A Radiological Evaluation of Radiol ucent Cages Containing Autogenous B one Graft or Bovine Hydroxyapatite (BH) in Cervical Fusion: a Retrospe ctive Study in 46 Consecutive Patie nts Wei-Chieh Chang , Hsi-Kai Tsou, Wen-Shian Chen ¹, Chi-Chang Chen ¹,Ting-Hsien Kao, Chiung-Chyi Shen Department of Neurosurgery, Taichung Veterans General Hosp ital, Taiwan ¹Department of Radiology, Taichung Veterans General Hospit al, Taiwan
Transcript
A Radiological Evaluation of Radiolucent Cages Containing Autogenous Bone Graft or Bovine Hydroxyapatite (BH) in Cervical Fusion: a Retrospe
Department of Neurosurgery, Taichung Veterans General Hospital, Taiwan
¹Department of Radiology, Taichung Veterans General Hospital, Taiwan
Purpose: Anterior cervical discetomy and fusion (ACD
F) with PEEK cages are widely used as the surgical treatment of cervical spondylosis.
Cages containing cancellous bone can improve the bony fusion. However, donor site pain is still the major problem.
Hydroxyapatite graft is then introduced as substitute materials. The authors investigated the radiological results in cervical fusion with radiolucent cages between cancellous bone and bovine hydroxyapatite graft.
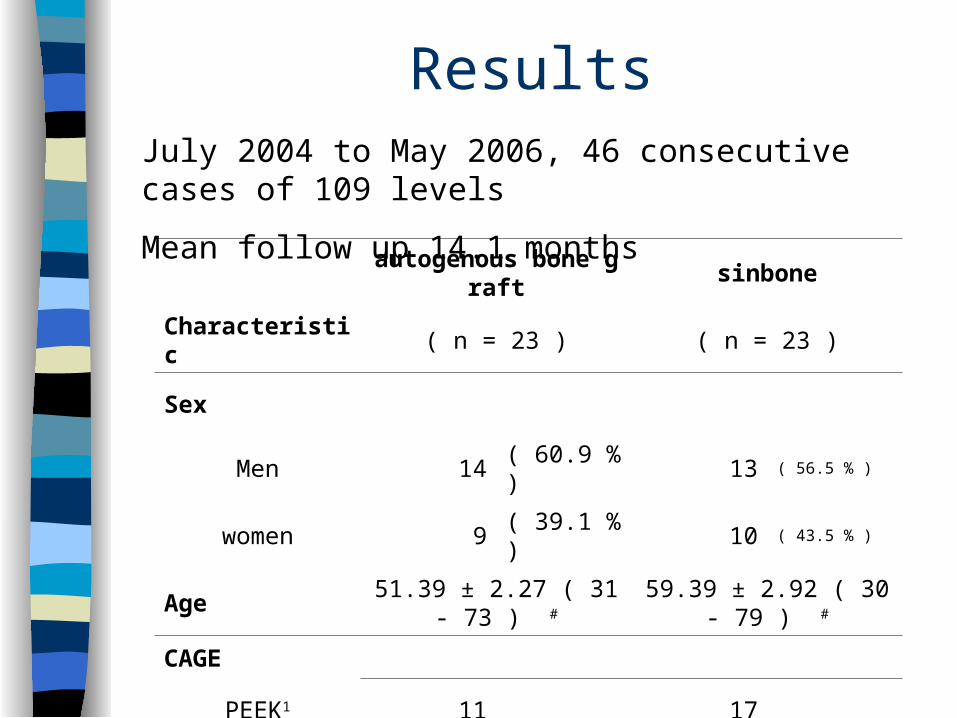
Materials and Methods: From July 2004 to May 2006, there wer
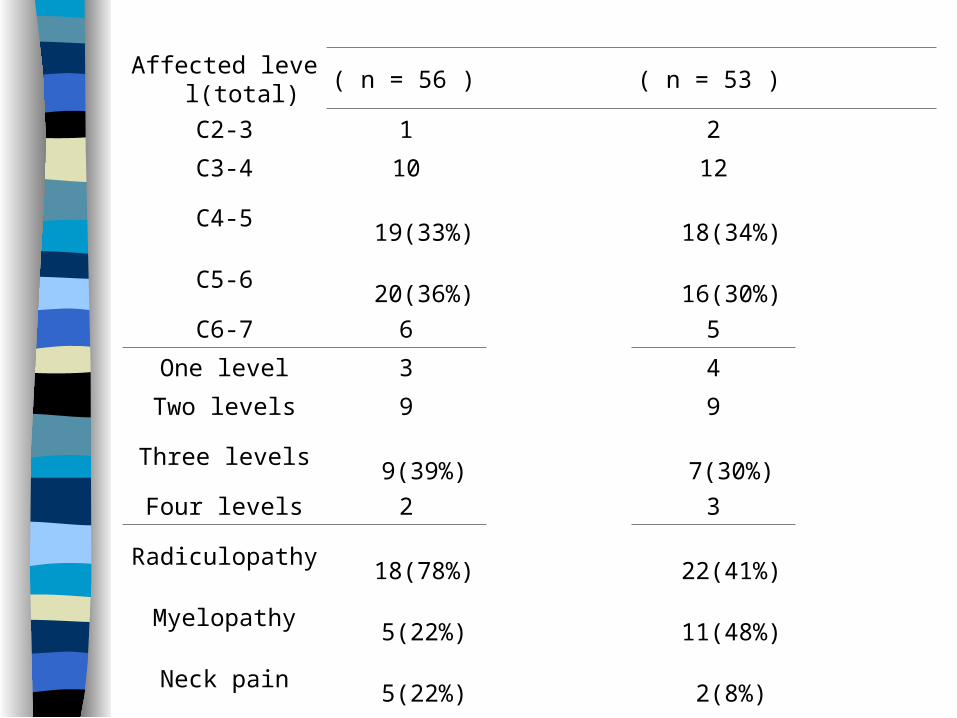
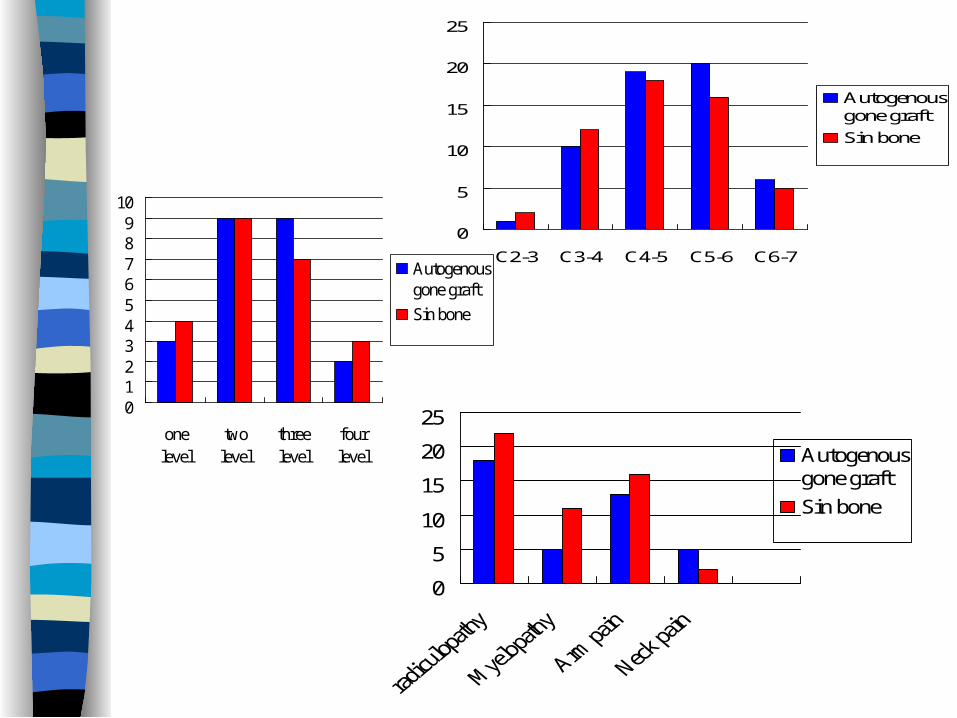
e 46 consecutive cases of 109 levels of cervical degenerative disease between C2 and C7.
A retrospective analysis of cage fillers were divided into two groups: Group A (23 patients with 56 levels) packed with bone marrow and group B (23 patients with 53 levels) packed with bovin hydroxyapatite graft.
Surgical procedure: Smith-Robinson right side and anterior lateral approach followed by neck collar 8-12 weeks
Radiological results were evaluated by two neuroradiologists blinded to any clinical data.
Bone fusion was defined by the presence of bony trabeculation across the graft-host interfaces
The Prolo scale and Odom’s criteria : economic and functional status
The fusion was evaluated at intervals of 4, 12 and 24 weeks.
Patients inclusion criteria:
>Failure in conservative therapy -- traction, physical or chiropractic therapy, radiofrequency and pharmacotherapy
Surgical levels :
>Neurologic deficits correlated with MRI and/or EMG/NCV findings
ResultsJuly 2004 to May 2006, 46 consecutive cases of 109 levels
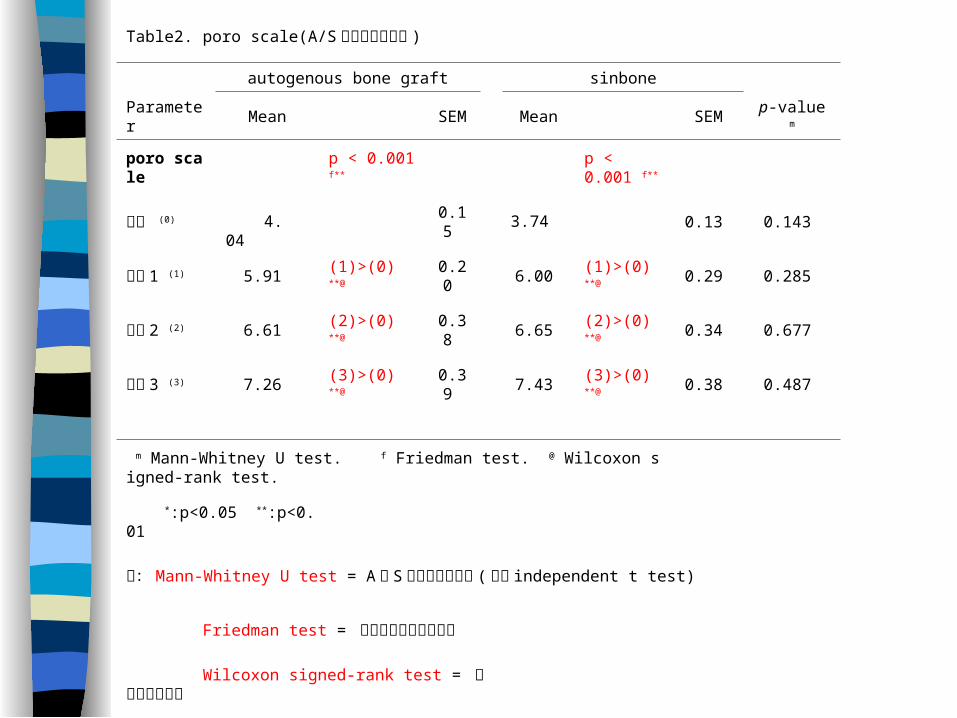
m Mann-Whitney U test. f Friedman test. @ Wilcoxon signed-rank test.
*:p<0.05 **:p<0.01
註:Mann-Whitney U test = A與 S兩組之比較差異 (類似 independent t test)
Friedman test = 四組術前術後之總比較
Wilcoxon signed-rank test = 術前術後兩兩較
4.04 3.74
Month
baseline 1 3 6
Sco
re
3
4
5
6
7
8
9
autogenous bone graftsinbone
**
**
**
Fusion
1. Two neuroradiologists blinded with clinical data
2. Post-op, 4 weeks, 12 weeks and 24 weeks
3. Lateral view of X-Ray
4. Osseous trabecular bone across the interface, trabecular bridging bone formation at the anterior and/or posterior cortex of the involved vertebral bodies, lucencies between cage and vertebral plates
Mrs Ju, 44 F, nuchal pain with radiating to right arm and lower limbs weakness for 6 months
CSMR, C3/4/5/6
1 M
4M fusion
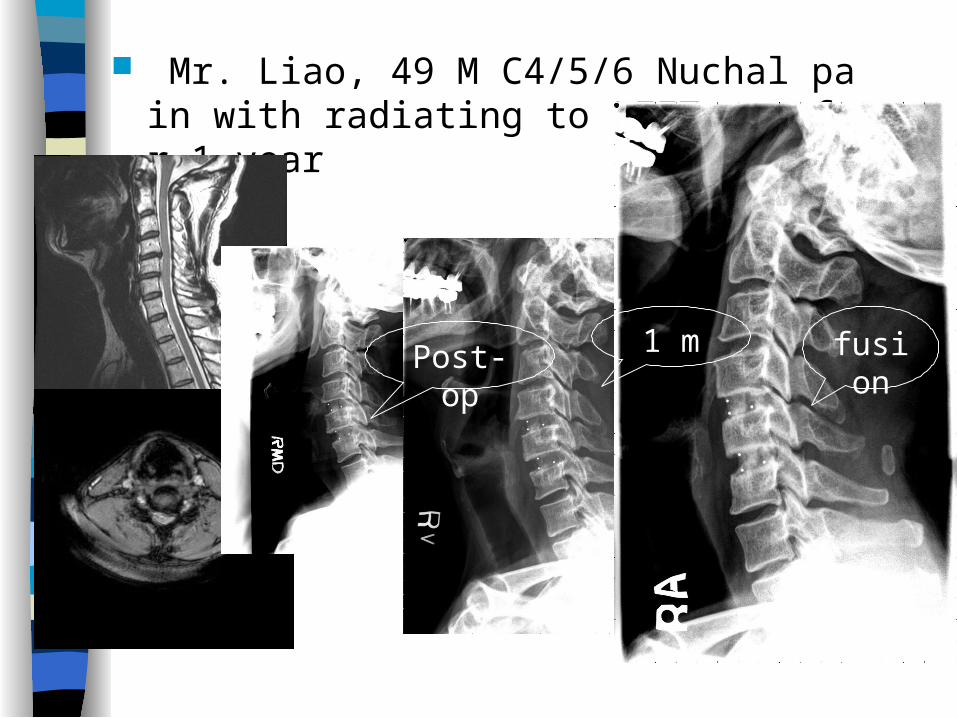
Mr. Liao, 49 M C4/5/6 Nuchal pain with radiating to LEFT arm for 1 year
fusion
1 mPost-op
Mr. Yang, 64 M, C3-4, 6-7 CSMR, progressive nuchal pain with radiating to upper arms and lower limbs weakness for 2 years
Post-op
1 MFusion
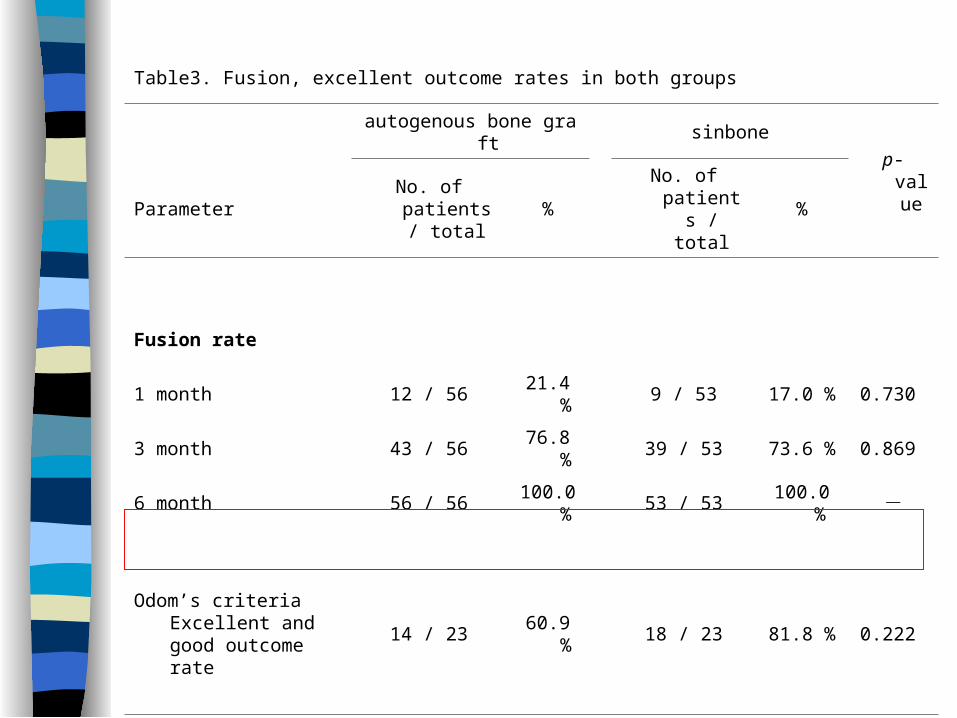
Table3. Fusion, excellent outcome rates in both groups
autogenous bone graft sinbone
p-valueParameter
No. of patients / total
% No. of patients /
total%
Fusion rate
1 month 12 / 56 21.4 % 9 / 53 17.0 % 0.730
3 month 43 / 56 76.8 % 39 / 53 73.6 % 0.869
6 month 56 / 56 100.0 % 53 / 53 100.0 % -
Odom’s criteria Excellent and good outcome rate
14 / 23 60.9 % 18 / 23 81.8 % 0.222
Yate's correction of contigency is used.
Complications
Autogenous bone graft
Sin bone
Iliac crest morbidity
Pain 18 0
Hematoma 1 0
Infection 0 0
Nerve injury 0 0
Interbody fusion
Breaking 0 0
Pull out 0 0
Subsidence 0 0
Pseudo-arthrosis 0 0
Re-open 1 0
Discussion Anterior approach to the cervical spine Cloward ( J. Neurosurg 15:602-16 ,1958),
Smith and Robinson (J. Bone Joint Surg Am 44:1569-87, 1962 )
Kyphotic angulation, narrowing foramina, loss normal sagittal alignment >> fusion
Waters and Levinthal (Spine 19:2343-7, 1994) fusion with iliac crest bone graft
Cages: immediate stability, resist axial displacement, minimize neck pain, maintain foraminal height and alignment, no donor site pain
Threaded titanium cage, polyestherstherketone (PEEK) cage, carbon fiber reinforced polymer (CFRP) cage containing autogenous bone graft for osteoconduction and osteoinduction, the mean time of fusion is less
Reduce the complication rate by 22% in comparison with autogenous iliac crest graft fusion --J Spinal Disord 13:511–514, 2000.
The PEEK cage is therefore a good substitute for AICG fusion in patients with cervical disc disease. --Neurosurgery 51:1343-1350, 2002
Radiolucent cage: similar elasticity behavior, no MR signal distortion in follow-up, evaluation in fusion
Sinbone® (Purzer, TWN) : Ceramic from bovine cancellous bone:Ca10(PO4)6(OH)2
Osteoinductive factors: osteoblast progenitor cells – periosteum, peritrabecular connective tissue and bone marrow ~J Cell Biocem 1994, 56:283-94
Osteoprogenitor cells were significantly more abundant in the iliac. It is advisable that iliac crest bone marrow would enhance vertebral interbody fusion. - Eur Spine J 2005, 14:645-8
In most studies, the cages were filled with autogenous bone taken from the iliac crest
~Acta Neurochir 1998 140:1-8
Radiolucent cage containing BH
The fusion rate is better in group A (21.4%) then in group B(17%) in first month (No statistical significant p=0.73) No difference in six months after OP
Poro scale: No statistical significant in pre-op, post-op 4,8 and 12 weeks between both groups
Odom’s criteria excellent and good outcome rate (group A: 60.9%, group B: 81.8%, p=0.22). >> Myelopathy: Group A/B: 22%/48% >> Donor site pain: Group A/B: 78%/0%
Conclusion
Hydroxyapatite is a good substitute material as a cage filler
There were no donor site complications The cervical fusion rate, postoperative Poro s
cale and Odom’s criteria had no difference. Extended studies on these patient are indicat
ed and are currently underway in our surgical group.