Principal Investigator/Program Director (Last, first, middle): Shellman, Juliette 1. The Candidate 1. A. Introduction I am applying for the Mentored Research Scientist Development Award (K01) to promote my growth as an independent scientist in patient-oriented research. My goal for this five year career development award is to obtain the advanced training I need to develop a culturally appropriate peer-to-peer reminiscence intervention and test its effects on decreasing depressive symptoms in older African-Americans in a pilot study. This career development proposal builds on my two years of post-doctoral work as a John A Hartford Foundation Scholar as I tested the effects of reminiscence on depressive symptoms in older African- Americans. Conducting this pilot study enabled me to gain entry into African- American church communities. Preliminary results indicate that integrative reminiscence has a positive effect on reducing depressive symptoms in community- dwelling older African-Americans. However, this experience of working with church communities highlighted my need for further training in community-based participatory research to develop community approaches that will result in a sustainable reminiscence program for older African-Americans. This K01 award will not only provide opportunities for in-depth training to effectively partner with African-American communities, but will also build upon my current research skills to analyze the functions of reminiscence in older African-Americans and collect preliminary data in a pilot test for feasibility and directional effectiveness of the peer-to-peer reminiscence intervention on depressive symptoms in a pilot study. Late-life depression is a public health problem in the U.S. with significant economic and health consequences. According to the National Institute of Mental Health (2003), an estimated two million of the 35 million American older adults have a depressive illness and another five million have subsyndromal or minor depression. The economic cost of depression in older adults has been estimated to cost $43 billion dollars annually in the United States (American Association of Geriatric Psychiatry, 2001). There is little published research on the use of therapeutic interventions to decrease depressive symptoms in older adults and even less regarding depression in older African-Americans. With the expected increase in the older African-American population there is a critical need for the development and testing of innovative and cost-effective interventions such as peer to peer reminiscence programs. Reminiscence programs have been shown to decrease depression (Haight & Webster; 1995; 2002). This reminiscence intervention is innovative because it utilizes a peer-to-peer approach that can assist in overcoming barriers to African-American older adults’ participation in mental health research and decrease depressive symptoms. Effectively managing minor depressive symptoms in older African Americans has major implications for their quality of life. In response to the health disparities among older African-Americans, Haug and Wykle (1999) called for the following: 1) improved education and increased trust- PHS 398/2590 (Rev. 09/04, Reissued 4/2006) Page 1 Continuation Format Page
Transcript
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliette1. The Candidate1. A. IntroductionI am applying for the Mentored Research Scientist Development Award (K01) to promote my growth as an independent scientist in patient-oriented research. My goal for this five year career development award is to obtain the advanced training I need to develop a culturally appropriate peer-to-peer reminiscence intervention and test its effects on decreasing depressive symptoms in older African-Americans in a pilot study. This career development proposal builds on my two years of post-doctoral work as a John A Hartford Foundation Scholar as I tested the effects of reminiscence on depressive symptoms in older African-Americans. Conducting this pilot study enabled me to gain entry into African-American church communities. Preliminary results indicate that integrative reminiscence has a positive effect on reducing depressive symptoms in community-dwelling older African-Americans. However, this experience of working with church communities highlighted my need for further training in community-based participatory research to develop community approaches that will result in a sustainable reminiscence program for older African-Americans. This K01 award will not only provide opportunities for in-depth training to effectively partner with African-American communities, but will also build upon my current research skills to analyze the functions of reminiscence in older African-Americans and collect preliminary data in a pilot test for feasibility and directional effectiveness of the peer-to-peer reminiscence intervention on depressive symptoms in a pilot study.
Late-life depression is a public health problem in the U.S. with significant economic and health consequences. According to the National Institute of Mental Health (2003), an estimated two million of the 35 million American older adults have a depressive illness and another five million have subsyndromal or minor depression. The economic cost of depression in older adults has been estimated to cost $43 billion dollars annually in the United States (American Association of Geriatric Psychiatry, 2001). There is little published research on the use of therapeutic interventions to decrease depressive symptoms in older adults and even less regarding depression in older African-Americans. With the expected increase in the older African-American population there is a critical need for the development and testing of innovative and cost-effective interventions such as peer to peer reminiscence programs. Reminiscence programs have been shown to decrease depression (Haight & Webster; 1995; 2002). This reminiscence intervention is innovative because it utilizes a peer-to-peer approach that can assist in overcoming barriers to African-American older adults’ participation in mental health research and decrease depressive symptoms. Effectively managing minor depressive symptoms in older African Americans has major implications for their quality of life.
In response to the health disparities among older African-Americans, Haug and Wykle (1999) called for the following: 1) improved education and increased trust-building efforts to educate older African-Americans about the value their contributions can make to science, 2) increased funds to attract minorities and those interested in studying older African-Americans, and 3) improved health care policies affecting minority elders through cost analyses and studies of different health care delivery models utilized by minority groups. Despite this call to action, mental health disparities and low research participation rates among older African-Americans still exist (Rooks & Whitfield, 2004). My K01 career development award directly responds to these needs. By completing the proposed training and research plan, I will gain expertise in a community-based participatory research approach with older African-Americans to increase their trust and participation in research, mentor young African-American researchers, and develop a sustainable peer to peer reminiscence intervention program based on the strength of African-American oral traditions. The training and research plans described in this proposal will position me to carry out independent investigations designed to translate an empirical understanding of the functions of reminiscence in older African-Americans into an innovative and cost-effective peer to peer approach to decrease depressive symptoms in this population.
Specifically, the K01 Career Development Award will provide me additional skills, training and mentoring in: 1) community-based participatory research that includes the use of ethnographic research method, development and management of effective interdisciplinary teams, and formation of partnerships with key stakeholders, 2) the functions of integrative reminiscence in older African-American adults, 3) development of a culturally appropriate peer to peer reminiscence training manual in partnership with African-American communities, 4) research methods and statistical techniques appropriate to design and implement randomized clinical trials for psychosocial interventions. 5) the responsible and ethical conduct of psychosocial intervention
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteresearch, and 6) gaining expertise in grantsmanship through mentored development of an R-series grant application to conduct a clinical trial testing the peer to peer reminiscence intervention in lowering depressive symptoms in older African-Americans. The research aims listed below compliment the training goals for this career development award. The research aims for this project are: 1) to explore the meaning and perceived benefits of integrative reminiscence in community-dwelling older African-Americans, 2) to test the cultural relevance, acceptability, and psychometric properties of the Reminiscence Function Scale with older African-Americans, 3) to describe the functions of reminiscence in community-dwelling older African-Americans, 4) to develop and pilot test the peer reminiscence training manual for its appropriateness, feasibility and acceptability in an older African-American community, and 5) To pilot test the peer-to-peer reminiscence intervention for feasibility and directional effectiveness on depressive symptoms and reminiscence functions in older community-dwelling older African-Americans (N=24).
1. B. Career Goals and Objectives: Scientific BiographyMy professional career began in education. After earning both a Bachelor of Science and a Master of Science in Education and teaching for 12 years I entered the field of nursing. Upon graduation from nursing school, I first worked in a long term care facility caring for older adults on a sub-acute unit. This experience enabled me to develop clinical skills in the care of older adults with acute illnesses and management of psychosocial problems such as depression and end-of-life care. It was this experience that led to my interest in caring for older adults and the use of reminiscence as a possible intervention to decrease depression and increase life-satisfaction. During my graduate studies in nursing I was attracted to community health nursing because of its focus on prevention, restorative and maintenance health care for older adults. My community health clinical education included care of older adults in community-based settings as well as in the home. An important aspect of this education was conducting a community needs assessment in a rural area in Connecticut and my subsequent establishment of blood pressure clinics and wellness program for older adults at a senior center in Connecticut. This led to my first publication (Shellman, 2000) and recognition by the University of Connecticut with the Eleanor K. Gill Award for Excellence in Clinical Practice.
Predoctoral ExperienceWhile studying for a master’s degree in community health nursing at the University of Connecticut School of Nursing I formally began my research training under the mentorship of Dr. Patricia Neafsey who is well known for her work on preventing drug interactions in older adults. During this experience I learned recruitment strategies, focus groups techniques, and data collection methods. As project director for Dr. Neafsey’s study, Preventing over the Counter Drug and Prescription Medication Interactions in Older Adults, I trained undergraduate research assistants and carried out an interactive computer intervention. This work led to numerous publications as a co-author and multiple local and national presentations. The experience also enabled me to develop an appreciation for the methods and challenges of conducting field research. Simultaneously, I focused my graduate coursework on the use of reminiscence in nursing practice, gaining depth in its theoretical underpinnings and expertise in facilitating reminiscence with older adults in the community. My first study was conducted using reminiscence with Haitian elders as part of an international community health experience. While reminiscing with the older Haitians, it became apparent that reminiscence enabled the Haitian elders to remember the happier times of the past and relieve the pain of their present living conditions. In addition, the findings suggested that reminiscence could be beneficial for health care providers as a tool for learning about elders’ cultural beliefs and practices. These findings significantly informed my reminiscence work and research focus for my doctoral studies.
In 1999, I began pursuing my doctorate at the University of Connecticut under the guidance of Dr. Henrietta Bernal, RN, Ph.D., a nurse anthropologist. Throughout my doctoral experience I sought to gain a better understanding of the uses and benefits of reminiscence, while strengthening my clinical training in the care of older adults in the community. While at the University of Connecticut, I became involved in the development of the award winning CARELINK Model of Care for older adults in the community (Bernal, Shellman & Reid, 2004). In this community-university partnership, nursing students provide services during their community health practicum to older adults no longer eligible for compensated care through the regular visiting nurse services. As part of the CARELINK model of care, I developed a reminiscence education program to teach students how to facilitate reminiscence with older adults. My dissertation work emerged from this experience.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteFirst, I modified the Cultural Self-Efficacy Scale developed by Bernal & Froman (1987; 1993) and developed a reliable and valid scale to measure Students’ Eldercare Cultural Self–Efficacy (ECSES) (Shellman, 2006). A principal factor analysis revealed a four factor structure with alpha coefficients ranging from .82-.95. This 28 item scale was found to be reliable and valid measure of eldercare cultural self-efficacy in baccalaureate nursing students. Secondly, I employed an interrupted time series with a nonequivalent no-treatment control group design with the ECSES as the measurement. The Effects of a Reminiscence Education Program on BSN Students’ Cultural Self-Efficacy in Caring for Elders was conducted with senior nursing students. The quantitative findings indicated that nursing students receiving the reminiscence intervention had higher levels confidence in caring for older adults of different ethnic backgrounds than those not receiving the reminiscence intervention (Shellman, 2006). These findings were supported with contextual data gathered during the study that provided insight into the students’ perceptions of the reminiscence education program (Shellman, 2006). My dissertation work resulted in two published manuscripts and numerous presentations at local and regional nursing conferences. Upon graduation I received the Carolyn Ladd Widmer Award given to a doctoral candidate for outstanding dissertation research.
As part of my doctoral work and under the continued guidance of Dr. Bernal, I started the groundwork for patient-oriented research and focused work on the use of reminiscence with African-American elders. In addition to conducting my dissertation research, I was named an American Nurses Association Presidential Scholar and was funded by the American Nurses Foundation to conduct the study “Understanding Life Experiences of African-American Elders”. This phenomenological study revealed key themes as well as the benefits of reminiscence for African-American older adults (Shellman, 2004). This foundational reminiscence study provided important groundwork for the next phases of my reminiscence research program.
Postdoctoral ExperienceAfter my appointment as an Assistant Professor at the University of Connecticut School of Nursing in the fall of 2003, I began to formalize my program of research and continued focusing on patient-oriented reminiscence research. Through clinical work in the CARELINK program, I discovered the importance of the issues of depression and social isolation in community-dwelling minority older adults and the existing disparities in mental health care for this population. These observations in addition to my previous reminiscence work with older African-Americans led me to this research path of the use of reminiscence to decrease depressive symptoms.
In 2004 I submitted and was awarded a Large Faculty Grant from the UCONN Research Foundation to begin pilot work on Effects of a Structured Reminiscence Program on Depression and Life Satisfaction in African-American Elders. At the same time, I began establishing linkages with leaders in gerontological nursing at New York University. Subsequently, I was awarded a 2004 John A. Hartford Foundation Post-Doctoral Fellowship. Dr. Elizabeth Capezuti from New York University and Dr. Lois Evans from the University of Pennsylvania served as co-mentors. Both of these geriatric experts have been instrumental in my continuing on this path of reminiscence intervention research with older adults. With the support of the Hartford Foundation, I have been able to pursue my interest in reminiscence research and depression in African-American elders while developing important networks with other gerontological nursing leaders.
The pilot study Effects of a Structured Reminiscence Program on Depression and Life Satisfaction in African-American Elders has provided important contextual and quantitative data. One article describing qualitative results from the study “Keeping the Bully Out.” The Meaning of Depression in a Sample of African-American Elders is under review for the Journal of the American Psychiatric Nurses Association. Preliminary findings from this study have been disseminated at the Gerontological Society of America’s 58th Annual Conference and a manuscript is in progress. The experience of conducting this research has provided me with insight into the following challenges of conducting mental health research with minority populations. Specifically, 1) I experienced first-hand the mistrust and hesitancy of gatekeepers to allow me, a white researcher, entry into their communities, 2) recruitment and retention of both African-American research assistants and participants required constant effort, and 3) the sensitivity and stigma surrounding the topic of depression. While conducting this study, Dr. Bernal introduced me to Dr. Jean Schensul, Founder and Director of Research at the Institute for Community Research (ICR) in Hartford, CT. I have attended programs and met with various staff
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliettemembers from ICR including Dr. Schensul over the past two years. It has become evident to me from making these contacts and observing the work conducted at ICR that the community-based participatory research model practiced by ICR would be most appropriate for conducting my program of research.
During my post-doctoral experience, I was selected to participate in the National Institute of Aging’s Summer Institute on Aging Research Program in July, 2005. Through networking opportunities and individual research consultation provided at the institute, I was encouraged to examine my research career goals and identify the resources and skills I would need to attain these goals. All of these experiences were influential in my decision to pursue this career development award. I subsequently sought a faculty position in a research intensive environment and in the summer of 2006 was appointed as an Assistant Professor at Yale University School of Nursing. All of these experiences have been invaluable, and I am now ready to take the next step toward becoming an independent researcher.
Under the guidance of Drs. Capezuti and Evans, I have developed important research skills and have come to understand the value of networking with experts in the field of mental health aging research. As a result of their guidance, I have met with gerontological leaders such as Dr. Terry Mills from University of Florida and Dr. Peter Lichtenberg from Wayne State University to assist me in developing goals for this career development award. I am seeking additional training to address the mental health and well-being of older African-Americans with an innovative and community-developed reminiscence training manual. Additional mentoring from noted experts in the fields of community-based participatory research, depression, and minority research will enhance my expertise in developing community partnerships, interdisciplinary research teams, and the dissemination of a culturally appropriate and acceptable reminiscence training manual that will result in a sustainable peer to peer reminiscence intervention program for African-American communities.
According to the Surgeon General’s 2001 Mental Health Report: Culture, Race and Ethnicity, the disparities affecting mental health care of minorities are the result of having less access to mental health services, receiving poorer quality of care, and an under-representation of minorities in mental health research. Mistrust of health care providers, research, and researchers have been cited as factors for low minority participation in studies (Curry & Jackson, 2004). Using a participatory approach to research, and recognizing the community’s cultural values and health concerns are paramount in developing community partnerships. Interdisciplinary research partnerships can have immediate and long-term benefits (Schensul, 2006). One of the most significant challenges to conducting community-based participatory research is the significant time and effort required to build relationships among partners (Israel, Lichtenstein, Lantz, McGranagan, Allen, Guzman, Softley, & Maciak, 2001). At this phase in my career, protected time to pursue the proposed research career development plan, and develop relationships and community participatory activities is crucial. I will commit at least 75% effort to the research and career development activities outlined in this award for a period of five-years to meet the goals described in this plan (see letter of support from Dean Grey in appendix).
1. C. Career Development Activities during Award PeriodLong-term GoalsMy research experiences, as well as my academic training and clinical work, reflect my strong interest in the use of reminiscence to decrease depressive symptoms in older African-Americans. The major long-term goal of this five year career development award is to establish myself as an independent reminiscence researcher who will, in partnership with communities, develop a peer-to-peer reminiscence intervention that will decrease depressive symptoms in this population. My three year plan of development is to execute high-quality, original reminiscence research and make significant contributions to the field. The career development activities and research plan proposed in this application will provide me with the needed training and experience, as well as essential reminiscence pilot data to conduct a clinical trial in the future. During Year 3 of this career development award, I will begin to develop an application for an R series grant which will allow me to test this peer-to-peer reminiscence intervention in a larger scale study. My ultimate research goal after this career development award is completed and sufficient pilot data is gathered is to submit an R01 to test the clinical effectiveness of a reminiscence intervention on depressive symptoms and reminiscence functions in older African-Americans.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteShort-term Training Goals1) To pursue advanced training in community participatory research that include the use of ethnographic
research methods, development and management of effective interdisciplinary teams, and formation of partnerships with key stakeholders.
2) To analyze the functions of integrative reminiscence in African-American older adults.3) To develop a culturally appropriate reminiscence training manual in partnership with African-American
communities.4) To identify appropriate research methods and statistical techniques for designing and conducting
randomized clinical trials for psychosocial interventions.5) To describe the responsible and ethical conduct of psychosocial intervention research.6) To gain expertise in grantsmanship through mentored development of an R-series grant application to
conduct a clinical trial testing the peer to peer reminiscence intervention in lowering depressive symptoms in older African-Americans.
As a result of my pre and post-doctoral work, I have acquired a solid foundation in the use of reminiscence with older African-Americans. The career development plan and the community-participatory research activities described in this proposal will enhance this foundation and help me to establish myself as an expert in the development of a sustainable peer to peer reminiscence intervention for older African-Americans. The key strategies necessary to further my career development are: 1) mentoring, 2) structured activities, and 3) practical experience through involvement in community-based participatory research. I have identified some of the most experienced research scientists in these areas to assist me in meeting my career goals.
1.C.i. MentoringPrimary MentorGail D'Eramo Melkus, EdD, C-ANP, FAAN, is the Independence Foundation Professor of Nursing and Associate Director - Center for Excellence in Chronic Illness Care at Yale University School of Nursing. Dr. Melkus, a white researcher, has developed strong ties with the African-American population in the New Haven area. She is an expert in developing culturally sensitive interventions through the use the use of focus groups in underserved populations, specifically with African-Americans (Maillet, Knafl, Melkus, 1996; Melkus, Spollet, Jefferson, Chyun, Tuohy, Robinson, & Kaisen, 2004; Newlin, K, Melkus, Jefferson, Langerman, Womack, & Chyun, D, 2006). Her expertise in this area will be invaluable as I begin the process of developing sustainable relationships in the New Haven community. I asked Dr. Melkus to be my primary mentor because she is a senior faculty member at Yale School of Nursing and besides her success in conducting research with ethnic minority populations; she is well-known for mentoring emerging investigators at the school of nursing. We will meet weekly to discuss my progress and she will advise me on issues related to conducting research with ethnic minority populations, conducting focus groups, research design, and entering diverse communities. Dr. Melkus will also guide me in the R-series submission planned for Year 5 of this training award.
Co-MentorsPeter Lichtenberg, PhD, is Professor of Psychology and Director of the Institute of Gerontology at Wayne State University and Co-Director of the Michigan Center for Urban African-American Aging Research (MCUAAR), one of the six NIA/NINR funded resource centers for minority aging research. Dr. Lichtenberg is a well-known investigator in the field of geriatric depression as well as an outstanding mentor and faculty member at Wayne State University. He has been instrumental in the development of MCUAAR and programs such as successful Healthy Black Elders Center also funded by NIA. Dr. Lichtenberg will provide mentoring in community-based participatory research that will include my participation in programs and workshops offered through MCUAAR to observe this model of successful community-participatory research created to reduce health disparities between minority and non-minority older adults.
Jean Schensul, PhD, Senior Scientist and Founder and Director of Research at the Institute for Community Research in Hartford, CT, is a medical anthropologist with over 20 years of experience in community-based participatory research and is nationally and internationally known for her work in the conduct of HIV prevention, minority mental health and other health-related research in urban areas of the United States and in developing countries. Her areas of expertise include research methods, minority mental health, drug
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteresearch, sexuality and HIV, and school and community based structural approaches to interventions (Schensul, Robison, Reyes, Radda, Gaztambide, & Disch, 2006) She has been responsible for a number of federal, state and foundation funded studies and intervention projects, and is currently the principal investigator on three NIH-funded HIV and drug related grants utilizing community-based participatory research. Her mentoring will include career development related to community-participatory research methods including ethnography, development of interdisciplinary, intersectoral research teams, and guidance in the factors needed to implement a successful partnership. Dr. Schensul is located in the Hartford area at the Institute for Community Research and is easily accessible for consultation during the training period and research project.
ConsultantsTerry Mills, PhD, is Professor of Sociology and Associate Dean for Minority Affairs at the University of Florida. Dr. Mills is a Fellow of the American Geriatric Society and was recently appointed to serve a 4-year term on the National Advisory Council of Aging at the National Institutes of Health and is Chair, NIA Minority Task Force on Aging. His area of research focuses on the social, environmental, and physical health factors associated with late-life depression. Dr. Mills is an African-American researcher and has debriefed me during my most recent pilot study. He will mentor me specifically for the cultural appropriateness of the Reminiscence Functions Scale and the reminiscence training manual.
Phillipe Cappeliez, PhD, is a Professor of Psychology at the University of Ottawa in Canada. He has worked extensively on the functions of reminiscence and mental health in older adults and developing Model of Reminiscence and Health in Older Adults (Cappelize & O’Rourke, 2003; 2005; 2006). Dr. Cappeliez will provide guidance in the development of the reminiscence training manual and assist me with analyzing the functions of reminiscence in older African-Americans.
Lois Evans, PhD, RN, FAAN, the van Ameringen Professor in Nursing Excellence, is Chair, Family and Community Health Division and Program Director, Psychiatric-Mental Health Nursing, at the University of Pennsylvania. Dr. Evans has been instrumental in my development as an emerging scholar in the field of gerontological nursing. Drawing from her extensive background in aging, geriatric mental health and community and long term care systems, she will continue to mentor me in geropsychiatric nursing and, specifically, with the ethical conduct of mental health research with older adults. Her mental health expertise and familiarity with my reminiscence work will provide continuity for me and she will assist me in furthering my development as an independent investigator.
Significant ContributorM. Tish Knobf, PhD, RN, FAAN, AOCN, is the American Cancer Society Professor of Oncology Nursing and a Fellow in the American Academy of Nursing. Her current research to address the breast cancer experience of women of color is funded by the Yale-Howard Center to Reduce Health Disparities for a Community Based Participatory Research project, called "Connecting Sisters." Dr. Knobf’s current research targets persistent and late effects of cancer treatment in breast cancer survivors and she and her research team completed a pilot exercise intervention to assess the effect on bone mass, body composition and physical and psychological symptom distress. Dr. Knobf will provide consultation in regards to conducting community-participatory research with African-Americans and will assist me with entry into the New Haven African-American communities.
Community StakeholdersI have met with Karen Bailey Addison, LCSW Program Manager of the Northend Senior Center, Yvette Huyghue-Pannell, Director of Senior Services, Bloomfield Connecticut, and Millicent Wilson, Director of N.E.A.T., Bethel African Methodist Episcopal Church in Bloomfield. They are key stakeholders in this project. (See Appendix for letters of support.)
Structured Activities/Practical ExperiencesStructured, integrated activities will be established to develop my skills as a community-based researcher. Activities will include coursework, directed readings with annotated bibliographies, a literature review, research seminars, and directed participant observations. I will devote 8 hours per week in year one to coursework,
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliettedirected readings and structured activities. Practical experiences will include visits and observations at Wayne State University, Institute of Gerontology, ethnography practicum coursework, attending research seminars at conferences and at Yale Claude Pepper center, and continuing relationships through blood pressure clinics and wellness programs with the Northend and Bloomfield Senior Centers, The N.E.A.T group at Bethel Apostolic Church in Bloomfield. These organizations have agreed to participate in the focus groups and development of the peer-to-peer reminiscence training manual.
As a faculty member, I will take advantage of auditing formal coursework at Yale University in the areas of African-American studies (AFAM), Health Policy and Administration (HPA), Sociology (SOCY), and community-based participatory research. These courses have been selected in consultation with my mentors to develop new methodological skills and expand my knowledge base in the areas of community-based mental health research with African-American older adults. It is expected that coursework experience will occur in years one and three. These activities are described in more detail under each goal.
Goal #1To pursue advanced training in community participatory research that include the use of ethnographic research methods, development and management of effective interdisciplinary teams, and formation of partnerships with key stakeholders.
Coursework at Yale University: SOCY509B Ethnographic Research Methods–Spring – YR 1I selected the seminar in Ethnographic Research Methods because I have had no formal education in conducting this type of research. This particular course is a practicum in participant observation that will provide me with the necessary training to conduct participant observations described in the research plan. The bulk of the course focuses on workshop-style discussion of students' experience in their field sites. Participants are required to spend four hours per week in a field site and to write and share field notes with other students. Dr. Gail Melkus will assist me in selecting an appropriate field site in New Haven for the course. Dr. Schensul will provide directed readings in the areas of development and management of effective interdisciplinary teams and partnerships with key stakeholders. I will then develop an annotated bibliography on the recommended readings provided by Dr. Schensul. This goal is directly related to my research plan outline in this proposal to conduct community-based participatory research through participant observations and development of partnerships.
Practical ExperienceTo strengthen my ability to conduct research with older African-Americans, I will attend the Summer Training Workshop on African American Aging Research at the Michigan Center for Urban African American Aging Research (MCAUAAR). This resource center for minority aging research is co-facilitated by the University of Michigan and Wayne State University. I selected this resource center because of its focus on African-American aging research and The Healthy Black Elders Center (HBEC). HBEC is a diverse group of educators, community members, national advisors, and researchers who work to improve the health of older African –American adults living in the Detroit area. It is located at the Wayne State University Institute of Gerontology. During our last meeting, Dr. Lichtenberg suggested that I attend the Summer Training Workshop in African-American Aging Research and to plan to visit the facility, talk with staff members and observe participants at the HBEC when I attend my quarterly meetings with Dr. Lichtenberg. Other workshops offered 2- 3 times per year are aimed at providing investigators with opportunities to expand their knowledge and understanding of methodologies utilized in conducting research on racial/ethnic health disparities in elderly African Americans. My quarterly meetings with Dr. Lichtenberg will be coordinated with the scheduling of the workshops that I attend each year throughout the award. I will attend the annual Gerontological Society of America conferences to disseminate my latest work, and attend the workshops and seminars related to CPBR. One other structured experience to assist me in meeting this goal will be to conduct a literature review of community-based participatory research conducted with older adults. This information will assist also me to meet Goal # 1 and develop the expertise needed to utilize the community-based participatory research approach with older African-Americans described in the research plan.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteGoal #2To analyze the functions of integrative reminiscence in African-American older adults.
Coursework at Yale University: AFAM525B Psychosocial Study of Black Autobiography–Spring YR 1I selected the course work because it focuses on autobiographies of black men and women. The stories are analyzed to gain an understanding of the authors’ development over time, with attention to problem solving, satisfactions, disappointments, grief, and fulfillment. This course will be important in assisting me to analyze the functions and adaptive nature of reminiscence of reminiscence in older African-Americans. I have been following Dr. Cappeliez’ work on the Model of Reminiscence and Health since I started my graduate work in reminiscence His latest article, Empirical Validation of a Model of Reminiscence and Heath in Later Life (Cappeliez, 2006) prompted me to begin dialogue with him via e-mail to discuss the application of his model with older African-American adults. Contextual information and data gathered from my pilot study testing the effects of a reminiscence education program on depression and life satisfaction and my conversations with Dr. Cappeliez indicate that there are knowledge gaps in the reminiscence literature regarding the benefits of reminiscence for older African-Americans. Specifically, Dr. Cappeliez will provide directed readings on the functions of reminiscence and his adaptive model so that I can effectively evaluate the functions of integrative reminiscence in older African-American adults. He will assist me in analyzing the reminiscence data and provide consultation in the development of the reminiscence training manual. We will continue our e-mail dialogue throughout the 3 year award and I will meet with Dr. Cappeliez in year 2 to discuss manual development and study findings.
Practical ExperienceThe International Life Review and Reminiscence Group holds conferences and workshops every other year in conjunction with the Gerontological Society of America’s annual conferences. I will attend the conferences, disseminate my work, and attend workshops where reminiscence scholars present their latest reminiscence research. The majority of the practical experience to assist me in meeting this goal will be through methods of data collection as described in the research plan.
Goal #3To develop a culturally appropriate reminiscence training manual in partnership with African-American communities.
One of the key objectives of this career development plan is to develop expertise in the process of a community-developed reminiscence training manual. This goal is directly related to the research questions outlined in my research plan and will be completed in years two and three. I will incorporate what I learn from the coursework, attending community-based participatory workshops at Wayne State University and the directed readings from mentors. The process will be a bottom up approach using data gathered by participant observation, key informant interviews, and focus groups. The development of the manual will use continuous feedback from participation of the target communities so that the final product will represent as much of the opinions of the community as possible. The research plan describes the development and testing of the training manual using the principles of community-based participatory research (Israel, 2006). Drs. Schensul and Lichtenberg are both noted experts in community based participatory research with current NIH funding in community based participatory research projects (see biosketches). Dr. Lichtenberg will recommend pertinent community based participatory research workshops to attend at Wayne State and Dr. Schensul will provide directed readings in this area. Since Dr. Schensul is located in Hartford Connecticut, it is expected that she will provide more face to face feedback in regard to the process and structure of developing the manual. Dr. Evans will provide consultation regarding the training manual to ensure the identification of appropriate geriatric mental health resources should referrals be necessary.
Goal #4To pursue advanced training in research methods and statistical techniques for designing and conducting randomized clinical trials for psychosocial interventions.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteCoursework at Yale University: BIO 5401A Fundamentals of Clinical Trials–Fall– YR 1 and NUR943B Methodological Issues in the Study of the Management of Health and Illness – Spring – YR 1My long-term goal of conducting a large scale randomized trial will require advanced training in statistics and study design. During year one of the award period (see Figure 1); I will take courses in methodological issues in the study of management and health as well as fundamentals of clinical trials. N943B focuses on intervention development with a focus on self-management. The BIO 5401A course addresses issues related to the design, conduct, and analysis of clinical trials. Topics include protocol development, examination and selection of appropriate experimental design, methods of randomization, sample size determination, appropriate methods of data analysis including time-to-event data, and interim monitoring and ethical issues
Practical Experience
Attend the NIH sponsored summer training program in randomized trials for the social and behavioral sciences (Office of Behavioral and Social Science Research) or Quantitative Methods of Social Research at the Institute for Social Research at the University of Michigan
The Claude Pepper Center at Yale University provides resources for junior faculty members. I will attend the monthly Aging Seminars for junior and senior researchers and junior faculty retreats. These sessions provide opportunities for career development, dissemination of work and feedback, and collaboration with experts in geriatric research. Attending the sessions will allow me to receive feedback on my research and network with other gerontological researchers. The Center also provides Research Resource support in study design and data management.
Goal #5
To describe the responsible and ethical conduct of psychosocial intervention research.
Consideration of ethical issues is vital when designing clinical intervention studies in mental health research with minority populations in the community. Dr. Evans and Dr. Knobf will provide supervision and training for the responsible and ethical conduct of research. I have received training in the treatment of human subjects at Yale University, on-line training through the National Institute of Mental Health, and at the 2005 National Institute of Aging’s Summer Research Institute. Specific activities to continue my education and training in this area are: 1) continue to serve as a member of Yale School of Nursing’s Human Subjects Review Committee, 2)directed readings fromHoward Hughes Medical Institute website such as Making the Right Moves A Practical Guide to Scientific Management for NewFaculty( http://www.hhmi.org/resources/labmanagement , 3) attend seminars provided by Yale University’s Donaghue Initiative in Biomedical and Behavioral Research Ethics , and 4) receive ongoing training and supervision on responsible and ethical conduct of community-based participatory research from Dr. Evans.
Goal#6
To gain expertise in grantsmanship through a mentored experience of developing an R-series grantApplication to conduct a clinical trial testing the peer to peer reminiscence intervention in loweringdepressive symptoms in older African-Americans.
The goal of this training plan is to develop an R series to test the effects of the reminiscence intervention using the peer-to-peer approach on lowering depressive symptoms in older African-Americans in a clinical trial. Data derived from preliminary studies and the research conducted during this proposal period will guide the development of the grant. Dr. Melkus and Dr. Evans will provide ongoing consultation for the development of the proposal. Dr. Melkus will lend her expertise on study design for intervention research with minoritypopulations, and grant development. Dr. Evans will advise me regarding ethical issues related to mental health and aging research.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteThe practical experience of developing the grant will take place in year three of the award proposal. The described coursework, my experiences with the community participants and the data gathered during years one and two will guide the development of the grant proposal.
Goal #6To describe the responsible and ethical conduct of psychosocial intervention research.
Consideration of ethical issues is vital when designing clinical intervention studies in mental health research with minority populations in the community. Dr. Evans and Dr. Knobf will provide supervision and training for the responsible and ethical conduct of research. I have received training in the treatment of human subjects at Yale University, on-line training through the National Institute of Mental Health, and at the 2005 National Institute of Aging’s Summer Research Institute. Specific activities to continue my education and training in this area are: 1) continue to serve as a member of Yale School of Nursing’s Human Subjects Review Committee, 2)directed readings from the Howard Hughes Medical Institute website such as Making the Right Moves A Practical Guide to Scientific Management for New Faculty( http://www.hhmi.org/resources/labmanagement 3) attend seminars provided by Yale University’s Donaghue Initiative in Biomedical and Behavioral Research Ethics , and 4) receive ongoing training and supervision on responsible and ethical conduct of community- based participatory research from Dr. Evans and Dr. Knopf.
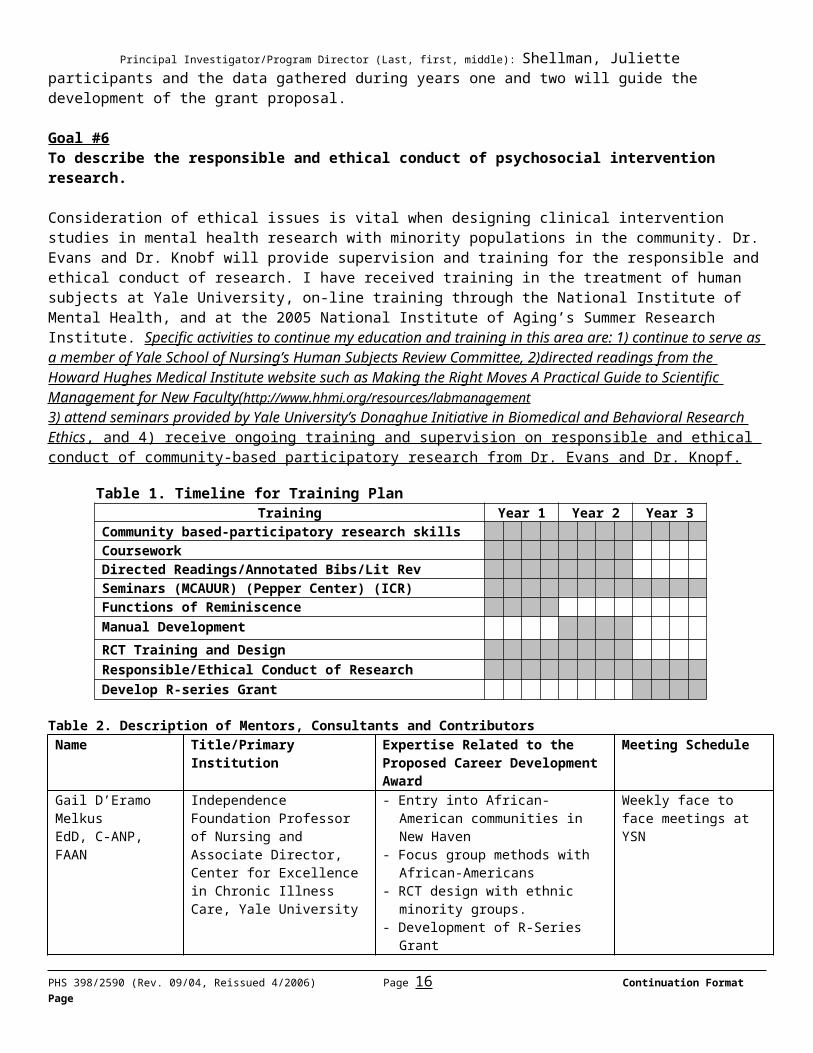
Table 1. Timeline for Training PlanTraining Year 1 Year 2 Year 3
Community based-participatory research skillsCourseworkDirected Readings/Annotated Bibs/Lit RevSeminars (MCAUUR) (Pepper Center) (ICR)Functions of Reminiscence Manual Development RCT Training and DesignResponsible/Ethical Conduct of ResearchDevelop R-series Grant
Table 2. Description of Mentors, Consultants and ContributorsName Title/Primary Institution Expertise Related to the Proposed
Career Development AwardMeeting Schedule
Gail D’Eramo MelkusEdD, C-ANP, FAAN
Independence Foundation Professor of Nursing and Associate Director, Center for Excellence in Chronic Illness Care, Yale University
- Entry into African-American communities in New Haven
- Focus group methods with African-Americans
- RCT design with ethnic minority groups.
- Development of R-Series Grant
Weekly face to face meetings at YSN
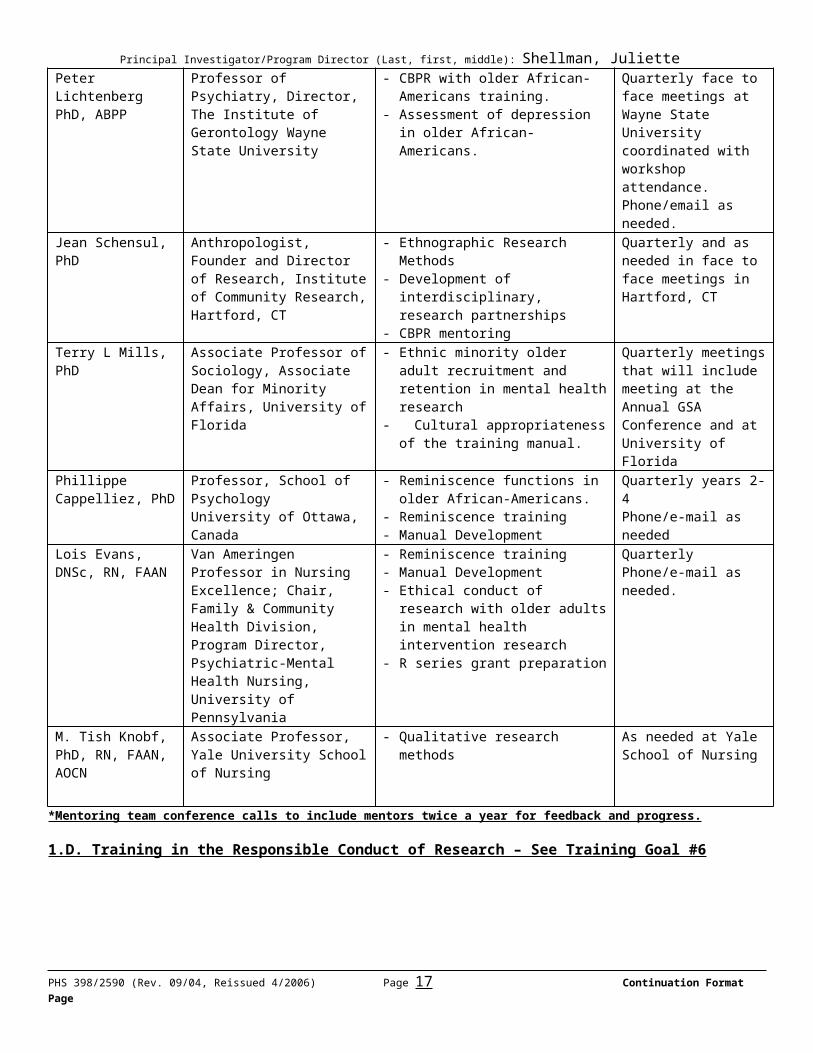
Peter LichtenbergPhD, ABPP
Professor of Psychiatry, Director, The Institute of Gerontology Wayne State University
- CBPR with older African-Americans training.
- Assessment of depression in older African-Americans.
Quarterly face to face meetings at Wayne State University coordinated with workshop attendance. Phone/email as needed.
Jean Schensul, PhD Anthropologist, Founder and Director of Research, Institute of Community Research, Hartford, CT
- Ethnographic Research Methods- Development of interdisciplinary,
research partnerships- CBPR mentoring
Quarterly and as needed in face to face meetings in Hartford, CT
Terry L Mills, PhD Associate Professor of Sociology, Associate Dean for Minority Affairs, University of Florida
- Ethnic minority older adult recruitment and retention in mental health research
- Cultural appropriateness of the
Quarterly meetings that will include meeting at the Annual GSA Conference and at
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliettetraining manual. University of Florida
Phillippe Cappelliez, PhD
Professor, School of PsychologyUniversity of Ottawa, Canada
- Reminiscence functions in older African-Americans.
- Reminiscence training- Manual Development
Quarterly years 2-4Phone/e-mail as needed
Lois Evans, DNSc, RN, FAAN
Van Ameringen Professor in Nursing Excellence; Chair, Family & Community Health Division, Program Director, Psychiatric-Mental Health Nursing, University of Pennsylvania
- Reminiscence training- Manual Development- Ethical conduct of research with
older adults in mental health intervention research
- R series grant preparation
QuarterlyPhone/e-mail as needed.
M. Tish Knobf, PhD, RN, FAAN, AOCN
Associate Professor, Yale University School of Nursing
- Qualitative research methods
As needed at Yale School of Nursing
*Mentoring team conference calls to include mentors twice a year for feedback and progress.
1.D. Training in the Responsible Conduct of Research – See Training Goal #6
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliette3. Environment and Institutional Commitment to Candidate3. A. Description of Institutional EnvironmentYale University provides a wealth of opportunity that can be harnessed for the development of junior investigators. Yale University is composed of the College and 11 Graduate and Professional Schools and 1,425 full-time faculty. The School of Nursing is an autonomous unit of the University, parallel to the Faculty of Arts and Sciences (Yale College and the Graduate School) and to the other graduate and professional schools. The School is a strong partner in the Yale-New Haven Medical Center. We have a wide array of clinical facilities available to us within the Center and enjoy excellent collaborative relationships with the School of Medicine and Public Health. The wealth of expertise in the form of multidisciplinary research scientists, diverse patient population base, and research infrastructure are optimal for a junior faculty member planning a career in the area of minority aging and mental health. The following is a list of resources available to provide opportunities for career enhancement and support for Dr. Shellman’s proposed research plan.
3.A.i Centers, Departments, and Research Support
Yale Program on AgingThe philosophy of the Yale Program on Aging is based on the premise that the greatest advancements in our understanding of normal aging, diseases associated with aging, and the effective and efficient use of health services by a growing elderly population will come about when knowledge is integrated across sciences. The Program on Aging encourages research on aging within and across departments in the Medical School, stimulating aging research from the basic sciences to epidemiology, from clinical care strategies to health policy, encompassing work in laboratories as well as population-based research.
Claude Pepper CenterThe Yale Program on Aging encompasses a number of research initiatives including the Claude D. Pepper Older Americans Independence Center, the Yale Health and Aging Project, falls and injury prevention projects, and studies of recovery from serious illness. The Center will provide Dr. Shellman with access to needed aging research resources such as participation in our Junior Faculty Aging Workshops and Aging Seminars. Participation in the workshops and seminar will enable Dr. Shellman to present her research-in-progress for peer review, allow for networking with researchers interested in geriatrics from an interdisciplinary group, and enhance her knowledge base in the latest areas of aging research.
Research SupportThe Office of Scholarly Affairs provides support to faculty and students conducting clinical research. The office is directed by Lawrence Scahill, PhD, RN, Acting Associate Dean for Scholarly Affairs. In addition to Dr. Scahill the office is staffed by the assistant director for research activities, two statisticians, a data manager, a senior administrative assistant, and a part-time editor.
Partnership Center on Reducing Health DisparitiesIn 2002, Yale School of Nursing (YSN) and Howard University Division of Nursing (HUDON) launched the Partnership Center on Reducing Health Disparities. The Center is funded for 5 years, and builds on the collaborative work of YSN and HUDON faculty. The goals of the Center are: 1) Facilitate the growth of the research infrastructures at the partnering institutions; 2) Enhance collaboration within and across the partnering institutions in key areas of research on health disparities; 3) Provide faculty development through training and mentorship to broaden the base of scholarship in the study of health disparities; and 4) Begin to expand the scientific base of nursing practice by drawing conclusions about the impact of self-management interventions across population groups likely to experience health disparities and disseminating these results.
The Center for Excellence in Chronic Illness CareThe Center for Excellence in Chronic Illness Care was established in 1999 to study the unique experience of chronic illness as it affects patients, families and survivors. The Center's work focuses on multiple areas in which Yale School of Nursing (YSN) faculty has a strong tradition of research expertise. The Center’s ultimate aim is to examine not just specific disease, but the paradigm of chronic illness, the impact that it has on individuals, and the ways that the health care system can better help patients and families manage that impact
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteto achieve a better quality of life. The school’s longstanding tradition of clinical scholarship ensures that the research agenda of this center will be formulated by scholars actively engaged in care and more importantly, scholars who look at problems from a patient-centered perspective. Dr. Melkus is Associate Director of the Center for Excellence in Chronic Illness Care and will facilitate my participation in the Center’s activities.
Computer ResourcesThe School of Nursing maintains a microcomputer laboratory with 26 workstations (Dell GX280). Software available on the network includes statistical programs (SAS, SPSS, nQuery, EpiInfo). One of the computer workstations is equipped with a scanner to enable scanning of documents and images by students and faculty. Several high-speed, high-capacity printers are available in the computer lab. Campus network services have been provided to all faculty. Wireless network access to also available throughout the School of Nursing building and across the entire Yale campus. The network provides faculty and students with access to all of the library resources as well as to the Internet. Faculty and students have access to technical support for computer-related hardware and software issues through the YSN helpdesk and by making appointments with the in-house technical support provider. Help for literature searches and bibliographic software is provided by the School of Nursing librarian. Dr. Shellman will have full access to computer resources for development of the peer training manual.
Media CenterThe School of Nursing building has state-of-the-art audio-visual capability including video projectors, slide projectors and tape recorders, television monitors, and videotaping equipment. All classrooms are fully A-V capable. A full-time audio-visual technician is available to assist faculty and students. Dr Shellman will have full access to our media center for development of her reminiscence training program that includes a video-taped training session.
3. B. Institutional Commitment to Candidate’s Research Career
See letter of support from Dean Margaret Grey on following page.
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliette4. Research PlanThe proposed research plan complements my career development goals and will lead to my scientific career goal to develop and conduct a clinical trial that tests the effects of a culturally appropriate peer-to-peer reminiscence intervention on depressive symptoms in older African-Americans. As I conduct the research described in this proposal I will at the same time be applying what I learn in the training portion of this award particularly as it relates to community based participatory research. I will conduct the research guided by the nine principles of Community-Based Participatory Research (CBPR) proposed by Israel (2005). The goals of CBPR are to increase knowledge and understanding of the given phenomenon, integrate knowledge gained from the community with interventions, and optimally create social change to improve the health and quality of life of the community (Israel, 2005). I will use a modified community-based participatory research approach as described in Section 4. Specifically, in this proposal, the data gathered from participants in Phase 1 (Years 1 & 2) of the research plan will identify the functions of reminiscence in older African-Americans. That data will result in the development of a reminiscence training manual. Subsequently in Phase 2 (Year 3) of the plan, the manual will be evaluated and revised by mentors and participants. Once the manual has been revised, training of peer facilitators will be completed. In Phase 3 (Years 4 & 5) the peer-to-peer reminiscence intervention will be pilot tested for feasibility, and effectiveness on depressive symptoms and reminiscence functions in a sample of community-dwelling older African-Americans.
4.A. Specific AimsThe research aims for this project are:1) To describe patterns and the perceived benefits of integrative reminiscence in community-dwelling older
African-Americans.2) To test the cultural relevance, acceptability, and psychometric properties of the Reminiscence Function
Scale with African-American older adults.3) To describe the functions of reminiscence in community-dwelling older African-Americans.4) To pilot test the community developed reminiscence-training manual for its appropriateness, feasibility, and
acceptability in an older African-American adult community.5) To pilot test the peer-to-peer reminiscence intervention for feasibility and directional effectiveness on
depressive symptoms and reminiscence functions in older community-dwelling older African-Americans (N=24).
4.B. Background, Significance and Rationale
Depression and Older Adults: The Presenting ProblemAccording to the National Institute of Mental Health (2003), an estimated two million of the 35 million older adults in American have a depressive illness and another five million have subsyndromal or minor depression. The consequences of untreated depression in older adults include increased mortality, suicidal ideation and decreased functional abilities (Cook, Pearson, Thompson, Black & Rabins, 2002; Frojdh, Hakansson, & Molarius, 2003). Studies examining the impact of depression on health care costs found that depressed elderly patients have significantly higher health care costs than non-depressed elders regardless of chronic morbidity (Katin, Lin, Russo, & Unitzer, 2003). While late-onset depression may be a common illness among older adults, few receive adequate treatment. It has been shown that older adults who died as a result of suicide, 40% visited a primary care physician within a week before their suicide (Conwell, 2001).
Subsyndromal DepressionSubsyndromal or minor depression is one of the most common types of depression in older adults. Subsyndromal depression is initially defined in the Research Diagnostic Criteria (RDC) as a relatively sustained mood of depression that does not meet the full diagnostic criteria for depressive disorder. When seen as a continuum, an episode of minor depression is often a precursor of major depression. The incidence of significant minor forms of depression increases with age and rises even more so after age 80 (Lavretsky & Kumar, 2003). Minor depression has been estimated to affect 8% to 16% of community-dwelling older adults (Blazer, 2003). The consequences of untreated minor depression are significant. Older adults with minor depression suffer from functional and emotional impairment that affects quality of life and are at increased risk for hospitalization. It has been shown that as many as 10% to 25% develop major depression within the next
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteyear after being diagnosed with minor depression (Hybels, Blazer, & Peiper, 2001; Lyness, Heo, Datto et al., 2006). While minor depression is common in older adults and results have indicated that older adults with subsyndromal should receive interventions to reduce the risk of major depression and functional and emotional impairment (Lyness et al, 2006), there are few randomized control treatment trials that include minor depression. In a review of the literature of the treatment of minor depression Oxman & Sengupta (2002) reported only ten studies that met the criteria for randomized control trial (RCT) inclusion. The evidence, although limited, suggests that antidepressant and counseling have a relatively small benefit, while brief, nonpharmacologic interventions show the largest effect size.
Despite the statistics supporting the prevalence of depression in older adults, there is even less research in the literature on depression and psychosocial well-being among older African-Americans. With the expected increase in the older African-American population, there is a critical need for research on depression with this group of older adults. The United States Census Bureau predicts that by the year 2030, African-American elderly will represent the highest number of minority elders in the United States. In a review of the literature of depression, mental health, and psychological well-being among African-American elders, Mills (2000) reported major gaps in the literature. Few studies were found addressing antecedents and consequences of depression symptoms in older black men and women, and interventions to decrease major depression. Studies of brief therapies for depression have not included adequate samples of ethnic minority patients to evaluate their effectiveness (U.S. Department of Health and Human Services, 2001). There is also a call for more aggressive screening, identification and treatment of depression in African-American elders (Skarupski, Mendes de Leon, Bienias, Barnes, Everson-Rose, Wilson, & Evans, 2005). Recent studies have shown that African-American elders are less likely to be identified as depressed (Gallo, Bogner, Moreales, & Ford, 2005) and find counseling and anti-depressant medication less acceptable than whites (Cooper, Gonzales, Gallo, Rost, Meredith, Rubenstein, Wang, & Ford, 2003). The roots of these health disparities that present today in many African-American communities can be traced to racism and socio-economic consequences of slavery and sharecropping that left a majority of African-Americans powerless and economically disadvantaged. The inability to obtain jobs with good pensions and health benefits has left many older African-Americans without access to the health care system. Additionally, a general mistrust of white health care professionals, particularly in the mental health arena, has resulted in reduced access and use of these services. Lack of access to mental health services for older African-Americans in addition to the prevalence of subsyndromal depression in older adults, and existing gaps in the literature related to treatment protocols for minor depression support the need for the development and testing of a cost-effective, sustainable, and culturally-appropriate peer-to-peer reminiscence intervention for older African-Americans.
Reminiscence: The Proposed InterventionReminiscence can be defined as the recollection of past experiences. In 1963 Robert Butler postulated that reminiscence in older adults was part of a normal life review process brought about by the realization of approaching death. It is characterized by the progressive return of past experiences to consciousness and the resurgence of unresolved conflicts for reexamination and reintegration. This process may take place individually, occur silently, or be conducted as part of a group process. However, it is enhanced in the presence of a supportive listener. If the reintegration is successful, reminiscence can give new significance and meaning to life and prepare the person for death by diminishing fear and anxiety. Based on Erikson’s eighth stage of psychosocial development ego-integrity versus despair, Butler proposed that unsuccessful reexamination of memories accounted for late-life depression, while those individuals who were able to come to terms with past events attained ego-integrity and a sense of self-worth. Both Butler (1963) and Erickson (1959) regard reminiscence as a core process of the final stage of one’s life.
Reminiscence ResearchReminiscence research is in its beginning stages. Since Butler first writings on the functions and process of reminiscence in 1963, there has been a great deal of literature describing the therapeutic effects of using reminiscence with older adults. More recently, there has been an increased interest in examining the effects of reminiscence on quality of life outcomes such as decreasing depressive symptoms and increasing life satisfaction and self-esteem (Haight & Webster, 2002). Unfortunately, many studies are plagued with poor methodology (Shellman, 2006) and inconsistencies in the types of reminiscence used as the intervention. In a
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliettereview of the literature of the effects of reminiscence on depression Hseih and Wang (2003) found inconclusive results due to small sample sizes, lack of a clear definition of reminiscence, and variations in treatment protocols. Similarly, in a meta-analysis of the effects of reminiscence on depressive symptoms conducted by Bohlmeijer, Smit, & Cuijpers (2003) very few high quality studies were found that met the criteria for inclusion in the meta-analysis they conducted. However, descriptive results from the analysis indicate reminiscence to be a potentially effective treatment to decrease depressive symptoms especially in community-dwelling older adults. The authors recommend that the findings need to be confirmed by randomized control trials using rigorous designs and methods. Findings from these research reviews on the therapeutic effects of reminiscence have been contradictory and demand the need for a more rigorous approach in future studies.
To improve outcome studies, reminiscence researchers and scholars have been striving to develop a taxonomy of the kinds of reminiscence and their functions. Reminiscence has been grouped into as few as two types (Romaniuk & Romanuik 1981) and as many as six types (Watt & Wong, 1991; Webster, 1993). For instance, Romaniuk and Romaniuk (1981) grouped reminiscence as intrapersonal and interpersonal. Intrapersonal, was described as a private process and more evaluative in nature while interpersonal reminiscence was identified as conversational and a social process. Watt and Wong (1991) identified a taxonomy of reminiscence that included six different types. Their taxonomy includes: 1) integrative reminiscence when there is acceptance of self and others and integration of the past and present; 2) instrumental reminiscence, defined as drawing from past experiences to solve present day problems; 3) transmissive reminiscence, similar to storytelling and oral history when there is a sharing of personal wisdom from one generation to another; 4) escapist reminiscence, referred to as defensive reminiscence occurs when one seeks comfort from people and events; 5) obsessive reminiscence, characterized by persistent rumination of unpleasant events often accompanied by feelings of guilt, shame and resentment; and 6) narrative reminiscence, having more of a descriptive nature, consisting of the recounting of past events without interpretation or evaluation. The development of this taxonomy has led to work on the specific functions of reminiscence in order to understand the therapeutic effects that clinicians observe as they facilitate reminiscence with older adults, and improve outcome studies.
The Functions of ReminiscenceIn 1993, Webster developed and tested the Reminiscence Functions Scale (RFS) that allows for the measurement of eight functions of reminiscence identified as: 1) identity, 2) problem-solving, 3) teach/inform, 4) conversation, 5) boredom reduction, 6) bitterness revival, 7) death preparation, and 8) intimacy maintenance. The RFS, a 43-item scale, is designed to measure all of the stated reminiscence functions across the life span. Item generation and subsequent testing were performed on mostly Caucasian, Canadian populations across the life-span with ages ranging from18-67, with an average educational level of 12.5 years (Webster 1989; 1993). In 1997, Webster conducted a replication and validity study of the RFS with 399 subjects ranging in ages from 17-45. Internal consistency score on each function or subscale ranged from .74 to .86. (Additional information regarding the items and responses can be found in the instrument section of the research plan). The sample for the 1997 study included students from Langara College in Canada. Although the sample was identified as “demographically diverse”, no race information is provided. While examining the functions of reminiscence has been a major topic in reminiscence research, little research has been conducted on the functions of reminiscence in older African-Americans. In a personal conversation with Jeffrey Webster (2006), he acknowledged the limitation of the homogenous samples, he stated, “you have my permission to use the scale. This would add to the reminiscence literature as there has been little psychometric testing with different ethnic groups.” The development of the RFS is the first step in reminiscence researchers’ attempts to specifically define the function of reminiscence and improve the quality of intervention studies. Subsequent empirical research has examined the functions of reminiscence in relation to stress, personality, attachment, and psychological functioning. For instance, Cully, LaVoie, Gfeller, (2001) found that depressed and anxious older adults commonly use reminiscence more frequently and would be appropriate candidates for a reminiscence intervention. Molinari, Cully, Kendjelic, & Kunikk, (2001) found positive correlations between extroverted older adults and Conversational reminiscence and openness personality type with Identity and Problem-solving reminiscence functions. These studies led to Dr. Cappeliez’s work and interest in the association between reminiscence and mental health. In a study( N=420) that examined the extent to which different functions of reminiscence predict life satisfaction and psychiatric distress in later life,
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliettereminiscing for Conversation and for Death Preparation were associated with positive mental health while reminiscing to relieve Boredom and for Intimacy Maintenance were associated with greater psychiatric distress (Cappeliez, O’Rourke, & Chaudhury, 2005). More recently, these findings were further validated in a study that examined the adaptive nature of reminiscence with respect to mental and physical health in older adults (N=412). It is important to note that both studies were conducted via the Internet with the majority of respondents residing in New Zealand and Australia. Dr. Cappeliez has agreed that this proposed research involving older African-Americans will greatly inform the reminiscence literature and assist with examining the adaptive functions of reminiscence in older adults in relation to mental health (personal communication, Nov 1, 2006).
Conceptual FrameworkMy program of reminiscence research is based on the theory of Cognitive Adaptation (O’Rourke, 2002). According to this theory, the way that people interpret their interpersonal relations and life histories is significantly associated with wellness in later life. The key construct of the theory is “cognitive reconstruction.” Individuals are helped to think differently about a phenomenon. For example, positive interpretation of memories is associated with positive well-being. It is hypothesized that facilitating the reminiscence process with an older adult by a supportive listener and validating the older adult’s life experiences, acknowledging past coping skills, and emphasizing accomplishments will assist the older adult to develop a sense of self-worth and attain ego-integrity through a positive recollection of experiences. This process decreases feelings of regret, despair and depression. Therefore, it is important that the facilitator be trained to conduct reminiscence to encourage the older adult to interpret his or her experiences in a positive way. The specific type of reminiscence used in my program of research is interpersonal and integrative reminiscence. This type of reminiscence is implemented because it is reflective and can give the participants a chance to review their experiences and increase their self-worth and self-esteem as they tell stories of past accomplishments and coping methods (Wong & Watt, 1991) in the presence of a supportive listener.
Baker (1994) proposed that the use of a reminiscence approach with older African-Americans enables health care professionals to learn the older adult’s personal history, identify coping mechanisms and resources for positive mental health strategies. However, little research has been conducted to validate these propositions. My program of research has been focused on the use of integrative reminiscence as a positive mental health intervention to decrease depressive symptoms in older African-Americans. The following section describes preliminary work that has led me to the need for and development of this K01 career development award.
4 .C. Preliminary Studies
The Effects of a Reminiscence Education Program on Baccalaureate Nursing Students’ Eldercare Cultural Self-Efficacy (Funding: Sigma Theta Tau Mu Chapter)This pilot study tested the effects of a reminiscence education program on BSN students’ cultural self-efficacy in caring for elders. An interrupted time series design with a nonequivalent no-treatment control group was used with 64 nursing students recruited from a northeast university in the United States. The intervention consisted of a two-hour reminiscence education program and a 13 week period in which the experimental group implemented integrative reminiscence with elders during their community health practicum. The Eldercare Cultural Self-Efficacy Scale (Shellman, 2006) was the outcome measure. Results indicated that students receiving the reminiscence education program demonstrated significantly higher levels of eldercare cultural self-efficacy F(1, 62) = 5.34, p = .024 than those not receiving the intervention. Teaching nursing students to facilitate integrative reminiscence improves their confidence in caring for older adults of different ethnic backgrounds. This is the first study to report such findings. Results have been presented as a paper at the ENRS Annual Conference as well as the annual University of Connecticut Research Conference. A manuscript describing the findings has been published in Nurse Education Today (2007).
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliette“Making a Connection” Baccalaureate Nursing Students Perceptions of Reminiscing with Older Adults The purpose of this qualitative study was to investigate the phenomenon of nursing students’ experiences reminiscing with elders. The study used a qualitative approach within a survey design. Students (N= 41) completed the survey at the end of a 13-week period in which they reminisced with older adults during home visits. Editing Analysis Style (Crabtree & Miller, 1999) was used to analyze the data. Three major themes emerged: 1) Making a Connection, 2) Seeing the World through their Eyes, and 3) Benefits of Reminiscence. This study supports previous works showing that reminiscence can provide an opportunity for healthcare professionals to learn about and appreciate the life of the individual as well as to gather information regarding psychological factors, health beliefs, coping skills, and cultural perspectives (Shellman 2001, 2004; Soltys and Coats, 1995). Reminiscing with elders provided a way for theses students to make a connection with their clients. This connection led to student reflection, a deeper understanding of the elder culture, and allowed the students to view elders in a different light. This manuscript is published in Journal of Nursing Education (2006)
Understanding Life Experiences of African-American Elders (Funding: American Nursing Foundation)The primary purpose of the study was to increase the knowledge available about the cultural heritage, worldviews, and life experiences of African-American elders. It was important to observe the participants’ acceptance of reminiscing with a white researcher as the facilitator. Using an interpretive phenomenological design, reminiscence interviews were conducted with older African-Americans, from a northeast urban community, until saturation was reached (N=7). Data were analyzed using Speigelberg’s phenomenological method. The following themes emerged: 1) nobody ever asked me before, 2) stories of discrimination, 3) coping with discrimination, 4) the hurt of discrimination, and 5) positive self-discoveries. This study was undertaken to obtain groundwork for conducting a reminiscence intervention study with this population. The following conclusions were derived from the contextual data collected during and after the interviews: 1) the reminiscence interviews allowed for trust to develop between the participants and myself, 2) the participants enjoyed the reminiscence experience and were able to identify positive coping strategies, 3) the process of reminiscence can inform nurses about the cultural heritage, worldviews, and life experiences of African-Americans and improve the nurses’ ability to deliver culturally competent care to this population. These data provided important groundwork for the next preliminary study. My clinical work informed me about the issues of depression in community-dwelling older adults, this study gave me insight into facilitating reminiscence and learning about the life experiences of older African-Americans. The next phase of my program of research was to test an integrative reminiscence intervention on depression and life satisfaction in community-dwelling older adults.
The Effects of a Structured Reminiscence Intervention on Depression and Life Satisfaction in older African-Americans (Funding: John A Hartford Foundation & University of Connecticut Research Foundation)This pilot study was conducted to assess the feasibility of conducting a reminiscence intervention study with older African-Americans. My role as a visiting nurse had enabled me to gain access to churches and senior centers in the Central Connecticut area by conducting blood pressure clinics at these sites. The specific aims were: 1) to measure the effects of an integrative reminiscence intervention on depression and life satisfaction in older African-Americans, 2) to describe the meaning of depression in a sample of older African-Americans, and 3) to identify what aspects of integrative reminiscence such as number and length of sessions that may contribute to decreased levels of depressive symptoms and increased life satisfaction in African-American elders. Since the reminiscence literature had shown inconclusive results due to poorly designed studies, steps were taken to ensure treatment fidelity, a sound research design (see Table 2), and the hiring of African-American research assistants to collect data and conduct the intervention. Pre and post data were collected using the Center for Epidemiological Center Depression Scale and the Life Satisfaction Index Scale. Both scales have been shown to be highly reliable with African-American older adults (Baker, Velli, Friedman, & Wiley, 1995; Rao, VN. & Rao VV, 1982).
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteTable 3. Research Design for The Effects of a Structured Reminiscence Intervention on Depressionand Life Satisfaction in older African-Americans
Group (randomized)
Pretest 1 Intervention Postest1 Postest2
Treatment(n=20)
On admissionfollowing consent form completion
Reminiscence8 weeks/1 session a week
immediately after session 8
30 days afterPosttest 1
Control(n=20)
On admissionfollowing consent form completion
Health Education 8 weeks/1 session per week (HP)
immediately after week 8
30 days afterPosttest 1
Control(n=20)
On admission Following consent form completion
None(will have choice of treatment after Posttest 2
immediately after week 8
30 days afterPosttest 1
Quantitative Results (Preliminary Findings)A total of 61 participants originally consented to be in the study. Three participants were referred to mental health services provided at the senior center. Four participants dropped out after the first data collection for the following reasons: 1) not enough time, and 2) “I’m not depressed”. One participant was hospitalized and the two others were in the health education groups and felt that they didn’t need any more education. Current preliminary findings for the effectiveness of reminiscence on CES-D scores indicate a decrease in scores (depressive symptoms) pre and post intervention (see Table 3). However, it is difficult to make generalizations as data are still being collected.
Table 4. CES-D Pre-Post Test MeansGroup CES-D Score Pretest
MeansPosttest 1
MeansPosttest 2
MeansReminiscence Group 11.2 (S.D. 8.1)
N=196.8 (S.D. 6.8) 8.5 (S.D. 5.0)
Health Education Group 11.5 (S.D. 7.5)N=15
10.5 (S.D. 7.3 10.5 (S.D. 7.3)
Traditional Control 9.5 (S.D. 10.3)N=17
12.8 (S.D. 9.4) 11.9 (S.D. 10.2
Qualitative Results (Findings)
“Keeping the bully out.” The Meaning of Depression in a Sample of African-American EldersThe purpose of this study was to examine the meaning of depression in African-American elders using a qualitative approach embedded within a survey design. The purposive sample included African-American elders (N=51) over the age of 60 born and living in the United States. Participants were recruited from senior centers and senior housing sites in a Northeast state. Data were collected through semi-structured interviews conducted by African-American research assistants. The participants’ descriptions of the meaning of depression were analyzed using Crabtree and Miller’s Editing Analysis Style. Four major themes emerged from the data: 1) “Keeping the Bully Out.”, 2) “God will provide.”, 3) Losing Control and 4)”That’s not me.”. Participants perceived depression as something that can be controlled and they associated it with negative connotations such as seeing depression as “a bully” and considering it not an illness, but a weakness. This suggests that under-diagnosis and under-treatment may be related to the failure by African-American elders to seek care for depression because they do not view it as a medical problem, but rather as a personal weakness that can be overcome. Results from this study were presented as a poster at the 59th Gerontological Society of America’s conference and a manuscript describing the results is currently being revised for publication in the Journal of the American Psychiatric Nurses Association. Since this was a feasibility study, evaluative data were collected throughout the study to inform the next phase of the research process. The following reports highlight these data.
Experiences and Methodological Considerations in Conducting Mental Health Research in Older African-AmericansThe specific aim of this study was to identify both positive and negative issues for conducting reminiscence research with older African-Americans. Process evaluation consisting of journals, debriefing sessions with research assistants, and survey data were used to identify successes and challenges associated with
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteconducting the study. Primary challenges of conducting this study included recruitment and retention of older African-Americans into the study, as well as the recruitment and retention of African-American research assistants. Even though my role as a visiting nurse had enabled me to gain access to churches in the Central Connecticut area by conducting blood pressure clinics at the sites, gatekeepers for churches and senior centers were hesitant to participate in a study that dealt with a mental health problem. Issues such as mistrust of a white researcher, the stigma of depression, age difference between the African-American research assistant and participants emerged immediately. While some of these challenges were expected and prepared for by recruiting African-American nursing students and engaging the research assistants as partners to create a team approach to the research study, there were challenges in retention of these nursing students due to: 1) nursing curriculum demands, 2) family responsibilities, and 3) leaving the study for full-time employment. Despite weekly debriefing meetings and a team approach to conducting research, two research assistants had to leave for personal reasons, two graduated and went on to full-time employment and four others although they were interested, could not commit because of nursing curriculum demands. These challenges led to the hiring of an older African-American professional to collect data and assist in recruitment for the study and an African-American Ph.D. student from the University of Connecticut with more experience and interest in research. From the beginning of their participation in the study, recruitment and retention improved. Also, during this period I contacted and met with Dr. Terry L Mills at the University of Florida to discuss participant and African-American researcher recruitment and retention issues. It was during that meeting that we began the discussion of using CBPR approach to research with African-Americans, peer reminiscence strategies and the development of a career development award. A paper entitled The Experiences and Methodological Considerations of Conducting Mental Health Research with African-American Elders was presented as a paper at the Gerontological Society of America’s 58th Annual Conference. My research assistants will be presenting these data at the 19th Eastern Nursing Research Society Conference in April 2007. A manuscript describing this experience is in development.
Conducting Reminiscence with Older African-Americans: A Researcher’s ExperienceThe reminiscence facilitators kept a reflective journal throughout the intervention study. The aims were to document personal experiences of reminiscing and progress in conducting reminiscence with older African-Americans. This journal was used during our weekly debriefing meetings and for evaluation of the 8-week reminiscence intervention. The research assistant has been able to identify through journaling the following benefits of reminiscence: 1) that trust was developed as a result of the reminiscence sessions, 2) the participants enjoyed the experience, 3) participants were able to identify important lifetime coping strategies, 4) there are benefits for the reminiscence facilitator with regard to learning about the life of the individual, and 5) termination of the sessions was difficult because of the relationship developed through reminiscence. Results demonstrate that reminiscence is an intervention to increase trust between the researcher and participant and there are benefits for all involved.
SummaryThe disparities affecting mental health care of minorities are the result of minorities having less access to mental health services, receiving poorer quality of care, and being under-represented of in mental health research. Specifically, African-Americans are more likely to be underdiagnosed and under-treated for depression than other ethnic groups (Das, Olfaon, McCurtis, & Weissman, 2006). My preliminary research work has provided evidence that integrative reminiscence is an intervention that can have benefits for both the person facilitating the reminiscence and the older African-American reminiscing. Healthcare providers learn about the cultural perspectives of the individual, life histories, and coping strategies and “make connections” with the older adult, while older adults begin to feel positive about themselves and begin to realize their accomplishments. Through the experience of conducting my most recent pilot study work, trends indicate that a reminiscence intervention can decrease depressive symptoms. However, the issues of mistrust, age differences between participants and research assistants, and resistance to participation in mental health studies has led me to conclude that creating a sustainable reminiscence intervention program would require a new approach centered on increased community participation. Peer-to-peer interventions have been shown to be effective approaches with African-Americans in diabetes management (Samuel-Hodge, Keyserling, France, Ingram, Johnston, Pullen, Davis & Cole (2006), weight loss (Kennedy, Paeratakeul, Champagne, Ryan, Harsha, Johnson, Deyhim, Forsythe & Bogle (2005) and to increase prostate cancer screening (Weinrich,
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteBoyd, Weinrich, Greene, Reynolds & Metlin, 1998). In this proposal, the development and testing of a peer-to-peer integrative reminiscence intervention using a modified community based participatory approach is described.
4.D. Research DesignCommunity-Based Participatory ResearchA modified community-based participatory research approach will be used to engage the communities as partners and develop the reminiscence intervention. The reason for choosing this approach is to mitigate against the factors that have resulted in reluctance among African-Americans to participate in research studies. These factors include a history of discrimination, negative experiences with healthcare and research, and cultural differences (Dennis & Neese, 2000). Based on my preliminary work, these factors do exist. My experiences have shown that ministers and families of older adults act as gatekeepers to protect their members because of lack of trust in the researchers and research process. While stricter safeguards have been implemented in recent years to protect human subjects, these safeguards have not erased the fear among African-Americans that they may be taken advantage of for the sake of research. Additionally, many research studies do not look at the strengths of African-Americans to overcome health disparities, instead research is undertaken to see how they are different from Whites (Rooks & Whitfield, 2004). It is assumed that this research proposing a peer to peer reminiscence intervention focuses on the strength of the African-American oral traditions. The major functions of folklore and storytelling include cultivating a harmonious African-American community, sustaining their unique cultural identity, and by enabling people to have a clearer picture of their situation and options available to them through empowerment (Cannon, 1995; Stewart, 1997).
Community-based participatory research (CBPR) is an interactive approach between researchers and participants from a given community that allows data and information to flow back and forth between these two entities. The aim of community-based participatory research is to increase knowledge and understanding of a given phenomenon and use the knowledge gained with interventions to improve the health and quality of life of the community (Israel, Eng, Schulz, & Parker 2005). I am using a modified CBPR approach in which participants of the community will provide information in the development of a reminiscence intervention and I will provide feedback, information and education as needed about such topics as confidentiality, protection of human subjects and the community, and depression and mental health issues in older adults to promote community capacity building and improve health. Benefits of using CBPR are that the research topic: 1) reflects concerns of the community, 2) enhances the relevance and application of the research data by all stakeholders, 3) brings partners with different skill levels, knowledge and expertise together to address complex issues, 4) increases the quality, validity, sensitivity, and practicality of research by incorporating the knowledge of the participants, and 5) increases the possibility of overcoming the mistrust of research that regards communities as “subjects” (Israel et al. 2006).
Israel identified 9 guiding principles of CBPR that underpin this design. They are as follows: 1) recognize the community as a unit of identity, 2) build on the strengths and resources of within the community, 3) facilitate a collaborative and equitable partnership, 4) foster co-learning and capacity building, 5) achieve balance between knowledge generation and intervention for mutual benefit for all partners, 6) focus on local relevance of public health problems, 7) develop systems using a cyclical and iterative process, 8) disseminate results to all partners and involve them in wider dissemination of results, and 9) commit to long-term process and sustainability. Figure 1 identifies my research plan and the community structure and functions that will guide the research and develop sustainability of the reminiscence intervention. It is important to note the following: this community structure is already in process in the Hartford area; therefore research will be conducted in Hartford to facilitate Phase 1. Phases 2 and 3 will be conducted in the New Haven area to ensure treatment fidelity and avoid contamination of the pilot clinical trial. Both Dr. Melkus and Dr. Knobf have established relationships with African-American groups and will assist me to enter the New Haven community. The community structure and functions will continue in Hartford. The training of facilitators to implement the peer-to peer reminiscence program in Hartford will begin after the pilot study in New Haven is finished.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteFigure 1. Overview of Research Plan
Community Participatory Structure and Functions
1) Develop/Sustain Collaborative Partnerships (stakeholders and participants)
Build on strengths 2) Provide Consultation
Consent forms/Instruments/Ethical Issues Reminiscence Facilitator Recruitment Community Mental Health Resources
3) Study Feedback/Dissemination/Program Evaluation Foster co-learning, build on resources
4) Sustain program after Year 5. Develop support systems
Key
Indicates linear relationship
Indicates continuous interactive relationship
Limitations of Community-Based Participatory ResearchAlthough there is an increase in interest in the literature regarding the CBPR approach to research many investigators have not received direct training or opportunities to strengthen their skills in this area (Israel et. al, 2006). This lack of training poses limitations for its use that include institutional constraints that encourage investigators’ independence and thus favor “solo” investigatory approaches as well as single-author publications and differing emphases on goals, values, and priorities between the institution and community (Schensul, 2006). Yale School of Nursing has expressed commitment to this career development award (see Dean’s letter of support) which will provide the training and mentoring I need to become an expert in CBPR. Another possible limitation is that I am a white researcher. Shared group membership has been described as a way of facilitating discussion and disclosure of sensitive topics (Jackson, 1991) and inclusion of researchers who belong to the ethnic group under study has the potential to reduce the threats to a valid research process (Porter & Vallarruel, 1993). One African-American research assistant will be hired to assist with data, collection, focus groups, and recruitment. The following section describes the 3 Phases of the research plan with careful considerations given to the limitations that can occur in this type of research approach.
Focus Groups – 6 groups of 8 (N=48) 1) Describe perceptions of reminiscence. 2) Test cultural relevance, readability, acceptability of Reminiscence Function Scale. 3) Modify as needed. 4) Collect psychometric data (N= 300) 5) Analyze focus group and RFS data.Develop reminiscence training manualRecruitment of peer reminiscence facilitators for Phase 2.
Phase IIYear 3
1) Testing of training manual with facilitators (N=10) for acceptability, appropriateness, and feasibility. 2) Revise as needed. 3) Training of peer reminiscence facilitators. 4) Recruitment of participants for Phase 3.
Phase IIIYears 4 and 5
1) Pilot test for feasibility and directional effectiveness of the peer-to-peer reminiscence program on depressive symptoms and reminiscence functions in older African- Americans (N= 24).2) Analyze data 3) Develop R- Series for RCT.
Principal Investigator/Program Director (Last, first, middle): Shellman, JuliettePhase I. Gather data regarding the functions and perceived benefits of reminiscence in older African-Americans and develop the peer-facilitated training manualThe purpose of Phase 1 of the research plan is to gather pertinent data to develop a culturally appropriate reminiscence peer-training manual. Data gathered in Phase 1 will inform the next steps of the research plan: testing the manual, training of the facilitators, and pilot testing the feasibility and effects of the intervention on depression and reminiscence functions in older African-Americans.
Research Aims1) To explore the meaning and perceived benefits of integrative reminiscence in community-dwelling older
African-Americans.2) To test the cultural relevance, acceptability, and psychometric properties of the Reminiscence Function
Scale with older African-Americans.3) To describe the functions of reminiscence in community-dwelling older African-Americans.
MethodsSetting: This study will take place in senior communities an urban center located in the northeast section of the United States. One church and two senior centers whose participants are African-American and Caribbean Black will compose the participating communities. The majority of the people attending these churches come from a blue-collar working class population with an average of 10.2 years of education (Shellman, 2006). The total estimated membership including the three settings is (N= 850). This will allow for a sufficient population from which to draw samples for focus groups and psychometric testing of the Reminiscence Function Scale.Participants: Participants who are interested in and willing to share their thoughts and opinions about reminiscence and the Reminiscence Function Scale must be African-American, English speaking, intact cognition, and over the age of 55. In this study, African-American is defined as persons having origins in any of the Black racial groups of Africa.
ProceduresHiring/Training of Research Assistant: The hiring and training of one African-American research assistant will begin early in year 1. The research assistant will be trained in human subjects’ protection, data collection, community-based principles, and interview techniques. Methods used to train the research assistant will be: 1) directed readings with discussion, 2) role-playing activities with PI feedback and 3) weekly debriefing sessions will be held to ensure the integrity of data collection, treatment fidelity, and for progress reports. Although the hiring and training will begin early in Year 1, it is expected that this process will occur throughout the five-year period as situations occur such as graduation and other life events. Consent for Participation: Participants should have the full capacity to consent. Based on the PI or research assistant assessment, the client will receive mini-mental status examination if suspected to be cognitively impaired. The Short Portable Mini Mental Exam (Pfeiffer, 1975) will be used because it has been found to be useful in identifying cognitive impairment in older African-Americans. Large print surveys will be distributed to visually impaired clients or they will have the surveys read to them. Hearing impaired clients will be given written materials that cover both consent and information regarding the study. In order to answer further questions, written communication will be used. Individual consent forms will be developed for any member of the community who is willing to participate either as a key informant, in focus group, or as a reminiscence facilitator. The participants will be informed that they are free to withdraw from the study at any time. This study will be reviewed by Yale School of Nursing’s Human Subjects Research Review Committee. The community sites do not have review boards, but letters of permission will be provided from the advisory groups formed at each site. This is described in detail in Section E Data Collection: Participant observation, key informant interviews, and focus groups will be used to gather data from the participants at each site for Aims 1, 2, and 3. Data will be collected in the form of field notes, reflective journaling, taped interviews and through administration of the Reminiscence Functions Scale. Interview guides for the focus groups and key informant interviews will be developed with the assistance of Drs. Melkus, Lichtenberg and Schensul. Dr. Melkus and Dr. Schensul will provide guidance for participant observation as well as debriefing sessions as needed for me to discuss the experiences. I will meet weekly with the research assistant to debrief him or her and provide guidance.Instruments: A demographic data form, developed by the PI, will be completed by the participants. The Reminiscence Functions Scale (RFS) developed by Webster (1993; 1997) will be reviewed by focus groups for PHS 398/2590 (Rev. 09/04, Reissued 4/2006) Page 34 Continuation Format Page
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteacceptability and use with members of this population. This scale has been found to be reliable and valid with certain homogenous populations. The purpose of the RFS is to measure how often an individual reminisces with a certain function in mind: 1) identity, 2) problem-solving, 3) teach/inform, 4) conversation, 5) boredom reduction, 6) bitterness revival, 7) death preparation, and 8) intimacy maintenance. The stem “When I reminisce it is….” is followed by items such as “to transmit knowledge that I’ve acquired to someone else.” There are six responses ranging from 1 = never to 6 = frequently. The eight factor, 43 item scale was found to have an internal consistency ranging from .74 to .86. Gable (1993) recommends alpha levels in the high 80’s as typical for good instruments. There will be a two-step process for collecting data on the Reminiscence Functions Scale. First, the scale will be presented to the focus groups for their feedback regarding acceptability, readability, and cultural relevance for use with older African-Americans. Each item will be reviewed. Modifications will be made as necessary from the data gathered from the focus groups. Then, the modified RFS will be administered (N=300) to gather reliability and validity data. Table 5 identifies the data collection approaches that will be used in Phase 1 and is followed by a detailed description of each approach.
Table 5. Community-Based Participatory Research Approaches and Data Collection for Phase 1CBPR Approach Data Collection
MethodsData Collected Mentors
Participant Observation
Field NotesAttend senior center functions; lunches, social gatherings, church group meetings
Is reminiscence part of the community culture?Where and when does reminiscence occur?Who reminisces with whom? Where do they reminisce? Does reminiscence occur spontaneously?Does reminiscence occur more often in some activities than others?
SchensulLichtenbergMills
Key Informant Interviews
Informal interviews, discussing and observing.Formal Interview.
History and culture of community/Social GroupingsRelationships with other agencies.Perceived barriers to reminiscence project. Current health programs.Suggestions for appropriate peer reminiscence facilitators.
SchensulLichtenbergMills
Focus GroupsChurch members
Senior center members
Interview guide developed by PI.Field notesAudio-taped sessionsReminiscence Function Scale
Research Questions1) What are older African-Americans perceptions of the benefits of reminiscence?2) Is the Reminiscence Function Scale culturally appropriate and acceptable to older African-Americans?3) What are psychometric properties of Reminiscence Functions Scale with older African-Americans?
MelkusCappeliez
Participant Observation: The framework of Bogdewic’s (1999) method of participant observation will be used by the PI to observe behaviors and establish rapport by participating in activities in the churches and senior centers. The advantages to using participant observation to investigate cultural groups are: 1) in time the participants are less likely to alter their behavior due to your presence, 2) differences between real and verbal behavior become apparent as the information the PI obtains from interviews may not reflect actual behavior, 3) questions can be formed in the language of the participants, and 4) the richness and complexity of the human condition can be more fully understood and appreciated (Bogdewic, 1999). Activities such as blood pressure clinics, bingo, lunches, craft workshops and meetings will be attended by the PI and research assistant. (Drs. Lichtenberg, Schensul, and Mills will provide guidance.)Key Informant Interviews: Key informant interviews can assist in understanding cultural differences in health and disease concepts, development of interventions, and identifying community resources (Gilchrist & Williams, 1999; Israel, 2006). In this study, key informants will share information regarding the history of their respective institutions, barriers or strengths of their communities for the use of peer-to-peer interventions, and relationships with other health service organizations. The key informants will be helpful in identifying reminiscence facilitators as well as other key informants within the organization to enhance understanding of the cultural group. It is expected that key informants will include but will not be limited to pastors, pastors’ wives, senior center directors, senior center nurses, and other members of the organizations. These informants will be identified by asking other key informants who would be an appropriate person to interview. These interviews will be conducted until saturation of data is reached. (Drs. Lichtenberg, Schensul, and Mills will provide guidance).
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteFocus Groups: Focus group methodology will be employed to determine participants’ perceptions of reminiscence, and the appropriateness, acceptability, reliability, and content validity of the Reminiscence Function Scale as well as to evaluate the acceptability and feasibility of using the reminiscence training manual. The value of using focus groups with African-Americans has shown to identify beliefs and practices African-American women with type 2 diabetes (Maillet, D’Eramo-Melkus, & Spollett, 1996) and to develop diabetes prevention program for African-American church groups (Boltri, Davis-Amith, Zayas, Schellneberg, Seale, Blaloch, & Mbadinuju, 2006). The focus groups will be conducted by the PI and the African-American research assistant who has been trained by the PI. Participants will be recruited through key informants, flyers, and through presentations at various meetings at each site. Focus group size has been recommended to be between 6 -12 participants while numbers of focus groups in the study is recommended to be between 4 -12 (Brown, 1999). It is expected that at least 6 focus groups with 8 members in each will participate in this study.Dr. Melkus and Dr. Cappeliez will provide guidance).Data Analysis: Key informant interviews, focus groups and the participants’ descriptions of their perceptions of reminiscence will be analyzed using an immersion-crystallization approach as described by Borkan (1999). This approach consists of cycles where the data analyst immerses herself into and experiences the data. The approach involves a systematic iterative process, a going back and forth of text interpretation and categorization. The immersion aspect of this technique will be conducted by two researchers reviewing the transcripts for each interview and focus group and listening to the audiotape to enhance the written word for the nuance and tone. Facilitator notes will be reviewed for insights that are gathered during the interview or focus groups. During the reading and rereading of transcripts, each reviewer will search for meaningful segments of information related to the research questions. The researchers will come together to discuss their independent findings and establish codes through discussion and agreement. The codes are developed based on the frequency, intensity, and consistency of meaningful segments. From the meaningful segments, common themes or exemplars are developed. The findings and decision trail will be reviewed by one researcher not involved with the study, but with experience in immersion crystallization techniques. Finally, the results will be discussed with the participants. Qualitative data will be analyzed using Atlas.ti 5.08. (Dr. Knopf will provide guidance with qualitative data analysis).Qualitative Rigor: To ensure the validity of this study, reflexivity, depth of description, accuracy, and searching for alternative interpretations will be undertaken (Borkan, 1999) throughout data collection and analysis. The researcher will practice reflexivity throughout the study. This technique involves reflecting on how one’s role influences the data and analysis. The PI and research assistant will journal and debrief each other to promote the process of reflexivity. Avoiding premature conclusions, reviewing data to ensure that the questions and issues were explored will enhance the depth of description. Accuracy of the results will be assessed by reporting the findings to the participants and asking for feedback. The investigators will review results to be sure that the iterative process was undertaken and alternate interpretations were examined. Dr. Schensul and Dr. Melkus will guide me during this process to ensure that the steps to this approach were taken.Quantitative Data Analyses: Descriptive statistics regarding demographic data and Reminiscence Functions Scores will be collected from participants. Quantitative analysis such as calculation of means, standard deviations and Cronbach’s alpha for reliability will be calculated using SPSS 14.0. Sample size for reliability analysis should be at least 5 times as many subjects as items or at least 200 to 300 respondents whichever is largest (Nunnally, 1978) and at least 5-10 per item for a confirmatory factor analysis (Cattell,1978; Nunnally, 1978). For the purpose of this study, 325 participants will be sought so that there will be at least a 7:1 ratio of observations versus number of items.Data Management: The RA’s will provide me with written data, and I will verify and supervise the entry of written data. All data will be saved to the server (backed up daily). Server access is protected through limited right of entry and passwords. All data will be stored in a locked office in a locked cabinet at the school of nursing. I will review printouts of data files, conduct preliminary analysis periodically, and identify issues requiring the help of the statistician. The anonymous data will be shared with the participants on a continual basis for review and modifications, as necessary, before external dissemination.Training Manual Development: Data collected from the focus groups, key informants, participant observations, and the Reminiscence Functions Scale will provide information to develop an integrative reminiscence intervention that includes a training manual for peer reminiscence facilitators. It is expected that the training manual will include an integrative reminiscence education curriculum including role-playing activities, questions to facilitate reminiscence with peers, techniques for identification of who may not be
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteappropriate for reminiscence, maintaining confidentiality, a list of mental health community resources for referrals if needed and an evaluation for the facilitators to complete after training. These items may change during the process of development of the manual and with consultation from Dr. Cappeliez and Dr. Evans. The first level of evaluation will be periodic process reviews of the manual by Drs. Lichtenberg and Schensul to ensure that I take the appropriate community-based participatory methods towards the development of the manual. Dr. Evans will review the manual for its appropriateness for older adults and Dr. Cappeliez will review the manual for its reminiscence content. The second level of evaluation will occur in Phase II of the research plan.
Phase II: (Year 3) – Aim #4Testing of training manual with facilitators (N=10) for acceptability, appropriateness, and feasibility and training of the peer facilitators.
Purpose: The purpose of Phase II of the research plan is to test the reminiscence training manual with the peer facilitators. Phases 2 and 3 of the research plan will occur in New Haven. Dr. Melkus and Dr. Knobf have relationships with African-Americans and will assist me in entering the community. The training and testing will occur in a different site (New Haven) to avoid contamination between participants. The facilitators will review the manual and provide feedback on its readability, cultural appropriateness, and usefulness with older African-Americans. Once the manual is approved by mentors and the participants, then 10 peer facilitators will be trained to facilitate integrative reminiscence.
MethodsSample: Recruitment of peer reminiscence facilitators will begin in Year 2 through participant observations andkey informant interviews. Participants willing to be trained to facilitate reminiscence and to complete human subjects training must be African-American, English speaking, with intact cognition, and over the age of 55.Data Collection: Focus group methodology will be employed to determine the appropriateness and acceptability of the training manual to the population. Questions to guide the focus groups to evaluate the manual will be developed by the PI with the mentoring of Drs. Cappeliez and Lichtenberg. Revisions will be made as necessary.
Training Approach of the Peer Facilitators (N=10)I have had extensive experiences training nursing students to facilitate reminiscence through a training manual. Focus group data will identify specific learning approaches that the peer facilitators respond to in a positive way. It is expected that the training component will include a PI-developed video that will address reminiscence techniques such as active listening, presence, silent space and body language. In addition, the facilitators will conduct 2 audio-taped reminiscence sessions with an older adult and the PI will provide feedback for learning purposes. The taped sessions will provide the PI with the ability to assess the reminiscence intervention for content, facilitator delivery and validation of the older adults’ experiences, and to make modifications in the manual again if necessary. For sustainability of the reminiscence intervention, once the manual has been tested with the peer facilitators, training will include key informants, senior center nurses, and social workers.
Phase III (Years 4 & 5) Aim #5Pilot test for feasibility and directional effectiveness of the peer-to-peer reminiscence program on depressive symptoms and reminiscence functions in older African-Americans (N= 24).
Purpose: To assess the feasibility and directional effectiveness of the peer to peer reminiscence intervention in a small randomized, controlled clinical trial. I will evaluate how adequately the intervention can be implemented and how acceptable it is to participants. In addition, I will assess changes from pre to post reminiscence intervention to gather preliminary data on reducing depressive symptoms. A secondary purpose of this study is to analyze the effect of the reminiscence intervention on increasing positive reminiscence functions and frequency. These data will be important in refining the intervention for future studies.Research Questions: 1) What is the directional effect of the peer-to-peer reminiscence program on depressive symptoms in the experimental group as compared to the control group? 2) What is the directional
Principal Investigator/Program Director (Last, first, middle): Shellman, Julietteeffect of the peer-to-peer reminiscence program on reminiscence functions in the experimental group as compared to the control group? 3) What are participants’ perceptions of the peer-to-peer reminiscence program?Research Design and Methods: The design for the study will be a pretest-posttest randomized control trial design, which optimizes control for threats to internal validity (Campbell & Stanley, 1963). The study design controls for threats to external validity by independent and random assignment to groups following informed, signed consent. Given the practical limitations of this award, there will be a simple 2 group design (experimental and control) rather than the more complex 3 group (reminiscence, regular treatment and control) design. A sample of 24 new participants who meet inclusion criteria will be randomly assigned to either begin the reminiscence program immediately (n=12) or be part of the 6-week wait-list condition (n=12). Participants will be evaluated immediately before beginning treatment, and immediately following the reminiscence and 30 days later for follow-up. All participants assigned to the wait-list condition will be offered the structured intervention following their waiting period of 6 weeks plus 30 days.Participants: African-Americans who are willing to share life experiences will be included in the study. Inclusion criteria includes the following: 1) subjects will be English speaking, 2) at least 55 years of age and born in the United States by self-report, 3) intact cognition, and 4) minimum score of 10 on the Center for Epidemiological Studies Depression Scale. A score of 10-15 has been operationalized as minor depression (Hybels, C. Blazer, D. & Pieper, C, 2001) on the CES-D. Any participant who scores higher than 16 will be referred for further screening. The short portable mini-mental exam (Pfeiffer, 1974) will be used to screen the participants for any cognition difficulties that may inhibit the reminiscence interview. A list of mental health community services will be compiled before Phase 3 for referrals and will be listed in the manual.Sample Size: This pilot study will provide estimates of mean effects, standard deviations of study variables, and the correlations between repeated measurements on the same persons with minor depression that will be required to calculate power and sample size in designing subsequent studies. This study is not likely to have adequate power for statistical significance, but is expected to demonstrate directional support for future clinical trials.
InstrumentsShort Portable Mini-Mental Exam: The Short Portable Mini Mental Exam (Pfeiffer, 1975) will be used because it has been found to be useful in identifying cognitive impairment in older African-Americans.Demographic Form: A self-report demographic data form developed by the PI regarding age, gender, medical diagnoses, medications, socio-economic status, and social supports will be collected from the participants. Each of these characteristics is mentioned in the literature as having a possible association with depressive symptoms in elders.Center for Epidemiological Studies-Depression Scale (CES-D): Levels of depression will be measured using the Center for Epidemiological Studies Depression Scale (CES-D). The CES-D is a 20-item, reliable and valid instrument that has been used with diverse populations and has been found to be sensitive for detecting depression among African-American elders (Baker, Velli, Friedman, & Wiley, 1995). Reminiscence Function (Scale RFS): Reminiscence functions and frequency will be measured pre and post test using the modified RFS in Phase 1 and will be used to assess the reminiscence intervention for increasing the frequency and recall of positive memories.Reminiscence Evaluation Surveys. Reminiscence program satisfaction surveys will be completed by participants after the 6 week intervention. This questionnaire will provide data regarding perceived efficacy of the intervention, and regarding satisfaction with scheduling, intervention length and the reminiscence sessions.
Data Collection: A trained African-American research assistant will collect pre and post test data.
Reminiscence Intervention: The intervention will be 6 reminiscence sessions of integrative reminiscence conducted by trained peer facilitators. The sessions will be conducted for 45 minutes. Selections of duration and length of the reminiscence sessions were chosen based on preliminary findings indicating that 8 weeks was too long for the participants. The same peer facilitator will visit the participant for the duration of the study and completion of reminiscence sessions. Questions for facilitating reminiscence that were developed in Phases 1 and 2 will guide the facilitators for Phase 3 intervention.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteData Analysis: While the sample size limits significance testing, the following analyses will be undertaken to get a sense of direction of the effects of the reminiscence program. Data will be entered using SPSS 14. Descriptive statistics such as frequencies, means, standard deviations and ranges will be calculated for depressive symptoms scores, reminiscence functions, and demographic data at the pre and post testing points in both the control and experimental groups. If the groups are equivalent, repeated measures analysis of variance (RM-ANOVA) will be used to test for differences related to research hypothesis 1. If random assignment has not produced equivalent groups, analysis of covariance (ANCOVA) will be used with age, years of religion experience. Correlational analyses such as multiple regression will be used to examine possible relationships between demographic variables and depressive symptoms and reminiscence functions scores. The analysis plan may change after further consultation and training. Data on the variability of CES-D scores will be useful in estimating effect sizes for future, larger scale efficacy studies. Reminiscence Function Scale scores will be helpful to assess if the intervention increases the participants’ frequency of reminiscence and does the intervention assists the participant to reminiscence for a positive function.
Feasibility: Feasibility is operationalized in this study as including: 1) intervention delivery, and 2) intervention receipt. The delivery of integrative reminiscence will be assessed by the peer facilitators and the PI using a checklist to see if the reminiscence intervention was conducted as described in the manual. Treatment receipt will be assessed by participants after the reminiscence sessions to assess their perceived efficacy of the reminiscence intervention, satisfaction with scheduling, and intervention length (dose). Treatment receipt will also be assessed by pre-post test RFS scores for increase in frequency and positive memory recollections.Expected Outcomes: This research study represents a culmination of the training activities outlined in this award, specifically with respect to training in community-based participatory research, advanced statistics and RCT methodology. Developing expertise in the design and conduct of randomized controlled trials is one of my primary training goals for this award. Implementing this design under the guidance of Dr. Melkus will provide this training. The development of a culturally appropriate reminiscence intervention is a vital first step that should precede any larger scale efficacy analysis. Results from this project will make significant contributions to the reminiscence literature and provide groundwork for future studies. I will submit an R-series application under the guidance of Drs. Melkus and Evans during the 5th year of the award period. This will allow sufficient time for preliminary data analyses for the R series application, as well as protected time to conduct more detailed evaluation of the intervention during the last quarter of the K01 award period. Finally, the research activities outlined in this award provide the foundation for multi-site effectiveness of integrative reminiscence in decreasing depressive symptoms.
Table 6. Timeline for Research Plan Phase 1 Phase 2 Phase 3Research Activities Year 1 Year 2 Year 3 Year 4 Year 5
Stakeholder Meetings/Human Subjects Training Hiring/Training of research assistants (Phase 1) Participant Observations/Key Informant Interviews (Phase 1)Selection of reminiscence peer facilitators (Phase 1)Focus groups, RFS psychometrics (Phase 1)Development of Training Manual (Phase 2) Focus Groups – Training Manual (Phase 2)Training of Reminiscence Facilitators (Phase 2) Conduct Pilot Study (Phase 3)Data analysis for feasibility and directional supportDisseminate results to participants/Manuscript Development
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliette4.E. Human Subjects
1. Risks to the SubjectsA. Human Subjects Involvement and CharacteristicsInformed consent will be required from all participants in the study. It is expected that those who volunteer will participate in focus groups, key informant interviews, psychometric evaluation of the Reminiscence Function Scale, development of the peer training manual and training if the peer facilitators, and pilot testing the peer reminiscence intervention. Peer facilitators and stakeholders such as senior center directors, pastors, pastors’ wives or others designated as a stakeholder will be expected to complete human subjects training.
It is expected that there will be at least 300-400 African-American community participants over the age of 55 with intact cognition who participate in activities at the senior center or church. Key informants may be anyone of any race or ethnic background over the age of 21 associated with the identified community units (church and senior centers). This includes senior center directors, pastors, pastors’ wives, health committee members and senior center nurses.
Human subjects for the research study will involve older African-American men and women because reminiscence occurs primarily in older adults and the primary goal of this study is to develop and test a peer-to-peer reminiscence program on depression and reminiscence functions in older African-Americans. In addition, including older African-Americans in this study will facilitate the understanding of the functions of reminiscence in this specific population.
Collaborating sites include Northend Senior Center, Bloomfield Senior Center and the N.E.A.T. group at The Bethel African Methodist Episcopal Church. Participants from these sites will assist with development of the reminiscence training manual, modification and psychometric evaluation of the Reminiscence Function Scale. Dr. Melkus and Dr. Knopf will assist me with entry into New Haven communities such as Fair Haven Clinic and “Connecting Sisters” to training the peer facilitators and conduct the pilot study.
B. Sources of MaterialsData will be gathered by administration of the PI developed demographic form, Short Portable Mini-Mental Exam, the Center for Epidemiological Studies Depression Scale, Reminiscence Function Scale and a Reminiscence Evaluation. Interviews, focus groups, and reminiscence training sessions will be audio taped with participant permission. The PI and research assistants will maintain field notes and journals throughout the project. The data will be collected by the PI and a research assistant who will have completed human subjects training.
C. ConfidentialityI will keep names and identification numbers that will be kept in a coding book stored in a locked filing cabinet. All demographic data and Reminiscence Function Scores will use codes as identifiers. No forms, journals, or tapes will have personal identifiers. I will maintain the coding book, which will be stored in a locked filing cabinet in my office. No study participants’ names or other identifiers will be used in reporting the findings. I will keep all data confidential and I will monitor the data collection process to ensure confidentiality throughout the project. The research assistants, peer facilitators, and stakeholders as mentioned above will complete and pass the online Human Subjects Training as specified by NIH as part of their training.
D. Potential RisksThere is a risk of loss of confidentiality. However, procedures for protecting confidentiality include: 1) human subjects training for peer facilitators, research assistants, senior center directors or other personnel in the stakeholder group, 2) coding surveys and interviews, and 3) avoiding eliciting identifying information in all data collection formats. I expect that these methods will effectively minimize the loss of confidentiality. There may be an inconvenience of time, however, focus groups will be held at the suggested times of the participants to foster participation. Another potential risk of participation is feelings of sadness or anger when reminiscing about a more negative experience. However, the participant chooses what they want to share or not share. The PI has extensive experience in conducting reminiscence with older African-Americans and will
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliettetrain the data collectors and peer facilitators to watch for such feelings so that any participant who becomes uncomfortable can be encouraged to share feelings or stop the interview, whichever is preferred by the participant.
2. Adequacy of Protection Against Risks
A. Recruitment and Informed ConsentFlyers will be posted at the sites. The RA and PI will be available at the sites on a weekly basis for potential participants and community stakeholders (senior center and church directors) to answer questions and recruit interested participants. The PI and RA will attend and participate in events such as blood pressure screenings, lunches, wellness programs and other events identified by the community stakeholders. Participation will be voluntary. Children will not be included in this study as this research involves reminiscence in older African-Americans. The trained research assistant will obtain consent after reviewing information and procedures with participant. This will take approximate 5-10 minutes with additional time for questions. This process will take place in a private setting provided by the sites (see letters of support).
B. Protection Against RiskI expect that training the research assistant, community stakeholders and peer facilitators in human subjects protection will minimize the risk of loss of confidentiality. Based on my experience using reminiscence with older adults in several preliminary studies, I anticipate minimal risks. The peer facilitators will be thoroughly trained to identify depressive symptoms or situations that call for referral. The study risks and plans for ensuring participant safety follow. I am an advanced practice nurse and I will be available via cell phone throughout the study. Additionally, a list of community resources and personnel will be developed as part of the development of the training manual. The study will not be conducted without these resources in place. Community stakeholders will assist the PI with the development of available mental health resources.
3. Potential Benefits of the Proposed Research to the Subjects and OthersThere are individual and community benefits to participating in this research study. For individuals, it is expected that participants will gain satisfaction from providing their input into the development of the peer-to peer reminiscence intervention. Additionally, participants who reminiscence will have greater awareness of their life accomplishments and a decrease in depressive symptoms. For the community, there will be trained peer reminiscence facilitators and stakeholders (social workers, nurses etc.) that will sustain this reminiscence intervention for the community to improve health once the study has been completed. Through this process of community-based participatory research, the community will become aware of strengths, and their participation will lead to a greater understanding of the research process leading to increased trust between the community and researchers. The anticipated benefits to participants and the community outweigh the potential risks.
4. Importance of the Knowledge to be GainedThere will be a greater understanding of the functions of reminiscence in older African-Americans and the directional effectiveness of the peer-to-peer reminiscence intervention program on depressive symptoms and reminiscence functions in older African-Americans. Data will provide important information towards the development of a peer-to-peer intervention that can be used in multiple sites. Furthermore, this innovative and cost-effective program has the potential to have a positive effect on the mental health and well-being of older African-Americans.
5. Data Safety and Monitoring Plan
Risk AssessmentThe Yale School of Nursing Human Subjects Research Review Committee (HSRRC) will review the proposed research. I expect that HSRRC will find that the proposed studies pose minimal risks to the participants. Approval from HSRRC and from the community sites via stakeholders will occur before the research begins. Participants may experience negative feelings if they reminisce and talk about negative experiences. However, based on my extensive experiences of conducting reminiscence with older African-Americans, I expect minimal risk to the participants. The peer facilitators will be trained to identify positive coping strategies and validate
Principal Investigator/Program Director (Last, first, middle): Shellman, Juliettefeelings to provide support to the participants. The peer facilitators will be debriefed by the PI on a weekly basis to monitor for this risk.
Monitoring PlanDr. Melkus, Dr. Knobf and the community stakeholders will provide oversight and monitoring of the proposed study. This committee will annually review data quality and timeliness, participant recruitment, accrual and retention, and participant risk versus benefit. In addition, they will consider therapeutic developments that may have an impact on the safety of the participants or the ethics of the study, examine all adverse events for patterns or relationships to study participation. This committee will recommend whether to continue or conclude the trial. Confidentiality will be maintained.
Reporting PlansI will examine all adverse events and determine if the events were related to study participation, I will report adverse events to the Human Subjects Research Review Committee within 24 hours. Reporting of adverse events will be within the IRB guidelines and according to IRB protocol.
Data Accuracy and Protocol ComplianceAll records will be kept confidential and used only for research purposes. Participants will be assigned a numerical tracking number to protect confidentiality. I will be responsible for data accuracy and security.
Inclusion of Women and MinoritiesThere are no exclusion criteria in my study based on sex. Inclusion of Whites, Hispanics, Asian, Native Indian, Hawaiian or Pacific Islander, and Alaska Native is inappropriate because this study is investigating the effects of a peer-to-peer reminiscence program intervention on depressive symptoms and reminiscence functions in older African-Americans (see Targeted Enrollment form).
Inclusion of ChildrenChildren will not be included as this is a study of older adults.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteF. Vertebrate Animals – N/A
G. Select Agent Research – N/A
H. Literature Cited
American Association of Geriatric Psychiatry. (2006). Depression fact sheet. Retrieved December 1, 2006 from http://www.aagponline.org/p_c/depression.asp.
Baker, F. M. (1994). Psychiatric treatment of older African Americans. Hospital Community Psychiatry. 45(1):32-7. Review.
Baker, F. M., Velli, S. A., Freidman, J., & Wiley, C. (1995). Screening tests for depression in older black vs. white patients. American Journal of Geriatric Psychiatry, 3, 43-51.
Bernal, H., & Froman, R. (1987). The confidence of community health nurses in caring for ethnically diverse populations. Image: Journal of Nursing Scholarship, 19(4), 201-203.
Bernal, H., & Froman, R. (1993). Influences on the cultural self-efficacy of community health nurses, Journal of Transcultural Nursing, 4(2), 24-31.
Bernal, H., Shellman, J., & Reid, K. (2004). Essential concepts in developing community-university partnerships, Partners in caring, the Carelink model. Public Health Nursing, 21(1), 32-40.
Blazer, D. (2003). Depression in late life: Review and commentary. Journal of Gerontology: Medical Sciences, 58A(3), 249-265.
Bogdewic, S. (1999). Participant observation. In B. Crabtree & W. Miller (Eds.), Doing qualitative research (2nd
ed.) (pp. 109-126). Thousand Oaks, CA: Sage.Bogdewic, S. (1999). Participant observation. In B. Crabtree & W. Miller (Eds.), Doing qualitative research (2nd
ed.) (pp. 47-69). Thousand Oaks, CA: Sage.Bohlmeijer, E., Smit, F., & Cuijpers, P. (2003). Effects of reminiscence and life review on late-life depression: A
meta-analysis. International Journal of Geriatric Psychiatry, 18, 1088-1094.Boltri, J. M., Davis-Smith, Y. M., Zayas, L. E., Shellenberger, S., Seale, J. P., Blalock, T.W., & Mbadinuju, A.
(2006). Developing a church-based diabetes prevention program with African Americans: Focus group findings. Diabetes Educator, 32(6), 901-909.
Borkan, J. (1999). Immersion/crystallization. In B. Crabtree & W. Miller (Eds.), Doing qualitative research (2nd
ed.) (pp. 179-194). Thousand Oaks, CA: Sage.Brown, J. (1999). The use of focus groups in clinical research. In B. Crabtree & W. Miller (Eds.), Doing
qualitative research (2nd ed.) (pp. 109-126). Thousand Oaks, CA: Sage.Butler, R. N. (1963). The life review: An interpretation of reminiscence in the aged. Psychiatry, 26, 65-76.Butler, R. N. (1974). Successful aging and the role of life review. Journal of the American Geriatrics Society,
22, 529-535Cannon, K. (1995). Surviving the blight. In G. Wade-Gayles (Ed.), My soul is a witness: African-American
women’s spirituality (pp. 19-26). Boston: Beacon.Cappeliez, P., & O’Rourke, N. (2002). Profiles of reminiscence among older adults: Perceived stress, life
attitudes, and personality variables. International Journal of Aging Development, 54(4), 255-266.Cappeliez, P., & O'Rourke, N. (2006). Empirical validation of a model of reminiscence and health and later life.
Journal of Gerontological Sciences, Social Sciences, 61(4), 237-244.Cappeliez, P., O’Rourle, N., & Chaudhury, H. (2005). Functions of reminiscence in later life. Aging and Mental
Health, 9(4), 295-301.Conwell, Y. (2001). Suicide in later life: a review and recommendations for prevention. Suicide and Life
Threatening Behavior, 31(Suppl):32-47.Cook, J. M., Pearson, J. L., Black, B. S., & Rabins, P. V. (2002). Suicidality in older African Americans: findings
from the EPOCH study. American Journal of Geriatric Psychiatry, 10(4), 437-46.Cooper, L. A., Gonzales, J. J., Gallo, J. J., Rost, K. M., Meredith, L. S., Rubenstein, L. V., Wang, N. Y., & Ford,
D. E. (2003). The acceptability of treatment for depression among African-American, Hispanic, and white primary care patients. Medical Care. 41, 479-489.
Crabtree, B. F., & Miller, W. (Eds.) (1999). Doing qualitative research. Newbury Park, CA: Sage.Cully, J., LaVoie, D., & Gfeller, J. (2001). Reminiscence, personality, and functioning in older adults. The
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteCurry, L., & Jackson, J. (Eds.) (2004). Recruitment and retention of diverse ethnic and racial groups in health
research: An evolving science. In, The science of inclusion. Washington, DC: Gerontological Society of America.
Das, A., Olfson, M., McCurtis, H., & Weissman, M. (2006). Depression in African-Americans: Breaking barriers to detection and treatment: community studies tend to ignore high-risk groups of African-Americans. Journal of Family Practice, 55, 30-39.
Dennis, B., & Neese, J. (2000), Recruitment and retention of African-American elders into community-based research: Lessons learned. Archives of Psychiatric Nursing, 14(1), 3-11.
Erickson, E. H. (1959). Identity and the life cycle. New York: W.W. Norton.Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975) ‘Mini Mental State’: A practical method for grading the
cognitive state of patients for the clinician. Journal of Psychiatry Research, 12, 189-198.Frojdh, K., Hakansson, A., Karlsson, I., & Molarius, A. (2003). Deceased, disabled or depressed: A population-
based 6-year follow-up study of elderly people with depression. Social Psychiatry & Psychiatric Epidemiology, 38(10), 557-562.
Gable, R., & Wolf, M. (1993). Instrument development in the affective domain (2nd ed.). Boston, MA: Kluwer Academic Publishers.
Gallo, J. J., Bogner, H., Morales, K., & Ford, D. (2005). Patient ethnicity and the identification and active management of depression in late life. Archives of Internal Medicine, 165, 1962-1968.
Gilchrist, V., & Williams, R., (1999). Key informant interviews. In B. Crabtree & W. Miller (Eds.), Doing qualitative research (2nd ed.) (pp. 71-88). Thousand Oaks, CA: Sage.
Haber, D. (2006). Life review: implementation, theory, research, and therapy. International Journal of Aging and Human Development, 63, 2, 153-171.
Haight, B., & Webster, J. (1995). The art and science of reminiscing: Theory, research, and applications. Washington, DC: Taylor and Francis.
Haight, B., & Webster J. (2002). Critical advances in reminiscence work. New York, NY: Springer.Haug, M. R., & Wykle, M. L. (1999). Serving minority elders: Directions for future research. In M. L. Wykle & A.
B. Ford (Eds.), Serving minority elders in the 21st century (pp. 323-328). New York: Springer Publishing Company.
Hseih, H., & Wang J. (2003). Effect of reminiscence on depression in older adults: A systematic review. International Journal of Nursing Studies, 40, 335-345.
Hybels, C. F., Blazer, D. G., & Pieper, C. F. (2001). Toward a threshold for subthreshold depression: An analysis of correlates of depression by severity of symptoms, using data from an elderly community sample. Gerontologist,41, 357-365.
Israel, B. A., Lichtenstein, R., Lantz, P., McGranagan, R., Allen, A., Guzman, J. R., Softley, D., & Maciak, B. (2001). The Detroit community-academic urban research center: Development, implementation, and evaluation. Journal of Public Health Management, 7(5), 1-19.
Israel, B., Eng, E., Schulz, A., & Parker, E. (Eds.) (2005). Methods in community-based participatory research for health. San Franscisco, CA; Jossey-Bass.
Jackson, J. (1991). Methodological approach. In J. Jackson (Ed.), Life in black America (pp. 13-30). Newbury Park, California: Sage.
Katon, W., Lin., E., Russo, J., & Unutzer, J. (2003). Increased medical costs of a population-based sample of depressed elderly patients. Archives in General Psychiatry, 60, 897-903.
Kennedy, B. M., Paeratakul, S., Champagne, C. M., Ryan, D. H., Harsha, D. W., McGee, B., Johnson, G., Deyhim, F., Forsythe, W.,& Bogle, M. L. (1998). A pilot church-based weight loss program for African-American adults using church members as health educator: a comparison of individual and group intervention. Ethnicity and Disease, 15(3), 373-378.
Lyness, J. M., Heo, M., Datto, C., Ten Have, T., Katz, I., Drayer, R., Reynolds, C., Alexopoulos, G., & Bruce, M. (2006). Outcomes of minor and subsyndromal depression among elderly patients in primary care settings. Annals of Internal Medicine, 144(7), 496-504.
Maillet, N. A., D'Eramo Melkus, G., & Spollett, G. (1996). Using focus groups to characterize beliefs and practices of African-American women with NIDDM. The Diabetes Educator, 22(1), 39-45.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteMelkus, G. D., Spollett, G., Jefferson, V., Chyun, D., Tuohy, E., Robinson, T. & Kaisen A. (2004). Feasibility
testing of a culturally competent intervention of education and care for black women with type 2 diabetes. Applied Nursing Research, 17(1), 10-20.
Mills, T., Alea, N., & Cheong, M. B. (2004). Differences in the indicators of depressive symptoms among a sample of African-American and Caucasian older adults. Community Mental Health Journal, 40, 309-331.
Mills, T. L. (2000). Depression, mental health and psychological well-being among older African-Americans: A selective review of the literature. African American Research Perspectives, 6(2), 93-104.
Molinari, V., Cully, J. A., Kendjelic, E. M., & Kunik, M. E. (2001). Reminiscence and its relationship to attachment and personality on geropsychiatric patients. International Journal of Aging and Human Development, 52(3), 173-184.
National Institute of Mental Health. (2003). Older adults depression and suicide facts. Available at http://www.nimh.nih.gov/publicat/elderlydepsuicide.cfm. Retrieved September 1 2006.
Newlin, K., Melkus, G. D., Jefferson, V., Langerman, S., Womack, J., & Chyun, D. (2006). Recruitment of black women with type 2 diabetes into a self-management intervention trial. Ethnicity & Disease, 16, 956-962.
Nunnally, J. C., & Bernstein, L. H. (1995). Psychometric theory (3rd ed.). New York: McGraw-Hill.O’Rourke, N. (2002). A social cognitive model of well-being among older adults. Constructivism in the Human
Sciences, 7, 65-80.Oxman, T., & Sengupta, A. (2002). Treatment of minor depression. American Journal of Geriatric Psychiatry,
10(3), 256-264.Pfeiffer, E. (1975). A short portable mental status questionnaire for the assessment of organic brain deficits in
elderly patients. Journal of the American Geriatrics Society, 23(10), 433-441.Porter, C., & Villarruel, A. (1993). Nursing research with African-American and Hispanic people: Guidelines for
action. Nursing Outlook, 41, 59-66.Rao, V. N., & Rao, VV. (1982). Life satisfaction in the black elderly: An exploratory study. International Journal
of Aging Human Development, 14, 55-65.Romaniuk, M., & Romaniuk, J. G. (1981). Looking back: An analysis of reminiscence function and triggers.
Experimental Aging Research, 7(4), 477-489.Rooks, R., & Whitfield, K. (2004). Health disparities among older African-Americans: Past, present, and future
perspectives. In K. Whitfield (Ed.), Closing the gap. Improving the health of minority elders in the new millennium (pp. 45-54). GSA: Washington, DC.
Samuel-Hodge, C. D., Keyserling, T. C., France, R., Ingram, A. F., Johnston, L. F., Pullen Davis, L., Davis, G., & Cole, A. S. (2006). A church-based diabetes self-management education program for African Americans with type 2 diabetes. Preventing Chronic Disease, 3(3), A93.
Schensul, J. J., Robison, J., Reyes, C., Radda, K., Gaztambide, & Disch, W. (2006). Building interdisciplinary partnerships for community-based mental health research with older minority adults. American Journal of Community Psychology, 38, 79-93.
Shellman, J. (2000). Promoting elder wellness through a community-based blood pressure clinic. Public Health Nursing, 17(4), 257-263.
Shellman, J. (2000). A cross-cultural examination of reminiscence in older adults. Paper presented at Eastern Nursing Research Society’s 12 Annual Scientific Session, Newport, RI.
Shellman, J. (2004). “Nobody ever asked me before.” Understanding life experiences of African-American elders. Journal of Transcultural Nursing, 15, 308-316.
Shellman, J. (2006). Reliability and validity testing of the Eldercare Cultural Self-Efficacy Scale. International Journal of Nursing Education Scholarship, 3(1), Article 9. Available at: http://www.bepress.com/ijnes/vol3/iss1/art9.
Shellman, J. (2006). The effects of a reminiscence education program on BSN students’ cultural self-efficacy. Nurse Education Today. doi:10.1016/j.nedt.2006.02.009.
Shellman, J. (2006). Making a connection. BSN students’ perceptions of their reminiscence experiences with elders. Journal of Nursing Education, 45(12), 1-7.
Skarupski, K. A., Mendes de leon, C. F., Bienias, J. L., Barnes, L. L., Everson-Rose, S. A., Wilson, R. S., & Evans, D. A. (2005). Black-white differences in depressive symptoms among older adults over time. Journal of Gerontology: Psychological Sciences, 60, 136-142.
Snowden, L. R. (2001). Barriers to effective mental health services for African-Americans. Mental Health Services Research, 3, 181-187.
Principal Investigator/Program Director (Last, first, middle): Shellman, JulietteSoltys, F., & Coats, L. (1995). The solcos model: Facilitating reminiscence therapy. Journal of Psychosocial
Nursing, 33(1), 21-26.Stewart, C. (1997). Soul survivors: An African American spirituality. Louisville, KY: Westminster John Knox
Press.U.S. Department of Health and Human Services. (2001). Mental health: Culture, race and ethnicity: A report of
the Surgeon general. Available at http://www.surgeongeneral.gov/library/mentalhealth/chapter5/sec3.html.Watt, L., & Wong, P. T. (1991). A taxonomy of reminiscence and therapeutic implications. Journal of Mental
Health Counseling, 12, 270-278.Webster, J. D. (1993). Construction and validation of the reminiscence function scale. Journal of Gerontology,
48, 256-262.Webster, J. D. (1997). The reminiscence function scale: A replication. International Journal of Aging and
Human Development, 44, 137-148.Weinrich, S. P., Boyd, M. D., Weinrich, M., Greene, F,, Reynolds, W. A. Jr, & Metlin, C. (1998). Increasing
prostate cancer screening in African American men with peer-educator and client-navigator interventions. Journal of Cancer Education, 13(4), 213-219.
I. Consortium/Contractual Arrangements – N/A
J. Sharing Research ResourcesThe product (reminiscence peer training manual) developed through this research project does not fall under the category of unique research resources as described in the NIH Grants Policy Statement as biomedical research tools. The PI will begin sharing of research resources with manuscript publication of this NIH supported research in primary scientific journals such as Journal of Gerontology, Nursing Research, Aging and Mental Health and the Gerontologist. The peer training manual developed in this research project will be shared with community members. All publications will acknowledge NIH grant support. Since this is a pilot test for feasibility and directional effectiveness of the intervention, it is not expected that the manual will be ready for copyrighting at the end of the 5 Year award period. However, this will be re-assessed at the end of the 5-year career development award with my mentors.