A Neurological change A Neurological change Is it PNS or CNS??? Is it PNS or CNS??? Aliza Ben Aliza Ben - - Zacharia, ANP Zacharia, ANP The Corinne Goldsmith Dickinson The Corinne Goldsmith Dickinson Center for Multiple Sclerosis Center for Multiple Sclerosis The Mount Sinai Medical Center The Mount Sinai Medical Center
Transcript
A Neurological change A Neurological change Is it PNS or CNS???Is it PNS or CNS???
Center for Multiple SclerosisCenter for Multiple SclerosisThe Mount Sinai Medical CenterThe Mount Sinai Medical Center
Localization of Neurological S/SLocalization of Neurological S/S
ObjectivesObjectivesDistinguish peripheral from central neurological Distinguish peripheral from central neurological complaintscomplaintsReview some of the differential for peripheral Review some of the differential for peripheral neuromuscular complaintsneuromuscular complaintsDiscuss a few etiologies for peripheral Discuss a few etiologies for peripheral neuromuscular complaints and their neuromuscular complaints and their management management
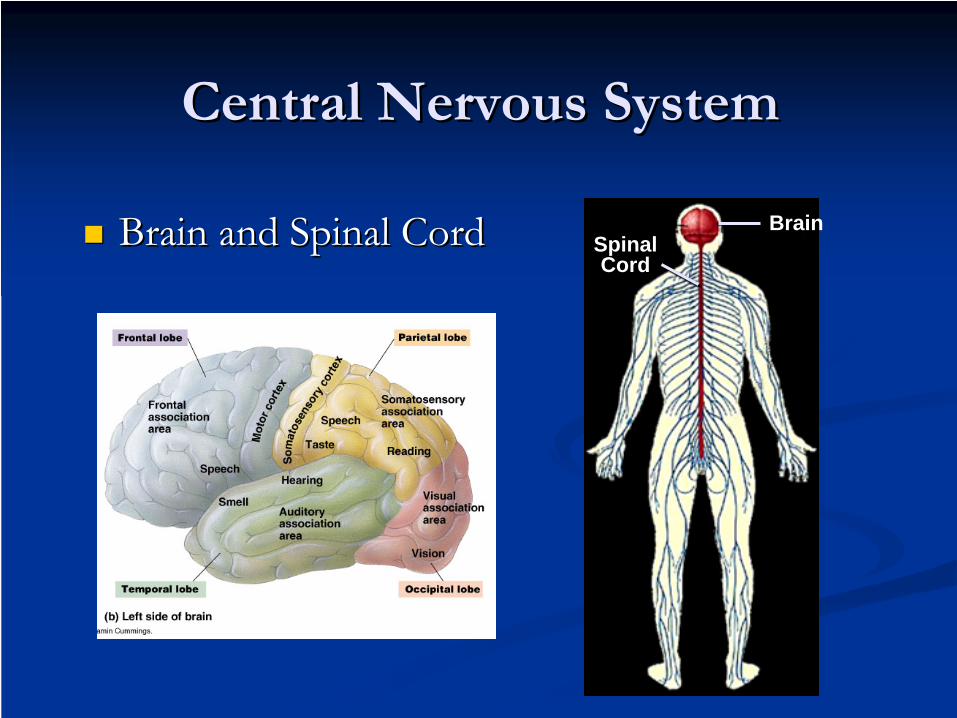
Central Nervous SystemCentral Nervous System
Brain and Spinal CordBrain and Spinal Cord SpinalCord
Brain
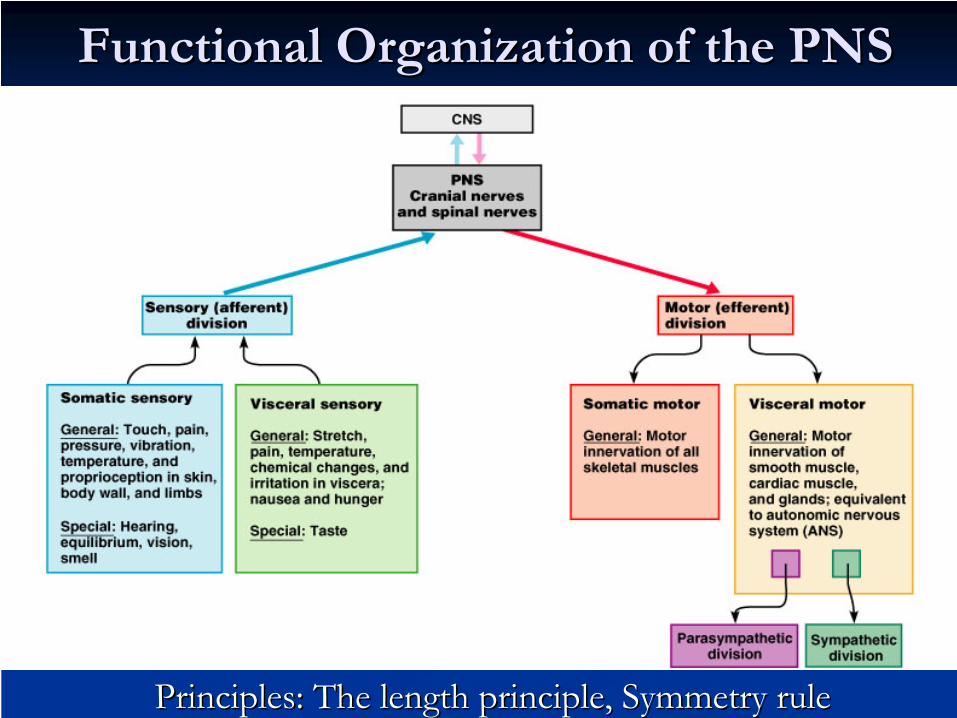
Functional Organization of the PNSFunctional Organization of the PNS
Principles: The length principle, Symmetry rulePrinciples: The length principle, Symmetry rule
Neurological AssessmentNeurological Assessment
Is it CNS or PNS?Is it CNS or PNS?If PNS If PNS –– is muscle or nerve?is muscle or nerve?If CNS If CNS –– lesion above or below the foramen lesion above or below the foramen magnum?magnum?If above foramen magnum If above foramen magnum –– is it above is it above tentorium cerebelli or below?tentorium cerebelli or below?If above tentorium If above tentorium –– R or L hemisphere R or L hemisphere –– gray gray matter or white matter?matter or white matter?Are multiple systems involved?Are multiple systems involved?
Localization of Signs/symptomsLocalization of Signs/symptomsNerve root Nerve root
Radiating pain corresponding to a nerve root distributionRadiating pain corresponding to a nerve root distributionNumbness or weakness in a nerve root Numbness or weakness in a nerve root Diminished reflexes (LMN signs) in territory of nerve rootDiminished reflexes (LMN signs) in territory of nerve root
Peripheral nervePeripheral nerveDistal paresthesias, sensory loss, or weaknessDistal paresthesias, sensory loss, or weaknessDiminished distal reflexesDiminished distal reflexes
Central Central Weakness or paralysis from Weakness or paralysis from the site of the lesion distallythe site of the lesion distallyUnilateral or bilateralUnilateral or bilateralUpper motor neuron signs Upper motor neuron signs are seen distally to the lesionare seen distally to the lesion
SpasticitySpasticityPositive BabinskiPositive BabinskiBrisk reflexesBrisk reflexesB & B involvementB & B involvement
Peripheral Peripheral
Paresis or paralysis of a Paresis or paralysis of a muscle or muscle group muscle or muscle group which they innervatewhich they innervatePeripheral lesions may be Peripheral lesions may be unilateral and limited in unilateral and limited in the degree of limb the degree of limb involvement or bilateral involvement or bilateral depending on the depending on the etiology (GBS)etiology (GBS)
Sensory Involvement Sensory Involvement
CentralCentralSpinal lesions are more Spinal lesions are more commonly bilateral, commonly bilateral, involve multiple involve multiple dermatomes and have a dermatomes and have a sensory level that is easily sensory level that is easily defineddefinedEnsure that you examine Ensure that you examine the dermatomes on the the dermatomes on the trunk as you may miss a trunk as you may miss a sensory levelsensory level
PeripheralPeripheralGenerally restricted, Generally restricted, expressed in a dermatomal expressed in a dermatomal distributiondistributionUsually have a sharp Usually have a sharp demarcation whereas demarcation whereas central lesions are more central lesions are more vague in their demarcationvague in their demarcationStockingStocking--glove distribution glove distribution is generally a peripheral is generally a peripheral neuropathyneuropathy
Bilateral SymptomsBilateral Symptoms
These may be peripheral or central (spinal cord)These may be peripheral or central (spinal cord)A definite sensory level means it is centralA definite sensory level means it is centralMotor loss R/T PNS disease tends to affect the Motor loss R/T PNS disease tends to affect the distal muscles of the legs more than the distal muscles of the legs more than the proximal ones except for certain varieties of proximal ones except for certain varieties of GBS & diabetic neuropathy GBS & diabetic neuropathy Associated autonomic dysfunction Associated autonomic dysfunction (incontinence) means central involvement(incontinence) means central involvementAssociated UMN signs means central Associated UMN signs means central
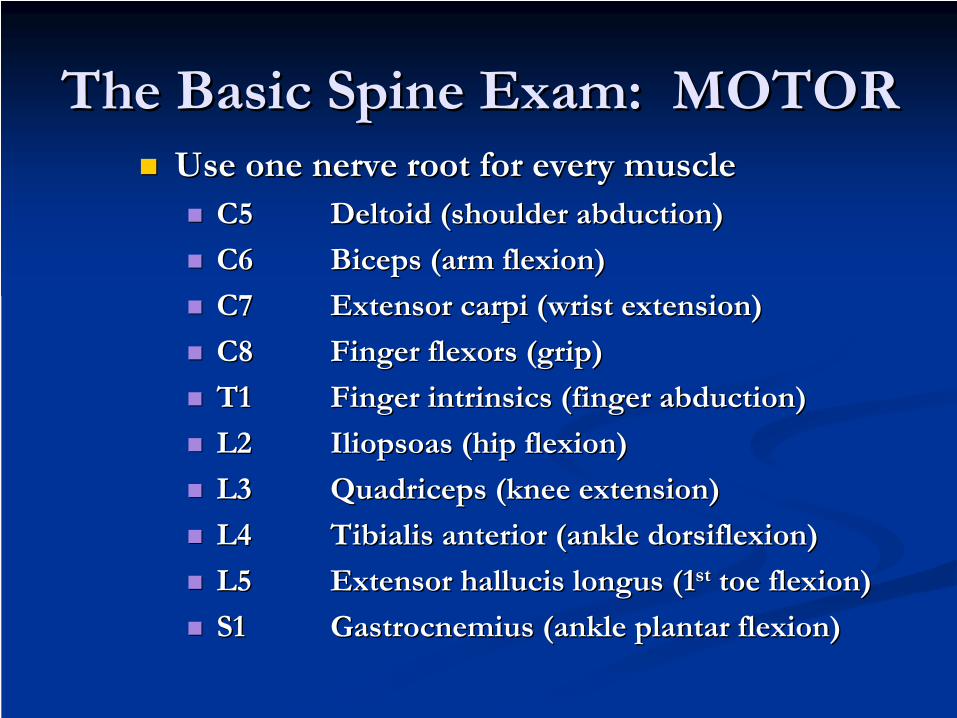
The Basic Spine Exam: MOTORThe Basic Spine Exam: MOTORUse one nerve root for every muscleUse one nerve root for every muscle
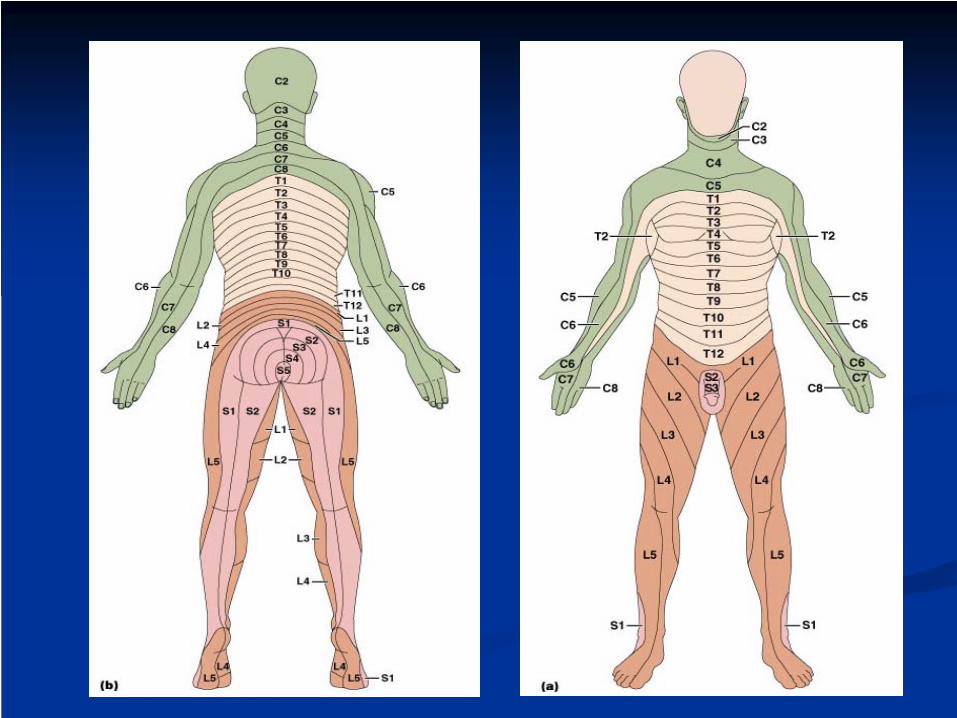
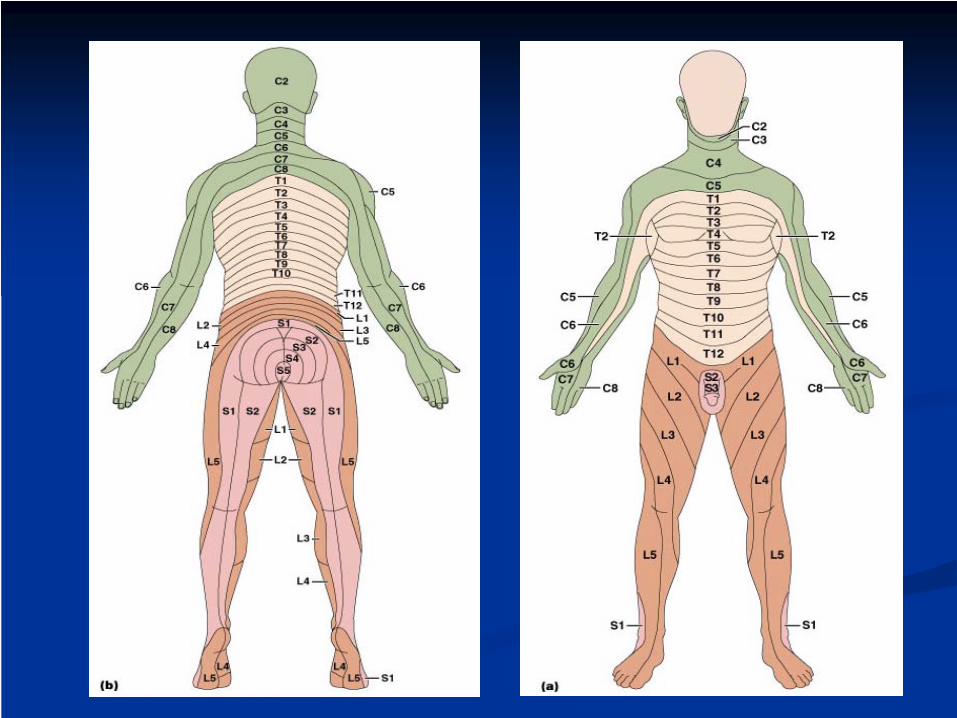
The Basic Spine Exam: The Basic Spine Exam: SENSORYSENSORY
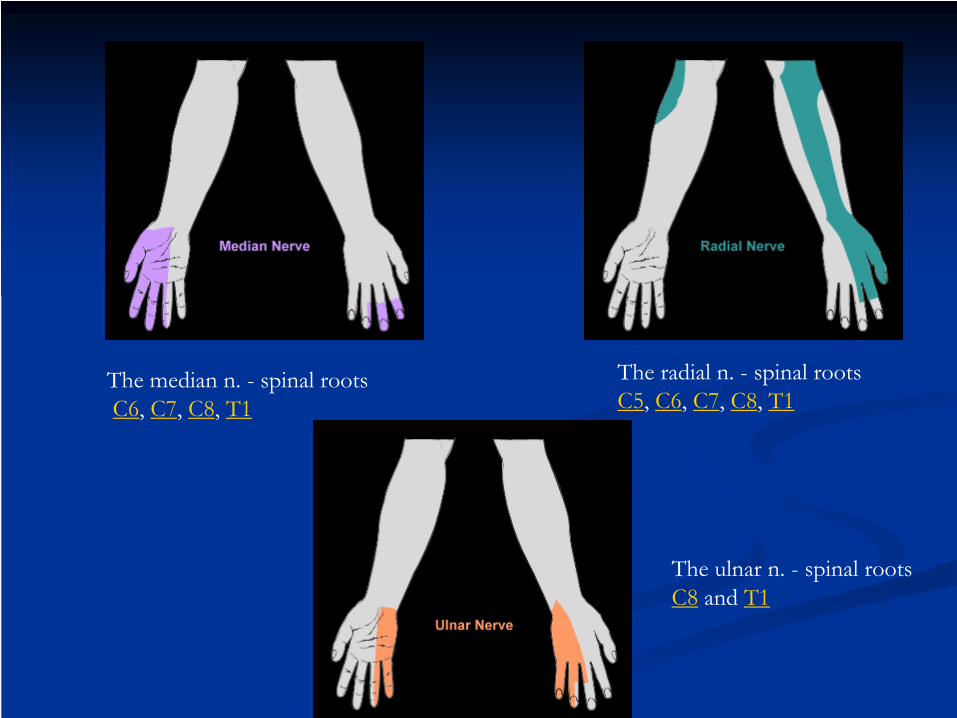
Use these key landmarksUse these key landmarksC6C6 11stst & 2& 2ndnd fingersfingers
C7C7 Middle fingerMiddle finger
C8C8 44thth & 5& 5thth fingersfingers
T4T4 NipplesNipples
T10T10 UmbilicusUmbilicus
L3L3 KneeKnee
L4L4 lateral dorsal portion of footlateral dorsal portion of foot
L5L5 Medial dorsal portion of footMedial dorsal portion of foot
S1S1 Plantar portion of footPlantar portion of foot
Deep Tendon ReflexesDeep Tendon Reflexes
The major deep tendon The major deep tendon reflexesreflexesBiceps Biceps –– C5C5--66Triceps Triceps –– C7C7--8 8 Patellar Patellar –– L3L3--44Achilles Achilles –– S1S1--22Planter reflex (babinski) Planter reflex (babinski) ––UMN process UMN process --dorsiflexion dorsiflexion of the big toe with fanning of the big toe with fanning out of the smaller toesout of the smaller toes
Symmetric hyporeflexia Symmetric hyporeflexia ––nonpathologic or metabolic nonpathologic or metabolic ds or peripheral neuropathyds or peripheral neuropathySymmetric Hyperreflexia Symmetric Hyperreflexia ––systemic systemic –– hypocalcemia or hypocalcemia or hyperthyroidismhyperthyroidismUnilateral hyperreflexia Unilateral hyperreflexia ––UMN processUMN processUnilateral hyporeflexia Unilateral hyporeflexia --LMNLMNAsymmetric reflexes Asymmetric reflexes --pathologicpathologic
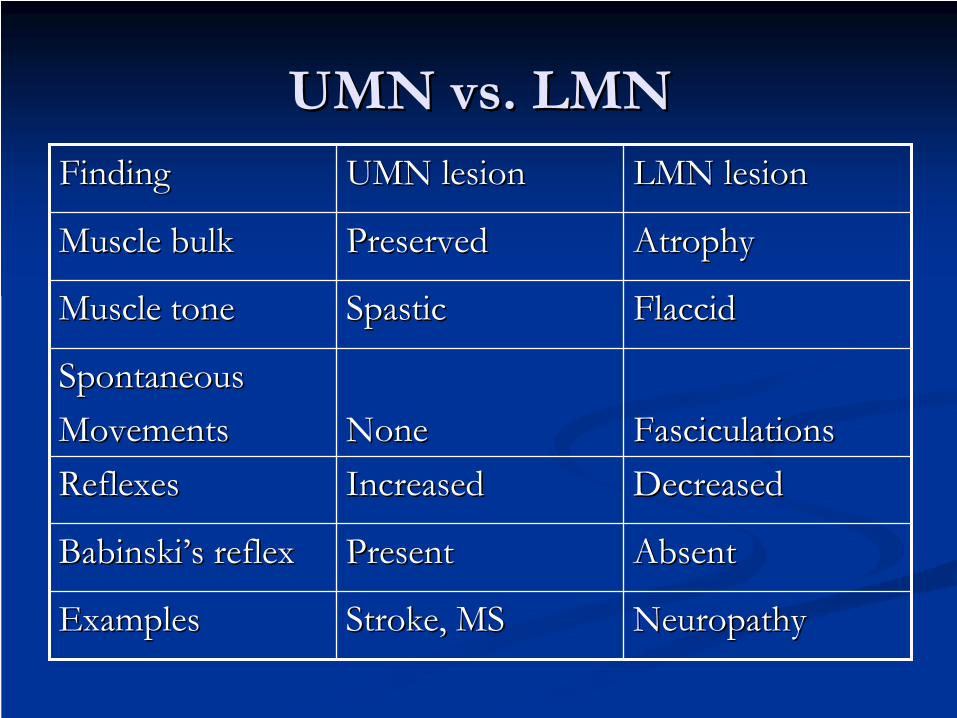
UMN vs. LMNUMN vs. LMNFindingFinding UMN lesionUMN lesion LMN lesionLMN lesion
ExamplesExamples Stroke, MSStroke, MS NeuropathyNeuropathy
Key ComponentsKey ComponentsOnset & time course of the symptomsOnset & time course of the symptomsSymmetry of symptomsSymmetry of symptomsIs the deficit motor, sensory or both (sensorimotor)?Is the deficit motor, sensory or both (sensorimotor)?Are the sensorimotor signs & symptoms proximal, Are the sensorimotor signs & symptoms proximal, distal or both?distal or both?Do the symptoms fluctuate, if so is it associated with Do the symptoms fluctuate, if so is it associated with activity?activity?Are there symptoms that suggest CN involvement such Are there symptoms that suggest CN involvement such as, diplopia, dysarthria, or ptosis?as, diplopia, dysarthria, or ptosis?
Case StudyCase Study
A 41 yr old male presents with left neck pain A 41 yr old male presents with left neck pain and left arm weakness over the past 6 weeksand left arm weakness over the past 6 weeksPain radiates down the radial aspect of his left Pain radiates down the radial aspect of his left forearm (lateral outside of arm) forearm (lateral outside of arm) The neck pain is aggravated when he sneezesThe neck pain is aggravated when he sneezesParesthesias of the left thumb and index fingerParesthesias of the left thumb and index fingerGait is slightly unsteadyGait is slightly unsteadyUrinary urgency for one weekUrinary urgency for one week
Neurological examNeurological examHe is in mild discomfort with VSSHe is in mild discomfort with VSSMental status & CN are normalMental status & CN are normalSpasticity in both LES with clonus in the anklesSpasticity in both LES with clonus in the anklesStrength: deltoids 5/5, biceps 4+/5, triceps 5/5, wrist Strength: deltoids 5/5, biceps 4+/5, triceps 5/5, wrist extensors 5/5, LEs strength normalextensors 5/5, LEs strength normalSensory: decreased pinprick over lateral aspect of left Sensory: decreased pinprick over lateral aspect of left arm, left thumb & 2arm, left thumb & 2ndnd digitdigitReflexes: triceps 3/4, biceps 0/4, brachioradialis 0/4, Reflexes: triceps 3/4, biceps 0/4, brachioradialis 0/4, knees 3+/4, ankles 4/4, Plantar responses are extensors knees 3+/4, ankles 4/4, Plantar responses are extensors bilaterallybilaterallyGait: normal, tandem with mild difficultyGait: normal, tandem with mild difficulty
The sensory loss seen The sensory loss seen –– lateral aspect of the left arm lateral aspect of the left arm extending to left thumb & 2extending to left thumb & 2ndnd digit digit –– The sensory The sensory distribution of left C6 nerve root (left C6 dermatome) distribution of left C6 nerve root (left C6 dermatome) ––lesion in the nerve rootlesion in the nerve rootA dermatome is a strip of skin supplied by an individual A dermatome is a strip of skin supplied by an individual spinal nerve rootspinal nerve rootA spinal cord lesion produce a sensory levelA spinal cord lesion produce a sensory levelA lesion in the brain stem produce a sensory loss only A lesion in the brain stem produce a sensory loss only on one side of the body (hemisensory loss)on one side of the body (hemisensory loss)
The left arm weakness is due to LMN lesion or The left arm weakness is due to LMN lesion or UMN lesion?UMN lesion?The left arm weakness is due to LMN The left arm weakness is due to LMN dysfunction dysfunction
The left biceps weakness is associated with absent The left biceps weakness is associated with absent left biceps & brachioradialis reflexesleft biceps & brachioradialis reflexesCervical nerve root lesion (radiculopathy)Cervical nerve root lesion (radiculopathy)
An UMN lesion would produce hyperactive An UMN lesion would produce hyperactive upper extremity stretch reflexesupper extremity stretch reflexes
Gait dysfunctionGait dysfunction
Gait dysfunction due to UMN lesionGait dysfunction due to UMN lesionThe knee & ankle are hyperreflexicThe knee & ankle are hyperreflexicBoth plantar reflexes are upgoingBoth plantar reflexes are upgoingLesion in the corticospinal tractsLesion in the corticospinal tractsYou can have a lesion in the tracts extending to You can have a lesion in the tracts extending to a nerve root a nerve root A combined UMN lesion (Myelopathy) & LMN A combined UMN lesion (Myelopathy) & LMN lesion (Radiculopathy)lesion (Radiculopathy)
Woman with chronic painWoman with chronic pain
A 38 year old secretary A 38 year old secretary Right wrist pain Right wrist pain –– worst at nightworst at nightWeakness when grasping thingsWeakness when grasping thingsPeriodic tingling and numbness in her right thumb & Periodic tingling and numbness in her right thumb & index fingerindex finger
CTS DiagnosisCTS DiagnosisTinel's sign Tinel's sign Phalen's sign Phalen's sign Check for atrophy in the Check for atrophy in the affected handaffected handEMGEMGSymptomsSymptoms
Pain which is aggravated Pain which is aggravated by wrist flexion & by wrist flexion & extension and may radiate extension and may radiate to elbowto elbow
Waking with pain at night Waking with pain at night due to flexion during due to flexion during sleepsleepBurning, numbness or Burning, numbness or tingling in the fingers and tingling in the fingers and hand, sometimes hand, sometimes extending to the elbow extending to the elbow Grasping objects may be Grasping objects may be difficultdifficult
*** Remember: HNP, a.k.a. herniated disk *** Remember: HNP, a.k.a. herniated disk or slipped disk or ruptured disk or slipped disk or ruptured disk –– all mean all mean essentially the sameessentially the same
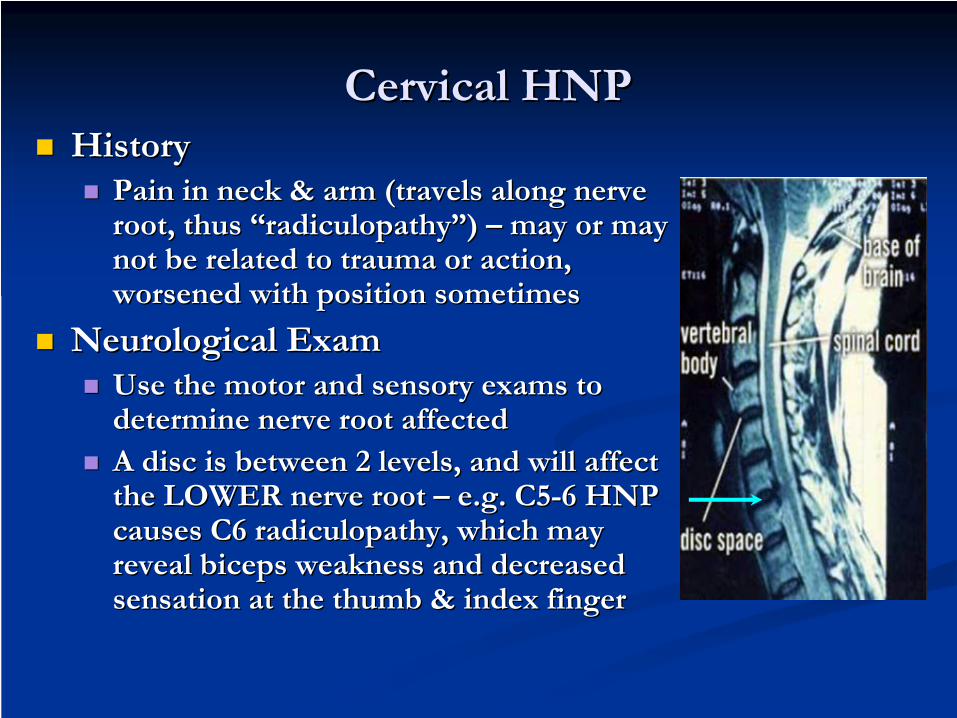
Cervical HNPCervical HNPHistoryHistory
Pain in neck & arm (travels along nerve Pain in neck & arm (travels along nerve root, thus root, thus ““radiculopathyradiculopathy””) ) –– may or may may or may not be related to trauma or action, not be related to trauma or action, worsened with position sometimesworsened with position sometimes
Neurological ExamNeurological ExamUse the motor and sensory exams to Use the motor and sensory exams to determine nerve root affecteddetermine nerve root affectedA disc is between 2 levels, and will affect A disc is between 2 levels, and will affect the LOWER nerve root the LOWER nerve root –– e.g. C5e.g. C5--6 HNP 6 HNP causes C6 radiculopathy, which may causes C6 radiculopathy, which may reveal biceps weakness and decreased reveal biceps weakness and decreased sensation at the thumb & index fingersensation at the thumb & index finger
http://www.josephmaroon.com/mded2.htm
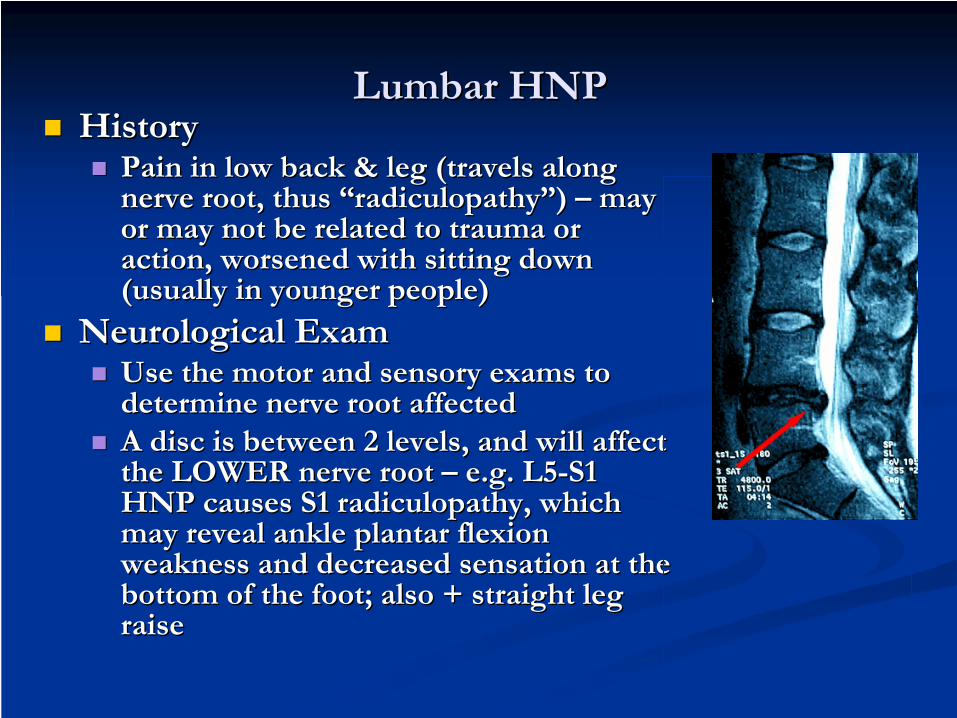
Lumbar HNPLumbar HNPHistoryHistory
Pain in low back & leg (travels along Pain in low back & leg (travels along nerve root, thus nerve root, thus ““radiculopathyradiculopathy””) ) –– may may or may not be related to trauma or or may not be related to trauma or action, worsened with sitting down action, worsened with sitting down (usually in younger people)(usually in younger people)
Neurological ExamNeurological ExamUse the motor and sensory exams to Use the motor and sensory exams to determine nerve root affected determine nerve root affected A disc is between 2 levels, and will affect A disc is between 2 levels, and will affect the LOWER nerve root the LOWER nerve root –– e.g. L5e.g. L5--S1 S1 HNP causes S1 radiculopathy, which HNP causes S1 radiculopathy, which may reveal ankle plantar flexion may reveal ankle plantar flexion weakness and decreased sensation at the weakness and decreased sensation at the bottom of the foot; also + straight leg bottom of the foot; also + straight leg raiseraise
Similar as for HNP, but associated Similar as for HNP, but associated with bladder >bowel incontinencewith bladder >bowel incontinence
ExamExamSimilar as with radiculopathy, but Similar as with radiculopathy, but need to check postneed to check post--void residual void residual (HIGH, as normal is less than (HIGH, as normal is less than 100cc) and rectal exam (decreased 100cc) and rectal exam (decreased tone)tone)
RadiographsRadiographsSignificant compression of cauda equinaSignificant compression of cauda equina
Most common cause of acute facial paralysisMost common cause of acute facial paralysisSudden facial weakness, difficulty with articulation, Sudden facial weakness, difficulty with articulation, problems keeping an eye closed, or inability to keep problems keeping an eye closed, or inability to keep food in the mouth one side.food in the mouth one side.One sided weakness of the face involving the foreheadOne sided weakness of the face involving the forehead
TreatmentTreatment--acycloviracyclovir--Steroid controversialSteroid controversial--Eye care to avoid corneal abrasionsEye care to avoid corneal abrasions
--
lacrilube and patchinglacrilube and patching
NormalNormalRightMotorCortex
LeftMotorCortex
RightFacial
Nucleus
LeftFacial NucleusThe upper part
of the facial nucleus receives UMN fibers from both cortices.
However, the lower part has from only the opposite cortex.
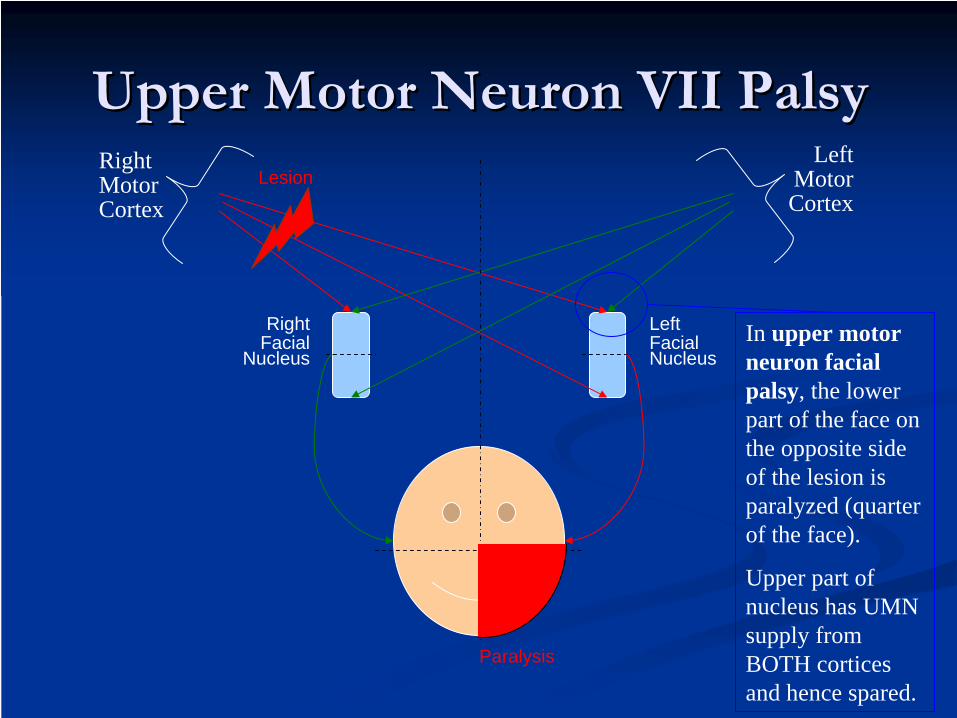
Upper Motor Neuron VII PalsyUpper Motor Neuron VII PalsyRightMotorCortex
LeftMotorCortex
RightFacial
Nucleus
LeftFacial Nucleus
In upper motor neuron facial palsy, the lower part of the face on the opposite side of the lesion is paralyzed (quarter of the face).
Upper part of nucleus has UMN supply from BOTH cortices and hence spared.
Lesion
Paralysis
Lower Motor Neuron VII PalsyLower Motor Neuron VII PalsyRightMotorCortex
LeftMotorCortex
RightFacial
Nucleus
LeftFacial NucleusIn lower motor
neuron facial palsy, the entire one side (half) of the face on the side of lesion is paralyzed.
Facial nerve is the final neural pathway.
Lesion
Paralysis
PNS VS CNSPNS VS CNS
SubjectiveSubjectiveVertigoVertigo
ObjectiveObjectiveAssessmentAssessmentPlanPlan
TinnitusTinnitusPeripheral vertigo Peripheral vertigo –– Vertigo due to disturbances in the Vertigo due to disturbances in the vestibular apparatus of the inner earvestibular apparatus of the inner earCentral vertigo Central vertigo –– Vertigo caused by disease of the CNSVertigo caused by disease of the CNSConductive hearing loss Conductive hearing loss –– Hearing loss resulting from Hearing loss resulting from lesion to structures in the outer or middle ear that lesion to structures in the outer or middle ear that converts air conduction into bone conductionconverts air conduction into bone conductionSensorineural hearing loss Sensorineural hearing loss –– Hearing loss from a lesion Hearing loss from a lesion in the inner ear or 8in the inner ear or 8thth CNCNElectronystagmogram (ENG) Electronystagmogram (ENG) –– A record of nystagmus A record of nystagmus activity measured by detecting the electrical activity of activity measured by detecting the electrical activity of the extraocular musclesthe extraocular muscles
Case Study Case Study
A 45 yr old female who noted recent hearing A 45 yr old female who noted recent hearing loss loss –– progressively worse in monthsprogressively worse in monthsOne day she started hearing better louder but One day she started hearing better louder but felt the room spinning + n/vfelt the room spinning + n/vLying down in bed with her eyes open made it Lying down in bed with her eyes open made it betterbetterA few episodes of hearing loud noise + vertigoA few episodes of hearing loud noise + vertigoNeuro exam Neuro exam –– nystagmus fast beating to the nystagmus fast beating to the rightright
Central VertigoCentral Vertigo Peripheral VertigoPeripheral Vertigo
Vertigo is mildVertigo is mild Vertigo is severeVertigo is severe
Brain stem signs are presentBrain stem signs are present No brain stem signsNo brain stem signs
Hearing loss is rareHearing loss is rare Hearing loss is commonHearing loss is common
Nystagmus is:Nystagmus is:MultidirectionalMultidirectionalNonfatigableNonfatigableAbrupt in onsetAbrupt in onsetOf long durationOf long duration
Nystagmus is:Nystagmus is:UnidirectionalUnidirectionalFatigableFatigableOf long latency of onsetOf long latency of onsetOf short durationOf short duration
Patients with vestibular disorders causing peripheral vertigo Patients with vestibular disorders causing peripheral vertigo prefer to lie on the unaffected ear because this allows them to prefer to lie on the unaffected ear because this allows them to look toward the affected side decreasing the nystagmuslook toward the affected side decreasing the nystagmusNystagmus with fast beating component to the right suggests Nystagmus with fast beating component to the right suggests dysfunction of vestibular apparatus on the left sidedysfunction of vestibular apparatus on the left sideThe fast nystagmus beats away from the affected ear and the The fast nystagmus beats away from the affected ear and the slow beats towards the affected ear because lesions in the slow beats towards the affected ear because lesions in the vestibular apparatus decrease the rate of firing of the semicircvestibular apparatus decrease the rate of firing of the semicircular ular canals on the side of the lesion affecting the input of signal icanals on the side of the lesion affecting the input of signal into nto the brain stem oculomotor systemthe brain stem oculomotor systemThe eyes tend to drift toward the affected ear (slow component The eyes tend to drift toward the affected ear (slow component of nystagmus)of nystagmus)The cerebral cortex provides a corrective saccade to the oppositThe cerebral cortex provides a corrective saccade to the opposite e direction (the fast component of nystagmus)direction (the fast component of nystagmus)
Disorder of the PNS: Myasthenia GravisDisorder of the PNS: Myasthenia GravisMyasthenia gravis Myasthenia gravis
Progressive weakening of the skeletal musclesProgressive weakening of the skeletal musclesFasiculations & muscle atrophy (ALS)Fasiculations & muscle atrophy (ALS)Intermittent ptosisIntermittent ptosisAn autoimmune disorderAn autoimmune disorderAntibodies destroy acetylcholine receptors Antibodies destroy acetylcholine receptors
Peripheral Nervous SystemPeripheral Nervous SystemWhen the sensory component is involved, test When the sensory component is involved, test for proprioception, vibratory sensation, and pain for proprioception, vibratory sensation, and pain and temperature sensibilityand temperature sensibilityWhen the motor system is involved there is When the motor system is involved there is wasting, fasciculations, & weaknesswasting, fasciculations, & weaknessIn peripheral nerve process there is reduction or In peripheral nerve process there is reduction or absence of reflexesabsence of reflexesAutonomic dysfunctions may cause pupillary Autonomic dysfunctions may cause pupillary dysfunction, orthostatic hypotension, and tachydysfunction, orthostatic hypotension, and tachy--and bradyarrhythmias.and bradyarrhythmias.
Clinical HighlightsClinical HighlightsTesting motor function Testing motor function –– asymmetric strength deficitsasymmetric strength deficitsNo need to evaluate every muscle groupNo need to evaluate every muscle groupCentral (UMN) lesion result in Hyperreflexia & Central (UMN) lesion result in Hyperreflexia & increased muscle tone but not atrophy or fasciculationsincreased muscle tone but not atrophy or fasciculationsPeripheral lesions result in hyporeflexia, decreased Peripheral lesions result in hyporeflexia, decreased muscle tone, atrophy, & fasciculationsmuscle tone, atrophy, & fasciculationsBabinski reflex is a useful indicator of UMN diseaseBabinski reflex is a useful indicator of UMN diseaseCombination of UMN & LMNCombination of UMN & LMNBalance/coordination requires the integration of Balance/coordination requires the integration of cerebellar, visual, vestibular, & proprioceptive function cerebellar, visual, vestibular, & proprioceptive function Consider each aspect individually in evaluating a Consider each aspect individually in evaluating a balance or coordination problembalance or coordination problem
What do you think can change What do you think can change neurons and their connections?neurons and their connections?