Page 1
IM - ORIGINAL
A pharmacoepidemiological study of the multi-level determinants,predictors, and clinical outcomes of biosimilar epoetin alfafor renal anaemia in haemodialysis patients: backgroundand methodology of the MONITOR-CKD5 study
Loreto Gesualdo • Gerard London • Matthew Turner • Christopher Lee • Karen MacDonald •
David Goldsmith • Adrian Covic • Philippe Zaoui • Christian Combe • Johannes Mann •
Frank Dellanna • Michael Muenzberg • Ivo Abraham
Received: 25 January 2011 / Accepted: 29 April 2011 / Published online: 18 May 2011
� SIMI 2011
Abstract Prior longitudinal observational studies have
examined the practice patterns and outcomes of anaemia
management, including the use of erythropoiesis-stimulating
agents (ESAs). Several dimensions of effectiveness remain
unaddressed; especially considering the revised ESA label
(target Hb levels between 10 and 12 g/dL), the recently
published TREAT study, and the European approval of the
first ESA biosimilar (HX575). Anecdotal evidence suggests
that patient outcomes are influenced by physician-related
variables and whether anaemia management is congruent
with practice guidelines, but this has not been studied sys-
tematically. MONITOR-CKD5 is an international, pro-
spective, observational, pharmacoepidemiological study
evaluating the multi-level factors and outcomes of treatment
with HX575 for renal anaemia in haemodialysis patients.
Driven by a novel, integrated, multi-focal framework for
post-approval observational studies, it examines determi-
nants of response at both the patient and the physician level;Trial Registration:clinicaltrials.gov NCT01121237
L. Gesualdo
Department of Nephrology, Universita degli Studi di Bari, Bari,
Italy
e-mail: [email protected]
G. London
Department of Nephrology and Hemodialysis, Centre Hospitalier
F. H. Manhes, Fleury-Merogis, France
e-mail: [email protected]
M. Turner � M. Muenzberg
Sandoz Biopharmaceuticals, Holzkirchen, Germany
e-mail: [email protected]
M. Muenzberg
e-mail: [email protected]
C. Lee � K. MacDonald � I. Abraham (&)
Matrix45, 620 Frays Ridge Road, Earlysville, VA 22936, USA
e-mail: [email protected]
C. Lee
e-mail: [email protected]
K. MacDonald
e-mail: [email protected]
C. Lee � I. Abraham
Center for Health Outcomes and Pharmaco-economic Research,
College of Pharmacy, The University of Arizona, Tucson, AZ,
USA
D. Goldsmith
King’s Health Partners, Guy’s and St Thomas’ NHS Foundation
Hospital, London, UK
e-mail: [email protected]
A. Covic
Dialysis and Transplantation Center, G. I. Popa University
Hospital of Medicine and Pharmacy, Iasi, Romania
e-mail: [email protected]
P. Zaoui
Centre Hospitalier Universitaire de Grenoble and Universite de
Grenoble, Grenoble, France
e-mail: [email protected]
C. Combe
Department of Nephrology and INSERM U889, Centre
Hospitalier de Bordeaux and Universite de Bordeaux 2–Victor
Segalen, Bordeaux, France
e-mail: [email protected]
J. Mann
Schwabing Klinikum and Friedrich Alexander Universitat
Erlangen-Nurnburg, Munich, Germany
e-mail: [email protected]
F. Dellanna
Dialysezentrum, Duesseldorf, Germany
e-mail: [email protected]
123
Intern Emerg Med (2013) 8:389–399
DOI 10.1007/s11739-011-0622-7
Page 2
integrates an advocated statistical methodology here to fore
used mainly in the social and behavioural sciences; assesses
factors potentially predictive of a poor treatment response;
and evaluates the extent to which treatment is congruent with
evidence-based guidelines, good practice evidence, and the
revised ESA label. This pan-European study will recruit at
least 1,000 patients from a minimum of 75 centres, and follow
them for up to 24 months following initiation of anaemia
management with biosimilar epoetin alfa. MONITOR-CKD5
will not only study the core issues addressed by prior obser-
vational studies but also aims to take knowledge discovery a
step further by assessing outcomes across varying cohorts of
patients, and examining the impact of evidence-based practice
on clinical outcomes, differentiating, in the process, between
physician-level and patient-level determinants.
Keywords Biosimilar � Erythropoietin � Haemodialysis �Pharmacoepidemiology � Renal anaemia
Abbreviations
ANOVA Analysis of variance
CKD Chronic kidney disease
CKD5 Chronic kidney disease stage 5
CRF Case report form
DOPPS Dialysis Outcomes and Practice Patterns
Study
eCRF Electronic case report form
ESA Erythropoiesis-stimulating agent
ESAM European Survey on Anaemia Management
GFR Glomerular filtration rate
Hb Haemoglobin
HR Hazard ratio
MANOVA Multivariate analysis of variance
RCT Randomized controlled trial
RRT Renal replacement therapy
v2 Chi-squared
Introduction
Normochromic normocytic anaemia develops in approxi-
mately two-thirds of patients with chronic kidney disease
(CKD), and in almost all patients with Stage 5 chronic
kidney disease (CKD5) requiring renal replacement ther-
apy (RRT) [1]. Referred to also as renal anaemia, the
predominant cause is inadequate erythropoiesis: failure of
the kidneys to produce endogenous erythropoietin to
stimulate the bone marrow to produce erythrocytes [2].
Renal anaemia is an amenable condition when properly
identified and treated.
CKD5 is defined as having a glomerular filtration rate
(GFR) \ 15 mL/min/1.73 m2 or the requirement of RRT
[3]. Renal anaemia is problematic in this population
because of the higher and graded risk and degree of
anaemia with a lower GFR [4], and the elevated risk of
morbidity, hospitalization, and mortality if not treated
effectively [5, 6]. Evidence-based guidelines such as
K/DOQI and the European Best Practice Guidelines[7–9]
advocate an anaemia work-up for CKD patients with a
haemoglobin (Hb) concentration below the age- and gen-
der-adjusted population mean minus two standard deviations
(i.e., Hb \ 11.5 g/dL in adult women, Hb \ 13.5 g/dL in
adult men, and Hb \ 12.0 g/dL in adult men age[70); and for
managing moderate anaemia with erythropoiesis-stimulating
agents (ESAs) to maintain a target Hb level of 11–12 g/dL
without exceeding 13 g/dL [7–9].
Despite these guidelines and about 20 years of clinical
experience with ESAs in renal anaemia (including the first
biosimilar), large observational studies such as ESAM and
DOPPS indicate that target Hb levels are often unrealized
[10–13]; with other aspects of the care of CKD5 patients
often not being in concordance with guidelines [10, 12, 14–
17]. This suggests that in addition to patient-level charac-
teristics [18, 19], ‘‘real-world’’ practice patterns of the
treating clinician, including selection of target Hb levels,
ESA dosing and frequency, and general CKD guideline
concordance, have an impact upon Hb outcomes in CKD5
patients [15, 16]. Specifically, it has not been studied how
physician-level variables contribute to CKD5 patients
remaining at risk for poor Hb control, morbidity, hospi-
talization and mortality despite ‘‘treatment.’’ Multi-level
modelling (considering both patient- and provider-level
characteristics) is a robust, advocated method for the
evaluation of treatment effectiveness in clinical nephrol-
ogy research [20], and helps fill important gaps in
explaining variability in Hb outcomes in CKD5 patients
[19, 21, 22].
Though the recently published TREAT study [23] was
focused on non-dialysed Type 2 diabetes patients with
moderate to severe CKD (and not on haemodialysis
patients), this study comparing protocol driven ESA ther-
apy with darbepoetin alfa to placebo, underscores the
importance of mapping current treatment practice in
varying cohorts of patients. The study’s findings have
produced commentaries from the negative [24] to the more
balanced [25]. Two common themes are, first, the extent to
which the same Hb target might apply across the board to
all potential recipients of ESAs—old versus young,
comorbidity-complicated versus uncomplicated, diabetic
versus not—given that the risk–benefit calculations might
diverge between these different patient groups. Second, is
the role of adequate and timely management of absolute
and functional iron deficiencies, and the integration of iron
management and ESA therapy. The issues must be
addressed through observational studies of real-world
390 Intern Emerg Med (2013) 8:389–399
123
Page 3
practice to better understand how variability in treatment
practice translates into variability in patient outcomes.
The adoption of evidence-based guidelines in medicine
has been called mixed and disappointing [26]. The extent
to which anaemia management in haemodialysis patients is
congruent with guidelines has not been studied. Further,
Port and colleagues used DOPPS data to show how six
modifiable haemodialysis parameters are associated with
reductions in mortality: dialysis dose, phosphate control,
anaemia, serum albumin (as a marker for nutrition), inter-
dialytic weight gain, and the use of catheters for vascular
access. It merits investigation of whether, on the whole,
adequate haemodialysis care translates into better patient
outcomes [15].
In addition to these scientific issues, the recent approval
of the first biosimilar recombinant human erythropoietin
(HX575, marketed as Binocrit� and Epoetin Alfa Hexal�)
[27–30] brings with it the need for observational studies to
examine how this agent is used in daily practice, and the
clinical outcomes achieved.
A last factor concerns the recent changes in the Euro-
pean label for ESAs, which set target Hb levels in the
10–12 g/dL range. Whether daily practice is congruent
with this revised label has not been evaluated.
Framework for observational effectiveness studies
Randomized controlled trials (RCT) are the indicated
method for determining the efficacy of pharmacological
agents. However, by necessity RCTs are constrained in
terms of patients and clinicians included, and treatments
must be limited to the agent under investigation so as to be
able to draw unconfounded efficacy inferences. Observa-
tional studies are needed to examine the effectiveness of
drugs previously documented to be efficacious: how a
treatment works under ordinary and variable conditions,
prescribed by licensed clinicians with varying degrees of
expertise, and practicing across the spectrum of healthcare
settings, to treat a heterogeneity of eligible patients. Most
observational studies focus narrowly on evaluating a
treatment’s effectiveness under ‘‘real-world’’ conditions,
leaving key questions unanswered. The question of
‘‘whether the treatment works?’’, while critical, does not
address the equally important questions of ‘‘when does the
treatment work, and when not?’’, ‘‘in whom does the
treatment work, and in whom not?’’, ‘‘why does the treat-
ment work in some patients but not in others?’’, ‘‘why does
the treatment work with some clinicians but not with oth-
ers?’’, and ‘‘why is the treatment tolerated by some patients
but not by others?’’ To answer these questions, the
MONITOR-CKD5 study has adopted an integrated
framework for observational effectiveness studies, used
now in several studies, that has become a de facto quality
model to assure clinical relevance, scientific value, and
technical merit (see Fig. 1).
Aims
Within the framework (Fig. 1), the study’s primary aim is
to describe the haemodialysis patient population with renal
anaemia being treated with marketed Binocrit� or Epoetin
Alfa Hexal� (HX575) per their prescribing physician’s best
clinical judgment; assess treatment patterns involving this
agent, (including the extent to which these are congruent
with the approved label and clinical practice guidelines);
evaluate Hb level and Hb variability outcomes; and
examine time to and determinants of any hospitalizations,
thrombo-embolic/vascular events, and mortality. Second-
arily, this study aims to identify patient cohorts who are
vulnerable to poor treatment response, and to understand
the differences between those patients who do and those
who do not respond to treatment with HX575.
Fig. 1 Framework for observational effectiveness studies
Intern Emerg Med (2013) 8:389–399 391
123
Page 4
Objectives and research questions
The study’s objectives and associated research questions,
as derived from the framework (Fig. 1), are as follows:
Primary objectives
• Case-finding and patient description
• Objective 1 To describe the patients requiring
haemodialysis who, in their treating physician’s
best clinical judgment, are receiving HX575 for the
treatment of renal anaemia in terms of demograph-
ics, clinical status, medical history, concomitant
comorbid conditions, current status of disease, and
prior and concomitant medications.
• Treatment patterns
• Objective 2 To describe HX575 treatment patterns
for renal anaemia over up to 24 months of
treatment.
• Congruence of treatment with labels and guidelines
• Objective 3 To determine the extent to which the
management of renal anaemia in haemodialysis
patients is in congruence with prevailing best
practice guidelines and approved label in terms of
target Hb levels, treatment initiation, and treatment
modification; and whether this is associated with
better treatment outcomes.
• Objective 4 To determine the extent to which the
overall management of patients with CKD5 is in
congruence with Port et al.’s [15] evidence regard-
ing modifiable risk factors for poor patient out-
comes; and whether this is associated with better
treatment outcomes.
• Description of observed outcomes
• Objective 5 To describe Hb outcomes observed over
up to 24 months of treatment with HX575 for renal
anaemia in patients with CKD5.
• Objective 6 To describe the distribution of safety
outcomes and estimate the time-to-event for first
overnight hospitalization, for thrombo-embolic/vas-
cular events, and for all-cause mortality over up to
24 months of treatment with HX575.
• Multi-level determinants of outcomes
• Objective 7 To examine the multi-level determi-
nants (patient and physician/centre) and Hb and
safety outcomes of treatment with HX575 to better
understand the variability in Hb and safety out-
comes achieved.
Secondary objectives
• Cohort identification and differentiation
• Objective 8 To identify different latent clusters of
patients with CKD5 receiving HX575 for the
treatment of renal anaemia using statistical data-
mining techniques to profile patients based on
medical history, concomitant comorbid conditions,
and current clinical status.
• Non-responder analyses
• Objective 9 To model patient- and physician/centre-
level variables between patients who respond, and
those who do not respond to treatment with HX575.
• Objective 10 To model patient- and physician/
centre-level variables between patients who had C1
overnight hospitalization, and those who were hospi-
talization-free during up to 24 months of treatment
with HX575.
• Objective 11 To model patient- and physician/
centre-level variables between patients with thrombo-
embolic events, and those free from thrombo-embolic/
vascular events during up to 24 months of treatment
with HX575.
• Objective 12 To model patient- and physician/
centre-level variables between patients who die, and
those who survive during treatment with HX575.
Safety, including immunogenicity, will also be monitored
throughout the study.
Methods/design
Study design
MONITOR-CKD5 is an international, prospective, obser-
vational, multi-level, pharmacoepidemiological study in
which haemodialysis patients are started on commercially
available HX575 (Binocrit� or Epoetin Alfa Hexal�) for
the treatment of renal anaemia per their prescribing
physician’s best clinical judgment. Potential centres and
physician-investigators are identified by the local affiliate of
the study sponsor (Sandoz Biopharmaceuticals, Holzkirchen,
Germany) using a Study Briefing document summarizing the
study (Fig. 2).
The multi-level design of this observational study is
warranted for both clinical and statistical reasons. Clini-
cally, it can be assumed that patients under the care of the
same physician (or, for that matter, at the same centre) are
uniquely and exclusively exposed to that physician’s
knowledge, experience, expertise, and clinical practice
patterns. At the centre level, patient care may be influenced
392 Intern Emerg Med (2013) 8:389–399
123
Page 5
by clinical policies, procedures, and protocols. Statistically,
this exposure to the same physician or centre means that
these patients are treated with a certain communality that
may be different across investigators and centres partici-
pating in the study. Extending this across physician-
investigators and centres, observations on the total sample
of patients are not independent, thus violating a major
assumption for statistical testing. In multi-level (or hierarchical
linear) modelling, the effect of class (e.g., treating physician)
on patient-level outcomes are estimated before the effect
of between-patient variability is determined; yielding an
attribution of variance and identification of level-specific
predictors of patient outcomes that separates between-class
and within-patient variability.
The enrolment period is 36 months. Patients will be
evaluated monthly for up to 24 months. The total duration
of the study protocol is 60 months. The MONITOR-CKD5
study is a pan-European study to which Austria, Belgium,
France, Germany, Italy, Spain, Switzerland, Poland,
Romania, Slovenia and the United Kingdom have already
committed (and assured the required sample size). Addi-
tional countries may join as HX575 market entry expands
in the coming years.
Identification of eligible patients
Both ESA-naive patients and patients previously treated
with other ESAs will be screened for eligibility. Those
meeting the inclusion and exclusion criteria will be
informed about the study and written informed consent will
be obtained.
Patient inclusion criteria
To be included, patients should be male or female adults
(age [ 18 years), on chronic haemodialysis for any dura-
tion due to end-stage renal disease (CKD5) of original or
grafted kidneys, diagnosed with renal anaemia, and treated
with commercially available HX575 (Binocrit� or Epoetin
Alfa Hexal�) per physician’s best clinical judgment, and
under consideration of available guidance and evidence.
Female patients must be either post-menopausal for 1 year,
surgically sterile, or using effective contraceptive methods
such as barrier method with spermicide, an intra-uterine
device, or oral contraceptives. Informed consent to partic-
ipate in the study must be granted by patient or a legal
guardian.
Fig. 2 Study briefing document used for centre and physician-investigator recruitment
Intern Emerg Med (2013) 8:389–399 393
123
Page 6
Patient exclusion criteria
Excluded are patients who demonstrate any of the fol-
lowing: known sensitivity to HX575 or any other ESA;
diagnosed with solid or haematological neoplasia treated
with chemotherapy; treatment with any myelosuppressant
medications; blood transfusion dependency; a history of
pure red cell aplasia; a bleeding episode in 30 days prior
to enrolment; orthopaedic surgery in 30 days prior to
enrolment; medical condition(s) that in the view of the
investigator prohibit(s) participation in the study; or
wilfully negligent non-adherence to their haemodialysis,
medication, nutrition, or other recommended treatment
regimens.
Setting
This study will be conducted in haemodialysis centres
throughout Europe. While patients are the main study
population, the multi-level design of the study also requires
a minimum number of physician-investigators. At least
1,000 patients (allowing for a 25% attrition rate) are to be
recruited by a minimum of 75 centres to achieve the
statistical power needed to meet the study objectives. To
enable the greatest possible diversity in physician-investi-
gators so as to better reflect the heterogeneity of providers,
physician criteria are limited to any person licensed to
practise medicine in his/her country of origin and practic-
ing, at least part-time, in a haemodialysis centre.
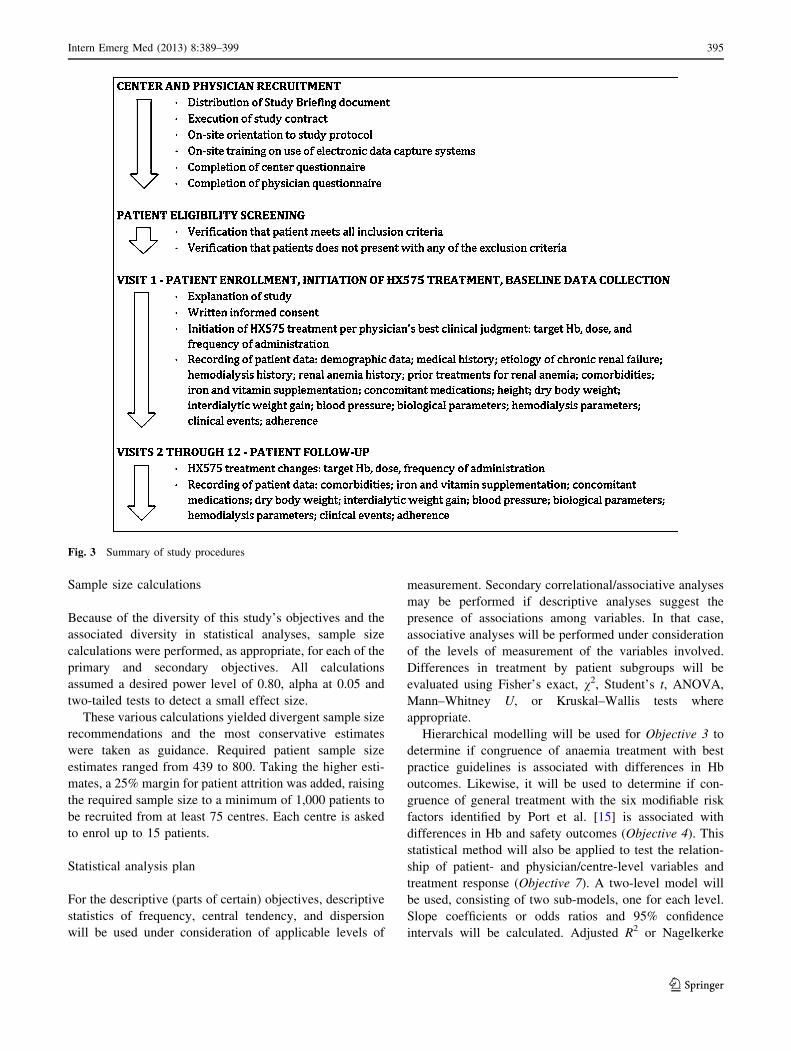
Data collection and management
Figure 3 summarizes the main procedures of the MONI-
TOR-CKD5 study. Table 1 presents the study’s timetable
and the assessments to be performed at each time point.
Being an observational study, all data will be recorded as
available. There are no mandatory treatment regimens,
assessments, and tests. Investigators enter data from source
documents into the electronic CRF (See Fig. 4 for an eCRF
screen shot). Centralized monitoring will be performed by
a contract research organization, which will also assure
query management. With the centres’ knowledge, a ran-
dom selection of 10% of patients will be identified for
complete on-site monitoring. Data will be transmitted by
the eCRF vendor to Matrix45 for assessment of data
integrity, statistical analysis, and dissemination.
Fig. 2 continued
394 Intern Emerg Med (2013) 8:389–399
123
Page 7
Sample size calculations
Because of the diversity of this study’s objectives and the
associated diversity in statistical analyses, sample size
calculations were performed, as appropriate, for each of the
primary and secondary objectives. All calculations
assumed a desired power level of 0.80, alpha at 0.05 and
two-tailed tests to detect a small effect size.
These various calculations yielded divergent sample size
recommendations and the most conservative estimates
were taken as guidance. Required patient sample size
estimates ranged from 439 to 800. Taking the higher esti-
mates, a 25% margin for patient attrition was added, raising
the required sample size to a minimum of 1,000 patients to
be recruited from at least 75 centres. Each centre is asked
to enrol up to 15 patients.
Statistical analysis plan
For the descriptive (parts of certain) objectives, descriptive
statistics of frequency, central tendency, and dispersion
will be used under consideration of applicable levels of
measurement. Secondary correlational/associative analyses
may be performed if descriptive analyses suggest the
presence of associations among variables. In that case,
associative analyses will be performed under consideration
of the levels of measurement of the variables involved.
Differences in treatment by patient subgroups will be
evaluated using Fisher’s exact, v2, Student’s t, ANOVA,
Mann–Whitney U, or Kruskal–Wallis tests where
appropriate.
Hierarchical modelling will be used for Objective 3 to
determine if congruence of anaemia treatment with best
practice guidelines is associated with differences in Hb
outcomes. Likewise, it will be used to determine if con-
gruence of general treatment with the six modifiable risk
factors identified by Port et al. [15] is associated with
differences in Hb and safety outcomes (Objective 4). This
statistical method will also be applied to test the relation-
ship of patient- and physician/centre-level variables and
treatment response (Objective 7). A two-level model will
be used, consisting of two sub-models, one for each level.
Slope coefficients or odds ratios and 95% confidence
intervals will be calculated. Adjusted R2 or Nagelkerke
Fig. 3 Summary of study procedures
Intern Emerg Med (2013) 8:389–399 395
123
Page 8
pseudo R2 also will be calculated where appropriate. The
intraclass correlation coefficient will be used to quantify
the variability in patient outcome attributable to within-
physician/centre variability before any patient-level deter-
minants are considered. This method will also be applied in
Cox proportional hazards modelling (calculating adjusted
hazards ratios and 95% confidence intervals) of safety
outcomes. In addition, in an exploratory fashion and data
permitting, time-dependent covariates will be assessed in
multivariate Cox proportional hazards models; evaluating
the multi-level determinants of the count of overnight
hospitalizations using hierarchical Poisson regression
modelling, calculating incident rate ratios and 95% confi-
dence intervals.
For Objective 5, a Nesselroade–Salthouse index of intra-
individual variation in Hb (‘‘Intra-Hb’’) levels will be
calculated. One-way (within-subjects) and factorial
(within-subjects and between-subjects) repeated measures
analysis of variance using the Geisser–Greenhouse
corrected F test will be used. In addition, though in an
exploratory fashion and data permitting, a time series
analysis under various scenarios of autoregressive lag will
be attempted to explore the presence of trend effects in the
data. Multiple classifications of Hb levels and variability
will be performed using descriptive statistics to be included
in predictive modelling and non-responder analyses.
Proportions, median follow-up duration, median event-
free survival times, and events per patient year will be used
to describe the safety endpoints of overnight hospitaliza-
tion, thrombo-embolic/vascular events and all-cause
mortality over the entire study period (Objective 6). The
distribution of events and event-free survival will be
described for the entire sample using Kaplan–Meier esti-
mator modelling. Mantel-Cox log-rank tests (weighing all
time points equally) or generalized Wilcoxon/Breslow tests
(weighing time points relative to the number of cases at
risk at each time point) will be used to evaluate bivariate
differences in survival distribution between identified
Table 1 Timetable and assessment schedule of the MONITOR-CKD5 Study
Visit 1 2 through up to 23 Up to 24
Month 1 2 through 23 Up to 24
Inclusion/exclusion criteria X
Informed consent/patient permission X
Demographic data X
Medical history X
Aetiology of chronic renal failure X
Haemodialysis history X
Renal anaemia history, incl. Hb values in 3 months prior to enrolment X
Prior treatments for renal anaemia, incl. data for 3 months prior to enrolment
(incl. blood transfusions, iron supplementation, ESAs)
X
Target Hb for HX575 treatment X X X
HX575 dose and frequency X X X
Comorbidities X X X
Iron supplementation X X X
Vitamin supplementation X X X
Relevant concomitant medications X X X
Height X
Dry body weight X X X
Interdialytic weight gain X X X
Blood pressure X X X
Biological parameters (Hb, iron parameters, serum albumin, C-reactive protein,
serum aluminium, phosphate and calcium)
X X X
Haemodialysis parameters (dialysis dose [Kt/V], hours of dialysis/week, blood
flow rate, membranes, vascular access)
X X X
Clinical events (infection, bleeding, thrombo-embolism, cardiovascular, surgery,
arteriovenous fistula thrombosis, neoplasia onset, renal transplantation, transfer
to peritoneal dialysis, blood transfusions, transfer to other haemodialysis centre, death)
X X X
Adherence assessment X X X
Physician’s questionnaire (demographics, knowledge of anaemia and general CKD guidelines) X
Centre characteristics, anaemia protocols, adoption of anaemia guidelines X
396 Intern Emerg Med (2013) 8:389–399
123
Page 9
subgroups. Cox proportional hazards modelling will be
used to analyse the multivariate effects of identified risk
factors and other determinants on survival under the pro-
portional hazards assumption. Adjusted hazards ratios
(HRs) and 95% confidence intervals will be calculated to
test the direction and strength of the influence of individual
factors on event-risk and event-free survival. Omnibus tests
of model coefficients, -2 log likelihood and Nagelkerke
pseudo R2 will be calculated to determine variable block
and overall model fit and significance.
For Objective 8, we will apply sequentially a series
of increasingly more complex procedures: aggregation
techniques (‘‘classification and clustering methods’’),
differentiation techniques (‘‘tree-based models’’), and
associative and pattern recognition techniques (e.g.,
‘‘neural networks’’). Aggregation procedures will be done
on the sample as a whole. However, if we need to migrate
to differentiation and associative/pattern recognition pro-
cedures, we will randomly divide the sample into a training
set (for model development) and a testing set (for model
validation).
Lastly, Objective 9 through 12 will be analysed using
multiple logistic regression, Kaplan–Meier estimation, and
Cox proportional hazards modelling.
In addition to the end-of-study analyses, interim analy-
ses are planned after patients enrolled in the first 3 months
of the enrolment period and all patients enrolled by month
36 have completed 12 months of follow-up (resp. months
15 and 48); and after 12 (resp. months 27 and 64) and 24
(resp. months 39 and 76) months later for each subgroup;
using a Pocock-adjusted level of statistical significance [31,
32].
Ethical considerations
Ethics Committee approvals for this study have been
sought in accordance with the laws and regulations appli-
cable to observational studies in each of the participating
countries. No centre will be allowed to begin eligibility
screening until the necessary approvals have been obtained.
Withdrawal from study
Subjects may withdraw from the study at any time and for
whatever reason as explained in the informed consent
materials.
Discussion
The ESAM and especially the DOPPS studies have contrib-
uted significantly to the understanding of practice patterns and
outcomes of anaemia management in haemodialysis patients.
While identifying practices, outcomes, and key determinants,
Fig. 4 Example of a webpage for electronic data collection
Intern Emerg Med (2013) 8:389–399 397
123
Page 10
several dimensions of effectiveness remain unaddressed.
Using a comprehensive, integrated framework, addressing the
need for effectiveness studies on biosimilar epoetin alfa, and
examining the relationship between guideline-, label- and
other evidence-congruent practice, the MONITOR-CKD5
intends to study the core issues addressed by ESAM and
DOPPS, but also to take knowledge discovery a step further by
examining the impact of evidence-based practice on clinical
outcomes—differentiating, in the process, between physician-
level and patient-level determinants. Further, the MONITOR-
CKD5 is the first pharmacoepidemiological study on anaemia
management in haemodialysis since there is a change in ESA
label and the target Hb level restriction to the 10–12 g/dL
range.
The MONITOR-CKD5 study is an international, pro-
spective, observational, pharmacoepidemiological study to
evaluate the multi-level factors and outcomes associated with
the use of HX575 in the treatment of renal anaemia in hae-
modialysis patients across varying cohorts of patients. It aims
to examine determinants of response at both the patient and the
physician level; integrates an advocated [20] statistical
methodology hereto used mainly in the social and behavioural
sciences; assesses factors potentially predictive of poor
treatment response; evaluates the extent to which treatment is
congruent with evidence-based guidelines and the revised
ESA label; while also relying on the experiences gained in
such observational studies as ESAM and DOPPS.
Acknowledgments The study is sponsored by research grants from
Sandoz Biopharmaceuticals, a Novartis company, Holzkirchen,
Germany. The authors thank Liam Smith for editorial, proofreading,
and administrative assistance. Data will be analysed independently
from the Sponsor, although the Sponsor will have the right of review
and comment.
Conflict of interest L. Gesualdo, G. London, D. Goldsmith, A.
Covic, P. Zaoui, C. Combe, J. Mann, and F. Dellanna serve as con-
sulting investigators to the MONITOR-CKD5 study. M. Turner and
M. Muenzberg are employees of Sandoz Biopharmaceuticals. C. Lee,
K. MacDonald, and I. Abraham are employees of Matrix45. By
company policy, they are prohibited from owning equity in client
organizations (except through mutual funds or other independently
administered collective investment instruments) or contracting inde-
pendently with client organizations. Matrix45 provides similar
services for other biopharmaceutical companies.
References
1. McClellan WM, Jurkovitz C, Abramson J (2005) The epidemi-
ology and control of anemia among pre-ESRD patients with
chronic kidney disease. Eur J Clin Invest 35(Suppl 3):58–65
2. Eckardt KU (2000) Pathophysiology of renal anemia. Clin
Nephrol 53(Suppl):S2–S8
3. (2002) K/DOQI clinical practice guidelines for chronic kidney
disease: evaluation, classification, and stratification. Am J Kidney
Dis 39 (Suppl 1):S1–266
4. Astor BC, Muntner P, Levin A, Eustace JA, Coresh J (2002)
Association of kidney function with anemia: the Third National
Health and Nutrition Examination Survey (1988–1994). Arch
Intern Med 162:1401–1408
5. Locatelli F, Pisoni RL, Combe C et al (2004) Anemia in
hemodialysis patients of five European countries: association
with morbidity and mortality in the Dialysis Outcomes and
Practice Patterns Study (DOPPS). Nephrol Dial Transplant
19:121–132
6. Rao M, Pereira BJ (2005) Optimal anemia management reduces
cardiovascular morbidity, mortality, and costs in chronic kidney
disease. Kidney Int 68:1432–1438
7. (2007) K/DOQI Clinical Practice Guideline and Clinical Practice
Recommendations for anemia in chronic kidney disease: 2007
update of haemoglobin target. Am J Kidney Dis 50:471–530
8. Locatelli F, Aljama P, Barany P et al (2004) Revised European
best practice guidelines for the management of anemia in patients
with chronic renal failure. Nephrol Dial Transplant 19(Suppl 2):
ii1–ii47
9. Locatelli F, Covic A, Eckardt KU, Wiecek A, Vanholder R
(2009) Anemia management in patients with chronic kidney
disease: a position statement by the Anemia Working Group of
European Renal Best Practice (ERBP). Nephrol Dial Transplant
24:348–354
10. Jacobs C, Horl WH, Macdougall IC et al (2000) European Best
Practice Guidelines 5: target haemoglobin. Nephrol Dial Trans-
plant 15(Suppl 4):15–19
11. Jacobs C, Frei D, Perkins AC (2005) Results of the European
Survey on Anemia Management 2003 (ESAM 2003): current
status of anemia management in dialysis patients, factors
affecting epoetin dosage and changes in anemia management
over the last 5 years. Nephrol Dial Transplant 20(Suppl 3):
iii3–iii24
12. Pisoni RL, Bragg-Gresham JL, Young EW et al (2004) Anemia
management and outcomes from 12 countries in the Dialysis
Outcomes and Practice Patterns Study (DOPPS). Am J Kidney
Dis 44:94–111
13. Horl WH, Vanrenterghem Y, Canaud B et al (2005) Optimal
treatment of renal anemia (OPTA): improving the efficacy and
efficiency of renal anemia therapy in hemodialysis patients
receiving intravenous epoetin. Nephrol Dial Transplant 20(Suppl
3):iii25–iii32
14. Port FK, Pisoni RL, Bommer J et al (2006) Improving outcomes
for dialysis patients in the international Dialysis Outcomes and
Practice Patterns Study. Clin J Am Soc Nephrol 1:246–255
15. Port FK, Pisoni RL, Bragg-Gresham JL et al (2004)
DOPPS estimates of patient life years attributable to modifiable
hemodialysis practices in the United States. Blood Purif
22:175–180
16. Gilbertson DT, Ebben JP, Foley RN, Weinhandl ED, Bradbury
BD, Collins AJ (2008) Hemoglobin level variability: associations
with mortality. Clin J Am Soc Nephrol 3:133–138
17. Kimata N, Akiba T, Pisoni RL et al (2005) Mineral metabolism
and hemoglobin concentration among hemodialysis patients in
the Dialysis Outcomes and Practice Patterns Study (DOPPS).
Nephrol Dial Transplant 20:927–935
18. Rayner HC, Pisoni RL, Bommer J et al (2004) Mortality and
hospitalization in hemodialysis patients in five European coun-
tries: results from the Dialysis Outcomes and Practice Patterns
Study (DOPPS). Nephrol Dial Transplant 19:108–120
19. Volkova N, Arab L (2006) Evidence-based systematic literature
review of hemoglobin/hematocrit and all-cause mortality in
dialysis patients. Am J Kidney Dis 47:24–36
20. Holden JE, Kelley K, Agarwal R (2008) Analyzing change: a
primer on multilevel models with applications to nephrology. Am
J Nephrol 28:792–801
398 Intern Emerg Med (2013) 8:389–399
123
Page 11
21. Strippoli GF, Navaneethan SD, Craig JC (2006) Hemoglobin and
hematocrit targets for the anemia of chronic kidney disease.
Cochrane Database Syst Rev 4:CD003967
22. Locatelli F, Nissenson AR, Barrett BJ et al (2008) Clinical
practice guidelines for anemia in chronic kidney disease: prob-
lems and solutions. A position statement from kidney disease:
improving global outcomes (KDIGO). Kidney Int 74:1237–1240
23. Pfeffer M, Burdmann EA, Cooper DE et al (2009) A trial of
darbepoetin-alfa in type 2 diabetes and chronic kidney disease.
N Engl J Med 361:1–14
24. Singh AK (2009) Does TREAT give the boot to ESAs in the
treatment of CKD anemia. J Am Soc Nephrol 21:2–6
25. Goldsmith D, Covic A (2010) Time to reconsider evidence for
anaemia treatment (TREAT) = essential safety arguments
(ESA). Nephrol Dial Transplant 25:1734–1737
26. Timmermans S, Mauck A (2005) The promises and pitfalls of
evidence-based medicine. Health Aff 24:18–28
27. Sorgel F, Thyroff-Friesinger U, Vetter A et al (2009) Bioequiv-
alence of HX575 (IV) (recombinant human epoetin alfa) and a
comparator epoetin alfa after multiple subcutaneous administra-
tions: an open-label randomised controlled trial. BMC Clin
Pharmacol 9:10
28. Sorgel F, Thyroff-Friesinger U, Vetter A et al (2009) Bioequiv-
alence of HX575 (human recombinant epoetin alfa) and epoetin
beta after multiple subcutaneous administration. Int J Clin Phar-
macol Ther 6:391–401
29. Brockmeyer C, Seidl A (2009) Binocrit: assessment of quality,
safety, and efficacy of biopharmaceuticals. Eur J Hosp Pharm
Pract 15:34–40
30. Haag-Weber M, Vetter A, Thyroff-Friesinger U et al (2009)
Therapeutic equivalence, long-term efficacy and safety of HX575
in the treatment of anemia in chronic renal failure patients
receiving hemodialysis. Clin Nephrol 72:380–390
31. Geller NL, Pocock SJ (1987) Interim analyses in randomized
clinical trials: ramifications and guidelines for practitioners.
Biometrics 43:213–223
32. Schulz KF, Grimes DA (2005) Multiplicity in randomised trials
II: subgroup and interim analyses. Lancet 365:1657–1661
Intern Emerg Med (2013) 8:389–399 399
123