Annals of Biomedical Engineering, Vol. 34, No. 3, March 2006 ( C 2006) pp. 465–476 DOI: 10.1007/s10439-005-9045-9 A Probabilistic Model of Glenohumeral External Rotation Strength for Healthy Normals and Rotator Cuff Tear Cases JOSEPH E. LANGENDERFER, 1, 2 JAMES E. CARPENTER, 1, 3 MARJORIE E. JOHNSON, 4 KAI-NAN AN, 5 and RICHARD E. HUGHES 1, 2, 3 1 MedSport and Orthopaedic Research Laboratories, University of Michigan, Ann Arbor, MI; 2 Department of Biomedical Engineering, University of Michigan, Ann Arbor, MI; 3 Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI; 4 Department of Physical Therapy and Human Movement Sciences, Northwestern University, Evanston, IL; and 5 Orthopaedic Biomechanics Laboratory, Division of Orthopaedic Research, Mayo Clinic and Mayo Foundation, Rochester, MN (Received 12 April 2005; accepted 1 December 2005; published online: 11 February 2006) Abstract—The reigning paradigm of musculoskeletal modeling is to construct deterministic models from parameters of an “aver- age” subject and make predictions for muscle forces and joint torques with this model. This approach is limited because it does not perform well for outliers, and it does not model the effects of population parameter variability. The purpose of this study was to simulate variability in musculoskeletal parameters on glenohumeral external rotation strength in healthy normals, and in rotator cuff tear cases using a Monte Carlo model. The goal was to determine if variability in musculoskeletal parameters could quantifiably explain variability in glenohumeral external rotation strength. Multivariate Gamma distributions for muscu- loskeletal architecture and moment arm were constructed from empirical data. Gamma distributions of measured joint strength were constructed. Parameters were sampled from the distributions and input to the model to predict muscle forces and joint torques. The model predicted measured joint torques for healthy normals, subjects with supraspinatus tears, and subjects with infraspinatus– supraspinatus tears with small error. Muscle forces for the three conditions were predicted and compared. Variability in measured torques can be explained by differences in parameter variability. Keywords—Shoulder, Stochastic, Monte Carlo, Musculoskeletal model, Infraspinatus, Supraspinatus, Teres minor. INTRODUCTION Healthy normal subjects demonstrate remarkable vari- ability in maximum glenohumeral external rotation strength. For example, the standard deviation of external ro- tation strength can be 41% of the mean. 33 Additionally, with rotator cuff tear there is variability in the amount of strength deficit which appears to depend on factors other than cuff tear size. 12,13, 40,41,74 Current musculoskeletal model- ing paradigms have been unable to explain the variation in strength, or the strength deficit. Observations of mus- Address correspondence to Richard E. Hughes, PhD, MedSport, Uni- versity of Michigan, 24 Frank Lloyd Wright Drive, POB 391, Ann Arbor, MI 48106-0391. Electronic mail: [email protected]culoskeletal parameters also exhibit variability. 1,6 , 61,77 One might hypothesize that the variation in strength can be ex- plained via quantifiable differences in musculoskeletal pa- rameter variability, specifically physiologic cross-sectional areas (PCSA), moment arms and the muscle length–tension relationships. The historical approach to musculoskeletal modeling has been to construct deterministic models from param- eter means of a sample assumed to be representative of the general population. Deterministic models have been made for many joint systems including the hand, 17 elbow, 11,34, 54 shoulder, 28,76 spine, 18,26, 73 and lower extremity. 31,39, 49,69 Such models have been used with great success to predict joint torques and muscle forces for the “average” subject. However this approach does not reflect the inherent variabil- ity in musculoskeletal parameters which ultimately results in variability in muscle force and joint strength. Conse- quently, it is questionable how well these models predict muscle forces and joint torques across the population, in particular for subjects quite different than the sample mean. Monte Carlo methods are a means for modeling naturally occurring variability and uncertainty in a population. A few Monte Carlo models have been developed to model biome- chanical and musculoskeletal phenomena, 14,20, 32,55, 56,59, 75 but such work has been limited. Monte Carlo methods uti- lize input parameter distributions to model intersubject vari- ability, and therefore provide distributions of output values. Monte Carlo simulations are useful because the distribu- tion of muscle forces in a population can be predicted. Muscle–force distributions are necessary for understand- ing the mechanical and biological responses to external loads placed on the human body. The question of why some athletes or laborers develop pathologies like rota- tor cuff tendon tear while performing a task, while oth- ers executing the same task do not develop the pathology, has not been answered with deterministic models based on average parameter data. Subject specific models could 465 0090-6964/06/0300-0465/0 C 2006 Biomedical Engineering Society
A Probabilistic Model of Glenohumeral External Rotation Strengthfor Healthy Normals and Rotator Cuff Tear Cases
JOSEPH E. LANGENDERFER,1, 2 JAMES E. CARPENTER,1, 3 MARJORIE E. JOHNSON,4
KAI-NAN AN,5 and RICHARD E. HUGHES1, 2, 3
1MedSport and Orthopaedic Research Laboratories, University of Michigan, Ann Arbor, MI; 2Department of Biomedical Engineering,University of Michigan, Ann Arbor, MI; 3Department of Orthopaedic Surgery, University of Michigan, Ann Arbor, MI; 4Department ofPhysical Therapy and Human Movement Sciences, Northwestern University, Evanston, IL; and 5Orthopaedic Biomechanics Laboratory,
Division of Orthopaedic Research, Mayo Clinic and Mayo Foundation, Rochester, MN
(Received 12 April 2005; accepted 1 December 2005; published online: 11 February 2006)
Abstract—The reigning paradigm of musculoskeletal modelingis to construct deterministic models from parameters of an “aver-age” subject and make predictions for muscle forces and jointtorques with this model. This approach is limited because itdoes not perform well for outliers, and it does not model theeffects of population parameter variability. The purpose of thisstudy was to simulate variability in musculoskeletal parameterson glenohumeral external rotation strength in healthy normals,and in rotator cuff tear cases using a Monte Carlo model. Thegoal was to determine if variability in musculoskeletal parameterscould quantifiably explain variability in glenohumeral externalrotation strength. Multivariate Gamma distributions for muscu-loskeletal architecture and moment arm were constructed fromempirical data. Gamma distributions of measured joint strengthwere constructed. Parameters were sampled from the distributionsand input to the model to predict muscle forces and joint torques.The model predicted measured joint torques for healthy normals,subjects with supraspinatus tears, and subjects with infraspinatus–supraspinatus tears with small error. Muscle forces for the threeconditions were predicted and compared. Variability in measuredtorques can be explained by differences in parameter variability.
Keywords—Shoulder, Stochastic, Monte Carlo, Musculoskeletalmodel, Infraspinatus, Supraspinatus, Teres minor.
INTRODUCTION
Healthy normal subjects demonstrate remarkable vari-ability in maximum glenohumeral external rotationstrength. For example, the standard deviation of external ro-tation strength can be 41% of the mean.33 Additionally, withrotator cuff tear there is variability in the amount of strengthdeficit which appears to depend on factors other thancuff tear size.12,13,40,41,74 Current musculoskeletal model-ing paradigms have been unable to explain the variationin strength, or the strength deficit. Observations of mus-
Address correspondence to Richard E. Hughes, PhD, MedSport, Uni-versity of Michigan, 24 Frank Lloyd Wright Drive, POB 391, Ann Arbor,MI 48106-0391. Electronic mail: [email protected]
culoskeletal parameters also exhibit variability.1,6,61,77 Onemight hypothesize that the variation in strength can be ex-plained via quantifiable differences in musculoskeletal pa-rameter variability, specifically physiologic cross-sectionalareas (PCSA), moment arms and the muscle length–tensionrelationships.
The historical approach to musculoskeletal modelinghas been to construct deterministic models from param-eter means of a sample assumed to be representative of thegeneral population. Deterministic models have been madefor many joint systems including the hand,17 elbow,11,34,54
shoulder,28,76 spine,18,26,73 and lower extremity.31,39,49,69
Such models have been used with great success to predictjoint torques and muscle forces for the “average” subject.However this approach does not reflect the inherent variabil-ity in musculoskeletal parameters which ultimately resultsin variability in muscle force and joint strength. Conse-quently, it is questionable how well these models predictmuscle forces and joint torques across the population, inparticular for subjects quite different than the sample mean.
Monte Carlo methods are a means for modeling naturallyoccurring variability and uncertainty in a population. A fewMonte Carlo models have been developed to model biome-chanical and musculoskeletal phenomena,14,20,32,55,56,59,75
but such work has been limited. Monte Carlo methods uti-lize input parameter distributions to model intersubject vari-ability, and therefore provide distributions of output values.Monte Carlo simulations are useful because the distribu-tion of muscle forces in a population can be predicted.Muscle–force distributions are necessary for understand-ing the mechanical and biological responses to externalloads placed on the human body. The question of whysome athletes or laborers develop pathologies like rota-tor cuff tendon tear while performing a task, while oth-ers executing the same task do not develop the pathology,has not been answered with deterministic models basedon average parameter data. Subject specific models could
potentially answer these questions,3 but require large num-bers of subjects to understand the affects of variabilityacross the population. Such large studies are costly in termsof time and experimental involvement. Furthermore, an-other strength of Monte Carlo methods is that the limi-tations of traditional methods utilizing average values areavoided,75 and conclusions can be made concerning outputprobability.
The purpose of this study was to probabilistically sim-ulate the effects of variability in PCSAs, moment armsand the muscle length–tension relationships on predictedmuscle forces and joint torque. The aim was to developa model tuned to available data for glenohumeral externalrotation strength and, if the model predicts the torques withsmall errors, then there is potential for predicting and an-alyzing muscle force distributions in different populations.Additionally, simulations such as this may help describewhy some subjects retain strength in the presence of rotatorcuff tear, while other subjects do not maintain strength,and may help guide clinical management of cuff tearinjuries.
There were three objectives for this study: (1) to de-velop a stochastic model of isometric glenohumeral ex-ternal rotation; (2) to tune the model to predict isometricexternal rotation torques, and to compare predicted andmeasured torques; and (3) to estimate and compare ex-ternal rotation muscle force distributions for normal sub-
jects and for subjects with supraspinatus, and infraspinatus–supraspinatus rotator cuff tears.
METHODS
Variability in musculoskeletal parameters and their ef-fects on glenohumeral external rotation strength in healthynormals and in rotator cuff tear cases was simulated using aMonte Carlo model (Fig. 1). Multivariate Gamma distribu-tions were generated from summary statistics of empiricalmoment arm, PCSA, and the muscle length–tension depen-dencies (Fig. 1A). Gamma distributions for joint strengthwere constructed from external rotation joint strength alsomeasured in the laboratory (1B). Predicted muscle forceand joint strength relationships described in the text wereused to make predictions from parameters sampled from thedistributions (1C). Muscle specific tension was predictedfor the healthy normal case by sampling from the distribu-tions and using a least squares method to minimize the sumof squared errors between measured and predicted strength(1D). A nonparametric 95% confidence interval adjustmentof PCSA input distributions was used to ensure measuredand predicted torques matched for the two rotator cuff tearcases (1E). Muscle forces and joint strength distributionswere then predicted with the model for the healthy normalcase, for isolated supraspinatus tear, and for supraspinatuswith infraspinatus tear (1F).
Multivariate Gamma DistributionsMomentarm PCSAL-T
Ext. Rot.Strength
2
1000
)(∑ −TmeasuredTpredictMinTmeasured
TpredictStrength Model
∑=
×=8
1
)(j
jjP FrT
F = σσσσ CSA [ α FL]Fmuscle
Tpredict Healthy
SSP-INF Tear
σσσσ healthy
PCSA Adjustment95% C.I. for:
Tmeasured
Tpredict
TmeasuredTpredict
s
s
xx −
SSP Tear
, centers 0
, centers 1
(B)
(A)
(C)
(D)
(F)(E)
FIGURE 1. Diagram depicting the Monte Carlo model. (A) Multivariate Gamma distributions generated from summary statistics ofmoment arm, PCSA, and the muscle length–tension dependencies measured in our lab. (B) Gamma distributions for joint strengthconstructed from measured external rotation joint strength. (C) Predicted muscle force and joint strength relationships describedin the text. (D) Muscle specific tension predicted for the healthy normal case (and assumed for all cases) using the method of Changet al.14 (E) The nonparametric 95% confidence interval adjustment of PCSA input distributions to ensure measured and predictedtorques matched for the two rotator cuff tear cases. (F) Muscle force and joint torque distributions predicted with the model for thethree cases.
Probabilistic Model of Shoulder External Rotation Strength 467
Musculoskeletal Model
An isometric model of glenohumeral external rotationwas developed that simulates maximum isometric externalrotation strength for the position of 15◦ humeral abduc-tion at neutral glenohumeral rotation. This position waschosen because it is relevant for functional activities, iseasily testable and frequently tested in a clinical setting,and is a position for which isometric strength data is avail-able. Three agonist muscles are included: supraspinatus,infraspinatus and teres minor. Infraspinatus was representedwith four subregions, supraspinatus with three subregions,and teres minor as one subregion (Fig. 2). The isomet-ric force and torque-generating capacity of these mus-cles/subregions were described by the physiologic cross-sectional area, the length–tension relationships, and musclemoment arms from empirical data collected in our labora-tory.44–46
Glenohumeral external rotation joint torque (TP) waspredicted with a biomechanical model as the summation ofthe products of muscle moment arm (rj) and muscle force(Fj) at the joint angle position simulated in this study:
T p =8∑
j=1
(r j × Fj ) (1)
Muscle force was modeled as a function of the currentmuscle length, the level of neuromuscular activation (α),muscle physiologic cross-sectional area (PCSA), and mus-cle specific tension (σ ) [Fig. (1C)]. Eq. (2) represents the
FIGURE 2. Muscles simulated in this model. Individualmuscles/subregion paths are depicted as red segments;Supraspinatus: three subregions, infraspinatus: four subre-gions, teres minor: one region.
dependence of muscle force on these factors. Formulationsfrom the literature82 are used to model the dependency ofactive muscle force (FL) on muscle length.
F = σPCSA[α FL] (2)
The level of neuromuscular activation was fixed at unitysince strength measurements, described in the next sec-tion, were obtained at conditions of maximum voluntaryisometric contraction. Tendons were modeled as inelasticwhich is a reasonable assumption for an isometric model atone joint angle position. Incorporation of tendon stiffnessresults in maximum tendon strain of 3.3%,82 and 1.99–3.68%50 at maximum isometric muscle force. Chang et al.,199915 found the discrepancy in muscle strain to be lessthan 3% when tendon was modeled as elastic versus in-elastic. For the muscles modeled here which are operatingnear the peak of the length–tension curve (normalized forceapproximately 0.9) a nominal muscle strain discrepancy of3% introduces an error of less than 5% for muscle force.
Strength Data
Isometric external rotation strength data for healthy nor-mals,33 and for patients with rotator cuff tears (unpublisheddata) was collected in the laboratory. The data collected onrotator cuff tear patients was collected by the same authors(Biomechanics Laboratory, Mayo Clinic, Rochester, MN),under the same conditions as the healthy normal data. Alldata were collected with an institutional review board ap-proved protocol. In each study, strength was measured witha Cybex II isokinetic dynamometer (Cybex, Ronkonkoma,New York). During testing, the elbow was flexed to 90◦ andsecured with an Orthoplast splint (AliMed Inc., Dedham,Massachusetts) to allow measurement of isolated gleno-humeral strength. One-hundred and twenty subjects (60men and 60 women, mean 44, SD: 15 years) were testedfor the healthy normal case, and 46 subjects (34 men,12 women, mean: 59, SD: 11 years) were tested for thecuff tear cases. Of the 46 subjects with cuff tears, 41 tearswere full thickness tears, five tears were partial thickness.Isolated supraspinatus tears were present in 23 subjects, and23 subjects had combined supraspinatus and infraspinatustears established via intraoperative observation.
Monte Carlo Simulation
Variability in musculoskeletal architecture and musclemoment arm were modeled as random variates with a MonteCarlo method (Fig. 1). Summary statistics of empirical datacollected in our lab44–46 were used to construct multivariateGamma probability distributions. Muscles and tendons ofsupraspinatus and infraspinatus were subdivided into threeand four equal width regions respectively. Excursions ofthese tendon subregions and teres minor were measured forfull ranges of rotation on 10 independent glenohumeral ca-daver specimens with the humerus abducted in the scapular
468 LANGENDERFER et al.
plane at the position simulated with this model. Momentarms were determined from tendon excursion via the prin-ciple of virtual work.2 On the same 10 specimens, mus-cle fascicle lengths, sarcomere lengths, pennation angles,and muscle volumes were measured. From these param-eter measurements and tendon excursions, optimal fasci-cle length, physiological cross-sectional area (PCSA), andmuscle length–tension dependence were calculated. Sum-mary statistics of these parameters are reported in Table 1(healthy normal case).
Because natural correlation exists among PCSA, themuscle length–tension relationship and muscle momentarms, parameter covariance was established by calculatingcovariance matrices of PCSA, normalized muscle force,and muscle moment arm. Frequently, the calculated covari-ance matrix was nonpositive definite. With small samplesize, sample covariance may be nonpositive definite dueto mere sampling fluctuation. An additional more likelycause of nonpositive definiteness is colinearities betweenvectors of the data from which the covariance is calculated.The colinearities result in a covariance matrix which lacksinformation, is mathematically rank deficient, and cannotbe inverted. Nonpositive definite covariance matrices weremade positive definite by smoothing. Ridge smoothing wasaccomplished by adding 10% to the diagonal terms.80 Mul-tivariate parameter distributions were generated with thepositive definite covariance matrix [Fig. (1A)].22,37,58 Thecovariance of the resulting multivariate distributions wereasymptotic to empirically determined covariance with sam-ple size. At small sample size, covariance of the model gen-erated distribution did not match empirical covariance, butas sample size approached infinity, the empirical covariancewas attained. At sample size of 1000, modeled and empir-ical covariances were identical and any additional samplesdid not increase agreement. Mean and variance of the gener-
ated distributions exactly matched summary statistics of theempirical data. Equivalency of the generated distributionsand the empirical data were assessed with Komolgorov–Smirnov goodness-of-fit tests and were always equivalent(p > 0.05).
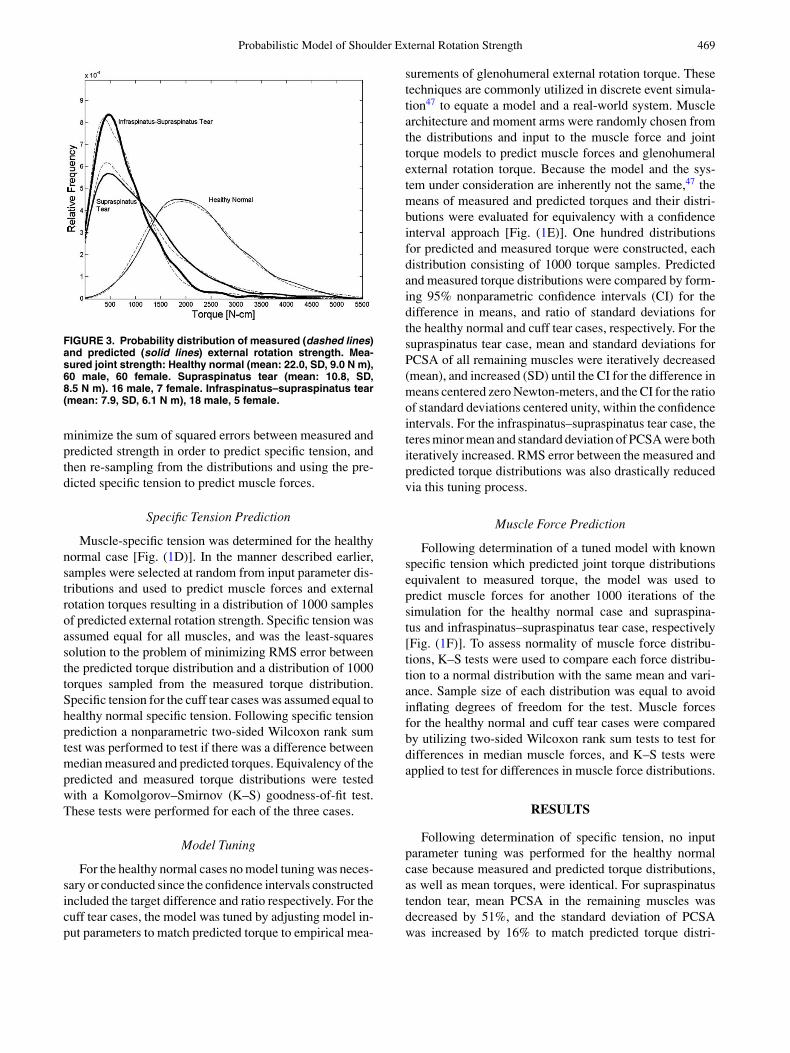
Since glenohumeral external rotation strength also ex-hibits variability among subjects, measured torque was alsomodeled as a random variate. Gamma probability distribu-tions were constructed from summary statistics for strengthfrom sources described earlier [Fig. (1B)]. Gamma distri-butions were chosen because, while exact distributions areunknown, PCSA, moment arm, normalized muscle force,and glenohumeral external rotation strength are all non-negative. Two rotator cuff tear cases were simulated in thisstudy; supraspinatus tendon tear, and infraspinatus withsupraspinatus tendon tear. The mean strength losses were51 and 64% for the two cases, respectively (Fig. 3). Cufftears were mathematically induced by setting PCSA forthe involved muscles equal to zero. The mean and varianceof constructed gamma strength distributions matched themean and variance of measured strengths (Fig. 3), andKomolgorov–Smirnov goodness-of-fit tests failed to de-tect differences between measured strength data and con-structed strength distributions (p > 0.05).
A random number generator chose samples from thedistributions for musculoskeletal parameters and measuredtorques. All simulations and data analysis were performedwith the statistics toolbox in Matlab 6.5 (Mathworks,Natick, MA). The simulation was conducted for the healthynormal case and the cuff tear cases. This modeling andsimulation was conducted in three phases: model tuning,muscle specific tension prediction, and muscle force pre-diction. Specific tension and muscle forces were predictedin the manner of Chang et al.14 [Fig. (1D)], by first samplingfrom the distributions and using a least-squares method to
TABLE 1. Musculoskeletal input parameters (mean and SD).
Note. Parameters for the healthy normal case were measured in our laboratory from 10 cadaver specimens. Moment armsand normalized muscle force (from calculated muscle length–tension relationships) were for the position simulated withthis model. Covariance between moment arm, PCSA and normalized force was determined and used to model multivariategamma input distributions formed from the mean and standard deviation of measured parameters. PCSA for the tearcases are the values for which the model was tuned to make measured and predicted torque distributions equivalent(p > 0.05).
Probabilistic Model of Shoulder External Rotation Strength 469
FIGURE 3. Probability distribution of measured (dashed lines)and predicted (solid lines) external rotation strength. Mea-sured joint strength: Healthy normal (mean: 22.0, SD, 9.0 N m),60 male, 60 female. Supraspinatus tear (mean: 10.8, SD,8.5 N m). 16 male, 7 female. Infraspinatus–supraspinatus tear(mean: 7.9, SD, 6.1 N m), 18 male, 5 female.
minimize the sum of squared errors between measured andpredicted strength in order to predict specific tension, andthen re-sampling from the distributions and using the pre-dicted specific tension to predict muscle forces.
Specific Tension Prediction
Muscle-specific tension was determined for the healthynormal case [Fig. (1D)]. In the manner described earlier,samples were selected at random from input parameter dis-tributions and used to predict muscle forces and externalrotation torques resulting in a distribution of 1000 samplesof predicted external rotation strength. Specific tension wasassumed equal for all muscles, and was the least-squaressolution to the problem of minimizing RMS error betweenthe predicted torque distribution and a distribution of 1000torques sampled from the measured torque distribution.Specific tension for the cuff tear cases was assumed equal tohealthy normal specific tension. Following specific tensionprediction a nonparametric two-sided Wilcoxon rank sumtest was performed to test if there was a difference betweenmedian measured and predicted torques. Equivalency of thepredicted and measured torque distributions were testedwith a Komolgorov–Smirnov (K–S) goodness-of-fit test.These tests were performed for each of the three cases.
Model Tuning
For the healthy normal cases no model tuning was neces-sary or conducted since the confidence intervals constructedincluded the target difference and ratio respectively. For thecuff tear cases, the model was tuned by adjusting model in-put parameters to match predicted torque to empirical mea-
surements of glenohumeral external rotation torque. Thesetechniques are commonly utilized in discrete event simula-tion47 to equate a model and a real-world system. Musclearchitecture and moment arms were randomly chosen fromthe distributions and input to the muscle force and jointtorque models to predict muscle forces and glenohumeralexternal rotation torque. Because the model and the sys-tem under consideration are inherently not the same,47 themeans of measured and predicted torques and their distri-butions were evaluated for equivalency with a confidenceinterval approach [Fig. (1E)]. One hundred distributionsfor predicted and measured torque were constructed, eachdistribution consisting of 1000 torque samples. Predictedand measured torque distributions were compared by form-ing 95% nonparametric confidence intervals (CI) for thedifference in means, and ratio of standard deviations forthe healthy normal and cuff tear cases, respectively. For thesupraspinatus tear case, mean and standard deviations forPCSA of all remaining muscles were iteratively decreased(mean), and increased (SD) until the CI for the difference inmeans centered zero Newton-meters, and the CI for the ratioof standard deviations centered unity, within the confidenceintervals. For the infraspinatus–supraspinatus tear case, theteres minor mean and standard deviation of PCSA were bothiteratively increased. RMS error between the measured andpredicted torque distributions was also drastically reducedvia this tuning process.
Muscle Force Prediction
Following determination of a tuned model with knownspecific tension which predicted joint torque distributionsequivalent to measured torque, the model was used topredict muscle forces for another 1000 iterations of thesimulation for the healthy normal case and supraspina-tus and infraspinatus–supraspinatus tear case, respectively[Fig. (1F)]. To assess normality of muscle force distribu-tions, K–S tests were used to compare each force distribu-tion to a normal distribution with the same mean and vari-ance. Sample size of each distribution was equal to avoidinflating degrees of freedom for the test. Muscle forcesfor the healthy normal and cuff tear cases were comparedby utilizing two-sided Wilcoxon rank sum tests to test fordifferences in median muscle forces, and K–S tests wereapplied to test for differences in muscle force distributions.
RESULTS
Following determination of specific tension, no inputparameter tuning was performed for the healthy normalcase because measured and predicted torque distributions,as well as mean torques, were identical. For supraspinatustendon tear, mean PCSA in the remaining muscles wasdecreased by 51%, and the standard deviation of PCSAwas increased by 16% to match predicted torque distri-
470 LANGENDERFER et al.
bution to the measured distribution. With infraspinatus–supraspinatus tendon tear, mean PCSA of the remainingmuscle, teres minor, was increased 93%, and the standarddeviation of teres minor PCSA was increased by a fac-tor of 3 in order to predict the measured external rotationdistributions (Table 1). For the healthy normal case sum-mary statistics for moment arms and the normalized forcefrom the length–tension relationship (Table 1) were equal tomeasurements made in our lab. Confidence interval widthsfor the difference in mean measured and predicted torqueswere 0.12, 0.09, and 0.09 N m wide for the healthy normal,supraspinatus, and infraspinatus–supraspinatus tear casesrespectively. The confidence interval widths for the ratioof measured and predicted standard deviations were 0.13,0.15, and 0.17 wide, respectively.
Muscle specific tension for the healthy normal case de-termined with the least squares approach was 1.43 MPa,and was assumed for the cuff tear cases. Equivalent dis-tributions for predicted and measured torques were de-termined with RMS error of 0.10 N m (Fig. 3) for thehealthy normal and cuff tear cases. The Wilcoxon rank sumtests indicated that median predicted and measured torqueswere not significantly different for the healthy normal(p = 0.5), supraspinatus tear (p = 0.8), and infraspinatus–
supraspinatus tear (p = 0.7) cases. Furthermore, dis-tributions of predicted and measured joint torque werenot significantly different for the healthy normal (p =0.8), supraspinatus tear (p = 0.7), and infraspinatus–supraspinatus tear (p = 0.4) cases.
With supraspinatus tear, muscle forces in all regions ofinfraspinatus and teres minor were reduced as compared tothe healthy normal cases (Fig. 4). For the infraspinatus–supraspinatus tear case, teres minor force was elevatedcompared to healthy normal. Muscle forces for the healthynormal case were normally distributed (p > 0.05), exceptfor posterior supraspinatus (p = 0.02). Conversely, forcedistributions for both cuff tear cases were not normallydistributed (p < 0.001). Muscle force distributions weresignificantly different (p < 0.001) between the healthy nor-mal and rotator cuff tear cases (Fig. 4). Median forcesfor all muscles were significantly different (p < 0.001)between the healthy normal and rotator cuff tear cases(Table 2).
Probabilities that muscle forces for the supraspinatustear case were less than the median muscle forces for thehealthy normal case are 0.88, 0.86, 0.83, 0.88, and 0.88for superior infraspinatus, superior middle infraspinatus,inferior middle infraspinatus, inferior infraspinatus
FIGURE 4. Probability distribution of muscle forces for the healthy normal, supraspinatus tendon tear, and infraspinatus–supraspinatus tendon tear cases.
Probabilistic Model of Shoulder External Rotation Strength 471
and teres minor, respectively. For the infraspinatus–supraspinatus tear case, the probability that teres minorforce is greater than the median healthy normal teres minorforce, (271.8 N) is 0.79 (Fig. 5).
DISCUSSION
In this study a probabilistic model was used to pre-dict measured torque distributions with small error. For thehealthy normal case predicted torque distributions matchedmeasured distributions of torque with no tuning of inputparameters aside from determination of specific tension.The strong agreement between measured and predictedtorque distributions illustrates how variability of muscle ar-chitecture and moment arm can explain variability in gleno-humeral external rotation strength as measured in healthynormal subjects. This result demonstrates strong potential
FIGURE 5. The probability that teres minor muscle force forthe infraspinatus–supraspinatus tear case exceeds the medianforce for the healthy normal case is 0.79, and is depicted graph-ically as the area under the probability distribution greater than271.8 N.
for utilizing probabilistic musculoskeletal models to predictmuscle forces for two different populations.
For rotator cuff tears, the model was tuned by adjustingthe distributions for muscle physiologic cross-sectional areain order to predict torque distributions with small error. Forthe supraspinatus tear case the PCSA was reduced by anaverage of 51%. Such a decrease in PCSA explains reducedability of the infraspinatus and teres minor to generate force.Reduced muscle force capacity of these muscles of coursetranslates to reduced external rotation strength and a disrup-tion of the force balance necessary for maintaining staticequilibrium of the humeral head relative to the glenoid. Forthe infraspinatus–supraspinatus tear case mean PCSA wasincreased by 93%. The increase in teres minor PCSA re-sults in increased force required for generation of measuredexternal rotation strength. Looking at the distributions ofpredicted muscle forces one can see that with infraspinatustendon tear, the median muscle force in the remaining mus-cles is reduced compared to healthy normals. Additionally,the model in this study allows for the calculation of theprobabilities that muscle forces for tear cases are differentthan muscle forces for healthy normals. The model pre-dicts high probability that infraspinatus forces are reducedcompared to healthy normals in the case of supraspinatustendon tear. Likewise, for the infraspinatus-supraspinatustear case the model predicts high probability of greaterteres minor muscle force as compared to the healthy normalforce. Results or insights such as these are previously un-elucidated utilizing deterministic models based on averageor subject specific parameters, and highlight some strengthsof stochastic modeling.
The parameter variability found via the tuning processis not known to be exact, but presents intriguing questionsgiven the probabilistic nature of measured parameters. Inthe future it would be interesting to measure these, andother parameters, in healthy normal subjects and subjectswith pathological conditions in order to better understandparameter variance. Measurement of parameters for esti-mating muscle force and torque generating capacity, par-ticularly the muscle length–tension relationship, has pri-marily occurred in cadaveric models.51,61 However, in vivomethods have recently been developed which approach the
472 LANGENDERFER et al.
ability to measure the parameters for representing relation-ships modeled here.5,67 This study is the first to quantify theeffects of muscle architecture and moment arm variabilityon muscle strength. With advances in imaging techniquesit might one day be possible to measure these parametersin vivo. The methodology utilized here can quantify theeffects of parameter variability when such data becomesavailable. Additionally, it would be interesting to simulatealterations in other parameters such as moment arm andmuscle length–tension relationships in a manner similarto how muscle hypertrophy/atrophy was simulated here.However, in this model we did not simulate these parame-ter changes with cuff tear because there is not experimen-tal or clinical evidence for these alterations at the presenttime.
The result of this study that muscle PCSA for thesupraspinatus tear case was reduced agrees with clinicalfindings following cuff tear with degradation of rotator cuffmuscles due to muscle atrophy via fatty infiltration.57,63,72
Of course, some period of time is necessary followinginjury for the atrophy to appear. Clinically, infraspinatusdegradation can occur in supraspinatus tendon tear caseseven if the infraspinatus tendon is intact.25 This modelsupports clinical observations. Additionally, the reductionin infraspinatus PCSA and force is suggestive of reducedability of infraspinatus to generate inferiorly directed forcenecessary to resist superior humeral head superior trans-lation and impingement with the acromion in the case ofsupraspinatus tendon tear.71
For the infraspinatus–supraspinatus tear case, the dataare more limited. However, the model developed heresupports clinical observations in some patients withsupraspinatus and infraspinatus tendon tear. Hypertrophyof teres minor allows for retention of some external rota-tion strength in patients with the dual tear case, and hasbeen linked to patients who are able to function in the pres-ence of dual cuff tear.78 Biomechanically, in healthy normalsubjects, teres minor contributes about 50% to external ro-tation strength.19 Hypertrophy of teres minor might allowpatients to present relatively normal or minimal reduction inexternal rotation strength with infraspinatus–supraspinatustendon tear as was modeled here.
A strength of this model is the consideration of correla-tions among muscle architecture and moment arm. In thissimulation correlation between PCSA, moment arms, andthe muscle length–tension relationship was incorporatedby utilizing multivariate distributions to model these pa-rameters. Use of multivariate distributions requires originalempirical data for calculation of covariance, or access todetermined parameter covariance. During the model de-velopment phase a univariate model, in which covarianceamong input parameters was ignored, was constructed andused to make predictions for the healthy normal case. Theunivariate model predicted a joint torque distribution withstandard deviation of one-half the measured torque stan-
dard deviation, but with identical means for predicted andmeasured torques. From this result it can be concluded thatcovariance is important for realistically modeling input pa-rameters in order to build a valid model which predictstorque distributions matched to measured distributions forthe real-world system. This finding is in agreement withothers who found that multivariate distributions containimportant information, and therefore perform better thanunivariate input distributions when attempting to predictdistributions of muscle forces and joint torques.32,58 Mea-surements of muscle architecture and moment arms in vivoand in cadavera have begun to address issues of parametercovariance.30,62,79
Several limitations exist in this study. We assumed thatall contractions were conducted under conditions of 100%muscle activation. It is possible there exists some variabilityin muscle activation even under conditions of maximum ex-ertion. Incorporation of an EMG-Activation model wouldbe a reasonable improvement given limited availability ofEMG data.70 However deterministic musculoskeletal mod-els commonly assume 100% muscle activation when EMGdata were not recorded.38,64,76 For our isometric stochasticmodel, the order of magnitude of errors associated withthis assumption is comparable. An additional limitation ofthis simulation is that we did not model the effect of age, orcontrol for the effect of gender on external rotation strength.Each of these variables could be controlled for using a nor-malization procedure, or by incorporating age and genderas multivariate model input parameters. Future models willrequire larger datasets to ensure the multivariate nature ofthese parameters can be effectively modeled. We did notinclude the effect of cocontraction of the subscapularis orother antagonist muscles. Incorporation of these muscleswould allow loading across the joint to be determined.
According to other sources, posterior deltoid accountsfor about 11% of the external rotation torque in the posi-tion simulated here.43 However, posterior deltoid was notincluded in this model for several reasons. First, we do nothave confidence in that data because there are no standarddeviations reported. Additionally, our method for measur-ing muscle moment arms differed from the methods ofKuechle et al. in a significant respect. In the other study,muscles remained attached to the specimens and cords wererouted along the surface of the muscle bellies. Cord pathswere further from the joint center of rotation than phys-iologic muscle and tendon centroids. Consequently, mo-ment arms were overpredicted since a longer cord pathresults in a greater excursion for a given rotation angle.In our study, we dissected muscles from the specimensand approximated the muscle-tendon paths with custommade low friction nylon guides to route the cords.46 Thistechnique is a better model since the cord path is morealigned with muscle and tendon centroids. In an early pi-lot test specimen we measured the moment arm of posterdeltoid in one specimen for three trials and concluded that
Probabilistic Model of Shoulder External Rotation Strength 473
posterior deltoid does not play a significant role in rota-tion strength for the position simulated here since momentarm is less than 10% of moment arm for infraspinatus,and posterior deltoid PCSA is equal to infraspinatus. Ourresults, agree with conclusions made by others66 that pos-terior deltoid does not play a significant role in externalrotation.
It is important to note that this model does not considerthat residual force generated in a cuff muscle tendon rupturemight contribute to joint strength via lateral force transmis-sion through an adjacent muscle or tendon. This simulationneglects these types of forces. Experimental models havedemonstrated lateral force transmission between adjacentmuscles.4,7,21,35,48,52 While the tools for modeling lateralforces in muscle exist,81 the changes in the muscle momentarm with cuff tear, and the analytical tools for modeling thechange, are not well understood.
Additionally, there is evidence that with rotator cuff tearmuscle activation could be altered due to pain or other fac-tors not completely understood. Recently, a trend has beenfound towards increased muscle activation in asymptomaticand symptomatic rotator cuff tear patients compared tohealthy controls.40 This model neglects such alterations inmuscle activation.
The muscle specific tension determined in this simula-tion, 1.43 MPa, is at the upper bound of values described inthe literature.8,16,23,36,65,68,76 Specific tension, like muscleactivation could be modeled as a random variable. How-ever, in this study it was decided to model specific tensiondeterministically, with the assumption that the probabilis-tic aspects of the parameter would be captured by model-ing PCSA stochastically. With a limited understanding ofspecific tension differences among healthy normals,9 it isreasonable to model specific tension as equal for all cases.Specific tension was determined for the healthy normal caseusing a common, simple mechanical model to ensure pre-dicted joint torques match externally measured joint torqueswith small errors.9,14,15,27,54 With reduced specific tension,and consequently reduced muscle forces, the model wouldnot have predicted measured joint torques with small error.However, others have found the same relative value forspecific tension of elbow and shoulder muscles determinedwith similar modeling approaches,9,10 including a recent-deterministic model which utilized 1.4 MPa for specifictension in order to match predicted moments to measuredvalues.29
The muscle forces predicted here have not yet been val-idated by direct measurement, or predicted by models us-ing kinematic and muscle activation data collected in vivoas inputs. Current models of the glenohumeral joint havebeen used to make muscle force predictions for other mo-tions.28,53,76 In the future it would be interesting to conductan experiment to obtain in vivo data for estimating muscleforces during external rotation as has been done for otherjoints and other motions.
Input parameters are not, most likely, Gamma dis-tributed. However, owing to small sample size for the inputparameters in particular, we found it necessary to assumeGamma distributions for these parameters. Gamma distri-butions result in generation of non-negative random vari-ates, which is favorable since PCSA, agonist moment arms,and normalized muscle force are all non-negative. Ideally,in the future it is possible that a larger data set will allowfor an easing of this assumption allowing parameters to bemodeled non-parametrically. By utilizing a Gamma distri-bution of 1000 samples more information is added to thesimulation concerning the input distribution than is actu-ally known. In fact, when distribution sample size exceedssample size of the empirical data, degrees of freedom areartificially inflated, and assumed distributions become lessrealistic.
Another method for simulating relationships betweeninput parameters and their effect on model output is a boot-strap model.24,60 Bootstrap models are attractive becausethe system under consideration is modeled directly fromempirical data in a nonparametric fashion. During the modeldevelopment phase of this study a bootstrap model was con-structed in which input parameters were sampled at randomwith replacement from the original empirical data describ-ing muscle PCSA’s, moment arms and normalized forcefrom length–tension relationships. In this manner covari-ance was modeled directly since parameters were sampledas vectors corresponding to each specimen from which datawas collected. Means and distributions of predicted torquesmatched measured torque means and distributions for thehealthy normal case determined by the confidence levelapproach described earlier. This result demonstrates strongpotential for multivariate probabilistic models.
More work is needed to determine how to utilize proba-bilitistic models to analyze differences in populations. Forexample, a random component exists to physical perfor-mance of labor and athletic tasks. If different people per-form the same task many times, task performance will differboth within a subject, and between subjects. Additionally,it is possible that combinations of outlying parameters withlow probabilities of occurrence within a population (shortmoment arm, large PCSA) may lead to pathological condi-tions such as rotator cuff tear. Furthermore, there is increas-ing evidence that mechanics of force generation at the sar-comere level is probabilistic,42 rather than deterministic aspreviously thought. Yet, little is understood concerning howthe probabilistic nature of these properties might contributeto pathologies such as rotator cuff tear. Additionally, morework is needed to understand how models can explain thelinks between the degree of randomness and the likelihoodof pathological condition.
In conclusion, in this study we incorporated the ef-fects of population variability into a musculoskeletal modelof glenohumeral external rotation strength. Muscle forceswere predicted with the model. Forces for healthy normal
474 LANGENDERFER et al.
subjects and two rotator cuff tear cases were compared.Differences in variability of measured torques for the threecases analyzed here are explained by differences in meansand distributions of muscle cross-sectional area. This studyfurthers our understanding of effects of parameter variabil-ity on variability in muscle force and shoulder externalrotation strength. The stochastic method accounts for dif-ferences in musculoskeletal parameters across a populationand has potential for modeling other joint systems, andfor increasing our understanding of differences betweenpopulations.
ACKNOWLEDGMENTS
We thank the reviewers for many constructive commentswhich added to the quality of this paper. This study wassupported by grants from the Whitaker Foundation and theNational Institutes of Health (AR048540, AR41171 andHD07447).
REFERENCES
1An, K. N., F. C. Hui, B. F. Morrey, R. L. Linscheid, and E. Y.Chao. Muscles across the elbow joint: A biomechanical analysis.J. Biomech. 14:659–669, 1981.
2An, K. N., K. Takahashi, T. P. Harrigan, and E. Y. Chao. Deter-mination of muscle orientations and moment arms. J. Biomech.Eng. 106:280–282, 1984.
3Arnold, A. S., S. S. Blemker, and S. Delp. Evaluation of a de-formable musculoskeletal model for estimating muscle-tendonlengths during crouch gait. Ann. Biomed. Eng. 29:263–274,2001.
4Asakawa, D. S., S. S. Blemker, G. E. Gold, and S. Delp.In vivo motion of the rectus femoris muscle after tendon transfersurgery. J. Biomech. 35:1029–1037, 2002.
5Asakawa, D. S., G. P. Pappas, S. S. Blemker, J. E. Drace, andS. L. Delp. Cine phase-contrast magnetic resonance imagingas a tool for quantification of skeletal muscle motion. Semin.Musculoskeletal Radiol. 7:287–295, 2003.
6Bassett, R. W., A. O. Browne, B. F. Morrey, and K. N. An.Glenohumeral muscle force and moment mechanics in a positionof shoulder instability. J. Biomech. 23:405–415, 1990.
7Bloch, R. J., and H. Gonzalez-Serratos. Lateral force transmis-sion across costameres in skeletal muscle. Exercise Sport Sci.Rev. 31:73–78, 2003.
8Brand, P. W., R. B. Beach, and D. E. Thompson. Relative tensionand potential excursion of muscles in the forearm and hand. J.Hand Surg. 6:209–219, 1981.
9Buchanan, T. S. Evidence that maximum muscle stress is nota constant: Differences in specific tension in elbow flexors andextensors. Med. Eng. Phy. 17:529–536, 1995.
10Buchanan, T. S., S. L. Delp, and J. A. Solbeck. Muscular resis-tance to varus and valgus loads at the elbow. J. Biomech. Eng.120:634–639, 1998.
11Buchanan, T. S., K. Manal, X. Shen, D. G. Lloyd, and R. V.Gonzalez. The virtual arm: Estimating joint moments using anEMG-driven model. In 12th Conference of the European Societyof Biomechanics. 2000, Dublin, Ireland.
12Burkhart, S. S. Arthroscopic treatment of massive rotator cufftears: Clinical results and biomechanical rationale. Clin. Or-thopaed. Relat. Res. 267:45–56, 1991.
13Burkhart, S. S., W. M. Nottage, D. J. Ogilvie-Harris, H. S. Kohn,and A. Pachelli. Partial repair of irreparable rotator cuff tears.Arthrosc.: J. Arthrosc. Relat. Surg. 10:363–370, 1994.
14Chang, Y.-W., R. E. Hughes, F.-C. Su, E. Itoi, and K.-N. An. Prediction of muscle force involved in shoul-der internal rotation. J. Shoulder Elbow Surg. 9:188–195,2000.
15Chang, Y. W., F. C. Su, H. W. Wu, and K. N. An. Optimum lengthof muscle contraction. Clin. Biomech. 14:537–542, 1999.
16Chao, E. Y., and K. N. An. Graphical interpretation of the so-lution to the redundant problem in biomechanics. J. Biomech.Eng. 100:159–167, 1978.
17Chao, E. Y., J. D. Opgrande, and F. E. Axmear. Three-dimensional force analysis of finger joints in selected isometrichand functions. J. Biomech. 9:387–396, 1976.
18Cholewicki, J., S. M. McGill, and R. W. Norman. Comparisonof muscle forces and joint load from an optimization and EMGassisted lumbar spine model: Towards development of a hybridapproach. J. Biomech. 28:321–331, 1995.
19Colachis, S. C., and B. R. Strohm. Effect of suprascapular andaxillary nerve blocks on muscle force in upper extremity. Arch.Phys. Med. Rehab. 52:22–29, 1971.
20Davidson, P. L., D. J. Chalmers, and B. D. Wilson. Stochastic-rheological simulation of free-fall arm impact in children: Appli-cation to playground injuries. Comp. Methods Biomech. Biomed.Eng. 7:63–71, 2004.
21Delp, S. L., D. A. Ringwelski, and N. C. Carroll. Transfer of therectus femoris: Effects of transfer site on moment arms aboutthe knee and hip. J. Biomech. 27:1201–1211, 1994.
22Devroye, S. Non-Uniform Random Variate Generation. NewYork: Springer Verlag, 1986.
23Edgerton, V. R., P. Apor, and R. R. Roy. Specific tension ofhuman elbow flexor muscles. Acta Physiol. Hung. 75:205–216,1990.
24Efron, B. Bootstrap Methods: Another Look at the Jackknife.Stanford University Press: Stanford, CA, 1977, pp. 1–37.
25Goutallier, D., J. M. Postel, J. Bernageau, L. Lavau, and M.C. Voisin. Fatty muscle degeneration in cuff ruptures. Pre- andpostoperative evaluation by ct scan. Clin. Orthopaed. Relat. Res.304:78–83, 1994.
26Granata, K. P., and W. S. Marras. An emg-assisted model of trunkloading during free-dynamic lifting. J. Biomech. 29:1309–1317,1995.
27Hatze, H. Estimation of myodynamic parameter values fromobservations on isometrically contracting muscle groups. Eur. J.Appl. Physiol. 46:325–338, 1981.
28Hogfors, C., D. Karlsson, and B. Peterson. Structure and inter-nal consistency of a shoulder model. J. Biomech. 28:767–777,1995.
29Holzbaur, K. R., W. M. Murray, and S. L. Delp. A model ofthe upper extremity for simulating musculoskeletal surgery andanalyzing neuromuscular control. Ann. Biomed. Eng. 33:829–840, 2005.
30Holzbaur, K., W. Murray, G. Gold, and S. Delp. Scaling ofmuscle volumes in the upper extremity. in XXth Congress of theInternational Society of Biomechanics and 29th Annual Meetingof the American Society of Biomechanics. 2005, Cleveland,Ohio.
31Hoy, M. G., F. E. Zajac, and M. E. Gordon. A musculoskeletalmodel of the human lower extremity: The effect of muscle,tendon, and moment arm on the moment-angle relationship ofmusculotendon actuators at the hip, knee, and ankle. J. Biomech.23:157–169, 1990.
32Hughes, R. E., and K.-N. An. Monte carlo simulation of a planarshoulder model. Med. Biol. Eng. Comp. 35:544–548, 1997.
Probabilistic Model of Shoulder External Rotation Strength 475
33Hughes, R. E., M. E. Johnson, S. W. O’Driscoll, and K.-N. An.Age-related changes in normal isometric shoulder strength. Am.J. Sports Med. 27:651–657, 1999.
34Hughes, R. E., A. G. Schneeberger, K.-N. An, B. F. Morrey,and S. W. O’Driscoll. Reduction of triceps muscle force aftershortening of the distal humerus: A computational model. J.Shoulder Elbow Surg. 6:444–448, 1997.
35Huijing, P. A. Muscle as a collagen fiber reinforced composite:A review of force transmission in muscle and whole limb.J. Biomech. 32:329–345, 1999.
36Ikai, M., and T. Fukunaga. Calculation of muscle strength perunit cross-sectional area of human muscle by means of ultrasonicmeasurement. Int. Z. Angew. Physiol. 26:26–32, 1968.
37Johnson, M. Multivariate Statistical Simulation. New York:Wiley, 1987.
38Karlsson, D., and B. Peterson. Towards a model for force pre-dictions in the human shoulder. J. Biomech. 25:189–199, 1992.
39Kaufman, K. R. A mathematical model of muscle and jointforces in the knee during isokinetic exercise. PhD Thesis, 1988,North Dakota State University.
40Kelly, B. T., R. J. Williams, F. A. Cordasco, S. I. Backus, J.C. Otis, D. E. Weiland, D. W. Altchek, E. V. Craig, T. L.Wickiewicz, and R. F. Warren. Differential patterns of mus-cle activation in patients with symptomatic and asymptomaticrotator cuff tears. J. Shoulder Elbow Surg. 14:165–171, 2005.
41Kirschenbaum, D., J. Coyle, P. Michael, J. P. Leddy, P. Katsaros,J. Tan, Fernando, and R. P. Cody. Shoulder strength with rotatorcuff tears: Pre- and postoperative analysis. Clin. Orthopaed.Relat. Res. 288:174–178, 1993.
42Kitamura, K., and T. Yanagida. Stochastic properties of acto-myosin motor. BioSystems 71:101–110, 2003.
43Kuechle, D. K., S. R. Newman, E. Itoi, G. L. Niebur, B. F.Morrey, and K.-N. An. The relevance of the moment arm ofshoulder muscles with respect to axial rotation of the gleno-humeral joint in four positions. Clin. Biomech. 15:322–329,2000.
44Langenderfer, J. E. A probabilistic approach to explain vari-ability in glenohumeral external rotation strength for healthynormals and patients with rotator cuff tear. 2005, PhD Thesis,The University of Michigan.
45Langenderfer, J. E., C. Patthanacharoenphon, R. E. Hughes,and J. E. Carpenter. Variability in isometric force and torquegenerating capacity of glenohumeral external rotator muscles.in Proceedings, XXth Congress of the International Society ofBiomechanics and 29th Annual Meeting of the American Soci-ety of Biomechanics. 2005, Cleveland, Ohio.
46Langenderfer, J. E., C. Patthanacharoenphon, R. E. Hughes,and J. E. Carpenter. Variability of glenohumeral external rotatormuscle moment arms. In Proceedings, XXth Congress of theInternational Society of Biomechanics and 29th Annual Meetingof the American Society of Biomechanics. 2005, Cleveland,Ohio.
47Law, A. M., and W. D. Kelton. Simulation, Modeling and Anal-ysis. New York: McGraw-Hill, 2000.
48Lieber, R. L., and J. Friden. Clinical significance of skeletalmuscle architecture. Clin. Orthopaed. Relat. Res. 383:140–151,2001.
49Lloyd, D. G., and T. F. Besier. An EMG-driven musculoskeletalmodel to estimate muscle forces and knee joint moments in vivo.J. Biomech. 36:765–776, 2003.
50Loren, G. J., and R. L. Lieber. Tendon biomechanical proper-ties enhance human wrist muscle specialization. J. Biomech.28:791–799, 1995.
51Loren, G. J., S. D. Shoemaker, T. J. Burkholder, M. D. Jacobson,J. Friden, and R. L. Lieber. Human wrist motors: Biomechanical
design and application to tendon transfers. J. Biomech. 29:331–342, 1996.
52Maas, H., G. C. Baan, and P. A. Huijing. Intermuscular interac-tion via myofascial force transmission: Effects of tibialis anteriorand extensor hallucis longus length on force transmission fromrat extensor digitorum longus muscle. J. Biomech. 34:927–940,2001.
53Makhsous, M., C. Hogfors, A. Siemienski, and B. Peterson.Total shoulder and relative muscle strength in the scapular plane.J. Biomech. 32:1213–1220, 1999.
54Manal, K., R. V. Gonzalez, D. G. Lloyd, and T. S. Buchanan. Areal-time emg-driven virtual arm. Comp. Biol. Med. 32:25–36,2002.
55McLean, S. G., X. Huang, A. Su, and A. J. van den Bogert. Sagit-tal plane biomechanics cannot injure the ACL during sidestepcutting. Clin. Biomech. 19:828–838, 2004.
56McLean, S. G., A. Su, and A. J. van den Bogert. Developmentand validation of a 3-d model to predict knee loading duringdynamic movement. J. Biomech. Eng. 125:864–874, 2003.
57Meyer, D. C., H. Hoppeler, B. von Rechenberg, and C. Gerber. Apathomechanical concept explains muscle loss and fatty changesfollowing surgical tendon release. J. Orthopaed. Res. 22:1004–1007, 2004.
58Mirka, G. A., N. F. Glasscock, P. M. Stanfield, and J. R. Wilson.An empirical approach to characterizing trunk muscle coacti-vation using simulation input modeling techniques. J. Biomech.33:1701–1704, 2000.
59Mirka, G. A., and W. S. Marras. A stochastic model of trunkmuscle coactivation during trunk bending. Spine 18:1396–1409,1993.
60Mooney, C. Z., and R. D. Duval, Bootstraping, a NonparametricApproach to Statistical Inference. Newbury Park: Sage, 1993.
61Murray, W. M., T. S. Buchanan, and S. L. Delp. The isometricfunctional capacity of muscles that cross the elbow. J. Biomech.33:943–952, 2000.
62Murray, W. M., T. S. Buchanan, and S. L. Delp. Scaling ofpeak moment arms of elbow muscles with upper extremity bonedimensions. J. Biomech. 35:19–26, 2002.
63Nakagaki, K., J. Ozaki, Y. Tomita, and S. Tamai. Fatty degen-eration in the supraspinatus muscle after rotator cuff tear. J.Shoulder Elbow Surg. 5:194–200, 1996.
64Nieminen, H., J. Niemi, E.-P. Takala, and E. Viikari-Juntura.Load-sharing patterns in the shoulder during isometric flexiontasks. J. Biomech. 28:555–566, 1995.
65Nygaard, E., M. Houston, Y. Suzuki, K. Jorgenson, and B. Saltin.Morphology of the brachial biceps muscle and elbow flexion inman. Acta Physiol. Scand. 117:287–292, 1983.
66Otis, J. C., C.-C. Jiang, T. L. Wickiewicz, M. G. E. Peterson,R. F. Warren, and T. J. Santner. Changes in the moment arms ofthe rotator cuff and deltoid muscles with abduction and rotation.J. Bone Joint Surg. 76-A:667–676, 1994.
67Pappas, G. P., D. S. Asakawa, S. L. Delp, F. E. Zajac, and J.E. Drace. Nonuniform shortening in the biceps brachii duringelbow flexion. J. Appl. Physiol. 92:2381–2389, 2002.
68Pruim, G. J., H. J. de Jongh, and J. J. ten Bosch. Forces actingon the mandible during bilateral static bite at different bite forcelevels. J. Biomech. 13:755–763, 1980.
69Redfern, M. S. Emg-torque modeling including cocontractionat the ankle. In: Advances in Industrial Ergonomics and Safety,edited by I. A. Mital. Philadelphia: Taylor & Francis, 1989,pp. 137–142.
70Reinold, M. M., K. E. Wilk, G. S. Fleisig, N. Zheng, S. W.Barrentine, T. Chmielewski, R. C. Cody, G. G. Jameson, andJ. R. Andrews. Electromyographic analysis of the rotator cuffand deltoid musculature during common shoulder external
476 LANGENDERFER et al.
rotation exercises. J. Orthopaed. Sports Phys. Ther. 34:385–394,2004.
71Sharkey, N. A., and R. A. Marder. The rotator cuff opposessuperior translation of the humeral head. Am. J. Sports Med.23:270–275, 1995.
72Shimizu, T., E. Itoi, H. Minagawa, R. L. Pradhan, I.Wakabayashi, and K. Sato. Atrophy of the rotator cuff musclesand site of cuff tears. Acta Orthopaed. Scand. 73:40–43, 2002.
73Thelen, D. G., A. B. Schultz, S. D. Fassois, and J. A.Ashton-Miller. Identification of dynamic myoelectric signal-to-force models during isometric lumbar muscle contractions. J.Biomech. 27:907–919, 1994.
74Thompson, W. O., R. E. Debski, I. Boardman, N. Douglas,E. Taskiran, J. J. P. Warner, F. H. Fu, and S. L.-Y. Woo. Abiomechanical analysis of rotator cuff deficiency in a cadavericmodel. Am. J. Sports Med. 24:286–292, 1996.
75Valero-Cuevas, F. J., M. E. Johanson, and J. D. Towles. Towardsa realistic biomechanical model of the thumb: The choice ofkinematic description may be more critical than the solutionmethod or the variability/uncertainty in musculoskeletal param-eters. J. Biomech. 36:1019–1030, 2003.
76van der Helm, F. C. T. A finite element musculoskeletal modelof the shoulder mechanism. J. Biomech. 27:551–569, 1994.
77Veeger, H. E. J., F. C. T. van Der Helm, L. H. V. VanDer Woude, G. M. Pronk, and R. H. Rozendal. Inertia and
muscle contraction parameters for musculoskeletal model-ing of the shoulder mechanism. J. Biomech. 24:615–629,1991.
78Walch, G., A. Boulahia, S. Calderone, and A. H. N. Robin-son. The ‘dropping’ and ‘hornblower’s’ signs in evaluation ofrotator-cuff tears. J. Bone Joint Surg. Br. Vol. B 80:624–628,1998.
79Ward, S. R., L. H. Smallwood, J. Friden, and R. L. Lieber. Ro-tator cuff muscle architecture: Implications for glenohumeraljoint stability. in Proceedings, XXth Congress of the Inter-national Society of Biomechanics and 29th Annual Meetingof the American Society of Biomechanics. 2005, Cleveland,Ohio.
80Wothke, W. Non-positive definite matrices in structural mod-eling. In: Testing Structural Equation Models, edited by K. A.Bollen and J. S. Long. Newbury Park: Sage, 1993, pp. 256–293.
81Yucesoy, C. A., B. H. F. J. M. Koopmana, G. C. Baan, H. J.Grootenboera, and P. A. Huijing. Effects of inter- and extra-muscular myofascial force transmission on adjacent synergisticmuscles: Assessment by experiments and finite-element model-ing. J. Biomech. 36:1797–1811, 2003.
82Zajac, F. E. Muscle and tendon: Properties, models, scaling,and application to biomechanics and motor control. Crit. Rev.Biomed. Eng. 17:359–411, 1989.