3
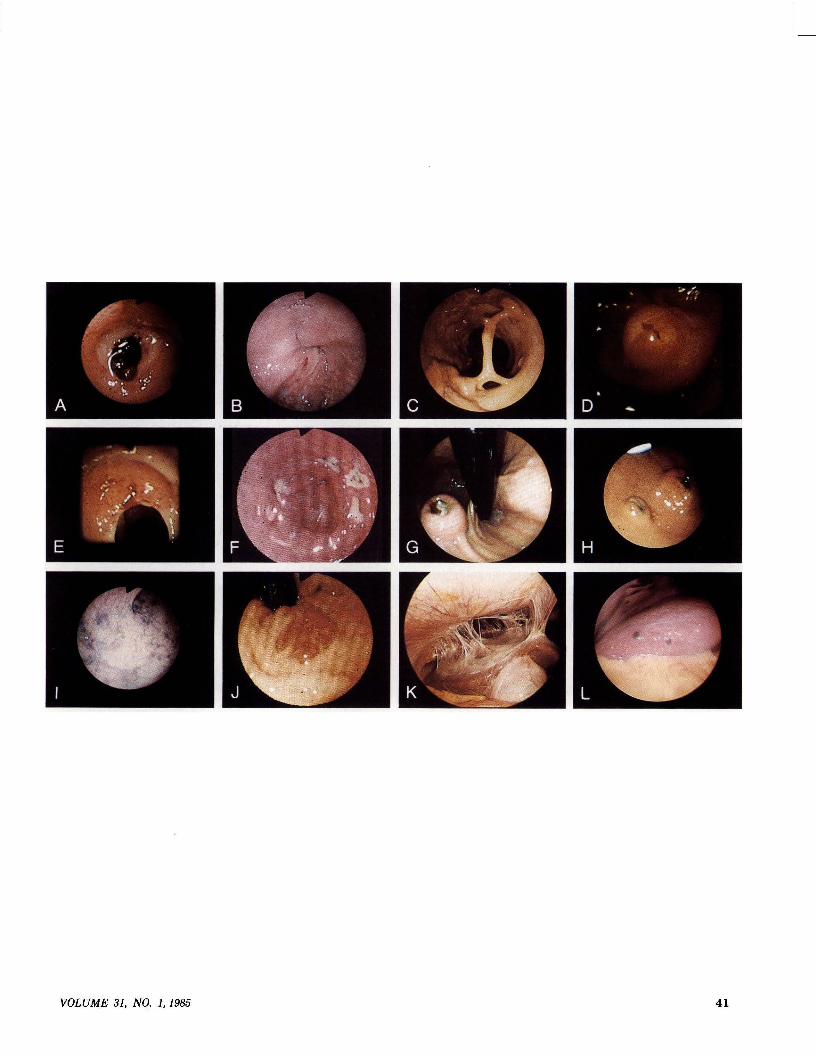
0016-6107/86/3101-0040$02.00 GASTROINTESTINAL ENDOSCOPY Copyright © 1986 by the American Society for Gastrointestinal Endoscopy Spectrum A selection of photographs from the 1984 A/S/G/E Learning Corner edited by Bennett E. Roth, MD Jay A. Noble, MD Burbank and Arcadia, California The following are true or false questions that refer to the A/S/G/E Learning Corner pfwtographs. The answers can be found on page 46. A. In regard to this finding following an acute upper gastrointestinal hemorrhage: 1. There is a high likelihood of rebleeding. 2. It is best to avoid endoscopic manipulation for fear of restart- ing bleeding. 3. Endoscopic electrocautery or laser therapy is usually recom- mended. 4. The central dark spot is the actual vessel. B. The sigmoidoscopic finding in this patient with symptoms of bowel obstruction can be attributed to: 1. Stricture of-colon. 2. Carcinoma. 3. Volvulus. 4. Ischemic colitis. C. This colonoscopy was done in a patient with longstanding ulcerative colitis. 1. The findings indicate a need for colectomy. 2. This usually occurs after many years of disease. 3. This may be seen without active symptomatology. 4. The band should be cut. D. The most likely diagnosis for this finding is: 1. Ampullary carcinoma. 2. Ulcerated duodenal polyp. 3. Lacerated papilla following spontaneous passage of stone. 4. Brunner gland hyperplasia. E. This ulcerating lesion was found in the mid esophagus. It is associated with: 1. Chronic esophagitis. 2. Increased risk of squamous cell carcinoma of esophagus. 3. Increased occurrence of colon carcinoma. 4. Esophageal stricture. F. A 26-year-old previously healthy man developed flu symptoms and medicated himself. Three days later he had the acute onset of hematemesis. Upper gastrointestinal endoscopy revealed these le- sions in the antrum. This patient most likely has: 1. Crohn's disease of the stomach. 2. Zollinger-Ellison syndrome with multiple ulcers. 3. Salicylate gastritis. 4. Gastric lymphoma. G. A 92-year-old woman was admitted with upper gastrointestinal bleeding. An upper gastrointestinal series revealed a smooth rounded mass in the fundus of the stomach which contained a central ulceration. Endoscopy showed the pictured lesion. 1. The lesion is most likely a pancreatic rest. 40 2. The lesion is most likely an ulcerated leiomyoma. 3. There is nothing to suggest the source of bleeding on this view. 4. Surgical excision is the treatment of choice in this patient. H. A 41-year-old woman with a past history of carcinoma of the breast 2years earlierpresented with upper gastrointestinal bleeding. These lesions were seen at endoscopy. 1. The multiplicity of the lesions rules out metastatic breast cancer. 2. Pinch biopsies of these lesions may not reveal the underlying histopathology. 3. These lesions should be surgically removed prior to any other form of therapy. 4. A course of sucralfate therapy would be helpful. I. A 76-year-old man with recurrent episodes of hematochezia had this appearance throughout the left colon on flexible fiberoptic sigmoidoscopy. He most likely has: 1. Angiodysplasia. 2. Cavernous hemangioma. 3. Colonic varices. 4. Peutz-Jeghers syndrome. J. A 21-year-old man admitted with chronic cough and shortness of breath underwent flexible fiberoptic sigmoidoscopy because of diarrhea. This lesion was found on retroverting the instrument inside the rectum. 1. These lesions are often asymptomatic. 2. Biopsies usually reveal interlacing bundles of spindle cells with extravasated red blood cells. 3. These lesions should be removed by hot-biopsy electrofulgur- ation. 4. Defects in the immune mechanism may be seen in association with these lesions. K. A 21-year-old woman developed right upper quadrant pain which became quite severe. This is a laparoscopic view of the area of the right lobe of the liver. The only positive finding on system review was the presence of a chronic vaginal discharge. This patient has: 1. Postsurgical adhesions. 2. Acute cholecystitis. 3. Acute hepatitis A. 4. Fitz-Hugh and Curtis syndrome. L. A 46-year-old man underwent laparoscopy as part of a staging procedure for malignant disease found elsewhere in the body. The presence of these lesions in the right lobe of the liver confirms the presence of: 1. Hemangiosarcoma. 2. Bronchogenic carcinoma. 3. Malignant melanoma. 4. Hodgkin's disease. GASTROINTESTINAL ENDOSCOPY