Page 1
A simple long-term stroke risk model for asymptomatic carotid stenosis – will it help
us select patients for intervention in the future?
MAC, 09.00 7th December 2017
Alison HALLIDAY, Dylan MORRIS, Richard BULBULIA, Hongchao PAN,
Richard PETO, Peter ROTHWELL
University of Oxford
Page 2
Global Burden of Stroke
Age-standardised stroke mortality declining,
but total number risingGBD 2015 Mortality and Causes of Death Collaborators, DALYs and HALE
Collaborators (2016), Lancet
1990 20152005
5. Cerebrovascular
Disease
3. Cerebrovascular
Disease
2. Cerebrovascular
Disease
4. Ischaemic Heart
Disease
3. Diarrhoeal Disease
2. Neonatal Preterm
Birth
1. Lower Respiratory
Infections
4. HIV/AIDS
5. Neonatal Preterm
Birth
2. Lower Respiratory
Infections
1. Ischaemic Heart
Disease
1. Ischaemic Heart
Disease
3. Lower Respiratory
Infections
4. Neonatal Preterm
Birth
5. Diarrhoeal Disease
Page 3
Carotid Artery Disease
• Important cause of ischaemic stroke (15-20%)
• Most (80%) carotid strokes have no warning
symptoms
• Asymptomatic stenosis: important long-term
stroke risk
• RCTs confirm net benefit of CEA among
asymptomatic patients
• Successful CEA ~halves long-term stroke risk
Page 4
Trial Characteristics – CEA vs not
1983-2008
VA ACAS ACST-1
Recruitment1983 -
1987
1987 -
1993
1993 -
2003
Participants 444 1 662 3 120
Region USA USA Europe
Follow-up, Median
[IQR]
5.7 [4.5-
7.0]
4.8 [3.7-
5.0]
9.0 [6.1-
11.1]
Page 5
VA, ACAS, ACST-1 Trials
Unpublished, not for reproduction
0 5 100
5
10
15
Years
Events/person-years
Years 0-4 Years 5-9 Years 10+
37/5399 (0.7% pa) 20/2160 (0.9% pa) 3/265 (1.1% pa)
79/5447 (1.5% pa) 32/2096 (1.5% pa) 3/220 (1.4% pa)
3%
8%
7%
14%
0 5 100
5
10
15
Years
Perioperative events/CEAs (%) + other events
Years 0-4 Years 5-9 Years 10+
26/1209 (2.2%) + 37 0/15 (0.0%) + 20 0/5 (0.0%) + 3
14/375 (3.7%) + 79 2/69 (2.9%) + 32 0/6 (0.0%) + 3
5%
10%
8%
16%
B. Any non−perioperative strokeA. Any stroke or perioperative death
Even
t R
isk %
, (S
E)
2291 Patients on triple therapy (ie, including
statin) before stroke
CEA +
TMT
TMT
alone TMT
alone
CEA +
TMT
Page 6
AIM: to develop a simple clinical risk score to identify patients with high risk asymptomatic carotid stenosis
Purpose of this Study
There is uncertainty as to which asymptomatic
patients benefit most from carotid intervention
Page 7
• IPD of ‘medically treatment’ patients from all 3
asymptomatic trials
• VA
• ACAS
• ACST-1
• Restricted to those with no CEA prior to stroke (ie,
medically managed)
• Stroke risk ratios (RR) from Cox regression
• Most important factors included in risk score (RR >1.3)
Methods
Page 8
0 5 100
10
20
30
Years
Even
t R
isk (
%,
SE
)
Score 0
Score 1
Score 2+
6.3%
11.4%
11.1%
21.6%
19.5%
31.6%
Score 0 21/1712 (1.2% pa) 6/573 (1.0% pa)
Score 1 67/2659 (2.5% pa) 14/615 (2.3% pa)
Score 2+ 124/2497 (5.0% pa) 16/501 (3.2% pa)
Events/person-years (% pa)Years 0-5 Years 5-10
0 1 2 3 4
Stroke RR (95% CI)Stroke RR (95% CI)
Participants
Events /
Person-years Stroke RR (95% CI)
1.00 (0.68-1.46)Score 0 773 27/2337
1.92 (1.55-2.39)Score 1 1376 81/3336
3.64 (3.08-4.31)Score 2+ 1359 143/3063
95% CI0.5 1 1.5 2 2.5 3
Stroke RR (95% CI)Stroke RR (95% CI)
Events / Person-yearsAt Risk Reference Stroke RR (95% CI)
1.32 (1.03-1.68)History of Diabetes 278/1075187/2433
1.23 (0.97-1.55)Male Sex 105/4553260/8631
1.16 (0.95-1.40)Total Cholesterol (per 2 mmol/L) 316/11665*
1.15 (1.00-1.33)Older Age (per 10 years) 365/13184*
1.09 (0.98-1.21)Systolic Blood Pressure (per 20 mmHg) 364/13147*
1.03 (0.83-1.27)History of Ischaemic Heart Disease 228/8559137/4625
Association of CV Risk Factors with Stroke (among medically managed)
Unpublished, not for reproduction
Page 9
0 5 100
10
20
30
Years
Even
t R
isk (
%,
SE
)
Score 0
Score 1
Score 2+
6.3%
11.4%
11.1%
21.6%
19.5%
31.6%
Score 0 21/1712 (1.2% pa) 6/573 (1.0% pa)
Score 1 67/2659 (2.5% pa) 14/615 (2.3% pa)
Score 2+ 124/2497 (5.0% pa) 16/501 (3.2% pa)
Events/person-years (% pa)Years 0-5 Years 5-10
0 1 2 3 4
Stroke RR (95% CI)Stroke RR (95% CI)
Participants
Events /
Person-years Stroke RR (95% CI)
1.00 (0.68-1.46)Score 0 773 27/2337
1.92 (1.55-2.39)Score 1 1376 81/3336
3.64 (3.08-4.31)Score 2+ 1359 143/3063
95% CI
Association of Cerebrovascular Events with Stroke
(among medically managed)
0.5 1 1.5 2 2.5 3
Stroke RR (95% CI)Stroke RR (95% CI)
Events / Person-yearsAt Risk Reference Stroke RR (95% CI)
1.57 (1.21-2.03)Brain Infarct on Imaging 158/630193/2435
1.57 (1.26-1.94)Prior Contralateral Event 232/9687133/3497
1.20 (0.95-1.53)Prior CEA 274/1036291/2821
1.14 (0.76-1.70)Prior Ipsilateral Event 282/1036128/1084
1.13 (0.84-1.53)Contralateral Stenosis >80% 274/1057751/1624
0.93 (0.74-1.16)Ipsilateral Stenosis >80% 204/7635123/4596
Unpublished, not for reproduction
Page 10
0.5 1 1.5 2 2.5 3
Stroke RR (95% CI)Stroke RR (95% CI)
Events / Person-years
At Risk Reference Stroke RR (95% CI)
1.57 (1.21-2.03)Brain Infarct on Imaging 158/630193/2435
1.57 (1.26-1.94)Prior Contralateral Event 232/9687133/3497
1.32 (1.03-1.68)History of Diabetes 278/1075187/2433
3 Important Stroke Risk Factors
0 5 100
10
20
30
Years
Even
t R
isk (
%,
SE
)
Score 0
Score 1
Score 2+
6.3%
11.4%
11.1%
21.6%
19.5%
31.6%
Score 0 21/1712 (1.2% pa) 6/573 (1.0% pa)
Score 1 67/2659 (2.5% pa) 14/615 (2.3% pa)
Score 2+ 124/2497 (5.0% pa) 16/501 (3.2% pa)
Events/person-years (% pa)Years 0-5 Years 5-10
0 1 2 3 4
Stroke RR (95% CI)Stroke RR (95% CI)
Participants
Events /
Person-years Stroke RR (95% CI)
1.00 (0.68-1.46)Score 0 773 27/2337
1.92 (1.55-2.39)Score 1 1376 81/3336
3.64 (3.08-4.31)Score 2+ 1359 143/3063
95% CI
Unpublished, not for reproduction
Page 11
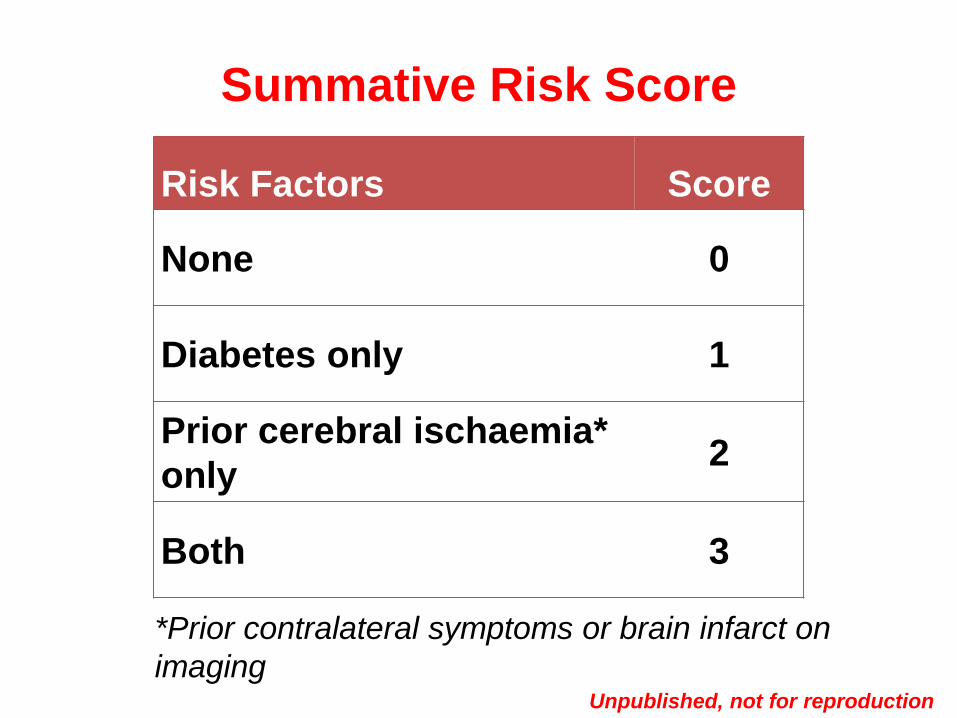
Risk Factors Score
None 0
Diabetes only 1
Prior cerebral ischaemia*
only 2
Both 3
Summative Risk Score
*Prior contralateral symptoms or brain infarct on
imagingUnpublished, not for reproduction
Page 12
0 1 2 3 4
Stroke RR (95% CI)Stroke RR (95% CI)
Risk Factors Participants
Events /
Person-years Stroke RR (95% CI)
1.00 (0.80-1.25)None 1597 78/4230
1.54 (1.06-2.24)Diabetes Only 438 28/929
2.15 (1.79-2.59)Prior Cerebral
Ischaemia Only*1145 113/2881
2.39 (1.69-3.39)Both 328 32/697
Risk Prediction
*Prior contralateral symptoms or brain infarct on imaging
None
(Score 0)
Diabetes
Only
(Score 1)
Prior Cerebral
Ischaemia only*
(Score 2)
Both
(Score 3)
Unpublished, not for reproduction
Page 13
Risk Prediction
If the 10-year stroke risk is:
9% (no risk factors) 10y Absolute gain from CEA ~5%
13%* (diabetes) 10y Absolute gain from CEA ~7%
20% (prior ischaemia) 10y Absolute gain from CEA ~10%
(1/3 of trial participants)
*Stroke risk in medically treated ACST-1 participants taking statins
Page 14
Implications
• Statins work: With CEA or without CEA, modern statin ~halves stroke risk
• And CEA works: With a statin or without a statin, successful CEA ~halves stroke risk
• Risk of stroke ~double with prior cerebral ischaemia
• Those with higher risk scores should derive greater absolute benefit from CEA
Page 15
Simple characteristics (diabetes, prior ischaemia)
can be used to identify high stroke risk patients
who might benefit most from CEA
Conclusion
Page 16
ACST-2 Surgery vs Stenting
Asymptomatic patients with tight stenosis requiring intervention:
Which procedure is generally better (in addition to good medical treatment)? :
carotid surgery (CEA)or
carotid stenting (CAS)?
Page 17
ACST-2 progress – High Stroke Risk patients
>2731/3600 now recruited, 869 still needed, by end of 2019
30% diabetic
35% previous symptoms or cerebral infarcts
Follow up to date - 3.5 years
Statin treatment is good
Page 18
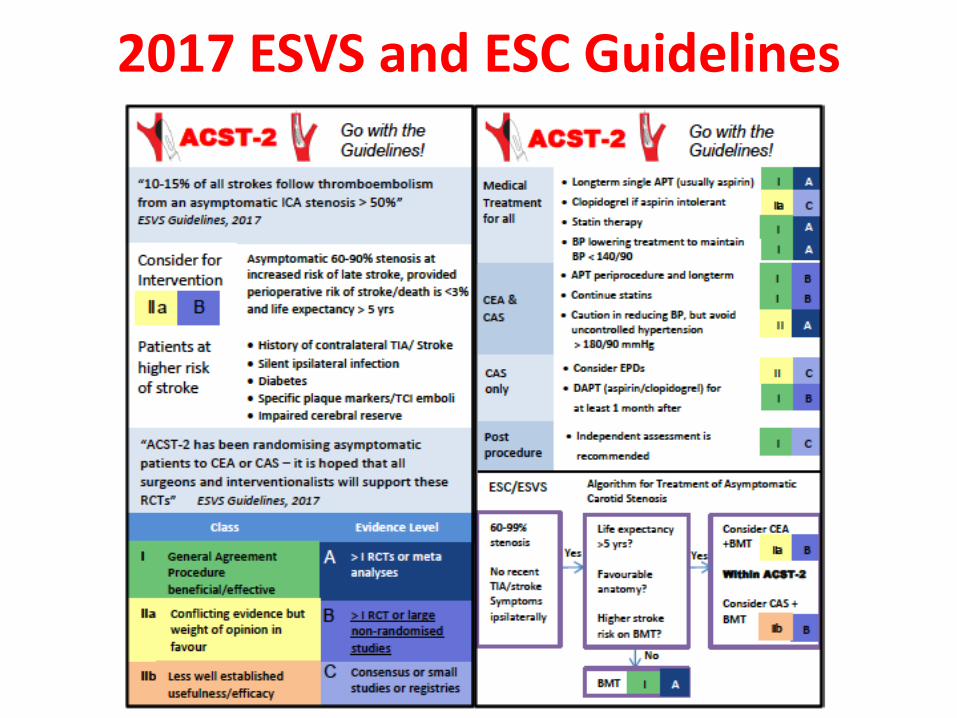
2017 ESVS and ESC Guidelines
Page 19
2009 2010 2011 2012 2013 2014 2015 2016
Statin Use by Year
Fre
qu
en
cy (
%)
Year
0
20
40
60
80
100
ACST-2: Long-term statin use >80%
Page 20
2013 2014 2015 2016
Intensity of Statin Therapy by YearF
req
uen
cy (
%)
Year
0
20
40
60
80
100 (Unclear)
High Dose
Moderate Dose
Low Dose
ACST-2: >75% on good (or very good) statin regimens
Simva 40 Atorva 20 Rosuva 10 Combined
Page 21
ACST, ACAS, VA Trialists and
to the participants who took
part
ACST-2 information
website acst-2.org
Acknowledgements