A quantitative comparative study measuring consumer satisfaction based on health record format by Moore, Vivianne E., D.M.
128
A QUANTITATIVE COMPARATIVE STUDY MEASURING CONSUMER SATISFACTION BASED ON HEALTH RECORD FORMAT by Vivianne E. Moore A Dissertation Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Management in Organizational Leadership UNIVERSITY OF PHOENIX February 2013
Transcript
A QUANTITATIVE COMPARATIVE STUDY MEASURING CONSUMER
SATISFACTION BASED ON HEALTH RECORD FORMAT
by
Vivianne E. Moore
A Dissertation Presented in Partial Fulfillment
of the Requirements for the Degree
Doctor of Management in Organizational Leadership
UNIVERSITY OF PHOENIX
February 2013
All rights reserved
INFORMATION TO ALL USERSThe quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscriptand there are missing pages, these will be noted. Also, if material had to be removed,
studies included the design of efficient EHR systems, best practices, communication, and data
collection for quality of care, cost, efficiency, and patient views (Stewart et al., 2010). This study
does not measure changes in communication patterns or changes in behavior that limit the factors
42
that contribute to consumer satisfaction as it relates to a health care provide-consumer
interaction.
Wager et al. (2009) noted consumers have concerns with privacy as well as how personal
medical information is being accessed and used. Concerns with third parties, such as health care
providers, insurance companies, government agencies, drug companies, and employers, may be
accessing medical data for inappropriate reasons are other consumer concerns. The discoveries
of these studies confirm how lack of information regarding data protection can promote mistrust
among consumers and health care professionals. This lack of trust is despite the laws,
regulations, and ethical requirements for health care data protection.
Zandieh et al. (2008) found privacy to be a concern for most patients and practitioners.
Ventres et al. (2006) through a study found a large gap in the patient understanding of the use of
EHRs in which patients lacked understanding of the use of EHRs in health care. Morpace
Omnibus conducted a study to measure consumer support of the nationwide system of medical
records. The study found most participants had little knowledge of the system, although 48%
supported the creation of the nationwide system (“Electronic Medical Records”, 2008).
Issues with communication can also have legal implications. Ervin and Berry (2006)
explored the physician’s views on health care information systems. Physicians noted that many
malpractice claims correlate to miscommunication between physician and patient (Ervin &
Berry, 2006). The issues with lack of consolidated historical information, data management, and
information inaccuracies surfaced during the study. Data management is a requirement for the
health care provider-consumer interaction to avoid mistakes with treatment protocols, data
gathering, medication error avoidance, and effective communication.
43
Cockcroft (2009) conducted a media analysis for evaluating the national health
information development. The analysis provides insight into the issues with communication and
the electronic health records implementation. Cockcroft noted the implementation of the EHRs
system is difficult to evaluate as there is no standard, and the systems are complex by nature.
Studies show that face-to-face interaction was still a requirement even when EHR systems were
in place (Cockcroft, 2009).
Context. The studies referenced provided supporting information for understanding the
issues with EHR implementation, consumer satisfaction, and communication channels. The
literature did not provide an example where the consumer views measured the use of medical
records and the communication channels available to the consumer or the effects to the health
care provider-consumer dynamic. This quantitative comparative study measuring the consumer’s
view on the implementation of EHR systems contributes to the existing literature by providing
the consumer views on the research parameters and how this may influence consumer
satisfaction.
Sample Population. Implications to the digitizing of medical records include concerns
with privacy, security, lack of control, data management, transcribing error rates, and
information dissemination. As consumers, several questions arise, such as How will the system
be managed and secured? How will the necessary information for access, protection, and usage
be acquired? What is the implication to privacy? These concerns will affect most consumers but
in particular the senior citizen population because they have limited avenues for information.
The senior citizen community has the greater need for health care due to their age and
health requirements (Bodkin & Miaoulis, 2007). The lack of understanding the implications of
privacy and controlling their health care information can contribute to misunderstanding or
44
misuse of medical records by the medical industry, vendors who support the industry, or
malicious individuals’ intent on identity theft. This community may also have limited access to
communication channels, and therefore may not be aware of the benefits or disadvantages of
using the Internet to gather information regarding health concerns.
Environment. The federal government has set the goal for most Americans to have
electronic health records by 2014. According to the National Health Statistics Reports, there
were only 19.6% EMR system implementations in 2007 (Hing & Hsiao, 2010). Hing and Hsiao
noted the expectation is only 64.5% EMR system implementations by 2010. A study conducted
in 2008 showed 41.5% of physicians report using all or partial EHR systems (Hsiao et al., 2010).
These statistics show the slow adoption of EHR systems and the current use of paper-
based medical records by health care professionals. The current environment with a mix of
paper-based and electronic health records should assist in measuring the consumer views on the
use of medical records and the effect on communication through consumer satisfaction. The
assumption is that consumers have access to either paper-based or electronic health records as
well as the communication channels to understand their use and protection.
Future Trends. As the adoption of EHRs becomes the norm, future considerations for
consumers should include appropriate legislation for security and access. Other considerations
should include consumer education on the use of health records to include methods of reporting
tests and results, and data interpretation on meaning of data provided (Wiljer et al., 2008). The
determination should also be made on how much information is available and limitations on who
can access this data. Consumer and health care provider education is critical in understanding the
implications and benefits of EHRs implementation and accessibility by the consumer. This
45
education would be supplemental to the health care provider interaction rather than a
replacement (Wiljer et al., 2008).
Synthesis
The literature review provided in this chapter aligns with the purpose and goal of the
quantitative comparative study. The purpose of this study was to measure how the consumers
perceive their interaction with health care providers based on the format of medical records
(electronic or paper) and how it affects communication and consumer satisfaction. The goal of
the study was to provide health care and government leadership the mechanism to gather
consumer feedback, to implement changes, and to improve the communication between
consumers and health care leadership by providing consumer education.
The overview information, issues, and gaps supported the study by identifying previous
research within the parameters to be measured in the quantitative comparative study. Issues with
implementation, lack of understanding legislation, health care and government leadership
communication, and the media’s role as a consumer communication vehicle aligned with what
the study was looking to measure. The sample population provided diverse views based on
gender, age, education, and race representative of the larger population who will benefit from the
discoveries of this study. The environment of medical record used in either digital or paper-based
format is appropriate in understanding how the implementation challenges and adoption affect
the consumer as it relates to communication and consumer satisfaction.
Chapter Conclusion
The health records digitization will cut health care cost, provide a source of information
for physicians and consumers, and save time in administrative functions with the ultimate goal of
improving health care. The government’s directive to have medical records digitized by 2014
46
will present many challenges. Some of these challenges will be in creating integrated systems for
access, security and management, policies, application of new technologies, and global
implementation. Digitizing medical records will have many benefits.
The benefits include a “patient-centered and patient-secure” system, promote information
sharing between systems, provide a source interface for consumers and physicians, cut costs,
possibly improve health care, and reduce paper (Noyes, 2009). How the changes will affect the
health care system and communication process is unclear; so it may be necessary for the
consumer to play a proactive role in attaining this information. As consumers, it is important to
understand the implications of digitizing medical records because the changes will have a direct
effect on information retrieval, review, and access. The benefits can also outweigh the
disadvantages. The Internet has given consumers a medium to understand these implications, but
this information is only useful if it is reliable and accurate.
Wager et al. (2009) noted the full effect of Internet resources may not be fully
understood. The Internet allows consumers universal connectivity and an affordable means to
connect to health care information and resources for personal health management. The Internet
was noted as a technology enabler that promotes the flow in information and breaks down
organizational boundaries (Wager et al., 2009).
Communication seems to be the dominant concept in the use of medical records. Some
studies reference the benefit in using EHRs for consumer-physician communication,
empowerment to consumer to self-manage health care as well as the anticipated improvements in
health care (Alkayid et al., 2009; Ouschan et al., 2006; Robb & Greenhalgh, 2006). Other studies
note the challenges in implementation and the lack of accurate communication channels in order
47
for the consumer to fully accept and understand the benefits of EHRs (Lanseng & Andreassen,
2007; Lee & Meuter, 2010; Stockdale, 2008).
Technology can bridge the information gap for many consumers, but it cannot replace the
face-to-face interaction with health care providers. Technology offers societal applications that
facilitate information gathering and provides knowledge to a consumer as it applies to medical
concerns or legislation; but it does not replace the health care provider-consumer dynamic that
can be achieved only through face-to-face interaction. This traditional form of medical
interaction provides personal interaction and individualized advice to the consumer (Alkayid et
al., 2009; Zickmund et al., 2007). The challenges in communication posed by the implementation
of medical health records align with the purpose and goal of this quantitative comparative study.
Summary
The growth of technology has evolved to the point where consumers may not require a
face-to-face meeting to obtain appropriate health care information. Advances in technology, such
as health care information systems, web portals, and the Internet, can provide an abundance of
information for the consumer and increase the consumer knowledge as well as self-management
of health care concerns. Self-management can improve health outcomes, cut costs in health care
resources, as well as empower the consumer to take an active role in managing his or her own
health.
The implementation of electronic health records should improve health care quality. The
challenges in implementation, lack of communication strategies, and the consumer lack of
knowledge in legislation in place to protect medical data may not fulfill this objective. Although
many studies have shown the benefits of using EHRs, there are many other studies that do not
support the assertion that in the current state of adoption, EHRs improve quality of care
48
(Zickmund et al., 2007). Issues with communication and technology, issues with lack of effective
communication channels, and insufficient information trickling down to the consumer may affect
the measurement of the quality of care.
Chapter 3 provides the research method for the study. The discussion includes the
justification for doing a quantitative study using the comparative design and elaborates on the
study goals. The sample population, the survey tool, and data collection process are also
presented. The discussion also includes the volunteer recruitment process that follows the IRB
guidelines for the protection of human subjects in research studies (Creswell, 2007).
49
Chapter 3: Research Method
Introduction
The purpose of this quantitative comparison research study was to ascertain if statistically
significant differences exist between paper versus electronic copies of health records,
communication, and consumer satisfaction. The instrument, PSQ-08 Electronic Health Records
Survey, was the tool to collect data regarding the consumers’ perceptions of the implications of
EHR and how this affects the health care provider-consumer dynamic. The data collected from
this study could be beneficial for government agencies, insurance companies, and health care
professionals in promoting communication, community services, and training toward
encouraging consumer awareness and health care providers’ adoption of EHRs.
Chapters 1 and 2 provide the overview of the research study and the literature review as it
applied to EHRs and communication channels. Chapter 3 provides the details of the research
design and appropriateness, the population, data gathering techniques, the survey instrument, and
the data analysis. The discussion includes the validity and reliability of the research tool. The
conclusion of Chapter 3 summarizes these concepts and introduces Chapter 4.
Research Questions
The study instrument provides answers to the research questions and hypothesis. The
research questions are:
General Question: What is the difference between the format of health record used (electronic
versus paper) and the level of consumer satisfaction with care provided and communication with
provider?
RQ1: What is the relationship between the format of the health record (paper versus electronic
versus both) and the consumer satisfaction with care received?
50
RQ2: What is the relationship between the format of the health record used (paper versus
electronic versus both) and the level of satisfaction with communication between health care
provider and consumer?
RQ3: After controlling for consumer demographic characteristics (gender, age, education, and
race), what is the relationship between the format of the health record (paper versus electronic
versus both) and the consumer satisfaction?
RQ4: After controlling for consumer demographic characteristics (gender, age, education, and
race), what is the relationship between the format of the health record (paper versus electronic
versus both) and effect on communication?
The hypotheses are:
H10: There is no significant relationship between the health record format in paper, electronic or
both, and consumer satisfaction with communication and care received.
H1A: There is a significant relationship between the health record format in paper, electronic or
both, and consumer satisfaction with communication and care received.
H20: There is no significant relationship between the health record format in paper, electronic or
both, and level of communication between health provider and consumer.
H2A: There is a significant relationship between the health record format in paper, electronic or
both, and level of communication between health provider and consumer.
H30: There is no significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and consumer
satisfaction.
51
H3A: There is a significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and consumer
satisfaction.
H40: There is no significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and the level of
communication.
H4A: There is significant relationship between the health record format in paper, electronic or
both, based on demographic characteristic (gender, age, education, and race) and the level of
communication.
Research Method and Design Appropriateness
Either the qualitative or quantitative method would be appropriate for this study. The
basis for quantitative research strategy is hypothetical deduction and statistical data analysis. The
quantitative research approach uses various measurement tools to observe behavior, measure
attitudes, or interview an individual (Creswell, 2007). The quantitative method requires a
sampling that would provide sufficient data to be generalizable to the larger population
(Creswell, 2007).
The basis for qualitative research is a central phenomenon that a researcher seeks to
understand and explore with a specific audience and in a predetermined location (Creswell,
2007). Qualitative research uses insight, inference, evidence, and verification. Carlson (2008)
added that qualitative research is interpretive and includes introspection. Qualitative research
provides data from the human experience and allows for data collection through interviews,
observations, documented sources, and visual data.
52
The basis for the quantitative method selection was on the statistical data that could be
attained. The quantitative comparative study was appropriate as it provided a measurement
mechanism to understand consumer satisfaction when comparing the use of either paper or
electronic health records and how this may affect communication. The PSQ-08 Electronic Health
Records Survey provides the statistical data on the consumer view based on the research
questions and related hypotheses.
Research Design
A quantitative study using the comparative design provides data to compare attitudes,
opinions, or beliefs as it relates to the implementation of EHRs when compared to using paper-
based medical health records. Comparative research permits the understanding of social life by
comparing across settings and locations (Miller & Brewer, 2003). Comparative methods also
allow for the understanding of variations in “socially worthwhile practices, policies, and
institutions” (Miller & Brewer, 2003, para. 2). A quantitative comparative study aims at
determining the similarity or differences within two distinct groups (Creswell, 2007). Black
(1999) adds comparative studies compare two populations to see if there are similarities between
the populations or if they belong to a different population “based on the trait in question” (p.
403).
The quantitative comparative study was appropriate as it provided a measurement
mechanism to understand consumer satisfaction when comparing the use of either paper or
electronic health records and how this may affect communication. A cross-sectional survey is a
tool to collect statistical data. Cross-sectional surveys allow for collection of data during a
particular time frame, measure consumer attitudes, and measure community needs relating to the
electronic health record implementation. The survey includes questions regarding health care
53
provider-patient interaction and demographic information from participants, such as gender,
race, age, and educational level.
The basis for the survey questions is the Rand Corporation PSQ-18. The questions
measure general satisfaction, interpersonal manner, and communication based on the PSQ-18
questionnaire. The survey was available in paper copies and was distributed at the senior centers.
Sample Population
Testing everyone in the population can be impossible so that only a sample that is a
subset of the population is used in research. As noted by Salkind (2008), a population is a group
of potential participants where generalizability can provide sufficient information for the entire
population of the phenomenon of interest. As it would be time and cost prohibitive to engage the
entire population that may have access to medical records in either electronic or paper format,
the senior citizen residents of Hunterdon County, New Jersey, were the sample population.
The national implementation of health record digitization will affect the U.S. population,
so the assumption is made for the general population. As it is impossible to survey the general
population, the senior citizens in Hunterdon County, New Jersey, were the specific population.
A sample of this population surveyed was the senior citizen centers in Hunterdon County, New
Jersey.
According to the U.S. Census Bureau, the population in Hunterdon County for 2009 was
130,034 (Hunterdon County Facts & Figures, 2010). This population size could provide the
specific population for the generalization of results to the general population. Based on the
literature, it is expected that approximately 40% of physicians are using electronic health record
systems (Hing & Hsiao, 2010; Hsiao et al., 2010) in the United States. Based on this percentage,
it is expected there will be reasonable representation of participants who have access to
54
electronic health records within Hunterdon County, New Jersey. The sample of the population of
senior citizens in Hunterdon County, New Jersey, could provide sufficient data for a
generalization for the larger population.
Approximately 80 volunteers from the senior centers in Hunterdon County, New Jersey,
provided their views on the use of EHRs through a cross-sectional survey. The volunteers
provided diverse views based on gender, age, educational background, and race. The population
was a sample of the target population as a list provided from senior center administrators
(Creswell, 2007).
The calculation of the approximate sample size for the sample population for this study
referenced a formula recommended by Tabachnick and Fidell (2006). The recommendation for
the sample size is calculated using the following formula:
Sample Size = 104 + m
where m equals the number of independent variables.
Given that formula, the anticipated sample size for this study was between 110–115 senior
citizens. There were five independent variables that included health record format, gender, age,
education, and race and were the basis for the calculation noted by Tabachnick and Fidell for
regression testing.
The sample population were senior citizens using a convenience sample method.
According to Cooper and Schindler (2010), convenience samples provide no restrictions as
researchers can choose the population based on the convenience of engaging participants. The
volunteers from senior citizen centers were convenient to recruit and provided ideas about the
subject of interest (Cooper & Schindler, 2010).
55
Creswell (2007) noted a generalization of results can be accomplished using a small
population sample within a quantitative research approach. The smaller sampling size would be
analyzed to apply the general concept to a “cross section of people from all socioeconomic
levels” (Creswell, 2007, p. 48). This concept can be beneficial as sampling a larger group could
be time and cost intensive, but sampling a small group would allow for a generalization of the
tested population.
The participants for the study were senior citizens who are members of senior centers in
Hunterdon County, New Jersey. The demographics section for the survey contained a question
regarding the age confirmation. All participants were required to sign an informed consent form
that was part of the study package. All participant data were kept confidential.
Sampling Frame
The senior citizen volunteers were retired male or female participants who belong to
senior centers in Hunterdon County. The assumption was that the senior citizen volunteers were
a diverse group ranging from 60 and above years old and had access to health records based on
health concerns or needs. The sampling frame included male and female senior citizens but not
limited to any specific nationality, education level, income level, or profession.
The sample size of the population under study was a limiting factor as the population
only included senior citizens in Hunterdon County, New Jersey. The sample population provided
diverse perspectives, but may not represent the full scope of experiences related to the EHR use
and implementation. The sample population does not include non-English-speaking consumers,
and is limited to senior citizens who were part of a senior citizen center in Hunterdon County
that also limited the dimensions of the results.
56
Based on the literature, it was expected that approximately 40% of physicians were using
electronic health record systems (Hing & Hsiao, 2010; Hsiao et al., 2010). Based on this
percentage, it was expected that there would be reasonable representation of participants who
had access to electronic health records; however, data gathering continued until 40 to 50% of
respondents fit the criteria for sufficient data analysis.
Informed Consent
The survey process followed the IRB guidelines for the protection of human subjects in
research studies to protect study volunteers. The participant requirement to be a volunteer for the
study was to provide consent to participate. The consent form ensured cooperation and that
participants understood the purpose of the study (Creswell, 2007). See Appendix A for a copy of
the Informed Consent form.
Prior to the beginning of the study, each participant was informed of the purpose of the
research, the benefits in participating, such as contributing to the knowledge base of EHRs and
possible improvements to consumer communication. All volunteers were ensured that all
personal information would be kept confidential. The removal of any identifying information
ensured the confidentiality of all participants.
The participants could withdraw at any time during the study. The withdrawal process
during the study required the participants to verbally express their wish to withdraw from the
study. Any information gathered would be shredded to ensure confidentiality.
The researcher contact information was provided to the participants should there be any
questions regarding the survey or study questions. After the data collection was complete, if the
volunteer decided to withdraw from the study, the researcher could be contacted via email or
57
telephone. The survey related to this participant would not be used and would be shredded to
ensure confidentiality.
The Informed Consent form was provided as part of the survey package. The survey
package included the introduction to the survey, the Informed Consent form, and the survey
instrument. Participants acknowledged the Informed Consent form by providing a signature on
the form to acknowledge consent. The signed consent forms are stored in a secured metal
container with access limited to the researcher. The data collected will be destroyed after six
years from the date of the study.
The study volunteers had the right to decide to participate in the research study. The
senior centers provided classroom-type activities where the researcher was given permission to
present the research details to seniors enrolled in high-participation classes. A list of classes was
provided to the researcher at the start of the study. Participants were informed of the researcher’s
presence by the senior citizen center’s personnel.
The senior citizen volunteers were asked to sit through a brief presentation of the study
topic, the objective of the study, the survey requirements, and the process for withdrawing from
the study. The survey was administered after the presentation and the surveys collected during
this time by the researcher. The participants were treated with respect and were guaranteed
confidentiality. The withdrawal process was explained, and the opportunity for any volunteer to
withdraw was honored at any time during the survey administration.
Confidentiality involves the individual’s rights to have control over the use and access of
personal information. Confidentiality also provides the expectation of privacy and protection of
personal information (Marczyk, DeMatteo, & Festinger, 2005). All study volunteers who wish to
withdraw from the survey were treated with respect, their wishes honored, and the survey
58
instrument shredded. The volunteers were required to state their preference to withdraw, the
survey instrument was shredded upon notification, and the participant was excused from the
senior citizen class. The survey was not to be part of the data analysis had a participant
withdrawn from the research study.
Confidentiality
All study participants were guaranteed confidentiality, as noted in the Informed Consent
form. The consent form had a signature line, but the information was not part of the final study
results. The hosting of signature forms is in a secure location and protected under lock and key at
the researcher’s home office. Access to the data collected is limited to the researcher.
All study participants were given the opportunity to withdraw from the study at any time.
The Informed Consent form noted that a participant may decline to participate or withdraw from
participation at any time without consequence. The request was honored by the researcher, and
all data collected from the individual asking to withdraw was immediately destroyed.
Geographic Location
The geographic location of the sample was Hunterdon County, New Jersey. Senior
citizens from local senior centers were a sample of the general population. According to the U.S.
Census Bureau, the population in Hunterdon County for 2009 was 130,034 (Hunterdon County
Facts & Figures, 2010). This population size could provide sufficient volunteers for the
generalization of result to the general population.
Data Collection
The dependent variables were consumer satisfaction and communication. The
independent variables were the demographic characteristics (gender, age, education, and race)
and the format of medical records (paper or electronic). Maheu et al. (2001) noted quantitative
59
research requires the research variable be measured numerically and uses closed-ended surveys
to collect data. The data collection process should allow for reliability, validity, responsiveness,
interpretability, and flexibility (Maheu et al., 2001).
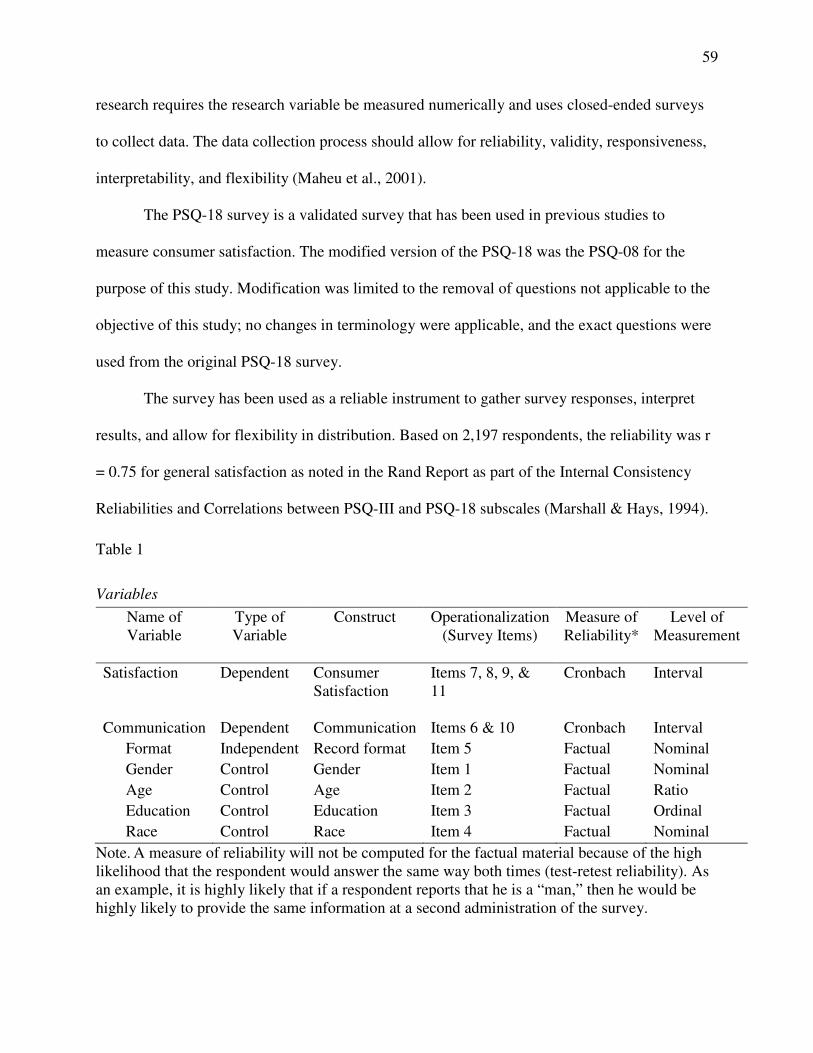
The PSQ-18 survey is a validated survey that has been used in previous studies to
measure consumer satisfaction. The modified version of the PSQ-18 was the PSQ-08 for the
purpose of this study. Modification was limited to the removal of questions not applicable to the
objective of this study; no changes in terminology were applicable, and the exact questions were
used from the original PSQ-18 survey.
The survey has been used as a reliable instrument to gather survey responses, interpret
results, and allow for flexibility in distribution. Based on 2,197 respondents, the reliability was r
= 0.75 for general satisfaction as noted in the Rand Report as part of the Internal Consistency
Reliabilities and Correlations between PSQ-III and PSQ-18 subscales (Marshall & Hays, 1994).
Table 1
Variables
Name of Variable
Type of Variable
Construct Operationalization (Survey Items)
Measure of Reliability*
Level of Measurement
Satisfaction Dependent Consumer Satisfaction
Items 7, 8, 9, & 11
Cronbach Interval
Communication Dependent Communication Items 6 & 10 Cronbach Interval
Format Independent Record format Item 5 Factual Nominal
Gender Control Gender Item 1 Factual Nominal
Age Control Age Item 2 Factual Ratio
Education Control Education Item 3 Factual Ordinal
Race Control Race Item 4 Factual Nominal
Note. A measure of reliability will not be computed for the factual material because of the high likelihood that the respondent would answer the same way both times (test-retest reliability). As an example, it is highly likely that if a respondent reports that he is a “man,” then he would be highly likely to provide the same information at a second administration of the survey.
60
The survey used a 5-point Likert scale (5 = Strongly Agree, 1 = Strongly Disagree)
to measure consumer satisfaction based on the format of health record. The analysis used
descriptive statistics. Creswell (2007) noted descriptive statistics assist in summarizing the trends
in the data, provides the understanding of the variation of the scores, and provides insight into
where a score falls in comparison to other scores.
Study Instrument
The study instrument was a cross-sectional survey based on a publicly available and
previously validated questionnaire: the Rand Corporation PSQ-18. The selection of the
questionnaire was on the applicability to the quantitative comparative study and the ease of
administration. The questionnaire was the tool to measure how the consumer perceived his/her
interaction with health care providers, but only the specific sections related to consumer
satisfaction were applicable. See Appendix B for a copy of the survey instrument. Other
instruments available such as the Patient Assessment of Care for Chronic Conditions (PACIC)
were not considered due to the lack of focus on consumer satisfaction. The PSQ-18 specifically
measures consumer satisfaction in the context of interaction with the health care provider.
The PSQ-18 is a shortened version of a 50-item Patient Satisfaction Questionnaire III
developed by Ware, Snyder, and Wright in 1976 (Marshall & Hays, 1994). The PSQ-18 is set up
to measure seven dimensions of medical care satisfaction that include general satisfaction,
technical quality, interpersonal manner, communication, financial aspects, time spent with
doctor, and accessibility and convenience using 18 questions. Only three dimensions of the
questionnaire related to the parameters of the study hence were the basis for the survey
questions. Questions regarding technical quality, financial aspects, and accessibility and
61
convenience of the medical visit were not relevant to the parameters of this study. The PSQ-08
referred to these areas of interest.
The PSQ-18 as a subset of the PSQ has been used in various studies for planning,
administration, and evaluation of health services delivery program (Marshall & Hays, 1994). The
questionnaire is a survey tool to measure patient satisfaction and has gone through several
revisions. The PSQ-08 was appropriate in this study as it provided the questions to measure
consumer attitudes toward the use of EHRs. The questions that related to general satisfaction,
interpersonal manner, communication, and time spent with doctor aligned with the goals of the
quantitative comparative study.
Questions selected from the PSQ-18 were in both the positive and negative form to
account for acquiescent responses. The questions related to the medical services recently
received but were not limited to any specific timeframe. The questions were based on the
consumer’s interaction with their primary health care provider. The survey used a 5-point Likert
scale (5 = Strongly Agree, 1 = Strongly Disagree). The survey also contained questions on
demographics and type of health record used (e.g., paper, electronic, or both).
Study Pilot Testing
McMillan and Schumacher (2010) noted after the questions for a survey have been
written, the survey should be tested to check for bias. Bias can be through the procedures, the
interviewers, or the questions. The PSQ-18 has been used numerous times to measure consumer
satisfaction and has been validated and proven reliable (Bhardwaj et al., 2011; Marshall & Hays,
1994; Vrijhoef et al., 2009). A pilot test was not necessary for the purposes of this study as the
questions selected were directly taken from the PSQ-18 questionnaire, hence previously tested.
62
Validity and Reliability
Chaloupke (2007) stated statistical “precision of measurement of any kind of
phenomenon has two aspects: reliability and validity” (p. 1295). Powell (2006) defined reliability
as the degree in which an instrument can consistently and accurately repeat results in each use
where validity is the degree in which the instrument does what it is supposed to do. Maheu et al.
(2001) added the determination of internal validity is the data collection process. Issues with
internal validity relate to research bias and problems with sample population.
To maximize the internal validity of the study, different study designs and strict control
processes need to be in place throughout the research process. External validity relates to the
generalization of study results across population, location, and time. Random sampling,
heterogeneous sampling, population selection that would be generalizable, and long-term
research can be effective to avoid issues with external validity (Maheu et al., 2001).
M. D. Gall, J. P. Gall, and Borg (2006) noted 12 threats to the external validity of a
research study. These include: (a) the extent to which one can generalize from the experimental
sample to a defined population; (b) the extent to which personological variables interact with
treatment variables; (c) explicit description of the experimental treatment; (d) multiple-treatment
RQ1: What is the relationship between the format of the health record (paper versus electronic versus both) and the consumer satisfaction with care received?
Record Format (item 5), Satisfaction, (items 7, 8, 9, & 11-13)
One way ANOVA, eta coefficient
F, η2 H10: There is no
significant relationship between the health record format in paper, electronic or both and consumer satisfaction with communication and care received. .
RQ2: What is the relationship between the format of the health record used (paper versus electronic versus both) and the level of satisfaction with communication between health care provider and consumer?
Record Format (item 5), Communication (items 6 & 10)
One way ANOVA, eta coefficient
F, η2 H20: There is no
significant relationship between the health record format in paper, electronic or both and level of communication between health provider and consumer.
66
RQ3: After controlling for consumer demographic characteristics (gender, age, education, and race) what is the relationship between the format of the health record (paper versus electronic versus both) and the consumer satisfaction?
Gender, Age, Education, Race (items 1 – 4) Record Format (item 5) Satisfaction (items 7, 8, 9, & 11)
Standard Multiple Regression
F, R2 H30: There is no
significant relationship between the health record format in paper, electronic or both based on demographic characteristic (gender, age, education, and race) and consumer satisfaction.
RQ4: After controlling for consumer demographic characteristics (gender, age, education, and race), what is the relationship between the format of the health record (paper versus electronic versus both) and effect on communication?
Gender, Age, Education, Race (items 1 – 4) Record Format (item 5) Satisfaction (items 6 & 10)
Standard Multiple Regression
F, R2 H40: There is no
significant relationship between the health record format in paper, electronic or both based on demographic characteristic (gender, age, education, and race) and the level of communication.
Note. For all test p < .05 is the chosen level of Statistical Significance.
The reporting of the data were through tables for a visual representation. The
analysis of the data obtained from the survey instrument was done using the Statistical Package
for the Social Sciences (SPSS) tool.
Chapter Conclusion
Quantitative comparative research measures attitudes toward a particular topic, allows a
direct comparison between paper copy and electronic health records and how the format may
affect communication and consumer satisfaction. Chapter 3 described the research method and
67
design for the quantitative comparative study on the consumer’s view on the implementation of
EHR systems. The discussion included the appropriateness of the research approach. To
accomplish the goals of the study, the sample population was senior citizens in Hunterdon
County, New Jersey, attained through a convenience sampling. The survey instrument used the
PSQ-08 questions that allowed the measurement of consumer’s view on health care provider-
consumer interaction, the use of medical records and technology, as well as the ease of use of
EHRs. The PSQ-18 questionnaire has been utilized previously in studies for the use of medical
records, patient satisfaction, and communication (Bhardwaj et al., 2011; Marshall & Hays, 1994;
Vrijhoef et al., 2009). The PSQ-08 survey was modified to use specific questions to meet the
objectives of this study.
Summary
The next chapter will present the findings and data analysis of the consumer views on
how consumers perceive their interaction with health care providers and how the format of health
records may affect the health care provider-consumer dynamic. Chapter 4 will present the details
of the quantitative comparative study, the data collection process, and data analysis procedures.
68
Chapter 4: Results
Chapter 4 contains the analysis of the data gathered through this research study. The
purpose of this quantitative comparative research study was to ascertain, if statistically
significant, differences existed between the format of health records (electronic versus paper)
and the level of consumer satisfaction with care provided and communication with provider. The
study used data focused on satisfaction and communication utilizing the PSQ-08, Electronic
Health Records Survey.
The first three chapters provided the overview of the research study, the literature review,
and the research method as they applied to the purpose of this quantitative comparative research
study. Chapter 4 provides the demographics of the participants, data analysis procedure, and
presentation of findings. The conclusion of Chapter 4 will summarize these concepts and
introduce Chapter 5.
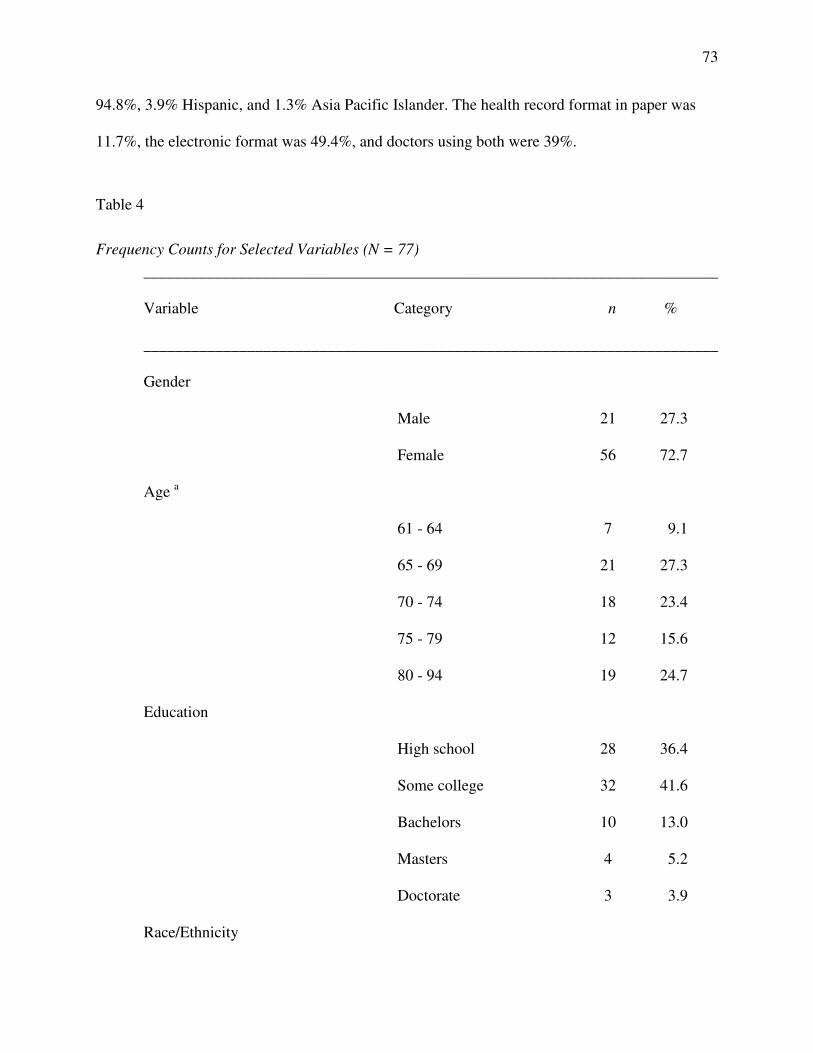
Demographics
The introduction and informed consent forms were distributed to (n=110) study
participants. Data was collected using a cross-sectional survey. Of the 110, (n=80) returned the
signed informed consent and a group of (n=77) responded to the PSQ-08. The final sample size
of respondents (n=77) was the core group for the data analysis.
Data Collection
This section describes the data collection procedure for this quantitative comparative
research study. Data collection and analysis began after the Academic and Internal Review
Boards of the University of Phoenix approved the current research study. The PSQ-08 survey
instrument was used to gather research data. The PSQ-08 specifically measures consumer
satisfaction in the context of interaction with the health care provider.
69
The PSQ-08 based on the PSQ-18 used is a well-established, approved, and tested survey
instrument. A pilot study was not conducted, as the PSQ-18 has been used numerous times to
measure consumer satisfaction. The PSQ-08 used 8 of the original 18 questions used in the PSQ-
18. Topics discussed were data collection methods, recruitment, and planning and procedure.
Additionally, data analysis was discussed.
The quantitative method was a comparative research design. This current research study
did not statistically identify a relationship between health record format and the consumer
satisfaction with care received. The results of the one way ANOVA test for satisfaction showed
no significant difference between the groups (F (3, 73) = 0.73, p = .49, reference Table 5). The
covariance model predicting consumer satisfaction based on demographic characteristics was not
significant (F (5, 71) = 0.72, p = .61, reference Table 8). This current research study also did not
statistically identify a relationship between health record format and the effect on communication
between health care provide and consumer. The results of the one way ANOVA test for
communication showed no significant difference between the groups (F (3, 73) = 1.79, p = .18,
reference Table 6).The covariance model predicting consumer communication based on
demographic characteristics was not significant (F (5, 71) = 2.08, p = .08, reference Table 10).
The chosen level of significance for all tests was p < .05.
Recruitment
In compliance with the regulations of the IRB, all participants were made aware of the
purpose of the research study, risks, and benefits in participating in this research study.
Participants were informed of the possible benefit of contributing to the knowledge base of
leadership and the implementation of electronic health records. The random selection of
volunteers from high participation classes at the Hunterdon County Senior Center was the
70
approach used to obtain the sample population. The Director of Senior Center Activities
provided a calendar and highlighted high participation classes where there would be a greater
potential for volunteers. A date and time were arranged for access to the various classes, and
team leaders were informed of the procedure for recruiting volunteers. The Informed Consent
forms and survey instrument were distributed on a predetermined date, time, and class schedule.
Planning and Procedure
The Informed Consent forms advised participants of the purpose of the research study
and addressed the risks and benefits in participating in this study. The Informed Consent forms
and the survey instrument were initially distributed to the Hunterdon County Senior Center
Division Head and the Director of Senior Center Activities for their review. A planning meeting
was scheduled two weeks prior to distribution to the members of the Hunterdon County Senior
Center.
The planning meeting addressed the procedure for survey distribution to include a brief
introduction at the beginning of each class by the team leader, recruitment of volunteers, and
requirement for survey distribution to be conducted after the classes were concluded. A calendar
of classes was provided with a list of classes that would provide the greatest possible number of
volunteers. The date was set for survey distribution, and a point of contact was established.
The survey collection time spanned two weeks. Participants were advised that personal
identifying information would be kept confidential. Participants were also advised of their right
to withdraw from the study at any point either before, during, or after survey distribution. The
process to withdraw from the study was included in the Informed Consent form.
Participants who wished to withdraw before, during, or after data collection was
completed could initiate the withdrawal process by contacting the researcher in person, by
71
cellphone, or by email. Upon notification, the collection of information from the participant to
identify data collected would be destroyed from the assessment results.
The participant received a package that included two copies of the Informed Consent
form (Appendix A) and the survey instrument (Appendix B). Participants were instructed to sign
one copy of the Informed Consent form and return to the researcher, and the other copy was for
their records. The package was numbered sequentially so that if needed, the survey can be
tracked to the Informed Consent form. Only signed Consent Forms and associated surveys were
considered for final data analysis.
The signed Consent Forms are locked in a filing cabinet in the researcher’s home. The
data collected will be destroyed after six years from the date of the completion and study to be
accepted. Participants’ confidential information that is limited to a signature was not disclosed
for any data-reporting purposes. The participants’ copy of the Informed Consent form provided
the researcher’s contact information to include cellphone number and email address.
Data Analysis Procedures
The research questions described in Chapter 3 guided this quantitative comparative
research study that determined the relationship between health record format, consumer
satisfaction, and the impact on communication. The data collection transpired as described in the
Nature of the Study section in Chapter 1 and the method section in Chapter 3. The analysis of the
data obtained from the survey instrument was done using the SPSS tool.
The data were analyzed using standard psychometric characteristics for the dependent
variables, and frequency counts for the independent variables. Research Questions 1 and 2 were
analyzed using one way ANOVA test and accompanying eta coefficients. For Research
Questions 3 and 4, analysis of covariance models was created.
72
Presentation of Findings
Table 3 displays the psychometric characteristics for the satisfaction and communication
scale scores. Mean satisfaction scores was M = 3.74, while the mean for communication was M =
3.92. The Cronbach alpha reliability coefficients were α = .83 for the satisfaction score and α =
.61 for the communication score. The typical rule of thumb for acceptable levels of internal
reliability is α ≥ .70 (Vogt, 2007). This level was achieved for the satisfaction score but not for
the communication score. Low levels of internal reliability are common when the scale score
only includes two items as is the case for the communication scale (Vogt, 2007).
Table 3
Psychometric Characteristics for Summated Scale Scores (N = 77)













































































































![Ancient history [by D.M. Masson]....Title Ancient history [by D.M. Masson]. Author David Mather Masson](https://static.documents.pub/doc/80x56/60ec6d4334ac5766a325c5a1/ancient-history-by-dm-masson-title-ancient-history-by-dm-masson-author.jpg)