Quantitative Analysis of Prenatal Intake of n-3olyunsaturated Fatty Acids and Cognitiveevelopment
oshua T. Cohen, PhD, David C. Bellinger, PhD, William E. Connor, MD, Bennett A. Shaywitz, MD
bstract: Although a rich source of n-3 polyunsaturated fatty acids (PUFAs) that may confer multiplehealth benefits, some fish also contain methyl mercury (MeHg), which may harm thedeveloping fetus. U.S. government recommendations for women of childbearing age are tomodify consumption of high-MeHg fish to reduce MeHg exposure, while recommenda-tions encourage fish consumption among the general population because of the nutri-tional benefits. The Harvard Center for Risk Analysis convened an expert panel (seeacknowledgments) to quantify the net impact of resulting hypothetical changes in fishconsumption across the population. This paper estimates the impact of prenatal n-3 intakeon cognitive development. Other papers quantify the negative impact of prenatal exposureto MeHg on cognitive development, and the extent to which fish consumption protectsagainst coronary heart disease mortality and stroke in adults.
ecause of evidence that prenatal exposure tomethyl mercury (MeHg) in fish may adverselyaffect cognitive development, the U.S. Food and
rug Administration (FDA) and the U.S. Environmen-al Protection Agency issued a joint advisory in March004 recommending that pregnant women modifyheir fish consumption.1 However, fish is a rich sourcef n-3 polyunsaturated fatty acids (PUFAs). The n-3UFAs may confer protection against coronary heartisease (CHD) and stroke in adults, and may benefitognitive development of the fetus during pregnancy.
rom the Harvard Center for Risk Analysis, Harvard School of Publicealth (Cohen), and Department of Neurology, Children’s Hospital
Bellinger), Boston, Massachusetts; Division of Endocrinology, Dia-etes and Clinical Nutrition, Oregon Health Sciences UniversityConnor), Portland, Oregon; and Department of Pediatrics andeurology, Yale University (Shaywitz), New Haven, ConnecticutAddress correspondence and reprint requests to: Joshua T. Cohen,
shD, Harvard Center for Risk Analysis, 718 Huntington Avenue,oston MA 02115. E-mail: [email protected].
Depending on how they are implemented, interven-ions to decrease exposure to MeHg may decrease overallsh consumption. For example, Oken et al.2 reported a7% decrease in fish consumption among pregnantomen following the release of the FDA’s 2001 MeHgdvisory. Moreover, other members of the populationould decrease their fish consumption as an unintendedonsequence of risk management actions targeting MeHgxposure among women of childbearing age.In order to understand the possible public health
amifications of alternative risk management actions, its necessary to quantify potential health benefits andisks associated with plausible changes in populationsh-consumption patterns. This paper reviews the liter-ture on the cognitive benefits of increasing n-3 intaken infants as a starting point for quantifying the benefitsf maternal n-3 intake during pregnancy, since there is
imited direct information on the relationship betweenaternal n-3 intake during pregnancy and cognitive
evelopment of the fetus. These benefits can then beompared to the risks associated with mercury expo-
ure associated with fish consumption. This paper
0749-3797/05/$–see front matterlished by Elsevier Inc. doi:10.1016/j.amepre.2005.06.008
qtIcmidftti
Jraitgc
ristificnst
nieraatg
Dn
OsrIdetbi
L
Tt
paoaa
bebfdFt
owfPssiapntim
osrbcmtn
soidcmtstmapcat
tit
uantifies the cognitive benefits of n-3 consumption inerms of changes in cognitive ability as measured by IQ.n particular, this analysis quantifies the permanenthange in child IQ score per gram per day increase inaternal n-3 PUFA intake. Developing this estimate
nvolves the aggregation of results across studies usingifferent test instruments, extrapolation of impactsrom early in childhood to later in life, and extrapola-ion of findings from studies investigating supplemen-ation of baby formula with n-3 PUFAs to maternalntake of n-3 PUFAs during pregnancy.
Three other papers in this issue of the Americanournal of Preventive Medicine develop dose–responseelationships between prenatal MeHg exposure and IQ,nd between adult fish consumption and both strokencidence and CHD mortality.3–5 A fifth paper, also inhis issue, combines these results to estimate the aggre-ate health effects of hypothetical changes in fishonsumption on public health.6
There have been at least two efforts to systematicallyeview the literature on cognitive function and infantntake of n-3 PUFAs.7,8 However, those reviews are notufficient for our purposes for two reasons. First, al-hough they summarize the findings of different stud-es, these reviews do not quantitatively aggregate thendings so that they can be expressed in terms of aommon metric (IQ points gained per gram per day of-3 PUFA intake). Second, these reviews do not con-ider several recent studies that were not available athe time of their publication.
The remainder of this paper has three parts. Theext section describes the methodology for aggregating
nformation across studies that have measured thisffect to quantify this relationship. The Results sectioneports the results in terms of the change in IQssociated with supplement intake. Finally, the findingsre discussed and the dose–response relationship be-ween IQ and maternal n-3 PUFA intake (IQ points perram per day of n-3 maternal intake) is quantified.
evelopment of a Dose–Response Relationship for-3 Intake and Cognitive Effects
ur methodology consists of three steps: identifyingtudies for inclusion in this analysis; aggregating theesults and re-expressing them in terms of a change inQ; and estimating the prenatal maternal intake ofecosahexaenoic acid 22:6 n-3 (DHA) that produces anquivalent DHA internal dose to the child. Combininghese results yields an estimate of the relationshipetween prenatal maternal DHA intake and the change
n child’s IQ.
iterature Included in Analysis
he theory that different types of lipids may be critical
o health in general and to early development in l
articular can be traced back to the 1920s.9 Becausenimals cannot synthesize n-3 PUFAs, humans dependn their diet for this nutrient.10 Marine animals containrelatively high concentration of n-3 PUFAs because
quatic plants synthesize these molecules.The n-3 PUFA molecule plays a crucial role in the
rain, accounting for one third of the PUFA content ofthanolamine and serine phosphoglycerides in therains of humans, monkeys, and rats. Studies haveound that completely removing n-3 PUFAs from theiet can adversely affect the nervous system in animals.or example, monkeys deprived of n-3 PUFAs duringhe prenatal period suffer visual disturbances.11
In human neonates, the debate over the essentialityf n-3 PUFAs has often been argued in the context ofhether infants fed breast milk are healthier than
ormula-fed infants (because breast milk contains n-3UFAs),12 and in the context of whether infant formulahould be supplemented with n-3 PUFAs. Althoughome investigators have concluded that maternal dietnfluences the supply of n-3 PUFAs to fetuses in utero,13,14
nd although at least one investigator found thatregnancy outcome may be influenced by the supply of-3 PUFAs,15 only one study was found that investigated
he potential association between maternal n-3 PUFAntake during pregnancy and later cognitive develop-
ent in offspring.16
This review therefore also includes randomized trialsf formula supplements for two reasons. First, as de-cribed below, there have been a substantial number ofandomized trials that have investigated the associationetween n-3 PUFA intake during infancy and laterognitive development. Second, there is evidence thataternal n-3 PUFA intake influences n-3 PUFA concen-
rations in breast milk, and hence influences neonatal-3 PUFA intake.17–19
This investigation omits from consideration the twotudies identified20,21 that have investigated the impactf formula supplementation on cognitive development
n preterm infants. Studies of preterm infants are notirectly comparable with studies of term infants be-ause the benefits conferred by formula supplementsay be greater for preterm infants than they are for
erm infants. For example, Fewtrell et al.21 observed atatistically significant improvement in developmentalest scores among preterm infants administered for-
ula supplements (gestation �30 months), but notmong infants with longer gestations. N-3 PUFA sup-lements may especially benefit preterm infants be-ause they are deprived of the typical n-3 PUFA supplyvailable in utero during the critical thirdrimester.22,23
This analysis also limits attention to randomizedrials, which make up the majority of the studiesnvestigating this issue, and avoids the uncertainty dueo confounding that is typically a much greater prob-
em in observational studies. In particular, omitted
Am J Prev Med 2005;29(4) 366.e2
ffrh
awcwiicraif
AD
Dbrsii[LitICav[(tmosHt
ocemtgtratite
ir
dbgtcdoai
bemota
pmoot3dtwtttcaamslrar
frtatgt
ilswsn
3
rom consideration are comparisons between formula-ed and breast-fed infants because of the confoundingole that socioeconomic status and lifestyle factors canave in such comparisons.24,25
This analysis identified potential studies for inclusions follows (Table 1): First, studies identified by Simmer8
ere reviewed. To ensure consideration of more re-ently published literature, Medline (October 2003)as searched for studies that had the term LCPUFA in
ts title or abstract, and attention was restricted tonvestigations of children (aged 0 to 18) with a publi-ation date no earlier than 2000. In addition, theeferences of all retrieved studies were reviewed for anydditional studies of cognitive function and infantntake of n-3 PUFAs. Studies available only in abstractorm37–39 were eliminated from consideration.
ggregation of Results Across Postnatalevelopment Studies
evelopment of a single estimate of an associationetween dietary supplements and cognitive functionequires aggregation of scores both within and acrosstudies. To accomplish this aggregation, each test useds first assigned to one of three domains: (1) generalntelligence (Bayley Scales of Infant DevelopmentBSID] Mental Development Index [MDI], Brunet–ezine Developmental Quotient [DQ], problem solv-
ng, Knobloch Passamanik and Sherrards Developmen-al Screening Inventory [KPSDSI], Fagan Test of Infantntelligence [FTII], Kaufman Assessment Battery forhildren [K-ABC], and Stanford–Binet IQ); (2) verbalbility (MacArthur Communicative Development In-entories, Peabody Picture Vocabulary Test-RevisedPPVT-R], mean length utterance); and (3) motor skillsBSID Psychomotor Development Index [PDI], andhe Beery Visual-Motor Index test). We realize that
any of the assessment tools classified here as measuresf general intelligence are more appropriately de-cribed as tests of development (e.g., the BSID MDI).owever, our classification reflects the finding that
hey are predictive of IQ performance at later ages.Within each test domain, this analysis uses at most
ne set of results for each treatment group. In eachase, the results recorded at the latest age are used. Forxample, Auestad et al.34 tested children at age 9onths using the FTII, and then at 12 months using
he BSID MDI. Because both of these tests fall into theeneral intelligence category, the FTII results are omit-ed in favor of the BSID MDI scores, which wereecorded at a later age. The FTII results are omitted inn effort to avoid “double counting” the results fromhe Auestad et al.34 study. The two studies that admin-stered tests from the vocabulary domain16,35 reportedwo sets of scores—one for comprehension and one for
xpression. In these two cases, the analysis first normal- p
66.e3 American Journal of Preventive Medicine, Volume 29, Nu
zes the scores (see next paragraph) and uses theesulting average.
To combine results across studies within each testomain, the analysis first normalizes the differenceetween the supplement group scores and the controlroup scores so that they are expressed in terms ofest-score standard deviations (SDs). For example, be-ause the IQ test has a population SD of 15 points, aifference of 1.5 IQ points corresponds to a differencef 0.10 SDs. If population norm characteristics are notvailable, the distribution reported for the study samples used to estimate the population SD.
Second, for studies that evaluated multiple formulas,oth treatment groups are included. Typically, forxample, one treatment group receives formula supple-ented with fish oil, which contains DHA, while the
ther receives formula supplemented with egg-derivedriglyceride (DTG), which contains both arachidoniccid (AA) and DHA.
Third, a weight is assigned to each result that is theroduct of its statistical precision (inverse of the nor-alized standard error [SE] squared), and an estimate
f its correlation with IQ scores later in life. In a reviewf the literature, McCall40concluded that the correla-ion between tests administered early in life (before age0 months) and IQ tests administered later in lifeepended on the age at which the tests were adminis-ered. In general, the greater the difference in ages, theeaker the correlation. Moreover, McCall40 concluded
hat “[t]he first and strongest effect is that the correla-ions increase linearly with the age at which the infantest is administered.” Regressing the marginal medianorrelations that McCall40 identified (0.12, 0.26, 0.39,nd 0.49) against the midpoint of the correspondingge ranges (1 to 6, 7 to 12, 13 to 18, and 19 to 30onths) suggests that the correlation with later IQ
cores increases by 0.0176 per month (R2�96%). Thisinear relationship is used to assign weights to testesults. For example, the weight assigned to a test resultt age 24 months is twice the weight assigned to a testesult at age 12 months.
The study conducted by Gibson et al.28 is eliminatedrom consideration because the investigators reportedesults only in terms of a correlation coefficient (be-ween various DHA-level measures and BSID scores),nd did not quantify the impact of DHA supplementa-ion on BSID performance in terms of the points lost orained for infants in the supplement group, comparedo infants in the control group.
Finally, the domain averages are combined by assign-ng each domain a weight. Although attention could beimited to the “general intelligence” domain, or even totudies that used the IQ test in particular, doing soould omit consideration of data that probably provide
ome indication of how supplements might affect cog-itive performance. The analysis therefore assigns some
ositive weight to the verbal ability domain and the
mber 4
mowsr
uwa
T
S
A
G
W
L
M
B
A
H
S
A k, wee
otor domain. Ideally, the weights assigned to thesether domains would correspond to the extent tohich they are correlated with general intelligence. A
earch of the ERIC database (keywords “IQ” and “cor-
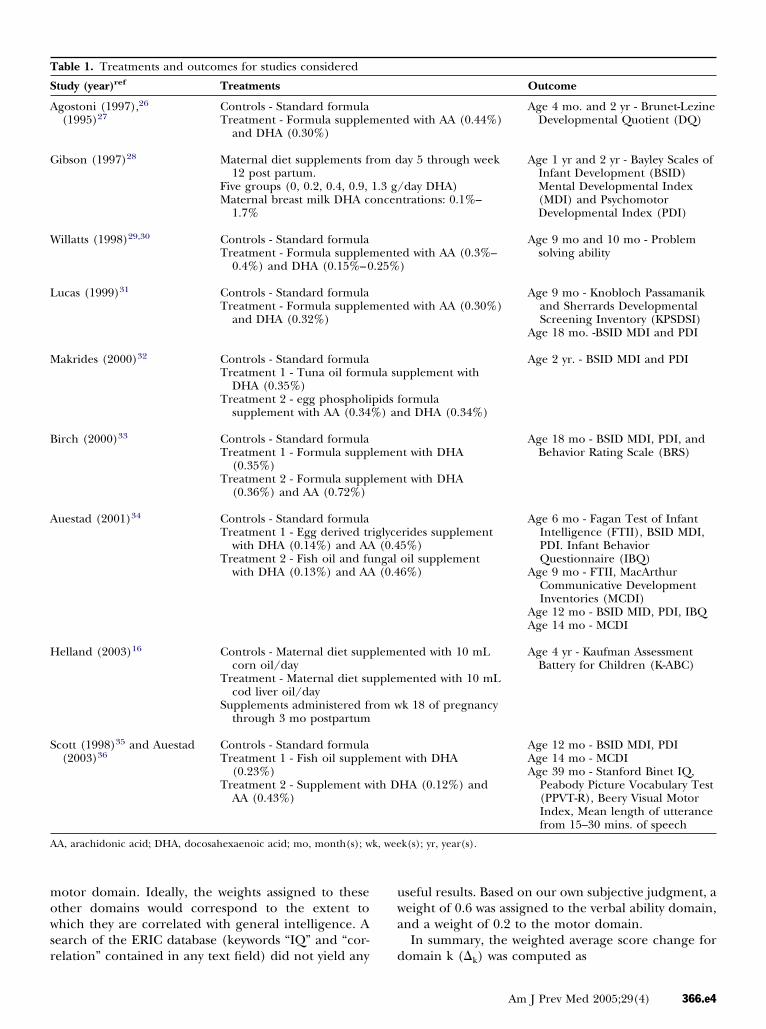
able 1. Treatments and outcomes for studies considered
tudy (year)ref Treatments
gostoni (1997),26
(1995)27Controls - Standard formulaTreatment - Formula supplem
and DHA (0.30%)
ibson (1997)28 Maternal diet supplements fr12 post partum.
Five groups (0, 0.2, 0.4, 0.9,Maternal breast milk DHA c
1.7%
illatts (1998)29,30 Controls - Standard formulaTreatment - Formula supplem
0.4%) and DHA (0.15%–0
ucas (1999)31 Controls - Standard formulaTreatment - Formula supplem
and DHA (0.32%)
akrides (2000)32 Controls - Standard formulaTreatment 1 - Tuna oil form
DHA (0.35%)Treatment 2 - egg phospholi
supplement with AA (0.34
irch (2000)33 Controls - Standard formulaTreatment 1 - Formula supp
Supplements administered frthrough 3 mo postpartum
cott (1998)35 and Auestad(2003)36
Controls - Standard formulaTreatment 1 - Fish oil supple
(0.23%)Treatment 2 - Supplement w
AA (0.43%)
A, arachidonic acid; DHA, docosahexaenoic acid; mo, month(s); w
elation” contained in any text field) did not yield any d
seful results. Based on our own subjective judgment, aeight of 0.6 was assigned to the verbal ability domain,nd a weight of 0.2 to the motor domain.
In summary, the weighted average score change for
Outcome
d with AA (0.44%)Age 4 mo. and 2 yr - Brunet-Lezine
Developmental Quotient (DQ)
ay 5 through week
day DHA)trations: 0.1%–
Age 1 yr and 2 yr - Bayley Scales ofInfant Development (BSID)Mental Developmental Index(MDI) and PsychomotorDevelopmental Index (PDI)
d with AA (0.3%–)
Age 9 mo and 10 mo - Problemsolving ability
d with AA (0.30%)Age 9 mo - Knobloch Passamanik
and Sherrards DevelopmentalScreening Inventory (KPSDSI)
Age 18 mo. -BSID MDI and PDI
pplement with
ormulad DHA (0.34%)
Age 2 yr. - BSID MDI and PDI
t with DHA
t with DHA
Age 18 mo - BSID MDI, PDI, andBehavior Rating Scale (BRS)
rides supplement5%)oil supplement6%)
Age 6 mo - Fagan Test of InfantIntelligence (FTII), BSID MDI,PDI. Infant BehaviorQuestionnaire (IBQ)
Age 9 mo - FTII, MacArthurCommunicative DevelopmentInventories (MCDI)
Age 12 mo - BSID MID, PDI, IBQAge 14 mo - MCDI
nted with 10 mL
ented with 10 mL
k 18 of pregnancy
Age 4 yr - Kaufman AssessmentBattery for Children (K-ABC)
with DHA
HA (0.12%) and
Age 12 mo - BSID MDI, PDIAge 14 mo - MCDIAge 39 mo - Stanford Binet IQ,
Peabody Picture Vocabulary Test(PPVT-R), Beery Visual MotorIndex, Mean length of utterancefrom 15–30 mins. of speech
k(s); yr, year(s).
ente
om d
1.3 g/oncen
ente.25%
ente
ula su
pids f%) an
lemen
lemen
iglyce(0.4
ngal(0.4
leme
pplem
om w
ment
ith D
omain k (�k) was computed as
Am J Prev Med 2005;29(4) 366.e4
wsamtww
wit
E
TnlinopwbmDicpptD(
RAR
TtcciAI1ti1
IM
Tmapm11saH
ID
O1naipmt
SW
Apnsovdesaawiaomomi
S
Fiatrt
3
�i
�i � SEi�2 � Agei
�i
SEi�2 � Agei
,
here �i is the standardized difference between theupplement group average score and the control groupverage score (positive value indicates superior perfor-ance among the supplement group subjects), SEi is
he SE of �i, and Agei is the age at which the subjectsere assessed. The overall standardized impact on IQas then calculated as
1
1.8(1.0�GI � 0.6�V � 0.2�M),
here the subscripts GI, M, and V refer to generalntelligence, verbal ability, and motor ability, respec-ively.
xtrapolation of Results to Prenatal Intake
he studies described above estimated the impact of-3 intake on cognitive development in terms of the
evel of DHA supplementation in formula. As describedn the technical appendix (located at www.ajpm-online.et), this analysis estimates that the impact on child IQf a 1-g/day increase in maternal DHA intake duringregnancy is 18% to 39% of the IQ impact associatedith a 1% increase in the DHA lipid fraction in eitherreast milk or formula. The appendix explains that toake this extrapolation, this analysis uses the childHA phospholipid fraction in plasma (or, alternatively,
n red blood cells [RBCs]) as a proxy for the biologi-ally effective dose. In particular, it is assumed here thatrenatal maternal DHA intake increasing the childlasma (RBC) DHA phospholipid fraction by 1% hashe same impact on cognitive development as formulaHA supplementation that increases the child’s plasma
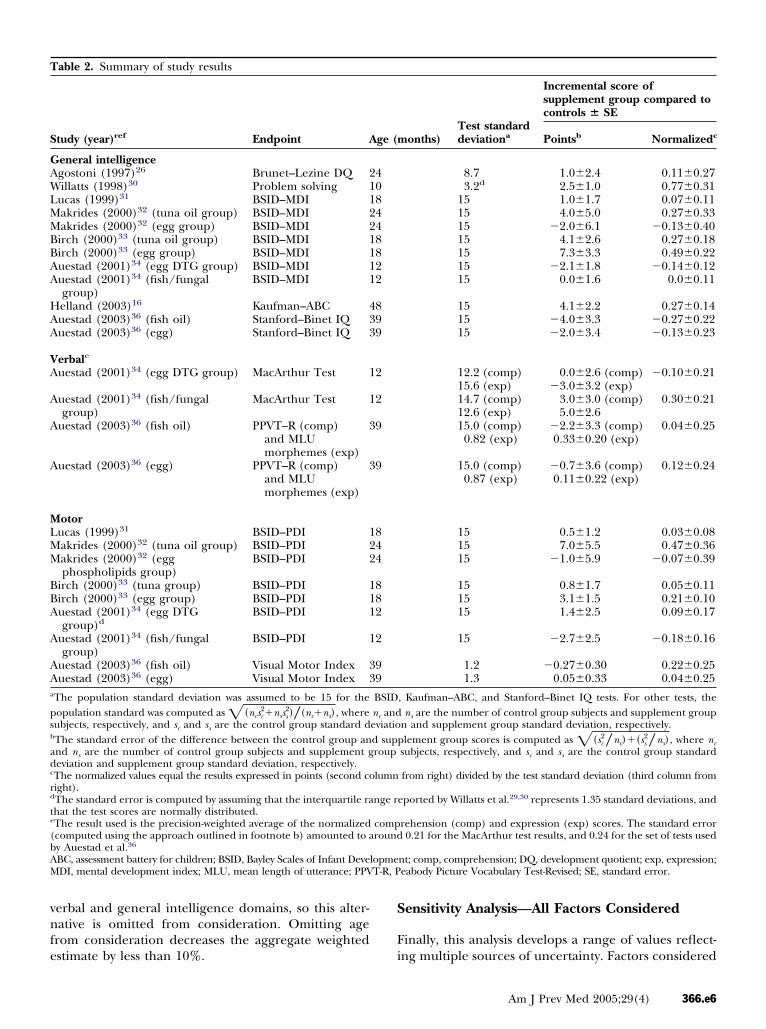
able 2 summarizes the study results used to estimatehe aggregate impact of infant n-3 PUFA intake onognitive function later in life. The weighted averagehanges for the three domains are 0.09 SDs (generalntelligence), 0.08 SDs (verbal), and 0.05 SDs (motor).ssuming that these impacts correspond to a change in
Q, they amount to 1.3 IQ points (general intelligence),.2 points (verbal), and 0.8 points (motor). Combininghe results across test domains yields a weighted averagencrease in test scores of 0.08 SDs, which corresponds to
.2 IQ points. i
66.e5 American Journal of Preventive Medicine, Volume 29, Nu
Q Points per 1% Increase in Formula or Breastilk DHA Lipid Fraction
o estimate � (change in IQ per 1% increase in breastilk or formula DHA phospholipids fraction), this
nalysis assumes that the aggregate increase of 1.2 IQoints corresponds to the average level of DHA supple-entation in the studies used here. All but one of the
2 supplement groups (Helland et al.16) listed in Tablethat were used to develop this estimate reported DHA
upplement concentrations. For these 11 groups, theverage DHA fraction was 0.26% with an SE of 0.03%.ence, ��1.2/0.26�4.6.
Q Points per Gram per Day Increase MaternalHA Intake During Pregnancy
ur methodology implies that the impact on IQ of a-g/day increase in maternal DHA intake during preg-ancy is equal to � multiplied by 18% to 39%. Hence,1-g/day increase in DHA intake during pregnancy will
ncrease the child’s IQ by 0.8 to 1.8 points. For theurpose of this analysis, it is assumed that the arith-etic mean of these values (1.3 IQ points) represents
he central estimate.
ensitivity Analysis—Accounting for Age in Studyeights
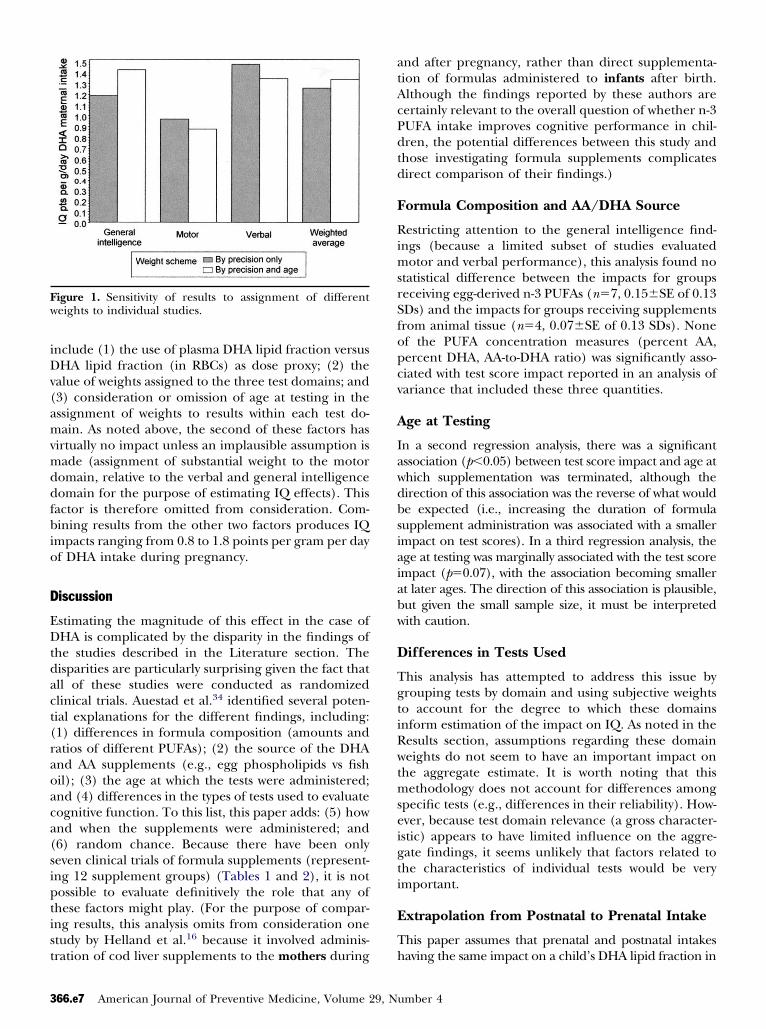
s illustrated in Figure 1, the central estimate of 1.3 IQoints per gram per day of DHA intake during preg-ancy is only modestly sensitive to the weightingcheme used. Each of the four pairs of bars representsne of the three test domains (general intelligence,erbal, and motor) and the weighted average of theseomains. Within each pair, the white bar represents thestimate produced when the weight assigned to eachtudy result reflects both the result’s statistical precisionnd the age at which cognitive development was evalu-ted. The gray bar represents the estimate producedhen age is omitted from the weight. Although not
llustrated in Figure 1, note that if all study results weressigned equal weight, the estimated aggregate impactn IQ would increase from 1.3 to 1.8 points pericrogram of DHA intake per day. This result is
mitted from further consideration because it does notake sense to disregard the statistical precision of the
ndividual study results.
ensitivity Analysis—Test Domain Weights
igure 1 also indicates that the verbal and generalntelligence domain values are similar to the weightedverage, suggesting that only by substantially increasinghe weight placed on the motor domain would theesults change substantially. However, it is implausiblehat the motor domain would contribute a great deal of
nformation to the estimation of IQ relative to the
mber 4
vnfe
S
F
T
S
GAWLMMBBAA
HAA
VA
A
A
A
MLMM
BBA
A
AAa
psb
adc
rd
te
(bAM T-R, P
erbal and general intelligence domains, so this alter-ative is omitted from consideration. Omitting age
rom consideration decreases the aggregate weighted
able 2. Summary of study results
tudy (year)ref Endpoint A
eneral intelligencegostoni (1997)26 Brunet–Lezine DQ 2illatts (1998)30 Problem solving 1
uestad (2003)36 (fish oil) Visual Motor Index 3uestad (2003)36 (egg) Visual Motor Index 3
The population standard deviation was assumed to be 15 for theopulation standard was computed as ��ncsc
2�nsss2�� �nc�ns� , where
ubjects, respectively, and sc and ss are the control group standard dThe standard error of the difference between the control group annd ns are the number of control group subjects and supplement geviation and supplement group standard deviation, respectively.The normalized values equal the results expressed in points (second coight).The standard error is computed by assuming that the interquartile rahat the test scores are normally distributed.The result used is the precision-weighted average of the normalizedcomputed using the approach outlined in footnote b) amounted to ay Auestad et al.36
BC, assessment battery for children; BSID, Bayley Scales of Infant DeveDI, mental development index; MLU, mean length of utterance; PPV
stimate by less than 10%. i
ensitivity Analysis—All Factors Considered
inally, this analysis develops a range of values reflect-
onths)Test standarddeviationa
Incremental score ofsupplement group compared tocontrols � SE
, Kaufman–ABC, and Stanford–Binet IQ tests. For other tests, thens are the number of control group subjects and supplement group
n and supplement group standard deviation, respectively.plement group scores is computed as ��sc
2�nc�� �ss2�ns� , where nc
subjects, respectively, and sc and ss are the control group standard
from right) divided by the test standard deviation (third column from
eported by Willatts et al.29,30 represents 1.35 standard deviations, and
rehension (comp) and expression (exp) scores. The standard error0.21 for the MacArthur test results, and 0.24 for the set of tests used
nt; comp, comprehension; DQ, development quotient; exp, expression;eabody Picture Vocabulary Test-Revised; SE, standard error.
ge (m
408448822
899
2
2
9
9
844
882
2
99
BSIDnc andeviatiod suproup
lumn
nge r
compround
lopme
ng multiple sources of uncertainty. Factors considered
Am J Prev Med 2005;29(4) 366.e6
iDv(amvmddfbio
D
EDtdact(raoaca(siptist
atAcPdtd
F
RimsrSfopcv
A
Iawdbsiaiabw
D
TgtiRwtmseigti
E
T
Fw
3
nclude (1) the use of plasma DHA lipid fraction versusHA lipid fraction (in RBCs) as dose proxy; (2) the
alue of weights assigned to the three test domains; and3) consideration or omission of age at testing in thessignment of weights to results within each test do-ain. As noted above, the second of these factors has
irtually no impact unless an implausible assumption isade (assignment of substantial weight to the motor
omain, relative to the verbal and general intelligenceomain for the purpose of estimating IQ effects). Thisactor is therefore omitted from consideration. Com-ining results from the other two factors produces IQ
mpacts ranging from 0.8 to 1.8 points per gram per dayf DHA intake during pregnancy.
iscussion
stimating the magnitude of this effect in the case ofHA is complicated by the disparity in the findings of
he studies described in the Literature section. Theisparities are particularly surprising given the fact thatll of these studies were conducted as randomizedlinical trials. Auestad et al.34 identified several poten-ial explanations for the different findings, including:1) differences in formula composition (amounts andatios of different PUFAs); (2) the source of the DHAnd AA supplements (e.g., egg phospholipids vs fishil); (3) the age at which the tests were administered;nd (4) differences in the types of tests used to evaluateognitive function. To this list, this paper adds: (5) hownd when the supplements were administered; and6) random chance. Because there have been onlyeven clinical trials of formula supplements (represent-ng 12 supplement groups) (Tables 1 and 2), it is notossible to evaluate definitively the role that any ofhese factors might play. (For the purpose of compar-ng results, this analysis omits from consideration onetudy by Helland et al.16 because it involved adminis-
igure 1. Sensitivity of results to assignment of differenteights to individual studies.
ration of cod liver supplements to the mothers during h
66.e7 American Journal of Preventive Medicine, Volume 29, Nu
nd after pregnancy, rather than direct supplementa-ion of formulas administered to infants after birth.lthough the findings reported by these authors areertainly relevant to the overall question of whether n-3UFA intake improves cognitive performance in chil-ren, the potential differences between this study andhose investigating formula supplements complicatesirect comparison of their findings.)
ormula Composition and AA/DHA Source
estricting attention to the general intelligence find-ngs (because a limited subset of studies evaluated
otor and verbal performance), this analysis found notatistical difference between the impacts for groupseceiving egg-derived n-3 PUFAs (n�7, 0.15�SE of 0.13Ds) and the impacts for groups receiving supplementsrom animal tissue (n�4, 0.07�SE of 0.13 SDs). Nonef the PUFA concentration measures (percent AA,ercent DHA, AA-to-DHA ratio) was significantly asso-iated with test score impact reported in an analysis ofariance that included these three quantities.
ge at Testing
n a second regression analysis, there was a significantssociation (p�0.05) between test score impact and age athich supplementation was terminated, although theirection of this association was the reverse of what woulde expected (i.e., increasing the duration of formulaupplement administration was associated with a smallermpact on test scores). In a third regression analysis, thege at testing was marginally associated with the test scorempact (p�0.07), with the association becoming smallert later ages. The direction of this association is plausible,ut given the small sample size, it must be interpretedith caution.
ifferences in Tests Used
his analysis has attempted to address this issue byrouping tests by domain and using subjective weightso account for the degree to which these domainsnform estimation of the impact on IQ. As noted in theesults section, assumptions regarding these domaineights do not seem to have an important impact on
he aggregate estimate. It is worth noting that thisethodology does not account for differences among
pecific tests (e.g., differences in their reliability). How-ver, because test domain relevance (a gross character-stic) appears to have limited influence on the aggre-ate findings, it seems unlikely that factors related tohe characteristics of individual tests would be verymportant.
xtrapolation from Postnatal to Prenatal Intake
his paper assumes that prenatal and postnatal intakes
aving the same impact on a child’s DHA lipid fraction in
mber 4
eTtoamiii
R
Tficcspkol
C
TDbBtwTallt
csiimtvelpctrot
TAMM
BcKPLmUmNasFtp
R
1
1
1
1
1
1
1
1
1
1
ither plasma or RBCs will have the same impact on IQ.he plausibility of this assumption is bolstered by findings
hat n-3 PUFA supplementation has its most unambigu-us impact on the neurologic function of preterm infants,s discussed in the introduction to this paper. Moreover,aternal PUFA status during pregnancy has an important
mpact on PUFA levels in newborns.16 For these reasons,t seems unlikely that prenatal n-3 intake would be lessmportant than postnatal intake.
andom Chance
he strength of this analysis is that it reflects the resultsrom a series of randomized control trials. These stud-es are generally less susceptible to systematic bias thatan affect observational studies due to the difficulty ofontrolling for confounders. While the small sampleize of some of the studies included here raises theossibility of chance confounding, it is important toeep in mind that this methodology places less weightn small studies (because their statistical precision is
ess than the statistical precision of larger studies).
onclusion
his analysis finds that an increase in maternal intake ofHA during pregnancy of 1 g/day will increase child IQy 0.8 to 1.8 points (central estimate of 1.3 points).ecause typical DHA intake associated with fish consump-
ion is well under 1 g/day, changes in fish consumptionill result in IQ effects amounting to a fraction of a point.hese differences are not clinically detectable. However,s with changes associated with exposure to neurotoxinsike lead,41 which are also typically undetectable at theevel of the individual, these changes can result in impor-ant impacts when aggregated over a population.
In interpreting this result, the factors complicatingomparisons across studies mentioned earlier in thisection must also be kept in mind, as well as the problemsntroduced by extrapolating these results (which predom-nantly reflect formula supplement studies) to the issue of
aternal n-3 PUFA intake during pregnancy. Finally,hese results reflect the extrapolation of results from aariety of test instruments administered very early in life tostimates of permanent changes in IQ later on. Nonethe-ess, the estimates developed here serve as a useful startingoint for the purpose of quantitatively evaluating theognitive benefits of maternal fish consumption, so thathese benefits can be compared to the attendant risksesulting from prenatal exposure to mercury. That trade-ff analysis is detailed in the final paper6 written as part ofhis project.
he expert panel convened by the Harvard Center for Risknalysis for this project was chaired by Steven M. Teutsch,D (Department of Outcomes Research and Management,
erck & Co., Inc., West Point PA). In addition to David
ellenger, William Connor, and Bennett Shaywitz, who areo-authors on this paper, the panel consisted of Penny M.ris-Etherton, PhD (Department of Nutritional Sciences,ennsylvania State University, University Park PA), Robert S.awrence, MD (Department of Health Policy and Manage-ent, Bloomberg School of Public Health, Johns Hopkinsniversity, Baltimore MD), and David A. Savitz, PhD (Depart-ent of Epidemiology, School of Public Health, University oforth Carolina, Chapel Hill NC). This work was supported bygrant from the National Food Processors Association Re-
earch Foundation (NFPA-RF) and the Fisheries Scholarshipund. Member companies of the NFPA-RF may be affected byhe findings of research that funded my participation on theanel that wrote this paper.
eferences1. U.S. Department of Health and Human Services, U.S. Environmental Protec-
tion Agency. What you need to know about mercury in fish and shellfish, 2004.Available at: www.cfsan.fda.gov/�dms/admehg3.html. Accessed December2004.
2. Oken E, Kleinman KP, Berland WE, Simon S, Rich-Edwards JW, GillmanMW. Decline in fish consumption among pregnant women after a nationalmercury advisory. Obstet Gynecol 2003;102:346–51.
3. Konig A, Bouzan C, Cohen JT, et al. A quantitative analysis of fish consumptionand coronary heart disease mortality. Am J Prev Med 2005;29:335–46.
4. Bouzan C, Cohen JT, Connor WE, et al. A quantitative analysis of fishconsumption and stroke risk. Am J Prev Med 2005;29:347–52.
5. Cohen JT, Bellinger DC, Shaywitz BA. A quantitative analysis of prenatalmethyl mercury exposure and cognitive development. Am J Prev Med2005;29:353–65.
6. Cohen JT, Bellinger DC, Connor WE, et al. A quantitative risk benefitanalysis of changes in population fish consumption. Am J Prev Med2005;29:325–34.
7. Willatts P, Forsyth JS. The role of long-chain polyunsaturated fatty acids ininfant cognitive development. Prostaglandins Leukot Essent Fatty Acids2000;63:95–100.
8. Simmer K. Longchain polyunsaturated fatty acid supplementation ininfants born at term. Cochrane Database Syst Rev, CD 000376, 2001;1.
9. Uauy R, Hoffman DR. Essential fat requirements of preterm infants. Am JClin Nutr 2000;71:245S–50S.
0. Neuringer M, Connor WE. N-3 fatty acides in the brain and retina:Evidence for their essentiality. Nutr Rev 1986;44:285–94.
1. Neuringer M, Connor WE, Lin DS, Barstad L, Luck S. Biochemical andfunctional effects of prenatal and postnatal omega 3 fatty acid deficiency onretina and brain in rhesus monkeys. Proc Natl Acad Sci U S A1986;83:4021–5.
2. Kurlak LO, Stephenson TJ. Plausible explanations for effects of long chainpolyunsaturated fatty acids (LCPUFA) on neonates. Arch Dis Child FetalNeonatal Ed 1999;80:F148–54.
3. Lauritzen L, Jorgensen MH, Hansen HS, Michaelsen KF. Fluctuations inhuman milk long-chain PUFA levels in relation to dietary fish intake. Lipids2002;37:237–44.
4. Connor WE, Lowensohn R, Hatcher L. Increased docosahexaenoic acidlevels in human newborn infants by administration of sardines and fish oilduring pregnancy. Lipids 1996;31:S-183–7.
5. Al MD, van Houwelingen AC, Hornstra G. Long-chain polyunsaturatedfatty acids, pregnancy, and pregnancy outcome. Am J Clin Nutr2000;71:285S–91S.
6. Helland IB, Smith L, Saarem K, Saugstad OD, Drevon CA. Maternal supple-mentation with very long chain n–3 fatty acids during pregnancy and lactationaugments children’s IQ at 4 years of age. Pediatrics 2003;111:E39–44.
7. Harris WS, Connor WE, Lindsey BS. Will dietary omega–3 fatty acidschange the composition of human milk. Am J Clin Nutr 1984;40:780–5.
8. Henderson RA, Jensen RG, Lammi-Keefe CJ, Ferris AM, Dardick KR. Effectof fish oil on the fatty acid composition of human milk and maternal infanterythrocytes. Lipids 1992;27:863–9.
9. Makrides M, Neumann MA, Gibson RA. Effect of maternal docosahexa-
enoic acid (DHA) supplementation on breast milk composition. Eur J ClinNutr 1996;50:352–7.
Am J Prev Med 2005;29(4) 366.e8
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
3
0. O’Connor DL, Hall R, Adamkin D, et al. Growth and development inpreterm infants fed long-chain polyunsaturated fatty acids: a prospective,randomized controlled trial. Pediatrics 2001;108:359–71.
1. Fewtrell MS, Morley R, Abbott RA, et al. Double-blind, randomized trial oflong-chain polyunsaturated fatty acid supplementation in formula fed topreterm infants. Pediatrics 2002;110:73–82.
2. Birch EE, Hoffman DR, Uauy R, Birch DG, Prestige C. Visual acuity andessentiality of docosahexaenoic acid and arachidonic acid in the diet ofterm infants. Pediatr Res 1998;44:201–9.
3. Wainwright PE. Dietary essential fatty acids and brain function: a develop-mental perspective on mechanisms. Proc Nutr Soc 2002;61:61–9.
4. Scott JA, Binns CW. Factors associated with the initiation and duration ofbreastfeeding: a review of the literature. Breastfeed Rev 1999;7:5–16.
5. Olds DL, Henderson CR, Tatelbaum R. Intellectual impairment in children ofwomen who smoke cigarettes during pregnancy. Pediatrics 1994;93:221–7.
6. Agostoni C, Trojan S, Bellu R, Riva E, Bruzzese MG, Giovannini M.Developmental quotient at 24 months and fatty acid composition of diet inearly infancy: a follow-up study. Arch Dis Child 1997;76:421–4.
7. Agostoni C, Trojan S, Bellu R, Riva E, Giovannini M. Neurodevelopmentalquotient of healthy term infants at 4 months and feeding practice: the roleof long-chain polyunsaturated fatty acids. Pediatr Res 1995;38:262–6.
8. Gibson RA, Neumann MA, Makrides M. Effect of increasing breast milkdocosahexaenoic acid on plasma and erythrocyte phospholipid fatty acidsand neural indices of exclusively breast fed infants. Eur J Clin Nutr1997;51:578–84.
0. Willatts P, Forsyth JS, DiModugno MK, Varma S, Colvin M. Effect oflong-chain polyunsaturated fatty acids in infant formula on problemsolving at 10 months of age. Lancet 1998;352:688–91.
1. Lucas A, Stafford M, Morley R, et al. Efficacy and safety of long-chain
66.e9 American Journal of Preventive Medicine, Volume 29, Nu
2. Makrides M, Neumann MA, Simmer K, Gibson RA. A critical appraisal ofthe role of dietary long-chain polyunsaturated fatty acids on neural indicesof term infants: a randomized, controlled trial. Pediatrics 2000;105:32–8.
3. Birch EE, Garfield S, Hoffman DR, Uauy R, Birch DG. A randomizedcontrolled trial of early dietary supply of LCPUFA and mental developmentin term infants. Dev Med Child Neurol 2000;42:174–81.
4. Auestad N, Halter R, Hall RT, et al. Growth and development in terminfants fed long-chain polyunsaturated fatty acids: a double-masked, ran-domized, parallel, prospective, multivariate study. Pediatrics 2001;108:372–81.
5. Scott DT, Janowsky JS, Carroll RE, Taylor JA, Auestad N, Montalto MB.Formula supplementation with long-chain polyunsaturated fatty acids: Arethere developmental benefits? Pediatrics 1998;102:e59.
6. Auestad N, Scott DT, Janowsky J, et al. Visual, cognitive, and languageassessments at 39 months: a follow-up study of children fed formulascontaining long-chain polyunsaturated fatty acids to 1 year of age. Pediat-rics 2003;112:e177–83.
7. Clausen V, Damli A, Schenck UV, Koletzko B. Influence of long-chainpolyunsaturated fatty acids (LCPUFA) on early visual acuity and mentaldevelopment of term infants. Proceedings of the American Oil Chemists’Society, Barcelona, 1996.
8. Janowsky J, Scott DT, Wheeler RE, Auestad N. Fatty acids affect earlylanguage development. Pediatr Res 1995;41:310A.
9. Scott DT, Janowsky JS, Hall RT, et al. Cognitive and language assessment of3.25-year-old children fed formulas with or without longchain polyunsatu-rated fatty acids in the first year. Pediatr Res 1997;41:240A.
0. McCall RB. The develoment of intellectual functioning in infancy and theprediction of later IQ. In: Osofsky JD, ed. Handbook of infant develop-ment. New York: Wiley, 1979:707–41.
1. Schwartz J. Societal benefits of reducing lead exposure. Environ Res
1994;66:105–24.
mber 4
Am J Prev Med 2005;29(4) 366.e10
3
66.e11 American Journal of Preventive Medicine, Volume 29, Number 4