......................................................... 138Table 9.1 Geographic Distribution of Travelling Resource Teachers and Resource Consultants . 144Table 9.2 Travelling Resource Teachers’ and Resource Consultants’ Experiential Background .. 144Table 9.3 Travelling Resource Teachers’ and Resource Consultants’ Educational Background .. 145Table 9.4 Resource Teachers’ and Resource Consultants’ Self-identified Learning Needs .. 145Table 9.5 Roles and Responsibilities of Travelling Resource Teachers and Consultants ..... 147Table 9.6 Travelling Resource Teachers’ and Consultants’ Perceptions of What
Distinguishes Extremely Effective Centres From Other Programs ......................... 148Table 9.7 Travelling Resource Teachers’ and Consultants’ Perception of What
Distinguishes Centres That Are Struggling With Inclusion From Other Programs 149Table 9.8 Changes Experienced by Travelling Resource Teachers and Consultants and
the Centres They Visit .................................................................................................. 150
FIGURES
Figure 1.1 Ecological Model of Inclusive Child Care ....................................................................... 7Figure 2.1 Inclusive Early Childhood Development (ECD) Services ............................................ 19Figure 5.1 Child Care Centre Types ................................................................................................. 66Figure 5.2 ECEs & In-House RTs ..................................................................................................... 69Figure 5.3 Centre Directors’ Roles .................................................................................................. 72Figure 7.1 Early Childhood Educators’ Attitudes Towards Inclusion ........................................ 106Figure 7.2 Resource Teachers’ Attitudes Towards Inclusion...................................................... 106
TABLE OF CONTENTS xi

Figure 8.1 Changes in Directors’ Feelings About Inclusion ....................................................... 130Figure 8.2 Cuts Affecting Support for Inclusion and Program Quality ...................................... 139Figure 10.1 A Virtuous Cycle That Supports Effective Inclusion ................................................. 162Figure 10.2 A Discouraging Cycle That Jeopardizes or Defeats Effective Inclusion ................. 163
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canadaxii

INTRODUCTION
Children with special needs are of-ten excluded from child care inCanada. Despite the acknowledgedrole high quality early childhood careand education has in promotingchildren’s development, most gov-ernments in Canada have failed tofully capitalize on the opportunitiesto use child care programs as a de-velopmental resource for childrenwith special needs. Moreover, exclu-sion of children with special needsfrom child care often means thattheir parents cannot participate inpaid employment, or receive thekinds of support that could assistthem as parents.
While all provinces and territorieshave made some provision for theinclusion of children with specialneeds, in no jurisdiction is it illegalto exclude a child from child careon the basis of disability or otherspecial needs. And while many pro-vincial officials and child care con-sultants have worked diligently tomake inclusion a reality in their ju-risdictions, written policies, train-ing requirements, and resource al-location seldom suggest systematic,stable support for inclusion. Con-sequently, it often falls to individualchild care centres to choosewhether to include or exclude thesechildren — a situation that is anti-thetical to the rights-based systemdefined in the UN Convention on theRights of the Child to which Canadais a signatory, and to the spirit of
OVERVIEW: A MATTER OF URGENCY
the 1998 In Unison accord of thefederal, provincial and territorialgovernments.
Despite the lack of pro-active legis-lation and policy that would pro-hibit exclusion and facilitate the ef-fective inclusion of children withspecial needs in child care, manycentres have gone ahead and in-cluded children with special needs.This study, A Matter of Urgency, fo-cuses on understanding what hasenabled and what has frustrated ef-forts to include children with spe-cial needs in Canadian child carecentres. It is based on a sample of136 child care centres that have along history with inclusion. It trackstheir experiences with inclusionover time, and identifies the mostcritical factors that have contrib-uted to their success or frustratedtheir efforts. The findings identifywhat steps are required to ensurethat other child care programs(typically with less experience withinclusion and often with fewer re-sources) will be able to provide ef-fective child care and developmen-tal stimulation to children with awider range of special needs.
The findings in A Matter of Urgencysuggest that regular Canadian childcare programs, when adequately re-sourced, can provide appropriatecare for children with special needs.However, the research findings alsodemonstrate that continued under-funding, cutbacks, lack of training,and lack of clear governmental di-
OVERVIEW: A MATTER OF URGENCY xiii

rectives compromise the capacity ofeven the most experienced andcommitted child care programs tocontinue to provide effective inclu-sive care and developmental stimu-lation to children with specialneeds.
The findings in A Matter of Urgencydemand unequivocal answers frompolicy makers and politicians re-garding the inclusion of childrenwith special needs in child care. In1982, under Canada’s Charter ofRights and Freedoms, children withspecial needs finally gained theright to attend school in all prov-inces and territories. In signing theUN Convention on the Rights of theChild in 1991, Canada made addi-tional commitments to childrenwith special needs. Today, it is amatter of urgency that children withspecial needs finally gain the rightto attend child care programs in allprovinces and territories with theirnon-disabled peers, and that theseprograms be adequately resourcedto meet their needs. These childrenmust no longer be excluded andsegregated.
FINDINGS
One of our main findings is thatearly childhood educators’ actualexperiences with inclusion, nottheir general attitudes and beliefs,most strongly influence their com-mitment to inclusion, their accep-tance of a broader range of childrenwith special needs being included,and their comfort and confidencein working with children with spe-cial needs. Positive experiences forthe staff and children depend onhaving additional resources to sup-port inclusion (e.g., appropriatetraining, additional staff, time toplan and work collaboratively withparents and community-based pro-fessionals, and sometimes struc-
tural modification if the program isnot accessible) that build on a baseof high quality care.
Positive experiences for the childrenalso require care provided by com-mitted, well-trained staff in centresthat have stable funding and areable to provide children with devel-opmentally appropriate experienceson a consistent basis. Poor experi-ences with inclusion occur whenstaff are not trained or resourcedto meet the needs of children withdisabilities, when they have few re-sources or supports availablewithin the centre, and no or littlesupport from specialists in the com-munity. Under these circum-stances, and with continued finan-cial pressures on centres, programsare hard pressed to include anychildren with special needs, or todo so with positive results.
A second very strong finding is re-lated to the crucial importance ofthe centre director as a leader. Sincechild care centres are not requiredto include children with specialneeds, it is not surprising that theirwillingness to do so is usuallyhighly influenced by the director’scommitment to inclusive principlesand practices. Centres that weredescribed by resource consultantsin our study as extremely effectivewith inclusion had directors whowere leaders, who showed sensitiv-ity to staff needs, and who were ef-fective in finding and allocatingadditional resources to support in-clusion.
Even these positive indicators mustbe tempered by the finding that89% of the directors reported reduc-tions in funding, staffing, or accessto professionals that had affectedtheir centre’s capacity to be inclu-sive, and 41.5% reported cuts orchanges that were causing serious
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canadaxiv

als, and to act as advocates for in-clusion.
Many child care centres in oursample were including childrenwith a wide range of special needs,and more than 60% of the direc-tors say that their centres have be-come more effective and inclusiveover time.
In our opinion, it is a credit to thisworkforce that they have reachedthis level of commitment despite thelack of clear policy directives fromgovernments and in the face of in-sufficient funding, inadequate staff-ing and resources, and the generallack of support for inclusive childcare. That said, it is critical to pointout that the limits of voluntary in-clusion may have been reached inthese centres, that they have goneabout as far as they can go withoutclear policy directives and guide-lines, and without additional fundsand resources.
Our findings confirm and extendthe published research on inclusivechild care. They point to obviousrecommendations for policy mak-ers, post-secondary training pro-grams in Early Childhood Educa-tion and related areas, for the childcare field, and for disability rightsadvocates and parents. Most im-portantly, our findings identify twomajor policy issues that must beaddressed if effective inclusive prac-tice is to become a reality acrossCanada: 1) The need for clear gov-ernmental directives and guidelinesregarding the responsibilities ofchild care centres to include chil-dren with special needs given ap-propriate resources to enable themto do so and, 2) The importance ofhigh quality child care programs asa necessary base for supporting theoptimal development of young chil-dren with special needs and their
OVERVIEW: A MATTER OF URGENCY xv
problems in maintaining that ca-pacity in the year preceding datacollection. Under these circum-stances, centres may cease to en-roll any children with special needs,or do so only on occasion, accept-ing children who fit a narrow bandof conditions that they feel they canaccommodate, retrenching from aview of their centre as an inclusiveprogram.
CONCLUSIONS
The results of our study indicatethat Canadian child care centres,when appropriately resourced, canand do include children with spe-cial needs, and have substantialpositive impacts on their develop-ment. 78.7% of staff who workedwith children who had moderate orsevere disabilities rated their suc-cess as high.
A large majority of front-line childcare centre staff and centre direc-tors in our sample believe that chil-dren with special needs shouldhave the right to attend child careprograms, and that legislationshould be passed to prevent theirexclusion. 89.5% feel that mostchild care centres would be willingto include children with specialneeds if adequate resources werein place to support their efforts.
Also on the positive side, the ma-jority of child care staff felt morecompetent and confident in work-ing with children with special needsas a result of positive experienceswith inclusion in their centres andthrough their attendance at work-shops and conferences. Directors ofcentres identified as extremely ef-fective at inclusion demonstratedleadership skills that enable themto access additional resources, toestablish productive relationshipswith staff and external profession-

typically developing peers.
1. Directives and Guidelines
Historically, many inclusive childcare centres have developed on anindividual basis, often as the resultof commitment by a strong direc-tor, who initially responded to theplea of a particularly persuasiveparent. Some funding and supportfrequently followed, and serviceagencies, as well as provincial childcare offices, began to refer childrenwith special needs to these centres.However, this situation is charac-terized by ad hoc-ery, wherein onecentre may include children withspecial needs and another, withidentical resources, may not.
Without policy directives and ap-propriate resources from govern-ment, inclusive child care is likelyto continue to be hit-and-miss, vari-able across and within jurisdic-tions, and sustainable only to thedegree that exceptional individualsmake it happen.
2. The Role of High Quality ChildCare in Achieving Effective Inclusion
The second major policy issue thatthis study raises is the relationshipbetween effective inclusion of chil-dren with special needs and thequality of child care centres.Whether one views effective inclu-sion as an optional but possibleadd-on to high quality programs, orwhether one views it as a more re-cently recognized dimension of highquality child care, the two conceptsare inextricably linked.
Despite the lack of both pro-active,supportive public policy in mostjurisdictions and appropriate fund-ing, inclusive child care does hap-pen. Children with special needsare included in many child carecentres across Canada and receive
a good, developmental experiencethere. Taking nothing away fromthose directors and staff who, withlimited supports, find a way tomake inclusion happen, it is obvi-ous that this is not a secure sys-tem. It is always fragile. It is sub-ject to changes in funding and sup-port and rests on the backs of ex-ceptional directors and staff. With-out a coherent child care systemand consistent coordination withrelated health professionals, thelikelihood of sustaining such cen-tres is questionable.
Research and practice lead to thesame conclusion: effective inclu-sion only happens in high qualitychild care.
Today, a convergence of three fac-tors provides a positive context forgovernments and early childhoodprofessionals to respond to the rec-ommendations in this report:
• new knowledge about the impor-tance of developmental stimulationin the early years and the benefitsof early intervention and supportfor children with special needs andtheir parents
• recognition of the rights of indi-viduals with disabilities to fullyparticipate in their communities,
• federal/provincial/territorialagreements to invest in a system-atic, long-term effort to build andstrengthen Early Childhood Devel-opment services
Doing so would not only benefitindividual children and families; itwould also move Canada further asa nation that has made importantcommitments to support familiesand communities in their efforts toensure the best possible future forALL of Canada’s children. This is,indeed, A Matter of Urgency.
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canadaxvi

1INTRODUCTION AND BACKGROUNDCHAPTER 1
INTRODUCTION
AND BACKGROUND
ents and advocates — for all peoplewho have a stake in fully includingchildren with special needs in childcare.
The abstract factors that are re-lated to successful inclusion —funding, commitment, experience,training, support, the base qualityof programs, etc. — are well knownand frequently discussed in the lit-erature and in public fora. Butwhat factors, this study asks, haveactually made a difference in Ca-nadian child care centres that suc-cessfully include children with spe-cial needs and in those centres thathave been less successful?
In 1990, one of the authors1 sur-veyed a purposive sample of childcare directors and front-line staffworking in child care centres thatincluded children with specialneeds. In 1996, the originalsample (augmented as necessary2)was surveyed again. By 1996-97,these centres had been includingchildren with special needs for atleast seven years, most of them formore than a decade. Thus, thisstudy is about centres and staffwhose level of experience, trainingand commitment to inclusion areunusual in Canada. In a largenumber of these centres, many ofthe major obstacles to successfulinclusion had been overcome or
1.1.1 INTRODUCTION
The present study is a unique, in-depth and multidimensional ex-amination of inclusive child care inCanadian child care centres. Ourpurpose was to develop a compre-hensive understanding of the vari-ous factors that affect the inclusionof children with special needs inearly childhood programs, based onthe perspectives and experiences offront-line staff, centre directors,and external resource consultants.
Our national sample of centres andchild care professionals was pur-posively selected to maximize theopportunity to learn from thosewho have had considerable experi-ence in including children with spe-cial needs. However, the informa-tion gained from this sampleshould be relevant to other pro-grams that have had less experi-ence or are struggling with inclu-sion, since the findings indicateboth factors that support positiveexperiences and result in a sus-tained, deepening commitment toinclusion, as well as those factorsthat are likely to be significant bar-riers and frustrators to effectiveinclusion.
This study will also provide impor-tant information for policy makers,trainers, related professionals, par-
Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy

2 A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada
Our goal was toanswer the ques-tion: “What pro-duces, enables,supports andsustains effectiveinclusion, fromthe standpoint ofstaff and direc-tors in child careprograms?”
made manageable. Thus this studyprovides a portrait of what inclu-sive child care can become in all ofCanada.
Typically, inclusion is consideredsuccessful if it has positive impactson children’s development, particu-larly for children with specialneeds, but also for typically devel-oping children who may becomemore tolerant, accepting of diver-sity and empathetic. It is thoughtthat all children are likely to ben-efit when centre staff become moreknowledgeable and skilled throughtheir work with a broader range ofchildren and when inclusion bringsadditional resources to the centre.
As a result, most studies focus ei-ther on some identifiable child out-comes, or on processes in whichchildren are engaged that mightsuggest successful inclusion (e.g.,progress in meeting Individual Edu-cational Program [IEP] goals; timespent in child-initiated activities inwhich both children with specialneeds and typically developing peersare involved; time spent in variouskinds of play activities with peersand objects, as opposed to timespent interacting with teachers oralone). Rigorous research that canassess the outcomes of participat-ing in inclusive programs for chil-dren requires a longitudinal designwith control or comparison groupsand valid measures or indicators ofprogress or success.
In contrast to these approaches,our study was directed towardsunderstanding how inclusive prac-tice is viewed and experiencedwithin centres by program staffthemselves, by the directors of childcare programs, and by external re-source consultants who provideassistance to those programs.Rather than assessing outcomes
for individual children and families,our focus was oriented towardsunderstanding inputs and pro-cesses within child care programsthat relate to staff’s experiences,attitudes, and capacities to includechildren with special needs in theirprograms and to do so effectively.In effect, our focus was on explain-ing what successful inclusion mightlook like from the standpoint of cen-tres and centre staff. Our goal wasto answer the question: “What pro-duces, enables, supports and sus-tains effective inclusion, from thestandpoint of staff and directors inchild care programs?”
Since we relied on survey data gath-ered through mailed questionnaireswith no direct observations of prac-tice, our analyses of correlates ofeffective inclusion are based on re-spondents’ perceptions and self-re-ports. However, we view these notas weak proxies for observable data,but as critically important in theirown right, reflecting the views andperceptions of front-line staff anddirectors. The importance of theirviews lies in the fact that if, in theireyes, the program is struggling toinclude children with special needs,or if staff are wavering in their com-mitment to inclusion, or if both di-rectors and teaching staff see re-sources as being inadequate to sus-tain their existing efforts and nega-tively affecting the quality of careprovided to children in the centre,then on-going, successful inclusionis compromised. On the other hand,if child care professionals see thattheir skills, resources, and supportsare enabling them to effectively in-clude children with special needs,then they provide evidence of howsuccessful inclusion can be accom-plished, and what is necessary tomaintain and enhance child care in-clusion in Canada.

3INTRODUCTION AND BACKGROUNDCHAPTER 1
1.2 BACKGROUND
In the last few years of the 1990s,consultations about the scope andimportance of a national agenda forchildren have been held acrossCanada, and the early years havebeen recognized (again) as a criti-cally important time to supportchildren’s optimal development.The National Children’s Agenda,Centres of Excellence for Children’sHealth and Well-Being, the NationalChild Tax Benefit and the Reinvest-ment Fund, and extended parentalleave under the Employment Insur-ance Program are the most visibleitems on the federal/provincial/territorial agenda related to youngchildren and their families.
Notwithstanding the rhetoric andsome renewed interest and rein-vestments in child care and earlyintervention programs in manyparts of the country, advocates forchildren with special needs wereable to make a compelling case in1999 that Canada is not in com-pliance with the UN Convention onthe Rights of the Child in its provi-sions for children with specialneeds.3 It is still the case that notall children in Canada have accessto the range of health, educational,and community-based servicesthat are needed to ensure theirhealthy development. Against thisbackdrop, those concerned aboutthe availability, affordability, andquality of early childhood servicesmust reflect on the capacities ofchild care programs to provide highquality, inclusive care for all ofCanada’s children and families.
Research on the topic of inclusiveearly childhood programs is quitelimited in Canada, but has been thesubject of a number of investiga-tions in the United States, in partdue to a different history that man-
dates access to free, appropriate edu-cation for children with special needsin the least restrictive environment.Currently, the published researchsuggests that, on the one hand, thereappears to be growing acceptance ofinclusion in early childhood pro-grams as an effective and appropri-ate way to support children’s devel-opment, and as a positive indicatorof program quality. On the otherhand, significant barriers to effectiveinclusion remain.
In Canada, no province or territorymandates access to early childhoodprograms for children with specialneeds. Hence, whether a centrechooses to enroll children with spe-cial needs at all, and/or whatcriteria are used for deciding whichchildren to enroll depend largely onthe director’s and staff’s attitudestowards inclusion, and theirperceptions of their centre’scapacities, given limited additionalresources. Federal and provincial/territorial policies that would pro-vide the necessary infrastructureand funding support to enable pro-grams and communities to ensureappropriate access remain unde-veloped.
In 1995, for example, no provincialor territorial government had writ-ten policies regarding equitableaccess to child care for childrenwith special needs. Fundingsupports for programs willing toinclude children with special needsvaried from none to limited grants,inequitably available across thecountry. Only two provinces hadany education/training require-ments for staff in child careprograms who are working withchildren with special needs, andnone had developed formal policiesto promote and support collabora-tion between program staff andcommunity-based professionals in

4 A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada
health, speech and language ser-vices, and other specialties.
Post-secondary Early ChildhoodEducation (ECE) training institu-tions have played a key role inmoving the field forward towardviewing child care as holistic, in-clusive and family-centred. Yet, in1996, across Canada, only 15% ofcertificate programs for EarlyChildhood Educators (ECEs), andonly 66% of the diploma programscontained either a course or signifi-cant mention (“explicit infusion ap-proach”) about special needs.4
Recent national data suggest thata substantial number of child carestaff are attending in-service work-shops on topics related to childrenwith special needs and that a sur-prisingly large proportion of cen-tres (as many as 60 to 70 percent)reportedly enrolled at least one ortwo children with special needs in1998.5 It therefore seems that somechild care centres and their staffare making considerable efforts tobegin to include children with spe-cial needs in their programs, evenin the absence of policies and pro-grammatic supports.
Meanwhile, despite a few proactiveand creative initiatives at the policylevel that have emerged from timeto time or been partially imple-mented, there have been no signifi-cant or systemic efforts made todetermine the extent to which earlychildhood programs in Canadahave the desire, the capacity, andthe resources needed to includechildren with special needs effec-tively — or to sustain their com-mitment to do so over time. Well-designed initiatives have not beenrigourously evaluated to determinewhat combinations of training,supports and resources are mosteffective for meeting the needs of
children, families, and communi-ties — with child care programs asa major partner in those efforts.Without such research, it is diffi-cult to make specific recommenda-tions to policy makers, to facultyin post-secondary institutions whoprovide pre-service and continuingeducation to the child care field, tochild care administrators, and torelated health and social serviceprofessionals that could addressthe unmet needs of child care cen-tres and their staff and provide theinfrastructure they need to providehigh quality, inclusive care.
1.3 DEFINING “INCLUSION”
Writers and researchers on thetopic of inclusive programs ac-knowledge that a single, clear defi-nition of inclusion would be use-ful, but no single definition has yetbeen accepted. The termsmainstreaming, integration, andinclusion have sometimes beenused as synonyms and sometimesas different and contrasting pointson a continuum that runs fromsegregation and exclusion on oneend to full inclusion on the other.We have adopted the views ofOdom, Peck, Hanson, Beckman,Kaiser, Lieber, Brown, Horn andSchwartz (1996) and Kontos, Mooreand Giorgetti (1998) who refer toinclusion (particularly in earlychildhood programs) as a multi-di-mensional concept that embodiesseveral aspects.
Odom et al. have written aboutfour features of inclusion:
“First, inclusion is the active par-ticipation of young children withspecial needs and typically devel-oping children in the sameclassroom....and/or communitysettings. Second, services should

5INTRODUCTION AND BACKGROUNDCHAPTER 1
be provided that support the childin accomplishing the goals estab-lished for him or her by the par-ents and a team of professionals.Third, these services are usuallyprovided through the collaborationof professionals from different dis-ciplines (e.g. early childhood edu-cation teachers, special educationteachers, speech pathologists).Fourth, the effect of the inclusionprogram on children with specialneeds is evaluated to determine ifthe child with special needs is mak-ing progress toward goals estab-lished by parents, teachers, andother professionals.”6
Kontos, Moore and Giorgetti (1998)suggest that definitions of inclusiontypically involve “a child with spe-cial needs receiving comprehensiveservices in a developmentally ap-propriate program side-by-sidewith children without special needsand participating in the same ac-tivities, with adaptations to thoseactivities (or the child’s involvementin them) as needed.” They also sug-gest that this definition of inclusionrepresents “a blended approachthat integrates early childhood spe-cial education, regular early child-hood education, and therapeuticinterventions and presumes a teamapproach to early intervention.”7
Other working definitions of inclu-sion add elements of anti-discrimi-nation. SpeciaLink,8 for example,proposes that, in full inclusion, nochildren are excluded because oflevel or type of special need. Build-ing on a base of high quality corechild care, this definition includesfive elements: 1) zero reject; 2)naturally occurring proportions oftypically developing children andchildren with special needs; 3) fullparticipation of all children in allactivities; 4) same range of options
for attendance of all children (e.g.,part-day; full-day, casual); 5) ad-vocacy, pro-action, and parent par-ticipation to the maximum extentdesired by parents.
The Division of Early Childhood(DEC) of the Council of ExceptionalChildren adopted the following po-sition in 1993:
“Inclusion, as a value, supports theright of all children, regardless oftheir diverse abilities, to participateactively in natural settings withintheir communities. A natural set-ting is one in which the child wouldspend time had he or she not hada disability. Such settings includebut are not limited to home andfamily, play groups, child care,nursery schools, Head Start pro-grams, kindergartens, andneighbourhood school class-rooms.”9
In 1994, the National Associationfor the Education of Young Chil-dren (NAEYC), the largest U.S. earlychildhood organization, endorsedthe DEC position and began to ad-dress issues related to inclusion intheir research, advocacy, confer-ences, and popular and scholarlypublications.
These discussions of definition arehelpful in clarifying some of theunderlying assumptions that mustbe examined before we can use theterm “inclusion” consistently andmeaningfully. Clearly, what is be-ing referred to is more than simplythe physical presence of childrenwith special needs in early child-hood programs or in a limited rangeof activities within those programs.A definition can also be an ideal. Itis understood that full inclusion ispremised on a program supplied bywell-trained and well-resourcedearly childhood educators, who are

6 A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada
1.4 OUR THEORETICAL MODEL:THE ECOLOGY OF INCLUSIVECHILD CARE
An ecological approach has beenused by a variety of researchersboth to study inclusion processesand outcomes, and to understandthe complexity of factors that af-fect the quality of child care pro-grams. Bronfenbrenner’s (1979)10
conceptualization of the ecology ofhuman development has beenadopted by many writers as a use-ful framework for understandingthe complex array of influencesthat shape children’s development.In simple form, this model is oftendescribed as a system of systems –from those most immediate to thedeveloping child to those that arefurther removed. Bronfenbrenner’sown analogy is to a set of Russiandolls with smaller ones nested inlarger ones. There are fourlevels of systemic influencesthat are typically referred to, in-cluding microsystems, mesosystemrelations, exosystems, and macro-system influences.
The microsystem level consists ofthe specific settings, such as thefamily or a child care classroom/group in which a child is an activeparticipant. Each microsystem canbe studied in terms of “the patternof activities, roles, and interper-sonal relations experienced by aparticular child in that setting, in-cluding its particular physical andmaterial characteristics.” The ma-jority of research on integratedearly childhood programs has fo-cussed on this level, includingmany studies that describe socialinteractions among children withspecial needs and their typicallydeveloping peers, characteristics ofchildren’s play and activities withpeers and objects, and the natureof teacher-child interactions.
supported by external profession-als as required
In this report, when we use theterm inclusion, we mean a blendedapproach — one that actively in-volves early childhood educators,resource teachers/support work-ers, resource consultants, centredirectors, parents, and a range ofcommunity-based specialists incollaboratively planning andcollaboratively implementing mu-tually supportive efforts to ensurethat the early childhood programand its staff provide an environ-ment that is developmentally ap-propriate for the full range of chil-dren who attend.
Research and practical experiencesuggest that this outcome is notlikely to emerge and be sustainedin the absence of sufficient re-sources and inputs — especiallywhen programs attempt to includechildren with more complex healthconditions or challenging be-haviours or when programs are notof high quality to begin with.
At issue is not only what is neededto provide support, appropriatestimulation, and program modifi-cation for individual children withspecial needs, but also what isneeded to include the child withspecial needs within a group ofyoung children while maintainingappropriate, responsive care for allof the children in attendance. Whilethere may not be agreement on theanswer to that question, it is es-sential that child care and relatedprofessionals and policy makersuse this research study and oth-ers to develop and act on an un-derstanding of what resources areneeded to assure effective inclusion— inclusion that works for the chil-dren, for the staff and their cen-tres, and for their communities.

7INTRODUCTION AND BACKGROUNDCHAPTER 1
The mesosystem level actually re-fers to the manner in which two ormore microsystems relate to eachother. Most obviously, the natureof home-school and parent-caregiver relations come to mind asimportant factors to consider inunderstanding how children maybe influenced differentially depend-ing on whether the links betweenthese microsystems are character-ized as strong or weak, mutuallysupportive or antagonistic, com-municative or distant, reflectingsimilar or different values and ex-pectations with regard to the child’sabilities and behaviour, and therole of parents, teachers, and oth-ers. Since the concept of inclusion,as defined earlier, requires collabo-ration and communication, thenature of these mesosystem linksis quite important, not only for theircontribution to positive child out-comes, but also because they af-fect the experience of each adultparticipant.
The exosystem level is defined byBronfenbrenner as consisting ofone or more external settings thatdo not involve the developing per-son as an active participant, but
are locations in which events oc-cur that affect, or are affected by,what happens in the setting thatdoes contain the developing child(or other target person). Examplesoften include a parent’s workplaceas an environment in which work-family conflicts may be engenderedor reduced, depending on workcharacteristics, the degree of flex-ibility provided to the parent em-ployee, etc. In terms of inclusivechild care, exosystems might in-clude municipal planning bodies,school boards, and health unitsand other agencies in the commu-nity, whose policies, resources, andorganizational mandates or struc-tures can affect the availability ofresources allocated/allocatable tosupport inclusion in child care pro-grams. Government policies, regu-lations and funding mechanismsacross a variety of program areas,but particularly those related toearly childhood services, play amajor role at the exosystem levelthat determine the nature ofmicrosystem resources andmesosystem relations that aremore immediate to the experiencesof children in inclusive programs.

8 A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada
influenced by a dynamic set of fac-tors operating inside and outsidethe classroom. Understanding thelinkages among the full range ofinfluences and outcomes is crucialto identifying the barriers to andfacilitators of preschool inclu-sion.”11
Moreover, Peck extends this discus-sion by referring to the importanceof studying changes over time andby referring to the importance of atransactional perspective, embod-ied within ecological analysis. Pecknotes that social processes andoutcomes of integrated programsare likely to change over timeas both individuals andsystems develop. He points outBronfenbrenner’s emphasis on un-derstanding relationships, pro-cesses, and events as they are ex-perienced by different individualsas factors that influence eachperson’s understandings, behav-iour and development. This phe-nomenological emphasis on under-standing inclusion as experienced isgermane to appreciating, for ex-ample, how inclusion is experiencedby, and affects, each of the individu-als involved (children, parents,teachers, directors, specialists).12
1.5 GOALS AND OBJECTIVES OFTHE PRESENT STUDY
Understanding inclusion as expe-rienced by early childhood profes-sionals and directors of child careprograms is at the heart of thepresent study. In it, we focus onunderstanding early childhood pro-fessionals’ attitudes and beliefsabout inclusion, and their experi-ences in providing inclusive careover the last several years.
We also obtained information fromcentre directors and external re-source consultants who could pro-
Finally, the macrosystem level isdescribed by Bronfenbrenner asreflecting broad organizationalproperties of a society, includingfundamental beliefs, assumptionsand values (ideologies) that influ-ence social organizations and so-cial structures, and are manifestlyevident in laws, professional prac-tices, and media images. Beliefsabout the role of government, in-dividuals, families and charitableinstitutions are part of themacrosystem, as are changingviews about people with disabilitiesand their citizenship rights. Themacrosystem refers to the cultureas a whole, general prototypes, andrecorded laws and regulationswhich overarch society. There maybe differences between subcultureswith respect to macrosystemvalues. While of overarching sig-nificance, macrosystem compo-nents are mutable and change overtime, especially as a result of con-certed influence by an electorate orpowerful individuals who are in aposition to effect significantchange.
In addition to articulating these dif-ferent levels of influence, an eco-logical analysis pays special atten-tion to the dynamic, reciprocal in-teractions that are always occur-ring between levels. As Odom et al(1996) and Peck (1993) have noted,studies of important factors at themicro-system level (e.g., teacher-child interactions or staff attitudes)that occur without reference to thesocial, organizational, resource, orpolitical/values context in whichprograms operate provide adecontextualized or partial per-spective on inclusion.
“Each aspect of the research pro-vides a view of one piece of thepuzzle — a single dimension of theinclusion process. Yet inclusion is
9INTRODUCTION AND BACKGROUNDCHAPTER 1
vide contextual information aboutcentres as organizations that areattempting to provide inclusivecare. We have supplemented thisdirect information with detail aboutthe policy context that has influ-enced the provision of child careand the resources available to sup-port inclusive early childhood prac-tices in Canada during the 1990s.
In broad terms, the main goal ofthis study was to develop an in-depth understanding of the ecologyof inclusive child care in Canada,and to use that knowledge to pro-mote more effective inclusion on adaily basis.
The specific objectives that guidedthe design and analysis of the studywere as follows:
✦ To describe the extent to whicha selected sample of child care pro-grams have continued to includechildren with special needs, howthese programs function, what is-sues or challenges they face, whatresources they rely on to effect posi-tive experiences for staff, children,and families.
✦ To assess whether early child-hood educators (ECEs) anddirectors in community-based childcare centres have changed theirattitudes about including childrenwith special needs since 1990 —whether they are more committedto the concept of inclusion; whetherthey are more accepting of abroader range of children; whetherthey are more comfortable workingwith children with special needs;and whether they feel more com-petent in working together to meetchildren’s needs.
✦ To learn what factors appear tobe most important for enablingfront-line staff to be successful intheir work with children with spe-
cial needs; for enabling programsto become more inclusive and/ormore effective in including childrenwith special needs; and for distin-guishing between programs thatare extremely effective from thosethat are doing a reasonable job orstruggling.
✦ To learn what kinds of informa-tion and training related to childrenwith special needs ECEs anddirectors have been exposed to inthe last 6-7 years, and to obtainteachers’ assessments of theusefulness of that information, aswell as current unmet educationalneeds.
✦ To learn about ECEs’ anddirectors’ experiences with inclu-sion, how they have adapted theirprograms, and what factors con-tribute both to success and frus-tration.
✦ To obtain ECEs’ and directors’perspectives on current resourcesavailable to them, and determinewhether financial constraints orrecent policy changes have affectedchild care programs in their capac-ity to maintain inclusiveness as adesired goal and feasible practicein their community.
✦ To take these lessons learnedfrom the field to develop specificrecommendations to support effec-tive inclusion by considering theirimplications for policies and fund-ing, training, and support for bestpractices.
1.6 UNIQUE CHARACTERISTICSOF THIS RESEARCH STUDY
There are four features of this par-ticular project that combine tomake this study unique.
The first is that we have used mul-tiple windows to view inclusive child

10 A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada
care. We obtained both parallel andcomplementary information fromthree sample groups: centre direc-tors; early childhood educators andin-house resource teachers; andtravelling resource consultantswho provided an external, validat-ing perspective on information ob-tained from child care staff.
The second feature is that we de-signed this study to allow us toobtain information on changes overtime in child care professionals’attitudes, commitment to inclu-sion, willingness to accept abroader range of children with spe-cial needs, comfort in working withchildren who have special needs,and experiences in providing inclu-sive care. This feature derives inpart from the desire to follow childcare professionals who were par-ticipants in an earlier study of at-titudes conducted by SpeciaLink in1990-91, and who were likely tohave been involved in providinginclusive care at that time.
We also obtained information fromcentre directors as to whether theyperceived their centre as having be-come more inclusive or more effec-tive in including children with spe-cial needs in the last few years, andwhat they perceive to have beenboth facilitators and limiting or re-stricting factors for their program.In addition, we asked centre direc-tors about specific cuts or changesin provincial policies that had oc-curred in the past year that theyperceived to have had adverse ef-fects on their centre’s capacities tobe inclusive. These questions wereasked in part to obtain participants’perceptions and reports of their ownexperience, and in part to developan understanding of how variousexperiences and influences mayhave shaped their current attitudes.
A third feature of this study is theincorporation of comparative datapoints that can aid interpretation.Fortuitously, one of the principalinvestigators on the research teamfor this study was also involved asa principal investigator on the na-tional You Bet I Care! study ofwages, working conditions and cen-tre practices. That connection en-abled the YBIC! study team to in-clude questions about the extentof inclusion of children with spe-cial needs, and other relatedquestions, in their national study.As a result, we have been able toinclude several data points thatallow some comparisons and abroader interpretation of studyfindings than would otherwise havebeen possible.
Finally, we believe another impor-tant feature of the study is its obvi-ous policy relevance. We look for-ward to seeing discussions andconcrete actions being taken as aresult of the study.
1.7 A “MATTER OF LANGUAGE”
In this study, we follow most majordisability organizations in our useof language. We speak about a childwith special needs, not about a spe-cial needs child — putting the childfirst. The words themselves are im-portant too. “Challenged,” as in“physically challenged,” seems to bethe current choice of word to replace“disabled” or “handicapped” or “im-paired.” We follow that usage, aswell, except when we are quoting arespondent or another author.
We also follow most major disabil-ity organizations in using thephrase “full inclusion” to mean“programs that encourage and ap-propriately support the enrollmentof children with special needs,
In broad terms,the main goal ofthis study was todevelop an in-depth under-standing of theecology of inclu-sive child care inCanada, and touse that knowl-edge to promotemore effectiveinclusion on adaily basis.

11INTRODUCTION AND BACKGROUNDCHAPTER 1
regardless of level or type of dis-ability or disorder.” Throughout thedocument, we use the word “inclu-sion” (or inclusive) to refer to pro-grams that identify themselves asincluding some children with spe-cial needs — “inclusive” replaces“integrated” or “mainstream” in thiscontext.
1.8 DEFINING “CHILDREN WITHSPECIAL NEEDS” FOR THECURRENT STUDY
The question “How do you define‘children with special needs’?” isextremely complex. Answers mightrange from “a child who has aphysical, intellectual, emotional,communicative or behavioural im-pairment, and who, in theminister’s opinion, requires addi-tional support services because ofthat impairment” (British Colum-bia)13 to the very restrictive defini-tion of a child with special needsas “A child who has a physical ormental impairment that is likely tocontinue for a prolonged period oftime and who as a result thereof islimited in activities pertaining tonormal living as verified by objec-tive psychological or medical find-ings and includes children with adevelopmental handicap” (OntarioDay Nurseries Act).14
That said, as researchers we werefaced with a need to develop“boundaries” in our definition —boundaries that would make theresearch possible. Different prov-inces use different definitions of“children with special needs” for theallocation of funding and additionalsupport. Some provinces require adiagnostic label before they deema child eligible for “special needsfunding.” Some query “activity limi-tation,” which parents often finddifficult to assess.
Since this study is about child careand about caregivers’ attitudes inchild care settings, when we say“children with special needs” we aretalking about “children with spe-cial needs in child care settings.”Further, we are talking about “chil-dren with special needs” for whomsome level of additional funding,consultative support, and/or re-source support is provided. Thus,for the purposes of this study, weprovided the following definition:
“Children with special needs” are“Children whose disabilities/disor-ders/health impairments meetyour province’s eligibility criteria foradditional support or funding inchild care settings. In areas withno additional support or funding,this term refers to children with anidentified physical or intellectualdisability that would be classifiedas moderate to severe. This defini-tion does not include children usu-ally described as being at high risk,who have not actually been identi-fied as having a significant disabil-ity or delay — even though suchchildren may require curriculummodifications and/or additional at-tention. Depending on your prov-ince/region, a child with significantemotional and/or behaviouralproblems may be classified eitheras a child with special needs or asa child at risk.”
This definition leaves out manychildren — children as yet uniden-tified, children on waiting lists forassessment, children whose dis-abilities or disorders do not fitwithin a province’s definition of“special needs,” and children atrisk because of environmental fac-tors. But this definition does reflectthe reality of a provincially-directedchild care system, one that isfraught with contradictions. It also

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada12
makes the research possible, be-cause it eliminates the subjectivitythat would result from asking the di-
rectors individually to define thechildren with special needs in theircentres.
END NOTES
1 Irwin, S.H. & DeRoche, J. (1992). Attitudes of Canadian mainstream child care staff towardinclusion of children with special needs. (Unpublished manuscript.)
2 For explanation about sample augmentation, see Chapter 4: Methodology.
3 Canadian Coalition on the Rights of Children (1999). The UN convention on the rights of thechild: How does Canada measure up? ON: Canadian Institute for Child Health.
4 Goss-Gilroy, Inc. (1996, Nov.). Component D: Curriculum analysis. Child care sector study:Technical Appendices (draft). (Unpublished report prepared for the Child Care Sector SteeringCommittee.)
5 Doherty, G., Lero, D.S., Goelman, H., LaGrange, A. & Tougas, J. (2000). You Bet I Care! ACanada-wide study on wages, working conditions and practices in child care centres. Guelph:University of Guelph (Centre for Families, Work and Well-Being).
6 Odom, S.L., Peck, C.A., Hanson, M., Beckman, P.J., Kaiser, A.P., Lieber, J., Brown, W.H., Horn,E.M. & Schwartz, I.S. (1996). Inclusion at the preschool level: An ecological systems analysis. InInclusion of young children with disabilities. MI: Society for Research in Child Development, SocialPolicy Report, 10(2&3), 18-30.
7 Kontos, S., Moore, D. & Giorgetti, K. (1998). The ecology of inclusion. Topics in Early ChildhoodEducation, 18(1), 38-47.
8 Irwin, S.H. (1993). The SpeciaLink book. NS: Breton Books.
9 Division of Early Childhood (1993). DEC Position on Inclusion. Pittsburgh, PA: Author.
10 Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design.Cambridge: Harvard University Press.
11 Odom, S.L., et al. (1996).
12 Peck, C.A. (1993). Ecological perspectives on implementation of integrated early childhood pro-grams. In C.A. Peck, S.L. Odom, & D.D. Bricker, (eds.), Integrating young children with disabilitiesinto community programs: Ecological perspectives on research and implementation, 3-15. Balti-more: Paul H. Brookes.
13 British Columbia Ministry for Children & Families (1996). Practice guidelines and proceduresfor supported child care (B.C. Benefits [Child Care] Act, section 1). BC: Author.
14 Ontario Legislative Assembly. The Day Nurseries Act. Revised Statutes of Ontario, 1990 (reprinted1998). Amended by the Services Improvement Act, effective January 1, 1998. Ontario LegislativeAssembly, Ontario Regulation 262, 1990. (Amended 1998, 1999).
CURRENT UNDERSTANDINGSCHAPTER 2 13
CURRENT
UNDERSTANDINGS
2.1 THE PREVALENCE OFSPECIAL NEEDS ANDCHRONIC HEALTHCONDITIONS IN CANADIANCHILDREN
Defining and estimating the num-ber of children in Canada with spe-cial needs is a complex problem,and these difficulties pervade allthe existing studies. Yet, becausechildren with special needs (includ-ing those with severe/profoundspecial needs) are much less fre-quently institutionalized than pre-viously, and now expect to partici-pate in all community activities, itis critical that policy makers haveaccurate data upon which to planand budget.
Within these limitations, there arethree national Canadian datasources from which estimates canbe derived: The National PopulationHealth Survey (NPHS, 1996-97);Canada’s Health and Activity Limi-tation Survey (HALS, 1991); andThe National Child Care Survey(NCCS, 1998). A fourth datasource, the National LongitudinalSurvey of Children and Youth(NLSCY) has not yet released itsestimates.
According to the 1996-97 NationalPopulation Health Survey (NPHS),there were approximately 169,537
(10%) male and 80,393 (5%)1 femalechildren between 0 and 9 years ofage, living in households, who hadspecial needs. For a child to be con-sidered to have a disability, the re-spondent (usually a parent) an-swered “yes” to the following (spo-ken) question: “Because of a long-term physical or mental conditionor a health problem, is/(your child)limited in the kind or amount ofactivity you/he/she can do?”2
Canada’s Health and ActivityLimitation Survey (HALS, 1991),which informs The Health ofCanada’s Children: A CICH Profile#3, as well as of a great deal of pro-vincial and federal planning,counts as a “child with a health oractivity limitation” one whoseparent reports that the child:
✦ has difficulty hearing, speakingor seeing;
✦ has a chronic condition such asdiabetes or muscular dystrophy;
✦ uses technical aids, such ascrutches, hearing aids, braces (ex-cluding braces for teeth);
✦ has a long-term condition orhealth problem that prevented orlimited participation in school, atplay or in any other activity consi-dered normal for a child his or herage;
2.Sharon Hope Irwin, Donna S. Lero, Kathleen Brophy

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada14
✦ attends a special school or inspecial classes;
✦ has a long-term emotional, psy-chological, nervous or mentalhealth condition; or
✦ has any other generallimitation.3
According to the 1991 Health andActivity Limitations Survey, 5.0% ofmale and 4.0% of female children0-4 years of age and 8.8% of maleand 5.8% of female children 5-9years of age have special needs.
Another national data source is the1988 National Child Care Survey(NCCS).4 According to the NCCS,about 241,000 families with at leastone child under 13 years of age(roughly 8.8%) have a child with along-term condition or health prob-lem. In 68,000 families, parents re-ported that their child’s conditionor health limited the kind of workthey were able to do or the hoursparents could work. About 77,200families reported that their child’scondition limited the child care op-tions that would otherwise be avail-able for that child, and 38,000 par-ents noted that their child’s condi-tion or health problem limited thechild care options they could con-sider for other children in the family.
We mention these three datasources because they are the bestavailable, but also to highlight theinadequacy of surveys such as theNPHS to fully identify disability fig-ures. The Roeher Institute estimatesthat an additional 145,000 children(ages 0-19) and youth could be“found” in the NPHS data if morevariables were examined. It alsohighlights the difficulties of lookingat “inclusion” strictly through amedicalized prevalence framework.The collection and analysis of ac-curate and timely data is essential,
because these are the figures uponwhich policies are developed andbudgets are built, and the HALS andNPHS questions are also the onesthat federal and provincial govern-ments use in establishing eligibilityfor certain services and funding.
Elements of the HALS definitionneed updating. For example, “atten-dance at a special school or in spe-cial classes” is not the determinantthat it once was because most prov-inces/territories have eliminatedspecial schools and many specialclasses. While this does not lowerthe prevalence of disability, it dis-torts the estimates. In March 2000,Statistics Canada announced thatit will carry out a new Health andActivity Limitation Survey that willinclude better, focused questionsregarding very young children.
Even if the prevalence figures wereaccurate, we would still have diffi-culty estimating the required spacesfor children with special needs inCanadian child care. Governmentpolicy often distorts the numbersand hides the problem. On the onehand, it is likely that children withspecial needs would be over-repre-sented in child care (unless they areconsciously excluded) because theirdevelopmental needs give them en-titlement in some provinces. On theother hand, it is likely that childrenwith special needs would be under-represented in child care, becausetheir mothers are more likely to beexcluded from the labour force, andmany provinces tie subsidies to pa-rental employment.
2.2 INCLUSIVE CHILD CARE:OPPORTUNITIES TO SUPPORTCHILD DEVELOPMENT ANDFAMILY WELL-BEING
“Accessible, high quality childcare is an enabler, a conduit for

CURRENT UNDERSTANDINGSCHAPTER 2 15
positive outcomes. The absenceof an effective child care systemis a major deficit in Canada’sinfrastrucure, adversely affectingour economic performance andhuman resources, now and inthe future. Child care’s place atthe centre of an array of socialpolicy objectives — healthy childdevelopment, parental job train-ing, learning and employment,women’s equality and healthycommunities — suggests that apolicy framework that legitimizeschild care would be an astutepublic investment.”
Friendly & Oloman5
Each component of this mix hasbecome more critical to familiesand to society as Canada hasmoved through the 1990s and intothe first decade of the 21st century.
Child care has long been at the cen-tre of the feminist movement’s drivefor women’s equality. Child careadvocates and feminists have rec-ognized that inadequate access toappropriate, high quality child carecreates a major barrier to women’sopportunities. In Canada, TheRoyal Commission on the Status ofWomen in 1970 was one of the firstofficial documents to recognize theimportance of child care forwomen’s equality and to call fornational child care legislation(Friendly, 1994).6 Yet, as JudyRebick (2000)7 tells us in 2000,“Thirty years after the publicationof the report of the Royal Commis-sion on the Status of Women, whichdescribed child care as a criticalsupport for women’s equality, youlook at the Report, compare it totoday’s reality, and see that noprogress has been made on childcare.”
Family economic well-being in-
creasingly depends on the wagesof both parents in two-parent fami-lies and, obviously, on the wagesof lone parents in lone-parent fami-lies. As Hertzman demonstrates(1998),8 one of the most importantdeterminants of health is secureattachment to the labour marketin well-paid, meaningful employ-ment. Parents with jobs, especiallygood jobs, tend to be healthier, asdo their children. Canadian wages,in general, have not increased dur-ing the past decade.
According to the Vanier Institute ofthe Family,9 “Non-indexation of theminimum wage has meant that italone can no longer keep a familyout of poverty. In addition, therapidity of changes in employmentpatterns has meant that incomesecurity is increasingly the task ofboth parents, not just the father.”
The National Council of Welfare,10
which usually promotes incometransfers for the poor to raise thevery low subsistence allowances ofprovincial welfare plans, has ar-gued for a service expenditure inthis case, saying that “The federal,provincial and territorial govern-ments must create a national sys-tem of child care and early child-hood education. Parents cannotparticipate fully in the labour mar-ket unless they find high-qualitychild care that they can afford.”
Another important aspect of highquality, affordable, accessible childcare is its contribution to healthycommunities. In this context, thephrase “healthy communities” re-fers to outcomes — the result ofpolicies, activities, and servicesthat help citizens of varied social,economic, linguistic and ethnicgroups live harmoniously together.Healthy communities have longbeen a justification for universal

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada16
socioeconomic lines...Head Starttracks economically disadvantagedchildren into separate programs inthe same way that low-achievingchildren and adolescents are oftensegregated in ‘dumb’ classes inelementary and high school. Whilewe show great concern for the del-eterious effects of stigmatizingschool-aged children, we ignore thestigma that results from participa-tion in a program for economicallydisadvantaged children. Thepresent policy not only contributesto the segregation of children alongethnic and social-class lines butdenies middle-class and disadvan-taged children, as well as the chil-dren from different ethnic groups,opportunities to learn from eachother (emphasis, authors). All chil-dren, especially those who other-wise have few opportunities to in-teract with children of differentraces and cultural backgrounds,can gain from preschool experiencethat exposes them to greater cul-tural diversity.”13
McCain and Mustard,14 in TheEarly Years: Reversing the RealBrain Drain, say: “it (early child-hood develpment and care) worksbest within a system available toeveryone,” and “parents across thesocioeconomic spectrum could useadvice and support in enhancingtheir parenting skills.” They fur-ther state: “Early child developmentand parenting initiatives must in-clude all children, including thoseliving with special difficulties andchallenges.” As to the issue of tar-geting, they say “We heard that allfamilies need non-parental care fortheir young children. Some needregular full-time or part-time carearrangements, while others needoccasional respite care. Even thecommunity meeting with parentsand grandparents who were not
public education. It’s not too hardto imagine an argument, 150 yearsago, proposing targeted publicfunding of education only for thepoor, in order that they gain suffi-cient skills and appropriate habitsto work in the factories and on thefarms of the country. It’s also notdifficult to imagine a counter-ar-gument that public funding of uni-versal education would be an in-strument for enlarging the socialsphere in which all economicclasses would learn together andlearn to live together.
Another example comes from theUnited States when, in the middleof the Great Depression, U.S. Sec-retary of Welfare Wilbur Cohen in-troduced a social security programfor all Americans. Many peoplewondered why that income shouldnot be means-tested. At such atime, they asked, wouldn’t it bebetter to designate money only tovery poor people who desperatelyneeded the money? Cohen an-swered, “Programs for the poorquickly become poor programs.”11
In a similar vein, Linda McQuaigin her book, The Wealthy Banker’sWife, says, “The reason targetedprograms don’t work, according tomany analysts, is that it is difficultto maintain political supportamong the population for programsthat benefit a small portion of so-ciety. On the other hand, if taxpay-ers feel that a program offers im-portant benefits for themselves andtheir family members, they aremuch more willing to support it —even pay high taxes to maintain it.”12
Even Edward Zigler, the father ofthe U.S. Head Start program forpoor children, is convinced thatsegregated programs for the poorare bad public policy. “(Head Start)...serves to segregate children along

CURRENT UNDERSTANDINGSCHAPTER 2 17
employed full-time outside thehome identified that full-time highquality child care arrangementsshould be available for parents whowant it for their children. But par-ents do not want to choose betweenearly childhood development andchild care. They would prefer earlychild development centres that in-clude non-parental care.”
While the three arguments ofwomen’s equality, family economicwell-being and healthy communi-ties are important, perhaps themost important argument for asubstantial public investment inearly childhood care and educationis based on healthy child develop-ment.
As McCain and Mustard state inThe Early Years: Reversing the RealBrain Drain, “Brain development inthe period from conception to sixyears sets a base for learning,behaviour and health over the lifecycle. Ensuring that all our futurecitizens are able to develop their fullpotential has to be a high priorityfor everyone. It is critical if we areto reverse ‘the real brain drain’....A society that wants to have ahighly competent population for thefuture to cope with the demands ofthe emerging knowledge-basedworld and global economy will haveto ensure that all its children havethe best stimulation and nourish-ment during the critical early yearsof development, regardless of fam-ily circumstances.... Investments inthe early period of life are as im-portant as investments in educa-tion, post secondary education andhealth care.”
If these four arguments — women’sequality, family economic well-be-ing, healthy communities, andhealthy child development — arevalid for all children and families,
they are especially important forchildren with special needs andtheir families.
The Women’s Equality argumentand children with special needs:
If all women with young childrenneed the opportunity to use highquality, affordable, accessible childcare for their children, mothers ofchildren with special needs need iteven more. They are more likely toface family breakdown; they havemore difficulty finding, keeping andpaying for appropriate child care;and many mothers in two-parentfamilies with one parent unem-ployed report that their child’s spe-cial needs are a major factor in theirunemployment.15 Moreover, recog-nizing that care of their childrenmay be a lifelong commitment, theyalso speak about their need foremployment as an issue of personalidentity and as respite from the iso-lation and challenges of caring fora child with additional needs. A1993 presentation to the Parlia-mentary Task Force on Social Se-curity Reform16 noted that, withoutspecial measures to assist withchild care and flexible employmentsupports, mothers of children withspecial needs were likely to consti-tute a ghetto within a ghetto ofunemployed, able-bodied workers.
The Family Economic Well-Beingargument and children withspecial needs
If most families with typically de-veloping children need two incomesto maintain a comfortable standardof living, this is often even moretrue for families with a child with adisability. Even without countingthe substantial “opportunity costs”lost by a parent (usually themother) leaving the labour force oraccepting fewer hours of work or a

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada18
lesser skilled job17 because of thedifficulties of finding and obtain-ing appropriate services for achild with a disability, they havemany costs which are disability-specific and which are involun-tary.18 Although the income taxsystem contains provisions to off-set some costs of disability, it doesnot begin to provide the tax fair-ness that would establish equitybetween families at the same levelof income which include a childwith a disability and those whichdo not. Moreover, the lack of bothsuitable, affordable child care andemployment provisions which rec-ognize the needs of parents ofchildren with special needs totake time off for medical andtherapeutic appointments as wellas for educational placementmeetings, etc., often makes em-ployment impossible for thecaregiving parent.19 As one par-ent at the 1993 Social SecurityReform hearings said:20 “It’s notthe disability that bothers me —it’s the poverty that I face becauseno systems are in place to permitme to work.”
The Healthy Communitiesargument and children withspecial needs
We live in an increasingly diverse,multi-cultural Canadian commu-nity, as well as in a global one.The early years provide the besttime for young children to learnto respect and enjoy differences,as well as similarities, of culture,language, gender, ability, etc.Thus, on a child-to-child level, theinclusive child care setting canhelp typically developing childrento appreciate the gifts and chal-lenges of their peers with specialneeds. Such experiences may gen-eralize to appreciation of other
differences as well. Anecdotal ex-periences indicate that qualitiesof empathy, sympathy, and car-ing expand when very young chil-dren have opportunities to playand learn with children of differ-ing abilities. When they go intoschool, such friendships oftencontinue, providing natural peersupports to children with specialneeds. Some parents, recognizingthe value of exposure to diversity,look for child care centres that in-tentionally include children fromdiverse backgrounds and childrenwith disabilities.21
The Healthy Child Develop-ment argument and childrenwith special needs
The research literature on thevalue of high quality inclusivechild care for children with spe-cial needs, as well as for typicallydeveloping children, is robust.22
According to Strain (1988),23 thereis no evidence that such programsare detrimental to typically devel-oping children and there is ampleevidence of the benefits to chil-dren with special needs. Hundert(1994)24 demonstrates, in a south-ern Ontario study, that childrenwith severe disabilities showgreater gains both cognitively andsocially in inclusive settings, com-pared to progress in segregatedsettings, even where the ratios ofstaff-to-child were higher andwhere more intensive interven-tions were used. Inclusive settingsmust, of course, provide addi-tional staffing, training, resourcesand supports to make the pro-grams work for all children.
In the famous Brown versus theBoard of Education (1954) deci-sion of the Supreme Court of theUnited States, Justice Marshallsaid, in a unanimous decision:

CURRENT UNDERSTANDINGSCHAPTER 2 19
“Does segregation of childrenin public schools solely on thebasis of race, even though thephysical facilities and other‘tangible’ factors may be equal,deprive the children of the mi-nority group of equal educa-tional opportunities? We be-lieve that it does...We concludethat...separate educational fa-cilities are inherentlyunequal....(They) generate afeeling of inferiority as to theirstatus in the community thatmay affect their hearts andminds in a way unlikely everto be undone.”25
This case has had a tremendousinfluence on other disadvantagedgroups, notably people with dis-abilities and their advocates, wholater argued that segregatedschools and institutions hadsimilarly negative effects on per-sons with disabilities.
An Appendix to the Appellants’Brief, prepared by Dr. KennethClark, a renowned Black psy-
chologist and others, contained asection on the impact of racismand segregation on children of themajority group. It states:
“Those children who learn theprejudice of our society are alsobeing taught to gain personalstatus in an unrealistic andnonadaptive way. The culturepermits and at times encour-ages them to direct their feel-ings of hostility and aggressionagainst whole groups of peopleperceived as weaker thanthemselves. Confusion, con-flict, moral cynicism and dis-respect for authority mayarise.”26
Regardless of the level or type ofdisability, healthy child develop-ment requires opportunities to par-ticipate in inclusive community-based early childhood programs. Aframework for such programs, de-scribed below in Figure 2.1, is es-sentially self-evident. It begins withthe premise that all children andfamilies require basic services, to
Figure 2.1
Inclusive Early ChildhoodDevelopment Services (ECD)
Adapted from: McCuaig, K.and Friendly, M. (1999)The Early Childhood Triangle
earlychild-hood
educa-tion
childcare
supportfor
parenting

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada20
some degree or another, of earlychildhood education, child care,and support for parenting. Selectedcommunities require additionalservices because of factors such asa high proportion of immigrants orrefugees, poverty, and other riskfactors. Finally, some individualchildren, including those identifiedas having special needs, mayrequire highly intensive services.
The United States, almost neverseen as progressive in its socialpolicies, now recognizes in law theimportance of participation by eli-gible children with special needs(ages 3-21) in “free and appropriateprograms (FRAP)” in “the least re-strictive environment (LRE),”27 andprohibits their exclusion from bothcentre-based and family daycarethrough the Americans with Dis-abilities Act (ADA),28 Canada con-tinues to rely on voluntarism andon a permissive approach to theissue of inclusion.
2.3 THE EVOLUTION OFINCLUSIVE CHILD CARE INCANADA
The evolution of inclusive child carein Canada has many parallels tothe evolution in public education.Both “systems” began with exclu-sion, moved to the development ofa segregated “special education” or“developmental program” track,moved to a resource room/pull-outmodel of integration, and thenmoved toward a model in which allchildren, regardless of ability/dis-ability, were educated within thesame classrooms. The drivingforces for both systems were thesame: the human rights movementand a growing belief that childrenof diverse abilities and culturescould benefit from being together.The current issues regarding inclu-
sion of children with special needsare also similar — lack of stafftraining, lack of appropriate re-sources and support, and most ofall — attitude.
There are, however, areas of evolu-tion toward inclusion that are notparallel in education and childcare. “Education” is a universalsystem, and since the proclamationof the Canadian Charter of Rightsand Freedoms, all age-eligible stu-dents must (by law) be accommo-dated within provincial educationsystems.29 As late as 1979,only three provinces — PrinceEdward Island, Nova Scotia, andSaskatchewan — had legislationstating that school boards mustprovide educational services to theexceptional student.30 The rights ofstudents with special needs to at-tend inclusive classrooms was ad-dressed by the Supreme Court ofCanada in the Eaton case, and thedecision, though not what disabil-ity advocates had hoped for, putsthe onus on school boards to jus-tify placement decisions that goagainst parental/student wishes.31
Child care, on the other hand, isnot a universal system. Child carecentres in Canada can develop ad-missions policies that specificallyexclude children with specialneeds. Neither the Charter of Rightsand Freedoms nor provincial hu-man rights legislation speaks abouta “right” to child care — not justfor children with special needs, butfor any children. Moreover, mixedpublic/private funding for childcare and mixed public/private aus-pices contribute to child care’schronic under-funding. The issueof “base quality” — of whether thequality of much child care is ad-equate for any child, but especiallyfor a child with complex needs —

CURRENT UNDERSTANDINGSCHAPTER 2 21
bedevils the efforts of inclusionadvocates.32
The 1950s and Before: Until the1960s, the care of children withspecial needs was usually seen asa family issue. The overarchingtheme was essentially “hopeless-ness” or “God’s special child” — andit was assumed that children withintellectual challenges couldn’tlearn and that children with physi-cal challenges would die young.Upon the birth of a child with spe-cial needs, families usually had twochoices: institutionalize the child(“It’s better for him,” or “He’ll behappier with his own kind,” theexperts would say) or take on thetotal task of raising the child athome without formal supports.Most provinces excluded manychildren with special needs fromschools and, of course, child carewas in its infancy.
Two important events — one ofrights and the other of hope — pro-pelled the growth of advocacy re-lated to children with special needs.
The “rights” discussion followed theU.S. Supreme Court 1954 decisionin Brown vs. Board of Educationwhich stated that “Segregation isinherently unequal.”33
The “hope” discussion followed thebehaviourists, who demonstratedthat everybody could learn if taskswere broken down into simplepieces, repeated many times, andrewarded for success. The newtechniques gave parents a feelingthat their children could learn.
In addition, the increasing use andsophistication of antibiotics meantthat children with physical specialneeds, who might have died soonafter birth, were living longer. Aswell, assistive technology and min-iaturization would offer mobility
and communicative possibilitieswhere none had existed before.
The 1960s and ’70s — Special-ized Pre-schools: The 1960s was adecade of hope for parents ofchildren marginalized by disabilityand/or by poverty. The be-haviourists (notably Skinner) haddemonstrated that there was aneffective way to teach anybodyanything. Their techniques ofbehaviour modification were incor-porated into training programs andinto methods of teaching peoplewith intellectual challenges. “Taskanalysis,” “mastery learning,” and“rewards” became the hopeful mo-tifs of the institutions where manypeople with intellectual challengeslived. Psychologists and disabilityspecialists designed many special-ized teaching methods and cur-ricula.
A system of developmental part-daypreschools was established for chil-dren with special needs, with en-couragement from the specialists.Driven by parents of children ex-cluded from the regular preschools,a strong system of Canadian Asso-ciation for the Mentally Retarded(CAMR, now CACL) nursery schoolsand Child Development Centre pre-schools (CDCs) for children withphysical special needs developedacross Canada. These programswere characterized by specializa-tion and segregation, by strongparent involvement (particularlythe CAMR programs), often sup-plied transportation, and were freefor eligible children (although par-ents were often involved in fund-raising). There were few, if any, full-day child care programs for chil-dren with special needs.
Through the 1960s and early ’70s,“regular” Canadian child care wasstill characterized by a distinction

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada22
between daycare centres and pre-schools/nursery schools. Mostchild care centres were seen ascustodial environments for thechildren of the working poor. Theyprovided a safe environment, nu-tritious meals, and adequate care.Nobody expected them to be muchmore. For middle class parents, onthe other hand, the preschool/nursery school was the choice for3- and 4-year olds. The child at-tended a social/developmentalprogram for two hours a morningor afternoon, and spent the restof the day with his/her mother orhousekeeper. Some targeted pre-school programs were funded inlow income neighbourhoods inCanada, based on the curriculumcomponent of U.S. Head Start, al-though not including the nutrition,parent support, and health ele-ments.
By the end of the ’70s, some pro-gressive child care centres wereenrolling children with specialneeds — often without legislation,core funding, training, or sup-port.34 Federal grant fundingthrough such programs as the Lo-cal Initiatives Program (LIP) andCanada Works were often crucialto these initiatives. These pioneersat child care inclusion became acadre offering skill enhancement,advocacy for changes in publicpolicy, and support for other cen-tres in their regions.
During this same period, publiceducation for children with spe-cial needs was extremely limited.School-age children with specialneeds often attended “specialschools” and residential institu-tions. Public education systemsstill did not have to admit chil-dren whom they considered“uneducable” or “not trainable.”35
1980s — The TransitionalDecade: With growing participa-tion of mothers of young childrenin the workforce, the need for asetting that expanded the length ofthe part-time preschool/nurseryschool day became obvious. Somepreschools added a “bridge” pro-gram at lunchtime between theirmorning program and their after-noon program to accommodatechildren of working parents. Somealso added “wrap-around” pro-grams, before 9:00 a.m. and after3:00 p.m. In addition, the tradi-tional daycare centres that hadbeen seen as primarily custodialsettings for low-income parentsbegan to expand their developmen-tal or educational components —and to include more and moremiddle class children of employedmothers.
Almost inadvertently, people real-ized that among the working moth-ers were mothers of children withspecial needs. Special needs wasnot part of the planning of any gov-ernment in Canada as they beganto develop child care legislation.
Although many more families ac-tually used non-licensed out-of-home care or care-by-relative, itcan be argued that the licensed,group child care setting “character-ized” the period as the locus inwhich new activity and policy de-velopment were taking place. Qual-ity measures were developed; train-ing programs and qualificationswere strengthened; provincial leg-islation began to reflect awarenessthat child care needed to meanmore than “safe and fed.” And justas middle-income parents werepressing the system to providehigher quality experiences, so didparents of children with specialneeds require child care too. Par-ents of children with special needs

CURRENT UNDERSTANDINGSCHAPTER 2 23
were in the workforce in greaterand greater numbers. But theyalso, individually and as part ofadvocacy groups such as CACL,were looking for “normalized” or“least restrictive placements” fortheir children with special needs —placements such as child care.
The Canadian Association for theMentally Retarded (CAMR) nurseryschools began to change form andfunction — first by turning into “re-verse integration” settings, wherethe totally segregated setting be-came one involving 50% typicallydeveloping children (usually apopulation composed of brothersand sisters, and neighbours) and50% children with intellectual spe-cial needs; then into a support andconsultation role for regular childcare programs, as their childrenmoved into those settings.
The Child Development Centre(CDC) preschools, which primarilyserved children with physical dis-abilities, changed more slowly.These were often connected to re-habilitation centres or hospitals,with therapists on site, and oftenincorporated more accessiblephysical design features. Theseprograms were more resistant to in-clusion. Therapies were consideredmore difficult to deliver in regularchild care. Basements, churchhalls, and other “found spaces”characteristic of daycare could noteasily accommodate children inwheelchairs and braces.
At the end of the 1980s, integratedchild care for a child with a physi-cal disability would often be char-acterized by a chopped-up day. Forexample, the child with specialneeds would go to a regular childcare setting when his mother leftfor work, be picked up in the CDCvan at 8:30, go to a two-hour thera-
peutic program for the morning,then be taken by van back to thechild care setting for the afternoon.Coordination between the two pro-grams would range from non-exis-tent to full coordination. But be-tween dressing for outdoors, wait-ing for the van, riding in the van,waiting to be undressed for in-doors, being dressed again for theride back, waiting for the ride,riding in the van, being undressedagain for indoors, an enormousamount of very passive time oc-curred.36
By the end of the 1980s, despitethe lack of legislated entitlement,Canadian child care programs wereenrolling more children with spe-cial needs, in programs increas-ingly inclusive.37 Modest financialincentives, additional training,strong parental advocacy, and agrowing awareness of the benefitsof inclusion encouraged thischange.
Schools, too, changed during thisdecade. Many of the “specialschools” were closed, and studentswith special needs were broughtinto segregated classrooms insidethe regular schools. They still rodeon the “handicapped bus”; theywere still segregated into specialclasses, but they were in the sameschool building. As time went by,many schools began to include all(or almost all) students in non-academic activities — often inhomeroom, gym, assembly, lunch,recess, art, and music. Academicsubjects were taught to childrenwith special needs through pull-outprograms in the resource room, akey characteristic of this period.Parents and advocates continuedto fight for full educational inclu-sion, but the Courts ruled againstthem.38

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada24
From 1990 to mid decade —policy and practice: Legislationand policy were beginning to catchup with the models of inclusive childcare across Canada. Many provinces(British Columbia, Saskatchewan,Ontario, New Brunswick, NovaScotia, Prince Edward Island) wererewriting their child care legislation,as it related to children with specialneeds. The dominant feature of thenew legislation was some attempt tosupport children with special needsin regular child care settings, ratherthan to support a separate, segre-gated track.
British Columbia conducted a no-table special needs review.39 Re-leased in Autumn 1994, it includeda plan to move toward supportedchild care for all children. Withcareful respect for local historiesand local strengths and needs, therecommendations raised thebaseline of social policy in Canadaas it relates to preschool childrenwith special needs.
On the other hand, Ontario’s strongmove toward a policy of family-cen-tered, inclusive child care wasslowed, if not halted, by thatgovernment’s decision not to con-tinue Child Care Reform in areaswhere new dollars were required.40
Nova Scotia’s draft regulations41
used the language of inclusion, andwould move provincial child carelegislation away from an add-onmodel of addressing special needstoward one that encourages fullparticipation in community-basedprograms. In addition, by 1993 NovaScotia had begun to support tenpercent of its new child care spaceswith “differential funding,” recogniz-ing that approximately ten percentof children will require additionalsupports to successfully participatein child care programs.42
New Brunswick’s new regulationsimproved provincial supports forchildren with special needs, butprovided less support to the regu-lar child care programs into whichthey would be integrated.43
Saskatchewan’s legislated changesspeak positively about “specialneeds,” but fiscally are very lim-ited.44
On the federal level, the discussiondocument on Social Security Re-form addressed issues of childrenwith special needs at several points,relating both to parental employ-ment and to healthy child develop-ment, but its recommendationsrelated to children with specialneeds were never implemented.45
Other federal programs of that pe-riod (e.g., Canada Assistance Plan,Dependent Care Allowance) thatimpact on child care did not evenmention “children with specialneeds.”
Despite the lack of legislated en-titlement, by mid 1990s Canadianchild care programs were includ-ing more children with specialneeds. Irrespective of provincial leg-islation, urban or rural status, orfunding, researchers found inno-vative inclusionary child care pro-grams in every province.46 Thequality as well as the quantity ofinclusion had increased in Canada.Both pre-service and in-servicetraining were being redirected froman emphasis on exceptionality to-ward strategies for inclusion. Thenumber of workshops on inclusionissues had increased significantly.Programs that had formerly in-cluded only children with mild tomoderate special needs were begin-ning to include children withtougher challenges. Partnershipsbetween child care staff and earlyintervention staffs had beenstrengthened in many settings.

CURRENT UNDERSTANDINGSCHAPTER 2 25
Collaborative efforts, such as teamplanning, transdisciplinary servicedelivery, and arena assessments,were becoming more prevalent.
From the perspective of inclusion,the early 1990s appears to havemarked the high point in Canadianchild care. Most provinces had ac-knowledged “child care” as a valu-able profession, although signifi-cant wage increases had not fol-lowed. Most provinces had ac-knowledged that “child care” hada significant role to play in the de-velopment and socialization of chil-dren with special needs. Voluntaryattendance of child care staff atconferences and workshops washigh and many staff were beginningto speak of their work as a profes-sion — not just a job to leave forbetter pay and working conditions.As well, surveys of centres seemedto suggest that the will to includechildren with special needs was in-creasing.47 Although no legislationhad passed, “child care” had beenan issue in the federal elections of1984, 1988, and 1993, and the RedBook promises on child care of thegoverning Liberals suggested thatbetter times were coming. The ini-tiation of an HRDC-funded SectorStudy on Child Care in 1995seemed to signal an acknowledg-ment by the federal governmentthat the child care workforce wassignificant in the overall picture ofCanadian employment.
2.4 APPRECIATING THE CONTEXTIN WHICH THE STUDY WASCONCEPTUALIZED ANDUNDERTAKEN, AND IN WHICHTHIS REPORT IS BEINGDISSEMINATED
When this study was conceptual-ized and initiated (1994-97), gov-ernments (federal as well as pro-
vincial/territorial) were consumedby their emphasis on debt, defi-cit, and devolution.
Indeed, the earlier optimism inthe child care community and itswillingness to volunteer for moretraining and to develop skills re-quired to include children withspecial needs had been, we think,contingent on the expectation ofbetter wages and working condi-tions, greater recognition and bet-ter support for centres. With theshift of federal emphasis in late1993 from promises of social re-form to an emphasis on debt, defi-cit, and developing a social unionframework — as well as with thedemise of the Canada AssistancePlan (CAP) and its replacement bythe smaller and less powerful suc-cessor, the Canada Health andSocial Transfer (CHST), the childcare community felt betrayed. TheLiberal Party’s Red Book (1993)promise of 150,000 new child carespaces had not been realized.Without CAP and with their owndebt/deficit/social union con-cerns, the provinces, too, slowedand then stopped their advancesin child care. “Children at risk”became a heightened federal/pro-vincial concern, and “childrenwith special needs”48 lost theirhigh profile at policy tables.
When this study was dissemi-nated (1999-2000) the fiscal sur-plus, rather than the earlier defi-cit and debt, was beginning toengage politicians, policy makers,and publics.
Approaching the millennium,families and providers were en-couraged by the announcement ofenhanced maternity/parentalbenefits, the possibility of a Na-tional Children’s Agenda, and byan increase in the National Child

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada26
Benefit and the ReinvestmentFund. On the other hand, they wereconcerned about the limitations ofthe enhanced maternity/parentalbenefits, the slowness of the NCAagreement and the likelihood thatit would not address employment-sensitive early childhood develop-ment services (i.e., child care), andthat the Reinvestment Fund cameat the expense of the poorest of thepoor.
Especially troubling, no children’sinitiative seemed to address “chil-dren with special needs” — andeven In Unison,49 a recent accordof the f/p/t governments (exceptQuébec), ignored young childrenand their families, focusing onadults and, perhaps, on teenagers.
At some level, all provinces and ter-ritories appreciate the need for in-clusive child care opportunities forchildren with special needs andhave developed some document orposition paper laying out their in-tentions to further address the is-sue. A special needs review(Saskatchewan); reorganization ofchild care and special needs ser-vices (Newfoundland, Ontario,Alberta, British Columbia) andamendments to child care legisla-tion (Nova Scotia) are currently inprogress (1999).
Many provinces seem to be wait-ing for federal leadership (or fund-ing) to so do; others are adding onan element (such as training), butin the absence of a universallyaccessible system of child care, theissues of equity, affordability, andaccessibility continue to haunt. Theimpending National Children’sAgenda and the Reinvestment Fundare seen by many provinces as po-tential vehicles through which toaddress inclusive child care.
2.5 THE EVOLUTION OF QUALITYCARE AS A CONCEPT THATENCOMPASSESINCLUSIVENESS ANDDIVERSITY — USINGASSESSMENT TOOLS AS ABENCHMARK
If “inclusiveness” and “diversity”are embedded in the concept of“quality” in early childhood careand education, we would expect tofind that assessment tools thatmeasure “quality” would reflecttheir presence. Thus, if a centremade no provisions or only verymodest provisions for the inclusionof children with disabilities, thatcentre could not be rated as meet-ing more than a minimal level ofquality, even if it excelled in everyother area. A similar statementcould be made about provision forchildren from diverse cultural andlinguistic backgrounds.
Comparing the 1980 EarlyChildhood Environment RatingScale (ECERS)50 with the 1998Early Childhood EnvironmentRating Scale Revised (ECERS-R)51
The ECERS, as it is usually called,was published in 1980 and hasprobably become the most fre-quently used instrument forassessing early childhood programquality. It uses a 7- point ratingscale, with “1” meaning “inad-equate” and “7” meaning “excel-lent.” There are seven areas of as-sessment, and a total of 43 items,each of which includes from one tofive indicators. Measures of both re-liability and validity of the 1980ECERS are high. Countless work-shops and training sessions, aswell as instructional videos andmanuals, have helped to keep in-ter-observer reliability quite high,despite the non-restricted use ofthe ECERS by people with a wide

CURRENT UNDERSTANDINGSCHAPTER 2 27
variety of qualifications. Because ofits wide use in research and itspopularity, we see it as a bench-mark tool for assessing “quality” inearly childhood education and care,while recognizing that major stud-ies of quality now use several otherindices along with this one. Manyprovinces now use the ECERS bothas a training tool and as a forma-tive measure of quality.
However, in the 1980 version of theECERS, there was only one itemthat mentioned “exceptional chil-dren.” In the Notes of Clarificationto #33, ECERS says, “Probes maybe needed, such as ‘Do you havechildren with handicaps or specialneeds?’ ‘How do you handle this?’‘Have you ever had such children?’‘What would you do if you had chil-dren with special needs?’”(p. 34)
The item itself ranges from “1”(Inadequate): “no provisions orplans for modifying the physical en-vironment, program, and schedulefor exceptional children; reluctanceto admit children with specialneeds” to “7” (Excellent): “Staffassess needs of children and makemodifications in environment, pro-gram, and schedule to meet thespecial needs of exceptional chil-dren” and “individually plannedprogram for exceptional childreninvolving parents and using profes-sionally trained person as consult-ant to guide assessment andplanning; referral to support ser-vices.” (p. 35). Inclusion, it is clear,was not seen as a critical compo-nent of quality in the ECERS of1980.
In 1998, the ECERS-R was pub-lished. In the introduction, the au-thors say, “During this time [since1980], inclusion of children withdisabilities and sensitivity to cul-tural diversity had become impor-
tant issues in the assessment ofprogram quality...”(p. 1). “In keep-ing with the suggestions of our fo-cus groups on inclusion and cul-tural diversity, we did not developseparate items but rather incorpo-rated indicators and examplesthroughout the scale” (p. 2).
In the ECERS-R, twelve items andfifteen indicators mention “childrenwith disabilities.” Generally speak-ing, the presence of a child with adisability currently in the programrequires some attention to rate a“3” on the item and often a morecomplex response to the child isrequired to rate a “5.” For mostitems related to “a child with a dis-ability” an N/A (not applicable) isto be written on the rating sheet ifno child with a disability is cur-rently present. Only in the itemreferring to “space and furnishings”does the “5” occur even when thereis no child with a disability cur-rently part of the program (“For ascore of 5, accessibility is requiredregardless of whether or not indi-viduals with disabilities are in-volved in the program,” p. 9). Inaddition, there is a whole sectioncalled “Provisions for children withdisabilities.” The Notes for Clarifi-cation state, “This item should beused only if a child with an identi-fied disability is included in theprogram. Otherwise, score thisitem N/A.” Fourteen indicators areincluded, ranging from four in “in-adequate” to three in “excellent.”The 3 indicators in “good” show thestaff following through on sugges-tions and goals set by outside pro-fessionals; the 3 indicators under“excellent” are inclusionary andcollaborative (p. 45).
These changes in ECERS between1980 and 1998 represent a majorchange in the instrument and evi-dence of the acceptance of the idea

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada28
that “quality” in child care encom-passes provisions that support andenhance inclusion and diversity.However, to many people involvedwith these issues, the ECERS-R,even with its changes, still does notadequately reflect the measuresneeded to assure that children withspecial needs and children fromnon-majority cultures and lan-guages are truly welcomed intochild care settings. To these advo-cates, high quality in child carewould require even more attentionto these areas. They would suggestthat there is more to inclusion thansimply responding if a child with adisability is currently present. Theywould say that such indicators asknowledge of common screeningand assessment tools, understand-ing of the rights of children withdisabilities to be present in childcare centres, experience with chil-dren with disabilities in group set-tings, and commitment to inclusionshould be present, even if a childwith a disability is not currentlyenrolled.
Early Childhood Special Educa-tion Program Design and De-velopment Guide (EC-SPEED)
In 1993, the Early Childhood Spe-cial Education Program Design andDevelopment Guide (EC-SPEED)was produced by Lynn G. Johnson,Paul McMillan, Paul A. Johnsonand Constance K. Rogers.52 Alongwith a set of eleven videos and acomprehensive bibliography re-lated to early childhood specialneeds, the EC-SPEED team devel-oped an assessment instrument foruse in early childhood settings.Their instrument, unlike ECERS,unapologetically addressed assess-ing “regular” group child care set-tings (including Head Start, nurs-ery schools, daycare) on the basisof their capacity to include children
with a full range of types and lev-els of disabilities. Developed origi-nally for use as a training tool inEarly Childhood Special Educationat the university level in the UnitedStates, the EC-SPEED instrumenthas been used widely for formativeassessment and for self-study, aswell as for course credit.
“Embedding” or “infusing” inclu-sion (then called “mainstreaming”)into every element of the instru-ment, a high score on the EC-SPEED (designed very much likethe ECERS) requires regular atten-tion to special needs issues. For ex-ample, in a fully inclusive centre,obvious accommodations will havebeen made for children with smallmuscle difficulties or for blind chil-dren — even in the way coathooksare designed and positioned. Whenwe asked one of the authors of EC-SPEED, in 1998, which indicatorshe thought were the most impor-tant, Lynn G. Johnson said,
“You could call it ‘ideological coher-ence,’” he said. “But I like to thinkabout it as centres where everybody— from the board of directors tothe cleaning staff — have boughtinto inclusion. We always visit thecook as well as the child care staff.At one of the best centres we vis-ited, the cook proudly told us howhe ground up food so that a childwith a swallowing problem couldeat with everybody else.”53
Unfortunately, for most programconsultants, trainers, and earlychildhood educators, the scoring ofEC-SPEED takes three full dayswith three trained observers tocomplete. However, its indicators,training manuals and its videosremain very helpful for under-standing the vision of full inclusion,and are useful for self-assessmentand planning. (The legal section is
“You could call it‘ideological coher-ence,’” he said.“But I like tothink about it ascentres whereeverybody — fromthe board of direc-tors to the clean-ing staff — havebought into inclu-sion. We alwaysvisit the cook aswell as the childcare staff. At oneof the best centreswe visited, thecook proudly toldus how he groundup food so that achild with a swal-lowing problemcould eat witheverybody else.”

CURRENT UNDERSTANDINGSCHAPTER 2 29
U.S.- based and is not relevant forCanada.)
DEC/NAEYC Statement onInclusion
Reflecting growing consensus inthe disability field about the ben-efits of inclusion, the Division ofEarly Childhood (DEC), Council forExceptional Children adopted itsPosition on Inclusion54 in 1993. In1994, the National Association forthe Education of Young Children(NAEYC), the largest early child-hood education organization in theUnited States, endorsed the DECstatement and revised its own defi-nition of program quality to includea greater emphasis on cultural di-versity, family concerns, and indi-vidual children’s needs(Bredekamp & Copple, 1997).55 Itis anticipated that changes toNAEYC’s Accreditation Programself-study guide and assessmentinstruments will follow. Thesechanges will promote attention toinclusion and diversity as criticalcomponents of pre-service trainingand of practice.
Reflecting Inclusion in Re-search: You Bet I Care!
In Canada, the You Bet I Care!project team56 utilized ECERS-R asa measure of process quality inchild care settings, but struck anad hoc task force on inclusionarypractices, as well as one on diver-sity to augment it. From theinclusionary practices group, theyadded five supplementary ques-tions related to enrollment of chil-dren with special needs to theirexisting questionnaire on wages,working conditions and practices;a four-item observational scale ofECERS-like items related to out-door physical environment/equip-ment, relationships with typically
developing children, communica-tion, and individualized programplanning; and twelve interviewquestions with the head teacher inthe room that had been observed.(A similar process was followedwith the diversity group, but thatis outside of our study). These ad-ditions to the ECERS-R make it, inthe opinion of the ad hoc task forceand of the principle investigatorsin YBIC!, a stronger indicator of theproper role of inclusionary prac-tices in Canadian child care.
2.6 THE CURRENT STATUS OFINCLUSION IN CANADIANCHILD CARE PROGRAMS
How many children with specialneeds are currently attending Ca-nadian child care programs? Howmany more would attend if centreswould admit them? Are there anysystemic areas of exclusion? Whatquality of experience are these chil-dren receiving? What sorts of sup-ports and resources are availableto the inclusive centres? What sortsof supports and resources wouldbe necessary to allow children withall levels and types of special needsto equitably participate?
While this study does not provideinformation about the current sta-tus of inclusion in nationally rep-resentative Canadian child carecentres, it does provide a templatefor looking at “typical centres”—when they have moved further to-wards inclusion. Researchers andadvocates have identified high staffturnover, limited education andtraining, limited experience at in-cluding children with specialneeds, and limited commitmentto inclusion, as reasons why vol-untary inclusion hasn’t movedvery far.57

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada30
By intention, our study looked at apurposive sample of “atypical cen-tres” — a group of over 130 cen-tres which had a rich history ofincluding children with specialneeds. We attempted to under-stand what was going on in someof the most committed, most expe-rienced, most knowledgeable staffsand centres in Canada regardinginclusion. Thus, all except five ofthe centres surveyed included chil-dren with special needs (or hadwithin the past year) and had beendoing so for most of the past sixyears or more. Similarly, we wouldexpect to find higher levels oftraining, experience, commitment,and reported competence atinclusionary practice in oursample.
If we turn to studies of a represen-tative sample of Canadian childcare centres that address the in-clusion issue, we find only You BetI Care ! (2000). According to YBIC!,“the percentage of centres whichhad no children with special needsranged from a low of 18.7% (MB)to 50% (NF).The proportion of cen-tres with three or more childrenwith special needs present washighest in Manitoba (45.2%),Ontario (45.9%) and Saskatchewan(49.5%). Specific initiatives to sup-port the inclusion of children withspecial needs exist in all three ofthese provinces. By auspice acrossCanada, 87.% of municipal centres(ON), 73.7% of non-profit centres,and 61.2% for-profit centres re-ported that they accommodatedchildren with some specialneeds.”58
According to Lero et al,59 whenasked about barriers to inclusion,about 40% of centre directors re-ported being unable to accept theapplication of at least one child
with special needs in the last threeyears. The most common reasonsfor not accepting children were: in-sufficient funds, building requiredmodifications, staff felt inad-equately trained, centre alreadyhad its maximum number of chil-dren with special needs. About 8%of the directors did not reply to thespecial needs questions, suggest-ing that the YBIC! figures are prob-ably slightly inflated for the posi-tive responses (including childrenwith special needs) and slightlydeflated for the negative ones (turn-ing away children with specialneeds). There is no way of knowingfrom the YBIC! data whether chil-dren with any particular healthcondition, disability or behaviourproblem are commonly excludedfrom representative child care pro-grams, although other researchclearly indicates that most oftenchildren with more severe problemsand those described as having ma-jor behaviour problems are ex-cluded. (See Chapter 3.)
It would probably be desirable to getcurrent provincial figures on thenumber of children with diagnosed,eligible special needs for whom ex-tra funding and/or support is pro-vided to child care centres, andcompare that to the estimated num-ber of children with special needsin the total population. In someprovinces, this data is available.However, the task of really under-standing who is served is compli-cated by such issues as “Is a ‘spe-cial needs space’ shared by two ormore children?”; “Do children withspecial needs attend for the full day,or only until noon or three o’clock?”As well, invisible children — thosewith special needs for whom no ex-tra funding and/or support is pro-vided — would be missed. But itcould be done, and should be done,

CURRENT UNDERSTANDINGSCHAPTER 2 31
if a reasonable benchmark of wherewe are is to exist. It is possible thatthe 2001 Health and Activity Limi-tations survey (HALS) will track thechild care question. Then, targetsof equitable access could be estab-lished, and progress could betracked. (It also appears that asurveillance project of the Centre ofExcellence for Children and Youthwith Disabilities might take on thisquestion.)
Early Childhood Care and Educationin Canada: Provinces and Territories199860 provides, province by prov-ince, a listing of the special needsgrants offered to child care centresfor the inclusion of children withspecial needs. Updated for 2000,61
these grants range from “none” inNewfoundland to $11.00/per hour(the average hourly wage of childcare workers in the facility for anextra staff person) in Manitoba anda maximum of $11.50/per hour foran extra staff person in Prince Ed-ward Island. This scan does not of-fer any indication of how long thewaiting list might be, or whetherchildren with certain special needsor health impairments are excluded,or the extent of staff training to ad-dress inclusionary practices.
2.7 REMAINING BARRIERS; ON-GOING CHALLENGES
It is obvious from the findings ofthis study and the YBIC! findingsof representative centres that all isnot well with inclusionary childcare in Canada. The base level ofquality (or “the health” of child care)is the foundation upon which in-clusion must take place. If thatquality is imperiled through suchfactors as decreased funding and
support, higher staff turnover,lower staff morale, shortage oftrained staff, more complex familyand child issues at the centres (asit has been in most provinces since1994), the potential for effective in-clusion is lost as well. Further, itmust be remembered that inclu-sion in Canada is permissive —there is no anti-discrimination leg-islation that requires centres toinclude all children, regardless ofspecial needs. When the going getsrough, the most vulnerable chil-dren suffer most.
If Canada is to live up to its com-mitments to all children, it mustquickly move toward equitable ac-cess for children with special needsin child care. Whether this requiresa new interpretation of the Charterof Rights and Freedoms, amend-ments to the human rights legisla-tion in the provinces and territories,or simply a recognition of Canada’sobligations as a signatory to the U.N.Convention on the Rights of theChild, we do not know. We do knowthat, in 2000, it is wrong for chil-dren to be excluded from child carecentres because of their specialneeds.
That said, it is critical that centres,training programs, external consult-ants and supports all be funded andsupported appropriately in order tofully include children with specialneeds. Thus far, many of the cen-tres have included children withspecial needs despite the lack ofresources, extra staffing, training,and support. In these situations,centres’ capacities are strained, andthe likelihood of their moving fur-ther toward inclusion without de-pendable resources is in question.
END NOTES
1 The figure for females is qualified by the phrase “with high sampling variability.”
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada32
2 Statistics Canada (1996-97). National Population Health Survey. Ottawa: Statistics Canada.
3 Statistics Canada (1991). Canada’s Health and Activity Limitation Survey. Ottawa: StatisticsCanada.
4 Lero, D.S., Pence, A.R., Shields, M., Brockman, L.M. & Goelman, H. (1992). Canadian na-tional child care study: Introductory report. Ottawa: Statistics Canada, Cat. No. 89-526E.
5 Friendly, M. & Oloman, M. (1998). Child care at the centre: Child care on the social, economicand policy agenda in the 1990s. In J. Pulkingham & G. Ternowetsky (eds.), Remaking Canadiansocial policy: Social security in the late 1990s, 273-285. Halifax, NS: Fernwood Publishing.
6 Friendly, M. (1994). Child care policy in Canada: Putting the pieces together. ON: Addison-Wesley Publishers Limited.
7 Rebick, J. (2000, April 9th). Plenary presentation to Child Care Human Resources RoundTable Symposium.
8 Hertzman, C. (1998). The contribution of early experience to health inequalities throughoutthe life course. Plenary Session at The Early Years: Birth to School Age conference. Conferencesyllabus. BC: British Columbia Association of Infant Development Consultants.
9 Vanier Institute of the Family (1994). Profiling Canada’s families. ON: Author.
10 National Council of Welfare (1999). Preschool children: Promises to keep. ON: Author.
11 Berkowitz, E.D. (1995). Mr. Social Security: The life of Wilbur J. Cohen. Lawrence, KS: Univer-sity Press of Kansas.
12 McQuaig, L. (1993). The wealthy banker’s wife: The assault on equality in Canada. ON: Pen-guin Books Canada.
13 Zigler, E. & Valentine, J. (1997). Project Head Start: A legacy of the war on poverty (2nd Ed.),488-490. Washington, DC: National Head Start Association.
14 McCain, M.N. & Mustard, J.F. (1999). Reversing the real brain drain: Early years study, finalreport. ON: Publications Ontario. (Website: www.childsec.gov.on.ca).
15 Irwin, S.H. & Lero, D.S. (1997). In our way: Child care barriers to full workforce participationexperienced by parents of children with special needs — and potential remedies. NS: BretonBooks. See also, Roeher Institute (2000). Finding a way in: Parents on social assistance withdisabled children. ON: Author.
16 Irwin, S.H. (1994). Toward a federal role for inclusion of children with special needs in Cana-dian child care programs: Report to the Standing Committee on Human Resources Development.Available from SpeciaLink.
17 Irwin, S.H. & Lero, D.S. (1997).
18 Canadian Association for Community Living (1999). Fair tax for families who have a child witha disability. ON: Author. See also, D.G. Duff. (2000), Disability and the federal income tax act.ON: Williams Research.com Inc.
19 Torjman, S. (1999). Will the “Children’s Budget” Include Kids with Disabilities? ON: CaledonInstitute of Social Policy.
20 Irwin, S.H. (1994). Toward a federal role for inclusion of children with special needs in Cana-dian child care programs: Report to the Standing Committee on Human Resources Development.A Supplementary paper. Available from SpeciaLink.
21 Johnson, L., Johnson, P., MacMillan, R.P. & Rogers, C. (1993). EC-SPEED: Early childhoodspecial education program design and evaluation guide. OH: The Ohio Department of Educationand the Northcentral Ohio Special Education Regional Resource Centre.

CURRENT UNDERSTANDINGSCHAPTER 2 33
22 Doherty, G. (1998). Assessing quality in child care settings. Interaction, 12(1), 16-20. See alsoDoherty-Derkowski, G. (1994). Quality matters: Excellence in early childhood programs. ON:Addison-Wesley Publishers.
23 Strain, P. S. (1988). Least restrictive environment (LRE) for children with handicaps: What weknow, and what we should be doing. Journal of Early Intervention, 14(4), 288-296.
24 Hundert, J., Mahoney, B., Mundy, F. & Vernon, M.L. (1994). Predictors of gains of childrenwith disabilities in specialized and community early childhood settings. Ottawa: Child Care Ini-tiatives Fund (Submission to the Department of National Health and Welfare, Social ServiceBranch). Summary by K.C. Ryerse in Focus (Sept, 1995), 7-11, the supplementary volume ofthe 7-part serial publication of the Canadian Child Care Federation.
25 Brown v. Board of Education (1954). See The Oyez Project at Northwestern University throughhttp://oyez.nwu.edu/cases/cases.
26 Clark, K.B. (1993). Unfinished business: The toll of psychic violence. In Newsweek, January11, 1993, 38.
27 Individuals with Disabilities Education Act (IDEA), P.L. 101-476, (1990), updating 94-142(1975) which mandated free and appropriate educational services in the least restrictive envi-ronment to individuals 3-21, mandated transition services and assistive technology services tobe included in a child’s or youth’s IEP, and added autism and traumatic brain injury to the listof categories of children and youth eligible for special education and related services. Part Hrefers to services for children 0-3 and their families.
28 Americans with Disabilities Act (ADA), P.L. 101-336, (1990). Based on concepts of the Reha-bilitation Act of 1973, this law guarantees equal opportunity for individuals with disabilities inemployment, public accommodation, transportation, state and local government services, andtelecommunications. It specifically includes children of all ages, in group child care and familydaycare.
29 Goguen, L. & Poirier, D. (1995). Are the educational rights of exceptional students protectedin Canada? In R. Ghosh, & D. Ray, (eds.), Social change and education in Canada (3rd ed.),310-322. Toronto: Harcourt Brace Canada.
30 Goguen, L. & Poirier, D. (1995).
31 Eaton v. Brant County Board of Education (1997), I S.C.R. 241. See both P.R. de Massy, TheEaton case before the Supreme Court of Canada: A “constructive” reading of the decision, andC.S. Judd, The Eaton and Eldridge cases: Same but different? and in entourage (10) 3/4 (1997).
32 Buysse, V., Wesley, P.W. & Keyes, L. (1998). Implementing early childhood inclusion: Barrierand support factors. Early Childhood Research Quarterly, 13(1), 169-184.
33 Brown v. Board of Education (1954).
34 Irwin, S.H. (1994). Integration of children with special needs into daycare and after-schoolprograms. Ottawa: Disabled Persons Unit, Health and Welfare Canada. (Available fromSpeciaLink.)
35 Goguen, L. & Poirier, D. (1995).
36 Irwin, S.H. (1993). The seamless day. In The SpeciaLink book (1993), 7. NS: Breton Books.
37 Irwin, S. H. (1992). Increasing enrollment of preschool children with special needs in regulardaycare programs through a peer-coaching, systems change approach. ERIC document.
38 Goguen, L. & Poirier, D. (1995).
39 Special Needs Day Care Review Reference Committee for the Minister of Social Services (1993).Supported child care: The report of the special needs day care review in BC. BC: Author.
40 Ontario Coalition for Better Child Care (1992). On the road to reform: The Ontario Coalition forBetter Child Care responds to: Setting the stage: A public consultation paper on child care reformin Ontario. ON: Author.
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada34
41 Nova Scotia (1994). Day care licensing manual discussion paper (draft).
42 Smith, Dr. Jim (1993). Nova Scotia Minister of Community Services (Press release).
43 New Brunswick (1994). New directions: Child care reforms. NB: Author.
44 Saskatchewan Social Services (1995). Child day care division: Child development programinformation (revised).
45 Standing Committee on Human Resources Development (1995). Canada: Security, opportuni-ties and fairness: Canadians renewing their social programs. Ottawa: Canada CommunicationGroup.
46 Irwin, S.H. (1992).
47 Irwin, S.H. (1995). Inclusive child care in Canada: Advances at risk. In As if children matter:Perspectives on children, rights and disability, 77-89. Toronto, ON: Roeher Institute.
48 National Network of Families (1999). Don’t exclude our children: Include all Canada’s childrenin the National Children’s Agenda. Toronto, ON: Canadian Association for Community Living.
49 In Unison, a 1998 agreement of f/p/t governments (except for Québec), provides a blueprintfor policy development in the area of disability. It makes an intergovernmental commitment tofull citizenship of people with disabilities and identifies three building blocks to guide policydevelopment — disability supports, income supports and employment supports.
50 Harms, T. & Clifford, R.M. (1980). Early childhood environment rating scale (ECERS). NewYork: Teachers College Press, Columbia University.
51 Harms, T. & Clifford, R.M. & Cryer, D. (1998). Early childhood environment rating scale, re-vised edition (ECERS-R). New York: Teachers College Press, Columbia University
52 Johnson et al (1993).
53 Johnson, L. (1998). Personal correspondence with author.
54 Division of Early Childhood (1993). DEC Position on Inclusion. Pittsburgh, PA: Author.
55 Bredekamp, S. & Copple, C. (eds.) (1997). Developmentally appropriate practice in early child-hood programs — revised edition. Washington, DC: National Association for the Education ofYoung Children.
56 Doherty, G., Lero, D.S., Goelman, H., LaGrange, A. & Tougas, J. (2000). You Bet I Care! ACanada-wide study on wages, working conditions and practices in child care centres. Guelph:University of Guelph (Centre for Families, Work and Well-Being).
57 Stoiber, K.A., Gettinger, M. & Goetz, D. (1998). Exploring factors influencing parents’ andearly childhood practitioners’ beliefs about inclusion. Early Childhood Research Quarterly, 13(1),107-124. See also Irwin, S.H. (1995). Inclusive child care in Canada: Advances at risk.
58 Doherty, G. et al. (2000).
59 Lero, D.S., Doherty, G., Goelman, H., LaGrange, A. & Tougas, J. (2000). A Profile of ChildCare Centres across Canada. In You Bet I Care! A Canada-wide study on wages, workingconditions, and practices in child care centres, Chapter 9, 111-124. Guelph: University of Guelph(Centre for Families, Work, and Well-Being).
60 Childcare Resource and Research Unit (1999). Early childhood care and education in Canada:The provinces and territories. Toronto: Author, Centre for Urban and Community Studies,University of Toronto. Update 2000: H. Sinclair (NF), K. Reid (MB) & C McCormack (PE).

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 35
LITERATURE
REVIEW: THE ROLES OF STAFF
ATTITUDE, EXPERIENCE, AND TRAINING
IN EFFECTIVE INCLUSION IN CHILD CARE
3.added the Division of Early Child-hood (DEC) in 1973. Membershipin that body, which holds its ownannual conference, and partici-pates in the general annual con-ferences of the parent body, nownumbers over 53,000 members.For a number of years, the Handi-capped Children’s Early EducationProgram (HCEEP) co-sponsoredannual conferences with the Divi-sion of Early Childhood (DEC), fea-turing information booths andworkshops by each of its outreachprojects.The Research Institutes onPreschool Mainstreaming, theEarly Intervention Research Insti-tutes, and the National Early Child-hood Technical Assistance System,funded by the U.S. government,continued to provide high quality,timely research and technical as-sistance into issues surroundingpreschool inclusion.
In Canada, during the same period,a major effort by voluntary organi-zations, with funding from founda-tions and from both the federal andprovincial governments, culmi-nated in the report, One MillionChildren (1970).2 Sponsored bysix major national voluntary orga-nizations, the goal of the CELDICCommission (Commission on Emo-
Sharon Hope Irwin, Kathleen Brophy, Donna S. Lero
3.1 HISTORICAL OVERVIEW OFTHE LITERATURE ON CHILDCARE INCLUSION
The short history of literature onpreschool inclusion can be datedfrom the early 1960s. In 1968, thepassage of the United States Pub-lic Law 90-538, the HandicappedChildren’s Early Education Act, sig-naled the intention of that govern-ment to assist in the developmentand demonstration of models forthe provision of exemplary compre-hensive services to preschool,handicapped children and theirfamilies (Swan, 1980).1 From theHandicapped Children’s Early Edu-cation Program (HCEEP), a re-search program to support PL 90-538, has flowed a wide variety ofexemplary program models, out-reach programs, a review panel,seven university-based researchinstitutes into topical issues in pre-school special needs, and numer-ous graduate level early childhoodspecial education programs. Themajor early childhood special edu-cation research journals were ini-tiated in the late 1970s and early1980s, forming the principal ve-hicles for dissemination of this re-search. The Council for ExceptionalChildren, established in 1922,
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada36
tional and Learning Disorders inChildren) was “to study the needsof the ‘one million children’ andyouth in Canada who experienceemotional and learning disorders;to search for new principles, struc-tures and models; and to reportupon and make recommendationsfor improving present efforts.”Mainly focused on educational op-portunities, the report briefly ad-dressed preschool programs andsuggested that “the reasons for seg-regation in preschool educationseem to be administrative and fi-nancial rather than educational,and indeed, (segregation) may bedetrimental to the educational ob-jective” (p. 86). However, the reporttends to frame daycare in terms of“working mothers,” and does notsuggest its use as a vehicle for in-clusion.
During the 1970s and early 1980s,research findings and demonstra-tion projects focused primarily onbehavioural techniques for achiev-ing measurable objectives for pre-school children with special needs.It was assumed that the basic tech-niques and strategies, consideredeffective in teaching cognitive andlanguage skills to persons withmental handicaps, could be com-bined with the social learning of theintegrated preschool.
For social skills, the commontheme of much of this early litera-ture was the “proximity theory,”namely that physical closeness tonormally developing children helpschildren with special needs to learnage-appropriate behaviours andthat, by creating a more “advanced”educational milieu, the children arepushed developmentally. By themiddle 1980s, the literature hadtaken “inclusion” as a startingpoint, and raised many questionsabout “proximity” as an effective
strategy for socialization in the in-tegrated preschool. Researchersbegan to consider a variety of tech-niques and strategies for makingintegrated placements more effec-tive. Social inclusion became amajor focus of research, demon-stration projects, and outreach.
By the late 1980s, it was recognizedthat the attitudes of staff towardinclusion of children with specialneeds would, to a large extent, de-termine the success of inclusion inregular child care centres. The lit-erature began to focus on a num-ber of factors thought to influencestaff attitudes toward includingchildren with special needs.
3.2 ORGANIZATION OF THELITERATURE REVIEW
Challenges to the inclusion of pre-school children with special needshave been categorized in severalways.
Peck (1990)3 discusses “context,process, and child-outcomes.” TheResearch Institute on PreschoolMainstreaming (Salisbury, 1991)4
identifies four primary challenges:administration, knowledge voids,compatibility of existing early child-hood curricula with the instruc-tional needs of handicapped learn-ers, and the necessity to carefullytranslate and pinpoint the “howand why” of inclusion to all relevantaudiences.
Smith and Rose (1994)5 outline sixareas of policy barriers: programstandards, personnel standards,fiscal policies, eligibility policies,transportation policies and coordi-nation policies. Although theirmandate was to focus on policy dis-incentives, “attitude” was so fre-quently cited as a barrier to pre-school mainstreaming that they felt

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 37
compelled to consider this humandimension as well. They asked thequestion, “Are there values or at-titudes that are acting as barriersto preschool main-streaming?” Al-most 58% of the respondents totheir survey indicated that thepresence of attitudinal barriers topreschool inclusion was secondonly to personnel requirements inimpeding inclusion. They furtherdivided “attitude” into five compo-nents: turf issues, teacher pre-paredness, awareness, “someonewill lose,” and lack of com-munication/collaboration/re-spect. While this was a UnitedStates study, carried out in 1993,we believe that the issues of atti-tude are as substantial in Canadaas they were/are in the UnitedStates.
We caution the reader to remem-ber that “attitude” does not existin a vacuum. Lack of resources,lack of training, general policy bar-riers and unrealistic expectationsall contribute to “attitude.” Indeed,over and over directors, (EarlyChilhood Educators) ECEs and(Resource Teachers) RTs reportedthat they believe in full inclusionin child care centres and are eagerto include children with specialneeds — but feel that they lack theresources and/or training to do so.6
Building on the work of Smith andRose, we have used a seven-component division of “attitude” toorganize this literature review. Thecomponents are: nature of thechild’s disability, training,experience in working with childrenwith special needs, confidence ofthe staff, availability of resources,collaboration with parents, and theleadership approach taken by earlychildhood directors. In Section 3.3,we discuss these seven compo-nents, which we believe are espe-
cially relevant to the Canadiancontext.
3.3 THE ROLES OF STAFFATTITUDE, EXPERIENCE, ANDTRAINING IN EFFECTIVEINCLUSION IN CHILD CARE
3.31 Nature of the Child’s SpecialNeeds
Characteristics of the child affecthow child care staff viewinclusion.Their attitudes towardsinclusion may vary in response tothe disability in question. Gener-ally, staff are more positive aboutincluding children with physicaldisabilities, learning disabilities,language delays, and mild cogni-tive disabilities than about includ-ing children with challengingbehaviours, autism, or complexneeds (Bochner, Denholm &Pieterse, 19907; Denholm, 19908;Eiserman et al., 19959; Garvar-Pinhas & Schmelkin, 198910; Irwin& DeRoche, 199211; Stoiber,Gettinger & Goetz, 199812).
A disability mathematics is oftenplayed to justify the exclusion ofchildren with more challengingneeds. If it can be shown that chil-dren with significant disabilities donot benefit from inclusion as muchas children with mild disabilities,then such an exclusion can be ra-tionalized. A similar disabilitymathematics points out that theimmediate costs of integratingmildly disabled children are lower— in terms of human resources,physical modifications, training —than the costs of integrating se-verely disabled children. However,most of the literature reports thatthe common conclusion is not ac-curate. Segregated programs aremore expensive and less effective

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada38
(Hundert, J., Mahoney, B., Mundy,F., & Vernon, M.L., 199413) andmedium and long-term savings arenot considered (Strain, 198914).And, taken from three other per-spectives, legal (in the UnitedStates), moral/ethical and societal(in Canada), measurably positivechild outcomes in the severely/pro-foundly disabled are not the onlybases on which these placementsshould be made.
Demchak & Drinkwater (1992)15
provide an overview of strategiesthat have been successful in im-proving the social integration ofchildren with severe disabilities —strategies that include staff train-ing, sensitization of non-handi-capped peers, as well as specifictechniques for working with se-verely disabled children. They iden-tify staff development as a crucialelement of successful integration ofthese children. Appropriate train-ing is necessary to eliminate fear,misinformation, and negative atti-tudes about children with severedisabilities. In-service training,grounded in validated “Best Prac-tices,” can alleviate insecurities andprovide child care staff with thenecessary skills to change theirprogramming and practices, to fa-cilitate the social inclusion of chil-dren with severe disabilities. Ap-propriate in-service training canalso instruct child care staff on howbest to modify the physical envi-ronment of the centre to encour-age social interaction between chil-dren with severe disabilities andtheir typically developing peers.
Shanks and Thompson (1991)16
reflect on family-focused objectives,and observe that parents of chil-dren with special needs often re-quire full daycare placements, notjust part-time “treatment” place-ments. Templeman, Fredericks, &
Udell (1989)17 describe the system-atic integration process of includ-ing children with moderate andsevere handicaps followed in oneregular child care centre.
Chandler and Dahlquist (1997)18
describe the two purposes of theirstudies: (1) to evaluate the effec-tiveness of the functional assess-ment interventions that were de-veloped for individual children, and(2) to evaluate the effectiveness offunctional assessment when it wasconducted by classroom teams,rather than by research staff.Classrooms studied included threetypes: segregated special needsclassrooms; classrooms exclusivelyenrolling children at risk; and regu-lar early childhood classrooms.Thestudy indicates that behaviour ofthe full groups of children withinpreschool classrooms improvedwhen functional assessment wasdeveloped for individual children.The study also found that childcare staff were able to conductfunctional assessment within theirclassrooms during interventionsand that they maintained func-tional assessment skills during themaintenance period.
3.32 Staff Training
The training of child care staff is aregulatory issue, a monetary issue,a philosophical issue — and a mat-ter of urgency. Pre-service trainingrequirements for centre teachers(Childcare Resource and ResearchUnit, 199919) vary substantiallyamong the provinces — with themedian level of required trainingbeing a one- or two-year commu-nity college diploma. Moreover,some provinces also permit vari-ants of “grandparenting” of un-trained, but experienced,caregivers. In addition, most prov-

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 39
inces do not require that all staffworking with a defined group ofchildren have training. And, finally,the quality and effectiveness oftraining are also critical issues.Competency-based measures ofskill as well as mentoring modelsof support, rather than strictlytraining-based requirements, haveperiodically been suggested beforecertification as an Early ChildhoodEducator, and have been tried invarious projects.20
Even in provinces where trainingis required, that training may notinclude any substantial amount ofinformation or practicum experi-ence related to special needs or in-clusion. In a 1996 curriculumanalysis of ECE post-secondarytraining programs in Canada, theHRDC Sector Study on the ChildCare Workforce21 reported that only15% of ECE certificate programsand 66% of diploma programs in-cluded either a course in whichspecial needs was a major compo-nent or an indication that the topicof special needs was specificallymentioned in several course de-scriptions (explicit infusion ap-proach). While not specifically men-tioned in the Sector Study analy-sis, it is fair to point out that theavailability of placements andpractica in inclusive community-based child care programs wouldbe another important vehicle forpre-service learning.
The research literature is quiteclear about the impact of trainingrelated to special needs on the at-titudes of child care staff. The train-ing that ECEs have received (pre-service, post-diploma/specialized,and in-service) can impact on theirattitudes, and a lack of knowledgeis viewed as a barrier to success(Dinnebeil et al., 199822; Peck,Hayden, Wandschneider, Peterson
& Richarz, 198923). ECEs withregular education training and withknowledge about inclusion andchild development are more posi-tive than ECEs without this train-ing (Bricker, 199524; Garver-Pinhas& Pedhauzur, 198925; Kontos &Diamond, 199726; Stoiber et al.,199827). ECEs with special educa-tion training are more positive thanECEs with only regular educationtraining (Bricker, 199528; Eisermanet al., 199529; Gemmell-Crosby &Hanzlik, 199430; Johnson, 199331;Stoiber et al., 199832). Case-specifictraining (e.g., delegated nursingcare) is particularly critical in situ-ations involving children with moreprofound disabilities (Bochner,Denholm & Pieterse, 199033; EarlyChildhood Educators, 199734;Irwin, 199235; Norton, 199136).
Pre-Service Training
Most ECE graduates will start workin child care without post-basic orspecialized training. If pre-servicetraining is to prepare these stu-dents to work in inclusive settings,the split between Early ChildhoodEducation (ECE) and Early Child-hood Special Education (ECSE)must be resolved. As noted above,much Canadian ECE training doesnot address children with specialneeds and training which does of-ten addresses exceptionalitiesrather than strategies for inclusion.
Heston, Raschke, Kliewer, Fitz-gerald & Edmiaston (1998)37 de-scribe their efforts to transform theearly childhood education majorand the early childhood specialeducation major into a single uni-fied major. This unified major isintended to prepare early childhoodeducators to address competentlythe educational needs of both chil-dren with and without disabilitiesin a general education classroom.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada40
They describe the events occurringat both the state and university lev-els that led to their efforts, and theprogress they have made duringthe first year of their work. Theyalso identify several challenges thatthey expect to confront.
Although Canadian pre-servicetraining has not separated earlychildhood education and earlychildhood special education intotwo disciplines to the extent thatAmerican programs have, the spe-cial needs course in an ECE train-ing program is usually more aboutthe nature of disabilities thanabout inclusion strategies. A num-ber of Canadian ECE training pro-grams have redesigned their cur-ricula to “embed” or “infuse” inclu-sion into all their courses. The ar-ticle by Heston et al speaks to alltrainers who are trying to do so andto those who are considering thischange.
Post -Dip loma/Specia l izedTraining
Further complicating the trainingpicture for inclusive child care is theissue of additional, possibly spe-cialized, training, beyond minimumrequirements. The conundrumhere is that, according to inclusionadvocates, all staff should be en-couraged to work with and inter-act with the children with specialneeds. If this work can only be as-signed to people with special needscredentials, then the child may wellbe isolated within the integratedsetting. In the best practice visionof inclusion advocates, all staffwould have basic training that in-cludes inclusionary principles andstrategies and would be expectedto include all children in theirgroups. Some staff would choose totake post-diploma and specializedtraining to enhance these skills and
to be recognized as specialists orresource teachers.
Currently, most provinces do notrequire additional training for staffwho work with children with spe-cial needs. Ontario recommends ahigher training standard for re-source teachers, and British Co-lumbia provides a post-basiccourse for people who want to workwith children with special needs.Training institutions in many prov-inces, including Nova Scotia,Ontario, Manitoba, Saskatchewan,and British Columbia, providepost-basic courses in inclusionand/or special needs. The comple-tion of such a credential does not,in most provinces, lead to a higherrate of pay or occupational desig-nation.
Frankel (1994)38 discusses thetraining and responsibilities of re-source teachers in Ontario, andrecommends that consultationskills and in-service be added totheir training. Through a question-naire, she examined the responsi-bilities, training competencies, andeducational backgrounds of theseresource teachers, against thebackdrop of guidelines establishedby the Ontario Ministry of Commu-nity and Social Services for thetraining and professional respon-sibilities of resource teachers.While there is no formal certifica-tion of resource teachers inOntario, the Ministry guidelinesstate that resource teachers shouldhave a diploma in early childhoodeducation and training in thetheory and practice of the needs ofhandicapped children. Althoughmost of the 124 respondents in this1994 study had some training inearly childhood education, onlyeighteen (14.5%) had the educa-tional background preferred by the

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 41
education is no exception.40 In-ser-vice training and professional devel-opment have been identified as criti-cal to positive staff attitude towardinclusion. Pre-service training, in-cluding post-diploma and special-ized training, cannot adequatelyprepare staff for the individualneeds of a child with very challeng-ing special needs. No early childreneducation or early childhood spe-cial education curriculum can ad-equately prepare students to re-member how to properly handlespecialized health-related equip-ment, how to properly modify thesetting’s physical environment, howto respond to multiple severe handi-caps, etc. For this reason, special-ized support services and case-spe-cific training must be provided(Early Childhood Educators, 199741;Irwin, 199242; Norton, 199143). Staffcan also keep apprised of newprojects, developments and re-source materials through profes-sional associations, workshops,journal literature, the World WideWeb and related newsletters.
The British Columbia PartnershipProject,44 funded through the fed-eral/provincial Strategic InitiativesProgram, is one notable province-wide in-service initiative related toinclusive child care. The training-the-trainer packages, developedthrough an extensive consultationand pilot process, generally involvea health professional, an ECE, anda parent as co-facilitators. Issues ofpaid in-service/professional devel-opment time have not been resolved,but the Project is a recognition byone province that the shift to sup-ported child care (inclusive childcare) cannot be accomplished with-out addressing training needs ofpeople currently in the field.
Manitoba’s Autism Outreach Pro-gram,45 in addition to funding
Ministry and twenty-eight (22.6%)had training in Early ChildhoodEducation for the DevelopmentallyHandicapped.39
Frankel’s survey results indicatethat pre-service training did notalways equip resource teachers forthe reality of their profession. Thistraining gap is evident in the factthat most resource teachers re-ported that they were trained in theneeds of the physically handi-capped and mentally handicapped,but were not trained in specializedtechniques for educating childrenwith behavioural challenges, hear-ing impaired children, etc. Also,some resource teachers reportedthat they had insufficient trainingin counseling, consultation skills,and case coordination.
Frankel concluded that efforts haveto be made to insure that trainingprograms keep pace with profes-sionals’ changing work environ-ments. With the shift in Ontario toa traveling resource teacher model,resource teachers will need moretraining as consultants in inclu-sion. She also noted that trainingfor regular child care staff must beupdated and brought more into linewith the training now offered inearly childhood special educationpost-diploma models, if they aregoing to properly work with chil-dren with special needs.
In-Service Trainingand Professional Development
Most occupational groups recom-mend or require professional devel-opment activities for individualsengaged in professional practice,including attendance at workshopsand conferences, membership inprofessional organizations, andparticipation in in-service educa-tion programs. Early childhood

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada42
support staff and providing in-cen-tre consultation, also includes atwenty-four hour classroom com-ponent on autism and strategies forincluding children with autism thatis available at no charge to childcare staff as well as to families.
Many agencies that deal with chil-dren with behavioural issues pro-vide highly professional workshopson these issues for the child carecommunity.
Unlike these specialized in-servicetraining opportunities, the Trainingfor Inclusion Project (Palsha &Wesley, 1998)46 approaches the is-sues of inclusion through an in-service model that focuses more onbase quality than on specific train-ing related to children with specialneeds. The authors believe that agreat deal of “pull-out” and one-to-one support could be eliminated ifthe overall quality of the centre’sprogram improved. After a pilotstudy in several counties of NorthCarolina, this inclusive in-servicetraining has been expandedthroughout the state and is nowbeing tested in three Canadianprovinces.47
The combination of advanced tech-nology and the time/distancecrunch experienced by Early Child-hood Educators is leading to inno-vations in the delivery of both pre-service and in-service training.48
One early example of such in-ser-vice training in inclusion is TheEarly Childhood Special EducationProgram (EC-SPEED), developed inthe early 1990s for use in ECEtraining in Ohio.49 It is quite mod-estly priced and includes an intro-ductory video, eleven video train-ing tapes and four booklets (Design& Evaluation Guide; AnnotatedBibliography; Curriculum Guide;Summer Institute Proceedings). Its
value as an instrument for self-study, as well as for course credit,has been widely recognized, andseveral other states now use it fortheir own training. Just as “video”was an early example of advancedtechnology, we expect to see use ofthe World Wide Web for dissemina-tion of information as well as forinteractive, credentialled trainingon child care inclusion.
3.33 Experience in Working WithChildren With Special Needs
The amount of experience childcare staff have in working with chil-dren with special needs can relateto their attitudes towards inclu-sion. Some researchers have foundthat experience has a positive ef-fect on staffs’ attitudes (Dinnebeil,McInerney, Fox & Juchartz-Pendry, 199850; Eiserman et al.,199551; Johnson, 199352; Munby,H. & Hutchinson, N., 199853;Stoiber, Gettinger & Goetz, 199854).Others have found that the in-crease in frustration, behaviourproblems, and effort to modify in-struction which occurs has de-terred them from future inclusivepractices. Peck’s study (1990)55 didnot find that the amount of staffexperience had any relation towhether an inclusive child care pro-gram survived or whether it re-trenched into a segregated model.
Dinnebeil, McInerney, Fox &Juchartz-Pendry (1998)56 foundthat families of young children withspecial needs had great difficultyin accessing child care. To identifyearly childhood personnel charac-teristics associated with an inter-est or willingness to care for thesechildren, they surveyed early child-hood personnel in northwesternOhio. Most respondents were inter-ested in caring for young children

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 43
with special needs. More than onehalf of the respondents reportedexperience in caring for such chil-dren and most were confidentabout their ability to do so. Themost frequently cited barrier to in-clusive child care was a lack ofknowledge regarding care require-ments for young children with spe-cial needs. Researchers identifieddifferences between home- andcentre-based providers in interestand willingness to care for childrenwith special needs. Implications ofthese findings for child carestaff training are discussed in thearticle.
To investigate beliefs concerningearly childhood inclusion, Stoiber,Gettinger, & Goetz (1998)57 devel-oped a 12-item brief scale and 28-item comprehensive measure, MyThinking About Inclusion (MTAI).The 28-item MTAI Total Scale hadan internal consistency of .91, andwas comprised of three beliefsubscales: core perspectives, ex-pected outcomes, and classroompractices. MTAI was administeredto 415 parents and 128 early child-hood practitioners.
Parents of children with disabilitieswere more positive in their beliefsthan were parents of children with-out disabilities, and parents’ beliefswere related to their level of edu-cation, number of children, andmarital status. Practitioners heldmore positive beliefs than did theparent participants. Practitioners’beliefs were associated with theirlevel of education, training back-ground, and years of experience.
3.34 Confidence of the Staff
Child care staffs’ confidence abouttheir own abilities to work withchildren with special needs can af-
fect their attitudes towards inclu-sion. They indicate more self-con-fidence when they have had moreexperience working with childrenwith special needs (Dinnebeil etal., 199858) and when they havehad training in early childhoodspecial education (Bochner et al.,199050; Denholm, 199060; Frankel& McKay, 199061; Peck, Killen &Baumgart, 198962). Perceived self-competence impacts on the inclu-sion process (Denholm, 199063;Eiserman et al., 199564; Garver-Pinhas & Pedhauzur Schmelkin,198965), and a lack of confidenceis viewed as a barrier to success-ful inclusion (Dinnebeil et al.,199866).
Gettinger, Stoiber, Goetz & Caspe(1999)67 investigated perceptionsof competence, training, and theimportance of professional skillsrelated to inclusion of childrenwith disabilities in early childhoodsettings. They surveyed parents ofchildren with disabilities, profes-sionals in early childhood pro-grams, university-based trainers,and pre-service students, for a to-tal of 172 respondents.
The survey was used to investigateperceptions of professional compe-tence or training, as well as the im-portance of skills in five domains:(a) working with families, (b) per-formance-based assessment, (c)interdisciplinary team functioning,(d) consultation, and (e) challeng-ing behaviours/attention deficits.The authors compared perceptionsacross respondent groups. In allskill domains, parents rated pro-fessionals’ competence lower thandid the professionals themselves;faculty and students agreed intheir ratings of training. In twodomains — teaming and challeng-ing behaviors — ratings differed

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada44
substantially among the fourgroups. The authors also discussimplications for interdisciplinarytraining efforts.
3.35 Availability of Resources
The availability of numerous re-sources is extremely important tothe inclusion process. A lack ofthese resources (funding, training,current information, access to spe-cialists, time and opportunity forconsultation and collaboration,supervision and support, materialsand equipment, and additionalhelp in the classroom) is viewed bychild care staff as a major barrierto successful inclusion (Bailey,McWilliam, Buysse & Wesley,199868; Buysse, Wesley & Keyes,199869; Eiserman et al., 199570;Irwin, 199171; Johnson, 199372;Odom & McEvoy, 199073; Norton,199174; Peck, Hayden, Wand-schneider, Peterson & Richarz,198975; Stoiber et al., 199876).
Buysse, Wesley & Keyes (1998)77
examined the underlying factorstructure of a rating scale designedto assess perceived barriers andsupports associated with earlychildhood inclusion. Participantsincluded over two hundred admin-istrators and direct service provid-ers from the early intervention,early childhood, and special edu-cation fields and nearly three hun-dred parents (primarily mothers) ofyoung children with disabilities(birth through 5 years) who re-ceived early intervention services.A four-factor solution for barriersthat accounted for 41% of the totalvariance emerged from an explor-atory factor analysis. Since one ofthe factors (attitude) was found tohave low internal consistency, athree-factor solution was used insubsequent analyses: 1) barriers
associated with early childhoodprogram quality, 2) community re-sources, and 3) coordinating andintegrating services for childrenwith disabilities and their families.A confirmatory factor analysis re-vealed a barriers factor structurefor parents that was consistentwith that obtained for profession-als. Background variables, such asrace, education, employment sta-tus and experience with inclusioncontributed to explaining ratings ofbarriers and supports amongparents, lending further support forthe validity of the factor structure.
3.36 Parental Attitudes andCollaboration With Parents
Collaboration with parents is a sig-nificant component of the inclusionprocess. Indeed, in the UnitedStates the IDEA Act requires thatlocal education agencies demon-strate that they have sought activeparental participation in theIndividual Program Planning (IPP)process, through such methods asflexible scheduling of meetings,babysitting services, transporta-tion, and translation services.78
Child care staff have stated thatsuccessful inclusion is hinderedwhen the involvement of parents inplanning special services is limitedand when communication betweenchild care staff and the parents ofchildren with special needs is lack-ing (Buysse et al., 1998).79 Also im-portant to staff attitude toward in-clusion is the sense that parentsof children in their centre are sup-portive of the effort. It has oftenbeen assumed that the attitudes oftwo groups — parents of typicallydeveloping children and parents ofchildren with special needs —might differ.
Allred, Briem & Black (1998)80

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 45
found that parents who feel own-ership of their child’s goals aremore likely to consider these goalsas top priorities in their family rou-tine, rather than as additional bur-dens that must be imposed on topof a full slate of family responsi-bilities. Just as parents need theguidance and support of earlychildhood professionals, so do pro-fessionals need the input and sup-port of the families. Family mem-bers provide insights into the indi-vidual strengths and needs of achild with a disability. Their knowl-edge of and intimate relationshipwith the child can help profession-als to make efficient use of theirtime, resources, and capabilities,and can help assure that plans andgoals are relevant and workablefrom a family perspective.
In inclusive settings, parents oftypically developing children mightbe expected to worry about the levelof staff attention for their children;about the effects of curriculummodification and adaptations forthe cognitive development of theirchildren; about the negativebehaviours that their childrenmight pick up in imitating childrenwith special needs. On the otherhand, parents of children with spe-cial needs might be assumed tohave a set of different concerns.Would the inclusive setting con-tinue to offer the specialized ser-vices of the segregated program?Would other children or other par-ents stigmatize their children?Would the emotional support ofstaff and other parents, often foundin the specialized setting, disappearin the community one? Parents ofboth groups want a normalizedenvironment for their children, butthey also are concerned about theacademic component of the pro-gram (Bailey & Winton, 198781;Reichart et al., 198982).
Other studies have also noted thatalthough parents of children withspecial needs desire normalizedpeer relationships for their chil-dren, the parents themselves oftendon’t interact with parents of typi-cally developing children and oftenfeel alienated (Bailey & Winton,198783; Blacher & Turnbull,198384). Many parents felt that inorder to ensure a strong inclusiveprogram which emphasizes thedevelopment of all children, sup-ports in the forms of training, ex-tra staff, and special equipmentwere often needed (Bailey &Winton, 198785; Reichart et al.,198986).
To determine whether the realitiesof inclusive preschools met withparents’ initial expectations, Baileyand Winton (1987)87 questionedboth families of children with spe-cial needs and families of typicallydeveloping children prior to enroll-ment and during the course of theprogram. The study was conductedat an established day care centrewhich had not previously servedchildren with special needs. Nineof the children enrolled had a vari-ety of handicaps; the other fiftychildren were non-handicapped.
Turnbull and Winton (1983)88 con-structed questionnaires from ob-servations gathered in earlier stud-ies on parental perspectives ofmainstreaming. Parents wereasked to select from the series ofstatements the “greatest benefit”and “greatest drawback” of themainstream program. The ques-tionnaires and attitude scales werefirst administered two weeks priorto enrollment, and again ninemonths after the beginning of themainstreamed program.
Generally speaking, both groups’expectations of the benefits of
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada46
mainstreaming did not change dur-ing the course of the study. Manyrespondents still believed the great-est benefits of mainstreaming werenormalization and community ac-ceptance of the handicapped. Ini-tially, parents of both groups wereconcerned that teachers would nothave enough time or training todeal with handicapped children,and there had been concerns thatthe handicapped children would beteased by the non-handicappedchildren. However, over time, mostof the perceived drawbacks had dis-sipated; one exception was thatfamilies of the handicapped chil-dren still felt alienated.
Mainstreaming was seen by bothgroups of parents as working well.The authors did note that the find-ings described ‘average’ responsesof groups of parents, but there wasconsiderable variability in the re-sponses of individual families inboth groups, suggesting that ser-vices to families should be individu-alized. The researchers also sug-gested that there is a need inmainstreamed day cares to encour-age “family-family interactions” asa means of alleviating the feelingsof alienation in the families ofhandicapped children.
3.37 The Leadership Approach Takenby Early Childhood ProgramDirectors
The leadership approach taken byearly childhood program directorscan have a large impact on the in-clusion process and on child carestaffs’ attitudes towards inclusion.The directors can control theamount of time for collaborationbetween parents, regular staff, andresource teachers/resource con-sultants, and they also may makedecisions about the quality of staff
development programs and theworkload given to the ECE who haschildren with special needs in her/his class (Garvar -Pinhas &Schmelkin, 198989; Kagan, S.& Bowman, B.T., 199790). Further-more, the director’s attitude aboutinclusion can affect the overall at-mosphere towards inclusion in thecentre. Yet, as Mitchell concludes,“Essentially no one prepares some-one to become an early childhoodadministrative leader; it more orless just happens.”91
In her commentary on leadershipin early care and education, JordeBloom (1997)92 notes that the or-ganizational literature from busi-ness and industry often differenti-ates between managerial functionsand leadership functions. Leader-ship functions relate to helping anorganization clarify and affirm val-ues, set goals, articulate a vision,and chart a course of action toachieve that vision. According toJorde Bloom, “Like an artist, theleader paints the picture, creatingthe images of what an organizationcould be. The leader’s job is to cre-ate a healthy tension between cur-rent reality and an imagined ideal.The importance of the leadershiprole of the child care centre direc-tor cannot be over-estimated.”
The leadership role of the earlychildhood director might be con-ceptualized as having both inter-nal and external dimensions. Inter-nal leadership would refer to shar-ing a vision of inclusion in the cen-tre so that it permeates every as-pect of the director’s work, andharnesses the energy and indi-vidual creativity of all staff to real-ize that dream (Espinosa, 1997)93.External leadership would be seenas advocacy — advocacy to meetthe centre’s unmet needs for addi-tional resources, staffing and fund-

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 47
ing, and advocacy to promote thefield and the concept of inclusion.
In a very recent article, Jorde-Bloom (2000)94 identifies leadershipand advocacy as a critical knowl-edge and skill area of director com-petence. The six components ofthat competency — 1) guiding theboard and staff in developing thecentre’s philosophy and missionstatement; 2) conducting organiza-tional climate assessment to im-prove the quality of work life forstaff; 3) evaluating centre practicesand implementing a program im-provement plan; 4) pursuing cen-tre accreditation; 5) mobilizing oth-ers to advocate for better child andfamily services; and 6) initiatingcommunity collaborations for moreefficient and cost effective servicedelivery — seem indispensable ina director of a centre moving towardfull inclusion.
Roger Neugebauer, in a seminal1981 article,95 Piaget’s Theory ofDirector Development, proposes afour stage development of directors,and suggests that it is unreason-able to assume that leadership willemerge until the director has mas-tered managerial functions.
Finally, VanderVen (1993)96 pro-poses a military strategy for childcare. She proposes that child careadvocates use the apparently mostpowerful and tried model for attain-ing goals known to history: wagingwar by adopting military strategy.In her tongue-in-cheek paper, andin her public presentations whichshe carries out in full military re-galia, Dr. VanderVen suggests thatwe consider our enemies, our or-ganization of forces, our theatre ofoperation, our offense, even ourdeception, plus our concentrationof forces, including flanking, psy-chological warfare, and guerrilla
warfare in the fight for proper fund-ing and policies to promote highquality services for children. In hermore scholarly work, Dr. Vander-Ven97 discusses the dilemma ofdeveloping assertive advocacy in afield that people generally enterbecause of their love of childrenand their capacities as caregivers.Like Jorde-Bloom, she suggeststhat the centre director has a criti-cal role in advocating for additionalfunding and services, not merely inmanaging the currently availableresources. But she is quite con-cerned that the personal charac-teristics of people who choosecaregiving do not naturally developinto the “cadre of assertive, pro-active practitioners able unam-bivalently to tackle the tremendousneeds for advocacy that promotesthe image of the field, alters nega-tive systems, and secures an ad-equate economic base.” Writing in1992, Dr. VanderVen had not wit-nessed the effective politicization ofanother occupation of caregivers,specifically nurses, in the late1990s. She would doubtless ana-lyze their victories in militaryterms.
3.4 SUMMING UP
In this chapter, we have reviewedthe research literature on youngchildren with special needs, as itrelates to their inclusion in childcare.
We see this body of literature asbeginning in the 1960s, with thepassage of the HandicappedChildren’s Early Education Act inthe United States and with thebeginnings of the U.S. Head Startprogram. Both Acts provided sub-stantial research funding and en-couraged the development and fo-cus of a research community in

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada48
that country. During the same de-cade, voluntary organizations inCanada were developing specializedpreschools for children with spe-cial needs. A small research com-munity developed in Canada de-voted to this topic, but no largepublic initiative encouraged orfunded its development. In manyrespects, and despite cultural andlegal differences between the twocountries, research in Canada re-lated to the inclusion of young chil-dren with disabilities has often fol-lowed directions set by U.S. re-search.
Since the 1970s when research re-lated to including preschool chil-dren with disabilities in communityprograms began in earnest, the re-search of each decade can be char-acterized by a particular focus. Inthe 1970s and early 1980s, thepolicy question was “Should chil-dren with special needs be includedin child care and preschool pro-grams?” and the research focusedon behavioural techniques forachieving measurable objectivesthat were comparable to outcomesin specialized programs. By themidddle 1980s, the literature hadtaken “inclusion” as a startingpoint, as the policy question shiftedto “How can children with specialneeds best be included in child careand preschool programs?
By the late 1980s, the focus of re-search had shifted away from rep-licating measurable outcomes to
enhancing the benefits in social-ization and communication thatmight occur when children withspecial needs were included incommunity programs. Attitudes ofchild care staff were seen as oneof the most important variablesthat could be a barrier to effectiveinclusion.
Our literature review has been or-ganized around seven componentsrelated to staff attitudes — natureof the child’s disability, staff’s edu-cation and training, experience inworking with children with specialneeds, confidence of the staff,availability of resources, collabo-ration with parents, and the lead-ership approach taken by earlychildhood directors. We were in-terested in the identification of keyfactors in effective integration aswell as barriers. Few studies, ifany, have described the lived ex-perience of inclusion by staff orconsidered multiple levels of influ-ences operating jointly. And fewerstill are the Canadian studies thatdescribe early childhood educa-tors’ experiences or consider themultiple levels operating withincentres or in ways that affect theircapacities for effective inclusion.
Because of the radically differentpolicy contexts in the UnitedStates and Canada, the U.S. lit-erature that touches the topic ofpreschool inclusion is often notrelevant. We have cited Canadiansources wherever possible.
END NOTES
1 Swan, W.W. (1980). The handicapped children’s early education program. Exceptional Chil-dren, 47(1), 12-16.
2 Commission on Emotional and Learning Disorders in Children (CELDIC) (1970). One millionchildren. Canada: Leonard Crainford.
LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 49
3 Peck, C.A., Furman, G.C., Helmstetter, E. & Reed, D. (1991). Factors affecting the survival ofearly childhood mainstreaming programs: A retrospective study. Vancouver, WA: WashingtonState University, Department of Educational and Counseling Psychology. Published as Integratedearly childhood programs: Research on the implementation of change in organizational contexts,Chapter 10, in C.A. Peck, S.L. Odom, and D.D. Bricker (1993), Integrating young children withdisabilities into community programs, 187-206. Baltimore: Paul H. Brookes.
4 Salisbury, C.L. (1991). Mainstreaming during the early childhood years. Exceptional Children,58(2), 107-124.
5 Smith, B.J. & Rose, D.F. (1994). Administrator’s policy handbook for preschool mainstreaming.Pittsburgh: Brookline Books — Administrative Issues in Education Series.
6 This information has been elicited at numerous workshops on inclusion issues that werefacilitated by SpeciaLink, held at provincial and national ECE conferences from 1990-1999.
7 Bochner, S., Denholm, C.J. & Pieterse, M. (1990). Attitudes to integration in preschool: A com-parative study of preschool directors in Canada and Australia. Victoria, BC: University of Victoria,School of Child and Youth Care.
8 Denholm, C.J. (1990). Attitudes of British Columbia directors of early childhood educationcentres towards the integration of handicapped children. British Columbia Journal of SpecialEducation, 14(1), 13-26.
9 Eiserman, W.D., Shisler, L. & Healey, S. (1995). A community assessment of preschool pro-viders’ attitudes toward inclusion. Journal of Early Intervention, 19(2), 149-167.
10 Garvar-Pinhas, A. & Schmelkin, L.P. (1989). Administrators’ and teachers’ attitudes towardmainstreaming. Remedial and Special Education, 10(4), 38-43.
11 Irwin, S.H. & DeRoche, J. (1992). Attitudes of Canadian mainstream child care staff towardinclusion of children with special needs. (Unpublished manuscript.)
12 Stoiber, K.A., Gettinger, M. & Goetz, D. (1998). Exploring factors influencing parents’ andearly childhood practioners’ beliefs about inclusion. Early Childhood Research Quarterly, 13(1),107-124.
13 Hundert, J., Mahoney, B., Mundy, F. & Vernon, M.L. (1994). Predictors of gains of childrenwith disabilities in specialized and community early childhood settings. Ottawa: Child CareInitiatives Fund (Submission to the Department of National Health and Welfare, Social ServiceBranch). Summary by K.C. Ryerse in Focus (Sept, 1995), 7-11, the supplementary volume ofthe 7-part serial publication of the Canadian Child Care Federation.
14 Strain, P.S. (1989). Least restrictive environment (LRE) for children with handicaps: What weknow, and what we should be doing. Journal of Early Intervention, 14(4), 288-296.
15 Demchak, M. & Drinkwater, S. (1992). Preschoolers with severe disabilities: The case againstsegregation. Topics in Early Childhood Special Education, 11(4), 70-83.
16 Shanks, P.S. & Thompson, B. (1991). An overview of the rationale for integrating preschoolerswith severe disabilities into mainstream preschool/child care programs. Lawrence, KS: Univer-sity of Kansas, Dept. of Special Education.
17 Templeman, T.P., Fredericks, H.D.B. & Udell, T. (1989). Integration of children with moderateand severe handicaps into a daycare center. Journal of Early Intervention, 13(40), 315-328.
18 Chandler, L.K. & Dahlquist, C.M. (1999). The effects of team-based functional assessment onthe challenging and appropriate behaviour of children in preschool classrooms. In S.H. Irwin,Challenging the challenging behaviors. NS: Breton Books, 27-30. See also: Chandler, L.K. &Dahlquist, C.M. (1998/9). Integration in the preschool for children with mild or moderate dis-abilities. In M. Coutinho & A. Repp (eds.). Inclusion: The integration of students with disabilities,206-235. USA: Wadsworth Publishing Company.
19 Childcare Resource and Research Unit (1999). Early childhood care and education in Canada:The provinces and territories. Toronto: Childcare Resource and Research Unit, Centre for Urbanand Community Studies, University of Toronto.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada50
20 Ferguson, E., McCormick, T., Singleton, C. & Soave, A. (1999). The partners in practice mentoringmodel: Reflection, caring, & sharing. Halifax: Partners in Practice.
21 Goss-Gilroy, Inc. (1998). Component D: Curriculum analysis. Child care sector study: Tech-nical appendices (draft). (Unpublished report prepared for the Child Care Sector Steering Com-mittee.)
22 Dinnebeil, L.A., McInerney, W., Fox, C. & Juchartz-Pendry, K. (1998). An analysis of theperceptions and characteristics of childcare personnel regarding inclusion of young childrenwith special needs in community-based programs. Topics in Early Childhood Special Education,18(2), 118-128.
23 Peck, C.A., Hayden, L., Wandschneider, M., Peterson, K. & Richarz, S. (1989). Development ofintegrated preschools: A qualitative inquiry into sources of resistance among parents, adminis-trators, and teachers. Journal of Early Intervention, 13(4), 353-364.
24 Bricker, D.D. (1995). The challenge of inclusion. Journal of Early Intervention, 19(3), 179-194.
25 Garvar-Pinhas, A., et al. (1989).
26 Kontos, S. & Diamond, K. (1997). Preparing practitioners to provide early intervention ser-vices in inclusive settings. In P. Winton, J. McCollum & C. Catlett (eds.), Reforming personnelpreparation in early intervention. Baltimore: Brookes, 393-410.
27 Stoiber, K. A., et al. (1998).
28 Bricker, D. (1995).
29 Eiserman, W.D., et al. (1995).
30 Gemell-Crosby, S. & Hanzlik, J.R. (1994). Preschool teachers’ perceptions of including chil-dren with disabilities. Mental Retardation and Developmental Disabilities, 29(4), 279-290.
31 Johnson, K.M. & Johnson, J.E. (1993). Rejoinder to Carta, Atwater, Schwartz, and McConnell.Topics in Early Childhood Special Education, 13(3), 255-273.
32 Stoiber, K. A., et al. (1998).
33 Bochner, S., et al. (1990).
34 Early Childhood Educators of British Columbia (ECEBC) (1997). Children with nursing sup-port needs: Recommended practices for the child care field (2nd ed.). BC: ECEBC. (T. Norton,author.)
35 Irwin, S.H. (1992). Increasing enrollment of preschool children with special needs in regulardaycare programs through a peer-coaching, systems change approach. ERIC document.
36 Norton, T. (1991). Exceptional health care, phase I: Centre and staff needs assessment. BC:Fraser North Childcare Issues Society.
37 Heston, M.L., Raschke, D., Kliewer, C., Fitzgerald, L.M. & Edmiaston, R. (1998). Transform-ing teacher preparation in early childhood education: Moving to inclusion. Teacher Educationand Special Education, 21(4), 278-292.
38 Frankel, E.B. (1994). Resource teachers in integrated children’s centres: Implications for staffdevelopment. The International Journal of Early Childhood, 26(2), 13-20.
39 In 1996-7, when the A Matter of Urgency data was collected, only 24% of centre staff whoidentified themselves as resource teachers had a credential or certificate related to inclusion;although many more now have had a course or some coursework in their preservice college oruniversity program.
40 Powell, D.R. & Dunn, L. (1990). Non-baccalaureate teacher education. In B. Spodek, & O.N.Saracho (eds.), Yearbook in early childhood education, volume 1: Early childhood teacherpreparation, 45-66. New York: Teachers College Press.
LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 51
41 Early Childhood Educators of British Columbia (ECEBC). (1997).
42 Irwin, S.H. (1991). “Trach” — It rhymes with “Snake.” In The SpeciaLink book (1993). NS:Breton Books.
43 Norton, T. (1991).
44 Kwok, A. & Robinson, E. (1997). The partnership project. BC: Ministry for Children and Fami-lies, Province of British Columbia.
45 Jocelyn, L.J., Casiro, O.G., Beattie, D., Bow, J. & Kneisz, J. (1998). Treatment of childrenwith autism: A randomized controlled trial to evaluate a caregiver-based intervention programin community day-care centers. Developmental and Behavioral Pediatrics, 19(5), 326-334. Seealso: Autism in the Mainstream — A Team Approach on the video, The Mainstream is the RightStream. Available from SpeciaLink.
46 Palsha, S.A. & Wesley, P.A. (1998). Improving quality in early childhood environments throughon-site consultation. Topics in Early Childhood Special Education, 18(4), 243-253.
47 Van Raalte, D.L. (in process). Keeping the door open: Enhancing and maintaining the capacityof centres to include all children. For information, write to project coordinator at 310 MainStreet, Fredericton, NB E3A 1E4.
48 Beach, J. & Bertrand, J. (1997). Our child care workforce: From recognition to remuneration:Innovative training programs in early childhood care and education: Selected case studies. Ot-tawa: Canadian Child Care Federation.
49 Johnson, L., Johnson, P., MacMillan, R.P. & Rogers, C. (1993). EC-SPEED: Early Childhoodspecial education program design and evaluation guide. OH: The Ohio Department of Educationand the Northcentral Ohio Special Education Regional Resource Center.
50 Dinnebeil, L.A., et al. (1998).
51 Eiserman, W.D., et al. (1995).
52 Johnson, K.M. & Johnson, J.E. (1993).
53 Munby, H. & Hutchinson, N. (1998). Using experience to prepare teachers for inclusive class-rooms: Teacher education and the epistemology of practice. Teacher Education and SpecialEducation, 21(2), 75-82.
54 Stoiber, K. A., et al. (1998).
55 Peck, C.A., et al. (1991).
56 Dinnebeil, L.A., et al.(1998).
57 Stoiber, K. A., et al. (1998).
58 Dinnebeil, L.A., et al. (1998).
59 Bochner, S., et al. (1990).
60 Denholm, C.J. (1990).
61 Frankel, E.B. & McKay, D. (1990). An interactive model of integration in community-basedchild care centres. Paper presented at the 68th Annual Convention, Council of ExceptionalChildren, Toronto, ON. ERIC Document #ED 334 774.
62 Peck, C.A., Killen, C.C. & Baumgart, D. (1989). Increasing implementation of special educa-tion instruction in mainstream preschools: Direct and generalized effects of nondirective con-sultation. Journal of Applied Behaviour Analysis, 22(2), 197-210.
63 Denholm, C.J. (1990).
64 Eiserman, W.D., et al. (1995).
65 Garvar-Pinhas, et al. (1989).

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada52
66 Dinnebeil, L.A., et al. (1998).
67 Gettinger, M., Stoiber, K.C., Goetz, D. & Caspe, E. (1999). Competencies and training needsfor early childhood inclusion specialists. Teacher Education and Special Education, 22(1), 41-54.
68 Bailey, D.B., McWilliam, R.A., Buysse, V. & Wesley, P. (1998). Inclusion in the context ofcompeting values in early childhood education. Early Childhood Research Quarterly, 13(1), 27-47.
69 Buysse, V., Wesley, P.W. & Keyes, L. (1998). Implementing early childhood inclusion: Barrierand support factors. Early Childhood Research Quarterly, 13(1), 169-184.
70 Eiserman, W.D., et al. (1995).
71 Irwin, S.H. (1991).
72 Johnson, K.M. & Johnson, J.E. (1993).
73 Odom, S.L. & McEvoy, M.S. (1990). Mainstreaming at the preschool level: Potential barriersand tasks for the field. Topics in Early Childhood Special Education, 10(2), 48-61.
74 Norton, T. (1991).
75 Peck, C.A., Hayden, L., Wandschneider, M., Peterson, K. & Richarz, S. (1989). Development ofintegrated preschools: A qualitative inquiry into sources of resistance among parents, adminis-trators, and teachers. Journal of Early Intervention, 13(4), 353-364.
76 Stoiber, K. A., et al. (1998).
77 Buysse, V., et al. (1998).
78 Individuals with Disabilities Education Act (IDEA). See also, Knoblauch, B. (May 1998). Rightsand responsibilities of parents of children with disabilities. ERIC Digest E567.
79 Buysse, V., et al. (1998).
80 Allred, K.W., Briem, R. & Black, S.J. (1998). Collaboratively addressing needs of young chil-dren with disabilities. Young Children, 53(5), 32-36.
81 Bailey, D.B. & Winton, P. (1987). Stability and change in parents’ expectations aboutmainstreaming. Topics in Early Childhood Special Education, 7(1), 73-88.
82 Reichart, D.C., Lynch, E.C., Anderson, B.C., Svobodny, L.A., Dicola, J.M. & Mercury, M.G.(1989). Parental perspectives on integrated preschool opportunities for children with handi-caps and children without handicaps. Journal of Early Intervention, 13(1), 6-13.
83 Bailey, D. B. & Winton, P. (1987).
84 Blacher, J. & Turnbull, A.P. (1983). Are parents mainstreamed? A survey of parent interac-tions in the mainstreamed preschool. Education and Training of the Mentally Retarded, 18(1),10-16.
85 Bailey, D. B. & Winton, P. (1987).
86 Reichart, D. C., et al. (1989).
87 Bailey, D. B. & Winton, P. (1987).
88 Turnbull, A. P. & Winton, P. (1983). A comparison of specialized and mainstreamed pre-schools from the perspective of parents of handicapped children. Journal of Pediatric Psychol-ogy, 8(1), 57-71.
89 Blacher, J. & Turnbull, A.P. (1983).
90 Garvar-Pinhas, A. & Pedhazur Schmelkin, L. (1989).
91 Kagan, S. & Bowman, B.T. (1997). Leadership in early care and education. Washington: Na-tional Association for the Education of Young Children.

LITERATURE REVIEW: THE ROLE OF STAFF ATTITUDE ON EFFECTIVE INCLUSIONCHAPTER 3 53
92 Mitchell, A. (1997). Reflections on early childhood leadership development: Finding your ownpath. In S.L. Kagan & B.T. Bowman (eds.), Leadership in early care and education. Washington:National Association for the Education of Young Children, 85-94. (Website: http:/www.naeyc.org/naeyc)
93 Jorde-Bloom, P. (1997). Commentary. In S.L. Kagan & B.T. Bowman, (eds.), Leadership inearly care and education, 34-37. Washington, D.C.: National Association for the Education ofYoung Children.
94 Espinosa, L.M. (1997). Personal dimensions of leadership. In S.L. Kagan & B.T. Bowman(eds.), Leadership in early care and education, 97-102. Washington, D.C.: National Associationfor the Education of Young Children.
95 Jorde-Bloom, P. (2000). How do we define director competence? Child Care Information Ex-change, 3/00, 13-18.
96 Neugebauer, R. (1981, Sept/Oct). Piaget’s theory of director development. Child Care Informa-tion Exchange, 1-5.
97 VanderVen, K. (1993). Military strategy and the economic base of child care: A radical pro-posal for our future. (From the 1987 Albert E. Trieschman Memorial Conference.) Condensedversion in The SpeciaLink book, 69-86. NS: Breton Books. Full 19-page article available fromSpeciaLink.
98 VanderVen, K. (1990). The relationship between notions of caregiving held by early childhoodpractitioners and stages of career development. In B. Po-King Chan (ed.), Early childhood towardthe 21st century: A worldwide perspective, 245-255. Hong Kong and Gaithersberg, MD: YewChung Education Publishing Company.
METHODOLOGYCHAPTER 4 55
about the factors that may have af-fected child care professionals’ at-titudes and perceived competen-cies, including any additional train-ing they may have taken, as wellas the kinds of experiences theyhave had working with childrenwith special needs in inclusive childcare programs. We also wanted tocompare child care practitioners’current attitudes to those obtainedfrom an earlier sample of child careprofessionals who were surveyed in1990. Finally, because we were in-terested in understanding direc-tors’ and child care staff’s experi-ences with inclusion from an eco-logical perspective, it was desirableto try to obtain information fromthe perspectives of both front-lineteaching staff and directors whowere involved together in the samechild care program, along with ad-ditional information about eachcentre as an organizational envi-ronment, itself functioning in aparticular context bounded by ac-cess to community resources tosupport inclusion, and affected byprovincial policies and constraints.
These criteria suggested that a pre-ferred sampling approach would beone that could allow us to obtaincomplementary data from pairs ofdirectors and front-line staff whoworked in centres that had somehistory of enrolling children withspecial needs, ideally for some time.In effect, we were interested in
4.1 INTRODUCTION
This chapter provides informationabout the sampling approach usedin this study; response rates; thedevelopment and content of ques-tionnaires for centre directors,front-line staff, and travelling re-source teachers/resource consult-ants; and data analysis proce-dures. Chapter 5 will describe theobtained samples of centres, cen-tre directors and selected front-lineteaching staff in those centres, anda separate sample of travelling re-source teachers/resource consult-ants who provided an external per-spective on inclusion in child careprograms.
4.2 ISSUES THAT AFFECTED OURSAMPLING APPROACH
The specific sampling proceduresutilized in this study were deter-mined on the basis of several crite-ria — particularly their suitabilityfor study purposes, as well as thelack of an existing national sam-pling frame of centres that provideinclusive care. In order to addressthe goals and objectives outlined inChapter 1, it was important to ob-tain information from front-lineteaching staff and directors whohad been involved for several yearsin providing early childhood edu-cation and care to children withspecial needs. This criterion wasessential, since we wanted to learn
METHODOLOGY 4.Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada56
studying a somewhat select groupof child care professionals — thosewhose experiences might be mostuseful for providing us with infor-mation that would be relevant topolicy and practice implications.
The researchers recognized at thetime the study was proposed thatno existing national samplingframe existed that would suit thesepurposes. Nor could provincial/ter-ritorial governments supply a listof centres that met our criteria.Some provincial governmentsmight have been able to provide alist of centres that were then re-ceiving specialized funding orgrants to support inclusion, butwithout any assurance that theprograms had done so for any par-ticular period of time. Moreover,those lists were not immediately ac-cessible nor up to date. Because wehad no idea how common or howrare experience with inclusion wasin 1996, the prospect of a multi-stage screening process that wouldhave involved contacting a randomsample of centres in each provincewas deemed unsuitable.
Fortunately, another option wasavailable that was very well suitedto our objectives. This option wasto follow up participants from anearlier, related survey and to addto that sample selectively. In 1990SpeciaLink conducted a survey ofchild care practitioners’ attitudestowards inclusion. The survey wasbased on an obtained sample of489 child care professionals, in-cluding 123 ECEs, 61 resourceteachers or special needs workers,and 143 directors from acrossCanada, all of whom had some ex-perience in providing care to chil-dren with special needs. The origi-nal sample frame from which the1990 sample was obtained con-sisted of directors in child care pro-
grams who were deemed eligible toinclude children with special needsand/or to receive special fundingfor that purpose by the provincialor territorial government.
In the earlier study each eligiblecentre was sent two questionnairesand two letters — one with a coverletter addressed to the centre di-rector and the other intended forthe “most experienced” staff mem-ber in half the centres and the“least experienced” permanent staffmember in the other half. At thetime, 1697 surveys were originallydistributed to centre directors andstaff, including a small group ofchild care specialists in advisoryroles, such as resource consult-ants, directors of early interventionprograms, and local coordinatorsof services. Of the 548 returnedquestionnaires, 489 were includedin analysis (approximately 36% ofthose mailed out). The final sampleincluded participants from all prov-inces and territories.
Since one objective of the currentstudy was to see if child care pro-fessionals’ attitudes towards inclu-sion had changed in the interven-ing six year period, the opportunityto re-survey participants from theearlier study was very attractive.Moreover, because SpeciaLinkmaintained a national mailing listfor the purpose of distributing anewsletter, information about con-ferences, etc., an infrastructureexisted that allowed SpeciaLink tomaintain contact with many of therespondents to the earlier study. Aquick field test of 25 directors madein early 1995 indicated that asmany as 75% of the directors whocould be contacted were still em-ployed at the same centre. As a re-sult, the study team determinedthat an appropriate sampling strat-egy would be to follow up directors

METHODOLOGYCHAPTER 4 57
and teaching staff from the earlierstudy, when possible, and to aug-ment that group to meet study pur-poses.
4.3 SAMPLE SELECTION ANDAUGMENTATION
By autumn of 1996, it was appar-ent that, partially because of bud-getary cutbacks and financial re-straints in child care, the attritionrate had increased for directors,and was likely to be even higheramong resource teachers andECEs. Hence, it would be necessaryto augment the sample of earlierparticipants we were likely to beable to contact. Moreover, the 1996survey design required, ideally, thatwe be able to pair directors andECEs/RTs in the same centres inorder to gain multiple perspectivesand see centres through parallel“windows”; a purpose that requiredefforts to ensure a dyadic match ineach centre.
Consequently, we adopted severalstrategies to obtain a sample of Di-rector-ECE or Director-RT pairs incentres that had a history of includ-ing children with special needs. Foreach director, ECE, or RT we couldtrack from the earlier sample, and/or for each centre in which a 1990participant had been located, weendeavoured to add her/his coun-terpart. Where we could success-fully locate a director, ECE or RTin the same centre they had beenin before, we also tried to add acomplementary respondent for the1996 sample; i.e. pairing a newECE/RT with a 1990 director anda new director with a 1990 ECE/RT.
In an attempt to include as manyoriginal respondents as possible,we “followed” 1990 respondents to
their new centres, if they remainedin the field and they could be lo-cated. For example, if a directormoved from Centre A to Centre B,we called Centre B, spoke with thedirector about participating in the1996 follow-up study, AND askedfor the name of an appropriateECE/RT at Centre B. As well, if aparticipant was no longer workingat her 1990 centre, we attemptedto replace her with her occupa-tional replacement – a director fora director; an ECE or RT for anECE or RT (in this example, add-ing the director in Centre A toreplace the director who hadmoved on). An additional stipula-tion was that the replacementECE/RT was to be the newest per-manent member of that centre’sstaff complement of ECEs or RTsbecause our original sample hadattempted to include both the“most senior” and “the newest”front-line staff, and we wanted toensure some diversity within thepopulation in terms of length oftime in the field and/or centre. Ob-viously, by 1996 staff who hadbeen the newest in 1990 were nowfairly senior.
Although opportunities for promo-tions are limited in the child carefield, ECEs/RTs and directors dooccasionally move up the occupa-tional ladder. ECEs/RTs becomedirectors; some directors becomegovernment officials, trainers, etc.We followed respondents into theirnew positions within the field,pairing them at new centres andreplacing them (and pairing theirreplacements) at their original cen-tres. If any 1990 respondents hadbecome travelling RTs or consult-ants, we included them as mem-bers of that third category in ournew sample.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada58
4.4 OUR OBTAINED SAMPLES
The process of sample selection andaugmentation took place in Octo-ber of 1996. Following telephonecontacts with 1990 participants intheir new and old locations andcontacts with new directors in cen-tres that had been represented inthe earlier study, survey question-naires were mailed to 177 directors,181 Early Childhood Educators(ECEs) and in-house ResourceTeachers (RTs), and 32 TravellingResource Teachers/ResourceConsultants ( TRTs/RCs).
Tables 4.1, 4.2, and 4.3 provide in-formation on response rates. Re-sponse rates were quite high: 81%for directors, 70% for ECEs andRTs, and 78% for TRTs/RCs. Theserates were adjusted when 12 sur-veys were found to be incompleteor missing vital information, result-ing in final response rates of 76.8%
for directors, 68.5% for ECEs andRTs and 71.9% for TRTs/RCs — afinal overall response rate of 72.6%across all three groups. We weresuccessful in obtaining completedata from 106 pairs of directors andECEs/RTs who worked together inthe same centres. Responses wereobtained from an additional un-matched 30 directors and 18 ECEs/RTs. In this report, all surveys wereanalysed. A second report based onpaired data analyses will be releasedseparately.
Consequently, our final samplesfrom which data are analysed in thisreport consisted of 136 directors ofchild care centres, 124 ECEs andRTs, and 23 TRTs/RCs. Of the 136directors, 62 (46%) had participatedin the 1990 study. Only 27 of the124 ECEs and RTs (21.8%) had par-ticipated in the 1990 study. Eigh-teen of the 23 TRTs/RCs (78%) hadparticipated in 1990, including ten
Province/ Questionnaires Number Number Final Percent FinalTerritory Mailed Out Received Unusable Sample Received Response Rate
NF 4 4 0 4 100.0% 100.0%PE 7 7 0 7 100.0% 100.0%NS 9 9 1 8 100.0% 88.9%NB 4 3 0 3 75.0% 75.0%QC 55 34 2 32 61.8% 58.1%ON 39 37 3 34 94.9% 87.1%MB 17 16 1 15 94.1% 88.2%SK 11 6 0 6 54.5% 54.6%AB 16 14 0 14 87.5% 87.5%BC 13 11 0 11 84.6% 84.6%YT 2 2 0 2 100.0% 100.0%NT 0 0 0 0TOTAL 177 143 7 136 80.8% 76.8%
Table 4.1
Response Rates from Directors of Child Care Centres

METHODOLOGYCHAPTER 4 59
Province/ Questionnaires Number Number Final Percent FinalTerritory Mailed Out Received Unusable Sample Received Response Rate
NF 0 0 0 0PE 0 0 0 0NS 1 1 0 1 100.0% 100.0%NB 2 1 0 1 50.0% 50.0%QC 0 0 0 0ON 17 13 1 12 76.5% 70.6%MB 1 1 0 1 100.0% 100.0%SK 0 0 0 0AB 4 3 1 2 75.0% 50.0%BC 4 3 0 3 75.0% 75.0%YT 2 2 0 2 100.0% 100.0%NT 1 1 0 1 100.0% 100.0%TOTAL 32 25 2 23 78.1% 71.9%
Table 4.3
Response Rates from Travelling Resource Teachers/Resource Consultants
Table 4.2
Response Rates from ECEs and In-House Resource Teachers
Province/ Questionnaires Number Number Final Percent FinalTerritory Mailed Out Received Unusable Sample Received Response Rate
NF 2 2 0 2 100.0% 100.0%PE 6 5 0 5 83.3% 83.3%NS 8 7 0 7 87.5% 87.5%NB 4 4 0 4 100.0% 100.0%QC 55 26 0 26 47.3% 47.3%ON 39 37 1 36 94.9% 92.3%MB 18 13 1 12 72.2% 66.7%SK 9 4 0 4 44.4% 44.4%AB 19 12 1 11 63.2% 57.9%BC 18 14 0 14 77.8% 77.8%YT 2 2 0 2 100.0% 100.0%NT 1 1 0 1 100.0% 100.0%TOTAL 181 127 3 124 70.2% 68.5%

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada60
who had been directors in 1990,four who had been ECEs or In-house RTs, and four who had beenresource consultants at that time.
4.5 QUESTIONNAIREDEVELOPMENT ANDDESCRIPTIONS
Three separate questionnaireswere designed by the co-investiga-tors. Successive drafts were re-viewed by the study team to ensurethat we would be collecting dataappropriate for the study’s objec-tives. All three questionnaires con-tain sections that cover demo-graphic information and some in-formation about the participant’srole functions. Thus, directors wereasked if they also had teaching re-sponsibilities or were mainly ad-ministrative directors; ECEs andIn-house RTs were asked abouttheir position and the children forwhom they had primary responsi-bility. Because little is known abouttravelling resource teachers and re-source consultants, several ques-tions were included that probed thenature of their role functions. Allthree questionnaires included thesame questions or items to assess:
✦ attitudes about including chil-dren with various special needs orconditions in regular preschool orchild care programs, based on ascale originally developed byBochner, Denholm, & Pieterse(1990)1
✦ general beliefs about inclusion,developed by the authors for thisstudy, and
✦ questions which asked respon-dents if they felt they had changedtheir views and attitudes towardsinclusion of children with specialneeds. Specifically, whether, as aresult of their experiences, they felt
they were more committed to theconcept of inclusion now or lesscommitted; more accepting of abroader range of children beingserved or more cautious about therange of children who can be ac-commodated in regular child careprograms; more comfortable work-ing with children with special needsthan they were before or less so.
Beyond these elements, each sur-vey questionnaire containedunique questions designed to meetstudy objectives. Both open andclosed-ended questions were used,although the latter predominated.All questionnaires were available inboth English and French. A briefdescription of each instrumentfollows. (Copies of the actual ques-tionnaires are appendixed to thisReport, as appendices A, B, and C.)
4.51 The Questionnaire for Directors
The survey questionnaire for direc-tors served as a source of infor-mation both about the directorsthemselves and about their cen-tres and centre practices relatedto inclusion. Through a variety ofquestions we attempted to obtaintwo types of information: informa-tion about current circumstances,attitudes, and practices, and in-formation about changes that hadoccurred since 1990 (or, in a fewcases, within a shorter period oftime). The director’s questionnairewas divided into five major sec-tions. The first section consistedof several demographic questionsthat included information on thedirector’s main responsibilities,length of time in their present po-sition, length of time in the childcare field, and number of yearsthey had worked with children inspecial needs in child careprograms.

METHODOLOGYCHAPTER 4 61
The second section requested infor-mation about the centre such as thenature of the program, auspice, li-censed capacity and age range ofchildren served, the number of chil-dren with special needs who were en-rolled at the time of data collection,and how the number and complex-ity of those children compared towhat was typical for the centre. Thissection also included questionsabout the centre’s experience in ac-cepting or rejecting applications ofchildren with special needs in thelast three years, and the reasonschildren had not been accepted, ifapplicable. As well, we askedwhether the participation of any ofthe children with special needs waslimited to a part-time basis for anyof several reasons.
In addition, a number of questionswere used to obtain a profile of prac-tices within the centre, includingwho among staff was involved in de-veloping Individual Program Plans(IPPs), and how communication andcoordination with parents and com-munity professionals was handled.Information on which specific re-sources were available to the centreto support inclusion was also ob-tained. These resources could in-clude additional full and/or part-time staff, resource consultants andEarly Intervention workers, specificprofessionals in the community, andstudents and volunteers.
The third section of the director’squestionnaire focussed on thedirector’s education and training,particularly related to inclusion, anddirectors’ identification of topic ar-eas on which they would like moreinformation.
Section four included the Denholmscale to assess support for inclusion,the items designed to assess beliefsand opinions about inclusion, and
questions about any change in val-ues (“Are you more or less commit-ted, accepting of a broader range ofchildren, comfortable working withchildren with special needs?”) thatwere common across the three ques-tionnaires. An additional componentin section four asked directorswhether they felt that their centrehad become more inclusive and/ormore effective in integrating childrenwith special needs since 1990. Fol-low-up questions asked directors toidentify which of ten factors had beenimportant positive contributors thatenabled the centre and staff to be-come more inclusive, as well aswhich of ten factors provided hadlimited or frustrated the centre’s ca-pacity to be inclusive or more effec-tive in integrating children with spe-cial needs. The option to write inother factors besides those listed wasprovided.
The last section in this questionnaireasked directors to identify whetherthey had experienced any reductionsin funding or support services thathad begun to affect their program’scapacities to include children withspecial needs in the year precedingdata collection. Six specific kinds ofreductions or limits were queried,including three that related to gen-eral support for child care programsand/or the base level of quality (suchas lower morale and increased turn-over among teachers in the centre),and three were items that relatedmore specifically to support for in-clusion (funding or subsidies for chil-dren with special needs, and accessto PT/OT, speech and language spe-cialists, etc.).
4.52 The Questionnaire for ECEs andIn-House Resource Teachers
The survey questionnaire for ECEsand in-house RTs (together referred

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada62
to as front-line staff) consisted ofsix sections. The first section of de-mographic questions parallelledthose asked in the director’s ques-tionnaire, as did the second sec-tion that focussed on therespondent’s education and train-ing with some slight modifications.The third section duplicated thequestions about attitudes and be-liefs described previously.
The main focus in section four waschild care staff’s direct experienceswith inclusion, including what hadbeen some of their most success-ful and some of their most frustrat-ing experiences. Questions in thissection asked respondents to recalla situation in the last two years inwhich they felt they had been mostsuccessful in effectively includinga child with special needs in theirgroup. With regard to that circum-stance, we asked teachers to indi-cate what resources had helpedthem work successfully with thischild, and in what areas they feltthey had been most successful. Wealso asked what teachers foundmost frustrating or problematic intheir work with that same child, byproviding a set of issues or catego-ries in which they may have expe-rienced some frustration or diffi-culty. Other questions in this sec-tion were open-ended and enabledrespondents to tell us what re-sources they feel would have helpedthem to work more effectively inthis situation, as well as what frus-trations or problems they encoun-tered in at least one other situa-tion in which they were less suc-cessful.
Section five in the questionnaire forECEs and in-house RTs containeditems on which respondents couldindicate their sense of confidencein their knowledge and abilities, re-
flecting a sense of efficacy orcompetence, and items on whichthey felt they needed to improve.
Section six was important in that itspecifically asked respondents whatthey felt had changed for them ortheir centre in the last few years.Specifically, we inquired about thecomplexity of children’s needs, stafftime provided for planning/consult-ing, effectiveness of centre staff inworking together as a team withinthe program, the availability andinvolvement of resource teachers,integration workers and others, andtheir own competencies and knowl-edge base. In each instance, weasked what had increased or im-proved, not changed, or decreasedor declined. This section providedan interesting parallel to the infor-mation obtained from directorsabout changes in their program’s ef-fectiveness with inclusion.
4.53 The Questionnaire for TravellingResource Teachers & Consultants
The questionnaire for TRT/RCsconsisted of six sections. The firstsection contained some general de-mographic questions, includinglength of experience in the child carefield, and as a resource teacher orresource consultant. The secondsection on education and trainingwas similar to that used in the ques-tionnaires designed for the other twogroups, although two unique ques-tions inquired about therespondent’s interest in a variety oftopics for additional training, work-shops and information sharing, aswell as whether respondents hadcontact with other RTs and RCs forinformation and support when de-sired. The third section containedthe Denholm attitude items and ourquestions that gauged beliefs aboutinclusion.

METHODOLOGYCHAPTER 4 63
The fourth section of this question-naire was developed specifically forthis study and for this sample. Itincluded ten questions that in-quired about TRT/RCs’ primary re-sponsibilities in their communitiesand in the child care centres theyvisited. Three additional questionsin this section probed respondents’views about centres’ capacities tobe inclusive. Specifically, respon-dents were asked to consider thecentres and preschool programsthey visited regularly and to indi-cate what proportion of those pro-grams they felt were extremely ef-fective in including children withspecial needs, doing a reasonablygood job, or struggling with inclu-sion. Two follow-up questionsasked TRT/RCs to indicate whichof 11 possible features of directors,centres and staff they felt weremost important for distinguishingcentres that had been extremely ef-fective with inclusion from othercentres, and centres that are strug-gling with inclusion from other cen-tres. An opportunity was providedfor open-ended comments and ad-ditional suggestions in both cases.
Section five in this questionnaireasked respondents to indicate howconfident and competent they feelabout their abilities in a numberof areas which we considered rel-evant to their role. These items in-cluded some that related to theircapacities to work with childrenwith special needs; to workcollaboratively with parents, and asteam members with ECEs; and toprovide workshops and informa-tion to ECEs and others.
Section six asked respondentsabout changes they had experi-enced themselves in the last fewyears or that they had observedamong the centres they visited (in-
creases or improvements, de-creases or declines, and instanceswhere there was no change). Itemsincluded the complexity ofchildren’s special needs, theircaseload size, the effectiveness ofcentre staff in working together asa team within their program, thestress level and need for supportamong child care staff, as well asother items.
4.6 PRETESTING
Pretesting of first versions of allthree questionnaires was carriedout with the cooperation of direc-tors and ECEs in British Columbia,Alberta, Manitoba, and Nova Scotia,as well as several directors and stafflocated in Guelph, Ontario. In to-tal, pretest responses with valuablesuggestions for revision were re-ceived from nine directors, eightECEs, and four in-house RTs. Sixtravelling resource teachers/con-sultants, including the coordinatorof a local resource teacher network,provided advice on the question-naire for TRT/RCs. All pretestingwas done in September-October of1996, with modifications made im-mediately thereafter.
4.7 DATA COLLECTIONPROCEDURES
In the first week of November 1996,packages containing an explana-tory letter, the appropriate ques-tionnaire (either Director, ECE/RTor TRT/RC), and a stamped ad-dressed return envelope weremailed to all potential respondents(in either French or English). “Onedozen lobsters—delivered” was of-fered as an incentive, through adraw from the names of respon-dents who wished to be considered.Since most respondents to the

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada64
1990 survey had been located orreplaced by the current employeein their positions and some tele-phone contact had been part ofthat process (see Section 4.4, “OurObtained Samples”), we felt con-fident that very few “address un-knowns” would appear. If the“identified respondent” was a di-rector who had agreed to recruitan appropriate ECE/RT, bothquestionnaires and letters weresent to the director, with two sepa-rate return envelopes. Threeweeks later, a reminder note wassent to all potential participantswho had not yet responded. Sixweeks later (after Christmas) a fol-low-up telephone call was madeto all potential participants whohad not responded to the re-minder. At that time, we learnedof missing or misplaced question-naires, of job changes, and of afew unavoidable delays. Addi-tional copies of the questionnaireswere sent out, as requested, andwe did our best to answer anyquestions or concerns that mighthave resulted in delayed re-sponses. All questionnaires weretreated as confidential. This three-step process brought our responserate to 81% for directors, 70% forECEs and R Ts, and 78% forTRTs/RCs. (Incomplete or miss-ing data in 12 questionnaires re-duced these rates slightly).
4.8 PREPARATION FOR DATAANALYSIS
Coding of each questionnaire wascarried out according to detailedcoding manuals that were devel-oped at the University of Guelph.All open-ended questions were en-tered verbatim and longer lists ofcodes were condensed based onconsensus among the co-investiga-tors. We particularly appreciatedthe diligent assistance provided byLaura Coulman, an M.Sc. studentin the Department of Family Rela-tions and Applied Nutrition at theUniversity of Guelph. Derived vari-ables were specified and scales con-structed where appropriate. TheDenholm items on attitudes to-wards including a range of childrenin regular child care programs wereused both individually and to yielda scale score for each individual.Statistical analysis indicated thatthese items loaded on one generalfactor. Inter-item consistency coef-ficients were computed on the atti-tude scale scores, yielding Kuder-Richardson Reliability coefficients of.96 for the directors and .98 for ECEsand In-House RTs. The Beliefs itemstapped more than one dimension,hence construction of a single Beliefsscore was not justified. All analysiswas done at the University of Guelphusing SPSS8 on the University’smainframe computer.
END NOTES
1 Bochner, S., Denholm, C.J. & Pieterse, M. (1990). Attitudes to integration in preschool: Acomparative study of preschool directors in Canada and Australia. Victoria, BC: University ofVictoria, School of Child and Youth Care. See also Denholm, C.J. (1990). Attitudes of BritishColumbia directors of early childhood education centres towards the integration of handicappedchildren. British Columbia Journal of Special Education, 14 (1), 13-26.

CHAPTER 5 DESCRIPTIVE INFORMATION ABOUT THE CENTRES, STAFF & DIRECTORS 65
5.1 INTRODUCTION
As described in Chapter 4, Meth-odology, the centres, directors, andteaching staff included in thisstudy were selected based on par-ticular criteria — specifically, eithertheir participation in the 1990SpeciaLink study of inclusive childcare programs,1 or the likelihoodthat they had been involved in pro-viding inclusive child care for someyears. As a result, the centres andchild care professionals in thissample form a unique referencegroup. They were not selected to bea representative sample, fromwhich population estimates couldbe inferred; consequently, it is im-portant to understand the natureof our samples in order to mean-ingfully interpret the findings.
In this chapter, we outline some ofthe general and demographic char-acteristics of the centres, teachingstaff, and directors in our sample.At the end of each section of thechapter, we compare our centres,staff, and directors to recent, na-tional profiles drawn from informa-tion available from provincial/ter-ritorial governments and from therecently completed You Bet I Care!national study.2
DESCRIPTIVE
INFORMATION ABOUT THE CENTRES,STAFF AND DIRECTORS IN OUR SAMPLE
5.
5.2 OUR CHILD CARE CENTRES
5.21 Location
While not a statistically represen-tative sample, the 136 child careprograms included in our samplewere drawn from all regions ofCanada, spanning large urban ar-eas, small towns and rural commu-nities. Of the 136 centres includedin the sample, 22 (16.2%) werefrom the Atlantic Provinces; 32(23.5%) were from Québec; 34(25.0%) were from Ontario; 35(25.7%) were located in one of thePrairie provinces of Manitoba,Saskatchewan or Alberta; 11 (8.1%)were from British Columbia; and 2programs (1.5%) were located in theYukon Territories.
5.22 Centre Type
Centre directors were asked to de-scribe their program as a special-ized centre for children with spe-cial needs, a centre designated asintegrated or one that has con-tracted spaces, a regular child carecentre with no designation, or ahalf-day preschool program. Infact, some checked off both half-day preschool and one of the other
Donna S. Lero, Kathleen Brophy, Sharon Hope Irwin

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada66
categories. Upon consolidation, wefound that of the 136 programs, 11(8.1%) were specialized centresthat, most often, included bothchildren with disabilities and typi-cally developing children, 62(45.6%) were centres that describethemselves as designated as inte-grated or one that has contractedspaces for children with specialneeds, and 63 (46.3%) were “regu-lar” day care centres and/or half-day programs with no particulardesignation.
The description directors providefor their programs is important,
both because it suggests differentmandates as the centres have de-veloped over the years and often dif-ferential funding, and because thedirector’s description is indicativeof the centre’s identity in the com-munity. Thus, while “regular” and“integrated” centres may both in-clude the same number of childrenwith special needs, the notion thatone identifies oneself, and is iden-tifiable in the community, as an in-tegrated centre may be a criticalindicator of the director’s andstaff’s commitment to having a con-tinuing role in providing inclusiveearly childhood education andcare.3
The distribution of programs bycentre type varied considerablyamong the provinces — in largepart reflecting the history of pro-gram development and the natureof provincial/territorial policies andfunding arrangements related to in-clusion. Both designated and regu-lar programs were located in everyprovince and territory in oursample. Regular programs ac-counted for more than 75% of thecentres sampled from Newfound-land, Québec, and Manitoba; whileprograms designated as integratedpredominated among centres inNew Brunswick, Ontario, andAlberta. Specialized programs weremostly found in Ontario (six of theeleven programs), with two eachfrom Nova Scotia and British Co-lumbia, and one in Manitoba.Seven of the eleven specialized pro-grams were integrating typicallydeveloping children into their pro-grams, and in some cases hadmultiple component services, suchas an integrated half-day preschoolthat operated alongside specializedtherapeutic and consultationservices.
8%Specialized
45%Designated
orContracted 47%
Regular
Figure 5.1
Child Care Centre Types

CHAPTER 5 DESCRIPTIVE INFORMATION ABOUT THE CENTRES, STAFF & DIRECTORS 67
5.23 Centre Size, Full or Part DayPrograms, Age of ChildrenServed, and Auspice
Directors reported that the num-ber of children their centre was li-censed for ranged from as few as10 children to more than 150, witha median of fifty. Seventy percentof specialized programs were li-censed for thirty children or fewer,while the majority of designatedand regular programs were li-censed for 31-60 children. In total,90% of specialized programs, 59%of designated programs, and 76%of regular programs were licensedfor 60 children or less, while 10%of specialized, 41% of designated,and 24% of regular programs couldaccommodate more than 60 chil-dren.
Of 120 programs who provided in-formation, almost 16% offered onlypart-time care and 12% offeredonly full-time care. The majority(72.5%) appeared to be providingcare on both a full and part-timebasis. Designated and regular pro-grams were most likely to provideboth full and part-time care, whilespecialized programs were morelikely to offer only part-time care.
While the most common age rangeof children served in individual pro-grams was 2-5 years, the programsin our sample included infants asyoung as three months old toschool age children up to and in-cluding 12 year olds. Two centresaccommodated children older thantwelve years of age.
✦ 65% of programs provided in-fant and toddler care to childrenunder two years of age, includingforty programs (29%) that offeredcare to infants younger than 12months old.
✦ 28% of the programs accom-
modated school age children olderthan 6 years of age.
Inclusion of children with diverseability levels may actually be moreeasily accommodated in such pro-grams.
Only 13 of the 136 programs in oursample described themselves asprivate or commercial. The largemajority (90%) are non-profit cen-tres, including two centres that aremunicipal/regional centres.
5.24 A Glimpse of Child CareInclusion
Chapter 6 provides detailed infor-mation about the nature and ex-tent of inclusion within the 136programs included in our sample.At the time data were collected, 117programs (86%) had at least onechild with identified special needsattending the centre (as per thestudy’s definition of that term),while 19 programs had no childrenwith special needs at that time. Inthe majority of those centres, thiswas an unusual or temporary cir-cumstance. The most common casefor all centres in our sample wasinclusion of one or two childrenwith identifiable special needs(26.4%). While having only one ortwo children with special needsenrolled was the most commoncase, it should be noted that onethird of the regular and designatedprograms in this study accommo-dated five or more children withspecial needs in 1996.
In addition to children with identi-fied disabilities, delays, and healthconditions, directors in 93 of thecentres in our sample (68.4%) con-firmed that they also provide edu-cation, care and support to chil-dren “at risk” or those who havesignificant delays, but are not

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada68
identified as having special needsfor funding/support purposes. Insome cases, children “at risk” maybe identified as having specialneeds at a later point, or pendingassessment. Others fall into grayareas (e.g., children with challeng-ing behaviours, more subtle lan-guage or learning difficulties, orthose whose family background isdifficult or unstable). These chil-dren frequently also require addi-tional supports or a modified cur-riculum in order to fully participatein the program, for which addi-tional funding and resources aregenerally not allocated. Programsin rural areas and those servingconcentrated populations of chil-dren and families in difficult cir-cumstances may receive more thanthe typical number of referrals,both for children with special needsand those who are not identified assuch, but who require additionalsupport and curriculum modifica-tions.
5.25 How Our Centres Compare toAvailable National Profiles
Two sources of information wereconsulted to compare our sampleto national data. The first, whichprovides information about provin-cial distribution and auspice, is thereport on the Status of Day Care inCanada, 1995 and 1996,4 whichcoincides with the time when datafor this study were collected. Thesecond source is information aboutcentres included in the final reportof the YBIC! project,5 with data col-lected in 1998.
Province and auspicecomparisons
In comparison to 1996 nationaldata, the sample of 136 centres inthis study does not dramatically
over or under-represent any prov-ince or region of the country. Oursample most over-represents cen-tres from the Atlantic provinces(16.2% of our sample compared to6.7% of the national distribution)and Manitoba (11.0% of our samplecompared to 7.8% of the nationaldistribution), and under-repre-sents centres from BritishColumbia and Ontario (which makeup 8.1% and 25.0% of our sample,respectively, compared to 17.1%and 33.6% of the national distri-bution). A more telling differenceis that 90.4% of sample centreswere from the non-profit sector (in-cluding a few municipal programs),compared to 72.6% of all centresincluded in the 1996 Status of DayCare report.
Inclusion comparisons
Data collected in 1998 for the YBIC!research project were obtainedfrom 848 centres, representing4,636 programs nationwide. Basedon that information, between63.9% and 70.1% of child care cen-tres were estimated to include atleast one child with special needs,using a definition similar to the oneused in the present study. Slightlyless than one in eight programsnationally (12.2%) reportedly in-cluded five or more children withspecial needs, compared to 39% ofour full sample, and 33.6% of regu-lar and designated programs in thesample. Just under 5% of the YBIC!centres provided specialized con-sultation to other centres, for ex-ample on the inclusion of childrenwith special needs.
“Our centre islocated in a smallrural community.We have had chil-dren with specialneeds, i.e., Down’sSyndrome,behaviour prob-lems, cerebralpalsy, Soto syn-drome, etc., in-cluded in ourprograms. Fund-ing is a problem,as subsidy is notavailable to fami-lies living in thesurrounding orga-nized townships.”
(director of a programdesignated as integrated inOntario)
“Many childrenhave undiagnosedand invisibledisabilities. Theseare often thechildren most atrisk.”(director of a specialized childcare centre in Manitoba)
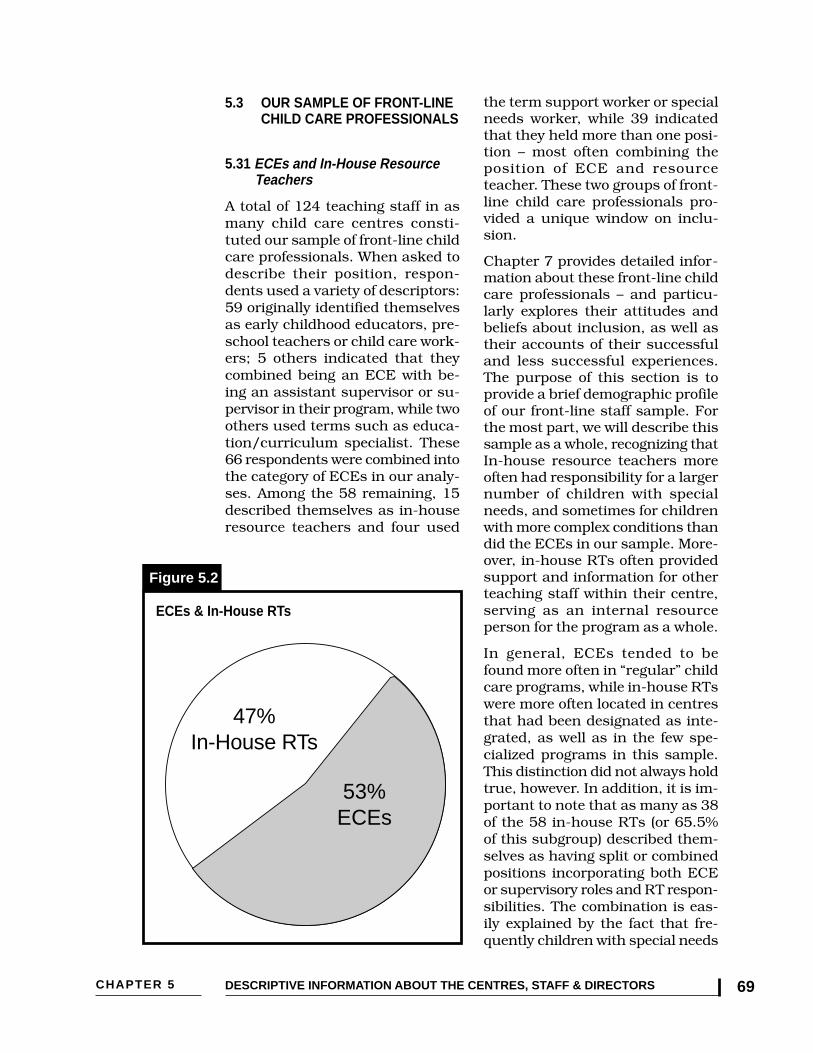
CHAPTER 5 DESCRIPTIVE INFORMATION ABOUT THE CENTRES, STAFF & DIRECTORS 69
5.3 OUR SAMPLE OF FRONT-LINECHILD CARE PROFESSIONALS
5.31 ECEs and In-House ResourceTeachers
A total of 124 teaching staff in asmany child care centres consti-tuted our sample of front-line childcare professionals. When asked todescribe their position, respon-dents used a variety of descriptors:59 originally identified themselvesas early childhood educators, pre-school teachers or child care work-ers; 5 others indicated that theycombined being an ECE with be-ing an assistant supervisor or su-pervisor in their program, while twoothers used terms such as educa-tion/curriculum specialist. These66 respondents were combined intothe category of ECEs in our analy-ses. Among the 58 remaining, 15described themselves as in-houseresource teachers and four used
the term support worker or specialneeds worker, while 39 indicatedthat they held more than one posi-tion – most often combining theposition of ECE and resourceteacher. These two groups of front-line child care professionals pro-vided a unique window on inclu-sion.
Chapter 7 provides detailed infor-mation about these front-line childcare professionals – and particu-larly explores their attitudes andbeliefs about inclusion, as well astheir accounts of their successfuland less successful experiences.The purpose of this section is toprovide a brief demographic profileof our front-line staff sample. Forthe most part, we will describe thissample as a whole, recognizing thatIn-house resource teachers moreoften had responsibility for a largernumber of children with specialneeds, and sometimes for childrenwith more complex conditions thandid the ECEs in our sample. More-over, in-house RTs often providedsupport and information for otherteaching staff within their centre,serving as an internal resourceperson for the program as a whole.
In general, ECEs tended to befound more often in “regular” childcare programs, while in-house RTswere more often located in centresthat had been designated as inte-grated, as well as in the few spe-cialized programs in this sample.This distinction did not always holdtrue, however. In addition, it is im-portant to note that as many as 38of the 58 in-house RTs (or 65.5%of this subgroup) described them-selves as having split or combinedpositions incorporating both ECEor supervisory roles and RT respon-sibilities. The combination is eas-ily explained by the fact that fre-quently children with special needs
47%In-House RTs
53%ECEs
Figure 5.2
ECEs & In-House RTs
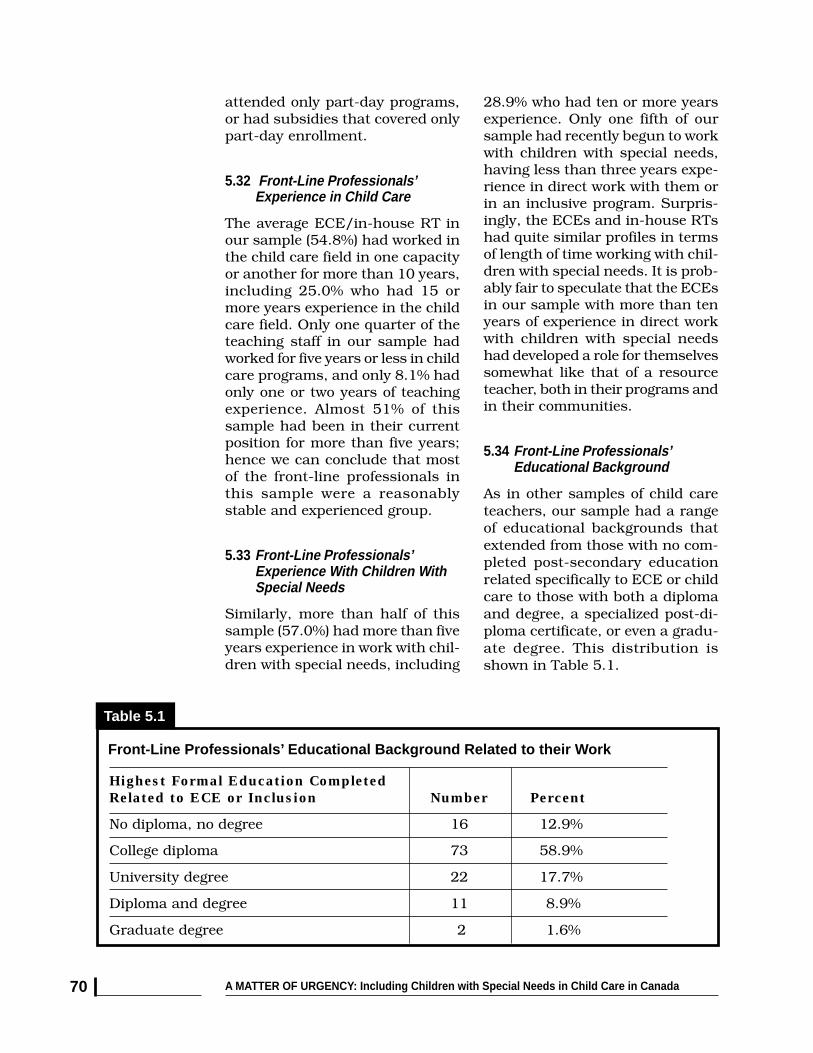
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada70
attended only part-day programs,or had subsidies that covered onlypart-day enrollment.
5.32 Front-Line Professionals’Experience in Child Care
The average ECE/in-house RT inour sample (54.8%) had worked inthe child care field in one capacityor another for more than 10 years,including 25.0% who had 15 ormore years experience in the childcare field. Only one quarter of theteaching staff in our sample hadworked for five years or less in childcare programs, and only 8.1% hadonly one or two years of teachingexperience. Almost 51% of thissample had been in their currentposition for more than five years;hence we can conclude that mostof the front-line professionals inthis sample were a reasonablystable and experienced group.
5.33 Front-Line Professionals’Experience With Children WithSpecial Needs
Similarly, more than half of thissample (57.0%) had more than fiveyears experience in work with chil-dren with special needs, including
28.9% who had ten or more yearsexperience. Only one fifth of oursample had recently begun to workwith children with special needs,having less than three years expe-rience in direct work with them orin an inclusive program. Surpris-ingly, the ECEs and in-house RTshad quite similar profiles in termsof length of time working with chil-dren with special needs. It is prob-ably fair to speculate that the ECEsin our sample with more than tenyears of experience in direct workwith children with special needshad developed a role for themselvessomewhat like that of a resourceteacher, both in their programs andin their communities.
5.34 Front-Line Professionals’Educational Background
As in other samples of child careteachers, our sample had a rangeof educational backgrounds thatextended from those with no com-pleted post-secondary educationrelated specifically to ECE or childcare to those with both a diplomaand degree, a specialized post-di-ploma certificate, or even a gradu-ate degree. This distribution isshown in Table 5.1.
Front-Line Professionals’ Educational Background Related to their Work
Table 5.1
Highest Formal Education CompletedRelated to ECE or Inclusion Number Percent
No diploma, no degree 16 12.9%
College diploma 73 58.9%
University degree 22 17.7%
Diploma and degree 11 8.9%
Graduate degree 2 1.6%

CHAPTER 5 DESCRIPTIVE INFORMATION ABOUT THE CENTRES, STAFF & DIRECTORS 71
The fact that about 87% of oursample of teaching staff had com-pleted a post-secondary diploma ordegree is noteworthy. In the ma-jority of cases, those with a diplomahad graduated from an ECE pro-gram; those with a degree typicallymajored in Education or SpecialEducation, Psychology, or ChildStudies. By and large, ECEs andIn-House RTs had similar back-grounds; however, of those with nodiploma or degree, the majoritywere ECEs. The majority of teach-ing professionals with both a di-ploma and degree were In-houseresource teachers.
5.35 How Our Front-LineProfessionals Compare toAvailable National Profiles
The most recent and extensivesource of information about childcare staff is the 1998 You Bet I Care!study, which surveyed 4,154 staffin full-day child care programs.YBIC! sample data representedmore than 38,000 front-line teach-ing staff across Canada who wereengaged in both full-time and part-time teaching positions at the as-sistant teacher, teacher, and super-visor levels. The most logical com-parison is to full-time teachers inthe YBIC! sample, when possible.
The YBIC! data indicates that in1998 among teachers nationwide,almost 41% had been in the childcare field for five years or less, and22.3% had three years or less ex-perience in the field. Approximately31% of the national sample had tenyears or more experience in childcare, compared to almost 55% ofour sample of front-line teachers.
Our sample also compares quitefavourably to the 1998 YBIC! infor-mation on the educational back-
grounds of full-time teachers.Among YBIC! teachers, 14.5% hadless than a one year ECE creden-tial, but only 11.1% had an ECE-related university degree. In oursample however, 28.2% had a uni-versity degree (sometimes in com-bination with a diploma or post-di-ploma certificate).
It should be reiterated that thesample of child care teaching staffselected for this study was not re-cruited in a way that would leadus to assume that they representall ECEs and in- house RTs nation-wide, or even all teaching staff inthe programs from which they wereselected. We deliberately chose par-ticipants who were likely to be moreexperienced in working with chil-dren with special needs in childcare programs. That requirementtends to lead to a selection of teach-ers who have more experience ingeneral, and perhaps additionaleducation and professional devel-opment activities to support themin their work. This certainly seemsto be the case. As a result, readersshould probably anticipate that oursample of child care professionalsmay represent the views of childcare teachers who are more expe-rienced, and perhaps more commit-ted to their work than would beevident among teachers drawnfrom a random sample of child careprograms.
5.4 OUR SAMPLE OF DIRECTORS
Directors of the 136 programs de-scribed in section 5.2 also providea unique window on inclusive childcare. Their view is a holistic onethat must incorporate many facetsof the centre and the people whoare involved in it: children and par-ents, staff, and sometimes boardmembers. The director’s role in

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada72
promoting inclusive child care, anddirectors’ attitudes and beliefs aredetailed in Chapter 8 of this report.This section provides a brief pro-file of directors’ experience andeducational background and somecomparative information that willbe useful for locating this samplerelative to all directors nationwide.
5.41 The Roles of Centre Directors
Directors in this study were askedas a first question whether theydescribed their position as being adirector/supervisor with adminis-trative responsibilities only or asone that included teaching respon-sibilities. Sixty-one percent of di-rectors had full-time administrativeroles, while 39% also had teachingresponsibilities in their centre.Four directors specifically men-tioned having responsibilities as aresource teacher; one was involvedin an innovative partnership in
which she provided support andconsultation to another centre. Infact, directors have many roles intheir centre and in their commu-nity, including roles involving thecoordination of many people’s ef-forts when children with specialneeds are involved, and an advo-cacy role for parents, children andstaff.
5.42 Directors’ Experience in theChild Care Field
The average centre director in thissample (56.0%) had more than fif-teen years of experience in the childcare field. Another 28.4% had be-tween ten and fourteen years ex-perience. Only eight directors(6.0%) had five years or less expe-rience in the child care field. Ap-proximately 39% of directors hadheld their present position for tenyears or longer, while a similar pro-portion had been in their currentposition for five years or less.
5.43 Directors’ Experience WithChildren With Special Needs
Directors’ experience with childrenwith special needs ranged from di-rect hands-on experience as anECE or resource teacher or as ateaching director to a more distantrole in which they did not have di-rect 1:1 involvement with childrenwith special needs, but supportedthose who did. Overall, 64.3% ofthe directors in this sample report-edly had more than 10 years of ex-perience in work with children withspecial needs, including almost35% who reportedly had 15 or moreyears experience in this regard.Quite a number of directors pro-vided comments that reflected theirlengthy years of experience andtheir sophistication (and some-
Figure 5.3
Centre Directors’ Roles
Directors 5%CombinedDirector/RT
56%ExclusivelyDirectors
38%Combined
Director/ECE
“In Alberta, vari-ous agencies havea mandate withinwhich they work(eg., education,health). Somechildren fall intothe cracks and,because they donot qualify undervarious mandatesfor services, theydon’t get the helpthat is needed. Iwould like to seethis change.Therefore, I aminvolved and com-mitted to attend-ing meetings thatinvolve the re-structuring ofSocial Services.”
(director of a designatedcentre in Alberta)

CHAPTER 5 DESCRIPTIVE INFORMATION ABOUT THE CENTRES, STAFF & DIRECTORS 73
times their frustration over the lackof systemic responses to childrenwith special needs and to supportfor high quality child careprograms.) Some have become ac-tively involved in their communi-ties in efforts to bring about de-sired changes.
5.44 Directors’ EducationalBackground
Our sample of directors includeda range that extended from thosewho had no formal ECE-relatededucation to those with a gradu-ate degree.
More than 92% of this sample ofdirectors had completed a post-secondary diploma or degree in anarea related to their work. Themajority of those with a diplomahad graduated from an ECE pro-gram. Those with a university de-gree typically studied Child orFamily Studies, Education or Spe-cial Education, or Psychology. Ap-proximately half of the directors inthis sample had also obtained apost-diploma certificate, either inECE or on a topic related either toinclusion/ resource teacher prepa-ration (16.9% of directors), admin-
istration or management (14.7%),or a related area. The vast major-ity of directors had also attendedmany conferences over the yearsand took an active role in support-ing their own and their staff’s on-going learning and skill develop-ment.
5.45 How Our Directors Compare to aNational Profile
Again, the recent data from the1998 You Bet I Care! study providesa basis for comparing our sampleof directors compared to a nationalprofile. The findings confirm thatthe centre director’s educationalbackground in early childhood edu-cation/child development is one ofthe most potent contributors to thequality of child care programs.6
In the YBIC! national sample of di-rectors, 18.0% of directors had noformal post-secondary ECE-relatededucation, while the majority hada two-year college credential;20.2% had an ECE-relatedBachelor’s degree or more. Theeducational background of oursample of directors is considerablystronger. Fewer than 8% of oursample had no formal post-second-
Highest Formal Education CompletedRelated to ECE or Inclusion Number Percent
No diploma, no degree 10 7.6%
College diploma 72 55.0%
University degree 24 19.3%
Diploma and degree 17 13.0%
Graduate degree 8 6.1%
* Based on information provided by 131 directors
Directors’ Educational Background Related to their Work*
Table 5.2

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada74
ary ECE-related credential, while37.1% have a Bachelor’s degree orhigher. Two recent U.S. studieshave suggested that child care pro-grams that are inclusive tend tohave higher scores on the Harmsand Clifford observational mea-sures of global quality.7 Unfortu-nately, we do not have Canadiandata on that point as yet; howeverthe findings identified here suggestthat a similar result might be ob-tained in the Canadian context aswell, on the basis of the educationalbackgrounds (and other character-istics) of this sample of directors,along with other factors.
5.5 SUMMING UP
This chapter has provided an over-view of our sample of child carecentres, ECEs and in-house re-source teachers, and directors. It
is important that readers appreci-ate the characteristics of this refer-ence group in order to interpret theresearch findings and evaluate theconclusions we draw. No nationalsampling frame of inclusive childcare programs was available to usfor this research. The description ofour samples, particularly in com-parison to recent national data, in-dicates that we likely have a morestable, committed, and educatedpopulation of front-line profession-als and directors. This referencegroup’s experiences with inclusion,therefore, can provide powerful in-formation about how well inclusionis working, and about the chal-lenges being faced by centre person-nel in programs that are attempt-ing to meet the needs of all childrenand families in their communities,in the context of limited resourcesbeing allocated for that purpose.
END NOTES
1 Irwin, S.H. & DeRoche, J. (1992). Attitudes of Canadian mainstream child care staff towardinclusion of children with special needs. (Unpublished manuscript).
2 Doherty, G., Lero, D.S., Goelman, H., LaGrange, A. & Tougas, J. (2000). You Bet I Care! ACanada-wide study on wages, working conditions and practices in child care centres. Guelph:University of Guelph (Centre for Families, Work and Well-Being).
3 Peck, C.A. (1993). Ecological perspectives on implementation of integrated early childhoodprograms. In C.A. Peck, S.L. Odom, & D.D. Bricker (eds.), Integrating young children with dis-abilities into community programs: Ecological perspectives on research and implementation 3-15. Baltimore: Paul H. Brookes.
4 Human Resources Development Canada (1997). The status of daycare in Canada, 1995 and1996. Ottawa: Minister of Supply and Services. Cat. H74-14/1996E.
5 Doherty, G., et al. (2000).
6 Doherty, G., et al. (2000). See also, Jorde-Bloom, P. (1992). The child care director: A criticalcomponent of program quality. Educational Horizons (Spring) 138-145.; Jorde-Bloom, P. &Sheerer, M. (1992). Changing organizations by changing individuals: A model of leadershiptraining. The Urban Review, 24, 263-286; Bredekamp, S. & Copple, C., eds. (1997).Developmentally appropriate practice in early childhood programs. Rev. ed. Washington, DC:National Association for the Education of Young Children.
7 Kontos, S. & Diamond, K. (1997). Preparing practitioners to provide early intervention servicesin inclusive settings. In P. Winton, J. McCollum & C. Catlett (eds.), Reforming personnel prepa-ration in early intervention. Baltimore: Brookes, 393-410. See also Buysse, V., Wesley, P.W. &Keyes, L. (1998). Implementing early childhood inclusion: Barrier and support factors. EarlyChildhood Research Quarterly, 13(1), 169-184.

CHAPTER 6 THE NATURE AND EXTENT OF INCLUSION – CENTRE PRACTICES 75
6.THE NATURE
AND EXTENT OF INCLUSION –CENTRE PRACTICES
6.1 INTRODUCTION
The purpose of this chapter is todescribe inclusion as practiced inchild care centres in our sampleat the time data were collected.We provide information on thenumber of children with specialneeds who were enrolled, who wasattending and under what condi-tions, and how many childrenwere not accepted in these pro-grams in the previous three yearsand for what reasons. In addition,we explore how directors andfront-line centre staff were in-volved in coordinating their ac-tions with parents and with otherservice professionals in order tomeet the needs of the childrenenrolled.
Finally, this chapter providessome information about the re-sources available to centres andincludes information from direc-tors on some of the challengesthey face in trying to match cen-tre resources to the goal of pro-viding inclusive care that bestmeets everyone’s needs.
This chapter relates quite directlyto Chapter 7, in which inclusionis examined from the standpointof ECEs and in-house resource
teachers within these centres, andChapter 8, which examines inclu-sion as experienced by directors.
6.2 INCLUDING CHILDREN WITHSPECIAL NEEDS: CHILDRENIN CHILD CARE PROGRAMS
A discussion of the nature and ex-tent of inclusion of children withspecial needs in child care pro-grams requires consideration notonly of the number of childrenwith special needs who are en-rolled, but also the nature of theirparticipation and the kinds of ef-forts made to meet their needs. Inmany centres, the participation ofchildren with disabilities is lim-ited, as evidenced by the numberof children who are not accommo-dated or who participate on onlya part-time basis for reasonsother than parental choice.
The capacities of centres and theresources available to support in-clusion are referred to repeatedlyas critical factors that must alsobe considered — both in the re-search and practice-based litera-ture on inclusion, and by direc-tors and child care staff in theirwritten comments to our questions.
Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada76
6.21 The Number of Children WithSpecial Needs Included in ChildCare Programs
At the time of data collection in1996-97, 117 of the 136 centres inour sample (86%) included at leastone child with special needs, while19 programs (14.4%) had nochildren with special needs en-rolled at the time. Across the 117centres in our sample, at least1,256 children with disabilities, sig-nificant delays, behavioural prob-lems, and chronic health condi-tions were receiving developmentalsupport. This number includes oneregional centre that served 300children with special needs in arange of programs. In general, onlya few children with special needsattended most regular and inte-grated programs. (See Tables 6.1and 6.2.)
Across all centres for which infor-mation was available, 24.4% of di-rectors replied that they had fewerchildren with special needs thanwas typical of the last three years,while two thirds (66.1%) indicated
that they had the usual number en-rolled. Twelve directors (9.4% ofthose who replied) indicated thatthey had more than their usual num-ber of children with special needs en-rolled. Most of those programs hadbetween five and nine children withspecial needs attending when datawere collected.
The 19 centres that had no childrenwith special needs attending at thetime data were collected consistedof four designated programs and fif-teen regular programs. (Designatedprograms are identified by the pro-vincial or territorial government asbeing contracted or being eligible tohave a contract to provide care forchildren with special needs, forwhom additional funding or person-nel supports will be made available.Regular programs are not designatedas such, but may receive additionalsupport if they accept children withspecial needs.) According to our data,less than 7% of designated centreshad no children with special needs,compared to almost 24% of the regu-lar programs in our sample.
The Number of Children with Special Needs Included in All Sample Child CarePrograms*
Table 6.1
Number of Children with Special Needs Child Care Programs
Number Percent
None 19 14.4%
1 or 2 children 35 26.5%
3 or 4 children 26 18.9%
5 - 9 children 22 16.2%
10 or more children 31 22.8%
(unspecified, but at least one child) 3 2.2%
* Based on 136 programs. Of the 11 specialized programs, 10 were in the 10+ group, and one programenrolled 5-9 children with special needs.
“Our centre doesnot have a spe-cial needs li-cense, so there-fore, parents donot qualify forfinancial assis-tance.”(director of a centre in NewBrunswick with no childrenwith special needs enrolled)

CHAPTER 6 THE NATURE AND EXTENT OF INCLUSION – CENTRE PRACTICES 77
Twelve of these nineteen directorssaid that the number of childrenwith special needs attending wasless than usual compared to thelast three years, while five repliedthat having no children with spe-cial needs was typical; two direc-tors did not reply. Further exami-nation revealed a number of rea-sons why programs might not haveany children with special needs en-rolled, or have fewer children withdisabilities than they have had atother times. These reasons include:policies or funding restraints thatlimit parents’ access to subsidiesand/or centres’ access to specialfunds, centres being full and un-able to accept additional children,temporary dips in referrals, andsome situations where directorsfeel less certain about their capaci-ties to include children with spe-cial needs or are far more selectiveabout whom they will accept, givenlimited resources.
6.22 The Nature and Severity ofChildren’s Conditions AmongChildren Enrolled
We did not ask directors to tell usabout the specific conditions or di-agnoses of the children enrolledwithin their centres, but relied onthe definition we provided to set theboundaries for responses. However,an indication of who was being in-cluded can be drawn from the re-sponses 100 ECEs and in-houseRTs gave when asked to describe achild with special needs with whomthey had been most successful inthe last two years. Front-line staffdescribed the children they workedwith as spanning a considerablerange, including children with de-velopmental or global delays, cere-bral palsy, autism, health impair-ments, learning disabilities, emo-tional/behavioural disorders, andhearing, vision, and speech impair-ments. Approximately 11% of front-line staff described the child with
The Number of Children with Special Needs Included in Regular and IntegratedChild Care Programs*
Table 6.2
Number of Children with Special Needs Child Care Programs
Number Percent
None 19 15.2%
1 or 2 children 35 28.0%
3 or 4 children 26 20.8%
5 - 9 children 21 16.8%
10 or more children 21 16.8%
(unspecified, but at least one child) 3 2.4%
* Based on 125 regular and integrated programs

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada78
whom they had been most success-ful as having a mild disability orhealth condition, 47% describedthe condition as moderate, and42.5% described the child’s condi-tion as severe. (See Chapter 7 formore information about teachers’experiences with these children.)
Based on these responses and oth-ers received on both the staff anddirectors’ questionnaires, it ap-pears that centres were includinga reasonably wide range of childrenwith special needs. Furthermore,many directors and staff indicatedthat over the years, and with moreexperience, centres that had posi-tive experiences with inclusionwere willing to accept a broaderrange of children.
We asked directors if the complex-ity of children’s special needs theircentre accommodates had in-creased, decreased, or remainedthe same since 1990. Of 130 direc-tors who responded,
✦ 60 directors (46.2%) said thatsince 1990 the complexity ofchildren’s conditions that were be-ing accommodated had increased,
✦ 61 directors (46.9%) reported nochange, and
✦ 9 directors (6.9%) reported a de-crease in the complexity of condi-tions evident among the childrenwith special needs between 1990and 1996.
6.23 Is Participation Limited to Part-Time Attendance?
Previous experience alerted us tothe fact that ofttimes children withspecial needs in child care pro-grams attend full-day programsonly on a part-time basis for vari-ous reasons. When part-time par-ticipation reflects parental prefer-
ences and what is best for the child,then these children are not beingtreated differently from other chil-dren whose parents might have asimilar preference. However, whenchildren with special needs cannotparticipate on a full-time basis be-cause of arbitrary funding arrange-ments or because staff are unableto address a child’s needs at lunchor nap time, then barriers to fullinclusion are evident.
We asked directors if any of thechildren with special needs in theircentre were limited to part-timeattendance for any of several rea-sons. Sixty directors (51.3% ofthose with at least one child withspecial needs attending their pro-gram) indicated that attendancewas limited to part-time for one ormore reasons described below.
Directors in all three program types(specialized, designated and regu-lar child care programs) indicatedthat limits on funding for full-timesubsidies was the most commonreason children’s attendance is lim-ited; funding limits also directlyconstrain the availability of re-source teachers and support work-ers who are seen as essential re-sources to support inclusion. Di-rectors’ comments thus confirmedthat there are systemic barriers tomany children’s participation on afull-time basis — a situation thataffects the child, the program, andthe child’s parents.
Lack of full-time care has beennoted as one of the salient factorsthat constrain mothers’ involve-ment in the labour force in fami-lies with children who have specialneeds, with negative impacts onfamily income and longer term eco-nomic security.1, 2 Part-time subsi-dies and part-time spaces can alsoaffect centres to the extent that
“We have nospecial needschildren attend-ing our centre,but in the pastwe have had oneor two.”(director of a centre inNova Scotia)
“I feel that thereis a better under-standing of howspecial needschildren affectthe other childrenand staff. Wenow do not ac-cept every childbut weigh theirneeds againstthe rest of theprogram. When aspecial needschild is with-drawn, we as astaff decide whoand what wecan deal withand sometimeschoose to take ashort break be-fore filling thespot.”(director of a regular centrein Manitoba)

CHAPTER 6 THE NATURE AND EXTENT OF INCLUSION – CENTRE PRACTICES 79
special need from their program inthe last three years.
✦ 63 directors (46.3%)answered yes
✦ 66 directors (48.5%)answered no
✦ 7 directors (5.1%) didnot reply.
Based on their responses, we cal-culated that approximately 336children with special needs wereturned away from the 63 centresfor which directors provided infor-mation. (Note: Other families whomight have approached these cen-tres, or who made only preliminaryor indirect inquiries, are not rep-resented in these estimates.) Mostdirectors indicated they had turnedaway only a few children, but tenprograms were not able to acceptthe applications of ten or more chil-dren with special needs in theircommunity.
The reasons most commonly givenfor not accepting a child with spe-cial needs were then classified intoseveral domains. A centre mayrefuse a child for a variety of rea-sons. Our analyses suggest that the
they create empty half-day slots inthe afternoons in full-day programsthat are harder for many centres tofill, and create more half-day staff-ing patterns. Children who mightbenefit from longer days or whomight experience better, more reli-able, less fragmented care arrange-ments are also deprived of the op-portunity to stay with their teach-ers and peers under these circum-stances. On the other hand, onedirector commented that limitingchildren with special needs to part-time was a strategic choice, since itallowed more children to participateby sharing the space available. Thisrationale may seem reasonable incircumstances when access to highquality programs is limited, but itcan create other difficulties thatimpede children’s developmentaland social progress and theirparents’ access to employment.
6.3 TO WHAT EXTENT ARECHILDREN WITH SPECIALNEEDS NOT ACCOMMODATEDIN CHILD CARE PROGRAMS?
Directors in our sample were askedif they had turned down any chil-dren with an identified disability or
Reasons Children with Special Needs Are Limited to Part-Time Attendance*
Table 6.3
Reasons Given Number of Programs
Parent’s choice/seen as best for child 12
Subsidy available for part-time attendance only 35
Resource teachers/support workers only available 11 part time or part day
Overall staffing can’t accommodate full day 11
Transportation constraints 7
Difficulty with nap time, health procedures, etc. 6
* Some directors provided more than one reason why some children with special needs are limitedto part-time attendance.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada80
most common threads runningthrough the reasons given and theindividual comments directorsmade indicate that the main barri-ers do not emanate from a lack ofwillingness on the part of child carestaff or a lack of commitment toinclusion. Most commonly, direc-tors’ responses suggested that lim-its placed on the centres them-selves limit the centre’s capacitiesto accept more children. Limitedfunds or staffing, or provincial poli-cies often translate into a “maxi-mum number” of children with spe-cial needs a centre can accept, or aperceived maximum number ordegree of complexity of needs thatcentre staff feel they can handlewithout compromising the qualityof care provided to other childrenor experiencing serious stressthemselves. Other factors were alsooperating, as shown in Table 6.4.
Further analysis of the reasonsgiven by directors of specialized,
designated, and regular programsrevealed some interesting differ-ences. Directors of specialized pro-grams were most likely to say thatchildren were turned down becausethe program already had its maxi-mum number of children with spe-cial needs and/or because the pro-gram could not address the com-plex needs of the child and familyat the time. These were also the twomost common reasons given by di-rectors of designated programs.Directors of both designated andregular programs more often statedthat they were limited by a lack offunding and the lack of (or loss of)resource teacher support or sup-port from other professionals andagencies to assist them in theirwork with children with specialneeds. Interestingly, only directorsof regular programs indicated thataccess to the centre (transporta-tion) and staff being untrained,unwilling, or burned out were fac-
Table 6.4
Main Reasons That Caused You to Turn Down a Child (Children) with Special Needs*
Reasons Given # of ProgramsA) Program or Funding Constraints
Already had maximum number of children with special needs 30No funding available; centre not eligible for special funding 20Physical access to program or rooms would be problematic 7Unable to access external support services (resource teachers, physiotherapists, etc.) 6Loss of centre-based resource teacher or support worker 4
B) Perceived difficulty in meeting child’s needs; Inability to accommodateComplex health concerns could not be addressed 10Child too aggressive 9Child needs 1:1 staffing, more structured program 26Difficult to meet parents’ expectations 2
C) Staff attitudes or lack of training
“I have alwayssupported theconcept of inclu-sion, but thedollars are soscarce now andthe ‘regular’children are soneedy that mystaff simplycan’t cope witha special needschild within ex-isting ratios.”(director of a regular centrein Québec)
Staff not trained or not willing 5D) Other Reasons
Centre is full 7* Some directors provided more than one reason for not being able to accommodate a child with specialneeds in their program.
CHAPTER 6 THE NATURE AND EXTENT OF INCLUSION – CENTRE PRACTICES 81
tors in refusing to accept a childwith special needs into their pro-gram (five directors cited these asreasons). Directors of regular pro-grams also gave what one mightdescribe as “normative” reasons forturning away children with specialneeds, i.e., the fact that the centreitself was full.
An interesting point of comparisonwas available to us as a result ofthe You Bet I Care! national studyof child care programs conductedin 1998. When asked a parallelquestion to the one used in thepresent study, directors in close to40% of the national sample re-ported not having been able to ac-cept at least one child with specialneeds into their program in thethree years prior to data collection(which would have been 1995-1998).
Centre directors in the YBIC! studyprovided a number of reasons fornot accepting children with specialneeds whose parents had appliedto their programs, with most direc-tors providing more than one rea-son. The most common reasonsgiven for not accepting childrenwith special needs were:
✦ insufficient funds to provide forthe required additional staffing(55.1%);
✦ the building would haverequired structural modifica-tions (33.2%);
✦ staff did not feel adequatelytrained to care for the child(25.9%);
✦ the centre already had its maxi-mum number of children withspecial needs (22.4%);
✦ insufficient funds for necessaryequipment (17.3%);
✦ limited access to external con-sultants (e.g., physiotherapist,resource teacher, early interven-tion consultant) (16.6%); and
✦ limited capacity or willingnesson the part of staff to includechildren with complex problemsor challenging behaviours(18.6%).
The major similarity in findingsacross YBIC! and our current studyis that limited funding and limitedadditional staffing restrict centres’capacities to include children withspecial needs. The major differ-ences between the two studies sug-gest that in a broader populationof centres physical accessibility andstaff attitudes and training arelikely to be more significant barri-ers than was observed in our moreselected sample.
6.4 CENTRE PRACTICES RELATEDTO INCLUSION
Directors provided informationabout a number of centre practicesthat are important to successfulinclusion. In most cases, directorsindicated that program and activ-ity planning and curriculum modi-fications, communication and in-volvement with parents, and theeffective coordination of actionstaken with or involving other pro-fessionals in the community involveboth the director and centre staff,and team work and communicationamong centre personnel.
6.41 Program Planning
Individual program planning is awell-accepted means of ensuringthat appropriate curriculum goalsare developed and activities imple-mented to achieve them. The ma-jority of directors (79.4%) indicated

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada82
that individual program plans weremade for each child with specialneeds.
We were interested in knowing whoactually does the program planningand/or is responsible for this rolein centres. Most often, directorsindicated that this is not done byan individual ECE or RT alone, butinvolves two, and often more,people working together as a team.The most common response was“ECE and RT,” but many combi-nations and permutations wereprovided. In 82% of centres, anECE was involved. In 77% of cen-tres, a special needs worker/resource teacher/resource consult-ant was involved. Parents report-edly were involved in 21% of cen-tres when individual program plan-ning was done, and the director orsupervisor was involved in 18% ofcentres that do program plans.
6.42 Communication With Parents
We asked directors, “Who is mostinvolved in discussions and com-munication with the parents ofchildren with special needs in thecentre?” Again, most often a com-
bination was mentioned. About63% of directors mentioned a com-bination, typically involving the di-rector and either an ECE or re-source teacher/special needsworker. About 27% of directors in-dicated that an ECE is the primaryperson who liaises with the parent,while in 6% of the centres the di-rector was solely involved.
6.43 Degree of Parents’ Involvement
While we recognized that the de-gree of involvement of child carestaff with parents of children withspecial needs might vary acrossfamilies, we asked directors to in-dicate what was the most commonmanner in which parents of chil-dren with special needs related tothe centre and its staff. Based ondirectors’ reports, the majority ofparents are involved to a fairly sig-nificant degree when children withspecial needs are included in theprogram. This is consistent withwhat the literature defines as acritical element in inclusive pro-grams, as described in Chapter 1,and is another component in stafftime and engagement related toinclusion.
Extent of Parental Involvement in Centres Including Children with Special Needs
Table 6.5
Manner in which parents are involved: Percent of programs
Extensive involvement;parents and teachers work as partners 50%
Not involved on an on-going basis, but meet regularly;involved in planning and decisions 31%
Meet and communicate on as-needed basis; parents notinvolved in planning with us, but perhaps with others 16%
Parents and centre staff meet infrequently 3%

CHAPTER 6 THE NATURE AND EXTENT OF INCLUSION – CENTRE PRACTICES 83
6.44 Coordinating Services forChildren With Special Needs inthe Centre
Supports to children with specialneeds and to the staff who work withthem in centres may involve a vari-ety of people — in addition to thedirector, the teacher(s) who workmost directly with the child, andpossibly the child’s parents. Com-munication and consultation can becomplex. Consequently, typicallyone person is most directly involvedin communications and liaison, par-ticularly with external health andsocial service professionals. Whenasked who serves as the primary co-ordinator, directors indicated thatthis was a function they were likelyto have themselves: 64% of direc-tors who replied indicated that theywere the primary coordinator. Inanother 17% of centres, an in-houseresource teacher coordinated ac-tions and communications. An ex-ternal resource teacher, resourceconsultant, or another agency wasnamed as the primary coordinatorin 9% of centres, parents werenamed in 2.3% of centres, and in6% of centres, the director indicatedthat the role varied — there was notone primary coordinator.
How well is the coordinationgoing?
Beyond direct interactions and ser-vice to the children, coordinationmust also be effective to have de-sired effects and minimize frictionand additional workload. Directorsindicated that coordination wasgenerally being handled quite well.
✦ 41% said that coordinationmost often was handled “verywell, no major problems”;
✦ 46% said coordination wasgoing “fairly well, minor prob-lems get resolved”;
✦ 9% indicated that there were“some problems that had not yetbeen resolved”; and
✦ 3% of directors indicated thatthere were some serious prob-lems with coordination aroundinclusion.
6.5 THE RESOURCES AVAILABLETO CENTRES TO SUPPORTINCLUSIVE CHILD CARE
Earlier sections of this chapter havealready indicated that effective in-clusion involves a considerableamount of staff time and engage-ment. The absence of additional fi-nancial resources, additional staff,and the involvement of parents andvarious professionals in the com-munity can be a significant barrierto enrolling children with specialneeds in the first place, and canalso cause significant difficulties forcentres in their efforts to meet thechildren’s needs once they beginattending the program.
We asked each director to indicateon a checklist which of a variety of(additional) resources were cur-rently available to support effectiveinclusion of children with specialneeds in their program. The resultsare shown in Table 6.6. Becausethe question asked about the“availability” of resources ratherthan actual use, it is likely that thenumber of positive responses ac-tually overestimates the true avail-ability of resources to child carecentres. Table 6.6 includes actual“yes” responses, with the percent-age calculated out of all 136 cen-tres, including those that had nochildren with special needs en-rolled when they were surveyed.The profile of resources availableto centres varied, of course, de-pending on whether the centreswere specialized or community-
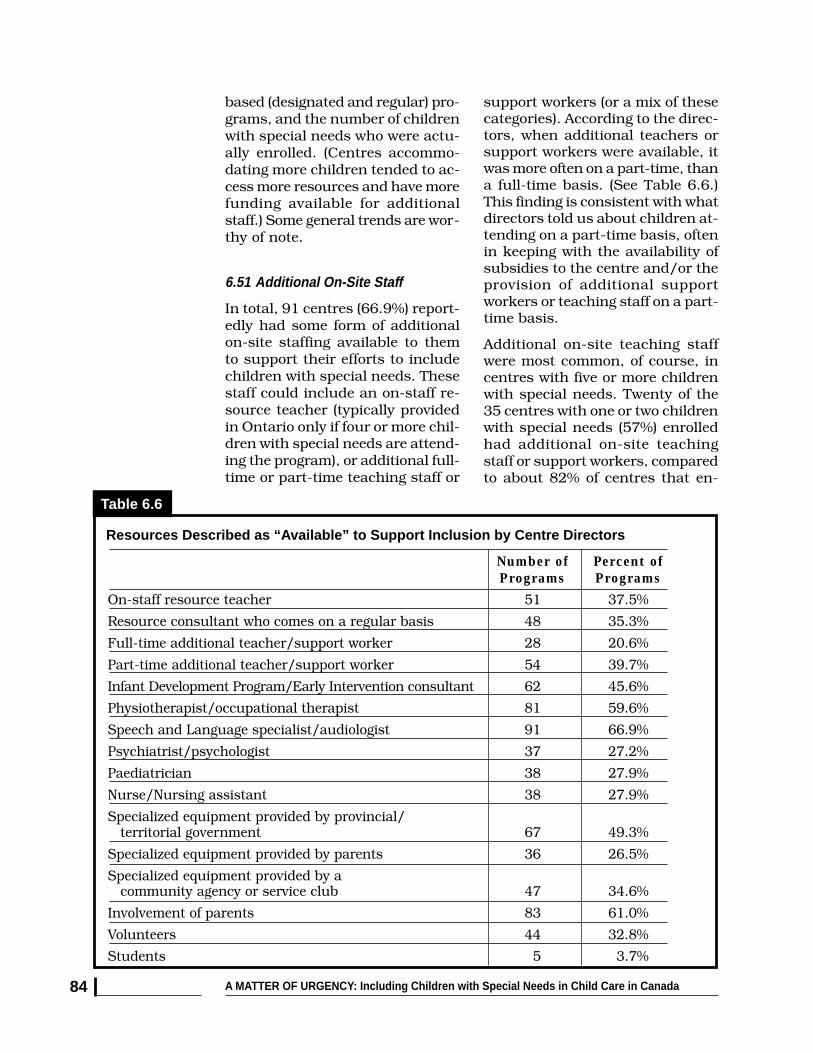
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada84
based (designated and regular) pro-grams, and the number of childrenwith special needs who were actu-ally enrolled. (Centres accommo-dating more children tended to ac-cess more resources and have morefunding available for additionalstaff.) Some general trends are wor-thy of note.
6.51 Additional On-Site Staff
In total, 91 centres (66.9%) report-edly had some form of additionalon-site staffing available to themto support their efforts to includechildren with special needs. Thesestaff could include an on-staff re-source teacher (typically providedin Ontario only if four or more chil-dren with special needs are attend-ing the program), or additional full-time or part-time teaching staff or
support workers (or a mix of thesecategories). According to the direc-tors, when additional teachers orsupport workers were available, itwas more often on a part-time, thana full-time basis. (See Table 6.6.)This finding is consistent with whatdirectors told us about children at-tending on a part-time basis, oftenin keeping with the availability ofsubsidies to the centre and/or theprovision of additional supportworkers or teaching staff on a part-time basis.
Additional on-site teaching staffwere most common, of course, incentres with five or more childrenwith special needs. Twenty of the35 centres with one or two childrenwith special needs (57%) enrolledhad additional on-site teachingstaff or support workers, comparedto about 82% of centres that en-
Table 6.6
Resources Described as “Available” to Support Inclusion by Centre Directors
Number of Percent ofPrograms Programs
On-staff resource teacher 51 37.5%
Resource consultant who comes on a regular basis 48 35.3%
Full-time additional teacher/support worker 28 20.6%
Part-time additional teacher/support worker 54 39.7%
Infant Development Program/Early Intervention consultant 62 45.6%
Physiotherapist/occupational therapist 81 59.6%
Speech and Language specialist/audiologist 91 66.9%
Psychiatrist/psychologist 37 27.2%
Paediatrician 38 27.9%
Nurse/Nursing assistant 38 27.9%
Specialized equipment provided by provincial/
community agency or service club 47 34.6%
Involvement of parents 83 61.0%
Volunteers 44 32.8%
Students 5 3.7%
territorial government 67 49.3%
Specialized equipment provided by parents 36 26.5%
Specialized equipment provided by a

CHAPTER 6 THE NATURE AND EXTENT OF INCLUSION – CENTRE PRACTICES 85
rolled between five and nine chil-dren with special needs.
6.52 Itinerant Staff andResource Consultants
Itinerant consultants include trav-elling resource teachers/resourceconsultants and consultants frominfant development or early inter-vention programs. When thisbroader category is used, we notethat 83 directors (62.4%) reportedlyhave itinerant consultants availableto them to help support their staff’sefforts. Travelling consultants werereportedly “available” to 42% of cen-tres that had no children with spe-cial needs enrolled, to 57% of cen-tres with only one or two childrenwith special needs in attendance,and to 61.5% of centres with threeor four children with special needsin their programs. Travelling re-source and early intervention con-sultants were reportedly available to73-74% of centres with more thanfive children with special needs.
6.53 The Availability of Both On-Siteand Travelling Consultants
We were interested in exploringwhether there were any discerniblepatterns in the availability of bothof these categories considered to-gether. Analyses indicated thatamong 133 programs for whichcomplete information was available:
✦ 60 centres had both on-site staffand travelling consultants avail-able to assist them,
✦ 31 programs had only addi-tional in-house or on-site staffavailable,
✦ 23 programs had only travellingconsultants and early interven-tion workers available,
✦ 19 programs had neither on-siteteachers nor travelling consult-ants available to assist them.
This latter group included nine ofthe nineteen centres that had nochildren with special needs en-rolled when surveyed, eight centreswith one or two children, one cen-tre with 5-9 children, and one cen-tre that reportedly had ten or morechildren with special needs en-rolled in the program.
6.54 The Availability of OtherProfessionals
Speech and language specialistsand PT/OT specialists were avail-able to the majority of child careprograms to support inclusion.Medical and behavioural resourcesin the form of paediatricians,nurses, psychiatrists and psycholo-gists were less commonly available(each was available to less than30% of centres in our sample). It isnot known how extensively variousspecialists are/were involved withthese programs from our data.
6.55 Support From Parents
It should be noted that supportfrom parents is an important andcommon resource for programs.While parents of the children withspecial needs are a vital source ofsupport, information, and directassistance, the involvement andsupport of parents of other childrenmay also be very helpful.
6.6 SUMMING UP
This chapter has provided an over-view of how inclusion is practicedand experienced in the 136 centresin our sample. Looking through thewindow of centres, we captured

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada86
information about the nature andextent of inclusion, the kinds ofactivities and staff involvement inactivities that are important ad-juncts to support positive experi-ences for the children enrolled, andthe availability of resources to sup-port inclusion. Data from a recentnational sample of centres extendour analysis and allows us to un-derstand some of the importantbarriers to inclusive early child-hood education and care for chil-dren with special needs in Canada.Most importantly, we hope readershave begun to develop a sense ofchild care programs as organiza-tions, with resources within them(directors, staff and sometimes spe-cialized resource teachers or sup-
port workers) that can be utilizedto promote optimal developmentand provide support to a wide rangeof young children and their fami-lies, to the extent they are able todo so. These centres operate withinboth a community context and apolicy and funding context that caneither promote or constraintheir efforts to provide effective,inclusive and high quality care.
In the following chapters we exam-ine the experiences and attitudesof ECEs and in-house resourceteachers and the directors them-selves. Understanding the centresin which they operate provides theframework for interpreting theirresponses.
END NOTES
1 Irwin, S.H. & Lero, D.S. (1997). In our way: Child care barriers to full workforce participationexperienced by parents of children with special needs — and potential remedies. NS: BretonBooks.
2 Roeher Institute (2000). Finding a way in: Parents on social assistance with disabled children.Toronto, ON: Author.
CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 87
INCLUSION AS
EXPERIENCED BY CHILD CARE STAFF
7.1 INTRODUCTION
As described in the literature re-view provided in Chapter 3, staffattitudes, experiences, and train-ing have been identified as criticalfactors affecting the extent to whichinclusion is undertaken or resistedin early childhood programs, aswell as the extent to which it islikely to be effective and sustainedover time. To date, few studies havetreated staff’s experiences with in-clusion as a central focus of inves-tigation, despite the fact that thisreflection-on-action (Wein, 1998)1
provides a critical window, both forviewing and understanding theecology of inclusion and for devel-oping additional training and sup-ports for early childhood staff in in-clusive programs.
Our perspective is that under-standing inclusion as experiencedby front-line staff is a critical is-sue. Experiences on the front line,both successful and unsuccessfulones in the eyes of staff, with orwithout adequate resources andsupports, go on to affect a staff at-titudes and ongoing commitmentto inclusion, as well as her senseof confidence and competence inworking with children with specialneeds. In turn, the experiences offront-line staff with children, with
parents, with co-workers in thecentre, and with external resourcepersonnel are likely to affect boththe individual staff and her centrein ways that make that centre amore or less hospitable climate inwhich effective inclusion canflourish.
This chapter provides informationobtained from early childhood edu-cators and in-house resourceteachers in centres that have atleast a six-year history of includ-ing children with special needs. Wefirst describe these staff in termsof their education, experience, andgeneral attitudes and beliefs aboutinclusion at the time data were col-lected. We then turn to an in-depthexamination of what staff told usabout their most successful andless successful experiences withinclusion in their centres in the lasttwo years.
This part of our study provides de-tailed information about staff‘s ex-periences, and about the factorsthat helped support them whenthey were successful or that mighthave been helpful to them. We alsolearned about sources of frustra-tion and difficulty, and providestaff’s own comments about theirexperiences. Child care staff told usquite directly that their experienceson the front line, perhaps more
7.Kathleen Brophy, Donna S. Lero, Sharon Hope Irwin
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada88
than any other factor, are respon-sible for changes in their commit-ment to inclusion, their willingnessto accept a broader range of chil-dren in the program or to be morecautious, and their feelings of com-fort and confidence in working withchildren with special needs. To-ward the end of this chapter weexplore the extent to which staff’straining, experience in the field,and length of experience workingwith children with special needsappear to be related to their cur-rent attitudes toward inclusion,their sense of competence or effi-cacy in working with children withspecial needs, and their stated pref-erences for additional informationand training.
This chapter weaves together infor-mation about the past and presentin staff’s lives, recognizing thatprior education, specialized train-ing, and length of experience in thefield are assets that staff bring totheir experiences with inclusion.Specific experiences in their workwith children with special needsfurther shape staff’s attitudes andexpectations and provide opportu-nities for new learning. At the sametime, we recognize that staff’s ex-periences are affected by the con-texts in which those experiencesoccur — including the specific con-text of the centre in which theywork, and the broader policy andcommunity contexts that affect theresources available to centres andtheir staff.
7.2 STAFF CHARACTERISTICS
It is important to understand someof the characteristics of our staffbefore we discuss their attitudesand their specific experiences intheir centres. Readers are referredback to the general description of
front-line staff provided in Chap-ter 5. (See Section 5.3.) [NOTE: Asdiscussed in the next section, thefull sample of staff consists of twogroups: early childhood educators(ECEs) and those with more spe-cialized duties and training, whodescribed themselves as in-houseresource teachers (RTs). When re-ferring to the full sample, we inter-changeably use the words staff,child care professionals, teachers,or teaching staff. Otherwise, weidentify the subgroups of ECEs andRTs separately, indicating bothsimilarities and differences be-tween them.]
7.21 Specific Roles of Front-LineStaff
Of the 124 front-line teaching staffin our sample, 66 (53%) describedthemselves as early childhood edu-cators (ECEs), and 58 (47%) de-scribed themselves as on-site (or in-house) resource teachers, supportworkers, or special needs workers.
The latter group includes a sizableproportion who indicated that theirposition combined being a resourceteacher with being an ECE or su-pervisor. Based on their own report,those who described themselves asin-house RTs often had a more sa-lient role in their centre in terms ofinclusion. These teachers, for ex-ample, were more likely to be work-ing with children with special needsat the time data were collected, and,in fact, to be working with morechildren with special needs in theircentre than staff who describedthemselves as ECEs. Resourceteachers, in comparison to the ECEsin our sample, also appear to havehad more experience working withchildren whose disabilities or healthconditions were described by themas severe. (See Table 7.1.)
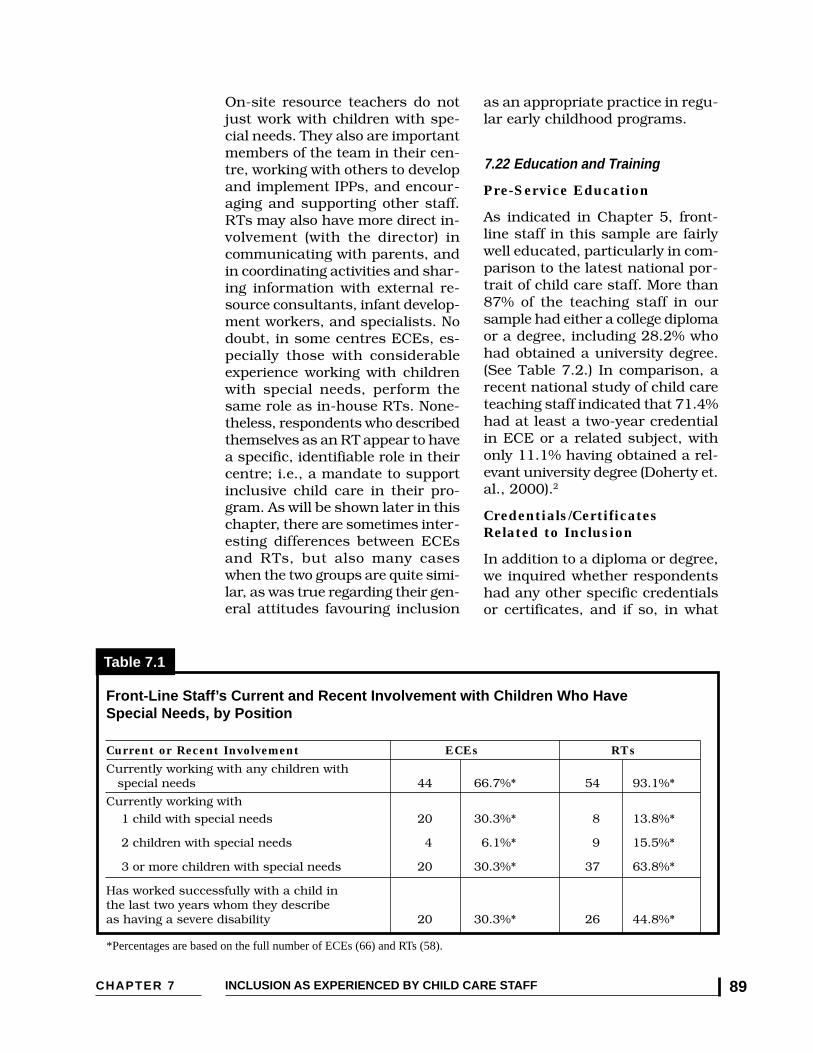
CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 89
Current or Recent Involvement ECEs RTs
On-site resource teachers do notjust work with children with spe-cial needs. They also are importantmembers of the team in their cen-tre, working with others to developand implement IPPs, and encour-aging and supporting other staff.RTs may also have more direct in-volvement (with the director) incommunicating with parents, andin coordinating activities and shar-ing information with external re-source consultants, infant develop-ment workers, and specialists. Nodoubt, in some centres ECEs, es-pecially those with considerableexperience working with childrenwith special needs, perform thesame role as in-house RTs. None-theless, respondents who describedthemselves as an RT appear to havea specific, identifiable role in theircentre; i.e., a mandate to supportinclusive child care in their pro-gram. As will be shown later in thischapter, there are sometimes inter-esting differences between ECEsand RTs, but also many caseswhen the two groups are quite simi-lar, as was true regarding their gen-eral attitudes favouring inclusion
as an appropriate practice in regu-lar early childhood programs.
7.22 Education and Training
Pre-Service Education
As indicated in Chapter 5, front-line staff in this sample are fairlywell educated, particularly in com-parison to the latest national por-trait of child care staff. More than87% of the teaching staff in oursample had either a college diplomaor a degree, including 28.2% whohad obtained a university degree.(See Table 7.2.) In comparison, arecent national study of child careteaching staff indicated that 71.4%had at least a two-year credentialin ECE or a related subject, withonly 11.1% having obtained a rel-evant university degree (Doherty et.al., 2000).2
Credentials/CertificatesRelated to Inclusion
In addition to a diploma or degree,we inquired whether respondentshad any other specific credentialsor certificates, and if so, in what
Front-Line Staff’s Current and Recent Involvement with Children Who HaveSpecial Needs, by Position
Table 7.1
*Percentages are based on the full number of ECEs (66) and RTs (58).
Currently working with any children with special needs 44 66.7%* 54 93.1%*
Currently working with
1 child with special needs 20 30.3%* 8 13.8%*
2 children with special needs 4 6.1%* 9 15.5%*
3 or more children with special needs 20 30.3%* 37 63.8%*
Has worked successfully with a child inthe last two years whom they describeas having a severe disability 20 30.3%* 26 44.8%*

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada90
than one third of whom reportedlyhad attended ten or more such pre-sentations since 1990.
In summary, compared to moretypical samples of front-line staffin child care programs, this sampleof ECEs and in-house RTs, delib-erately chosen for their current orprevious involvement in inclusiveprograms, had more formal educa-tion and preparation related toECE. A significant proportion alsohad obtained specialized training,either through a formal programleading to a certificate or other cre-dential and/or by attending con-ferences and workshops that re-lated to including children withspecial needs. Since the literatureindicates that higher ECE-specificeducation and more specific train-ing related to inclusion are corre-lated with pro-inclusion attitudesand greater self confidence, read-ers can anticipate that these atti-tudes were also prevalent in ourparticular sample.
area. One sixth of our front-linestaff (10.6% of ECEs and 24.1% ofin-house RTs) had taken someform of specialist training relatedto inclusion (such as a resourceteacher certificate or post-diplomacourse work related to childrenwith special needs).
Professional Development
We also asked respondentswhether they had attended anyworkshops or conference presen-tations related to inclusion since1990. Quite clearly, this is a majorway that staff in this sample haveexpanded their learning. Of 117staff who replied, 83% had at-tended at least one conference pre-sentation or workshop on inclu-sion. An impressive 61.6% had at-tended three or more conferencepresentations or workshops, in-dicative of their interest in thisarea. Conferences and workshopswere a particularly common formof professional development andcontinuing learning for RTs, more
Front-Line Staff’s Education and Training, by Position
Table 7.2
Nature of Education and All Staff ECEs In-House RTsTraining (%) (%) (%)
Formal Education No diploma, no degree 12.9% 18.2% 6.9% Diploma, no degree 58.9% 51.5% 67.2% Degree, no diploma 17.7% 16.7% 19.0% Degree and diploma 8.9% 12.1% 5.2% Graduate degree 1.6% 1.5% 1.7%
Has obtained a credential orcertificate related to inclusion/ 16.9% 10.6% 24.1%children with special needs
Number of conferencepresentations or workshops relatedto inclusion attended since 1990:* None 17.1% 23.8% 9.3% 1 or 2 21.4% 30.2% 11.1% 3 - 5 26.5% 27.0% 25.9% 6 - 9 13.7% 11.1% 16.7% 10 or more 21.4% 7.9% 37.0%* Based on replies from 117 front-line staff (7 respondents did not reply, including 3 ECEs and 4 RTs.

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 91
7.23 Experience in the Child CareField
As described in Chapter 5, front-line staff in this study also had con-siderable experience as child careprofessionals to draw on. Only 25%of the ECEs and RTs in our samplehad five years or less experience inthe child care field, while 55% hadbeen in the field for ten or moreyears, including a full 25% who had15 or more years of experience inchild care programs. The profilesfor ECEs and in-house RTs werealmost identical in this regard. Staffwith ten or more years experiencein the child care field typically havehad many varied experiences, andhave had time to consolidate theirunderstanding of children’s devel-opment and to consider their ownvalues and philosophy.
7.3 STAFF’S ATTITUDES ANDBELIEFS ABOUT INCLUSION
A critical concern of much of theresearch on inclusion centresaround staff’s attitudes, in largepart because attitudes have beenfound to be so critical for the suc-cess of inclusion processes(Bricker, 19953 ; Eiserman, Shisler& Healey, 19954 ; Garvar-Pinhas &Schmelkin, 19895 ). Staff’s attitudesvery much shape all aspects of theinclusion process. In this study,several different components ofstaff’s attitudes were assessed.These different components in-cluded two that were fairly broad(a general measure of support forinclusion, and a measure of staff’sbeliefs about inclusion), and twothat were more personal in nature.The latter consisted of questionsthat asked about changes in staff’spersonal views over time and ameasure of each person’s sense ofefficacy/competence in working
with children with special needs.(Change in personal views andstaff’s sense of efficacy and com-petence are discussed in sections7.5 and 7.7, respectively.) Whileattitudes affect experiences, wealso note that past experiencescolour staff’s current attitudes aswell.
7.31 Staff’s Attitudes Toward Inclusion
The main measure of support forinclusion used in this study is onethat was developed by Bochner andPieterse and adapted by Denholmin 1989. This measure asks re-spondents to indicate the extent towhich they agree or disagree thatchildren with a range of specificdisabling conditions or specialneeds should be enrolled in a regu-lar preschool or child care program.(See question 3.1 in Appendix B.)Research has indicated that the na-ture of a child’s disability is one ofthe factors that influences staff’sattitudes. Generally, the more com-plex the disability, the less positivethe attitude. Children with emo-tional and behavioural issues havealso been regarded with some con-cern (Denholm, 19906 ; Eiserman,Shisler & Healey, 19957 ; Stoiber,Gettinger & Goetz, 19988 ). In thisstudy we wanted to learn if the at-titudes of early childhood profes-sionals across Canada were influ-enced by, or related to, specificneeds of the children.
Staff were asked to rate on a 5-point scale (with 1 = strongly dis-agree and 5 = strongly agree)whether they felt children with spe-cific characteristics should be en-rolled in regular child care pro-grams. The most striking resultwas that early childhood profes-sionals generally held extremelypositive attitudes toward the inclu-

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada92
sion of children with special needsfor all children, regardless of levelor type of disability.
Across thirty different conditions orspecial needs, the average score forall front-line staff was 4.1, withECEs having a mean score of 4.0and in-house RTs obtaining amean score of 4.2 out of a maxi-mum of 5.0. In fact, in 17 of the 30conditions, 80% or more front-linestaff agreed or strongly agreed thatchildren should be included inregular early childhood programs.As was the case with directors, fewstaff expressed strong disagree-ment. Lower average ratings onparticular items generally reflectedmore answers of “uncertain.”
These responses from our front-linestaff indicate very strong supportfor inclusion as an appropriatepractice in general in early child-hood programs. While there wassome variation in responses thatreflected staff’s concerns about in-cluding children with more seriousconditions, our research findingsdid not show a large discriminatorygradient based on the nature of achild’s disability. This is particu-larly noteworthy since previous re-search has noted more positive at-titudes toward inclusion for chil-dren with milder difficulties, suchas learning disabilities or moder-ate delay, than for children withbehaviour problems or more severeneeds. What was striking were thecomments from these staff that in-dicated that it was not the childrenwho were the issue, but rather theavailability and adequacy of sup-port services and resources thataffected their responses.
“In most situations my answeris also dependent on a numberof variables: physical environ-ment, philosophy of the pro-
gram, curriculum focus, numberof children, skill of leaders,amount of adult/professionalsupport, as well as looking atindividual needs of child andfamily. You just can’t do a‘dump’ and ‘run’... It is impor-tant to provide a range of pro-gram types to meet the indi-vidual needs of children andfamilies in our community. If weare to include children, we mustbe committed to providing thenecessary support to make itwork. If the right supports arein place, I believe most childrencan be successfully included.”(An ECE in British Columbia, with10 years experience in the field)
“When I disagree that some chil-dren should attend it is becauseof the lack of support if the cen-tre is not integrated (with sup-port people!) or if the physicallayout of a centre is not suit-able.” (On-site resource teacher inOntario who has worked for 10years in the child care field)
There were only eight circum-stances in which fewer than 75%of front-line staff agreed that chil-dren with a particular conditionshould be included, as shown inTable 7.3.
Several points are worth noting.First, in most cases, it is the na-ture of the assistance that is re-quired for inclusion to be success-ful that appears to be the deter-mining factor in these situations.The assistance required appears torange from structural modifica-tions that are needed to enablechildren to have adequate accesswithin the environment; to assis-tance with personal tasks, such ascatheterization with which staffmay be unfamiliar; to the need foran extra pair of hands or an addi-

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 93
tional staff person when one-on-onesupervision is required to allow thechild to participate safely. A secondpoint is that even in cases whenstaff are more hesitant, a substan-tial proportion, often a majority ofECEs and RTs, still agree that achild should be included in a regu-lar program with appropriate sup-port. A third point is that staff’s re-sponses match directors’ responsesvery closely. (Directors attained anaverage score of 4.2 on the samescale, and were hesitant about mostof the same conditions as were staff.See Table 8.2.) A final point, exem-plified in the quotes below, is thatstaff’s experiences modify their at-titudes. Positive experiences add tostaff’s skills and self-confidence;more difficult situations suggestwhere the limits to success may lie.In other quotes from staff scatteredthroughout this chapter, it is evi-dent that among the concerns staffhave is the availability of the sup-ports that are needed to ensure that
inclusion is successful for all of thechildren in a classroom or centre.
“Having experienced a numberof children with different needsat this centre, I have becomemore comfortable with the chil-dren. I remember being told Iwould have to catheterize achild and being quite uncomfort-able. Once I had to do it,though, I realized it wasn’tthat big of a deal.” (ECE,Alberta, 1 year in the field)
“I have learned that faculty andstaff have much to do with theability of a centre to care for oneor more children with specialneeds. Uncontrollably aggressivebehaviour, Tourette’s Syndromewere children we could not carefor successfully. One-on-one su-pervision was a great help forother conditions where fundingallowed.” (Early EducationTeacher, Yukon, 7 years, adminis-tration)
Circumstances in Which Fewer Than 75% of Front-Line Staff Agreed or Strongly Agreed ThatChildren with Special Needs Should Be Enrolled in Regular Early Childhood Programs
Table 7.3
artificial bowel - no parent assistance 51.8% 46.5% 57.1%
A child who at times is uncontrollably aggressive 58.7% 57.4% 59.6%
A child who is blind 69.1% 60.6% 78.9%
A child who has a phobic resistance to school attendance 63.9% 62.9% 64.9%
A child who has a multi-disabling condition 71.8% 66.7% 77.6%
A child who often cannot recognize situations involving danger to himself/herself 73.5% 70.3% 77.2%
* Statistically significant difference between ECEs and RTs, p<.05
Disability or Condition Percent of Front-Line StaffWho Agreed or Strongly Agreed
All Staff ECEs RTsA child with mobility difficulties - access 41.8% 32.2% 51.9% unsuitable
A child who requires catheterization - no parent assistance * 53.3% 42.6% * 63.6% *
A child who requires assistance with

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada94
7.32 Staff’s Beliefs About Inclusion
While child care staff’s attitudestoward inclusion are important, itis also useful to examine their be-liefs about inclusion, and to con-sider the general opinions earlychildhood professionals hold aboutinclusion as a social right, as apolicy approach, and as one of sev-eral factors that can affect otherchildren as well as child care staff.The fundamental beliefs staff holdabout the broader system that sup-ports or directs inclusion are im-portant to consider.
Seven statements about inclusion,developed specifically for thisstudy, were utilized. We asked par-ticipants to indicate their level ofagreement with each statement ona 5-point scale with 1 = stronglydisagree and 5 = strongly agree.The items tap beliefs about inclu-sion in principle; beliefs about theeffects of having children with spe-cial needs on centre staff and onother children; views as to whethermost child care programs are ac-cepting of and willing to provideinclusive care; and an item thatexamines staf f’s views aboutwhether the goal of universal in-clusion (with all children eligible tobe included in all programs) is sus-tainable when financial and humanresources are constrained.
An additional item probed front-line staff’s opinions about the ad-equacy of ECE training as prepa-ration for inclusive practice. Staff’sresponses to the seven beliefs state-ments are shown in Table 7.4.
In general, this sample of earlychildhood professionals held beliefsthat are supportive of inclusion,consistent with their responses onthe attitude scale. A large majority(77.9%) were in favour of legisla-
tion to enable full access to childcare programs, and almost 90% ofboth ECEs and in-house RTs be-lieve that most child care programsare willing to include children withspecial needs if adequate resourcesare available. It is not knownwhether a random sample of childcare staff would express this opin-ion as strongly.
Front-line staff were somewhatmore reserved about universal in-clusion when asked about all chil-dren, regardless of their individualneeds (with ECEs slightly more re-served than RTs), and when askedto respond about the situationwhen resources are not availableto support universal inclusion (itemnumber 6). In the latter circum-stance strong support for inclusionas a principle is tested. Front line-staff, as well as their directors,must then consider what will bestmeet the needs of children, parentsand staff — and painfully, manyfind this situation one that is diffi-cult to answer, since it pits theirsupport for the principle of inclu-sion against their concerns for thewell-being of all involved.
Overall, early childhood educatorsand in-house resource teachersresponded in a similar manner, al-though they did differ significantlyon two items. Resource teacherswere more likely to respond thatlegislation should be passed to en-sure that families with disabledchildren have full access to childcare programs. This is not surpris-ing since the role of resource teach-ers is to support the inclusion ofchildren with identified needs inregular programs. Resource teach-ers also were more likely to agreethat having children with specialneeds in child care programs ben-efits other children.

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 95
Early childhood educators in thisstudy, more than the RTs, consis-tently mentioned in their com-ments that they sometimesstruggled with trying to meet theneeds of all of the children in theirprogram — those with specialneeds and those without specialneeds. The ECEs reflected theirprimary mandate to provide devel-opmentally appropriate, high qual-ity care for all children. It is pos-sible that this concern is less sa-lient for resource teachers, in partbecause they most likely have lessresponsibility for the class as awhole, and tend to focus more di-rectly on including the child withspecial needs.
Of interest is the fact that neithergroup of professionals feels that theinclusion of children with special
needs puts too much pressure onstaff. (Almost 48% of ECEs dis-agreed or strongly disagreed withthis statement, while 13.8% wereuncertain; 55.2% of RTs disagreedor strongly disagreed, and 12.1%were uncertain.) It appears thatthese professionals are very confi-dent in the ability of their co-work-ers to rise to the occasion whenchildren with special needs are in-cluded (provided adequate re-sources are in place).
Interestingly, both groups had alow opinion of the training mostECEs have to prepare them to pro-vide inclusive care. Fewer than 40%of both groups agreed that ECEs’pre-service training provides themwith a good background for inclu-sive practice. Many staff com-mented that it has been their ex-
Belief Statements Percentage of Front-Line StaffWho Agreed or Strongly Agreed
All Staff ECEs In-House RTs1. Day care programs should accept all children,
regardless of their individual needs. 62.0% 54.0% 70.7%
2. Legislation should be passed to ensure disabled children and their parents have full 77.9% 73.5% * 82.8% * access to child care programs. *
3. Having children with special needs in most child care centres puts too much pressure on 35.7% 38.4% 32.8% the staff.
4. Having children with special needs in child 87.7% 81.3% * 94.8% * care benefits the non-disabled children. *
5. Most child care programs would be willing to include children with special needs, if 89.5% 89.4% 89.6% adequate resources were available.
6. It would be better to have some child care programs accept children with special needs 49.6% 56.3% 42.2% (with specialized resources) than try to have all child care programs be inclusive.
7. Training for early childhood educators has provided them with a good background to 37.9% 39.4% 36.2% support inclusion.
* Statistically significant difference between ECEs and RTs, p<.05
Front-Line Staff’s Beliefs About Inclusion, by Position
Table 7.4
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada96
periences (rather than their formaltraining) that have enabled themto feel more comfortable in theirwork with children with specialneeds and more committed toinclusion.
On a positive note, the greatest con-cern about pre-service training(highest level of agreement with thisstatement) was expressed by indi-viduals who had been in the fieldthe longest time. More recentgraduates appear to have morepositive views of the adequacy ofpre-service training experiences.
7.4 STAFF’S EXPERIENCES INPROVIDING INCLUSIVE CHILDCARE
Of all the influences on staff’s atti-tudes, their direct experience inworking with children with specialneeds is probably the most criticaland immediate factor that affectsthem. Staff who have little experi-ence are more hesitant and anxious;those who have negative experi-ences are more likely to be resis-tant; and those who have positiveexperiences are likely to be far morecommitted to inclusion and willingto extend themselves further (e.g.,Eiserman et. al., 19959 ; Dinnebeilet. al., 199810). It is possible thatstaff who are less comfortable andless committed to inclusion will se-lect centres to work in that won’tchallenge them, and that a similarselection bias operates so that cen-tres, such as many of those in ourstudy, attract and retain staff whoare supportive of inclusion. Clearly,responses from directors (in Chap-ter 8) and external resource consult-ants (in Chapter 9) confirm that thecompetencies and commitment ofcentre staff are critical to centres’effectiveness and success with in-clusion.
As described in Chapter 5, almost80 percent of the front-line staff inthis study had at least three yearsof experience in working with chil-dren with special needs. Approxi-mately 56% of the ECEs and 58%of the in-house RTs had more thanfive years’ experience, including29% of both groups who had tenor more years of experience in workwith children with special needs.At the time data were collected, 98of the 124 early childhood profes-sionals in our sample (79%) wereactively working with at least onechild with special needs.
It would be impossible to capturethe full range and richness of theseprofessionals’ experiences in theirwork with children, parents, otherstaff, directors, agencies and oth-ers over a lengthy period. Instead,we focussed our efforts on gainingan understanding of front-linestaff’s most recent experiences —particularly in the two years pre-ceding data collection.
We constructed a series of ques-tions that enabled staff to tell usboth about the experience in whichthey were most successful in thelast two years, and a situation inwhich they were less successful. Inanalysing and interpreting theirresponses, particularly to open-ended questions, we were mindfulof the multiple factors that influ-enced their experiences — thosepertaining to the child with whomthey were working, their own ex-pectations for themselves, and thesupport available to them withinthe centre and from communityprofessionals. These multiple influ-ences confirm both the importanceof adopting an ecological or trans-actional perspective for under-standing early childhood educators’experiences, and the valueof undertaking research that
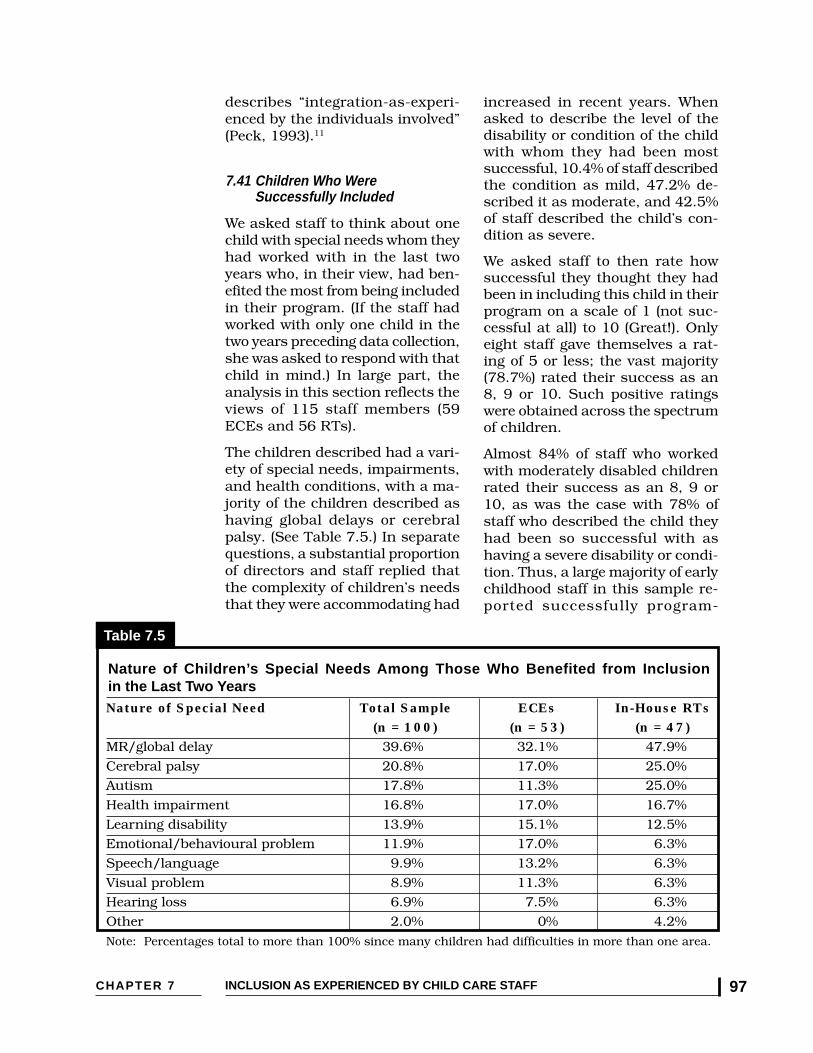
CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 97
describes “integration-as-experi-enced by the individuals involved”(Peck, 1993).11
7.41 Children Who WereSuccessfully Included
We asked staff to think about onechild with special needs whom theyhad worked with in the last twoyears who, in their view, had ben-efited the most from being includedin their program. (If the staff hadworked with only one child in thetwo years preceding data collection,she was asked to respond with thatchild in mind.) In large part, theanalysis in this section reflects theviews of 115 staff members (59ECEs and 56 RTs).
The children described had a vari-ety of special needs, impairments,and health conditions, with a ma-jority of the children described ashaving global delays or cerebralpalsy. (See Table 7.5.) In separatequestions, a substantial proportionof directors and staff replied thatthe complexity of children’s needsthat they were accommodating had
increased in recent years. Whenasked to describe the level of thedisability or condition of the childwith whom they had been mostsuccessful, 10.4% of staff describedthe condition as mild, 47.2% de-scribed it as moderate, and 42.5%of staff described the child’s con-dition as severe.
We asked staff to then rate howsuccessful they thought they hadbeen in including this child in theirprogram on a scale of 1 (not suc-cessful at all) to 10 (Great!). Onlyeight staff gave themselves a rat-ing of 5 or less; the vast majority(78.7%) rated their success as an8, 9 or 10. Such positive ratingswere obtained across the spectrumof children.
Almost 84% of staff who workedwith moderately disabled childrenrated their success as an 8, 9 or10, as was the case with 78% ofstaff who described the child theyhad been so successful with ashaving a severe disability or condi-tion. Thus, a large majority of earlychildhood staff in this sample re-ported successfully program-
Nature of Children’s Special Needs Among Those Who Benefited from Inclusionin the Last Two Years
Table 7.5
Nature of Special Need Total Sample ECEs In-House RTs(n = 100) (n = 53) (n = 47)
MR/global delay 39.6% 32.1% 47.9%
Cerebral palsy 20.8% 17.0% 25.0%
Autism 17.8% 11.3% 25.0%
Health impairment 16.8% 17.0% 16.7%
Learning disability 13.9% 15.1% 12.5%
Emotional/behavioural problem 11.9% 17.0% 6.3%
Speech/language 9.9% 13.2% 6.3%
Visual problem 8.9% 11.3% 6.3%
Hearing loss 6.9% 7.5% 6.3%
Other 2.0% 0% 4.2%
Note: Percentages total to more than 100% since many children had difficulties in more than one area.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada98
ming for and integrating childrenwith moderate and severe disabili-ties in ways they described as hav-ing been a positive experience, bothfor the child and for them as front-line staff.
7.42 Areas In Which Child Care StaffWere Most Successful
Inclusion of children with specialneeds in early childhood programsis grounded in a belief in the im-portance of social skill develop-ment, and the value of having op-portunities to learn and modelthose skills when children play to-gether in early childhood programs(Hanline, 1990) .12 Front-line staffin this study indicated that the twoareas in which they had been mostsuccessful in their work with achild with special needs were so-cialization and communication,with 50% of staff reporting social-ization as the area in which theywere most successful, followed by43.5% who said that communica-tion and language use had beensignificant areas of improvement.Other aspects of development suchas motor and self-help skills, emo-
tional development, and integrationin interacting with other childrenwere mentioned as well.
An ECE from Nova Scotia with tenyears of experience in the field de-scribed the child she had beenmost successful with:
“The child went from an at-homeone-to-one situation to five halfdays at day care within oneyear. He started to become an in-dependent little guy who wasable to care for his own needs,such as eating, toiletting, etc. Hebegan social interactions withpeers, and built up enoughstrength to go from walking forfive minutes to walking for anhour. These are just a few of hissuccesses.”
Child care staff reported consider-able success with social skill de-velopment regardless of the se-verity of the child’s disability. Thesecomments provided by staff indi-cate other substantial improve-ments:
“With support from parents,other staff, a visiting teacher,and therapists we all worked
Areas in Which Staff Were Most Successful
Table 7.6
Areas in Which Staff All Staff ECEs In-House RTsWere Most Successful (n = 115) (n = 59) (n = 56)
Socialization 50.0% 43.2% 56.3%
Communication 43.5% 45.5% 41.7%
Motor and self-help skills 33.7% 25.0% 41.7%
Emotional development 21.7% 25.0% 18.8%
Integration 21.7% 22.7% 20.8%
Deal with conflict 15.2% 20.5% 10.2%
Team approach 12.0% 6.8% 16.7%
*Multiple responses were permitted. As a result, percentages sum to more than 100.

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 99
together to achieve specificgoals for this child. By the timethis child left our program shehad made many wonderfulgains in all her areas of devel-opment.” (ECE from Alberta with11 years in the field)
“This child moved from beingnon-verbal with minimal playskills (e.g., wandering) to a childwith a wide variety of appropri-ate play skills, some expressivelanguage, and good receptivelanguage skills.” (ECE in NovaScotia with 10 years in the field)
“I was able to offer this childone-on-one resource time that fo-cused on programs crucial to herdevelopment (language, cogni-tive, fine and gross motor), aswell as the social and other as-pects of being in an integratedsetting.” (RT in N.S. with 4 yearsin the field)
Child care staff commented onother areas in which they experi-enced success, such as influenc-ing co-workers’ acceptance of in-clusion, working effectively as ateam with other professionals, andin their relationships with families:
‘(I was successful in) creating anawareness in the child care cen-tre staff that all children are inneed. Some, like M., have greaterneeds than others. Since M., thechild care staff have becomemuch more accepting when Imention a new enrollment. Par-ents have become more relaxedwith the concept of inclusion.”(ECE in Ontario with 16 years inthe field)
“Problem-solving within thechild’s team including classroomstaff, therapists, parents andfamily support workers.” (SNW/ECE in B.C. with 6 years in the field)
“Rapport with the family andchild were perhaps the areas Ifelt were the most successful.This positive relationship al-lowed all of us to enjoy our worktogether and make the best oftimes.” (RT in Ontario with 5years in the field)
7.43 Resources That Enabled Staff toBe Successful
We asked those ECEs and in-houseRTs who had worked (successfully)with a child with special needs toidentify what resources had as-sisted them and, when possible, toindicate those resources that hadbeen most crucial to their success.Most child care staff indicated thatseveral factors had been important.Responses differed somewhatacross ECEs and RTs, in part re-flecting differences in the extent towhich staff in each group had beeninvolved with a child who had moresevere or specialized disabilities orhealth problems. Across bothgroups, however, the presence of anextra special needs worker, re-source consultant and/or in-houseresource teacher was the resourcethat was most frequently men-tioned as a necessary condition forsuccessful inclusion. Two thirds offront-line staff (66.1%) said that thepresence of additional in-houseresource teachers and/or externalresource consultants/early inter-vention workers helped them besuccessful. Moreover, 21% of ECEsand in-house RTs indicated thatthe presence of extra on-site re-source teachers/special needsworkers had been crucial to theirsuccess.
Almost as many front-line staff(64.3%) reported that consultationswith, and support provided bytherapists and other specialists in
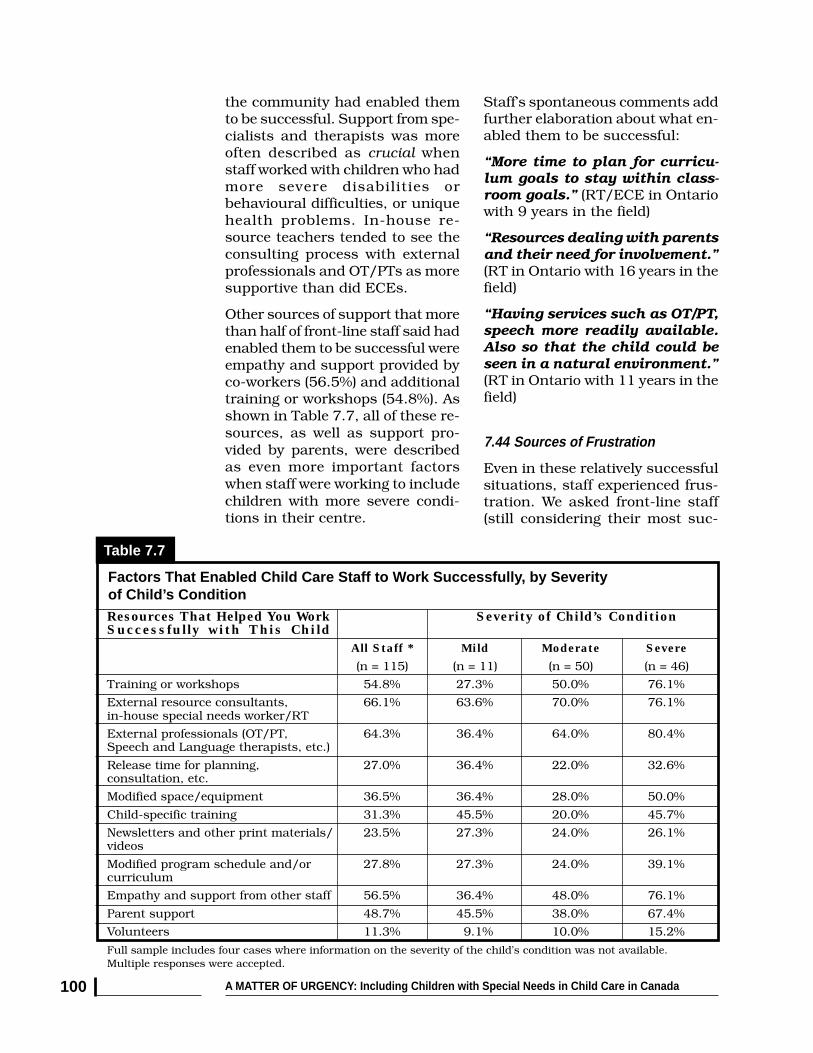
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada100
the community had enabled themto be successful. Support from spe-cialists and therapists was moreoften described as crucial whenstaff worked with children who hadmore severe disabilities orbehavioural difficulties, or uniquehealth problems. In-house re-source teachers tended to see theconsulting process with externalprofessionals and OT/PTs as moresupportive than did ECEs.
Other sources of support that morethan half of front-line staff said hadenabled them to be successful wereempathy and support provided byco-workers (56.5%) and additionaltraining or workshops (54.8%). Asshown in Table 7.7, all of these re-sources, as well as support pro-vided by parents, were describedas even more important factorswhen staff were working to includechildren with more severe condi-tions in their centre.
Staff’s spontaneous comments addfurther elaboration about what en-abled them to be successful:
“More time to plan for curricu-lum goals to stay within class-room goals.” (RT/ECE in Ontariowith 9 years in the field)
“Resources dealing with parentsand their need for involvement.”(RT in Ontario with 16 years in thefield)
“Having services such as OT/PT,speech more readily available.Also so that the child could beseen in a natural environment.”(RT in Ontario with 11 years in thefield)
7.44 Sources of Frustration
Even in these relatively successfulsituations, staff experienced frus-tration. We asked front-line staff(still considering their most suc-
Resources That Helped You Work Severity of Child’s ConditionSuccessfully with This Child
All Staff * Mild Moderate Severe
(n = 115) (n = 11) (n = 50) (n = 46)
Training or workshops 54.8% 27.3% 50.0% 76.1%
External resource consultants, 66.1% 63.6% 70.0% 76.1%in-house special needs worker/RT
External professionals (OT/PT, 64.3% 36.4% 64.0% 80.4%Speech and Language therapists, etc.)
Release time for planning, 27.0% 36.4% 22.0% 32.6%consultation, etc.
Modified space/equipment 36.5% 36.4% 28.0% 50.0%
Child-specific training 31.3% 45.5% 20.0% 45.7%
Newsletters and other print materials/ 23.5% 27.3% 24.0% 26.1%videos
Modified program schedule and/or 27.8% 27.3% 24.0% 39.1%curriculum
Empathy and support from other staff 56.5% 36.4% 48.0% 76.1%
Parent support 48.7% 45.5% 38.0% 67.4%
Volunteers 11.3% 9.1% 10.0% 15.2%
Full sample includes four cases where information on the severity of the child’s condition was not available.Multiple responses were accepted.
Factors That Enabled Child Care Staff to Work Successfully, by Severityof Child’s Condition
Table 7.7

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 101
cessful situation in the previoustwo years) what, if anything, theyhad found frustrating or problem-atic in their work with this child. Avariety of options were presentedthat respondents could check off,and space was also provided forother aspects to be identified.
Specific items were then groupedinto broader categories. Overall,
✦ 87% of child care staff foundthat coping with the child’s inability to communicate, and/orthe child’s behaviours, was achallenge for them,
✦ two thirds of staff (67%) men-tioned limited centre resources(most often insufficient time forplanning and consulting withothers) as a frustrating factor, and
✦ comparable percentages of staff(between 48 and 55%) men-tioned one or more frustrationsor problems related to thechild’s family, issues about feel-ing pulled by the needs of otherchildren, or being frustrated bytheir own limited knowledge orskills.
Overall, ECEs and RTs respondedsimilarly, with a few important dif-ferences. (See Table 7.8.) In gen-eral, however, the problems thatwere described by staff as havingbeen frustrating for them, even ina more successful situation, weresimilar to those reported in otherresearch studies (Buysse, Wesley &Keyes, 199813 ; Stoiber, Gettingerand Goetz, 199814) in which lim-ited time to plan, lack of knowledgeor training, and lack of communi-cation with families were identifiedas barriers to inclusion.
In this study, an important pointto underscore is that ECEs, in par-ticular, identified “feeling pulled by
the needs of other children” as aproblematic or frustrating factor forthem. Almost 51% of ECEs saidthis had been a source of frustra-tion or stress, as did 43% of the in-house RTs. This is a unique find-ing in the inclusion research, andone that obviously reflects inclu-sion-as-experienced by a substan-tial proportion of front-line childcare staff in our sample, given thecircumstances existing in their pro-grams, and the type and level ofresources available to support in-clusion.
ECEs were also far more likely toreport that their own lack of knowl-edge or training was a source offrustration for them (mentioned by42.4% of ECEs, compared to 19.6%of RTs). In contrast, RTs (whotended to be involved with childrenwith more severe conditions) weremore likely to say that the child’sinability to communicate or beengaged had been frustrating orproblematic for them.
7.45 Resources That Would HaveHelped
We next asked front-line staff to tellus what would have helped themwork more effectively when prob-lems did arise. The most frequentlymentioned resource (provided by51.4% of respondents) was, again,more support for staff — especiallythe need for additional centre-based personnel such as an in-house resource teacher or supportworker. Additional information andtraining was mentioned by almost42% of front-line staff in oursample, and more frequently byECEs than in-house RTs. [We re-mind readers that these responseswere provided by a sample that hasmore formal training, more in-ser-vice training and conference expo-
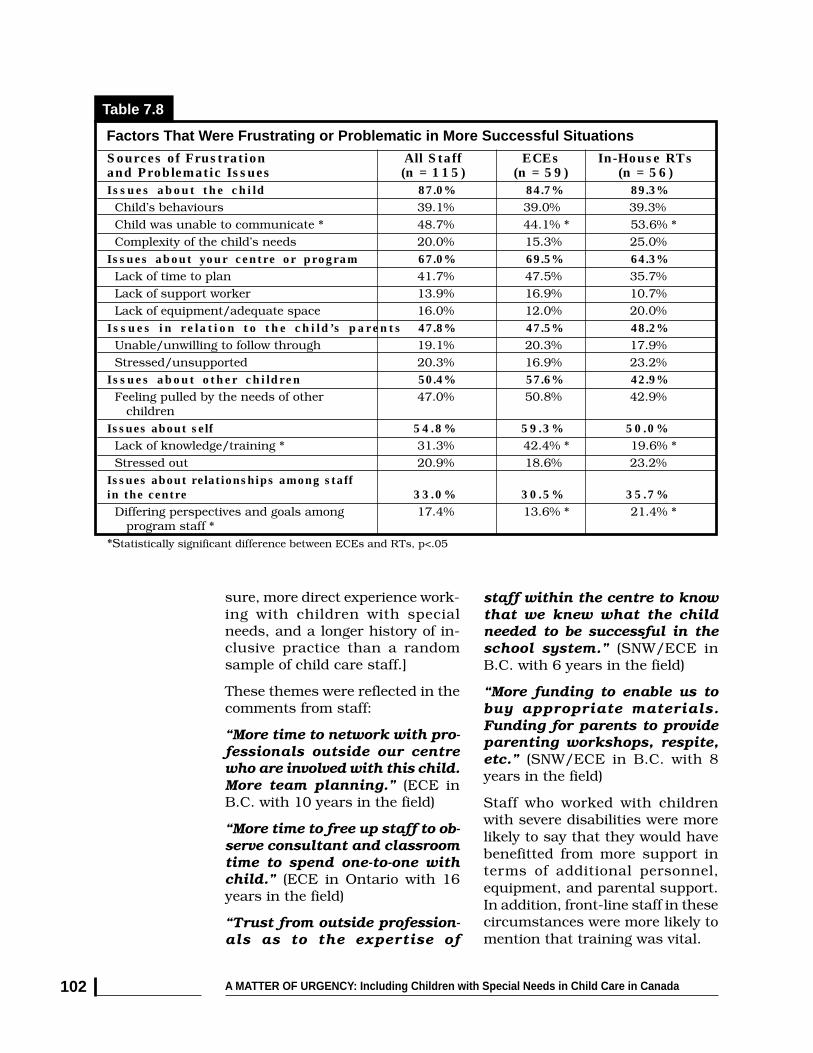
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada102
sure, more direct experience work-ing with children with specialneeds, and a longer history of in-clusive practice than a randomsample of child care staff.]
These themes were reflected in thecomments from staff:
“More time to network with pro-fessionals outside our centrewho are involved with this child.More team planning.” (ECE inB.C. with 10 years in the field)
“More time to free up staff to ob-serve consultant and classroomtime to spend one-to-one withchild.” (ECE in Ontario with 16years in the field)
“Trust from outside profession-als as to the expertise of
staff within the centre to knowthat we knew what the childneeded to be successful in theschool system.” (SNW/ECE inB.C. with 6 years in the field)
“More funding to enable us tobuy appropriate materials.Funding for parents to provideparenting workshops, respite,etc.” (SNW/ECE in B.C. with 8years in the field)
Staff who worked with childrenwith severe disabilities were morelikely to say that they would havebenefitted from more support interms of additional personnel,equipment, and parental support.In addition, front-line staff in thesecircumstances were more likely tomention that training was vital.
Sources of Frustration All Staff ECEs In-House RTsand Problematic Issues (n = 115) (n = 59) (n = 56)Issues about the child 87.0% 84.7% 89.3% Child’s behaviours 39.1% 39.0% 39.3% Child was unable to communicate * 48.7% 44.1% * 53.6% * Complexity of the child’s needs 20.0% 15.3% 25.0%Issues about your centre or program 67.0% 69.5% 64.3% Lack of time to plan 41.7% 47.5% 35.7% Lack of support worker 13.9% 16.9% 10.7% Lack of equipment/adequate space 16.0% 12.0% 20.0%Issues in relation to the child’s parents 47.8% 47.5% 48.2% Unable/unwilling to follow through 19.1% 20.3% 17.9% Stressed/unsupported 20.3% 16.9% 23.2%Issues about other children 50.4% 57.6% 42.9% Feeling pulled by the needs of other 47.0% 50.8% 42.9% childrenIssues about self 54.8% 59.3% 50.0% Lack of knowledge/training * 31.3% 42.4% * 19.6% * Stressed out 20.9% 18.6% 23.2%Issues about relationships among staffin the centre 33.0% 30.5% 35.7% Differing perspectives and goals among 17.4% 13.6% * 21.4% * program staff **Statistically significant difference between ECEs and RTs, p<.05
Factors That Were Frustrating or Problematic in More Successful Situations
Table 7.8

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 103
7.46 Staff’s Less SuccessfulExperiences
Inclusion is not always a success-ful or positive experience. For anumber of reasons, barriers anddifficulties can arise, making theprocess difficult and stressful. Inorder to fully understand child carestaff’s experience and take steps toreduce barriers and the likelihoodof poor experiences for children,parents, staff and centres, it is im-portant to study these situationsas well. Accordingly, we also askedour sample of ECEs and in-houseRTs to tell us about a situation inthe last two years in which they hadbeen less successful and to explainwhat had been most problematicor frustrating for them. This sec-tion was open-ended, allowing staffto express themselves more freely.Staff’s responses are summarizedin Table 7.10.
Two points are of particular inter-est: staff’s difficult experiences inworking with parents, and the frus-tration early childhood staff expe-rience when insufficient support
frustrates their efforts to includechildren with major behaviouralproblems, given their commitmentto try to include all children in childcare programs.
Both ECEs and in-house RTs(43.6% of all staff) mentioned diffi-culties working with parents as aprimary source of frustration wheninclusion was problematic. Inter-estingly, parent support was alsoidentified as a critically importantresource when children with moresevere conditions or behaviouralproblems were successfully in-cluded. It thus seems that parent-staff relationships function as adouble-edged sword — potentiallymaking or breaking the success ofinclusion efforts. When parents area resource, they are vital for success.
However, when communication ispoor, there is a lack of shared com-mitment, or conflict cannot be re-solved, the success of staff’s effortsis very much in jeopardy. Clearly,this is an issue that should be ad-dressed, to the extent it can be,through in-service workshops and
Resources That Would Have All Staff ECEs In-House RTsHelped (n = 115) (n = 59) (n = 56)
More information or training 41.9% 48.6% 35.1%
More staff support 51.4% 56.8% 45.9%
Equipment 12.1% 8.4% 18.9%
Help from specialists, external 16.2% 13.5% 18.9%sources (OT/PT, etc.)
More time to plan 14.9% 16.2% 13.5%
Funding 2.7% 2.7% 2.7%
Parent support 12.2% 10.8% 13.5%
Other 4.1% 5.4% 2.7%
Resources That Would Have Helped When Problems Arose
Table 7.9
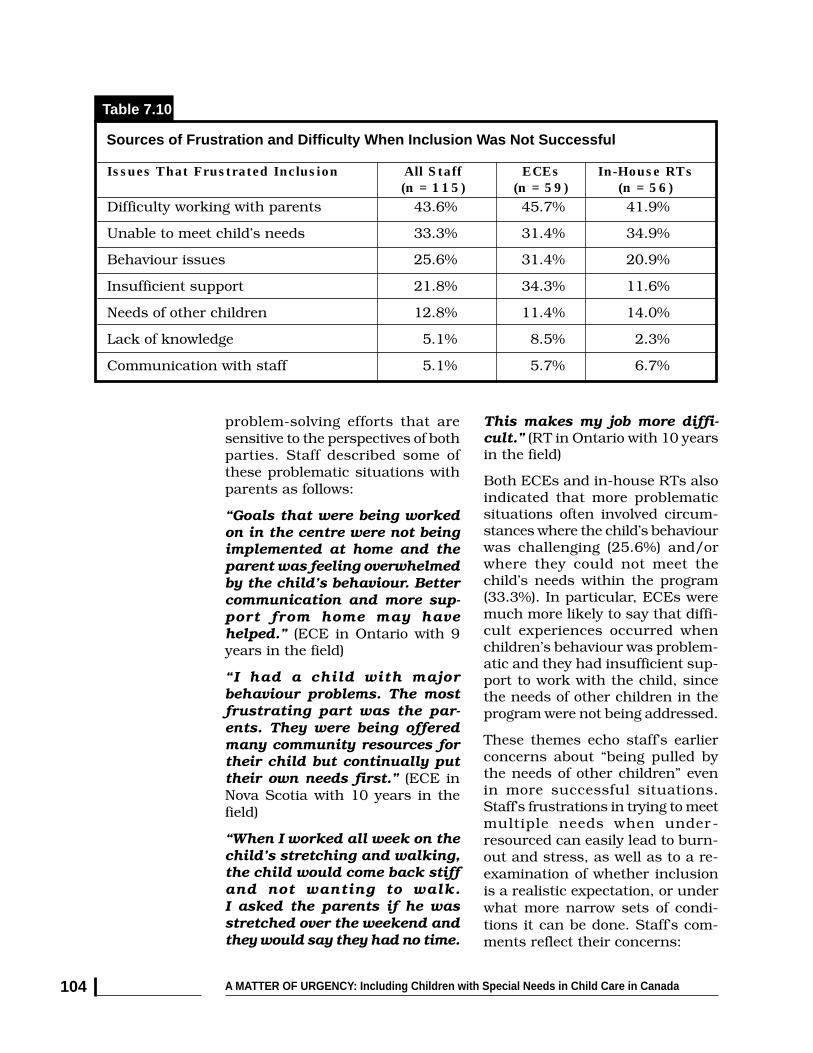
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada104
problem-solving efforts that aresensitive to the perspectives of bothparties. Staff described some ofthese problematic situations withparents as follows:
“Goals that were being workedon in the centre were not beingimplemented at home and theparent was feeling overwhelmedby the child’s behaviour. Bettercommunication and more sup-port from home may havehelped.” (ECE in Ontario with 9years in the field)
“I had a child with majorbehaviour problems. The mostfrustrating part was the par-ents. They were being offeredmany community resources fortheir child but continually puttheir own needs first.” (ECE inNova Scotia with 10 years in thefield)
“When I worked all week on thechild’s stretching and walking,the child would come back stiffand not wanting to walk.I asked the parents if he wasstretched over the weekend andthey would say they had no time.
Issues That Frustrated Inclusion All Staff ECEs In-House RTs(n = 115) (n = 59) (n = 56)
Difficulty working with parents 43.6% 45.7% 41.9%
Unable to meet child’s needs 33.3% 31.4% 34.9%
Behaviour issues 25.6% 31.4% 20.9%
Insufficient support 21.8% 34.3% 11.6%
Needs of other children 12.8% 11.4% 14.0%
Lack of knowledge 5.1% 8.5% 2.3%
Communication with staff 5.1% 5.7% 6.7%
Sources of Frustration and Difficulty When Inclusion Was Not Successful
Table 7.10
This makes my job more diffi-cult.” (RT in Ontario with 10 yearsin the field)
Both ECEs and in-house RTs alsoindicated that more problematicsituations often involved circum-stances where the child’s behaviourwas challenging (25.6%) and/orwhere they could not meet thechild’s needs within the program(33.3%). In particular, ECEs weremuch more likely to say that diffi-cult experiences occurred whenchildren’s behaviour was problem-atic and they had insufficient sup-port to work with the child, sincethe needs of other children in theprogram were not being addressed.
These themes echo staff’s earlierconcerns about “being pulled bythe needs of other children” evenin more successful situations.Staff’s frustrations in trying to meetmultiple needs when under -resourced can easily lead to burn-out and stress, as well as to a re-examination of whether inclusionis a realistic expectation, or underwhat more narrow sets of condi-tions it can be done. Staff’s com-ments reflect their concerns:

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 105
“Lack of support for behaviouralproblems that require a specialneeds worker, seeing other chil-dren miss their activities and/or time with an ECE becausemost of the time is taken upguiding or coping with onechild’s behaviour problems.”(ECE in Manitoba with 8 years inthe field)
“Even with all our resources andsupports we often feel stretchedto the limit. We are getting chil-dren with more and more com-plex needs and conditions asother institutional settingsclose. Being denied support nec-essary for the proper inclusionof a child means we all lose.”(ECE in Nova Scotia with 10 yearsin the field)
“Lack of progress with very ag-gressive behaviour. Child neededone-to-one but funding was un-available. Parent wasn’t in-volved in supporting our ef-forts.” (ECE in Yukon with 7 yearsin the field)
“Spread too thinly — not enoughtime to do the kind of job I feelis most beneficial to the stu-dent.” (RT in Ontario with 11 yearsin the field)
“Dealing with child’s behaviourwhen resource person was notaround. Having to devote 100%of attention on one child whenthere are 7 others in the group.”(ECE in Ontario with 16 years inthe field)
“Lack of support. Not being ableto give the other children in myclass the attention I wanted togive because I had no aide andhe needed so much 1:1, espe-cially during transitions andcircle time.” (ECE in Alberta with12 years in the field)
To summarize, lack of supportfrom parents and limitedresources (especially limitedresource staff) figured prominentlyin front-line staff’s accounts ofless successful inclusion experi-ences. On-site resource staff,support from other professionals,training, parent and co-workersupport, and time for plan-ning were the resourcesidentified as most important forsuccess.
7.5 PERSONAL CHANGE INSTAFF’S VALUES ANDFEELINGS
In addition to assessing more gen-eral attitudes and beliefs about in-clusion at the time data were col-lected and obtaining staff’s de-scriptions of their experiences inworking with children with specialneeds, we also wanted to under-stand whether staf f hadexperienced any significantchanges in their personal valuesand feelings. Accordingly, weasked staf f whether theirexperiences since 1990 hadaffected their personal views andfeelings. Specifically, we asked allfront-line staff three questions:
✦ Are you more committed to theconcept of inclusion now or lesscommitted?
✦ Philosophically, are you moreaccepting of a broader range ofchildren being served or morecautious about the range ofchildren who can be accommo-dated in regular child careprograms?
✦ Are you more comfortableworking with children who havespecial needs now than youwere before, or less so?

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada106
We also invited staff to write in com-ments if they so wished. Staff’s re-sponses are summarized in Figures7.1 and 7.2.
Clearly, the majority of front-linestaff in this selected sample re-ported changes in personal viewsthat are supportive of inclusion.
✦ More than two thirds (67.8%)said they were more or some-what more committed to inclu-
RESOURCE TEACHERS’ ATTITUDES TOWARDS INCLUSION
Figure 7.2
Committed Accepting Comfortable
More No Change Less
72%
23%
5%
68%
20%12%
71%
27%
2%
20%
30%
0%
10%
60%70%
40%
50%
100%
80%
90%
sion than they had been previ-ously;
✦ About 60% were accepting of abroader range of children par-ticipating in child care pro-grams, and
✦ A very large percentage (76.9%)said they were more comfortableworking with children with spe-cial needs than they had beenpreviously.
EARLY CHILDHOOD EDUCATORS’ ATTITUDES TOWARDS INCLUSION
Figure 7.1
Committed Accepting Comfortable
More No Change Less
64%
27%
9%
54%
31%
15%
82%
17%
1%
20%
30%
0%
10%
60%70%
40%
50%
100%
80%
90%

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 107
Compared to directors, front-linestaff reported both more change intheir personal values and morepositive change. (About 50% of cen-tre directors were more committedto inclusion and 53% of directorswere more accepting of a broaderrange of children being included.Sixty percent of directors said theywere more comfortable workingwith children with special needs.Many directors experienced littlechange since 1990 in these threeareas, sometimes indicating, forexample, that they had always beencommitted, or had always beencomfortable working with childrenwith special needs. See Chapter 8,Section 8.5.)
Interestingly, there were no signifi-cant differences betwen ECEs andin-house resource teachers. Therewas, however, evidence of a pro-gression. Many staff stated that itwas their experience working withchildren with special needs thathad enabled them to become morecomfortable. Once their comfortlevel increased, they tended to thenbecome more committed to inclu-sion and more accepting of abroader range of children beingserved in child care programs.
Of all front-line staff, only nine saidthey were less committed now thanthey had been previously, and onlytwo said they were less comfortableworking with children with specialneeds. However seventeen childcare staff (or one in seven who re-plied) said they were somewhatmore cautious about the range ofchildren who could be accommo-dated in regular child care pro-grams. In some cases, this re-sponse clearly reflected the resultsof a less successful experience withinclusion. In contrast, however,staff who had positive experienceswere more accepting, as demon-
strated in the quotes that follow.
LESS COMMITTED AND LESSACCEPTING:
“I have seen too many timeswhen staff have no choice.Children are brought into theprograms without the re-sources in place....
“More cautious, especiallynow that they are trying tomainstream autistic children.”(Comment from an ECE in Ontariowith 16 years experience in child care)
MORE ACCEPTING AND MORECOMFORTABLE:
“I am much more accepting,having worked with a broaderrange of children. Each isunique and brings somethingspecial to our class...
“Much more comfortable. In thepast, I would have been muchmore apprehensive — a typi-cal fear of the unknown. Ihave learned so much fromthese children and am certainthere is much more to learn.”(Both quotes from an ECE in NewBrunswick, 3 years in the field)
MORE ACCEPTING AND MORECOMFORTABLE:
“Experience is the bestteacher. We have given twoweeks, then a one-month trialperiod in situations we wereunsure of and have many suc-cess stories...
“There is still so much tolearn. All children have spe-cial needs.” (Comments from anECE in the Yukon with 7 years ex-perience)

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada108
MORE COMMITTED, ACCEPTINGAND COMFORTABLE:
“I feel that now that I am ac-tively working as a resourceteacher that my responsibili-ties have changed. I now striveharder to achieve inclusion formy families and assist the ECEstaff at the day care centre tounderstand how inclusion isessential for all children, andhow they can achieve inclu-sion in the classroom...
“Practical experience hasgiven me the understanding,skills and resources to workwith children with specialneeds and their families.”(Comments from a resourceteacher in Ontario, 7 years in thefield)
Based on these results, it could besaid that the majority of early child-hood professionals in this samplehave fully embraced the philosophyof inclusive practice, in the waythey act and feel about children.No longer is it necessary to try toconvince these early childhood pro-fessionals about the value of inclu-sion. Rather the question is howbest to support their commitment sothat all children with disabilitiescan be included with the necessaryresources in place to make the pro-cess a success.
7.6 CHANGES IN CENTRES THATIMPACT ON INCLUSION
In the last section we observed thatboth positive experiences and theacquisition of additional knowledgeand skills based on those experi-ences are important contributorsto staff’s comfort level and commit-ment. However, staff’s experienceswith individual children do nothappen in a vacuum. They occur
in centres that are, themselves,benefiting from past experience,adapting to change, and experienc-ing different demands. Centres arealso affected by changes in policiesand funding allotments that caneither promote or jeopardize thecentre’s capacity to effectively in-clude children with special needs.(These matters are described inChapter 8.)
We asked front-line staff to tell us,from their perspective, how thingshad changed for them or their cen-tre in the last few years. Specifi-cally, we asked staff to tell uswhether the complexity ofchildren’s special needs in the pro-gram had increased, decreased orstayed the same. Similar questionswere asked about time provided forplanning or consulting; the effec-tiveness of centre staff working to-gether as a team within the pro-gram; the availability and involve-ment of resource teachers, integra-tion workers and others; and theirown competencies and knowledgebase.
As shown in Table 7.11, 45.4% offront-line staff reported that, overtime, their centre has accepted chil-dren with more complex conditionsor special needs — a finding thatis consistent with reports from pro-gram directors. Almost as manystaff (41.2%) reported no change inthis regard; few staff or programsin this sample are working withchildren with less complex or chal-lenging needs than was the case inthe recent past. Was there a com-mensurate increase in resources tosupport inclusion or even sustainexisting capabilities?
According to our sample, the mostpositive changes related to an in-crease in their own knowledge andcompetence and, in some cases,
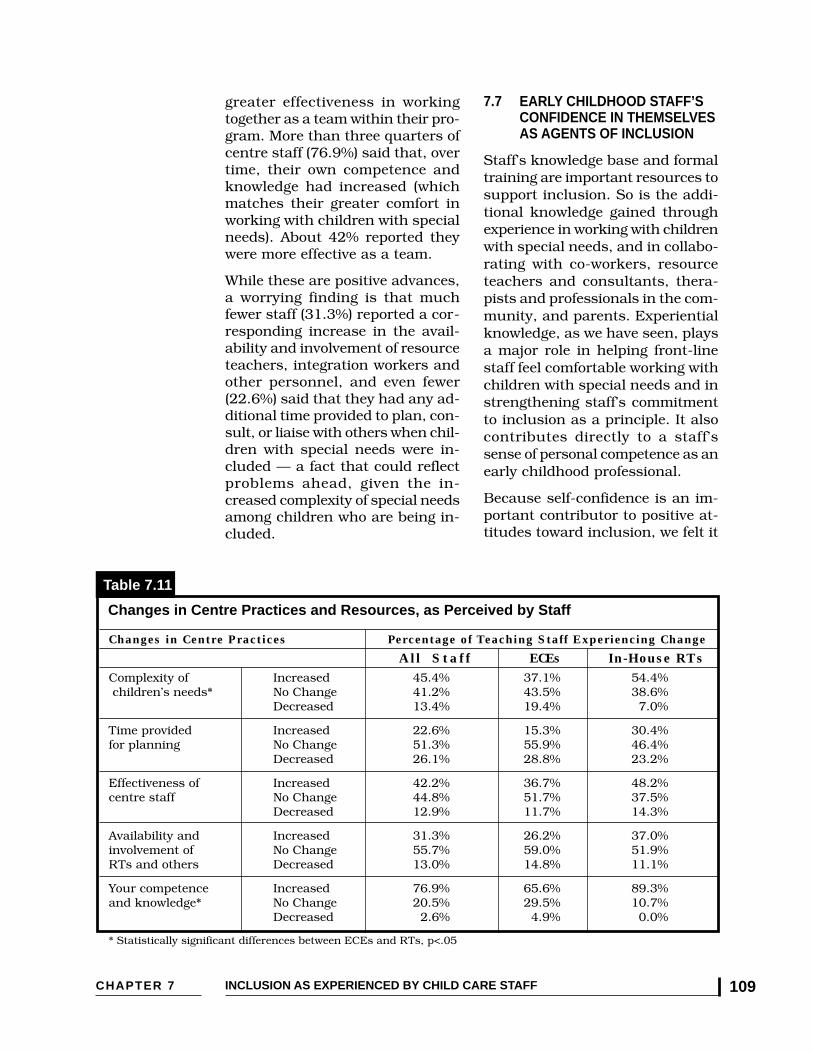
CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 109
greater effectiveness in workingtogether as a team within their pro-gram. More than three quarters ofcentre staff (76.9%) said that, overtime, their own competence andknowledge had increased (whichmatches their greater comfort inworking with children with specialneeds). About 42% reported theywere more effective as a team.
While these are positive advances,a worrying finding is that muchfewer staff (31.3%) reported a cor-responding increase in the avail-ability and involvement of resourceteachers, integration workers andother personnel, and even fewer(22.6%) said that they had any ad-ditional time provided to plan, con-sult, or liaise with others when chil-dren with special needs were in-cluded — a fact that could reflectproblems ahead, given the in-creased complexity of special needsamong children who are being in-cluded.
7.7 EARLY CHILDHOOD STAFF’SCONFIDENCE IN THEMSELVESAS AGENTS OF INCLUSION
Staff’s knowledge base and formaltraining are important resources tosupport inclusion. So is the addi-tional knowledge gained throughexperience in working with childrenwith special needs, and in collabo-rating with co-workers, resourceteachers and consultants, thera-pists and professionals in the com-munity, and parents. Experientialknowledge, as we have seen, playsa major role in helping front-linestaff feel comfortable working withchildren with special needs and instrengthening staff’s commitmentto inclusion as a principle. It alsocontributes directly to a staff’ssense of personal competence as anearly childhood professional.
Because self-confidence is an im-portant contributor to positive at-titudes toward inclusion, we felt it
Changes in Centre Practices Percentage of Teaching Staff Experiencing Change
All Staff ECEs In-House RTsComplexity of Increased 45.4% 37.1% 54.4% children’s needs* No Change 41.2% 43.5% 38.6%
Decreased 13.4% 19.4% 7.0%
Time provided Increased 22.6% 15.3% 30.4%for planning No Change 51.3% 55.9% 46.4%
Decreased 26.1% 28.8% 23.2%
Effectiveness of Increased 42.2% 36.7% 48.2%centre staff No Change 44.8% 51.7% 37.5%
Decreased 12.9% 11.7% 14.3%
Availability and Increased 31.3% 26.2% 37.0%involvement of No Change 55.7% 59.0% 51.9%RTs and others Decreased 13.0% 14.8% 11.1%
Your competence Increased 76.9% 65.6% 89.3%and knowledge* No Change 20.5% 29.5% 10.7%
Decreased 2.6% 4.9% 0.0%
* Statistically significant differences between ECEs and RTs, p<.05
Changes in Centre Practices and Resources, as Perceived by Staff
Table 7.11
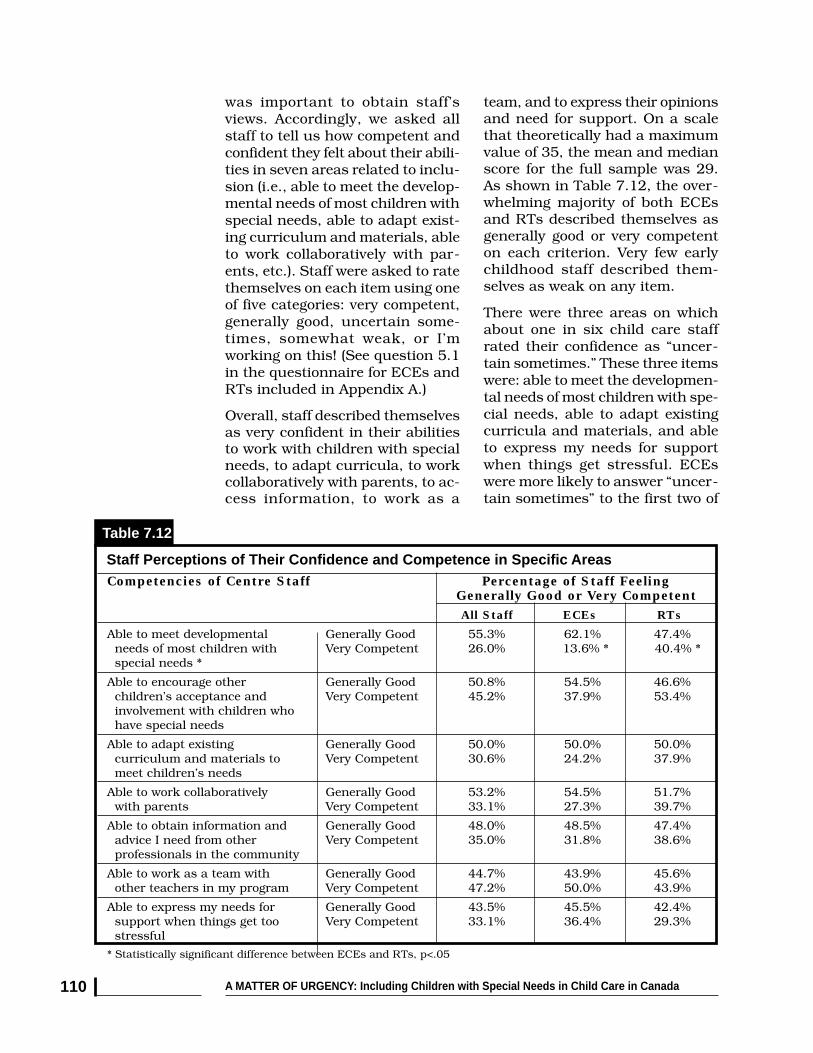
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada110
was important to obtain staff’sviews. Accordingly, we asked allstaff to tell us how competent andconfident they felt about their abili-ties in seven areas related to inclu-sion (i.e., able to meet the develop-mental needs of most children withspecial needs, able to adapt exist-ing curriculum and materials, ableto work collaboratively with par-ents, etc.). Staff were asked to ratethemselves on each item using oneof five categories: very competent,generally good, uncertain some-times, somewhat weak, or I’mworking on this! (See question 5.1in the questionnaire for ECEs andRTs included in Appendix A.)
Overall, staff described themselvesas very confident in their abilitiesto work with children with specialneeds, to adapt curricula, to workcollaboratively with parents, to ac-cess information, to work as a
team, and to express their opinionsand need for support. On a scalethat theoretically had a maximumvalue of 35, the mean and medianscore for the full sample was 29.As shown in Table 7.12, the over-whelming majority of both ECEsand RTs described themselves asgenerally good or very competenton each criterion. Very few earlychildhood staff described them-selves as weak on any item.
There were three areas on whichabout one in six child care staffrated their confidence as “uncer-tain sometimes.” These three itemswere: able to meet the developmen-tal needs of most children with spe-cial needs, able to adapt existingcurricula and materials, and ableto express my needs for supportwhen things get stressful. ECEswere more likely to answer “uncer-tain sometimes” to the first two of
Competencies of Centre Staff Percentage of Staff Feeling Generally Good or Very Competent
All Staff ECEs RTs
Able to meet developmental Generally Good 55.3% 62.1% 47.4% needs of most children with Very Competent 26.0% 13.6% * 40.4% * special needs *
Able to encourage other Generally Good 50.8% 54.5% 46.6% children’s acceptance and Very Competent 45.2% 37.9% 53.4% involvement with children who have special needs
Able to adapt existing Generally Good 50.0% 50.0% 50.0% curriculum and materials to Very Competent 30.6% 24.2% 37.9% meet children’s needs
Able to work collaboratively Generally Good 53.2% 54.5% 51.7% with parents Very Competent 33.1% 27.3% 39.7%
Able to obtain information and Generally Good 48.0% 48.5% 47.4% advice I need from other Very Competent 35.0% 31.8% 38.6% professionals in the community
Able to work as a team with Generally Good 44.7% 43.9% 45.6% other teachers in my program Very Competent 47.2% 50.0% 43.9%
Able to express my needs for Generally Good 43.5% 45.5% 42.4% support when things get too Very Competent 33.1% 36.4% 29.3% stressful
* Statistically significant difference between ECEs and RTs, p<.05
Staff Perceptions of Their Confidence and Competence in Specific Areas
Table 7.12

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 111
these three items; in-house RTswere more uncertain about theirconfidence in being able to expressneeds for additional support. Onthe whole, however, staff in thissample presented a remarkablypositive sense of their capabilitiesacross all seven areas.
While both ECEs and in-house RTsrated themselves as feeling good orvery competent across all areas,some differences are worthy ofnote. Resource teachers (40.4%)were significantly more likely todescribe themselves as very confi-dent of their ability to meet the de-velopmental needs of children withspecial needs than were ECEs(13.6%). This is not surprisingwhen one considers the fact thatthe training resource teachers re-ceive is much more directed towarddeveloping individual programplans to meet developmental needsfor children with disabilities. Whatwas exciting was the fact that mostECEs in this sample do feel goodabout their ability to meetchildren’s developmental needs —again, most often as a result ofpositive experiences with inclusion.While not a statistically significantdifference, it is interesting to notethat RTs were more likely thanECEs to describe themselves as veryconfident and competent on all butthe last two items: able to work ef-fectively as a team with other staff,and able to express their own needsfor personal support.
7.8 FUTURE TRAINING NEEDS TOSUPPORT INCLUSION
We also asked staff to identify thoseareas in which they would like ad-ditional training, technical assis-tance, or information from alengthy check list. The answersprovided by front-line staff indicatesignificant interest on a range of
topics and similarities and differ-ences between ECEs and RTs.More than a third of ECEs who re-sponded were receptive to moretraining or additional informationon 7 of the 13 items presented;more than a third of RTs were re-ceptive to having more informationor training on 9 of the 13 items onour list. In fact, all of the topics weprovided on a broad menu were ofinterest to at least one quarter ofall front-line staff. (See Table 7.13on following page.)
While there were some importantdifferences between ECEs and RTs,it is interesting to note that morethan half of both groups identifiedstrong interest in additional infor-mation and training on two topics:how to work with and support fami-lies, and promoting social interac-tions between children with specialneeds and other children. We haveseen previously that relationshipswith parents is a critical factor inboth successful and difficult inclu-sion experiences. The strong inter-est in promoting social interactionsamong children with different abil-ity levels appears to be one thatepitomizes successful inclusion.
There was a statistically significantdifference in the percentage ofECEs and in-house resource teach-ers who wanted more informationor training in five areas. ECEs ex-pressed more interest on two verygeneral topics (often identified bythose who have less experience orformal training in an area): generalinformation on children with spe-cial needs, and caring for childrenwith special needs. In contrast, in-house resource teachers were morelikely to want additional informa-tion/training on how to maintainquality care in a period of dimin-ishing resources, on how other cen-tres mainstream effectively, and

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada112
how to work collaboratively withspecialists — which is one of theirmajor responsibilities. The differ-ences in training needs between thetwo groups is not surprising(Kontos & File, 199315). ECEswould like more information onchildren with special needs andhow to work with them directlywithin their classrooms. Resourceteachers, who have more special-ized training, struggle more withoverriding questions related toquality and inclusion, which per-haps ECEs work with more con-cretely on a daily basis. On thewhole, staff would like training onhow to work with families, promotesocial interactions, and maintainquality care, as well as more spe-cific in-depth information on chil-dren with special needs. Whilethere are some advantages to pro-viding information sessions and
training to mixed groups, it is alsoimportant to ensure that there besome opportunities for separatesessions so that staff can partici-pate in in-service activities thatbest meet their particular needs.
7.9 RELATIONSHIPS BETWEENEDUCATION, ATTITUDES ANDEXPERIENCE
It is beyond the scope of this re-port to go into detailed analyses ofhow multiple dimensions of edu-cation and training, attitudes, andexperience relate to each otheramong front-line staff and in ourtwo subgroups. Analysis of inter-relationships were undertaken andwill be reported in more detail else-where.
In general, and in contrast to theliterature reviewed in Chapter 3, we
Areas for Future Training Percentage of Staff Who Would LikeFurther Training
All Staff ECEs RTs
General information about special needs * 27.5% 35.9% * 17.9% *Specific in-depth information about particular 49.2% 45.3% 53.6% disabilitiesCaring for children with special needs * 31.9% 45.3% * 16.4% *How to work with and support families 53.3% 51.6% 55.4%How to work collaboratively with agencies 37.2% 31.3% 43.9% (CAS, schools, etc.)Promoting social interactions between children 53.3% 54.7% 51.8% with special needs and other childrenMaintaining and promoting quality care in a 50.4% 37.5% * 64.9% * period of diminishing resources *How other centres mainstream effectively * 40.5% 32.8% * 49.1% *Adapting my curriculum to suit individual needs 27.7% 31.3% 23.6%Developing and implementing individual 32.8% 34.4% 30.9% program plansAdvocating on behalf of children and families 30.0% 25.0% 35.7% with special needsHow to work collaboratively with specialists * 31.7% 23.4% * 41.1% *How to work as a team within the centre on 31.9% 25.4% 39.3% behalf of children with special needs* Statistically significant difference between ECEs and RTs, p<.05
Percentage of Staff Wanting Additional Information or Training on a Variety of Topics, by Position
Table 7.13

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 113
found few specific, statisticallysignificant associations betweenthe amount of formal ECE-relatededucation staff had and their atti-tudes or beliefs about inclusion, orthe extent to which they reportedany positive change in their per-sonal values (more committed,more accepting of a broader rangeof children being included, morecomfortable working with childrenwith special needs).
This is not surprising to us for threereasons. The first is that thissample was selected in a way thatmaximized the likelihood of recruit-ing staff who had positive attitudestowards inclusion, since they hadeither participated in an earlierstudy on this topic or were work-ing in centres that had a history ofproviding inclusive care within apermissive policy structure. In-deed, the vast majority of staff inthis sample, as we have shown, arestrongly supportive of inclusion asa general practice in early child-hood education and child care.
The second factor accounting forlimited correlations between edu-cation/training and attitudes isthat this sample was fairly homo-geneous with respect to their edu-cational background. Almost allhad a two-year diploma or univer-sity degree in ECE or a related field.Even staff who had little special-ized training as part of their for-mal pre-service education attendedconferences and in-service pro-grams and many had workedalongside others, including in-house resource teachers or travel-ling consultants, to supplementtheir formal education. As a result,there was little range among staffin their education or their attitudestowards inclusion, or their feelingsof confidence in working to supportinclusion. When there is little vari-
ability within a sample, there islittle likelihood of finding statisti-cal associations among variables.A third factor, as staff told us, isthat it is their direct experienceswith children and families that hasmost affected their comfort level,their attitudes toward inclusion,and their views about the range ofchildren who can be included suc-cessfully.
A second and interesting summarypoint to share with readers was asomewhat unanticipated findingthat linked both years of experiencein the child care field in general andyears of experience working withchildren with special needs withstaff’s feelings of confidence andcompetence and their desire formore information and training.
Specifically, while we found an ex-pected general trend indicating thatthose with the most experience aremore confident, we also found evi-dence that staff with 3-5 years ofexperience in child care, on thewhole, express less confidence intheir skills related to inclusion thanany other group.
Further, we find that staff juststarting out with only one or twoyears of experience in child care orin working with children with spe-cial needs were more likely to wanttraining on almost all facets relatedto inclusion, and to have beliefsthat were somewhat more ambiva-lent about whether inclusion putstoo much pressure on staff, andabout expecting inclusion to be auniversal practice when resourcesare limited.
We interpret these findings as evi-dence that confirms theoreticalperspectives about how early child-hood professionals continue todevelop once in the field, with

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada114
in the Renewal Stage in Katz’stheory, in which they may be ques-tioning their own skills and prac-tices, which impact on their feel-ings of confidence. Early childhoodstaff in this stage seem to be par-ticularly interested in comparingtheir practice and their centre’spractices with others. Staff with 3-5 years experience in our sampleexpressed less interest in topicssuch as caring for children withspecial needs, advocating for chil-dren and families, or promotingsocial interactions among children.Instead, they were particularly in-terested in learning how other cen-tres mainstream effectively.
Centre directors and those with re-sponsibility for designing in-serviceworkshops at conferences and con-tinuing education programs mightnote these findings and take theminto account in providing learningexperiences for child care staff.Those who are in the Renewal stageof their development may need ad-ditional emotional support and, inparticular, may benefit from dis-cussions with peers in other pro-grams and from spending time ob-serving other programs.
7.10 SUMMING UP
The front-line staff who partici-pated in this study provided uswith much rich information. Whilethis group is not representative ofa broader national sample, they didprovide a window through whichwe could view what they experienceas front-line professionals whohave already embraced a commit-ment to inclusion, and who are try-ing very hard to make it work well,both for children with special needsand for all the other children intheir care. They confirmed for usthe extent to which many early
specific reference to Lillian Katz’swritings about early childhood edu-cators’ developmental stages (Katz,1995 ).16 Our data indicate that theearly childhood professionals in oursample with 1-2 years experienceworking with children with specialneeds are in the Stage I - Survivaland Stage II - Consolidation peri-ods. During Stage I - Survival, staffrequire “direct help with specificskills and insights into complexbehaviors” (Katz, p. 206). DuringStage II - Consolidation, staff startto focus on individual children’sneeds.
Therefore, it is not surprising thatthose staff with least experiencewould want more training of a spe-cific nature, would want informa-tion on caring for children withspecial needs, and support on howto promote social interaction. Be-cause they want to consolidatetheir own skills, these staff wereleast interested in visiting othercentres, but the most interested inlearning how to adapt their cur-riculum, how to develop individualprogram plans, and how to workwith other specialists.
Interestingly, the staff who mostrecently entered the field were morelikely to say that ECE programsprovide a good background forworking in inclusive programs. Thismay suggest that training pro-grams are beginning to catch up tothe needs of the field.
Staff with 3-5 years experience inworking with children with specialneeds were significantly less confi-dent of their ability to adapt exist-ing curricula and to work withother staff. They also expressed lessconfidence in their ability to ask forand obtain additional support fromthose around them. These findingsreflect the characteristics of staff

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 115
childhood professionals continue toextend themselves beyond theirinitial education and training, andeven beyond the resources avail-able to them in child care programsto meet the needs of all childrenand families in their communities.
The staff who participated in thisstudy were reasonably well edu-cated and quite experienced. About87% had a diploma and/or a de-gree in early childhood educationor a related field. More than halfhad been working in the field ofchild care for over 10 years and hadalso been working with childrenwith special needs for about thesame period of time. Many had at-tended a variety of conferences andworkshops on inclusion.
Given the number of years manyhad been in the field, the bulk ofthis group of early childhood edu-cators and in-house resourceteachers had experienced the tran-sition to inclusive practice withintheir various programs.
As a result, their voices are thatmuch stronger since they bringwith them the knowledge and skillsof many years working through thisprocess. When they provide sug-gestions of what works or cautionabout what is needed, they mustbe listened to carefully. If this groupof experienced and committed staffare feeling stressed, unsupported,and/or unable to put the time andenergy into making inclusion a suc-cessful experience for the childrenin their programs, then individu-als with less experience and lesseducation, and with fewer supportsin their programs would feel muchmore pressure. At the same timetheir commitment to the processand their overwhelming positivebelief that inclusion can work inmost cases demonstrates that this
is a programmatic direction thatbenefits all involved.
As has been discussed previously,attitudes of early childhood profes-sionals form the foundation uponwhich the actual practice of inclu-sion is based. Early childhood pro-fessionals’ positive attitudes arevital for quality, inclusive programsto develop and be sustained. Al-most all staff in this study held verypositive attitudes toward the inclu-sion of children with a wide rangeof disabilities into their programs.Regardless of whether they wereECEs or resource teachers, theseprofessionals were very positiveabout their ability to meet theneeds of the children included.
What is also affirming is that con-trary to the research, these earlychildhood professionals were aspositive about including childrenwith severe and complex conditionsas they were of children with lesserchallenges. In addition, childrenwith behavioural issues were alsoaccepted as having a right to at-tend quality programs, as long asthere is adequate staff support.Indeed, the caveat that, withoutadequate support, inclusion can-not be successful was repeated overand over.
Where reluctance or uncertaintyabout including children with se-vere disabilities or health condi-tions was voiced, it was primarilyout of concern for meeting thechild’s needs and/or staff’s capac-ity to meet those needs if additionalsupports are not available. Theseprofessionals did not view the dis-abilities or conditions of the childas the primary issue for decidingwhether a child should be included.Rather, they saw the absence ofappropriate resources andsupports as the critical potential

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada116
also very important, enabling all towork together as an effective team.Limited access to resource teach-ers and consultants, and limitedcentre resources (such as sufficienttime for planning and meeting withtherapists or consultants) werefrustrating and problematic, espe-cially given the significant chal-lenges involved when children areunable to communicate or are dif-ficult to engage and/or havebehaviours that are challengingand difficult for staff to deal with.
ECEs who feel that the quality ofthe program they can provide toother children is compromised byinclusion and who feel that re-sources are inadequate to meetchildren’s needs may retreat fromtheir strong support for inclusionin principle, and question the rangeof children who can be includedunder the circumstances. This is-sue of engaging in a “disability cal-culus” — trying to estimate whichchildren can be accommodated,when, and under what circum-stances, is a difficult one that isalso noted in the responses pro-vided by directors in the next chap-ter. Staff were very clear in indi-cating that the two most frustrat-ing factors they experienced wheninclusion was not successful weredifficulty working with parents, andinability to meet the child’s needs.In both cases, insufficient re-sources were exacerbating factors.
Despite the frustration staff expe-rienced when situations were prob-lematic, and the fact that someclearly lack the resources theyneed, most ECEs and in-house RTsin this study said that their expe-riences had helped them becomemore comfortable working withchildren with special needs, morecommitted to inclusion, and moreaccepting of a broader range of chil-
barrier to inclusion. Resources —whether physical (walkers, accessramps), personnel (in-house re-source teachers, an additional staffperson, access to external consult-ants and specialists such as OT/PTs), or training (pre- and in-ser-vice workshops) were seen as thedetermining factors affecting thelikely success of inclusion.
Resources were also critical deter-minants of successful experiences.It was heartening to learn that al-most 80% of child care staff de-scribed themselves as having hada very successful experience withinclusion in the two years preced-ing our study, and that success hadbeen attained in situations thatinvolved children with moderateand severe conditions, as well asthose who may have been easier towork with in a group.
Front-line staff described them-selves as particularly successful insocialization experiences, and inpromoting communication andmotor/self-help skills. Importantly,many staff saw the experience as apositive one for themselves as well,teaching them a great deal andhelping them be more comfortablein their work with children withspecial needs, as well as more con-fident of their abilities in thisregard.
Two thirds of staff indicated thatthe resources that were most im-portant, indeed critical, for suc-cessful inclusion were access to in-house resource teachers or supportworkers, external resource consult-ants, and professionals in theircommunity — the latter, especiallywhen children had more severe orcomplex conditions. Training orworkshops that meet staff’s needs,and empathy and support fromother staff and from parents, were

CHAPTER 7 INCLUSION AS EXPERIENCED BY CHILD CARE STAFF 117
dren being included. Within thissample, experience was the mostimportant factor affecting staff’s at-titudes. Positive experiences with in-clusion go a long way to help staffdevelop the knowledge and skillsthey need to cope with diverse situ-ations. Given the trend for programsto accept children with more com-plex conditions, this is very impor-tant, but we emphasize that positiveattitudes can also be eroded or di-minished if inadequate resourcesfrustrate staff’s efforts and lead tofailures with inclusion due to a lackof commensurate support (time, ad-ditional staff and specialist sup-port, assistance in working in part-nership with parents, and opportu-nities for continual staff renewal).
Front-line staff indicated that theyare receptive to additional train-ing and information to supporttheir efforts, with many wantingtraining on how to work with andsupport parents of children withspecial needs, and how to promotesocial interactions between chil-dren in their program. Our analy-ses suggest that additional learn-ing opportunities can be, andshould be, tailored to meet theneeds of early childhood educatorsand resource teachers at differentstages in their professional ca-reers. We hasten to add, however,that while such trainers might as-sume pro-inclusive attitudes atthis point in time, these attitudesshould not be taken for granted.
END NOTES
1 Wein, C.A. (1995). Developmentally appropriate practice in “Real life.” New York: TeachersCollege Press.
2 Doherty, G., Lero, D.S., Goelman, H., LaGrange, A. & Tougas, J. (2000). You Bet I Care! ACanada-wide study on wages, working conditions and practices in child care centres. Guelph:University of Guelph (Centre for Families, Work and Well-Being).
3 Bricker, D.D. (1995). The challenges of inclusion. Journal of Early Intervention, 19(3), 179-194.
4 Eiserman, W.D., Shisler, L., Healey, S. (1995). A community assessment of preschool provid-ers’ attitudes toward inclusion. Journal of Early Intervention, 19(2), 149-167.
5 Garvar-Pinhas, A. & Schmelkin, L.P. (1989). Administrators’ and teachers’ attitudes towardmainstreaming. Remedial and Special Education, 10(4), 38-43.
6 Denholm, C.J. (1990). Attitudes of British Columbia directors of early childhood educationcentres towards the integration of handicapped children. British Columbia Journal of SpecialEducation, 14(1), 13-26.
7 Eiserman, W.D., Shisler, L., Healey, S. (1995).
8 Stoiber, K.A., Gettinger, M. & Goetz, D. (1998). Exploring factors influencing parents’ andearly childhood practitioners’ beliefs about inclusion. Early Childhood Research Quarterly, 13(1),107-124.
9 Eiserman, W.D., Shisler, L., Healy, S. (1995).
10 Dinnebeil, L.S., McInerney, W., Fox, C. & Juchartz-Pendry, K. (1998). Analysis of theperceptions and characteristics of childcare personnel regarding inclusion of young childrenwith special needs in community-based programs. Topics in Early Childhood Special Education,18(2), 118-128.
11 Peck, C.A. (1993). Ecological perspectives on implementation of integrated early childhoodprograms. In C.A. Peck, S.L. Odom, & D.D. Bricker, (eds.), Integrating young children withdisabilities into community programs: Ecological perspectives on research and implementation,3-15. Baltimore: Paul H. Brookes.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada118
12 Hanline, M.F. (1990). A consulting model for providing integration opportunities for pre-school children with disabilities. Journal of Early Intervention, 14(4), 360-366.
13 Buysse, V., Wesley, P.W. & Keyes, L. (1998). Implementing early childhood inclusion: Barrierand support factors. Early Childhood Research Quarterly, 13(1), 169-184.
14 Stoiber, K.A., Gettinger, M. & Goetz, D. (1998).
15 Kontos, S. & File, N. (1993). Staff development in support of integration. In C.A. Peck, S.L.Odom & D.D. Bricker (eds.), Integrating young children with disabilities into community pro-grams: Ecological perspectives on research and implementation, 169-186. Baltimore: Paul H.Brookes.
16 Katz, L.G. (1995). The developmental stages of teachers. In L.G. Katz, Talks with teachers ofyoung children, 203-210. Norwood, NJ: Ablex Publishing Corporation.

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 119
INCLUSION AS
EXPERIENCED BY CENTRE DIRECTORS
8.8.1 INTRODUCTION
Although centre directors have notbeen the subject of extensive re-search in the field of early child-hood education and child care, anumber of major works have iden-tified the critical importance of thedirector’s knowledge, administra-tive talents, human resource skills,personality, and communicationabilities for overall program qual-ity. Research confirms that chil-dren in centres with more experi-enced and better educated direc-tors tend to experience higher lev-els of quality care and perform bet-ter on measures of language andsociability with peers.1
A director’s administrative capabili-ties, experience, and sensitivity af-fect staff as well, influencing boththe extent to which staff are ableto be positive and supportive withthe children in their care, andstaff’s skills in providing develop-mentally appropriate program-ming. Staff’s job satisfaction, per-ceived level of supervisory support,and the quality of co-worker rela-tionships are also affected, all ofwhich have been correlated withboth the quality of care staff pro-vide and with staff’s experiences oftheir work environment. Americanresearchers such as Jorde-Bloom
(1992)2 and Helburn (1995)3 havealso found a relationship betweendirectors’ skills and effectiveness insupporting staff with levels of re-ported job stress and burnout, aswell as with actual staff turnoverrates.
In many ways, the centre directorstands at the interface or nexus ofecological influences:
✦ transforming and mediatingprovincial and municipalpolicies;
✦ negotiating the simultaneousand sometimes competingneeds of children, families, andstaff;
✦ representing the centre and itsrole in the community;
✦ articulating and promotingstandards and practices thatare critical to the provision ofhigh quality care and tochildren’s and families’ well-being; and
✦ marshalling resources for thecentre to maintain and improvequality over time.
Clearly, the role of a centre direc-tor is both complex and challeng-ing. Administrative decisions mustreflect the goals of the centre as awhole, the needs and interests of
Donna S. Lero, Kathleen Brophy, Sharon Hope Irwin

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada120
the children and parents, and theconcerns and capabilities of thestaff — often in the context of con-tinued underfunding. Directors areleaders and models for their staffand set the expectations and val-ues that characterize a centre’sethos or identity.
As described in Chapters 2 and 3of this report, directors’ (and front-line staff’s) attitudes, experience,and capabilities are particularlycrucial for the effective inclusion ofchildren with special needs in Ca-nadian child care programs. In theabsence of legislative mandates, di-rectors’ attitudes, ongoing commit-ment, and capacities to work effec-tively — both with centre staff andwith professionals in the commu-nity — are likely to be among thestrongest determinants of the qual-ity of inclusion for all concerned.
For these reasons, we thought itwas especially important to exam-ine and understand directors’ per-spectives on inclusion. In particu-lar, in this chapter we focus on di-rectors’ attitudes and beliefs aboutinclusion and some of the factorsthat may affect directors’ commit-ment, as well as their concernsabout their centre’s capabilities inthis regard. We also examine someof the challenges directors havefaced or are facing in the contextof continued fiscal restraint forfunding child care services, andobtain directors’ views about whathave been the most importantenablers and frustrators to effec-tive inclusion in their programs.Throughout this chapter, we haveoccasion to reflect on changes overtime that may have occurred in di-rectors’ attitudes and experiences,and in their centre’s capacities toeffectively include children withspecial needs. Taken together, thepreceding chapter on front-line
child care professionals’ experi-ences with inclusion and this chap-ter provide a rich understanding ofthe ecology of inclusion as experi-enced within child care programs.
8.2 DIRECTORS’ EDUCATION ANDEXPERIENCE: A FOUNDATIONFOR EFFECTIVE INCLUSION
In Chapter 5 we noted that almost92% of the 136 centre directors inthis sample had completed a post-secondary credential in EarlyChildhood Education or a relatedsubject: 55.0% had completed acollege diploma program, 31.3%completed a Bachelor’s degree, and6.1% had attained a graduate de-gree. Approximately half of the di-rectors had also obtained a post-diploma certificate related to ECE,inclusion, or child care administra-tion. Relative to the national pro-file of directors in the YBIC! study,this sample of directors is quitewell-educated.
Similarly, we noted that thissample of directors has consider-able experience. Almost 85% of thedirectors had been in the child carefield for ten years or longer, includ-ing 56% who had more than 15years experience. Moreover, 64.3%of the directors in this sample hadmore than ten years of experiencein work with children with specialneeds.
This wealth of education and ex-perience provides a strong founda-tion for directors to draw on whenmaking complex decisions. In ad-dition to serving as a resource toguide her/his own decisions, adirector’s education and experienceare likely to help her better appre-ciate the needs of her staff, and theissues that must be considered infacilitating and maintaining effec-tive collaborative relationships with

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 121
parents and other community pro-fessionals. Moreover, education,experience, and a commitment tomaking inclusion work are all likelyto motivate directors to seek outnew information and to capitalizeon the resources that might im-prove inclusive practice.
8.21 Continued Learning: Coursesand Conferences
Two questions were posed to direc-tors to determine if they had beenengaged in efforts to expand theirknowledge about inclusion. In re-sponse, 34% of directors repliedthat they had taken at least oneuniversity or college level courserelated to the inclusion of childrenwith special needs since 1990 (ayear which likely fell considerablylater than most directors’ initialpost-secondary diploma/degreecompletion, given the directors’ agedistribution and length of time inboth the child care field and in theirpresent position). Furthermore,75.7% of directors had attendedworkshops or conference presen-tations on children with specialneeds since 1990, with most hav-ing been to several different con-ferences or workshops between1990 and 1996. (Almost 26% of thetotal sample had actually been toa conference or workshop offeredby SpeciaLink: The National Cen-tre for Child Care Inclusion.)
8.22 Providing Workshops to Others
A related question asked directorswhether they had provided anyworkshops or in-service training toothers on topics related to childrenwith special needs since 1990. In-deed, 69 directors in our sample(51.1%) had done so. In all likeli-hood, most of these directors had
been directly involved in providingin-service development for theirown staff, either personally or byarranging to have someone withmore expertise do so. But there arealso examples of directors in thissample who have given workshopsand conference presentations oninclusion to other child care pro-fessionals in their local area, andeven at provincial or national meet-ings of child care professionals. Inthis way, they provide substantialleadership to their staff and toothers.
Directors in specialized and desig-nated programs were more likely tohave university degrees and morespecialized educational back-grounds, and longer experienceworking with children with specialneeds. They were also moreinvolved in both attending confer-ences and providing in-servicetraining and workshops than weredirectors in “regular” child careprograms.
8.23 Directors’ Interests in AdditionalTraining and Information
In our experience, the uniquelearning needs of centre directorsare often not considered as such.We asked directors in this uniquesample what areas of additionalinformation or training would beuseful to them. The results, shownin Table 8.1, indicate the breadthof areas about which directorswould like more information.
8.3 DIRECTORS’ INVOLVEMENT INPROGRAM PLANNING,COMMUNICATING WITHPARENTS, ANDCOORDINATING RESOURCES
Information presented in Chapter5 also indicated that directors of-

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada122
“Co-ordinationvaries, dependingon the number ofagencies involved.Group meetingscan be very diffi-cult to organize.”(director of a centrein Manitoba)
Directors’ Self-Identified Learning Needs
Table 8.1
tion are problematic. In such cases,considerable personal commitmentand perseverance may be required.
As a director of a Manitoba childcare centre explained:
“Most of the special needs chil-dren we’ve enrolled in the past3-4 years were not identified assuch at enrollment. While manyhad social workers, few of themtook the leadership role to man-age cases, do referrals, etc. Thiswork fell to the day care (i.e.,me) as did providing the ‘extrapair’ of hands often needed onthe floor. This takes up a LOTof time and is work that is notrecognized as a role played bythe day care...Those childrenwho are referred by agenciesprior to enrollment may spendmany months waiting for ser-vice if the child requires staffsupport and subsidy fees. Bothhave to be available at the sametime and rarely are....The childday care office may fund fewerhours per day than the child at-tends — expecting the centre tomake up the difference... It’shard to find a trained ECE will-ing to work part-time.”
Technical Assistance or InformationMaintaining and promoting quality care in a period of diminishing resources 72.1%How to help staff be effective in their work with children who have special needs 65.4%How to help parents make informed choices and decisions about their child’s care 41.9%Promoting social interactions between children with special needs and other children 40.4%Staff evaluation and feedback to those working with children who have special needs 38.2%Specific, in-depth information about particular disabilities 31.6%How other centres mainstream effectively 29.4%How to work collaboratively with agencies and specialists 28.7%Advocating on behalf of children and families with special needs 22.1%
Other 3.7%
Topic Areas on Which Directors Would Like Additional Training, Percent
ten had a personal role in programplanning, communicating with par-ents, and coordinating resources tosupport inclusion. Directors in thissample were less often involved inindividual program planning for thechildren (18%); they were morelikely to be involved in communi-cating with parents (69%) and co-ordinating services for the childrenwith special needs enrolled in theircentre (64%). The latter responsi-bility typically involves contactswith other agencies and profession-als, and sometimes with local rep-resentatives of various provincialministries.
Communicating with parents, co-ordinating services, and overseeingand supporting centre staff in theirefforts all can take considerabletime and energy on the director’spart, again reinforcing the impor-tance of her/his commitment toinclusion. Many directors are will-ing to do this and see it as an im-portant component of their role.Other directors may have more dif-ficulty, especially when communityand centre resources are limitedand coordination and communica-

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 123
8.4 DIRECTORS’ ATTITUDES ANDBELIEFS ABOUT INCLUSION
A major part of this study was fo-cussed on directors’ and child carestaff’s attitudes and beliefs aboutinclusion. This was a critical focusof our investigation both becauseprevious literature has identifiedattitudes as a major barrier to (sus-tained) inclusion, and because wewere interested in exploringwhether child care professionals’attitudes, beliefs, and personal per-spectives on inclusion had changedsince the earlier study undertakenby SpeciaLink in 1989-90. Atti-tudes and beliefs are generallyhighly related to each other, butmeasuring both can provide aricher understanding of a person’sviews and identify where inconsis-tencies, contradictions and pointsof ambivalence may lie.
According to Odom and Diamond(1998)4 attitudes, beliefs, and ide-ologies related to inclusion cur-rently reflect several different, butrelated, rationales for this practice.A philosophical/ethical rationale ispredicated on the belief that chil-dren with disabilities should beable to participate in the same highquality early childhood programsas typically developing children sothat they can become members ofthe classroom and local communityand develop positive relationshipswith others. Legal/legislative man-dates provide another rationale,based on civil rights, that are de-signed to remove barriers that dis-criminate against children with dis-abilities and preclude them fromparticipating in ways that would bebeneficial for them and enablethem to lead as normal a life aspossible. An educational rationalefor inclusion emphasizes the devel-opmental benefits that are expectedfrom participating in high quality
integrated early childhood pro-grams.
The measures used in the currentstudy appear to tap the first tworationales described above, withsome reflection of the third (edu-cational) rationale as well. The firstattitudinal measure is one origi-nally developed by Sandra Bochnerand Moira Pieterse of MacquaireUniversity and Carey Denholm ofthe University of Victoria.5 Thismeasure asks respondents to in-dicate the extent to which childrenwith a wide range of special needs(30 different conditions) should beenrolled in a regular preschool orchild care program. (See question4.1 in Appendix B.) Based on itsuse in the 1990 survey of child careprofessionals by SpeciaLink (Irwin& DeRoche, 1990),6 we clarified theintroduction to the question byindicating that in referring to a“regular preschool or child careprogram,” we meant an “average,community-based program (not es-pecially designated as an integratedprogram) with the resources avail-able to most centres in your prov-ince or territory.” Nonetheless, inthis study, as in 1990, respondentsfrequently stated that their answer(typically agreement) was condi-tional upon the assumption thatappropriate resources wouldbe made available to supportinclusion.
Both the pattern of responses ob-tained and, in particular, writtencomments and elaborations pro-vided by both centre directors andfront-line ECEs and in-house re-source teachers indicate that thismeasure reflects a philosophical/ethical rationale for inclusion, aswell as the belief that early child-hood programs should beresourced so that they can inte-grate children with a wide range of

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada124
disabilities and conditions.
The second measure presentedparticipants with seven statementsin the form of beliefs about inclu-sion that were developed specifi-cally for this study. Statementswere developed by extracting keythemes from the literature on in-clusion and putting them intosimple statements that we thoughtmight elicit some differential re-sponses. (See question 4.2 inAppendix B.)
8.41 Directors’ Current AttitudesTowards Including Children withSpecial Needs in RegularPreschool and Child CarePrograms
Directors’ responses to this scalewere generally very positive, andremarkably similar to those givenby ECEs and in-house resourceteachers, as described in Chapter7. The average score across allitems, originally coded on a scaleof 1 (strongly disagree with inclu-sion) to 5 (strongly agree) was 4.17,with a standard deviation of 0.605.Scores ranged from 1.3 to 5.00,with only 37% of average scoresfalling below 4.00. Over ninetypercent of directors or more agreedor strongly agreed that childrenwith the following conditions/char-acteristics should be enrolled in aregular preschool or child care pro-gram (with appropriate supports):
✦ a child who is hyperactive,
✦ a child who is deficient in self-help skills (dressing, feeding,etc.),
✦ a child with mild mobility diffi-culties (e.g., needs crutches,wears calipers),
✦ a child with moderate mobility
difficulties (e.g., needs wheel-chair) if the program is reason-ably accessible,
✦ a child who requires specializedand/or adapted instructionalmaterials to progress in pre-academic skills (e.g., tactilepuzzles, special scissors),
✦ a child who has impaired lan-guage skills,
✦ a child who is noticeably with-drawn,
✦ a child who is mildly intellectu-ally disabled (IQ 55-75/80),
✦ a child with a mild visualimpairment which cannot becorrected fully by wearingeyeglasses or contact lenses,
✦ a child with moderate visualimpairment (needs specialequipment or services), and
✦ a child with a moderate hearingloss (who needs special equip-ment or services).
Across the 30 disabling conditionsor circumstances, there were onlyseven that less than 75% of direc-tors agreed could be accommo-dated in regular early childhoodprograms. In all seven of these in-stances, directors were more likelyto say they were uncertain aboutincluding children with these con-ditions in a regular child care pro-gram, rather than disagreeing.Both the child’s condition and theextent to which additional assis-tance would be available/unavail-able were often the deciding factors.
In general, however, the directors’responses indicate strong accep-tance of the view that children witha wide range of conditions shouldbe able to attend a local child careprogram if supports are provided.
“I feel that everychild should beincluded in childcare programsand no childshould be ex-cluded becausehe/she has specialneeds, just aslong as the childhas the appropri-ate equipment, orresource staffavailable.”(director of a regular childcare program in Newfound-land)
“With the rightapproach, staff,and resources, Ifeel no doorshould be closedto any child.”(director of a designatedprogram in PEI)

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 125
8.42 Differing Perspectives AmongDirectors
While there was much similarity onmany of the items, readers shouldbe aware that there were differentperspectives among the directors inour sample. In particular, directorsof specialized/segregated programswere the most reserved, comparedto directors of regular and desig-nated programs. Directors in spe-cialized programs had an overallaverage score of 3.74 compared to4.02 for directors in regular pro-grams and 4.37 for directors indesignated integrated programs.While there was overlap across thegroups, directors in specialized pro-grams were more likely to voiceconcerns about the extent to whichchildren’s needs could be met inregular child care programs andwere most likely to comment thatplacement should reflect children’sneeds and parents’ wishes. Direc-tors of regular programs appeared
to be more dubious about whetheradequate supports would be inplace, expressing concern aboutthe staff’s and centre’s capacitiesto cope with more than the de-manding challenges they were al-ready facing. These same concernsreappeared in spontaneous com-ments at several points in the sur-vey questionnaire. (See next page.)
8.43 Have Directors’ AttitudesChanged?
There are two ways to address thisquestion. One is by comparing ourfindings with those obtained fromearlier studies that used the samemeasure and to see if there areobservable differences in averagescores or scores on specific itemsthat might indicate a change in at-titudes. The other is to ask direc-tors if their views have changedover time, and in what way. In thissection we compare our 1996 data
Directors were more reserved about including children in thefollowing seven circumstances:Characteristic or condition Percent who agreed
or strongly agreed
A child with moderate mobility difficulties (e.g., needs wheelchair) when access is unsuitable 41.0%
A child who is, at times, uncontrollably aggressive 53.8%
A child who has a phobic resistance to school attendance 60.0%
A child who requires assistance with an artificial bowel or bladder if parents are not willing or unable to assist 42.1%
A child who requires catheterization if parents are not willing or are unable to assist 39.7%
A child who often cannot recognize situations involving danger to himself/herself 69.9%
A child who has a multi-disabling condition, e.g., physical and intellectual disabilities 71.2%
Table 8.2

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada126
with results obtained in 1989 and1990 studies. A later section of thischapter addresses directors’ re-ported change in their commitmentto inclusion and their comfort levelin working with children with spe-cial needs.
Results from two earlier studiesthat used substantially the sameinstrument to assess attitudes to-wards inclusion were examined.These studies were Denholm’s1989 study of directors in BritishColumbia and the study conductedby SpeciaLink in 1990, from whichresponses of 143 directors could beextracted from their larger, mixedsample of child care professionals.Comparing findings across studiesthat use different samples withsome variation in the introductionto the scale provides an imperfect,but still useful, point of compari-son. In order to enable direct com-parisons, we recoded our scoringprocedure to be the same as thatused in the earlier studies — i.e.,strongly agree was recoded to a 1,so that the lower the score, themore accepting directors were re-garding inclusion.
Comparisons between the twoSpeciaLink samples revealed mini-mal change in attitudes between1990 and 1996-97. In both stud-ies average responses to only sixitems — indeed, the same six items— were higher than 2.0, with nonehigher than 2.8 on a 5-point scale.It is important to remind readersthat in both instances respondingdirectors were a selected group.These directors were in programsalready providing care and educa-tion to children with special needs(or were likely to do so), and likelywere more committed and accept-ing of inclusion than directors withlittle or no history of including chil-dren with special needs in their
centres. At least for this populationof centre directors, positive atti-tudes towards inclusion appear tohave remained consistently highover the 6-7 year period betweenthe two studies.
An interesting point to note is thatin 1990 Irwin and DeRoche’s analy-sis indicated that items in this scaleloaded on nine separate factors,based on commonality of conditionand/or degree of accommodativeeffort that might be required. In our1996 data, only one common fac-tor was identifiable, to which direc-tors displayed more or less sympa-thy. This difference implies that thebasis for supporting inclusion as ageneral approach and as a principleof practice may have solidified, withacceptance depending less on theparticulars of children’s conditionsand more on a philosophical basethat favours inclusion, tempered bythe availability of supportive re-sources, especially in situationsthat would demand more in theway of skills, time and specializedeffort on the part of centre staff.
Table 8.3 provides average itemscores for the two SpeciaLinksamples and Denholm’s sample ofB.C. directors. The comparisons re-veal that the two SpeciaLinksamples were both slightly morefavourable to including childrenwith special needs than Denholm’s1989 sample of B.C. directors. It isinteresting to note, however, thatthe relative ordering of items wassimilar across all three samples onmost items.
8.44 Directors’ Beliefs AboutInclusion
The seven belief statements usedin this study also required direc-tors to indicate their level of agree-ment on a 5-point scale, where 5
“I could onlyagree to a childgoing into a regu-lar program if it’sthe parents’ wishand if supportsare available. Itisn’t in the child’sbest interest to beput into a regularclassroom inorder to fill ‘in-clusion’ criteria.”(director of a specializedprogram in B.C.)
“Most of the abovesituations wouldrequire some formof additionalsupport. If itwasn’t availableand the child waspart of our regu-lar 1:8 ratio, Iwould disagree tomost of the situa-tions.”(director of a regular programin Québec)

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 127
Disability or Special Need Current SpeciaLink Denholm1996-97 1990 1989 (BC)
Mild mobility difficulties 1.5 1.0 1.7Requires specialized or adapted instructional 1.4 1.0 1.7 material to progress in pre-academic skillsImpaired language skills (not ESL) 1.4 1.1 1.5Moderate mobility difficulties — program is 1.5 1.1 1.7 reasonably accessibleMild visual impairment which cannot be corrected 1.6 1.1 1.7 by wearing spectacles, contact lensesMildly intellectually disabled (IQ 55-75/80) 1.5 1.1 1.7Moderate hearing loss (needs special equipment 1.6 1.1 1.8 and/or services)Requires assistance with artificial bowel 1.7 1.1 1.7 or bladder with parents willing to assistDeficient in self-help skills 1.5 1.1 2.0Requires catheterization; parents are willing 1.8 1.1 2.0 to assistIs noticeably withdrawn 1.5 1.2 1.6Moderate visual impairment (needs special 1.7 1.3 1.7 equipment and/or services)Eneuretic (inadequate bladder control) 1.7 1.4 2.4Moderately intellectually disabled (IQ 30 - 55) 1.7 1.5 2.1Displays inappropriate social behaviour 1.9 1.5 2.2Is Deaf 1.8 1.5 —-Incontinent (inadequate bowel control) 1.7 1.5 2.6Requires medical monitoring by program staff 1.9 1.6 2.1Hyperactive 1.7 1.6 2.1Uncontrollable, but not aggressive —- 1.6 2.2Has tested HIV positive 1.8 1.7 —-Has AIDS 1.9 1.7 —-Is blind 1.9 1.7 —-Requires intensive individualized instruction —- 1.8 2.3 to progress in academic skillsA multi-disabling condition 2.0 2.0 2.7Can’t recognize situations involving danger 2.1 2.1 2.6 to him/herselfHas a phobic resistance to school 2.2 2.2 2.3Requires catheterization; parents not willing 2.6 2.2 3.2 or able to assistRequires assistance with artificial bowel or bladder 2.6 2.3 3.2 with parents not willing or able to assistUncontrollably aggressive at times 2.4 2.4 2.7Moderate mobility difficulties; access is unsuitable 2.8 2.7 3.3
Note: Items were scored from 1 to 5; Strongly Agree = 1, Uncertain = 3, Strongly Disagree = 5. Average item scores have beenrounded to the nearest tenth. All three samples are of directors of child care programs. Both SpeciaLink samples includedirectors from across Canada, selected as providing or likely providing care for children with special needs. The Denholm samplewas limited to directors of child care programs in British Columbia. There were variations in instructions to respondents and insamples that may have affected responses.
A Comparison of Average Item Scores on Attitudes Towards Inclusion of Childrenwith Special Needs in Regular Programs Across Three Studies
Table 8.3

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada128
indicated strong agreement. Theitems were developed to probe di-rectors’ views about inclusion inprinciple (statements 1 and 2); theirbeliefs about the impacts of inclu-sion on staff and other children(items 3 and 4); directors’ views asto whether the field (in the form ofmost child care programs/mostdirectors) is generally receptive toinclusion (statement 5); and astatement that asked directorswhether inclusion efforts should bemore concentrated, given limitedallocations of resources (item 6). Anadditional statement assessed di-rectors’ views of early childhoodeducators’ background preparation— given the need for a wider set ofskills and knowledge among staffin inclusive programs. Table 8.4summarizes directors’ responses.
A strong majority of directors (87%)agreed that legislation should bepassed in Canada to ensure thatdisabled children and their parents
have full access to child care pro-grams. Support for a legal mandatefor inclusion would be aligned withother efforts to ensure equality forpeople with disabilities in otherareas (education and employment)in keeping with Canada’s Charterof Rights and Freedoms, and inparallel to US legislation (the IDEAAct) that has supported progresstowards inclusion in that country.Furthermore, such legislation, ifpassed, would require adequatefunding and programmatic sup-ports to comply with the legislativeintent. Even without such legisla-tion, 61% of directors agreed orstrongly agreed that day care pro-grams should accept all children,regardless of their individual needs.Disagreement and reservationsabout this statement again fo-cussed on centres’ capacities andlimited resources.
Responses to item 3 indicate amore mixed perspective on how
Directors’ Beliefs about Inclusion
Table 8.4
Opinion and Belief Statements Directors’ Responses(%)
Mean Item Strongly Agree Uncertain Disagree StronglyScore Agree Disagree
1. Child care programs should accept all children, 3.7 30.5 30.5 15.3 21.4 2.2 regardless of their individual needs.
2. Legislation should be passed to ensure disabled 4.3 45.0 42.0 7.6 4.6 0.8 children and their parents have full access to child care programs.
3. Having children with special needs in most child 3.3 15.2 37.9 13.6 28.0 5.3 care centres puts too much pressure on the staff.
4. Having children with special needs in child care 4.5 57.0 37.8 4.4 0.7 0.0 benefits the non-disabled children.
5. Most child care programs would be willing to 4.4 59.3 29.6 5.9 5.2 0.0 include children with special needs, if adequate resources were available.
6. It would be better to have some child care programs 2.9 7.6 34.1 18.2 23.5 16.7 accept children with special needs (with special- ized resources) than try to have all child care pro- grams be inclusive.
7. Training for early childhood educators has provided 2.9 10.4 26.7 14.8 40.7 7.4 them with a good background to support inclusion.

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 129
inclusion affects centre staff. Onethird of directors disagreed thatinclusion puts too much pressureon centre staff, but 53% admittedsome concerns in this regard. Theresponse to item 4 was uniformagreement. It was widely acceptedamong members in this samplethat inclusion benefits non-dis-abled children. Most directors alsoagreed with item 5, indicating thatthey see the child care field as hav-ing accepted inclusion as an appro-priate or normal practice, if ad-equate resources are in place. [Itwould be interesting to know if thesame level of agreement couldbe found among a more represen-tative, unselected sample ofdirectors.]
Item 6 reflects an ongoing, prag-matic and ethical dilemma. Despitewidespread agreement with inclu-sion as appropriate practice in earlychildhood programs, is it better toconcentrate limited resources tosupport effective inclusion in fewerprograms than to ask all programsto be inclusive without adequateresources? Under these con-straints, 41.7% of directors agreedor strongly agreed that resourcesshould be targeted to a smallernumber of child care programs;almost the same percentage dis-agreed with this conclusion, and18.2% remained uncertain. Theanswers to this question indicatewhere one of the major fault linesis in child care professionals’ com-mitment to inclusion. Concernsreflect both what would be betterfor centres and also what is in thebest interests of individual chil-dren, particularly those with spe-cial needs, if resources areconstrained.
The last statement in this seriesasked about perceptions of earlychildhood educators’ background
preparation — an important point,since the education and skills ofstaff are central to the success ofinclusion efforts. Among thissample, 47% of directors believethat ECEs’ training has not ad-equately prepared them for inclu-sion, while 37% expressed a morepositive view. Clearly, there is roomfor improvement.
As was the case with the attitudesitems, directors were not homoge-neous in their responses to thesebelief statements. Statistical analy-sis revealed significant differencesamong directors in response to be-lief statements 1, 2, 3 and 6. Di-rectors of integrated programs an-swered in a way that was signifi-cantly more supportive of inclusionas an ideal, a legal right, and a chal-lenge staff could meet. Interest-ingly, they were also more likely toagree with item 6 on the basis oftheir concern that children’s needsbe met effectively, rather thanpoorly, despite their strong supportfor inclusion as an ideal practicein all child care programs.
8.5 PERSONAL CHANGE INDIRECTORS’ VALUES ANDFEELINGS
In addition to the more structuredassessments of child care profes-sionals’ current attitudes towardsincluding children with variousconditions in early childhood pro-grams, and their beliefs about in-clusion, a primary objective of thisstudy was to learn whether staffand directors’ personal views andfeelings about inclusion hadchanged over time and, if so, howand why. We asked both groups toconsider if their experiences overthe last six years had led them tochange their views towards inclu-sion. Specifically, we asked about
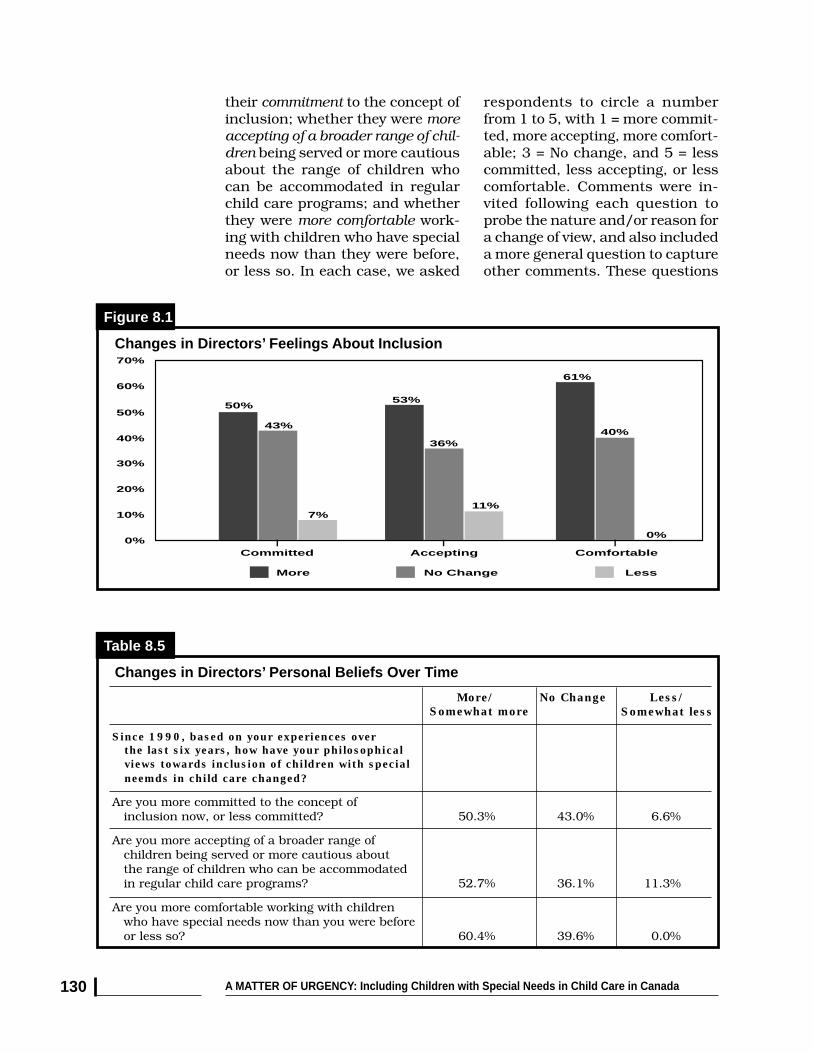
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada130
their commitment to the concept ofinclusion; whether they were moreaccepting of a broader range of chil-dren being served or more cautiousabout the range of children whocan be accommodated in regularchild care programs; and whetherthey were more comfortable work-ing with children who have specialneeds now than they were before,or less so. In each case, we asked
respondents to circle a numberfrom 1 to 5, with 1 = more commit-ted, more accepting, more comfort-able; 3 = No change, and 5 = lesscommitted, less accepting, or lesscomfortable. Comments were in-vited following each question toprobe the nature and/or reason fora change of view, and also includeda more general question to captureother comments. These questions
Changes in Directors’ Personal Beliefs Over Time
Table 8.5
More/ No Change Less/
Since 1990, based on your experiences over
Changes in Directors’ Feelings About Inclusion
Figure 8.1
Committed Accepting Comfortable
More No Change Less
50%
43%
7%
53%
36%
11%
61%
40%
0%
10%
0%
30%
20%
50%
40%
70%
60%
the last six years, how have your philosophical views towards inclusion of children with special neemds in child care changed?
Are you more committed to the concept of inclusion now, or less committed? 50.3% 43.0% 6.6%
Are you more accepting of a broader range of children being served or more cautious about the range of children who can be accommodated in regular child care programs? 52.7% 36.1% 11.3%
Are you more comfortable working with children who have special needs now than you were before or less so? 60.4% 39.6% 0.0%
Somewhat more Somewhat less
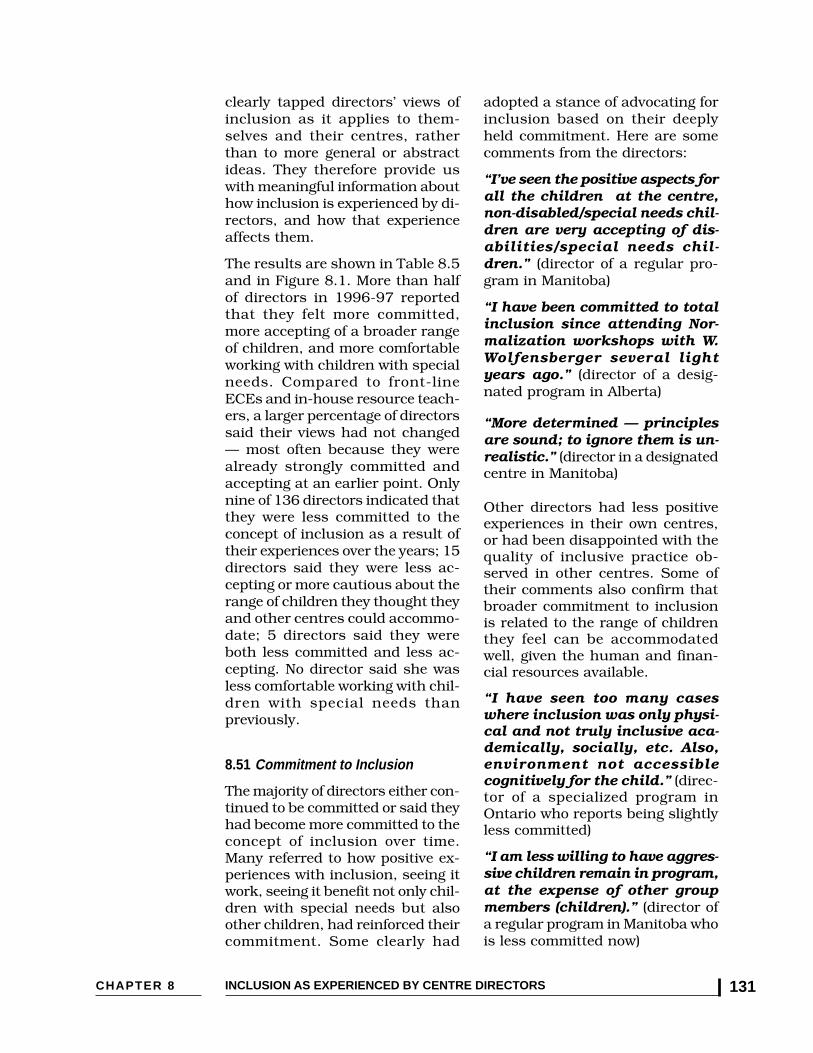
CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 131
clearly tapped directors’ views ofinclusion as it applies to them-selves and their centres, ratherthan to more general or abstractideas. They therefore provide uswith meaningful information abouthow inclusion is experienced by di-rectors, and how that experienceaffects them.
The results are shown in Table 8.5and in Figure 8.1. More than halfof directors in 1996-97 reportedthat they felt more committed,more accepting of a broader rangeof children, and more comfortableworking with children with specialneeds. Compared to front-lineECEs and in-house resource teach-ers, a larger percentage of directorssaid their views had not changed— most often because they werealready strongly committed andaccepting at an earlier point. Onlynine of 136 directors indicated thatthey were less committed to theconcept of inclusion as a result oftheir experiences over the years; 15directors said they were less ac-cepting or more cautious about therange of children they thought theyand other centres could accommo-date; 5 directors said they wereboth less committed and less ac-cepting. No director said she wasless comfortable working with chil-dren with special needs thanpreviously.
8.51 Commitment to Inclusion
The majority of directors either con-tinued to be committed or said theyhad become more committed to theconcept of inclusion over time.Many referred to how positive ex-periences with inclusion, seeing itwork, seeing it benefit not only chil-dren with special needs but alsoother children, had reinforced theircommitment. Some clearly had
adopted a stance of advocating forinclusion based on their deeplyheld commitment. Here are somecomments from the directors:
“I’ve seen the positive aspects forall the children at the centre,non-disabled/special needs chil-dren are very accepting of dis-abilities/special needs chil-dren.” (director of a regular pro-gram in Manitoba)
“I have been committed to totalinclusion since attending Nor-malization workshops with W.Wolfensberger several lightyears ago.” (director of a desig-nated program in Alberta)
“More determined — principlesare sound; to ignore them is un-realistic.” (director in a designatedcentre in Manitoba)
Other directors had less positiveexperiences in their own centres,or had been disappointed with thequality of inclusive practice ob-served in other centres. Some oftheir comments also confirm thatbroader commitment to inclusionis related to the range of childrenthey feel can be accommodatedwell, given the human and finan-cial resources available.
“I have seen too many caseswhere inclusion was only physi-cal and not truly inclusive aca-demically, socially, etc. Also,environment not accessiblecognitively for the child.” (direc-tor of a specialized program inOntario who reports being slightlyless committed)
“I am less willing to have aggres-sive children remain in program,at the expense of other groupmembers (children).” (director ofa regular program in Manitoba whois less committed now)

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada132
“...due to lack of supports andfunding.... Staff and myself arefrustrated with the present sys-tem.” (director of a designated pro-gram in Ontario explaining why shefeels both less committed and lessaccepting of a broad range of chil-dren in her centre)
“I would be more committed ifthe licensing regulations wereless ambiguous and much morerealistic and supportive.” (direc-tor of a regular program in NewBrunswick who is less committed,but more accepting and started anintegrated program some years ago)
“I have always supported theconcept of inclusion, but thedollars are so scarce now andthe ‘regular’ children so needythat my staff simply can’t copewith a special needs childwithin existing ratios.” (directorin Manitoba who said there hadbeen no change in her commitmentto inclusion, but that she was lessaccepting/more cautious about abroader range of children beingaccommodated in regular pro-grams)
“....$ budget insufficient!” (direc-tor of a regular centre in Québecwho is less committed and muchless accepting)
8.52 Accepting of a Broader Rangeof Children With Special Needsor More Cautious
As indicated above, some directors’difficult experiences led them to bemore cautious about the range ofchildren they felt they could accom-modate in their centre. Theirchange sometimes accompanied achange in their general commit-ment to inclusion, and sometimesoccurred separately. In these cases,directors seemed to be actively en-
gaged in sorting out what they andtheir staff could realistically do,even though it departs from theirideal of full inclusion.
On the other hand, other directorsdescribed how positive experienceswith children with special needshad enabled them to feel more com-fortable and develop new skills;hence, they were willing to take onnew challenges.
“As each new challenge is met,the ‘range’ grows automaticallyto include this ‘group’ — alwaysrealizing anew that the vision ofinclusion is not as narrow asothers would have usbelieve....Until the first time achild seizured in my arms, sei-zures frightened me — this is apretty commonplace reaction tothe feeling of not ‘being able’yourself.” (director of a designatedprogram in Manitoba, more accept-ing)
“Having too many children in aclassroom with global delays istoo taxing on the resourceteacher and staff, and less ben-eficial for the individual child.”(director of a designated programin Ontario, less accepting)
“Our government is looking atrelaxing regulation which mayinclude training and group sizechanges...how could I even con-sider integrating high needschildren! One ECE can’t dividethemselves into so many piecesand still provide some degree ofquality.” (director of a regular pro-gram in Manitoba, less accepting)
“I am cautious in terms of accom-modating children whose needscan not be met by the resourcesavailable.” (director of a regularprogram in B.C., no change)

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 133
“We have never turned away anychild without giving it an hon-est try. Tend to be cautiousthough, for children withbehavioural aggressive tenden-cies.... Lack of RT time is an is-sue in what we can manage.” (di-rector of a designated program inOntario)
8.53 More Comfortable With ChildrenWith Special Needs
As noted earlier, no director saidshe was less comfortable in herwork with children with specialneeds; about 40% of directors re-ported no change. Of the remain-der, 38% said they were much morecomfortable (a score of 5), and 22%said they were more comfortable(reply of 4 on a 5 point scale).Clearly, it was personal experiencethat made the difference — both fordirectors and for staff. Some of thedirectors’ comments are reflectedin the quotes already noted. Oth-ers said:
“The more experience I’ve had,the more comfortable I am.”(director of a regular program inManitoba)
“One of our children was moreprofoundly disabled thanwe had expected — turned outto be a wonderful learningand caring experience for us.”(director of a regular program inSaskatchewan)
“More committed as we’ve hadgreat success... The childrenchallenge your caregiving skillsand as a result, caregiving im-proves. I’m not so overwhelmedwith the disability, but strive ongetting to know the child.”(director of a designated programin Alberta)
These direct quotations were se-lected to give readers a strongersense of the experience of inclusionfrom the directors’ standpoint.Change in one aspect of a director’spersonal views often was correlatedwith change in another aspect.Whether or not a director said shewas more committed to the conceptof inclusion was statistically highlycorrelated with whether she saidshe was more (or less) acceptingand more comfortable (correlationswere .66 and .52, respectively —both significant at a .01 level).
8.6 DIRECTORS’ VIEWS OF THEIRCENTRE’S EFFECTIVENESS ININTEGRATING CHILDREN WITHSPECIAL NEEDS
One of our major goals in this studywas to learn from directors howthey feel their centres have changedover time and what they feel havebeen important enablers of positivechange, as well as factors that haveimpeded their centre’s success inintegrating children with specialneeds. Directors’ replies to this partof the questionnaire provide impor-tant information about the centresand also add to our understandingof inclusion as experienced bydirectors.
In this section, we first report ondirectors’ views as to whether theirprogram had become more inclu-sive or more effective at includingchildren with special needs be-tween 1990 and 1996-97 whendata were collected and provideseveral data points to validate thoseviews. We then examine directors’explanations of what factors en-abled their centre to become moreeffective, as well as what has lim-ited or frustrated their efforts.
Directors were asked this question:
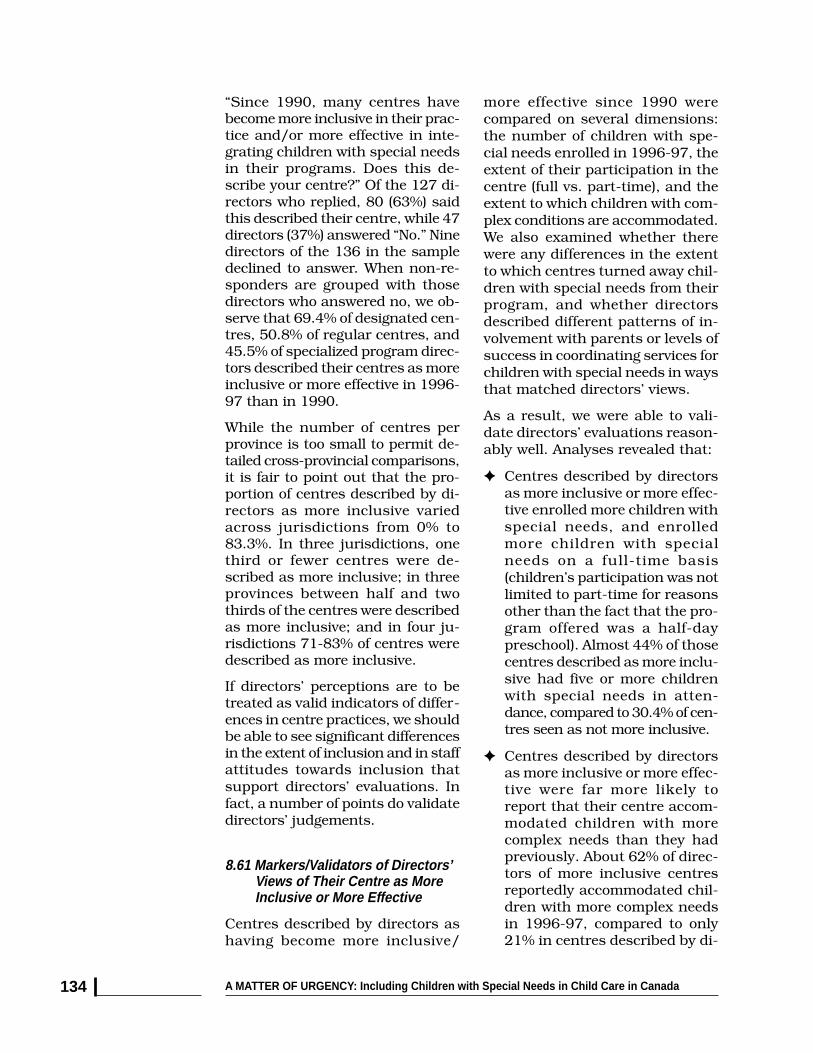
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada134
more effective since 1990 werecompared on several dimensions:the number of children with spe-cial needs enrolled in 1996-97, theextent of their participation in thecentre (full vs. part-time), and theextent to which children with com-plex conditions are accommodated.We also examined whether therewere any differences in the extentto which centres turned away chil-dren with special needs from theirprogram, and whether directorsdescribed different patterns of in-volvement with parents or levels ofsuccess in coordinating services forchildren with special needs in waysthat matched directors’ views.
As a result, we were able to vali-date directors’ evaluations reason-ably well. Analyses revealed that:
✦ Centres described by directorsas more inclusive or more effec-tive enrolled more children withspecial needs, and enrolledmore children with specialneeds on a full-time basis(children’s participation was notlimited to part-time for reasonsother than the fact that the pro-gram offered was a half-daypreschool). Almost 44% of thosecentres described as more inclu-sive had five or more childrenwith special needs in atten-dance, compared to 30.4% of cen-tres seen as not more inclusive.
✦ Centres described by directorsas more inclusive or more effec-tive were far more likely toreport that their centre accom-modated children with morecomplex needs than they hadpreviously. About 62% of direc-tors of more inclusive centresreportedly accommodated chil-dren with more complex needsin 1996-97, compared to only21% in centres described by di-
“Since 1990, many centres havebecome more inclusive in their prac-tice and/or more effective in inte-grating children with special needsin their programs. Does this de-scribe your centre?” Of the 127 di-rectors who replied, 80 (63%) saidthis described their centre, while 47directors (37%) answered “No.” Ninedirectors of the 136 in the sampledeclined to answer. When non-re-sponders are grouped with thosedirectors who answered no, we ob-serve that 69.4% of designated cen-tres, 50.8% of regular centres, and45.5% of specialized program direc-tors described their centres as moreinclusive or more effective in 1996-97 than in 1990.
While the number of centres perprovince is too small to permit de-tailed cross-provincial comparisons,it is fair to point out that the pro-portion of centres described by di-rectors as more inclusive variedacross jurisdictions from 0% to83.3%. In three jurisdictions, onethird or fewer centres were de-scribed as more inclusive; in threeprovinces between half and twothirds of the centres were describedas more inclusive; and in four ju-risdictions 71-83% of centres weredescribed as more inclusive.
If directors’ perceptions are to betreated as valid indicators of differ-ences in centre practices, we shouldbe able to see significant differencesin the extent of inclusion and in staffattitudes towards inclusion thatsupport directors’ evaluations. Infact, a number of points do validatedirectors’ judgements.
8.61 Markers/Validators of Directors’Views of Their Centre as MoreInclusive or More Effective
Centres described by directors ashaving become more inclusive/

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 135
rectors as not having becomemore inclusive or more effective.In the latter case, directors weremore likely to report that thecomplexity of children’s needstheir centre accommodated hadremained the same over thatperiod. Statistical comparisonswere highly significant(Chi square =19.176, p< .001).
✦ Centres described as moreinclusive or more effective bydirectors were slightly morelikely to report that parents weremore extensively involved withfrequent meetings and commu-nication. This difference was notstatistically significant, but wasin the expected direction.
✦ One might expect reports thatcoordination is problematic tobe rare in this population ofcentres that has a longer-termhistory with inclusion, andpresumably well-establishedrelationships with specialistsand community professionals.Directors of centres in both cat-egories were equally likely to saythat coordination of services forchildren with special needs wasgoing very well, with no majorproblems most of the time(40.5% of each group). However,almost twice as many centredirectors in the “not moreinclusive” group admitted thatthere were some problems orserious problems with coordina-tion that were occurring on aregular basis (19.0% vs. 10.2%,respectively).
In summary, several specific mark-ers appeared to validate directors’assessments of whether their cen-tre had become more inclusive ormore effective in inclusion practicesover time. The descriptions abovesuggest that centres described as
more inclusive had staff who weretaking on more responsibilities overtime and were doing reasonablywell in managing additional chal-lenges. What enabled these centresto function more effectively? Whatfactors impeded other centres?
8.62 Perceived Enablers of EffectiveInclusion
Directors who indicated that theircentre had become more inclusiveand/or more effective in integrat-ing children with special needssince 1990 were asked which ofseveral factors had enabled theircentre and their staff to becomemore inclusive during that period.Directors were asked to indicate allfactors that applied and note thetwo factors that had been most im-portant. Table 8.6 summarizes di-rectors’ responses (See followingpage.)
Of 10 possible enablers, five wereseen as important by half or moreof the directors, and eight of the10 factors were seen as having beenimportant by 25 percent of direc-tors. The single enabling factor onwhich there was greatest consen-sus among directors was accumu-lated experience in working withchildren with special needs (73%).We interpret this as most likelymeaning accumulated positive ex-periences in working with childrenwith special needs. Spontaneouscomments about the value of posi-tive experiences throughout thestaff and director surveys notedhow important such experiencesare for enabling staff to feel morecomfortable working with the chil-dren in their care, and giving themself-confidence.
The second factor identified mostoften by directors as important for
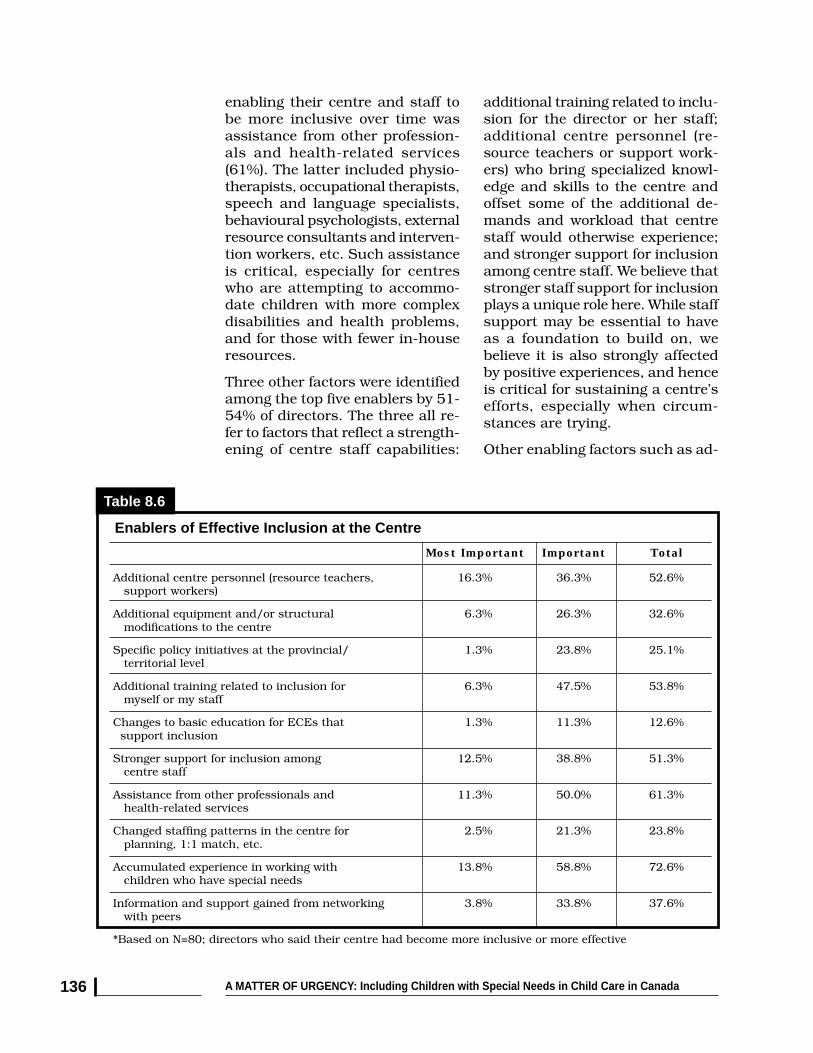
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada136
enabling their centre and staff tobe more inclusive over time wasassistance from other profession-als and health-related services(61%). The latter included physio-therapists, occupational therapists,speech and language specialists,behavioural psychologists, externalresource consultants and interven-tion workers, etc. Such assistanceis critical, especially for centreswho are attempting to accommo-date children with more complexdisabilities and health problems,and for those with fewer in-houseresources.
Three other factors were identifiedamong the top five enablers by 51-54% of directors. The three all re-fer to factors that reflect a strength-ening of centre staff capabilities:
additional training related to inclu-sion for the director or her staff;additional centre personnel (re-source teachers or support work-ers) who bring specialized knowl-edge and skills to the centre andoffset some of the additional de-mands and workload that centrestaff would otherwise experience;and stronger support for inclusionamong centre staff. We believe thatstronger staff support for inclusionplays a unique role here. While staffsupport may be essential to haveas a foundation to build on, webelieve it is also strongly affectedby positive experiences, and henceis critical for sustaining a centre’sefforts, especially when circum-stances are trying.
Other enabling factors such as ad-
Enablers of Effective Inclusion at the Centre
Table 8.6
Most Important Important Total
Additional centre personnel (resource teachers, 16.3% 36.3% 52.6% support workers)
Additional equipment and/or structural 6.3% 26.3% 32.6% modifications to the centre
Specific policy initiatives at the provincial/ 1.3% 23.8% 25.1% territorial level
Additional training related to inclusion for 6.3% 47.5% 53.8% myself or my staff
Changes to basic education for ECEs that 1.3% 11.3% 12.6% support inclusion
Stronger support for inclusion among 12.5% 38.8% 51.3% centre staff
Assistance from other professionals and 11.3% 50.0% 61.3% health-related services
Changed staffing patterns in the centre for 2.5% 21.3% 23.8% planning, 1:1 match, etc.
Accumulated experience in working with 13.8% 58.8% 72.6% children who have special needs
Information and support gained from networking 3.8% 33.8% 37.6% with peers
*Based on N=80; directors who said their centre had become more inclusive or more effective

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 137
ditional equipment and structuralmodifications are important, espe-cially if there are obvious barriersthat prevent certain children fromattending at all, but do not appearto be as significant to directors inthis sample as the other factorsalready mentioned. Provincialpolicy initiatives were seen as animportant enabler for programs byabout one quarter of centre direc-tors, but were not seen as one ofthe most important factors. (Theimportance of positive policy initia-tives may be less directly recogniz-able as such, although they maybe responsible for funding that al-lows the hiring of additional per-sonnel or additional training forcentre staff.)
Together, this profile of directors’responses regarding enabling fac-tors identifies the critical impor-tance of:
✦ accumulated positive experi-ences with inclusion in childcare centres,
✦ appropriate assistance beingprovided by other professionalsto support and complementstaff efforts, and
✦ resources that add to andstrengthen staff capabilitieswithin centres (the number ofstaff with specialized skills,additional training, and supportthat enables staff to continue tofeel positively about inclusionand be committed to makinginclusion work within the cen-tre for more children over time).The latter also reflects highermorale and cohesion.
8.63 Factors That Limit or FrustrateEffective Inclusion
Directors were asked similarly to
identify those factors which, intheir opinion, had “limited or frus-trated your centre’s capacity to beinclusive and/or your program’seffectiveness in integrating childrenwith special needs.” Once again,they were asked to indicate all ofthe factors from a list of 10 thatapplied and to identify the two mostimportant limiting factors. Table 8.7summarizes directors’ responses(See following page.)
Of 10 possible frustrators, only onewas seen as important by morethan half of the directors, whilethree others were seen as impor-tant by between 40 and 50% of oursample. The single limiting factoron which there was greatest con-sensus among directors was “No orlimited additional funding to sup-port inclusion.” This factor wasdescribed as an important limitingfactor by 56% of our directors, in-cluding one fifth of the sample whosaid it was the most important fac-tor that limited or frustrated inclu-sion. The three factors on whichthere was also substantial agree-ment were: reduced funding to sup-port inclusion (40% of directors);stress caused by additionalworkload and time demands oncentre staff (41%), and the generallevel of support/funding for childcare programs in your province/territory (44%). It is interesting tonote that the next set of limitingfactors referred to lack of access toin-house resource teachers, andinsufficient involvement or supportfrom external resource consultantsand community based profession-als (described as important limit-ing factors by about one quarter ofthe directors). Very few directorsindicated that their staff’s level oftraining or attitudes were signifi-cant limiting factors.
Frustrations about lack of funding

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada138
Most Important Important Total
No or limited additional funding to support inclusion 20.6% 35.3% 55.9%
Reduced funding to support inclusion 13.2% 27.2% 40.4%
No in-house RT or loss of centre-based RT or 7.4% 16.9% 24.3% support worker
Limited/insufficient involvement of external RTs 1.5% 22.8% 24.3% or resource consultants
Limited support/assistance from other professionals/ 8.1% 19.1% 27.2% health-related services
Stress caused by additional workload and time 15.4% 25.7% 41.1% demands on centre staff
Lack of support from other parents or the 0.7% 2.9% 3.6% centre’s board
Staff not adequately trained to meet 4.4% 14.0% 18.4% children’s needs
Staff not willing or not committed to extend 2.9% 5.9% 8.8% inclusive practices
General level of support/funding for child care 9.6% 34.6% 44.2% programs in province or territory
Based on N=136; all directors
and lack of human resources werenoted in many of the quotes in-cluded in earlier sections of thischapter. In fact, one director of aspecialized centre noted herfrustration related to lack offunding to enable more typically de-veloping children to attend the pro-gram, thus limiting her efforts toevolve from a more segregated pro-gram to one that was moreintegrated.
8.7 CURRENT AND FUTURECONCERNS ABOUTINCLUSION: THE PERCEIVEDIMPACTS OF FISCALRESTRAINT
Section 8.6 referred to directors’perceptions of change in their cen-tre that had occurred in the periodfrom about 1990 to 1996-97 whendata were collected. We also wanted
to assess the extent to which re-ductions in funding to child careprograms in the year precedingdata collection had or were havingany effects on child care qualityand the centre’s capacities for ef-fective inclusion. This matter wasa pressing concern to address sincethe combination of the terminationof the Canada Assistance Plan, re-duced federal-provincial transfers,and a preoccupation with debt anddeficit during the slow recoveryfrom the recession of the early1990s was being felt across thecountry at a time when the urgentneed for reinvestment in child carewas patently evident.
Indeed, we felt that effective inclu-sion might have been seriouslyjeopardized in some provinces andin many centres. Understandingthe more immediate financial con-text in which directors and centres
Frustrators of Effective Inclusion at the Centre
Table 8.7
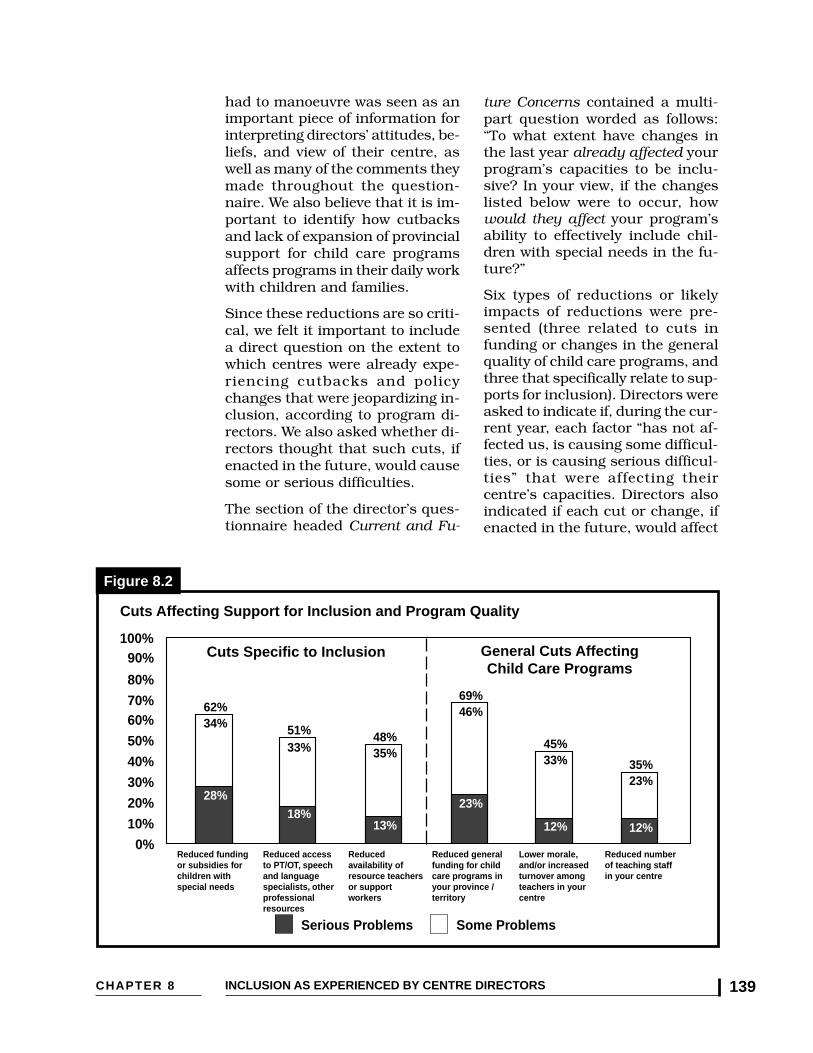
CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 139
had to manoeuvre was seen as animportant piece of information forinterpreting directors’ attitudes, be-liefs, and view of their centre, aswell as many of the comments theymade throughout the question-naire. We also believe that it is im-portant to identify how cutbacksand lack of expansion of provincialsupport for child care programsaffects programs in their daily workwith children and families.
Since these reductions are so criti-cal, we felt it important to includea direct question on the extent towhich centres were already expe-riencing cutbacks and policychanges that were jeopardizing in-clusion, according to program di-rectors. We also asked whether di-rectors thought that such cuts, ifenacted in the future, would causesome or serious difficulties.
The section of the director’s ques-tionnaire headed Current and Fu-
ture Concerns contained a multi-part question worded as follows:“To what extent have changes inthe last year already affected yourprogram’s capacities to be inclu-sive? In your view, if the changeslisted below were to occur, howwould they affect your program’sability to effectively include chil-dren with special needs in the fu-ture?”
Six types of reductions or likelyimpacts of reductions were pre-sented (three related to cuts infunding or changes in the generalquality of child care programs, andthree that specifically relate to sup-ports for inclusion). Directors wereasked to indicate if, during the cur-rent year, each factor “has not af-fected us, is causing some difficul-ties, or is causing serious difficul-ties” that were affecting theircentre’s capacities. Directors alsoindicated if each cut or change, ifenacted in the future, would affect
Serious Problems Some Problems
62%34%
28%
51%33%
18%
48%35%
13%
45%33%
12%
35%23%
12%
20%
30%
0%
10%
60%70%
40%
50%
100%
80%
90%
69%46%
23%
Reduced general funding for child care programs in your province / territory
Reduced funding or subsidies for children with special needs
Reduced access to PT/OT, speech and language specialists, other professionalresources
Reduced availability of resource teachers or support workers
Lower morale, and/or increased turnover among teachers in your centre
Reduced number of teaching staff in your centre
Cuts Specific to Inclusion
Figure 8.2
General Cuts AffectingChild Care Programs
Cuts Affecting Support for Inclusion and Program Quality

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada140
their program or would cause someor serious difficulties. The datapresented below focus only on re-ports of changes experienced in thelast year that had already affectedchild care programs’ capacities tobe inclusive.
Findings:
Of the 130 directors who respondedto this section of the survey, 89.2%said they had already experiencedreductions in funding, staffing, oraccess to community-based re-sources in ways that were affect-ing their centre’s capacities to beinclusive.
✦ More than 40% (41.5%) ofcentre directors reported havingexperienced one or more cuts orchanges that were causingserious difficulties for theircentre.
✦ Almost two-thirds of centredirectors reported some orserious problems as aresult of reduced general fund-ing for child care programs intheir province or territory or re-duced funding or subsidies forchildren with special needs(69%, and 62%, respectively).More than half also experiencedreduced access to physiothera-pists, occupational therapists,and/or speech and languagespecialists to support the effortsmade by staff in the child carecentre.
✦ Reductions in funding and staffsupport were not limited to onlya few provinces or regions of thecountry. Some difficulties wereexperienced in 75% of centresin 9 jurisdictions.
✦ A large majority of centre direc-tors (almost 75%) reported
experiencing two or more reduc-tions that were causing prob-lems in their centre. Of evengreater concern is the findingthat 30% of centre directors re-ported having already experi-enced reductions in two or moreareas that were seriously affect-ing inclusion!
✦ Typically, centres experiencedcuts and policy changes in waysthat affected both the base ofquality care through reductionsin general funding for child careprograms, a reduction in teach-ing staff in their centre, or as aresult of lower morale andincreased turnover related tocuts, as well as reductions insupports or funding specificallyneeded for effective inclusion(reduced availability of RTs orsupport workers, reducedaccess to PT/OT, speech andlanguage specialists and otherprofessionals, and reducedfunding or subsidies for childrenwith special needs). Approxi-mately 76.5% of centres hadexperienced problems relatedto general funding cuts or re-ductions; 72.8% of centresreported experiencing one ormore cuts to specific supportsfor inclusion.
8.8 SUMMING UP
This chapter provides extensiveinformation about directors andabout the experiences they havehad since 1990 in their efforts toprovide leadership to staff, to im-prove program quality, and to be-come more effective in integratingchildren with special needs intotheir child care centres. The chap-ter provides a moving portrait ofdirectors, many of whom are

CHAPTER 8 INCLUSION AS EXPERIENCED BY CENTRE DIRECTORS 141
committed to the concept of inclu-sion, and who have been attempt-ing to extend their efforts and thoseof their staff. It also demonstratesthat their individual motivationsand efforts are often not matchedby the availability of appropriatefunds and human resources tosupport inclusion.
Being more committed to inclusionand more accepting of a broadrange of children with special needswere found to be important at-tributes in directors. Not only dothey model these values for staff,but their presence is correlatedwith the director taking an activerole in advocating for support forinclusion and on behalf of childrenwith special needs. In these cases,the directors are more likely to pro-vide workshops on inclusion totheir staff and to others, and toaccept more children with specialneeds into their program.
While generally pro-inclusive intheir attitudes and beliefs, direc-tors provided many examples ofambivalence and frustration, andsometimes a rethinking of theirown view as to how and whetherthey could best meet the compet-ing needs of children, parents andstaff, given limited resources.
Directors provided examples oflearning from successful experi-ences and being chastened by situ-ations that were beyond the capaci-ties of themselves and their staffto handle. Clearly, one of the mainfindings was that attitudinal resis-tance to inclusion per se, and lackof appropriate education and expe-rience on the part of directors and
many of their staff were not signifi-cant barriers to inclusion, at leastamong this sample.
The most significant enablers ofeffective inclusion in these centreswere accumulated positive experi-ences in working with children withspecial needs, and the strengthen-ing of inclusive capacity amongcentre staff, in part through effec-tive support and collaboration withresource teachers/consultants andcommunity-based professionalsand specialists.
Barriers and factors that limit orfrustrate inclusion were also clearlyevident: expectations that are notmatched by resources to supportinclusion, and cutbacks and lackof government leadership to main-tain and build on, rather thanerode, the base quality of child careprograms, limit these programs’capacities to contribute effectivelyto the goals of early interventionand prevention and to the overallpromotion of healthy child devel-opment.
As one of our directors put it,“Early intervention programs forchildren with special needshave been proven to be suc-cessful. Preschools and daycare need to be a part ofearly intervention andpreparing young children fortheir future. All children, if it istheir parents’ choice, should beable to attend a regular pre-school program with the appro-priate supports in place for thatchild and for the teacher andthe preschool program.” (direc-tor of a specialized program in BC)

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada142
END NOTES
1 Kontos, S. & File. N. (1993). Staff development in support of integration. In C.A. Peck, S.L.Odom & D.D. Bricker (eds.), Integrating young children with disabilities into community pro-grams: Ecological perspectives on research and implementation. Baltimore: Paul H. Brookes,169-186.
2 Jorde-Bloom, P. and Sheerer, M. (1992). The child care director: A critical component of programquality. Educational Horizons (Spring), 138-145.
3 Helburn, S.W. (ed.) (1995). Cost, quality and child outcomes in child care centres. Denver, CO:University of Denver, Department of Economics, Centre for Research and Social Policy.
4 Odom, S.L. & Diamond, K.E. (1998). Inclusion of young children with special needs in earlychildhood education: The research base. Early Childhood Research Quarterly, 13(1), 3-25.
5 Bochner, S., Denholm, C.J. & Pieterse, M. (1990). Attitudes to integration in preschool: A com-parative study of preschool directors in Canada and Australia. Victoria, BC: University of Victoria,School of Child and Youth Care. See also Denholm, C.J. (1990). Attitudes of British Columbiadirectors of early childhood centres towards the integration of handicapped children. BritishColumbia Journal of Special Education, 14(1), 13-26.
6 Irwin, S.H. & DeRoche, J. (1992). Attitudes of Canadian mainstream child care staff towardinclusion of children with special needs. (Unpublished manuscript.)
CHAPTER 9 THE VIEWS OF TRAVELLING RESOURCE TEACHERS AND RESOURCE CONSULTANTS 143
9.1 INTRODUCTION
One of the windows available to usthat proved very valuable was ob-tained by surveying a small sampleof travelling resource teachers andresource consultants (TRT/RCs).These individuals were employed invarious jurisdictions by municipali-ties or provincial governments orthrough community-based non-profit agencies specifically for thepurpose of providing consultationand direct support to child carecentres, family daycare homes, andschool age programs that includechildren with special needs. Thisproject is one of a very few studiesto include this emerging sectorof the child care workforce inresearch.1
Travelling RTs/RCs provided aunique perspective in this researchproject. Most visit a variety of pro-grams and see which ones are do-ing well and which ones are hav-ing difficulty with inclusion. Theyalso develop an informed and in-forming perspective of those factors— both internal to child care pro-
AN EXTERNAL
WINDOW: THE VIEWS OF
TRAVELLING RESOURCE TEACHERS
AND RESOURCE CONSULTANTS
grams and external to them — thatdirectly affect centres’ capacities toprovide effective, inclusive care ofhigh quality.
Mailed surveys were used to obtaininformation from 23 TRT/RCs.Eighteen of the travelling RTs/RCswho responded (88%) had partici-pated in the 1990 study of attitudesand experiences of child careprofessionals conducted bySpeciaLink, and five were new re-cruits who replaced someone whohad participated in the earlierstudy.
The travelling RTs/RCs who hadbeen involved in the firstSpeciaLink study were not neces-sarily employed in their currentcapacity at that time — some hadbeen centre directors and some hadbeen front-line staff who had sincemoved into their current position.Twelve of the 23 travelling RTs/RCs(52%) were located in Ontario,where the model of travelling RTs/RCs has developed most rapidly;the remainder were scatteredamong other jurisdictions.2
9.Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada144
9.2 EXPERIENCE, EDUCATIONAND TRAINING OFTRAVELLING RESOURCETEACHERS/RESOURCECONSULTANTS
9.21 Experience
Almost half of the travelling RT/RCs (47.8%) had been in theirpresent position for five years orless, with another 39.1% havingbeen in their present position forbetween six and nine years. Therelatively large number of TRT/RCswith less than five years experiencein their present position is charac-teristic in occupations that areemerging, but belies the fact thatalmost 87% of the resource teach-ers/resource consultants had 10 or
more years experience in the childcare field, including 69.6% who had15 or more years experience inchild care programs. Likewise,slightly more than 60% of TRT/RCshad 10 or more years of combinedexperience in working with childrenwith special needs, either withinprograms or in a travelling capac-ity. (See Table 9.2)
9.22 Education and Training
Most travelling resource teachers/resource consultants (72.7%) hada community college diploma astheir primary form of post-second-ary education. Six TRT/RCs hada university degree, including threewith a graduate degree and twowith both a diploma and degree.
Geographic Distribution of Travelling Resource Teachers and Resource Consultants
Table 9.1
Jurisdiction Number PercentNS 1 4.3%NB 1 4.3%ON 12 52.2%MA 1 4.3%AB 2 8.7%BC 3 13.0%YT 2 8.7%NT 1 4.3%TOTAL 23 100.0%
Travelling Resource Teachers’ and Resource Consultants’ Experiential Background
Table 9.2
Average Length of Time in Years
1 - 2 3 - 5 6 - 9 10 - 14 15+
Years in present position 5.4 years 39.1% 8.7% 39.1% 8.7% 4.3%Years in child care field 16.8 years 0.0% 4.3% 8.7% 17.4% 69.6%Years worked with children with special needs as a resource teacher or consultant 11.8 years 13.0% 4.3% 21.7% 21.7% 39.1%
*Provinces without TRTs/RCs in our sample are not listed.

CHAPTER 9 THE VIEWS OF TRAVELLING RESOURCE TEACHERS AND RESOURCE CONSULTANTS 145
The majority of diplomas (84%) weregranted in early childhood education(ECE); degrees were awarded mostlyin psychology, special education,speech pathology or ECE. Eleven
RTs/RCs (47.8%) had an additionalcertificate or credential specific toinclusion (a Resource Teacher cer-tificate or another credential relatedto children with special needs).
Resource Teachers’ and Resource Consultants’ Self-identified Learning Needs
Table 9.4
Topic Areas in Which RTs and RCs Would Like Additional Training, PercentTechnical Assistance or Information
Accessing information about new assistive devices, learning tools and 69.6% specialized materials
Promoting social interactions between children with special needs and 65.2% other children
Maintaining and promoting quality care in a period of diminishing resources 60.9%
Training or helping ECEs to implement social skills programs 60.9%
Helping ECEs adapt curricula to suit individual needs 56.5%
Working as a team within centres on behalf of children with special needs 47.8%
How to help directors be more sensitive to issues within centres 47.8%
How to work collaboratively with agencies (FCS, schools) 47.8%
Learning about the experiences of other resource teachers/services 43.5%
Working with and supporting families 43.5%
Advocating on behalf of children and families with special needs 39.1%
How to promote the benefits of an itinerant model 39.1%
Training or helping ECEs to develop and implement IPPs 30.4%
How to work collaboratively with specialists (OT/PT, etc.) 26.1%
Specific, in-depth information about particular disabilities 21.7%
Developing and implementing individual program plans (IPPs) 17.4%
Travelling Resource Teachers’ and Resource Consultants’ Educational Background
Table 9.3
Formal Education Completed Number Percent*
Diploma - no degree 16 72.7%
No diploma - undergraduate degree 1 4.5%
Diploma and degree 2 9.1%
Graduate degree 3 13.6%
*based on N=22, 1 missing
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada146
All of the travelling resource teach-ers/resource consultants in thissample were actively supplement-ing their pre-service education withadditional learning activities.
Ten had taken a university or col-lege level course related to inclu-sion since 1990 and all had at-tended workshops or conferencessince then. In fact, 56% of the re-source teachers/resource consult-ants had attended ten or moreworkshops or conferences relatedto inclusion between 1990 and1996 (average = 16 workshops orconferences), and 20 of the 23 re-spondents had provided workshopsor in-service training to others onvarious topics related to childrenwith special needs.
When asked about their own learn-ing needs, RTs/RCs identified top-ics ranging from “accessing infor-mation about new assistive devices,learning tools and specialized ma-terials” (69.9%) to “developing andimplementing individual programplans” (17.4%). (See Table 9.4.)
9.3 ROLES ANDRESPONSIBILITIES OFTRAVELLING RESOURCETEACHERS/RESOURCECONSULTANTS
The roles and responsibilities oftravelling resource teachers/re-source consultants are multidi-mensional, complex, and variablefrom one individual or jurisdictionto another. Furthermore, roles andresponsibilities are changing in re-sponse to changing needs, the re-organization of community-basedservices and service delivery mod-els, changing policies, and changesto funding levels and funding allo-cations. At the time data werecollected:
✦ 5 resource teachers/resourceconsultants said their man-date/activities primarily or ex-clusively focussed on workingwith “identified” children only(those eligible for funding),
✦ 6 said their primary or exclu-sive mandate was to consultwith centres as problems or con-cerns are identified,
✦ 4 said both activities (workingwith identified children and con-sulting with centres) constitutedtheir primary mandate, and
✦ 1 consultant indicated that herprimary role was to promote thebenefits of the Resource Con-sultant model and its uses inher area.
In addition to working directly withchildren deemed eligible for specialservices, many resource teachers/resource consultants also workwith other, non-identified childrenwho require behavioural interven-tions, speech and languagetherapy, or are considered “at risk”for other reasons. Of those whowork directly with children, re-source teachers/resource consult-ants see an average of 10 childrenwith special needs per week (range5-16) with an average of 15 chil-dren with special needs in theiractive caseload (range 5-30). Oursample of TRT/RCs typically con-centrated on children age 0-6 yearsold, but some were involved in pro-viding support to caregivers of chil-dren 6-12 years old as well. Table9.5 provides additional informationabout the roles and responsibilitiesof travelling resource teachers andresource consultants, and confirmsthe importance of their role in sup-porting inclusive care.
In carrying out their many roles,travelling resource teachers/re-
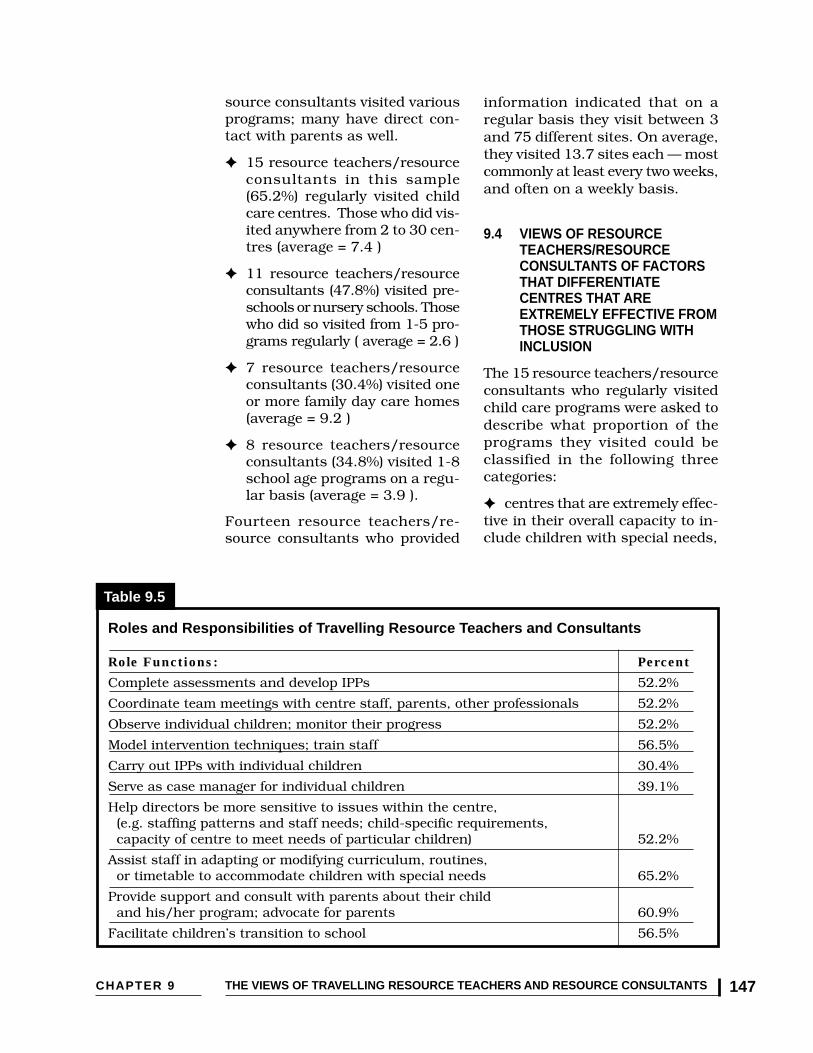
CHAPTER 9 THE VIEWS OF TRAVELLING RESOURCE TEACHERS AND RESOURCE CONSULTANTS 147
source consultants visited variousprograms; many have direct con-tact with parents as well.
✦ 15 resource teachers/resourceconsultants in this sample(65.2%) regularly visited childcare centres. Those who did vis-ited anywhere from 2 to 30 cen-tres (average = 7.4 )
✦ 11 resource teachers/resourceconsultants (47.8%) visited pre-schools or nursery schools. Thosewho did so visited from 1-5 pro-grams regularly ( average = 2.6 )
✦ 7 resource teachers/resourceconsultants (30.4%) visited oneor more family day care homes(average = 9.2 )
✦ 8 resource teachers/resourceconsultants (34.8%) visited 1-8school age programs on a regu-lar basis (average = 3.9 ).
Fourteen resource teachers/re-source consultants who provided
information indicated that on aregular basis they visit between 3and 75 different sites. On average,they visited 13.7 sites each — mostcommonly at least every two weeks,and often on a weekly basis.
9.4 VIEWS OF RESOURCETEACHERS/RESOURCECONSULTANTS OF FACTORSTHAT DIFFERENTIATECENTRES THAT AREEXTREMELY EFFECTIVE FROMTHOSE STRUGGLING WITHINCLUSION
The 15 resource teachers/resourceconsultants who regularly visitedchild care programs were asked todescribe what proportion of theprograms they visited could beclassified in the following threecategories:
✦ centres that are extremely effec-tive in their overall capacity to in-clude children with special needs,
Role Functions: Percent
Complete assessments and develop IPPs 52.2%
Coordinate team meetings with centre staff, parents, other professionals 52.2%
Observe individual children; monitor their progress 52.2%
Model intervention techniques; train staff 56.5%
Carry out IPPs with individual children 30.4%
Serve as case manager for individual children 39.1%
Help directors be more sensitive to issues within the centre, (e.g. staffing patterns and staff needs; child-specific requirements, capacity of centre to meet needs of particular children) 52.2%
Assist staff in adapting or modifying curriculum, routines, or timetable to accommodate children with special needs 65.2%
Provide support and consult with parents about their child and his/her program; advocate for parents 60.9%
Facilitate children’s transition to school 56.5%
Table 9.5
Roles and Responsibilities of Travelling Resource Teachers and Consultants
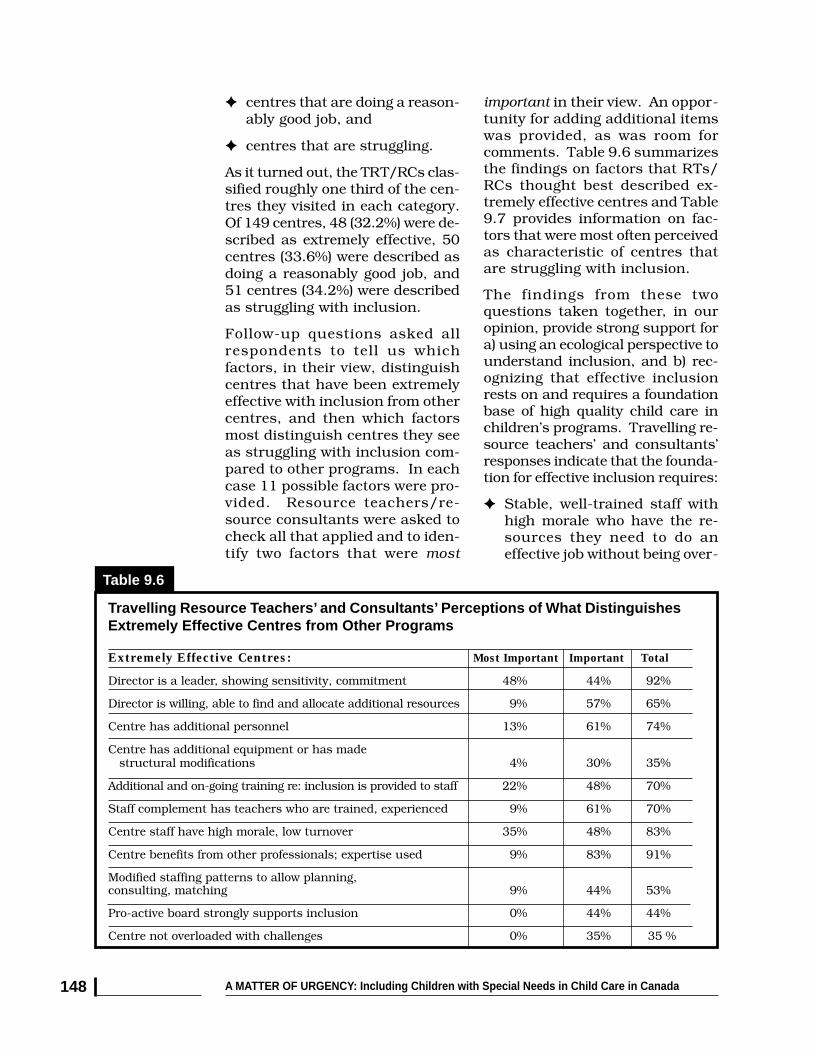
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada148
important in their view. An oppor-tunity for adding additional itemswas provided, as was room forcomments. Table 9.6 summarizesthe findings on factors that RTs/RCs thought best described ex-tremely effective centres and Table9.7 provides information on fac-tors that were most often perceivedas characteristic of centres thatare struggling with inclusion.
The findings from these twoquestions taken together, in ouropinion, provide strong support fora) using an ecological perspective tounderstand inclusion, and b) rec-ognizing that effective inclusionrests on and requires a foundationbase of high quality child care inchildren’s programs. Travelling re-source teachers’ and consultants’responses indicate that the founda-tion for effective inclusion requires:
✦ Stable, well-trained staff withhigh morale who have the re-sources they need to do aneffective job without being over-
✦ centres that are doing a reason-ably good job, and
✦ centres that are struggling.
As it turned out, the TRT/RCs clas-sified roughly one third of the cen-tres they visited in each category.Of 149 centres, 48 (32.2%) were de-scribed as extremely effective, 50centres (33.6%) were described asdoing a reasonably good job, and51 centres (34.2%) were describedas struggling with inclusion.
Follow-up questions asked allrespondents to tell us whichfactors, in their view, distinguishcentres that have been extremelyeffective with inclusion from othercentres, and then which factorsmost distinguish centres they seeas struggling with inclusion com-pared to other programs. In eachcase 11 possible factors were pro-vided. Resource teachers/re-source consultants were asked tocheck all that applied and to iden-tify two factors that were most
Table 9.6
Travelling Resource Teachers’ and Consultants’ Perceptions of What DistinguishesExtremely Effective Centres from Other Programs
consulting, matching 9% 44% 53%
Pro-active board strongly supports inclusion 0% 44% 44%
Centre not overloaded with challenges 0% 35% 35 %
structural modifications 4% 30% 35%
Additional and on-going training re: inclusion is provided to staff 22% 48% 70%
Staff complement has teachers who are trained, experienced 9% 61% 70%
Centre staff have high morale, low turnover 35% 48% 83%
Centre benefits from other professionals; expertise used 9% 83% 91%
Modified staffing patterns to allow planning,
Extremely Effective Centres: Most Important Important Total
Director is a leader, showing sensitivity, commitment 48% 44% 92%
Director is willing, able to find and allocate additional resources 9% 57% 65%
Centre has additional personnel 13% 61% 74%
Centre has additional equipment or has made

CHAPTER 9 THE VIEWS OF TRAVELLING RESOURCE TEACHERS AND RESOURCE CONSULTANTS 149
whelmed. These resources in-clude time, additional person-nel, additional training, effectivearrangements within the centreto facilitate teamwork, and theirdirector’s and board’s supportfor their efforts;
✦ Expertise, consultation, andsupport from relevant commu-nity professionals; and
✦ A director who is effective, sen-sitive to her staff, and highlycommitted to inclusion — aleader who motivates and sup-ports others and is directly in-volved in contributing to thecentre’s success.
It was interesting to note that whilemany factors were considered to beimportant for effective inclusion bytravelling RT/RCs, the centredirector’s leadership, commitment,effectiveness and sensitivity were
seen as most crucial, both in dis-tinguishing centres that are ex-tremely effective from others, andin distinguishing between centresthat are struggling with inclusioncompared to other programs.
“High level of caring and com-mitment from parents, staff,CDC — who all work together.”(resource consultant from theYukon Territories, describing cen-tres that are extremely effective)
“Attitude — willingness andopen-mindedness. In general,there is not enough commitmentfrom directors or staff to inclu-sive child care. My perceptionis that they feel they haveenough to do and that they donot have the funding to pay forthe extra time for meetings andworkshops.” (resource consultant,Ontario, describing centres that arenot effective)
Table 9.7
Travelling Resource Teachers’ and Consultants’ Perception of What DistinguishesCentres That Are Struggling with Inclusion from Other Programs
support inclusion 17% 61% 78%
No in-house RT or loss of centre-based RT or support worker 0% 35% 35%
No or limited additional equipment; structural
among RTs and ECEs 17% 57% 74%
Number of children with major challenges strains centre resources 9% 44% 53%
High staff turnover; low morale 17% 61% 78%
modifications not made 0% 39% 39%
Stress caused by additional workload and time demands 17% 61% 78%
Lack of support from other parents 0% 52% 52%
Staff not adequately trained to meet children’s needs 13% 78% 91%
Lack of effective team work, sharing of roles
Centres That Are Struggling with Inclusion: Most Important Important Total
Director is not effective or is insensitive to staff needs 30% 44% 74%
Director, staff, or board not really committed to inclusion 44% 35% 79%
No or limited additional funding or personnel to
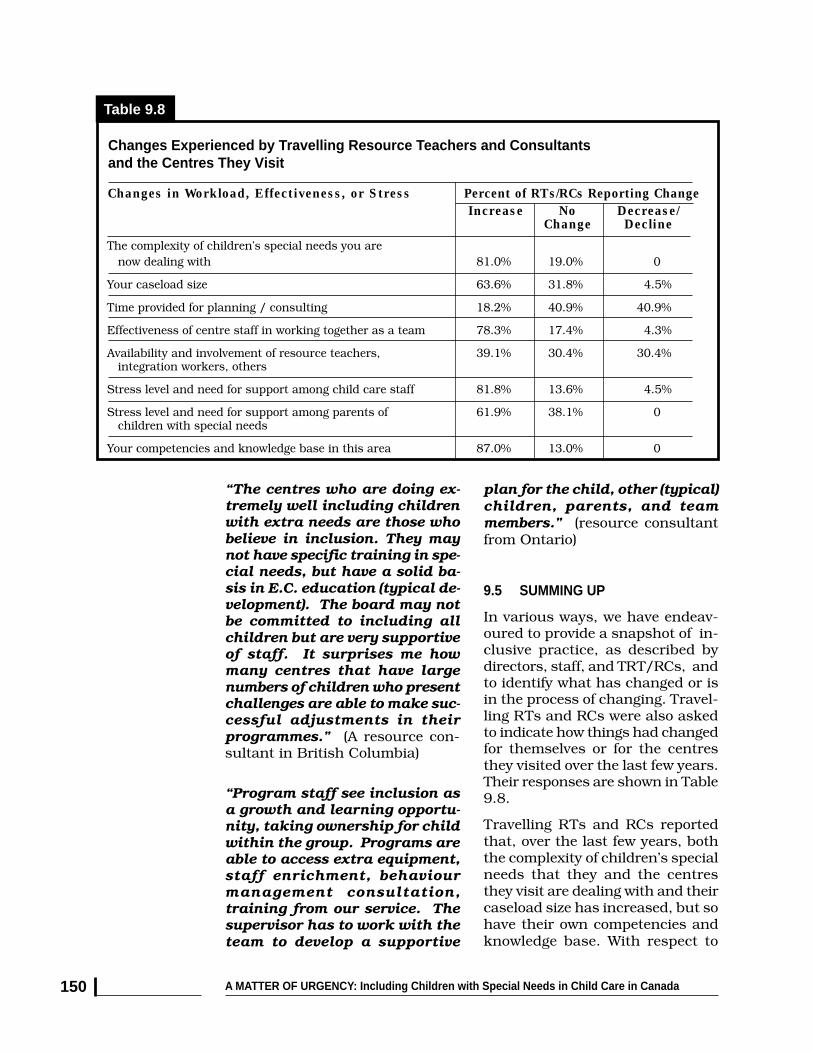
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada150
Changes in Workload, Effectiveness, or Stress Percent of RTs/RCs Reporting Change
Table 9.8
Changes Experienced by Travelling Resource Teachers and Consultantsand the Centres They Visit
Increase No Decrease/Change Decline
The complexity of children’s special needs you are now dealing with 81.0% 19.0% 0
Your caseload size 63.6% 31.8% 4.5%
Time provided for planning / consulting 18.2% 40.9% 40.9%
Effectiveness of centre staff in working together as a team 78.3% 17.4% 4.3%
Availability and involvement of resource teachers, 39.1% 30.4% 30.4% integration workers, others
Stress level and need for support among child care staff 81.8% 13.6% 4.5%
Stress level and need for support among parents of 61.9% 38.1% 0 children with special needs
Your competencies and knowledge base in this area 87.0% 13.0% 0
plan for the child, other (typical)children, parents, and teammembers.” (resource consultantfrom Ontario)
9.5 SUMMING UP
In various ways, we have endeav-oured to provide a snapshot of in-clusive practice, as described bydirectors, staff, and TRT/RCs, andto identify what has changed or isin the process of changing. Travel-ling RTs and RCs were also askedto indicate how things had changedfor themselves or for the centresthey visited over the last few years.Their responses are shown in Table9.8.
Travelling RTs and RCs reportedthat, over the last few years, boththe complexity of children’s specialneeds that they and the centresthey visit are dealing with and theircaseload size has increased, but sohave their own competencies andknowledge base. With respect to
“The centres who are doing ex-tremely well including childrenwith extra needs are those whobelieve in inclusion. They maynot have specific training in spe-cial needs, but have a solid ba-sis in E.C. education (typical de-velopment). The board may notbe committed to including allchildren but are very supportiveof staff. It surprises me howmany centres that have largenumbers of children who presentchallenges are able to make suc-cessful adjustments in theirprogrammes.” (A resource con-sultant in British Columbia)
“Program staff see inclusion asa growth and learning opportu-nity, taking ownership for childwithin the group. Programs areable to access extra equipment,staff enrichment, behaviourmanagement consultation,training from our service. Thesupervisor has to work with theteam to develop a supportive

CHAPTER 9 THE VIEWS OF TRAVELLING RESOURCE TEACHERS AND RESOURCE CONSULTANTS 151
child care centres, approximately78% of RTs and RCs reported hav-ing observed an increase or im-provement in the effectiveness ofcentre staff working together as ateam, but without commensurateincreases in time available for plan-ning and consulting or a significantincreased involvement on the partof resource teachers or integrationworkers.
Most troubling were the findingsthat more than 80% of TRT/RCsreported having observed an in-crease in the stress level and needfor support among child care staff,and that almost 62% of TRT/RCshad seen an increase in stressamong parents of children withspecial needs.
Overall, what emerges from thedata provided by travelling RTs andRCs — an important external win-dow on child care programs — isvalidated elsewhere in this report.
A consistent, mixed pictureemerges from the multiple windowsavailable. On the one hand, thatpicture is one of child care pro-grams and staff gaining more con-fidence in their work with childrenwith special needs and a strongercommitment to inclusion, accom-panied by greater efforts to includemore children with more complexor challenging conditions. On theother hand, the picture shows lim-ited resources and additionalstress. Moreover, examination ofthe roles, responsibilities and ex-periences of travelling RTs and RCsdemonstrates that they are a criti-cal part of the infrastructure thatsupports effective inclusion — andthat their capacity to do so is alsovulnerable when funding con-straints result in imbalances be-tween workload expectations andtheir capacity to provide support toparents, children, and child careprograms.
END NOTES
1 A separate, but related, study of the roles and responsibilities of in-house and travellingresource teachers/consultants in Ontario has recently been completed. See Coulman, L. (1999).Knowledge, attitudes, and experiences of resource teachers and resource consultants in inclu-sive child care centres in Ontario. Masters thesis, University of Guelph, Faculty of GraduateStudies. Other Canadian research studies on resource teachers and resource consultants in-clude: Brophy, K., Hancock, S. & Otoo, M. (1993). The role of the resource teacher in child careprograms: An Ontario study. Early Child Development and Care, 84, 75-80; Frankel, E.B. (1994).Resource teachers in integrated children’s centres: Implications for staff development. Interna-tional Journal of Early Childhood, 26(2), 13-20; and Hutchinson, N.L. & Schmid, C. (1996).Perceptions of a resource teacher about programs for preschoolers with special needs and theirfamilies. Canadian Journal of Research in Early Childhood Education, 5(1), 73-82.
2 Given the concentration of TRT/RCs from Ontario and the small number in other jurisdic-tions, we would recommend that a larger study of travelling RT/RCs’ views might be useful.However, the opinions provided, even by this small sample of “key informants,” are consistentwith the growing literature on inclusive child care.
CHAPTER 10 SUMMARY, INTEGRATION, AND CONCLUSIONS 153
INTEGRATING
WHAT WE HAVE LEARNED
10.needs? To what extent is theirparticipation limited to parttime attendance due to fundingand resource constraints? Howdo directors, ECEs, resourceteachers/support workers, ex-ternal consultants, and commu-nity professionals collaborate tomake inclusion work?
✦ What resources are required foreffective inclusion? What en-ables staff to work successfullywith children with specialneeds? What resources are nec-essary for programs to be effec-tive and to continually improvein this area?
✦ How can we characterize direc-tors’ and front-line teachingstaff’s attitudes, beliefs and feel-ings about inclusive child care?How have the experiences theyhave had with inclusion in theircentres affected their current at-titudes? What has changed overtime?
✦ What are some of the challengesstaff and programs face in theirongoing efforts to provide highquality, inclusive care? Whatare the most critical factors thatdistinguish programs that areextremely effective from otherprograms? What are the criticalfactors that are seen to be as-sociated with centres strugglingwith inclusion?
Donna S. Lero, Sharon Hope Irwin, Kathleen Brophy
10.1 INTRODUCTION
This study had a number of goalsand objectives. Our primary pur-pose was to develop an in-depthunderstanding of the factors thatare most critical to maintain andenhance inclusive child care inCanada. The approach we used toachieve that goal was to conduct amultifaceted study of child careprofessionals in centres that hadalready been involved in includingchildren with special needs forsome years. In effect, we wanted tounderstand their experiences —both successful and less success-ful — in order to determine whatpractical recommendations couldbe developed to support and en-hance the capacities of child careprograms to integrate children withspecial needs effectively and to sus-tain their capacities to do so overtime.
Among the many questions wewanted to answer were these:
✦ How do inclusive programsfunction? How many childrenwith special needs do they in-clude, and under what condi-tions? To what extent are chil-dren with severe disabilities,complex needs and challengingbehaviours turned away fromcentres that have and do acceptother children with special

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada154
✦ Have provincial funding cuts af-fected centres’ capacities to pro-vide high quality, inclusive care?What are the most critical policyand practice concerns that mustbe addressed to maintain andenhance the capacities of cen-tres and their staff to providehigh quality care for allchildren?
Our study involved viewing inclu-sive child care through four dis-tinct, but complementary “win-dows.” Those windows enabled usto consider:
1) what the research literature andpractice base related to inclusivechild care can tell us;
2) the views and experiences offront-line child care staff, consist-ing of both early childhood educa-tors and more specially trained in-house resource teachers/supportworkers;
3) the views and experiences of cen-tre directors in their multiple roles;and
4) the perspectives of travelling re-source teachers/resource consult-ants who visit and provide supportto early childhood programs andwho are in a position to identifywhich factors they see contribut-ing to successful inclusion andwhat remain as serious obstaclesto that goal.
Looking through different windowsat the same phenomenon, or view-ing it from different angles, cansometimes result in fragmentedand inconsistent images that don’tfit into a coherent whole. That wasnot the case in this instance. In-stead, we are struck with how con-sistent and coherent our emergingunderstanding of inclusive childcare is, and how helpful it is to be
able to integrate information ob-tained from the three sub-samplesincluded in this study.
Moreover, we have found that em-ploying an ecological theoreticalframework has helped us appreci-ate how the various person, pro-cess, and contextual factors relatedto inclusion operate in a complex,dynamic, but understandable fash-ion. This framework recognizes, forexample, the importance of ECEs’and resource teachers’ attitudesand training, directors’ attitudesand leadership capabilities, and theprogrammatic requirementsnecessary to support and accom-modate individual children, asexamples of person factors that arecritical elements to consider. Con-sideration of processes — specifi-cally, the experiences teachers anddirectors have with inclusion, andhow both successful and unsuc-cessful experiences affect their on-going commitment and willingnessto include a wide range of children— are also essential to this frame-work and to our understanding.Thirdly, considerations of contextprovide a much needed focus onthe human and financial resourcesavailable to support inclusion, aswell as the policy context that af-fects the base level of quality onwhich successful inclusion rests.
10.2 NECESSARY INGREDIENTSFOR SUCCESSFUL INCLUSION
The research literature and a baseof practice knowledge developedover more than a decade bySpeciaLink1 and others has con-firmed that successful inclusionrequires much more than havingchildren with special needs in at-tendance and the implementationof individual program plans forthese children within child care

CHAPTER 10 SUMMARY, INTEGRATION, AND CONCLUSIONS 155
centres. Based on our researchfindings we see effective inclusionas requiring and being sustainedby:
✦ positive attitudes toward inclu-sion on the part of the directorand program staff. Beyond that,it is evident from our research(as was suggested by Peck in aseries of studies)2 that long-termsuccess requires an ongoingand sustained commitment onthe part of all staff in a child careprogram, along with parentsand board members, to makeinclusion work well in the cen-tre and to continue to do so aspart of the centre’s ethos or ser-vice mission (that is, as an in-tegral component of the identityof that centre);
✦ high quality programs that canbe used to support successfulinclusion. This basic level ofquality presupposes that childcare programs have stable, well-educated and well-paid staff,most of whom have at least atwo-year community college di-ploma and some of whom havespecialized training related toincluding children with specialneeds, as well as appropriatestable funding to support theprovision of a well-designedcurriculum in an accessibleenvironment;
✦ a commitment to implementinclusion with respect for staffneeds and concerns, as evi-denced by directors taking stepsto enable centre staff to workwell as a team, and to providethe training, resources, andsupports needed to enable themto succeed;
✦ the practice of using experiences(both positive and difficult ones)
as a basis for ongoing learningand improvement for all centrestaff and for communities thatwant to have well-functioningearly childhood programs asservice partners in an integratedapproach to supporting childrenand families;
✦ effective collaboration with, andthe involvement of, external re-source consultants and relatedprofessionals in the community(e.g., speech and language spe-cialists, early intervention staff,physiotherapists, occupationaltherapists, public healthnurses, psychologists, socialworkers);
✦ centres developing and sustain-ing their capacity to involve andsupport parents of children withspecial needs in ways that arebeneficial to their child’sprogress and respectful of par-ents’ wishes and concerns;
✦ communicating with others,sharing experiences, and advo-cating for resources that are im-portant not only for one’s owncentre, but also for other pro-grams and for all children andfamilies; and
✦ ongoing research, professionaldevelopment, and policy analy-sis that can support all of theabove by providing both thetechnical assistance and fund-ing support that are required tosupport effective inclusion as acomponent of a high qualitychild care system.
[The sections below provide addi-tional observations and commentsrelated to several of these neces-sary ingredients.]
Despite uneven policy developmentand limited funding support, it ap-

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada156
pears that successful inclusion,when viewed in this holistic way,has become and is reflective of an-other level or dimension of qualityin child care settings that has beenadopted by child care professionals,as well as an obvious criterion for amore coherent, integrated child careservice system. This view is based,in part, on an ongoing articulationof standards to be met in high qual-ity, developmentally appropriate,inclusive care programs; and on theadoption of a code of ethics3 for thechild care field that includes anappreciation of the rights of all chil-dren and families to high qualitycare. (See Chapter 2, Section 2.5 forfurther discussion.)
10.3 SPECIFIC FINDINGS FROMOUR RESEARCH
The research findings highlightedin this section integrate resultsobtained from the three sub-samples within our study that arereported in Chapters 7, 8, and 9 ofthis report. In particular, we notethe convergence that is visiblewhen we consider what ECEs andin-house resource teachers tell ushas contributed to their success-ful experiences in including chil-dren with special needs in theircentres (and also what have beensources of frustration); what direc-tors tell us has enabled or limitedtheir centres from being effective inintegrating children with specialneeds; and what travelling RTs/RCs describe as the factors thatmost distinguish centres that areextremely effective with inclusionfrom those that are struggling. Inevery case the importance of thenecessary ingredients listed in theprevious section was confirmed.
As well, there is evidence of twoalternative potential dynamics that
we describe in more detail in Sec-tion 10.4 of this chapter.
One dynamic consists of what werefer to as a positive, or virtuous,cycle in which centre staff are en-abled and supported to experiencesuccess; which, in turn, results ina stronger commitment to inclu-sion, enhanced skills, more confi-dence, and a willingness to con-tinue to expand their efforts.
The second, competing dynamic,consists of a discouraging cycle inwhich centre staff are frustrated intheir efforts to successfully includechildren with special needs, in partbecause of a lack of appropriate re-sources and support available forthat purpose, and/or because oflimited supports to sustain the baselevel of quality in the centre. In thiscase it appears that both the direc-tor and centre staff become lessaccepting of the centre’s goal of in-cluding a broad range of childrenwith special needs, even if it remainsan ideal they agree with and endorseas a fundamental principle.
In such cases, centres may ceaseto enroll any children with specialneeds, or do so only on occasion,with children who fit a narrow bandof conditions that the centre feelscan be accommodated, retrenchingfrom a view of their centre as anintegrated program in their com-munity. It would appear that chil-dren with more severe disabilities,complex needs, and those withchallenging behaviours will mostlikely be excluded in such cases.
10.31 Positive Attitudes TowardInclusion and Staff’s Educationand Training
The literature reviewed in Chapter3 reflects the fact that through the1980s and 1990s research identi-

CHAPTER 10 SUMMARY, INTEGRATION, AND CONCLUSIONS 157
fied positive attitudes toward inclu-sion as a critical contributor to itssuccessful implementation, andsimilarly, resistant attitudes as oneof the largest barriers to inclusion,both in early childhood programsand in school-based settings.
Early childhood teachers who lackpost-secondary education in ECEor child development and addi-tional ongoing learning opportuni-ties to enable them to plan for andadapt curricula and activities ap-propriately are most likely to beconcerned about and less commit-ted to working with children withspecial needs.
Less positive attitudes toward in-clusion have been shown to reflecta number of factors. These include:resistance to including childrenwith specific disabilities or condi-tions that require more individual-ized, specific knowledge and ongo-ing 1:1 involvement (especiallywithout additional centre person-nel); limited self-confidence on thepart of teachers; limited prepara-tion for, or perceived skill in, work-ing collaboratively with parents andother professionals; and significantconcerns about the resources avail-able to support inclusion —particularly concerns aboutadditional workload, stress, andlack of planning and consultationtime.
Stoiber et al. (1998)4 have foundthat early childhood staff’s beliefsabout inclusion were associatedwith their level of education, theirtraining, and years of experience.Their findings and those of othersare generally based on heterog-enous samples from a range ofcommunity programs.
Our study used a rather select andspecialized sample — a purposive
sample — that focussed on front-line child care staff and centre di-rectors who already had consider-able experience with inclusion intheir programs. A high proportionof the early childhood educatorsand in-house resource teachers(87%) and directors (92%) had atwo-year diploma in ECE or a re-lated field or a university degree.In recent years, the majority hadattended a number of workshopsand conference presentations oninclusion or on children withspecial needs.
In our study, ECEs, in-house RTs,and directors expressed strongsupport for the view that childrenwith a wide range of disabilities,health conditions and behaviouraldifficulties should be enrolled inregular preschools or child careprograms, provided that the chil-dren have suitable access and thatresources are in place to meet thechild’s needs and maintain pro-gram quality. Of thirty specific con-ditions or circumstances, therewere only seven situations in whichless than 75% of program staff ordirectors did not agree that chidrenwith certain disabilities or chal-lenges should be included in regu-lar child care programs.In each case, the child’s circum-stances were seen to be particularlychallenging, either because accesswas unsuitable or 1:1 supervisionand/or more specialized assistancewas required. Overall, child carestaff in these programs, many ofwhom had several years experienceworking with children with specialneeds, expressed strong generalsupport for inclusion as an ideal.
They also responded to a series ofstatements designed to assess theircurrent beliefs about inclusion.Despite the lack of a legal mandateto do so, almost 90% of front-line

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada158
teaching staff endorsed the viewthat child care programs shouldaccept all children, regardless oftheir individual needs, and stronglyagreed with the statement: “Mostchild care programs would bewilling to include children withspecial needs, if adequateresources were available.”
In summary, within this sample ofrelatively well-trained teaching staffand directors, positive attitudestoward inclusion and a commit-ment to inclusion as a general goalwere the norm, and seemed to beimportant contributors to programsuccess, according to program di-rectors. “Stronger support for in-clusion among centre staff” and“Additional training related to in-clusion for me and/or my staff”were identified by centre directorsas among the top five contributingfactors that had enabled their cen-tre to become more inclusive/moreeffective in integrating childrenwith special needs between 1990and 1996-97.
Is this important to note? We be-lieve so. If an acceptance of diver-sity and a commitment to inclusionare becoming prevalent throughoutthe child care field, then a focuson efforts to persuade staff aboutinclusion and to promote positiveattitudes could still be useful as anadjunct approach, but probablyshould no longer be a main focusof attention. Meeting educators’needs for more specific informationand providing opportunities forthem to acquire skills and sharepositive experiences and strategieswould appear to be a more fruitfulapproach for those planning pro-fessional development and continu-ing learning activities, especially forchild care staff who already havesome background preparation andexperience.
We note, however, that pro-inclu-sion attitudes should neither beassumed nor taken for granted.While directors in our purposivesample indicated that, from theirperspective, the main barriers toinclusion did not emanate fromstaff unwillingness to accept chil-dren with special needs or a lackof commitment to inclusion, therecent You Bet I Care! 5 nationallyrepresentative sample revealed that“staff not feeling adequately trainedto care for children with specialneeds” and “a limited capacityor willingness on the partof staff to include children withcomplex problems or challengingbehaviours” were significant factorsin directors’ decisions to turn downan application or inquiry pertain-ing to a child with special needsfrom parents or community agen-cies who wished to refer a child toa local program.
We also note that our sub-sampleof travelling RTs/RCs who visit awide range of child care programsidentified “a lack of real commit-ment to inclusion on the part ofdirectors, staff, or the centre’sboard” as one of the most tellingfeatures that distinguished centresthat are struggling with inclusionfrom other centres. Furthermore,travelling resource consultantsidentified “staff not adequatelytrained to meed children’s needs”as among the most significant fac-tors that distinguished centres thatwere struggling with inclusion.
10.32 Supports Within Child CarePrograms
One of the observations that camethrough our study from each of thethree sub-sample groups and fromthe spontaneous comments madeby participants to our questions
CHAPTER 10 SUMMARY, INTEGRATION, AND CONCLUSIONS 159
was that centres clearly are colle-gial environments in which effec-tive supervisory support and co-worker relationships are criticalresources.
While external supports are alsoessential, ECEs and RTs in ourstudy confirmed that supportswithin the centre from co-workers,and adequate time to plan, consult,and liaise with parents and othersinvolved in the collaborative effortthat inclusion requires are criticalfactors — both in accounting fortimes when they were successful,and when they felt frustrated andtheir efforts were less successful.(See Chapter 7.) Staff felt most sup-ported when they could rely onadditional special needs workersand in-house RTs in the programto assist them, when other staff andthe director were supportive (bothinstrumentally and emotionally),when they had additional trainingto help them, and when positive re-lationships with parents were sus-tained.
Staff expressed most frustration,especially in working with childrenwith more complex or challengingconditions, when there were few orno additional resources to assistthem — no additional RT or inte-gration worker, lack of time to planand consult with parents and otherprofessionals, and in situationswhere the experience generally leftthem feeling pulled between thechild(ren) with special needs andthe needs of other children. In suchcases, staff can feel quite stressedand the experience can diminishboth their sense of competence andconfidence and their commitmentto inclusion.
We note, in particular, that whenasked how things had changed foryou or your centre in the last few
years, our sample of committedECEs and in-house RTs, as a whole,described a pattern that, on the onehand, indicated that their ownknowledge and competence had in-creased, as had their effectivenessas centre staff working together asa team. Both of these are particu-larly important since many front-line staff indicated that, comparedto earlier years, they were involvedwith children with increasingly com-plex special needs. On the otherhand, however, centre staff also re-ported that both time for planning/consulting and the availability andinvolvement of resource teachers,integration workers and others hadeither not changed commensuratelywith increasing demands, or hadactually decreased. (See Chapter 7,Section 7.6.)
Similarly, centre directors com-mented that limited funding or re-duced funding to support inclusion,limited general support from theirprovincial/territorial governmentfor child care programs, loss of cen-tre-based resource teachers or sup-port workers, and additionalworkload and time demands on cen-tre staff were factors that they felthad limited or frustrated theircentre’s capacity to be inclusiveand/or their program’s effective-ness. (See Chapter 8, Sections 8.6and 8.7.)
As confirmation, travelling resourceteachers and consultants reportedthat, in their view, centres that areextremely effective with inclusion aredistinguishable, particularly inhaving:
✦ directors who are leaders,who show sensitivity to staffneeds, and are effective infinding and allocating addi-tional resources to supportinclusion, and
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada160
✦ the capacity to benefit fromother professionals’ expertise.
These travelling RTs/RCs also con-firmed that centres that were ex-tremely effective with inclusion weremost likely to be those in which:
✦ the centre has additional per-sonnel to support inclusion;
✦ centre staff have high moraleand low turnover;
✦ centre teachers are trained andexperienced;
✦ additional and ongoing trainingrelated to inclusion is providedto staff; and
✦ staffing patterns are modified toallow planning and consultingtime.
Travelling resource teachers andconsultants similarly describedcentres that they see as strugglingwith inclusion as those in which:
✦ staff are experiencing additionalworkload and time demands;
✦ there is high staff turnover andlow morale;
✦ there is a lack of effective teamwork and sharing of roles;
✦ limited funding support andpersonnel are available to sup-port inclusion; and
✦ the director is not effective or isinsensitive to staff needs andconcerns.
10.33 The Role of Centre Directors asLeaders
Additional data analysis allowed usto explore in more detail how di-rectors function as leaders whosupport inclusion within child carecentres. Briefly, we reviewed direc-
tors’ responses to two questionsthat served as indicators of lead-ership. These were: a) whether thedirector had been involved since1990 in any advocacy activities re-lated to inclusion of children withspecial needs (such as presentinga brief, writing to an MP or MPP,being on a task force, etc.); and b)whether the director had providedany workshops or in-service train-ing to others on topics related tochildren with special needs.
We reasoned that participation inadvocacy activities in support of in-clusion is a strong, publicbehaviour that demonstrates com-mitment in a tangible way to childcare staff and others in the com-munity, and is oriented to secur-ing greater access to resources tomake inclusion work. The provisionof workshops or in-service trainingdemonstrates recognition of theimportance of addressing unmetinformation needs and enhancingskill development among staff andothers — another characteristic ofleadership. These two behaviours,while somewhat limited on theirown, are believed to be markers ofa broader constellation of directors’attitudes, skills and behaviours,including a pattern of relationshipswith staff, parents, board membersand community professionals thatshould result in high quality careand effective/successful inclusion.
According to directors’ self-reports,63 (47%) had been involved in ad-vocacy activities related to inclu-sion since 1990 and 69 (51%) hadprovided workshops or in-servicetraining to others on topics relatedto children with special needs.Based on these responses, we clas-sified directors as falling into threecategories indicative of leadership:

CHAPTER 10 SUMMARY, INTEGRATION, AND CONCLUSIONS 161
found to have higher scores on ourscale measuring general commit-ment to inclusion. Moreover, direc-tors who had engaged in neitherleadership behaviour describedthemselves as either less committedand/or less accepting of a broaderrange of children with special needsor as not having changed their viewover the years. Directors who hadeven been involved in one of the twoways of demonstrating leadershipwere more likely to say they weremore committed and more accept-ing of a broader range of childrenwith special needs.
Finally, and perhaps most impor-tantly, directors who exhibited lead-ership in either fashion were:
✦ more likely to enroll a largernumber of children with specialneeds, even when specializedprograms were excluded fromcomparisons;
✦ more likely to report that theircentres were accommodatingchildren with more complexneeds than they had previously; and
✦ more likely to say that since1990 their centre had becomemore effective or more success-ful with inclusion.
We believe these relationships arenot accidental. They confirm our in-terpretation that directors who takean active role in advocating for in-clusion and/or ensuring that theirstaff and others in the child carecommunity have access to in-ser-vice training are more committed toinclusion themselves and are alsoattentive to those conditions thatare needed to maintain theircentre’s effectiveness on an on-going basis.
✦ directors who had not been in-volved either in advocacy activi-ties in support of inclusion orin the provision of workshops orin-service training (46 directorsor 34%),
✦ directors who had been involvedin one of these two activities (46directors or 34%), and
✦ directors who had been involvedin both activities (43 or 32%) —these are the directors we referto as leaders.
Centre directors who were classi-fied as belonging to the middle cat-egory comprised 20 who had beeninvolved in advocacy activities onlyand 26 who had not been involvedin advocacy, but had providedworkshops or in-service training toothers on topics related to childrenwith special needs. Proportionately,82% of directors of specialized pro-grams met our definition of aleader, as did 39% of directors ofdesignated programs, but only 16%of directors of regular programs.
Analysis indicated that four back-ground variables contributed to adirector being a leader. Directorswho had more formal education (auniversity degree), those who hada credential or certificate related toinclusion or special needs, direc-tors who had more years of experi-ence in working with children withspecial needs, and those who at-tended more workshops and con-ferences and were involved in con-tinuous learning themselves weremore likely to be leaders in theircentres and communities.
Directors who were leaders (with ascore of two according to our clas-sificatory approach) were also
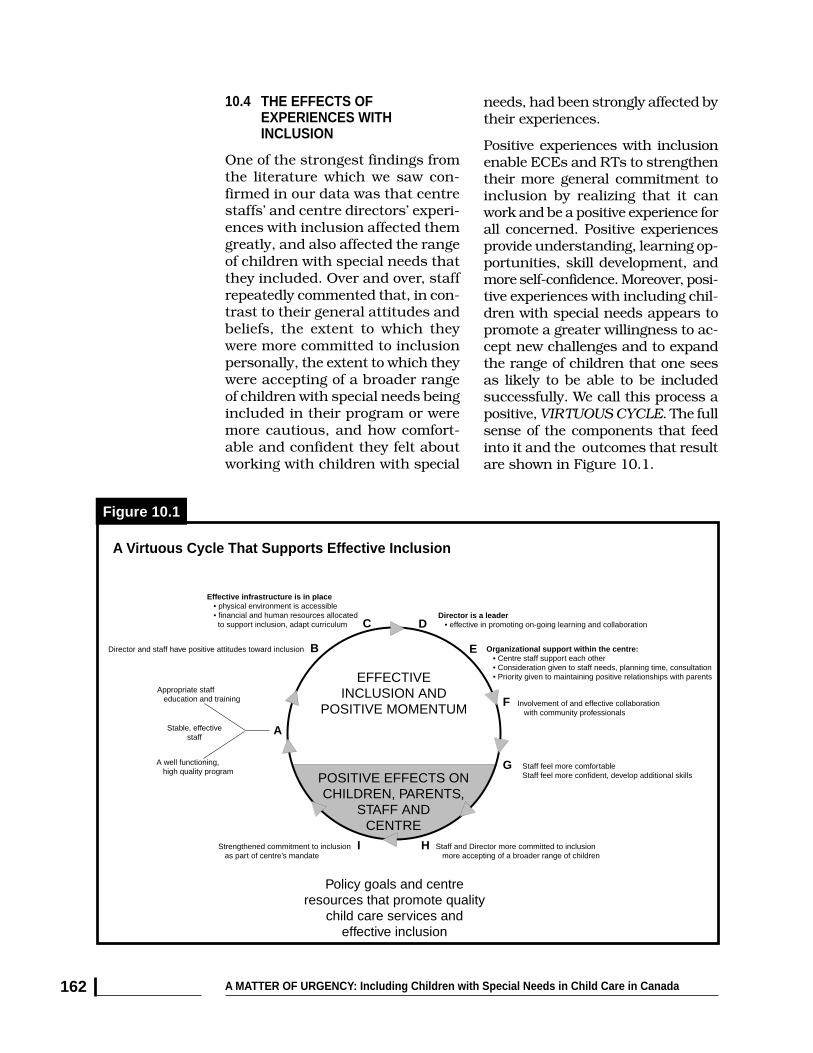
A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada162
10.4 THE EFFECTS OFEXPERIENCES WITHINCLUSION
One of the strongest findings fromthe literature which we saw con-firmed in our data was that centrestaffs’ and centre directors’ experi-ences with inclusion affected themgreatly, and also affected the rangeof children with special needs thatthey included. Over and over, staffrepeatedly commented that, in con-trast to their general attitudes andbeliefs, the extent to which theywere more committed to inclusionpersonally, the extent to which theywere accepting of a broader rangeof children with special needs beingincluded in their program or weremore cautious, and how comfort-able and confident they felt aboutworking with children with special
needs, had been strongly affected bytheir experiences.
Positive experiences with inclusionenable ECEs and RTs to strengthentheir more general commitment toinclusion by realizing that it canwork and be a positive experience forall concerned. Positive experiencesprovide understanding, learning op-portunities, skill development, andmore self-confidence. Moreover, posi-tive experiences with including chil-dren with special needs appears topromote a greater willingness to ac-cept new challenges and to expandthe range of children that one seesas likely to be able to be includedsuccessfully. We call this process apositive, VIRTUOUS CYCLE. The fullsense of the components that feedinto it and the outcomes that resultare shown in Figure 10.1.
A
B
C D
E
A well functioning, high quality program
Appropriate staff education and training
Stable, effectivestaff
EFFECTIVEINCLUSION AND
POSITIVE MOMENTUM
POSITIVE EFFECTS ONCHILDREN, PARENTS,
STAFF ANDCENTRE
F
G
HI
Policy goals and centreresources that promote quality
child care services andeffective inclusion
Staff feel more comfortableStaff feel more confident, develop additional skills
Staff and Director more committed to inclusion more accepting of a broader range of children
Strengthened commitment to inclusion as part of centre’s mandate
Involvement of and effective collaboration with community professionals
Organizational support within the centre: • Centre staff support each other • Consideration given to staff needs, planning time, consultation • Priority given to maintaining positive relationships with parents
Director is a leader • effective in promoting on-going learning and collaboration
Effective infrastructure is in place • physical environment is accessible • financial and human resources allocated to support inclusion, adapt curriculum
Director and staff have positive attitudes toward inclusion
Figure 10.1
A Virtuous Cycle That Supports Effective Inclusion

CHAPTER 10 SUMMARY, INTEGRATION, AND CONCLUSIONS 163
On the other hand, centre staff,and particularly centre directorswho, while still committed to inclu-sion in principle, described them-selves as less committed person-ally and/or less accepting of abroader range of children with spe-cial needs in their centre, oftendescribed a negative or DISCOUR-AGING CYCLE of experiences.
In these situations, lack of, or re-ductions in, financial and humanresources available to the centre tosupport their efforts with inclusion;administrative barriers and diffi-culties related to subsidies andtheir allocations, and reductions inthe base level of support for childcare quality generally that was ex-perienced by many centres as aresult of limited or regressive policy
changes, were constructing situa-tions in which further or even on-going efforts to include childrenwith special needs were seen asunsustainable. (See Figure 10.2.)
While resources are always finite,centre directors who were less ac-cepting of a broader range of chil-dren with special needs being in-cluded in their programs and whowere starting to be less committed,as well as some directors who de-scribed their centres as not havingbecome more successful in inte-grating children with special needsin the last few years, saw their re-sponses as realistic and perfectlyjustified on two bases. These were:1) their concern that children withspecial needs and other childrenwould be ill-served by having them
A
B
C D
E
Centre faces challenges in maintaining high quality program
Limited staff education and training re: inclusion
Limited staff/director experience
DIFFICULTEXPERIENCES
WITH INCLUSION
NEGATIVE EFFECTS ONCHILDREN, PARENTS,
STAFF ANDCENTRE
F
H
IJ
Policy goals and centre resourcesthat jeopardize the quality of
child care services andeffective inclusion
Staff and director may make heroic efforts, but without adequate supports
Difficult experiences lead to stress and discouragement for staffLess committed to inclusion in this centre; Much more cautious about range of children that might be included, if any.
Involvement with community professionals is limited or is unreliable
Organizational capacity within the centre is limited: • Staff have their hands full as is • Director cannot provide additional time for planning and/or consultation
Director is not willing or is not able to provide leadership, create momentum, find additional resources, motivate staff or board members
No infrastructure to support inclusion • physical environment is not accessible • financial and human resources to support inclusion are not available or are very limited
Director and/or staff have ambivalent attitudes toward inclusion
G Relationships with parents may be difficult – lack of coordination between centre and parents
KWeakened commitment to having inclusion as part of centre’s mandate and identity
Figure 10.2
A Discouraging Cycle That Jeopardizes or Defeats Effective Inclusion

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada164
in situations in which their needscould not be met effectively, and 2)their concern for their staff and forsafeguarding the overall quality ofthe program.
In either case, these directors foundthemselves facing ethical dilemmasthat sometimes caused them tostart rethinking their beliefs aboutinclusion as an appropriate goaland expectation for underfundedcommunity-based programs, giventhe scarcity of resources. We be-lieve this is exactly what explainsthe divergence of responses ob-tained to one of the six general be-lief statements about inclusion.When asked to respond to thestatement, “It would be better tohave some child care programsaccept children with special needs(with specialized resources) thantry to have all child care programsbe inclusive,” 40.2% of centredirectors agreed or strongly agreed,41.7% disagreed or stronglydisagreed, and 18.1% said theywere uncertain.6 This response wasin sharp contrast to the pattern ofresponses that was strongly pro-inclusive on most other statements.A split of a somewhat less severemagnitude was also evident amongfront-line staff, especially theECEs.
10.5 CONCLUSIONS
Our study is one of very few inCanada that has addressed issuesrelated to including children withspecial needs in child care centres.In addition, it is also somewhatunique in being able to capture andjuxtapose the experiences andviews of several groups: front-lineearly childhood educators, morespecialized centre staff who serveas in-house resource teachers/support workers, centre directors,
and travelling resource consult-ants. Our sample is also quiteunique in that we purposefully se-lected centres and child care pro-fessionals, most of whom had con-siderable experience with inclusionand who could share their reflec-tions with us on how their experi-ences with children with specialneeds had affected them, as wellas their program’s capacities tosustain effective inclusion effortsover time.
These child care professionals havecontributed valuable insights andobservations that have provided acoherent picture of the critical ele-ments needed to develop and sus-tain effective inclusion in Canadianchild care programs. On the whole,our findings confirm and extendthe published research on inclusiveearly childhood programs, which islargely in the American context.They point to obvious recommen-dations for policy makers, facultiesin post-secondary educational pro-grams in ECE and related areas,disability rights advocates, and thechild care field. Most importantly,we believe that our findings identifytwo major issues that must beaddressed if effective inclusivepractice is to become and remaina reality across Canada.
10.51 Revisiting Our Definition of,and Expectations for, InclusiveChild Care
The first major issue, which takesus back full circle to the beginningof this report, is the need for clearexpectations about what effectiveinclusion is supposesd to look likeand what purposes it is intendedto achieve. If inclusion is reallybased on principles of social jus-tice and equality that affirm therights of all children to accessible,

CHAPTER 10 SUMMARY, INTEGRATION, AND CONCLUSIONS 165
developmentally appropriate earlychildhood education and care incommunity-based settings, and abelief that such experiences areimportant for early child develop-ment and family support, then re-sources must be allocated to en-sure that the programs are acces-sible and developmentally appro-priate. A right to early childhoodcare and education, like a right topublic education, would not meanthat all children would be servedin the same way. For example, achild recovering from chemo-therapy would require a period ofin-home child care; a child who ishighly self-injurious might requireshort-term, full-time clinical care.But, in all cases, there would be aright to care.
The matter of how resources willbe made available to ensure thatparents have choices, and that cen-tres and staff have adequate train-ing and the resources they need toaccept children in their program,and provide some degree oftherapeutic support to achievepositive developmental outcomes,remains unspecified. Without thepolicy development that is neededto truly deliver integrated children’sservices, and in a period of contin-ued underfunding for child care,inclusive child care is likely to con-tinue to be hit and miss, variableacross and within jurisdictions,and sustainable only to the degreethat dedicated individuals continueto be committed to inclusion as aprinciple they believe in.
10.52 The Relationship BetweenEffective Inclusion and HighQuality Child Care
The second major issue that thisstudy raises is the relationship be-tween successful and sustained
efforts to effectively include childrenwith special needs and the need to sup-port high quality programs and policydevelopment. It is abundantly clearfrom our research findings and fromsome of the other recent research oninclusion that whether one views ef-fective inclusion as built on top of, andrequiring a solid foundation of qualitychild care (i.e., an optional but possibleadd-on to high quality programs) or asa more recently recognized dimensionof high quality child care centres andsystems, the two concepts are inextri-cably linked.7
Based on the responses of centre staff,directors, and travelling resource con-sultants in this study, an effective sys-tem of inclusive child care will seldomoccur and certainly cannot be sus-tained in the context of an unstable,poorly trained and poorly paid childcare workforce, whose work is not val-ued. It can and does occur in centresthat have more stable funding; addi-tional resources; and trained, stableand committed staff who continue toinvest in their own professional devel-opment and who embrace a strongcode of ethics.
It requires directors who are experi-enced both as human resource man-agers and as leaders who have the skillsto support collaborative, coordinatedworking relationships with parents andwith community-based professionalson behalf of the children in theirprograms.
Most of all, we believe that at this pointin history, it requires strong leadershipat the policy level to provide the re-sources that are required to have anational system of early childhood pro-grams that are funded to provide highquality care and education for all ofCanada’s children and to achieve thegoals of healthy child development andstrong cohesion that Canadians value.This, indeed, is A Matter of Urgency!

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada166
END NOTES
1 Irwin, S.H. (1992). Integration of children with disabilities into daycare and afterschool caresystems. Ottawa: National Welfare Grants, Disabled Persons Unit, Health and Welfare Canada.
2 Peck, C.A., Hayden, L., Wandschneider, M., Peterson, K. & Richarz, S. (1989). Development ofintegrated preschools: A qualitative inquiry into sources of resistance among parents, adminis-trators, and teachers. Journal of Early Intervention, 13(4), 353-364. See also, Peck, C.A., Carlson,P., Helmstetter, E. (1992). Parent and teacher perceptions of outcomes for typically developingchildren enrolled in integrated early childhood programs: A statewide survey. Journal of EarlyIntervention, 16(1), 353-364.
3 Such a code of ethics has been developed by the Canadian Child Care Federation. See Cana-dian Child Care Federation (2000). Partners in quality: Tools for practitioners in child care set-tings — code of ethics, 18-20. ON: Author.
4 Stoiber, K.A., Gettinger, M. & Goetz, D. (1998). Exploring factors influencing parents’ andearly childhood practitioners’ beliefs about inclusion. Early Childhood Research Quarterly, 13(1),107-124.
5 Doherty, G., Lero, D.S., Goelman, H., LaGrange, A. & Tougas, J. (2000). You Bet I Care! ACanada-wide study on wages, working conditions and practices in child care centres. Guelph:University of Guelph (Centre for Families, Work and Well-Being).
6 This response was provided more often by directors of specialized programs. When a limitednumber of centres include children either by design or default, their capacity to serve the fullpopulation of children who might benefit is limited, as is the capacity of community-basedcentres which lack the resources or supports to include some of those children.
7 Harms, T., Clifford, R.M. & Cryer, D. (1998), Early childhood environment rating scale, revisededition (ECERS-R). New York: Teachers College Press, Columbia University.

CHAPTER 11 RECOMMENDATIONS 167
11.11.1 INTRODUCTION
High quality child care and otherearly childhood development pro-grams1 have positive benefits forchildren with special needs, fortheir parents, for other children, forchild care staff, and for the com-munity. However, the participationof children with special needs islimited by a number of factors,some that are general to child careand others that are specific to theinclusion of children with specialneeds.
General conditions affecting childcare services that work against ef-fective inclusion include chronicunder-funding and unstable finan-cial resources, limited formal train-ing of child care staff, high levelsof staff turnover, low wages, a lim-ited supply of licensed spaces, andother factors that impede the over-all quality of the service.2 Address-ing these barriers requires addi-tional public investment to improvethe supply and quality of earlychildhood programs, as recom-mended in a number of major re-search studies and policy analyses.3
Based on findings in A Matter ofUrgency and as summarized in theliterature review in Chapter 3, weidentify two types of barriers thatare specific to inclusion. The hu-man resources barriers include
lack of additional early childhoodeducators and resource teacherswith specialized training to supple-ment existing program staff andameliorate the additional workload,and inadequate or limited accesson the part of early childhood pro-grams to specialists who can workin partnership with them to ad-dress children’s and families’unique needs. The financial andphysical resource barriers includereduced or limited funding to sup-port inclusion, both in the form offee subsidies to parents and addi-tional dollars allocated directly tocentres; and inadequate resourcesfor structural modifications, addi-tional equipment, and technicaltraining and assistance to supportinclusion efforts.
Attitudinal barriers on the part ofstaff, evidenced by resistance toinclusion and unwillingness to in-clude children with special needs,while very prominent in the re-search literature, did not emergeas major barriers in this Canadiansample of centres that had prior orongoing experience with inclusion.Negative or resistant attitudes,when evident in this study, werespecific to situations in which cen-tres were or would be under-resourced, placing them in the dif-ficult situation of not being able tomeet children’s needs effectively
RECOMMENDATIONS
Sharon Hope Irwin, Donna S. Lero, Kathleen Brophy

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada168
that these children have a right toquality early childhood educationand care that contributes to theirdevelopment and well-being. Butvoluntary inclusion efforts appearto have gone about as far as theycan go, without clear directives inlegislation and public policy andsubstantial public funding andsupport.
Given the recently signed federal/provincial/territorial Early Child-hood Development Agreement4
which provides a framework forpolicies and actions, plus the pub-lic commitments some provincialgovernments have already madetoward inclusion,we recommendthe following:
1. That federal, provincial andterritorial, and municipal gov-ernments make specific publiccommitments to ensure the eq-uitable inclusion of children withspecial needs in all child careprograms and other Early Child-hood Development services thatreceive any public funding orpreferential tax treatment.
2. That federal, provincial andterritorial governments developand implement policy frame-works and adequate funding pro-grams related to the inclusion ofchildren with special needs andtheir families with goals, targets,timetables and follow-up mecha-nisms that can be used to assessprogress. Sufficient funding must beallocated to cover the additional costsof extra staffing, training, equipment,structural modifications, and relatedservices that make the inclusion com-mitment achievable and ensure eq-uitable access to services for all chil-dren with special needs. These invest-ments must be put in place as partof base budgeting for children’sprograms, with amounts increasing
without causing undue stress forstaff and compromising the qual-ity of the program for other chil-dren. Limited or reduced resourcesto support inclusion efforts andless than successful experiencesthat occurred under such circum-stances were most often the pivotpoints that affected teachers’ anddirectors’ attitudes towards inclu-sion. The lack of clear, pro-active,pro-inclusion policies and appro-priate supports is the context inwhich most of these barriers reside.
11.2 RECOMMENDATIONS
The following 22 recommendationsare organized under two categories:Legislation, Policy Developmentand Funding; and Capacity-Build-ing, and these, in turn, are organ-ized into eight major areas.
11.21 A Focus on Legislation, Policy Development and Funding
While A Matter of Urgency identi-fies many tasks for post-secondaryEarly Childhood Education train-ing programs, the child care field,researchers, and advocacy organi-zations, we believe that the primaryresponsibility for ensuring thatchild care programs across Canadahave the resources they need toserve all children in the commu-nity — especially children with dif-ferent abilities — lies with all threelevels of government: the federalgovernment, provincial and terri-torial governments, and local andmunicipal governments, particu-larly those with service planningand monitoring responsibilities.This study and others have dem-onstrated the heroic measures thatstaff in child care programs havetaken to include children withspecial needs because they believe

CHAPTER 11 RECOMMENDATIONS 169
with the annual rate of inflation andmaintained over time, in keeping withcomprehensive service planning atboth the provincial/territorial andlocal levels. While foundations, pri-vate sector contributions, and chari-table donations may assist in theseareas, we believe that sufficient fund-ing to ensure effective inclusion mustbe assured by governments as a mat-ter of principle, in keeping with otherpublic policies designed to ensureequity, create opportunities to de-velop skills and enhance well-being,and promote the full inclusion of in-dividuals with disabilities in commu-nity life.
3. That federal, provincial andterritorial governments ensurethat early childhood develop-ment services (child care centresand family child care homes, pre-schools, resource centres, etc.)are of sufficient quality to pro-vide a base on which to buildfully inclusive services.
11.22 A Focus on Capacity-Building
A Matter of Urgency makes clear thecommitment and willingness ofchild care directors and front-linestaff to include children with spe-cial needs. It also makes clear thelimits that insufficient funding, re-sources, training, and staffing cre-ate in even the most committedstaff. Our non-governmental rec-ommendations focus on “capacity-building” — meaning, in this case,the expansion of this sector’s abil-ity to move toward full inclusion ofchildren with special needs.
This study highlights the importantleadership role that directors havein inclusive child care centres, andthe contributions that experienceand additional training make toincreased commitment and compe-
tence in front-line child care staff.While the growth of commitmentand capacity to include childrenwith special needs occurred overmany years in the centres in ourselected sample, today it is impor-tant to “jump-start” the inclusionprocess in centres that are cur-rently non-inclusive, and to ad-dress those difficulties that havesurfaced in centres that are strug-gling to include children with spe-cial needs.
The following recommendations aregrouped under the topics of edu-cation and training, ongoing learn-ing opportunities, child care prac-tices, research, and informationand public education. Variousstakeholders should be involved ineach area in order to draw on theircollective expertise and resources.Such stakeholders would includeuniversity and college instructors;centre directors, early childhoodeducators and resource teachers;child care consultants, relatedhealth professionals, researchers,advocates; and especially parents.Moreover, we recommend that eachprovince/territory designate across-sectoral working group ashaving primary responsibility forworking with government to ensurethat specific steps are taken in acoordinated fashion at multiple lev-els (in communities and across theprovince/territory). This workinggroup should have a clear mandateand terms of reference and be re-sponsible for developing a pro-ac-tive approach, with regular reportsmade to a designated Minister andto the public.
Education and Training
According to the 1998 Child CareSector Study, only 15% of earlychildhood education (ECE) certifi-

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada170
cate programs and 66% of ECE di-ploma programs included eitherspecified courses or an infused ap-proach related to the inclusion ofchildren with special needs. In afully inclusive child care system, allstaff would have at least a baselevel of education and training toprepare them to work effectivelywith children with special needswithin a regular child care environ-ment. Some teaching staff wouldhave additional training. Thesestaff (sometimes referred to as re-source teachers or supported childcare workers) may have more re-sponsibility for working directlywith children with more challeng-ing conditions, and for serving asa resource to other staff in the cen-tre. All directors and supervisorswould have additional trainingcommensurate with their roles andresponsibilities for supportingteaching staff within the program,facilitating program modificationswhen needed, supporting andworking in partnership with par-ents of children with special needs,and collaborating with other pro-fessionals.
To reach these goals, we recom-mend:
4. That all pre-service EarlyChildhood Education certificate,diploma, and degree programsand those in related fields in-clude course work on inclusiveprinciples and practices. Ideally,topics related to the inclusion of chil-dren with special needs should beinfused (or embedded) in all ECEcourses.
5. That all post-basic Early Child-hood Education certificate, di-ploma and degree programs bedesigned to reference “inclusion”as a basic principle. Whether anearly childhood professional is pur-
suing advanced training to be a re-source teacher, or whether she is in-terested in more general knowledgeabout early childhood development,the course work should presupposethat she will work with children andfamilies in an inclusive setting.
6. That specialized training fordirectors and supervisors, usu-ally offered in certificate pro-grams at the post-basic level,presuppose inclusive settings,and address the multiple, impor-tant roles directors have in pro-moting effective inclusion. Edu-cational opportunities for directorsshould specifically address thedirector’s overall role in promotinginclusion and include those topicsthat directors have identified as im-portant for them. (See Chapter 8.)Opportunities for shared learningamong directors already in the field,including those with considerableexperience with inclusion, should bedeveloped and sustained.
7. That field experiences (practica)in Early Childhood Educationtraining programs include sub-stantial opportunities for expe-rience in successful inclusivesettings. Learning opportunities insupport of inclusion should be a re-quired part of every program, espe-cially those (such as student place-ments and practica and mentoringprograms) that can also provide newinformation and support to those al-ready in the field.
Ongoing Learning Opportunities forPractitioners
In addition to formal education andtraining programs, there is a needfor ongoing learning and supportfor staff already working in childcare and other ECD programs.
To reach this goal, we recommend:

CHAPTER 11 RECOMMENDATIONS 171
8. That faculty in post-secondaryinstitutions work collaborativelywith child care organizations andleaders in the field to develop ap-propriate continuing educationopportunities and in-service andmentoring programs to address theongoing learning and supportneeds of all child care staff to pro-mote inclusion in all child careprograms and other ECD programs.
9. That in-service training andworkshops on inclusion issuesand strategies be developed tomeet the needs of staff with awide range of experience in thefield and various levels of formaltraining. Training and ongoing learn-ing supports must be made availableon a continuous, affordable and ac-cessible basis across the country.
10. That mini-courses and full-dayworkshops on critical topics in in-clusion be offered as part of pro-vincial Early Childhood confer-ences and be financially supported,providing bursaries or subsidiza-tion to participants who would oth-erwise be unable to attend.
Child Care Practices
In A Matter of Urgency, the leader-ship skills of directors were identi-fied as one of the most importantelements that distinguished highlyeffective centres from those thatwere struggling with inclusion. Incooperation with governments (forfunding) and with universities, col-leges, consultants, and child careorganizations (for planning andmonitoring), centres and directorsidentified as highly effective at in-clusion should be enabled to serveas “promising practice” examplesand be directly involved in provid-ing advice and training in leader-
ship on inclusion. Efforts to pro-mote and improve inclusive prac-tice should build on the positive ex-periences and practice wisdom evi-dent in successful programs andthe understanding many parents,professionals and communitygroups have developed over time.Leadership training, networking,information sharing and the devel-opment of materials (such as vid-eos and electronic learning fora)should build on existing expertiseand reinforce successful efforts.
To meet these goals, we recom-mend:
11. That initiatives be developedto involve directors and front-line staff of successful inclusiveprograms as key change agentsto help lead the child care fieldtoward full inclusion. These initia-tives would include such activities asleadership training institutes, net-working opportunities on inclusionissues, a mentorship program for in-clusion, a field-based speakers’ bu-reau on inclusion, skill-buildingworkshops for successful practitio-ners to become trainers, and intern-ships for potential inclusion leaders.
12. That partnerships, collabora-tive activities, cross-disciplinarytraining, and information-shar-ing between child care organiza-tions and advocacy organizationsfor the disabled be supported todevelop key resources for par-ents, child care programs andother ECD services, health andsocial service professionals, andcommunity organizations. Thesepartnerships should be used to en-sure that resources are used as ef-fectively as possible and as a force topromote responsive programs andservices.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada172
13. That existing levels of inclu-sion in child care programs besustained and built upon. Manyregular Canadian child care pro-grams have gone part of the way tofull inclusion; many formerly special-ized programs now include some typi-cally developing children. It is impor-tant to be positive about the stepsthese programs have taken and toencourage their development towardfully inclusive child care. Awarenessand planning materials should bedesigned to aid in this process. Suc-cesses should be publicized and cel-ebrated, and both successful andfrustrating experiences should beused as a basis for information-shar-ing within the child care community.
14. That the role of parents ofchildren with special needs asinclusion advocates, supportersand experts be acknowledged andstrengthened. Their successes inadvocating for inclusive child careand other early childhood develop-ment programs should be highlightedin presentations, and print and videoproducts. Parents should be presentas key reviewers, consultants andtrainers in inclusive child care ini-tiatives. Their involvement should becompensated, and arrangementsmade so that their children’s needsare considered when activities requiretheir time, energy and travel awayfrom home.
15. That provincial and nationalnetworks of inclusive child careprograms be supported to shareinformation and resources andidentify other unmet needs.
Research
There is a need for ongoing re-search related to the inclusion ofchildren with special needs in arange of programs, and for under-
standing how inclusion supportschildren’s development, familywell-being, and community serviceprovision. Currently there are noprovisions in any jurisdiction forongoing data collection related tothe inclusion of children with spe-cial needs in child care and relatedprograms for benchmarking andplanning purposes, and to assessnew ways that inclusion can andshould be supported.
There are only a handful of re-searchers who are studying inclu-sion in child care and other earlychildhood development programsin Canada, and funding for thiskind of research has been incon-sistent and limited. Two recent de-velopments — the federal/provin-cial/territorial agreement on aframework for funding Early Child-hood Development Services withaccountability measures built in,and the funding of complementaryCentres of Excellence — have thepotential to help promote and con-solidate research in this area.However, the need for stableongoing, committed funding forapplied research on inclusionefforts, that can be used to helpguide and evaluate policies andpractices and to inform the field,remains. If Canadian research oninclusion is to continue, specificcommitted sources of funds will berequired — both to conduct theresearch and disseminate researchfindings, and to educate the nextgeneration of researchers inuniversity programs.
Information about the extent of in-clusion, provincial/territorial poli-cies and funding to support inclu-sion, and centres’ experiences withinclusion should be collected, co-ordinated, and disseminated on aregular basis. Such information is

CHAPTER 11 RECOMMENDATIONS 173
important in order to assesswhether improvements are beingmade in the various areas identi-fied to date, and to determine whatare the most effective strategies tosupport inclusive practice. Devel-opment and demonstrationprojects on high-priority inclusiontopics should be supported and amechanism for the independentevaluation of the effectiveness ofthese projects/models should beestablished prior to dissemination.Support for replications and the ex-tension of demonstrably effectivemodels must also be provided.
With these goals in mind, we makethe following recommendations:
16. That research be undertakenon the effects of inclusive childcare, both for children with spe-cial needs and for typically de-veloping children. Research shouldalso address the linkages betweeneffective, inclusive services for chil-dren with special needs in child careprograms and other community-based initiatives designed to promotehealthy child development and sup-port parents. Research should befunded and undertaken to determinehow changes in child care-relatedpolicies, programs, and funding ap-proaches — including those intro-duced prior to and following the ECDServices Agreement — actually affectresources within communities,inclusion processes, and childrenwith special needs.
17. That funding for research,evaluation and innovation ontopics related to inclusion ofyoung children with specialneeds in child care be a sustainedhigh priority of governments. Itis important that such funding re-main, regardless of changes in gov-ernments, departments and pro-grams. Funding for Canadian re-
search, evaluation, and innovationabout inclusive child care programsand related ECD services should becontinued through vehicles such asthe F/P/T Early Childhood Develop-ment Agreement, Child Care Visions,Social Development Partnerships, theDisabled Persons Unit, and HealthCanada.
18. That funding for a panel ofsuccessful, innovative, and inclu-sive child care centres — one ineach region across Canada — beprovided to help strengthen theircapacity as demonstration andtraining sites for the field, andto help identify emerging re-search questions and practiceissues. A consortium, includingresearchers, health and programpractitioners, service organizations,and parents, would identify thecentres, based on objective criteriaand measures, a range of innovativepractices, and a regional, urban/rural/cultural/economic mix.
Information and Public Education
Currently, the extent to which chil-dren with special needs are in-cluded in or excluded from com-munity-based programs, and thechallenges and benefits of doing so,is largely an invisible topic. A com-mitment to promote the optimalhealth and well-being of all childrenin Canada requires awareness ofsome of the unique issues relatedto children with disabilities, includ-ing the extent to which services areappropriate and effective in includ-ing all children.
Consequently, we recommend:
19. That research findings re-lated to children with specialneeds and effective inclusionand best practices be widelydisseminated at no or low cost

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada174
to inform policy developmentand practice, and to promotepublic awareness.
20. That inserts in governmentmailings to the public, public ser-vice announcements, and gov-ernment promotional materialreinforce both the visual imagesand the language of inclusion re-lated to people with disabilitiesof all ages, including the veryyoung.
21. That high quality trainingmaterials and products related toinclusion, created under suchprograms as Child Care Visions,
the federal/British ColumbiaStrategic Initiatives Program,and university-based research, beupdated and made available at noor low cost for child care train-ing and to promote public aware-ness.
22. That newsletters, web sitesand other sources of informationabout children with special needsand about inclusion in child careand other early childhood devel-opment programs that can in-form multiple communities besupported, expanded andpromoted.
ENDNOTES
1 We use the phrases ”early childhood development services (ECD)” and “early childhood careand education services (ECCE)” interchangeably. Where we say “ child care” in this study, weare emphasizing “licensed, full-day, non-parental group settings” that provide care and educa-tion for children of infant, toddler and/or preschool age and/or after-school for children up toage twelve. Other ECD services such as nursery schools and preschools, family daycare set-tings, family resource centres and seasonal programs, were not included in our sample. How-ever, the general principles of inclusion would apply to them as well.
2 Doherty, G., Lero, D.S., Goelman, H., LaGrange, A. & Tougas, J. (2000). You Bet I Care! ACanada-wide study on wages, working conditions and practices in child care centres. Guelph:University of Guelph (Centre for Families, Work and Well-Being) website: http://uoguelph.ca/cfww; Goelman, H., Doherty, G., Lero, D.S., LaGrange, A. & Tougas, J. (2000). You Bet I Care!Caring and learning environments: Quality in child care centres across Canada. Guelph, ON:University of Guelph (Centre for Families, Work and Well-Being) website: http://uoguelph.ca/cfww; Kontos, S., Moore, D. & Giorgetti, K. (1998). The ecology of inclusion. Topics in EarlyChildhood Education, 18(1), 38-47; Buysee, V., Wesley, P.W., Bryant, D. & Gardner, D. (1999).Quality of early childhood programs in inclusive and noninclusive settings. Exceptional Children,65(3), 301-314.
3 Cleveland, G. & Krashinsky, M. (1998). The benefits and costs of good child care: The economicrationale for public investment in young children. Toronto: Childcare Resource and ResearchUnit, Centre for Urban and Community Studies, University of Toronto; Beach, J. & Bertrand, J.(1998). Our child care workforce: From recognition to remuneration: A human resource study ofchild care in Canada. Main report. Ottawa: The Child Care Sector Steering Committee; Goelman,H., Doherty, G., Lero, D.S., LaGrange, A. & Tougas, J. (2000). You Bet I Care! Caring andlearning environments: Quality in child care centres across Canada. Guelph, ON: University ofGuelph (Centre for Families, Work and Well-Being) website: http://uoguelph.ca/cfww; Kent, T.(1999). Social policy 2000: An agenda. ON: Caledon Institute of Social Policy. Website:www.caledoninst.org.
4 First Ministers (2000, September 11). First Ministers’ Meeting Communique on Early ChildhoodDevelopment. See full text at website http://www.scics.gc.ca/cinfo00/800038005 e. html.
REFERENCES 175
Allred, K.W., Briem, R., & Black, S.J. (1998). Collaboratively addressing needs of young chil-dren with disabilities. Young Children, 53(5), 32-36.
Americans with Disabilities Act (ADA), P.L. 101-336, (1990). Based on concepts of the Rehabili-tation Act of 1973, this law guarantees equal opportunity for individuals with disabilities inemployment, public accommodation, transportation, state and local government services, andtelecommunications. It specifically includes children of all ages, in group child care and familydaycare.
Bailey, D.B., McWilliam, R.A., Buysse, V. & Wesley, P. (1998). Inclusion in the context of com-peting values in early childhood education. Early Childhood Research Quarterly, 13(1), 27-47.
Bailey, D.B. & Winton, P. (1987). Stability and change in parents expectations aboutmainstreaming. Topics in Early Childhood Special Education, 7(1), 73-88.
Beach, J. & Bertrand, J. (1997). Our child care workforce: From recognition to remuneration:Innovative training programs in early childhood care and education: Selected case studies. Ot-tawa: Canadian Child Care Federation.
Beach, J., Bertrand, J. & Cleveland, G. (1998). Our child care workforce: From recognition toremuneration : A human resource study of child care in Canada. Main Report. Ottawa: The ChildCare Sector Study Steering Committee.
Berkowitz, E.D. (1995). Mr. Social Security: The life of Wilbur J. Cohen. Lawrence, KS: UniversityPress of Kansas.
Blacher, J. & Turnbull, A.P. (1982). Teacher and parent perspectives in selected social aspectsof preschool mainstreaming. Exceptional Children, 29(3), 191-199.
Blacher, J. & Turnbull, A.P. (1983). Are parents mainstreamed? A survey of parent interactionsin the mainstreamed preschool. Education and Training of the Mentally Retarded, 18(1), 10-16.
Bochner, S., Denholm, C.J. & Pieterse, M. (1990). Attitudes to integration in preschool: A com-parative study of preschool directors in Canada and Australia. Victoria, BC: University of Victoria,School of Child and Youth Care.
Bredekamp, S. & Copple, C. (eds.) (1997). Developmentally appropriate practice in early child-hood programs — revised edition. Washington, DC: National Association for the Education ofYoung Children.
Bricker, D.D. (1995). The challenge of inclusion. Journal of Early Intervention, 19(3), 179-194.
British Columbia Ministry for Children & Families (1996). Practice guidelines and proceduresfor supported child care (B.C. Benefits [Child Care] Act, section 1). BC: Author.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and de-sign. Cambridge: Harvard University Press.
Brophy, K., Hancock, S. & Otoo, M. (1993). The role of the resource teacher in child careprograms: An Ontario study. Early Child Development and Care, 84, 75-80.
REFERENCES

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada176
Brown v. Board of Education (1954). See Oyez Project at Northwestern University through http://oyez.nwu.edu/cases/cases.
Buysee, V., Wesley, P.W., Bryant, D. & Gardner, D. (1999). Quality of early childhood programsin inclusive and noninclusive settings. Exceptional Children, 65(3), 301-314.
Buysse, V., Wesley, P.W. & Keyes, L. (1998). Implementing early childhood inclusion: Barrierand support factors. Early Childhood Research Quarterly, 13(1), 169-184.
Canadian Association for Community Living (1999). Fair tax for families who have a child witha disability. ON: Author. See also, D.G. Duff (2000), Disability and the federal income tax act.ON: Williams Research,com Inc.
Canadian Child Care Federation) 2000). Partners in quality: Tools for practitioners in child caresettings — code of ethics. ON: Author.
Canadian Coalition on the Rights of Children (1999). The UN convention on the rights of thechild: How does Canada measure up? ON: Canadian Institute for Child Health.
Carta, J., Sainato, D. & Greenwood, C. (1988). Advances in the ecological assessment of class-rooms for young children with handicaps. In S.L. Odom, & M. Karnes (eds.), Early interventionfor infants & children with handicaps, 217-240. Baltimore: Paul H. Brookes.
Chandler, L.K. & Dahlquist, C.M. (1998/9). Integration in the preschool for children with mildor moderate disabilities. In M. Coutinho & A. Repp (eds.), Inclusion: The integration of studentswith disabilities, 206-235. USA: Wadsworth Publishing Company.
Chandler, L.K. & Dahlquist, C.M. (1999). The effects of team-based functional assessment onthe challenging and appropriate behaviour of children in preschool classrooms. In S.H. Irwin,(ed.), Challenging the challenging behaviours, 27-30. NS: Breton Books.
Childcare Resource and Research Unit (1999). Early childhood care and education in Canada:The provinces and territories. Toronto: Author, Centre for Urban and Community Studies, Uni-versity of Toronto.
Clark, K.B. (1993). Unfinished business: The toll of psychic violence. In Newsweek, January11, 1993, 38.
Cleveland, G. & Krashinsky, M. (1998). The benefits and costs of good child care: The economicrationale for public investment in young children. Toronto: Childcare Resource and ResearchUnit, Centre for Urban and Community Studies, University of Toronto.
Commission on Emotional and Learning Disorders in Children (CELDIC) (1970). One millionchildren. Canada: Leonard Crainford.
Coulman, L. (1999). Knowledge, attitudes, and experiences of resource teachers and resourceconsultants in inclusive child care centres in Ontario. Masters thesis. University of Guelph,Faculty of Graduate Studies.
Demchak, M. & Drinkwater, S. (1992). Preschoolers with severe disabilities: The case againstsegregation. Topics in Early Childhood Special Education, 11(4), 70-83.
Denholm, C.J. (1990). Attitudes of British Columbia directors of early childhood educationcentres towards the integration of handicapped children. British Columbia Journal of SpecialEducation, 14(1), 13-26.
Dinnebeil, L.S., McInerney, W., Fox, C. & Juchartz-Pendry, K. (1998). An analysis of the per-ceptions and characteristics of childcare personnel regarding inclusion of young children withspecial needs in community-based programs. Topics in Early Childhood Special Education, 18(2),118-128.
Division of Early Childhood (1993). DEC Position on Inclusion. Pittsburgh, PA: Author.
Doherty, G. (1998). Assessing quality in child care settings. Interaction, 12(1), 16-20. See alsoDoherty-Derkowski, G. (1994). Quality matters: Excellence in early childhood programs. ON:Addison-Wesley Publishers.
Doherty, G., Friendly, M. & Oloman, M. (1998). Women’s support, women’s work: Child care inan era of deficit reduction, devolution, downsizing and deregulation. ON: Status of Women Canada.(Website: http:www.swc-cfc-gc.ca/)

REFERENCES 177
Doherty, G., Lero, D.S., Goelman, H., LaGrange, A. & Tougas, J. (2000). You Bet I Care! A Canada-wide study on wages, working conditions and practices in child care centres. Guelph: University ofGuelph (Centre for Families, Work and Well-Being). (Website: http://uoguelph.ca/cfww)
Duff, D.G. (2000). Disability and the federal income tax act. ON: Williams Research.com Inc.
Eaton v. Brant County Board of Education (1997). See both P.R.de Massy, The Eaton case beforethe Supreme Court of Canada: A “constructive” reading of the decision, and C.S. Judd, TheEaton and Eldridge cases: Same but different? in entourage (10)3/4, (1997).
Early Childhood Educators of British Columbia (ECEBC) (1997). Children with nursing supportneeds: Recommended practices for the child care field. (2nd ed). BC: ECEBC. (T. Norton, author.)
Eiserman, W.D., Shisler, L., Healey, S. (1995). A community assessment of preschool providers’attitudes toward inclusion. Journal of Early Intervention, 19(2), 149-167.
Espinosa, L.M. (1997). Personal dimensions of leadership. In S.L. Kagan & B.T. Bowman (eds.),Leadership in early care and education, 97-102. Washington, DC: National Association for theEducation of Young Children.
Ferguson, E., McCormick, T., Singleton, C. & Soave, A. (1999). The partners in practice mentoringmodel: Reflection, caring, and sharing. Halifax: Partners in Practice.
First Ministers (2000, September 11). First Ministers’ Meeting Communique on Early ChildhoodDevelopment. See full text at website http://www.scics.gc.ca/cinfo00/800038005 e. html
Frankel, E.B. (1994). Resource teachers in integrated children’s centres: Implications for staffdevelopment. The International Journal of Early Childhood, 26(2), 13-20.
Frankel, E.B. & McKay, D. (1990). An interactive model of integration in community-basedchild care centres. Paper presented at the 68th Annual Convention, Council of ExceptionalChildren, Toronto, ON. ERIC Document #ED 334 774.
Friendly, M. (1994). Child care policy in Canada: Putting the pieces together. ON: Addison-WesleyPublishers Limited.
Friendly, M. & Oloman, M. (1998). Child care at the centre: Child care on the social, economicand policy agenda in the 1990s. In J. Pulkingham & G. Ternowetsky (eds.), Remaking Canadiansocial policy: Social security in the late 1990s, 273-285. Halifax, NS: Fernwood Publishing.
Garvar-Pinhas, A. & Schmelkin, L.P. (1989). Administrators’ and teachers’ attitudes towardmainstreaming. Remedial and Special Education, 10(4), 38-43.
Gemell-Crosby, S. & Hanzlik, J.R. (1994). Preschool teachers’ perceptions of including childrenwith disabilities. Mental Retardation and Developmental Disabilities, 29(4), 279-290.
Gettinger, M., Stoiber, K.C., Goetz, D. & Caspe, E. (1999). Competencies and training needs forearly childhood inclusion specialists. Teacher Education and Special Education, 22(1), 41-54.
Goelman, H., Doherty, G., Lero, D.S., LaGrange, A. & Tougas, J. (2000). You Bet I Care! Caringand learning environments: Quality in child care centres across Canada. Guelph, ON: Universityof Guelph (Centre for Families, Work and Well-Being). (Website: http://uoguelph.ca/cfww)
Goguen, L. & Poirier, D. (1995). Are the educational rights of exceptional students protected inCanada? In R. Ghosh & D. Ray, (eds.), Social change and education in Canada (3rd ed.), 310-322. Toronto: Harcourt Brace Canada.
Goss-Gilroy, Inc. (1996, November). Component D: Curriculum analysis. Child care sector study:Technical appendices (draft). (Unpublished report prepared for the Child Care Sector SteeringCommittee.)
Hanline, M. F. (1990). A consulting model for providing integration opportunities for preschoolchildren with disabilities. Journal of Early Intervention, 14(4), 360-366.
Harms, T. & Clifford, R.M. (1980). Early childhood environment rating scale (ECERS). New York:Teachers College Press, Columbia University.
Harms, T. & Clifford, R.M. & Cryer, D. (1998). Early childhood environment rating scale, revisededition (ECERS-R). New York: Teachers College Press, Columbia University.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada178
Helburn, S.W. (ed.) (1995). Cost, quality and child outcomes in child care centers. Denver, CO:University of Denver, Department of Economics, Centers for Research and Social Policy.
Hertzman, C. (1998). The contribution of early experience to health inequalities throughout thelife course. Plenary Session at the Early Years: Birth to School Age conference. Conferencesyllabus. BC: British Columbia Association of Infant Development Consultants.
Heston, M.L., Raschke, D., Kliewer, C., Fitzgerald, L.M. & Edmiaston, R. (1998). Transformingteacher preparation in early childhood education: Moving to inclusion. Teacher Education andSpecial Education, 21(4), 278-292.
Human Resources Development Canada (1997). The status of daycare in Canada, 1995 and1996. Ottawa: Minister of Supply and Services. Cat. H74-14/1996E.
Hundert, J., Mahoney, B., Mundy, F., Vernon, M.L. (1994). Predictors of gains of children withdisabilities in specialized and community early childhood settings. Ottawa: Child Care InitiativesFund (Submission to the Department of National Health and Welfare, Social Service Branch).Summary by K.C. Ryerse in Focus (Sept. 1995), 7-1l, the supplementary volume of the 7-partserial publication of the Canadian Child Care Federation.
Hutchinson, N.L. & Schmidt, C. (1996). Perceptions of a resource teacher about programs forpreschoolers with special needs and their families. Canadian Journal of Research in Early Child-hood Education, 5(1), 73-82.
In Unison, a 1998 agreement of f/p/t governments (except for Québec), provides a blueprint forpolicy development to the area of disability. It makes an intergovernmental commitment to fullcitizenship of people with disabilities and identifies three building blocks to guide policy devel-opment — disability supports, income supports and employment supports.
Individuals with Disabilities Educaton Act (IDEA), P.L. 101-476, (1990), updating 94-142 (1975)which mandated free and appropriate educational services in the least restrictive environmentto individuals 3-21, mandated transition services and assistive technology services to be in-cluded in a child’s or youth’s IEP, and added autism and traumatic brain injury to the list ofcategories of children and youth eligible for special education and related services. Part II refersto services for children 0-3 and their families.
Irwin, S.H. (1991). “Trach” – It rhymes with “Snake”. InThe SpeciaLink book (1993). NS: Breton Books.
Irwin, S.H. (1992). Increasing enrollment of preschool children with special needs in regular daycareprograms through a peer-coaching, systems change approach. ERIC document.
Irwin, S.H. (1992). Integration of children with special needs into daycare and after-school pro-grams. Ottawa: Disabled Persons Unit, Health and Welfare Canada. (Available from SpeciaLink).
Irwin, S.H. (1993). The seamless day. In The SpeciaLink book (1993), 7. NS: Breton Books.
Irwin, S.H. (1993). The SpeciaLink book. NS: Breton Books.
Irwin, S.H. (1994). Toward a federal role for inclusion of children with special needs in Canadianchild care programs: Report to the Standing Committee on Human Resources Development. Asupplementary paper. (Available from SpeciaLink.)
Irwin, S.H. (1995). Inclusive child care in Canada: Advances at risk. In As if children matter:Perspectives on children, rights and disability, 77-89. Toronto, ON: Roeher Institute.
Irwin, S.H. & DeRoche, J. (1992). Attitudes of Canadian mainstream child care staff towardinclusion of children with special needs. (Unpublished manuscript.)
Irwin, S.H. & Lero, D.S. (1997). In our way: Child care barriers to full workforce participationexperienced by parents of children with special needs — and potential remedies. NS: BretonBooks. See also, Roeher Institute (2000), Finding a way in: Parents on social assistance withdisabled children. ON: Author.
Jocelyn, L.J., Casiro, O.G., Beattie, D., Bow, J. & Kneisz, J. (1998). Treatment of children withautism: A randomized controlled trial to evaluate a caregiver-based intervention program incommunity day-care centers. Developmental and Behavioral Pediatrics, 19(5), 326-334.
Johnson, K.M. & Johnson, J.E. (1993). Rejoinder to Carta, Atwater, Schwartz, and McConnell.Topics in Early Childhood Special Education, 13(3), 255-273.

REFERENCES 179
Johnson, L. (1998). Personal correspondence with author.
Johnson, L., Johnson, P., MacMillan, R. P. & Rogers, C. (1993). EC-SPEED: Early childhoodspecial education program design and evaluation guide. OH: The Ohio Department of Educationand the Northcentral Ohio Special Education Regional Resource Center.
Jorde-Bloom, P. (1997). Commentary. In S.L. Kagan & B.T. Bowman (eds.), Leadership in earlycare and education, 34-37. Washington, DC: National Education Association for the Educationof Young Children.
Jorde-Bloom, P. (2000). How do we define director competence? Child Care Information Ex-change, 3/00, 13-18.
Jorde-Bloom, P. (1992). The child care director: A critical component of program quality. Edu-cational Horizons (Spring), 138-145.
Jorde-Bloom, P. & Sheerer, M. (1992), Changing organizations by changing individuals. A modelof leadership training. The Urban Review, 24, 263-286.
Kagan, S.L. & Bowman, B.T. (1997). Leadership in early care and education. Washington, DC:National Association for the Education of Young Children.
Katz, L.G. (1995). The developmental stages of teachers. In L.G. Katz, Talks with teachers ofyoung children, 203-210. Norwood, NJ: Ablex Publishing Corporation.
Kent, T. (1999). Social policy 2000: An agenda. ON: Caledon Institute of Social Policy. Website:www.caledoninst.org.
Knoblauch, B. (1998, May). Rights and Responsibilities of Parents of Children with Disabilities.ERIC Digest, E567.
Kontos, S. & Diamond, K. (1997). Preparing practitioners to provide early intervention servicesin inclusive settings. In P. Winton, J. McCollum & C. Catlett (eds.), Reforming personnel prepa-ration in early intervention, 393-410. Baltimore: Paul H. Brookes.
Kontos, S. & File, N. (1993). Staff development in support of integration. In C.A. Peck, S.L.Odom & D.D. Bricker (eds.), Integrating young children with disabilities into community pro-grams: Ecological perspectives on research and implementation, 169-186. Baltimore: Paul H.Brookes.
Kontos, S., Moore, D. & Giorgetti, K. (1998). The ecology of inclusion. Topics in Early ChildhoodEducation, 18(1), 38-47.
Kwok, A. & Robinson, E. (1997). The partnership project. BC: Ministry for Children and Fami-lies, Province of British Columbia.
Lero, D.S., Pence, A.R., Shields, M., Brockman, L.M. & Goelman, H. (1992). Canadian nationalchild care study: Introductory report. Ottawa: Statistics Canada, Cat. No. 89-526E.
Lero, D.S., Doherty, G., Goelman, H., LaGrange, A. & Tougas, J. (2000). A profile of child carecentres across Canada. In You Bet I Care! A Canada-wide study on wages, working conditionsand practices in child care centres, Chapter 9, 111-124. Guelph: University of Guelph (Centrefor Familes, Work, and Well-Being).
McCain, M.N. & Mustard, J.F. (1999). Reversing the real brain drain: Early years study, finalreport. ON: Publications Ontario. (Website: www.childsec.gov.on.ca).
McCormack, C. (2000). Personal Communication. See, Special Needs Grants, Funding Guidelines,2000-2001. Early Childhood Services, Department of Health and Social Services, PE.
McCuaig, K. & Friendly, M. (1999). The Early Childhood Development triangle. Part of numer-ous presentations by McCuaig & Friendly. Unpublished.
McQuaig, L. (1993). The wealthy banker’s wife: The assault on equality in Canada. ON: PenguinBooks Canada.
Mill, D. & Romano-White, D. (1999). Correlates of affectionate and angry behaviour in childcareeducators of preschool-aged children. Early Childhood Research Quarterly, 14, 155-178.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada180
Mitchell, A. (1997). Reflections on early childhood leadership development: Finding your ownpath. In S.L. Kagan & B. Bowman (eds.), Leadership in early care and education. Washington:National Association for the Education of Young Children, 85-94. (Website: http:/www.naeyc.org/naeyc).
Munby, H. & Hutchinson, N. (1998). Using experience to prepare teachers for inclusive class-rooms: Teacher education and the epistemology of practice. Teacher Education and SpecialEducation, 21(2), 75-82.
National Council of Welfare (1999). Preschool children: Promises to keep. ON: Author.
National Network of Families (1999). Don’t exclude our children: Include all Canada’s children inthe National Children’s Agenda. Toronto: Canadian Association for Community Living.
Neugebauer, R. (1981, Sept/Oct). Piaget’s theory of director development. Child Care Informa-tion Exchange, 1-5.
New Brunswick (1994). New directions: Child care reforms. NB: Author
Norton, T. (1991). Exceptional health care, phase I: Centre and staff needs assessment. BritishColumbia: Fraser North Childcare Issues Society.
Nova Scotia (1994). Day care licensing manual discussion paper (draft).
Odom, S.L., Diamond, K.E. (1998). Inclusion of young children with special needs in earlychildhood education: The research base. Early Childhood Research Quarterly, 13(1), 3-25.
Odom, S.L. & McEvoy, M.S. (1990). Mainstreaming at the preschool level: Potential barriersand tasks for the field. Topics in Early Childhood Special Education, 10(2), 48-61.
Odom, S.L., Peck, C.A., Hanson, M., Beckman, P.J., Kaiser, A.P., Lieber, J., Brown, W.H., Horn,E.M. & Schwartz, I.S. (1996). Inclusion at the preschool level: An ecological systems analysis.In Inclusion of young children with disabilities. MI: Society for Research in Child Development,Social Policy Report, 10(2&3), 18-30.
Ontario Coalition for Better Child Care (1992). On the road to reform: The Ontario Coalition forBetter Child Care responds to: Setting the stage: A public consultation paper on child care reformin Ontario. ON: Author.
Ontario Legislative Assembly (1990). The Day Nurseries Act, Revised Statutes of Ontario (re-printed 1998). Amended by the Services Improvement Act, affective January 1, 1998. OntarioLegislative Assembly. Ontario Regulation 262, 1990 (Amended 1998, 1999).
Palsha, S.A. & Wesley, P.A. (1998). Improving quality in early childhood environments throughon-site consultation. Topics in Early Childhood Special Education, 18(4), 243-253.
Peck, C.A. (1993). Ecological perspectives on implementation of integrated early childhood pro-grams. In C.A. Peck, S.L. Odom, & D.D. Bricker, (eds.), Integrating young children with disabili-ties into community programs: Ecological perspectives on research and implementation, 3-15.Baltimore: Paul H. Brookes.
Peck, C.A., Carlson, P. & Helmstetter, E. (1992). Parent and teacher perceptions of outcomes fortypically developing children enrolled in integrated early childhood programs: A statewide sur-vey. Journal of Early Intervention, 16(1), 353-364.
Peck, C.A., Furman, G.C., Helmstetter, E. & Reed, D. (1991). Factors affecting the survival ofearly childhood mainstreaming programs: A retrospective study. Vancouver, WA: WashingtonState University, Department of Educational and Counseling Psychology. Published as Inte-grated early childhood programs: Research on the implementation of change in organizationalcontexts, chapter 10, in C.A. Peck, S.L. Odom & D.D. Bricker (1993), Integrating young childrenwith disabilities into community programs, 187-206. Baltimore: Paul H. Brookes.
Peck, C.A., Hayden, L., Wandschneider, M., Peterson, K. & Richarz, S. (1989). Development ofintegrated preschools: A qualitative inquiry into sources of resistance among parents, adminis-trators, and teachers. Journal of Early Intervention, 13(4), 353-364.
Peck, C.A., Killen, C.C. & Baumgart, D. (1989). Increasing implementation of special educationinstruction in mainstream preschools: Direct and generalized effects of nondirective consulta-tion. Journal of Applied Behaviour Analysis, 22(2), 197-210.

REFERENCES 181
Powell, D.R. & Dunn, L. (1990). Non-baccalaureate teacher education. In B. Spodek & O.N. Saracho(eds.), Yearbook in early childhood education, volume 1: Early childhood teacher preparation, 45-66. New York: Teachers College Press.
Rebick, J. (2000, April 9th). Plenary presentation to Child Care Resources Round Table Sympo-sium.
Reichart, D.C., Lynch, E.C., Anderson, B.C., Svobodny, L.A., Dicola, J.M. & Mercury, M.G. (1989).Parental perspectives on integrated preschool opportunities for children with handicaps and chil-dren without handicaps. Journal of Early Intervention, 13(1), 6-13.
Reid, K. (2000). Personal communication. See Minimum salary scale guideline for group childcare centres: Phase 2–2000 and Grants for children with disabilities (schedule C), (subsection37(3)), Child Day Care, Family Services and Housing, Manitoba.
Roeher Institute (2000). Finding a way in: Parents on social assistance with disabled children.Toronto, ON: Author.
Salisbury, C.L. (1990). The least restrictive environment: Understanding the options. Albuquerque:Council of Administrators of Special Education (CASE).
Salisbury, C.L. (1991). Mainstreaming during the early childhood years. Exceptional Children,58(2), 146-155.
Saskatchewan Social Services (1995). Child day care division: Child development program infor-mation (revised).
Scallan, P.C. (1987, Nov.). Teachers coaching teachers: Development from within. Childcare Infor-mation Exchange, 3-6.
Shanks, P.S. & Thompson, B. (1991). An overview of the rationale for integrating preschoolers withsevere disabilities into mainstream preschool/child care programs. Lawrence, KS: University ofKansas, Dept. of Special Education.
Sinclair, H. (2000). Personal communication.
Smith, B.J. & Rose, D. (1991). Identifying policy options for preschool mainstreaming. Albuquer-que: Council of Administrators of Special Education (CASE).
Smith, B.J. & Rose, D.F. (1994). Administrator’s policy handbook for preschool mainstreaming.Pittsburgh: Brookline Books — Administrative Issues in Education Series.
Smith, Dr. Jim (1993). Nova Scotia Minister of Community Services (Press release).
Special Needs Day Care Review Reference Committee for the Minister of Social Services (1993).Supported child care: The report of the special needs day care review in British Columbia. BC:Author.
SpeciaLink (1992). Autism in the mainstream — A team approach. One part of the 5-part video,The mainstream is the right stream. (Available from SpeciaLink.)
Standing Committee on Human Resources Development (1995). Canada: Security, opportunitiesand fairness: Canadians renewing their social programs. Ottawa: Canada Communication Group.
Statistics Canada (1991). Canada’s health and activity limitation survey. Ottawa: Statistics Canada.
Statistics Canada (1996-97). National population health survey. Ottawa: Statistics Canada.
Statistics Canada and the National Day Care Research Network. (1988). The 1988 National ChildCare Survey Information Manual. Ottawa: Statistics Canada.
Stoiber, K.A., Gettinger, M. & Goetz, D. (1998). Exploring factors influencing parents’ and early child-hood practitioners’ beliefs about inclusion. Early Childhood Research Quarterly, 13(1), 107-124.
Strain, P.S. (1989). Least restrictive environment (LRE) for children with handicaps: What weknow, and what we should be doing. Journal of Early Intervention, 14(4), 288-296.
Swan, W.W. (1980). The handicapped children’s early education program. Exceptional Children,47(1), 12-16.

A MATTER OF URGENCY: Including Children with Special Needs in Child Care in Canada182
Templeman, T.P., Fredericks, H.D.B. & Udell, T. (1989). Integration of children with moderateand severe handicaps into a daycare center. Journal of Early Intervention, 13(40), 315-328.
Torjman, S. (1999). Will the ‘children’s budget’ include kids with disabilities? ON: Caledon Insti-tute of Social Policy.
Turnbull, A.P. & Winton, P. (1983). A comparison of specialized and mainstreamed preschoolsfrom the perspective of parents of handicapped children. Journal of Pediatric Psychology, 8(1),57-71.
Van Raalte, D.L. (in process). Keeping the door open: Enhancing and maintaining the capacityof centres to include all children. For information, write to project coordinator at 310 MainStreet, Fredericton, NB E3A 1E4.
VanderVen, K. (1993). Military strategy and the economic base of child care: A radical proposalfor our future. (From the 1987 Albert E. Trieschman Memorial Conference.) Condensed versionin The SpeciaLink book, 69-86. NS: Breton Books. Full 19-page article available from SpeciaLink.
VanderVen, K. (1990). The relationship between notions of caregiving held by early childhoodpractitioners and stages of career development. In B. Po-King Chan (ed.), Early childhood to-ward the 21st century: A worldwide perspective, 245-255. Hong Kong and Gaithersberg, MD:Uyew Chung Education Publishing Company.
Vanier Institute (1994). Profiling Canada’s families. ON: Author.
Wien, C.A. (1995). Developmentally appropriate practice in “Real Life”. New York: Teachers Col-lege Press.
Zigler, E. & Valentine, J. (1997). Project Head Start: A legacy of the war on poverty (2nd Ed.),488-490. Washington, DC: National Head Start Association.