A RETROSPECTIVE STUDY ON LOWER EXTREMITY AMPUTATION LEVELS FOLLOWING ENDOVASCULAR REPERFUSION: AN INSTITUTIONAL REVIEW OF PODIATRIC MANAGEMENT IN THE LIMB SALVAGE TEAM Tyler Wishau, DPM; Jesse Wolfe, DPM; Matt Van Natta, MPH; Allen Jacobs, DPM, FACFAS; Robert Fischer, MD Sundeep Das, MD, FAAC; H. John Visser, DPM, FACFAS, FACFAO
Transcript
A RETROSPECTIVE STUDY ON LOWER EXTREMITY AMPUTATION LEVELS
FOLLOWING ENDOVASCULAR REPERFUSION: AN INSTITUTIONAL
REVIEW OF PODIATRIC MANAGEMENT IN THE LIMB SALVAGE TEAM
Tyler Wishau, DPM; Jesse Wolfe, DPM; Matt Van Natta, MPH; Allen Jacobs, DPM,
FACFAS; Robert Fischer, MD
Sundeep Das, MD, FAAC; H. John Visser, DPM, FACFAS, FACFAO
INTRODUCTION
• CLI patients are at risk for limb loss and potentially fatal complications from progression of gangrene
and development of sepsis.1
• Leg amputation due to PAD gives rise to 5-year survival rate of less than 30%.2
• Improvements in the process of early detection and appropriate treatment of patients with CLI are
warranted.
1. Lumsden A, Davies M, Peden E. Medical and endovascular management of critical limb ischemia. J Endovasc Ther. 2009; 16(Suppl II):II31-1162.
2. Anahita D, Cheong LJ, Epidemiology of peripheral arterial disease and critical limb is ischemia. Tech Vasc Interventional Rad 2016; 19:91-95.
INTRODUCTION
• Multiple studies have demonstrated a reduction in both amputation and mortality
among individuals diagnosed with CLI through instituting
multidisciplinary limb-salvage teams.
Sanders L, Robbins J, Edmons M. History of the team approach to amputation prevention: Pioneers and milestones. J Vasc Surg. 2010; 52:3S-16S
Rogers L, Andros g, Caporusso J, et al. Toe and flow: Essential components and structure of the amputation prevention team. J Vasc Surg. 2010; 52:23S-7S.
Kim P, Attinger C, Evans K, et al. Role of the podiatrist in diabetic limb salvage. J Vasc Surg. 2012;56:1168-72.
Chung J, G, Ahn C, et al. Multidisciplinary care improves amputation-free survival in patients with chronic critical limb ischemia. J Vasc Surg. 2015;61:162-9.
Driverr V, GModrall oodman R, Fabbi M, et al. The impact of a podiatric lead limb preservation team on disease outcomes and risk prediction in the diabetic lower extremity.
Limb Salvage Team
Vascular
Surgeons
Infectious Disease
Endocrinology
Podiatric
Surgeons
Interventional Radiology
Cardiology
PURPOSE
• Better understand the importance of podiatry in the limb salvage team, and to
identify a correlation of amputation levels status post endovascular treatment with
and without podiatry involvement.
Limb Salvage Team
Vascular
Surgeons
Infectious Disease
Endocrinology
Podiatric
Surgeons
Interventional Radiology
Cardiology
METHODS
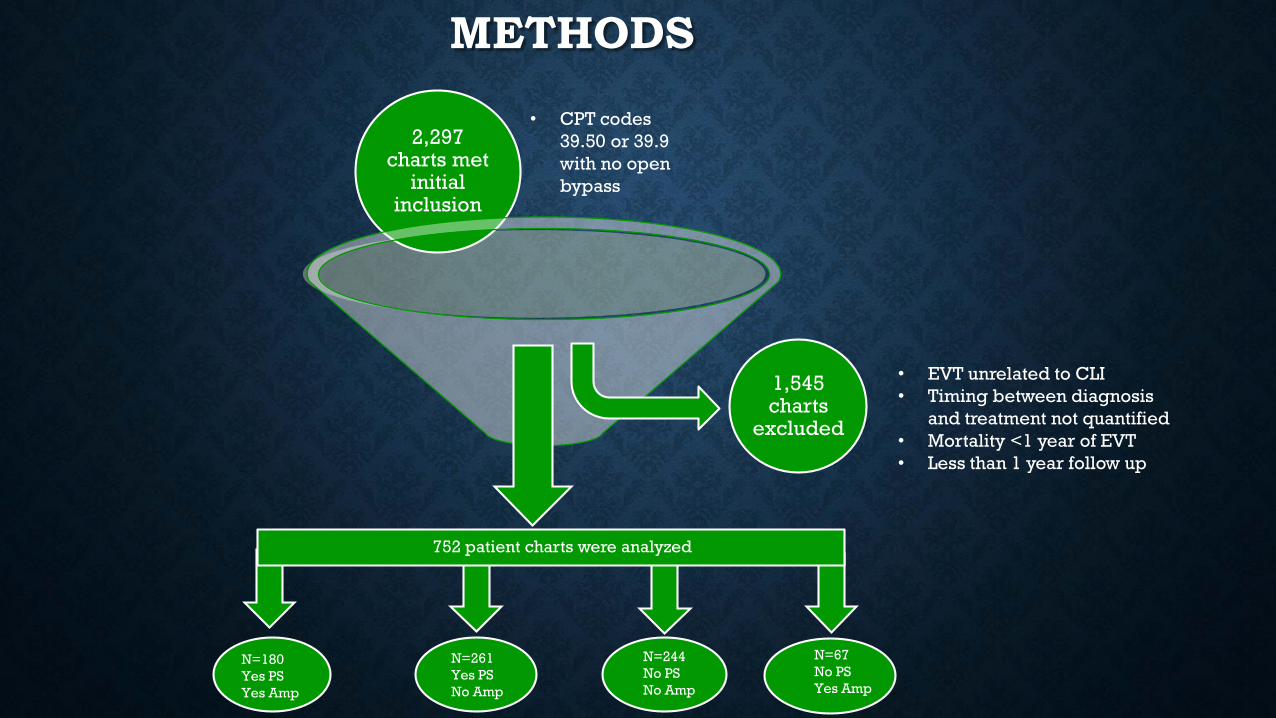
• Following IRB approval, a multi-center retrospective chart review was conducted
using CPT codes 39.50 and 39.90 defining non-coronary angioplasty/stenting.
• CLI risk factors (ICD-9 codes):
• Diabetes (250 – 250.99)
• Smoking (V15.82, 305.1)
• History of renal disease (443.9)
• Other demographics and risk factors will be identified and assessed for multivariate
Hingorani A, LaMuraglia G, Henke P, et al. The management of diabetic foot: A clinical practice guideline by the Society for Vascular Surgery in collaboration with the
American Podiatric Medical Association and the Society for Vascular Medicine. J Vasc Surg. 2016; 63:3S-21S.
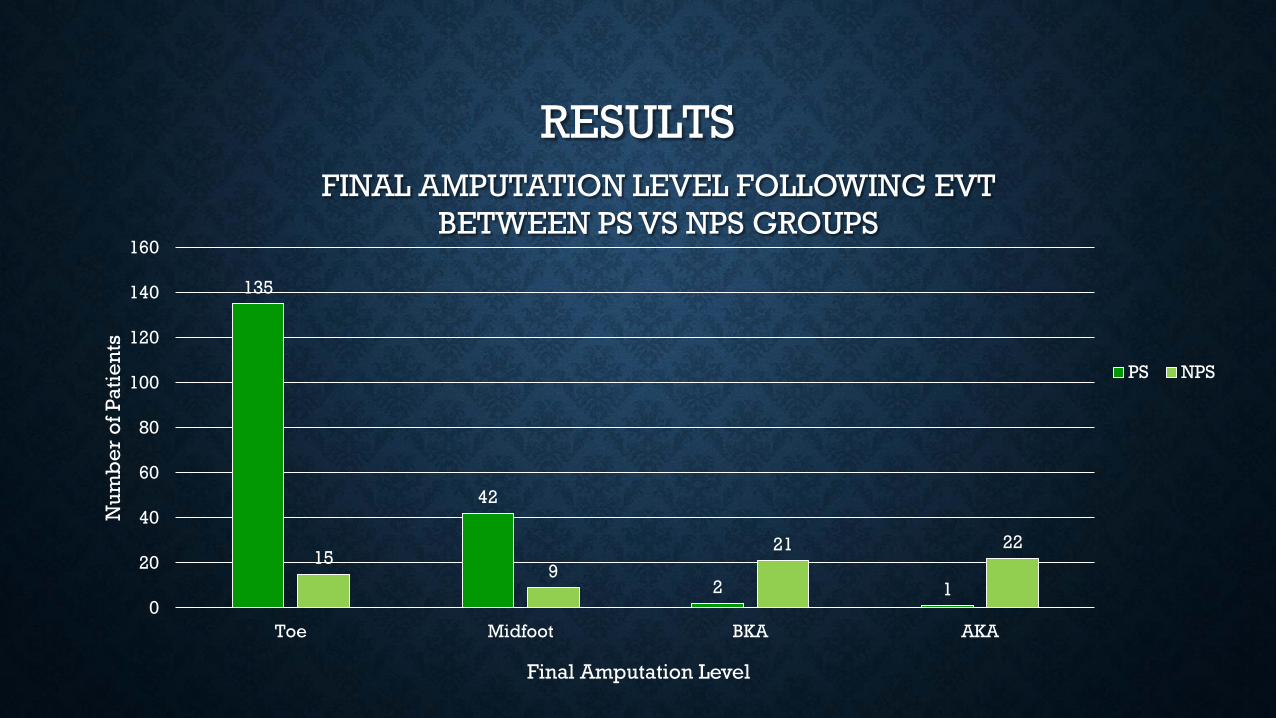
CONCLUSION
• A minor final amputation level correlated to PS consultation in patients status post
EVT compared to patients without PS consultation
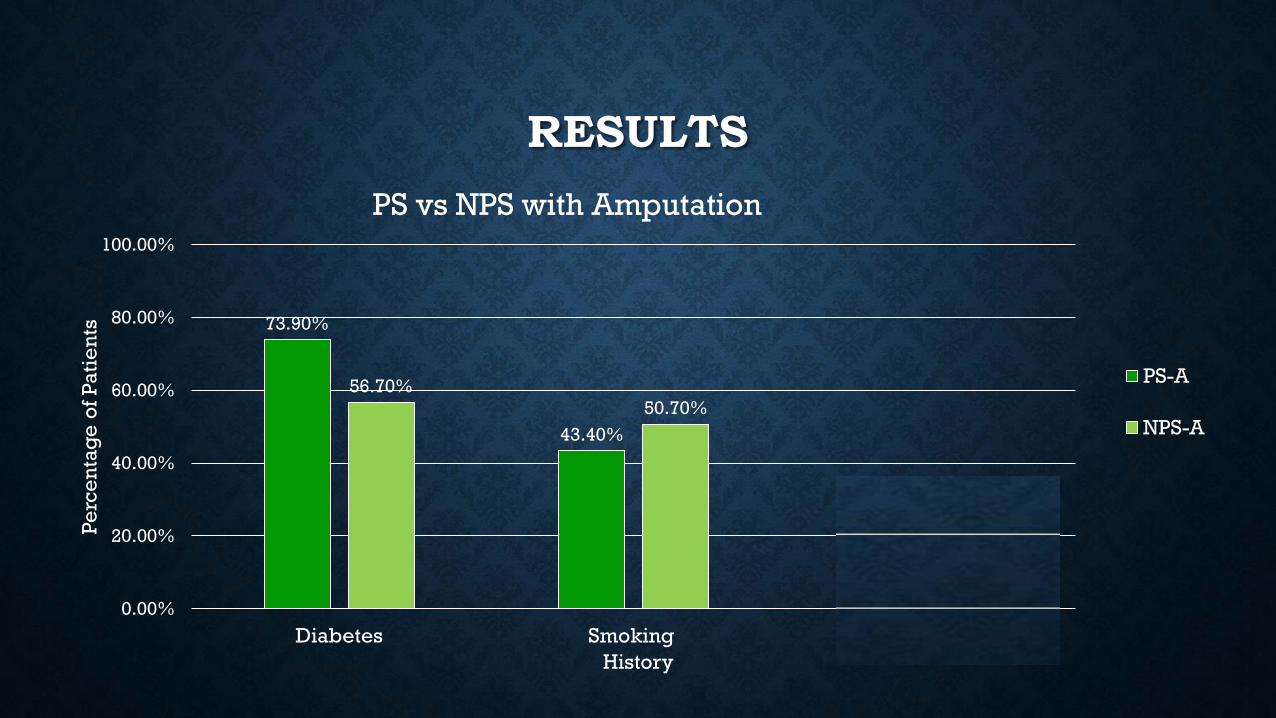
• The incidence of amputation was increased with PS consultation, but patients were
significantly more likely to have a minor final amputation level with PS involved
• Smoking history (V15.82, 305.1) did not correlate to increased incidence of
amputation following EVT
• PS inclusion in the limb salvage team offered CLI patients greater EVT success with
respect to improved preservation of limb length
REFERENCES
1. 1. Lumsden A, Davies M, Peden E. Medical and endovascular management of critical limb ischemia. J Endovasc Ther. 2009; 16(Suppl II):II31-1162.
2. Anahita D, Cheong LJ, Epidemiology of peripheral arterial disease and critical limb is ischemia. Tech Vasc Interventional Rad 2016; 19:91-95.
3. Dormandy J, Heeck L, Vig S. The fate of patients with critical limb ischemia. Semin Vasc surg. 1999; 12:142-147.
4. Norgren L, Hiatt WR, Dormandy J, et al. Inter-Society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007; 33(suppl 1):S1-S75
5. Sanders L, Robbins J, Edmons M. History of the team approach to amputation prevention: Pioneers and milestones. J Vasc Surg. 2010; 52:3S-16S
6. Rogers L, Andros g, Caporusso J, et al. Toe and flow: Essential components and structure of the amputation prevention team. J Vasc Surg. 2010; 52:23S-7S.
7. Kim P, Attinger C, Evans K, et al. Role of the podiatrist in diabetic limb salvage. J Vasc Surg. 2012;56:1168-72.
8. Chung J, Modrall G, Ahn C, et al. Multidisciplinary care improves amputation-free survival in patients with chronic critical limb ischemia. J Vasc Surg. 2015;61:162-9.
9. Driverr V, Goodman R, Fabbi M, et al. The impact of a podiatric lead limb preservation team on disease outcomes and risk prediction in the diabetic lower extremity.
10. Conrad M, Crawford R, Hackney L, et al. Endovascular management of patients with critical limb ischemia. J Vasc Surg. 2011;53:1020-5.
11. Conte M, geraghty P, Bradbury A, et al. Suggested objective performance goals and clinical trial design for evaluating catheter-based treatment of critical limb ischemia. J Vasc Surg.
2009;50:1462-74.
12. Rogers LC, Andros G, Caporusso J, et al. Toe and flow: essential components and structures of the amputation prevention team. J Vasc Surg 2010; 52(3 supple):23S-7S.
13. Hingorani A, LaMuraglia G, Henke P, et al. The management of diabetic foot: A clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric
Medical Association and the Society for Vascular Medicine. J Vasc Surg. 2016; 63:3S-21S.
14. Sumpio BE, Armstrong DG, Lavery LA, et al., Society for Vascular Surgery, American Podiatric Medical Association. The role of interdisciplinary team appraoch in the management of the
diabetic foot: a joint statement from the Society for Vascular surgery and the American Podiatric Medical Association. J Am Podiatr Med Assoc 2010;100:309-11
15. Krishnan S, Nash F, Baker N, et al. Reduction in diabetic amputations over 11 years in a defined U.K. population: benefits of multidisciplinary team work and continuous prospective audit.
Diabetes Care 2008; 31:99-101.
16. Sanders L, Robbins J, Edmonds M, et al. History of the team approach to amputation prevention: Pioneers and milestones. J Vasc surg 2010; 52:3S-16S.
17. Hioki H, Miyashita Y, Miura T, et al. Prognostic improvement by multidisciplinary therapy in patients with critical limb ischemia. J Angiology, 2015; 66(2): 187-194
18. Vartanina S, Kristin D, Robinson K, et al. Outcomes of neuroischemic wounds treated by a multidisciplinary amputation preventions service. Ann Vasc Surg 2015; 29:534-542.
19. Vinit N, Hogg, M Melina R, et al. Critical Limb Ischemia Review Article J Vasc Surg. 2010; 51 230-41.