43
Dementia Care A Person Centered Approach to Decreasing Behaviors Margaret Kimbell, RN, MSA, DHA, CDP Bettina Suarez Palacios, RN, BSN, MBA, RAC Erickson Living

Dementia Care A Person Centered Approach to
Decreasing Behaviors Margaret Kimbell, RN, MSA, DHA, CDP
Bettina Suarez Palacios, RN, BSN, MBA, RAC
Erickson Living

Objectives
• The purpose of this activity is to enable the learner to define Person Centered Approaches to Dementia care and how quality of life and quality of care can be one fluid act of kindness.
• The purpose of this activity is to describe the Think Comfort behavioral approach to understanding the actions and expressions of elders with cognitive impairment.
• The purpose of this activity is to describe the strength based three tiered approach to engagement for elders with dementia; meeting their needs while also decreasing neuropsychiatric symptoms.

What does aging mean to you?

• Peripheral (side) vision is reduced
• Presbyopia - diminished sharpness of vision and focusing, reading glasses are required
• Lens of the eye becomes cloudy diminishing the amount of light
• Glaucoma – loss of side vision
• Macular degeneration – loss of central vision
Vision Changes
Hearing Changes
• High-pitched sounds such as "s" or "th" are hard to distinguish from one another
• Background noise further complicates hearing difficulty
• Men's voices are easier to hear than women's
• Other people's voices sound mumbled or slurred
• Ringing in the ears
Presbycusis – slow progressive loss of hearing caused by changes to inner ear

Decrease in • Number of taste buds • Sensitivity to salt and sweet first
• Bitter and sour last longer • Amount of saliva production
Smell and Taste Changes
• Smell may diminish after age 70

• Use it or lose it
• Overall cognition (thinking) depends upon health of the brain
• The brain’s processing slows but given the opportunity….. processing does occur
• Forgetfulness – normal aging memory lapses
• Memory loss – disease related changes that are disabling affecting hobbies, social activities, relationships, etc.
Brain Changes

Person-Centered Approach
“Caring enough to understand the individual and customizing our approach to recognize the person’s gifts, their needs, their preferences, and their goals”

Self-
Actualization
Esteem
Love & Belonging
Safety
Physiological
Person-Centered Approach Model
Abraham Maslow’s Hierarchy of Human Needs

Self-Actualization
…continuous desire to fulfill potential, to “be all that I can be.”
Morality, Creativity, Problem Solving, Spontaneity, Lack of Prejudice, Acceptance
Communication
Honoring desires and wishes
Helping elders meet their needs
Death and dying
Grief
of Facts, Being All that I Can Be

Esteem
Self-respect
Appreciation for life’s contributions
Dignity
Recognition of accomplishments
Independence Self-esteem,
Confidence, Achievement, Respect of Others, Respect by Others,
Freedom

Love & Belonging
Get to the know the person and what is important to them
Relationships – past and present
Sense of community
Sadness and depression
Loneliness and social
anxieties
Therapeutic touch
Friendship, Family, Sexual Intimacy
Safety
Falls
Lifting and transferring
Lack of restraints/side rails
Health and well-being
Environmental hazards
Security of Body, Of Employment, Of Resources, Of Morality, Of the Family, Of
Health, Of Property

Physiological
Pain
Nutrition
Bowel and Bladder
Hydration
Pain management
Wound Care
Breathing, Food, Water, Sex, Homeostasis, Sleep, Excretion

Person-Centered Approach
• Helping the person make as many choices in their life as they can
• Making the person the center of care guided by their choices
• Remember, it’s not about staff’s work routine, it is about what helps the person achieve all levels of the pyramid!
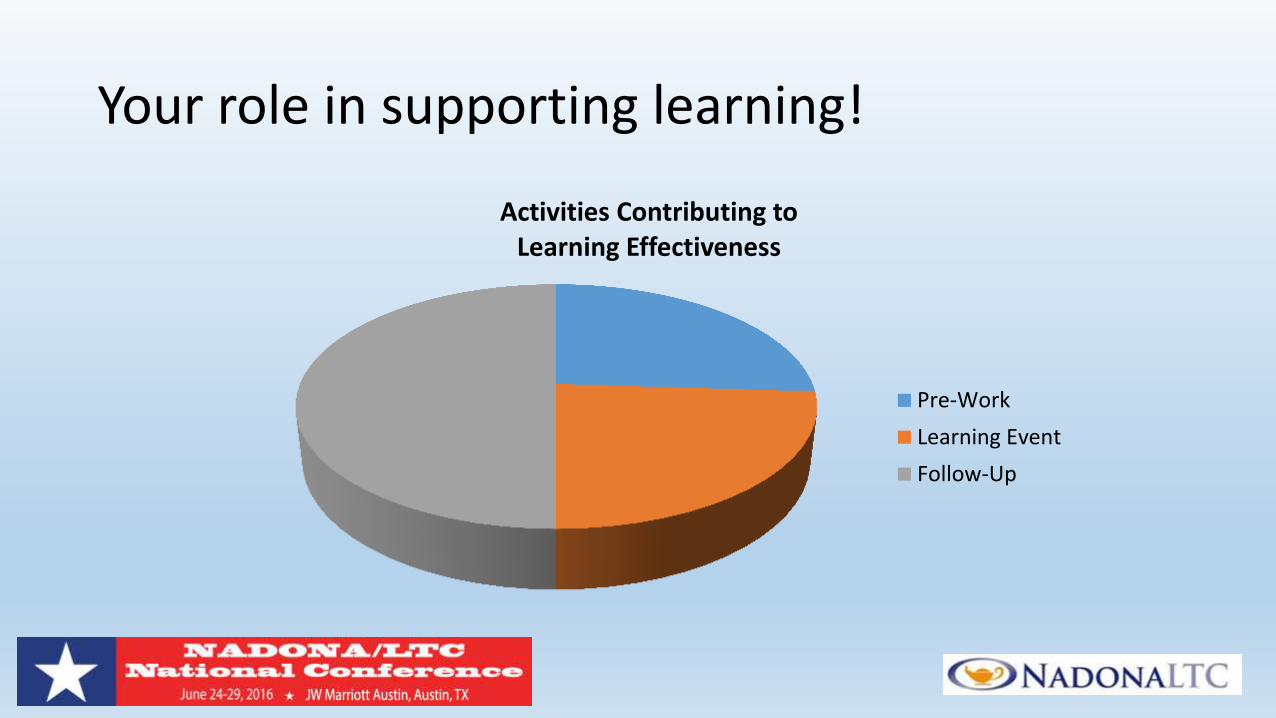
Your role in supporting learning!
Activities Contributing to Learning Effectiveness
Pre-Work
Learning Event
Follow-Up
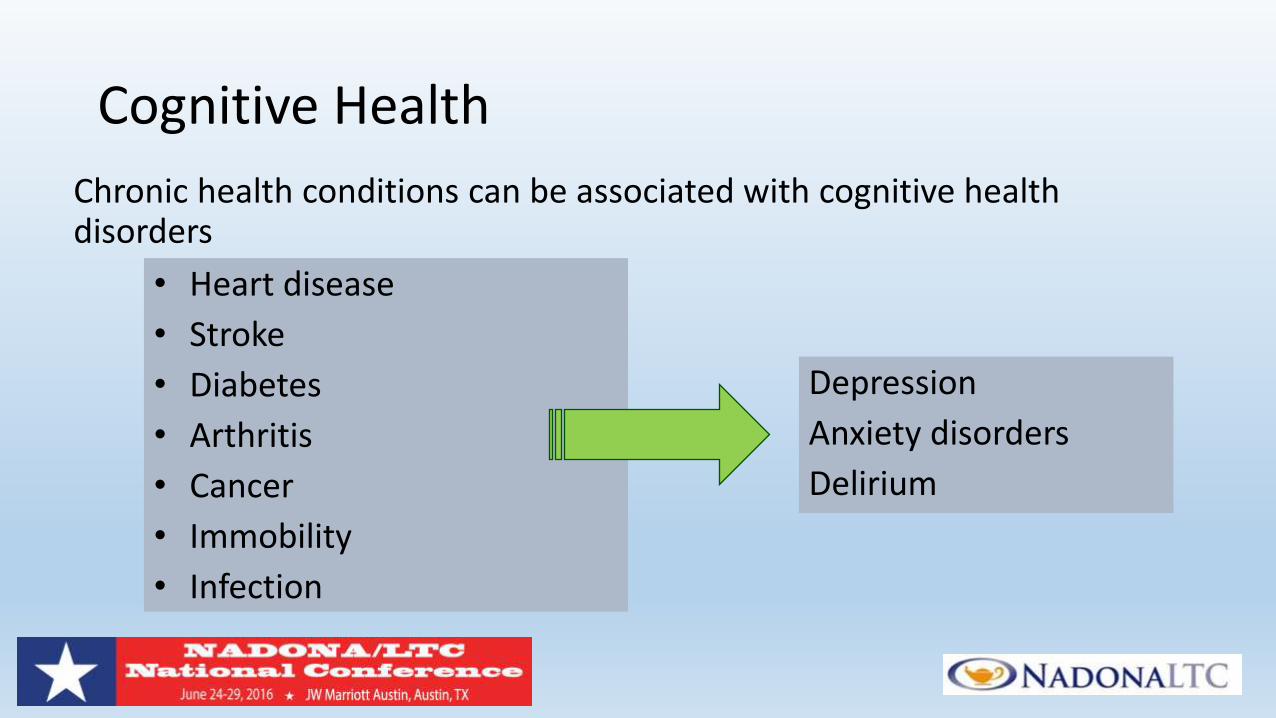
Chronic health conditions can be associated with cognitive health disorders
Cognitive Health
• Heart disease
• Stroke
• Diabetes
• Arthritis
• Cancer
• Immobility
• Infection
Depression
Anxiety disorders
Delirium

• What can cause memory loss?
• Depression
• Vitamin deficiency
• Thyroid imbalance
• Medications
• Alcohol abuse
• Dehydration
Brain Changes
Many causes of memory loss can
be reversed!

Dementia is not a specific disease. It's an overall term that describes a wide range of symptoms associated with a decline in memory or other thinking skills severe enough to reduce a person's ability to perform everyday activities.
Dementia
http://www.alz.org/what-is-dementia.asp

Disease/Condition = Dementia Symptoms
Disease/Condition Dementia Symptoms
• Alzheimer’s
• Parkinson’s
• Stroke
• Infection of Brain
• Thyroid Deficiency
• Vitamin Deficiency
Progressive decline in: •Remembering •Paying attention •Speaking and under-standing
language •Problem solving •Orienting to day, year, season •Orienting to where they are •Orienting to who they are

Aphasia
Agnosia
Apraxia
The Four “A”s of Dementia & the Brain
What does the person experience?
Dementia Experience
• Poor judgment and decision making
• Inability to manage a budget
• Losing track of the passage of time or the season
• Difficulty having a conversation
• Misplacing things and being unable to retrace steps to find them
Feelings

The Fear and Anxiety of Dementia
• Dementia affects the brains ability to: – Deal with uncertainty and change
– Communicate concerns and fears
– “Self-sooth,” keep fears from becoming an overwhelming experience
• Chronic pain, common in the elderly, further increases anxiety as individuals with dementia cannot tell us they are in pain
• Inability to cope with anxiety and fear can result in defensive actions
– Verbal aggressive behavior and/or
– Physically aggressive behavior

How Can We Help? Emotions and Feelings Remain
Emotions continue even when the event
cannot be remembered

Understanding Actions & Expressions
Actions
Body Language
E XPRE S S I ONS

Communication Techniques
Be aware of your non-verbal communication
Center yourself!
Be aware of the non-verbal
communication signs the
person is showing to you

Understand How the Person Feels

Triggers to Actions/Expressions
Expressions
Triggers Emotions
Actions

Communication Techniques
Communicate care and comfort
Speak simply, smile, good eye contact
Use Gentle Touch
Music, singing, or reading
Favorite smells
Understanding the person’s non-verbal message
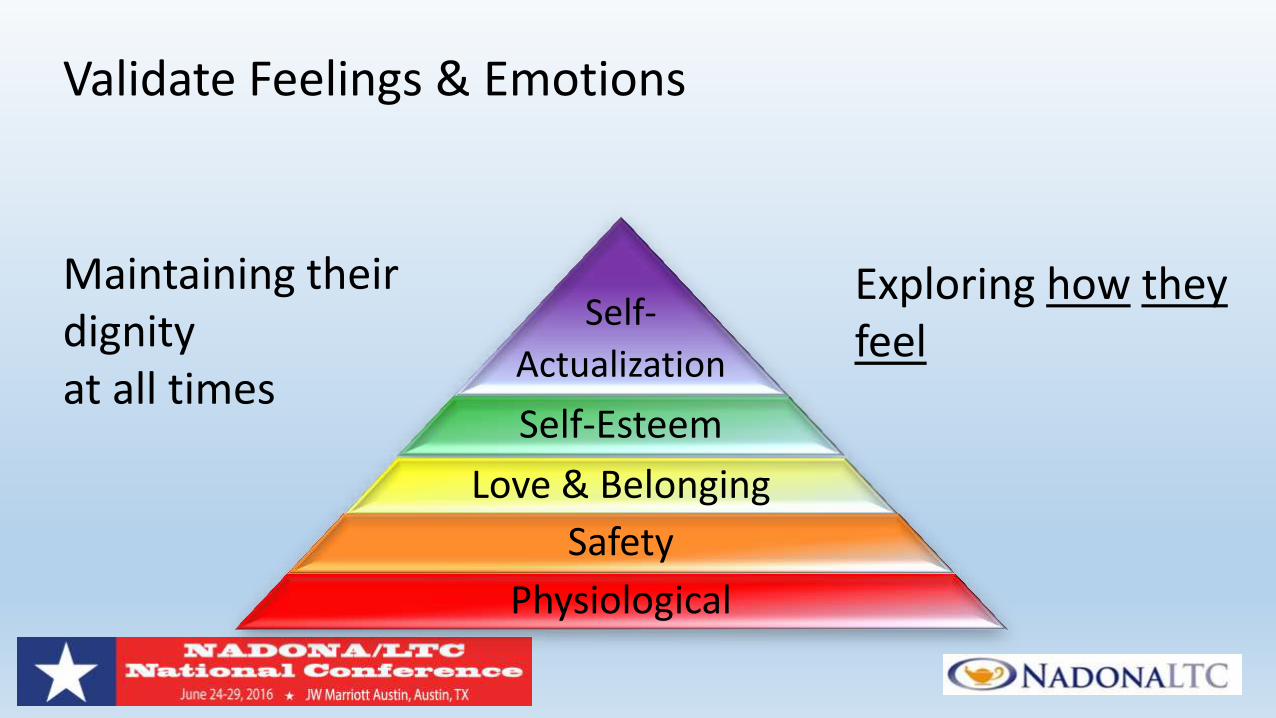
Validate Feelings & Emotions
Self-
Actualization
Self-Esteem
Love & Belonging
Safety
Physiological
Maintaining their dignity at all times
Exploring how they feel

PCA Think Comfort Model

Case Studies
• DON role in understanding actions and expressions
• Tracking actions and expressions - tools
• Route Cause Analysis adapted to the situation –
Think Comfort
• Finding the plan of care and services that matches
the needs/wants/desires of the person
• Staff critically thinking to obtained positive outcomes
• Decreasing antipsychotic medication utilization

Think Comfort!
Behavior
1. Agitated
2. Attempting to leave
3. Calling out repeatedly
4. Combative behaviors
5. Choosing not to take their medications
6. Resisting Care
7. Rummaging and Hording
8. Socially inappropriate behaviors
9. Wandering
Expression 1. I am overstimulated or bored
2. I want to go outside
3. I am in pain
4. You are not listening to me
5. I do not like the taste of the pills
6. I am cold; I am embarrassed; I do not know who your are
7. I am trying to find something or I do not wish to loose what is familiar
8. I want to be loved
9. I do not see anything familiar and am trying to find my home
The Resident Cannot Change, so...
Change the caregiver’s approach (ex - one instruction at a time)
Change the environment (ex - remove distractions)
Change the task (ex - are you trying to do something “for” or
“with” the person?)

Active Engagement ……..
• Supports relationships • Love and Belonging
• Engages the person in daily life • Self Esteem and Choice
• Offers a variety of creative and interesting choices • Self Actualization
• Allows for spontaneity • Just enjoyment of life!

Daily engagement ………………
• Allows the person to be productive
• Allows the person to experience success
• Retains and continues to build skills
• Provides the ability to control daily life
• Fulfills spiritual needs
• Experiences growth and learning
• Supports fun and enjoyment of life!

Levels of Programming
• Self Directed
• Structured
• Guided

Self- Directed Programming

Structured Programming

Guided Programming
A Person Centered Approach to Decreasing Actions/Expressions
Engagement in meaningful activities
is one of the most critical elements of an exceptional memory care program.
Activities help residents maintain
their functional abilities and can enhance quality of life. Alzheimer’s Association

References • Cohen-Mansfield, J., Marx, M. S., Regier, N. G., & Dakheel-Ali, M. (2009). The impact of personal characteristics on engagement in nursing home residents with dementia. Int. J. Geriat. Psychiatry, 24(7), 755-763.
doi:10.1002/gps.2192
• Cohen-Mansfield, J., Thein, K., Dakheel-Ali, M., & Marx, M. S. (2010). Engaging nursing home residents with dementia in activities: The effects of modeling, presentation order, time of day, and setting characteristics. Aging & Mental Health, 14(4), 471-480. doi:10.1080/13607860903586102
• Cohen-Mansfield, J., Marx, M. S., Dakheel-Ali, M., Regier, N. G., Thein, K., & Freedman, L. (2010). Can Agitated Behavior of Nursing Home Residents with Dementia Be Prevented with the Use of Standardized Stimuli? Journal of the American Geriatrics Society, 58(8), 1459-1464. doi:10.1111/j.1532-5415.2010.02951.x
• Roberts, G., Morley, C., Walters, W., Malta, S., & Doyle, C. (2015). Caring for people with dementia in residential aged care: Successes with a composite person-centered care model featuring Montessori-based activities. Geriatric Nursing, 36(2), 106-110. doi:10.1016/j.gerinurse.2014.11.003
• Vance, D. E., & Porter, R. J. (2001). Montessori Methods Yield Cognitive Gains in Alzheimer's Day Cares. Activities, Adaptation & Aging, 24(3), 1-22. doi:10.1300/j016v24n03_01
• Chirileanu, R. D., Simu, M., Rosca, C., Males, S., & Tocai, R. (n.d.). Mild Cognitive Impairment-Current Relevance of the concept, 2008.
• Flo, E., Gulla, C., & Husebo, B. S. (2014). Effective Pain Management in Patients with Dementia: Benefits Beyond Pain? Drugs Aging, 31(12), 863-871. doi:10.1007/s40266-014-0222-0
• PULSFORD, D., & DUXBURY, J. (2006). Aggressive behaviour by people with dementia in residential care settings: a review. Journal of Psychiatric and Mental Health Nursing, 13(5), 611-618. doi:10.1111/j.1365-2850.2006.00964.x
• Inouye, S. K. (2015). Enhancing Cognitive Aging: Clinical Highlights of a Report From the Institute of Medicine. Annals of Internal Medicine, 163(4), 307. doi:10.7326/m15-1228
• Kales, H. C., Gitlin, L. N., & Lyketsos, C. G. (2014). Management of Neuropsychiatric Symptoms of Dementia in Clinical Settings: Recommendations from a Multidisciplinary Expert Panel. Journal of the American Geriatrics Society, 62(4), 762-769. doi:10.1111/jgs.12730
• Ducharme, F., Kergoat, M., Coulombe, R., Lévesque, L., Antoine, P., & Pasquier, F. (2014). Unmet support needs of early-onset dementia family caregivers: a mixed-design study. BMC Nurs, 13(1). doi:10.1186/s12912-014-0049-3
• Hopper, T., Bourgeois, M., Pimentel, J., Qualls, C. D., Hickey, E., Frymark, T., & Schooling, T. (2013). An Evidence-Based Systematic Review on Cognitive Interventions for Individuals With Dementia. American Journal of Speech-Language Pathology, 22(1), 126. doi:10.1044/1058-0360(2012/11-0137)
• Cipriani, G., Vedovello, M., Nuti, A., & Di Fiorino, M. (2011). Aggressive behavior in patients with dementia: Correlates and management. Geriatrics & Gerontology International, 11(4), 408-413. doi:10.1111/j.1447-0594.2011.00730.x
• Bell, V., & Troxel, D. (1997). The best friends approach to Alzheimer's care. Baltimore, MD: Health Professions Press.
• Thomas, W. H. (1996). Life worth living: How someone you love can still enjoy life in a nursing home : the Eden alternative in action. Acton, MA: VanderWyk & Burnham.
• Power, G. A. (2010). Dementia beyond drugs: Changing the culture of care. Baltimore: HPP/Health Professions Press.
• Calkins, M. P. (2001). Creating successful dementia care settings. Baltimore, MD: Health Professions Press.

Question and Answer
• Margaret Kimbell [email protected]
410-402-2481
• Bettina Suarez Palacios [email protected]
410-402-2275

















