Page 1
1
A STUDY TO EVALUATE THE EFFECTIVENESS OF PLANNED
TEACHING PROGRAMME REGARDING KNOWLEDGE AND
ATTITUDE ON PREVENTION OF DENTAL CARIES AMONG
THE MOTHERS OF PRIMARY SCHOOL CHILDREN AT
ANEKAL DISTRICT, BANGALORE.
By
Ms. ANJU APPUKUTTAN
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment of the requirements for the degree of
MASTER OF SCIENCE
In
CHILD HEALTH NURSING
Under the guidance of
Mrs. Pushpakumari K
Professor
Department of child health Nursing
SPURTHY COLLEGE OF NURSING
MARASUR GATE, BENGALURU.
2013
Page 2
2
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis entitled. “A study to evaluate
the effectiveness of planned teaching programme regarding knowledge and attitude on
prevention of dental caries among mothers of primary school children at
AnekalDistrict Bangalore.” is a bonafide and genuine research work carried out by
me under the guidance of Mrs.pushpakumari k, Professor, Department of Child
Health Nursing.
Date: Signature of the Candidate
Place: Bangalore Ms. Anju Appukuttan
Page 3
3
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A study to evaluate the
effectiveness of planned teaching programme regarding knowledge and attitude on
prevention of dental caries among mothers of primary school children at
AnekalDistrict Bangalore.” Is a bonafide research work done by Ms. Anju
Appukuttan, in partial fulfillment of the requirement for the degree of Master of
Science in Child Health Nursing.
Signature of the Guide
Mrs.Pushpakumari K
Professor
Date: Place: Bangalore
Page 4
4
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF THE
INSTITUTION
This is to certify that the dissertation entitled “A study to evaluate the
effectiveness of planned teaching programme regarding knowledge and attitude on
prevention of dental caries among mothers of primary school children at
AnekalDistrict Bangalore.” is a bonafide research work done by Ms. Anju
Appukuttan, in partial fulfillment of the requirement for the degree of Master of
Science in Child Health Nursing.
.
Seal & Signature of the HOD Seal & Signature of the Principal Name: Mrs. Pushpakumari K Name:Prof .N.Muralidhar M.N
Date: Date: Place; Bangalore Place: Bangalore
Page 5
5
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka
shall have the rights to preserve, use and disseminate this dissertation / thesis in print
or electronic format for academic / research purpose.
© Rajiv Gandhi University of Health Sciences, Karnataka
Date: Place: Bangalore
Signature of the Candidate
Ms. Anju Appukuttan
Page 6
6
ACKNOWLEDGMENT
"When you're chewing on life's gristle....
Don't grumble, give a whistle and this'll help things turn out for the
best…..
And always look on the bright side of life.... ……..
And Always look on the light side of the life"....
Life is like a coin. You can spent it anyway you wish, But you only spent it
ones along with all, God's wish is the first
"Praise and glory to the God Almighty who is the sources of strength,
inspiration and blessing in every walk of my life and the function of knowledge and
wisdom".
I raise my heart in gratitude to God almighty, who has been my shepherd and
guiding force behind my all efforts. His Omni presence has been my anchor through
the hard time
With profound sentiments and gratitude, I the investigator of this study own
my heartfelt gratitude to all those who have contributed for the successful completion
of this dissertation.
Page 7
7
Any accomplishment requires the effort of many people. I feel it is a great
privilege to express my heartfelt thanks and gratitude to all who directly or indirectly
have given valuable guidance and timely suggestion throughout this dissertation
work.
It is my privilege to express my special thanks to MR. P. GOPALA REEDY,
CHAIRMAN, Spurthy Group of Institution,, Bangalore for giving me the opportunity
to undertake this study and avail facilities in this institution.
Grateful thanks to Mr.Vinay Secretary, Spurthy Group of Institutions of
nursing for his constant encouragement and help to complete this study.
It's my pleasure and privilege to express my deep sense of gratitude to our
respective PROF. N. MURALIDHAR.M.N Principal, the SPURTHY GROUP OF
INSTITUTIONS for his constant encouragement and support given to me during the
study.
Quality always makes difference through its generosity, richness, kindness and
intelligence. These quality aspects has been incorporated and accomplished in this
study through the effective, enriched, constant guidance and support from my guide
PROF. PUSPAKUMMARI. HOD, CHILD HEALTH NURSING, the Spurthy
Group of Institutions, Bangalore. I express my immense gratitude for her valuable
guidance and making this effort success.
Page 8
8
I express my sincere thanks to all experts in the field of Child health nursing
for validating the content of the tool and providing valuable suggestions and guiding
in validating the tool.
I sincerely express my special thanks to all MSc Nursing Lecturer's in Spurthy
Group of Institutions for their timely help, co-operation, valuable guidance and
suggestions to successful completion of my desertion work.
I am grateful to MRS. USHAPRADEEP, Lecturer in English, for editing the
report of my dissertation.
I wish to express my thanks to MR. BHASKER RAJ bio statistician, for his
guidance in statistical analysis and presentation of data.
My heartfelt thanks to Principal of St.philominas high schoo, anekal, district,
for allowing me to conduct the study and also give greatful thanks for mother's of
Primary school children for their kind cooperation for conducting the study
I thank heartily to Librarians of the RGUHS and Spurthy College of Nursing
for their cooperation and support throughout the study.
A word of appreciation to MR. SUDHARSHAN REDDY C. V. and MR.
SRINATH for their enthusiastic help and sincere efforts in editing the manuscript
meticulously with much valued computer skills.
Page 9
9
I extended my sincere gratitude to the NON-TEACHING STAFF of this
college for their cooperation.
I extent my thanks to my family, parents Mr. A P P U K U T T A N . P . R &
M r s . S A S I K A L A , mother-in-law Mrs. LAKSHMI & And Father-In-Law Mr.
RAMAKRISHNAN and brother in law Mr.SUJITH & Mr.SANTHOSH who gave
me meaning to my life in so many ways and for their full co-operation in completion
of my course
It is my proud privilege to express the deepest sense of gratitude to Mr.
RENJITH.T.M, for his continuous support, patience, encouragement and prayers
throughout my study period and life, without whom I would not undergone my
studies.
Next my heartfelt thanks to my dearest brother Mr. ROBIN.S and sister in
law Mrs ALBA, Mrs.RENU and my dearest friends Mrs BABITHA, Mrs.REKHA
for their support and prayer during the study period and it's my pleasure and privilege
to express my deep sense of gratitude.
My special heartfelt thanks to my classmates and friends Ms PRATHIBHA,
Mr.AJEESH, Ms JINCY, and my juniors of M.Sc. Nursing for their support in the
successful completion of the study.
Page 10
10
Last but not Least, I extend my thanks to all those who have been directly or
indirectly associated with my study at various levels, but not mentioned in this
acknowledgement.
Above all I bow my head in reverence to god almighty for guide me to reach
the steps and complete my study. Has omnipresence has been my anchor through the
fluctuating hard times and makes it all possible.
Thanks to all.
DATE: SIGNATURE OF THE CANDIDATE
PLACE: BANGALORE (MS.ANJUAPPUKUTTAN)
Page 11
11
LIST OF ABBREVATIONS
1. M: Mean
2. PTP: planned Teaching Programme.
3. X2: Chi square.
4. NS: Non significant.
5. %: percent.
6. S: Significant.
7. df: Degree of freedom.
8. WHO: World Health Organization.
Page 12
12
RESEARCH ABSTRACT
“Life’s not just being alive, but being well.”
BACKGROUND OF THE STUDY
Dental caries and periodontal disease, the most commonly seen oral disease
show striking geographic variation, socioeconomic patterns and severity of
distribution all over the World 1-5 Number of factors have been put forward to
explain the variation in prevalence and severity of dental caries and periodontal
disease that can be found between developing and technically developed countries,
but also between rural and urban communities.1
Assessing caries risk is important for all patients and the process has to be
repeated at intervals. Caries-promoting factors may change between visits and on a
population level the disease and its squeal are very widespread in adulthood. This
guideline seeks to identify those children who are at greatest risk of future dental
decay in time to prevent the ravages of dental caries. However, it must be appreciated
that primary prevention will be required in all children to maintain low caries risk
status.2
STATEMENT OF THE PROBLEM
“A study to evaluate the effectiveness of planned teaching programme regarding
knowledge and attitude on prevention of dental caries among mothers of
primary school children at AnekalDistrict Bangalore.”
Page 13
13
Objectives of the study
1. To assess the pre and post test level of knowledge on prevention of dental
caries.
2. To assess the pre test practice on prevention of dental caries
3. To introduce the structured teaching program regarding prevention of dental
caries.
4. To find out the difference between the pre test and post test knowledge on
prevention of dental caries.
5. To find out the difference between the pre test and post test attitude on
prevention of dental caries.
6. To find out the association between the pre tests knowledge on prevention
of dental caries among mothers of primary school children with their
demographic variables.
Hypothesis;
H 1 – There will be a significant difference between the pre test and post test
knowledge on prevention of dental caries among mothers of primary school children.
H 2 - There will be a significant association between the pre test and post test
knowledge on prevention of dental caries among mothers of primary school children
with their secured demographic variables.
H 3 - There will be a significant association between the pre test and post test
attitude on prevention of dental caries among mothers of primary school children with
their secured demographic variables.
Page 14
14
CONCEPTUAL FRAME WORK
The conceptual frame work chosen for this study is based on the Health Belief
Model. The Pender’s health belief model affects the health promotion and behavior
practice. Persons have to initiate and do active roles and this behavior is goal directed
for raising health and good living. The Pender’s health promotion model, first appear
in nursing literature in early 1980s and later the revised health promotion model
appears in 1996. In revised health promotional model, Pender represents that raising
health status and avoiding illness are the major motivational significance in health
promotional behavioral practice.
METHODOLOGY
A research approach tells us so as to what data to collect and how to analyze it. It
also suggests possible conclusions to be drawn from the data. In view of the nature of
the problem selected for the study and the objectives to be accomplished, a evaluate
survey research approach was considered as the best way to assess the knowledge and
attitude of primary school children mothers regarding dental caries.Evaluate design
with survey method was used in this study.
Part-I Socio-Demographic Data
The investigator constructed the tool to collect the Socio - demographic data of the
study subjects. It consists of demographic variables
Part-II
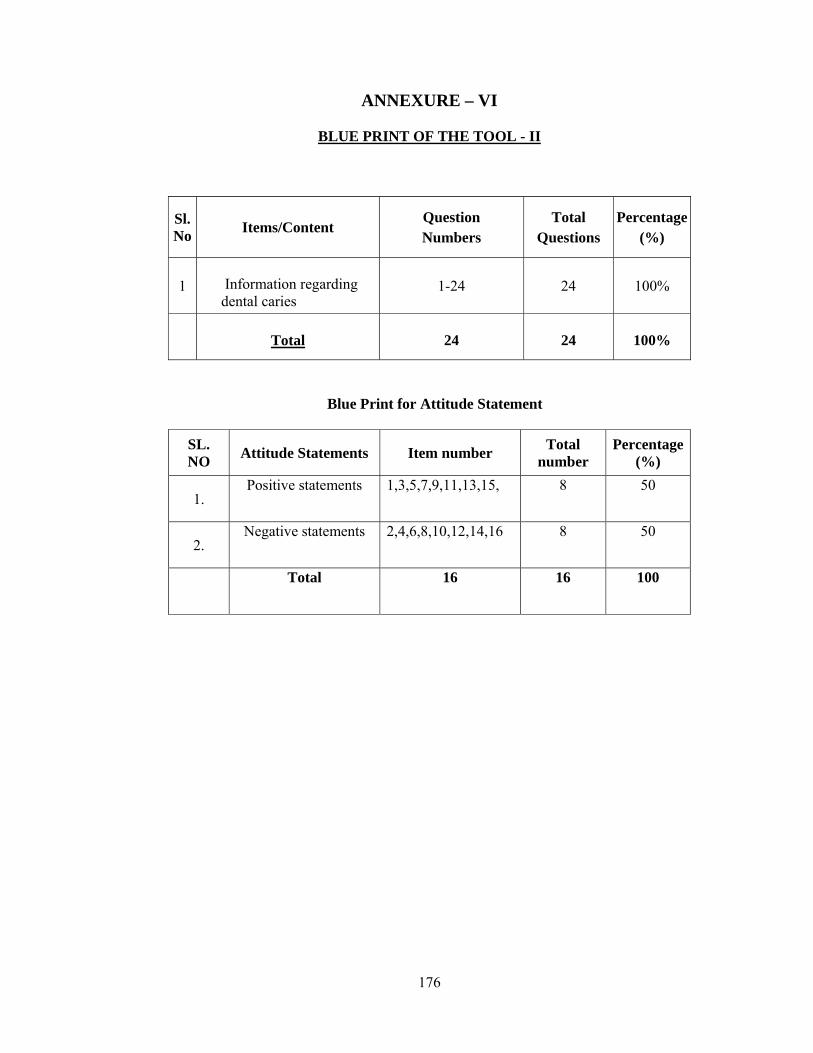
Investigator prepared structured knowledge questionnaire containing 24 knowledge
questions regarding dental caries.
Page 15
15
Part III:
Investigator prepared attitude rating scale regarding dental caries consisting of 16
statements, Attitude statements were given with the range score of 0 to 2 marks. The
data gathered was analyzed and interpreted interns of objectives of the study. The
mean, SD, Mean Percentage, mean difference percentage of knowledge and attitude
about the dental caries were analyzed by using descriptive and inferential statistics.
MAIN STUDY:
The total sample of the main study was consisted of 60 primary school children
mothers, data was collected from the sample by administering structured knowledge
questionnaire.
DATA COLLECTION METHOD:
A formal written permission was obtained from the principal of the primary
school, Bangalore. The data was collected from 60 primary school children mothers
who fulfilled inclusion criteria. Before conducted the study, consent was taken from
them by explaining purpose of the study.
DATA ANALYSIS:
The data was planned to analyze on the basis objective and hypothesis of study
.The obtained data was analyzed using descriptive are inferential statistics and
interpreted in the terms of objective and hypothesis of the study. The level of
significance was set at 0.01 and 0.05.
Page 16
16
MAJOR FINDINGS OF THE STUDY
Majority of the subjects were (25.0%) in the age group of 21-25years, 38.0%
had upto SSLC education and 25.0% were coolie orker. Most of the respondents
(37.0%) had family income fall beteen Rs 3000-4000 and majority of respondents
were belonged to Hindu religion (53.0%).They were belonged from rural area
(26.0%) ; majority of respondents are from nuclear family (36%) and majority of the
repondent got information from health personel about dental caries.
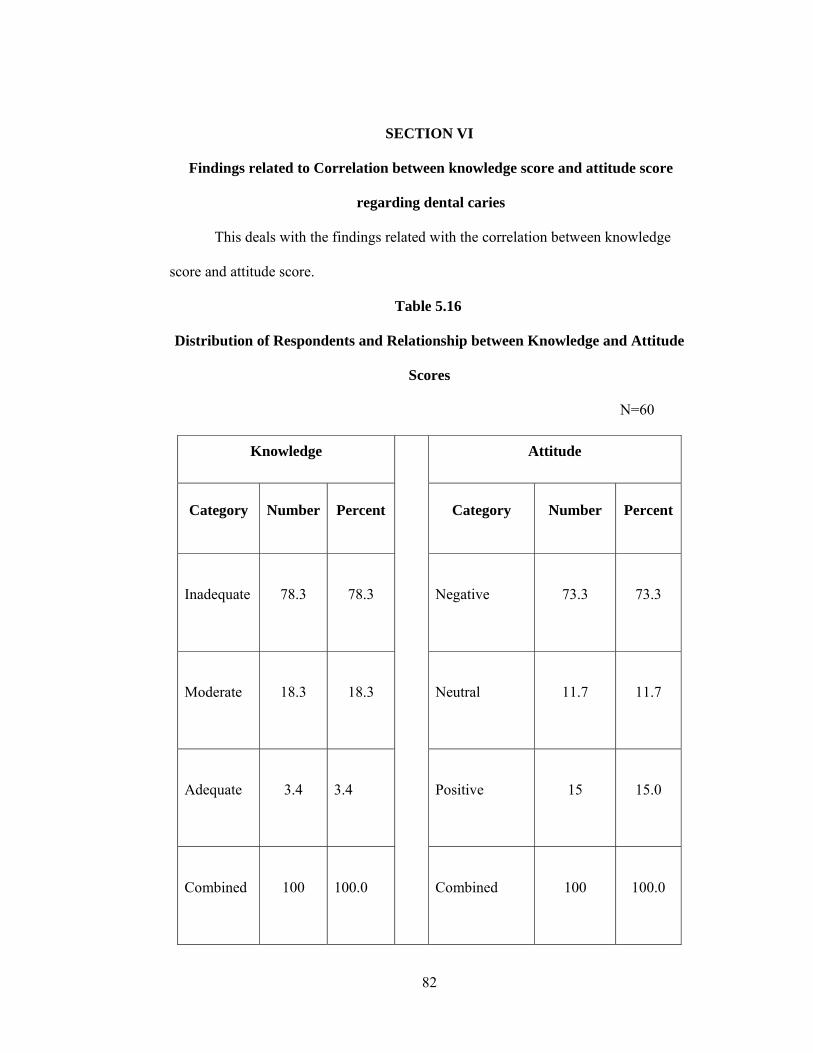
In this study out of 60 primary school children mothers, 78.3 (78.3%) had
inadequate knowledge, 18.3(18.3%) women had moderately knowledge and
3.4(3.4%) of the primary school children mothers had adequate knowledge regarding
dental caries. The respondent’s mean knowledge score is 97.96%. 73.3 (73.3%)
women had negative attitude, 15(15%) women had neutral attitude and 11.7 (11.7%)
had positive attitude regarding dental caries. The respondent’s mean attitude level
showed is 51.4%.
There is a significant association between Age and knowledge at the level of
5% (X2 =9.25 at P>0.05 level), Place of residence and knowledge at the level of 5%
(X2 = 5.568 at P<0.05 level), Type of family and knowledge at the level of 5% (X2 =
5.993 at P>0.05 level),Religion and knowledge at the level of 5%(X2 = 7.862 at
P>0.05 level),significant association between Age and attitude at the level 5%,(X2 =
18.72 at P>0.05 level), Place of residence and attitude at the level of 5%. (X2 =10.51at
P>0.05 level) and Source of information and attitude at the level of 5%. (X2 =24.98 at
P>0.05 level).
Page 17
17
There is a positive significant relationship between knowledge and attitude of
respondents on dental caries (r = +.0.894274).So this is highly correlated with each
other.
CONCLUSION AND RECOMMENDATION
The overall findings of the study clearly showed that primary school mothers had
inadequate knowledge and negative attitude towards dental caries.
Thus to conclude the investigator has achieved the objective for assessing
knowledge and attitude towards dental caries based on the study finding planned
teaching programme has been developed.
Page 18
18
LIST OF CONTENTS
Sl.No TITLE Page no
1. Introduction.
21-28
2. Objectives.
29-37
3. Review of Literature.
38-51
4. Methodology.
52-62
5. Results.
63-82
6. Discussion.
83-89
7. Conclusion.
90-94
8. Summary.
95-101
9. Bibliography.
102-107
10. Annexure.
108-181
Page 19
19
LIST OF TABLES
Sl.No Tables Pages
1. Frequency and percentage ditribution of primary school children
mothers according to demographic variables such as age, type of
the family, family income, education, occupation, number of
children, source of information, history of oral disorders.
65-72
2. Frequency and percentage ditribution of primary school children
mother according to their pre test and post test knowledge
assessment.
73
3 Aspect wise Mean, S.D and mean % knowledge score related to
dental caries.
74
4 Aspect wise Mean, Mean% and standard deviation of attitude
Scores related to dental caries
75
5. Frequency and percentage distribution of primary school children
mothers according to their pre test and post test attitude
assessment
76
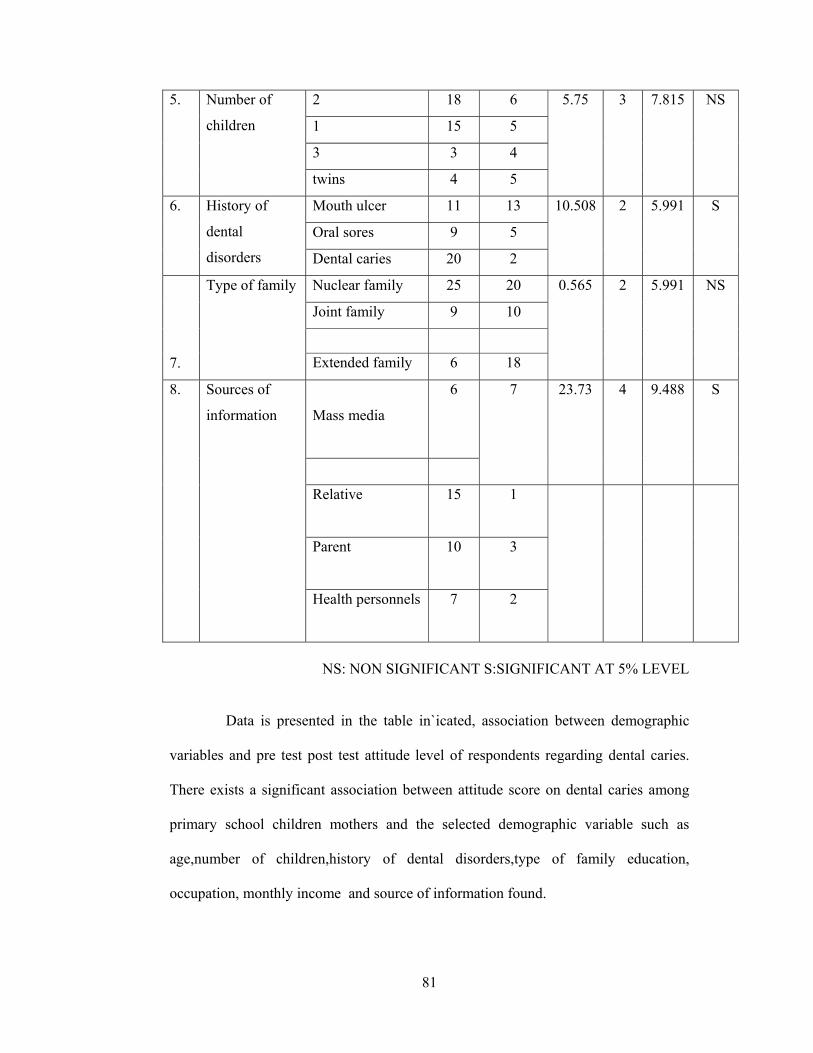
6. Association between pre test and post test Knowledge Level of
Respondents on dental caries with demographic variables
77-78
7. Relationship between Knowledge and Attitude Scores 79-80
8. Correlation between pre test and post test scores
81-82
Page 20
20
LIST OF FIGURES
Sl.No. Figures Pages
1. Conceptual frame work. 37
2. Schematic representation of research design/ research study. 62
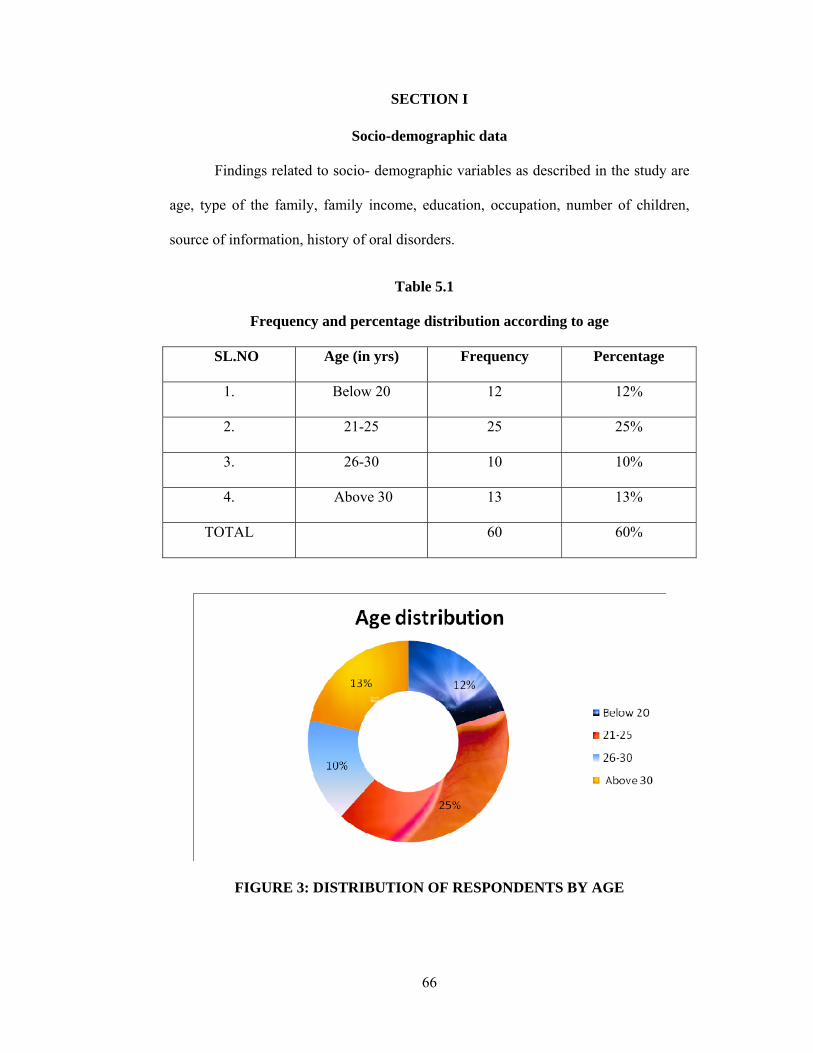
3. Pie Diagram showing the Classification of respondents by age 65
4. Cone Diagram showing the Classification of respondents by
education
66
5. Pie Diagram showing the Classification of respondents by
occupation
67
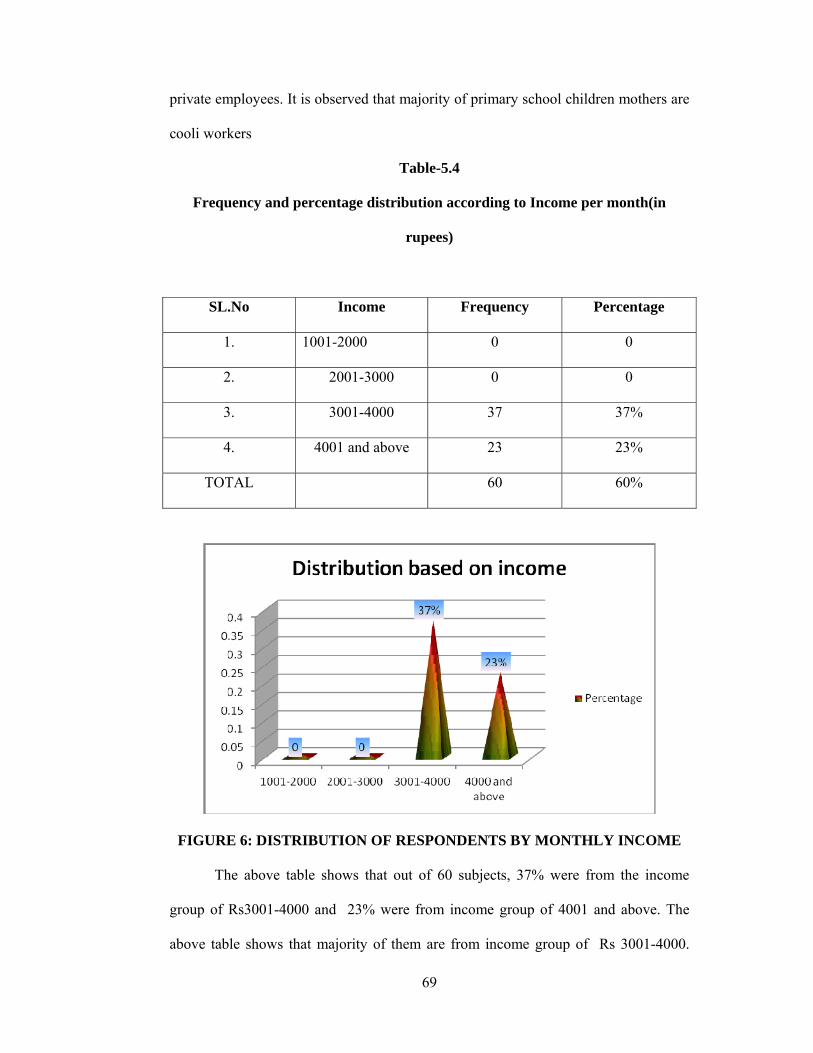
6. Bar Diagram showing the Classification of respondents by monthly
income
68
7. Bar Diagram showing the Classification of respondents by number
of children
69
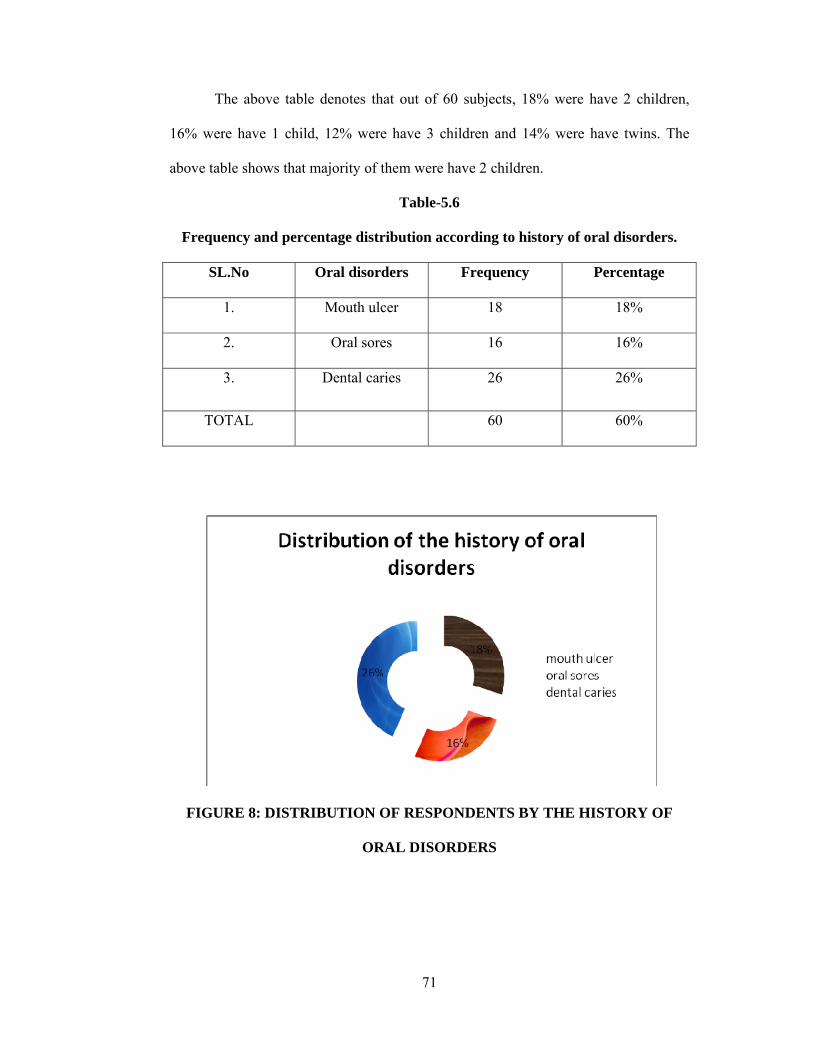
8. Pie Diagram showing the Classification of respondents by history
of dental disorders
70
9. Bar Diagram showing the Classification ofRespondents by type of
family
71
10. Pie Diagram showing the Classification of respondents by source of
information
72
Page 21
21
INTRODUCTION:-
Page 22
22
Every tooth in a man's head is more valuable than a diamond.
~Miguel de Cervantes, Don Quixote, 1605
Children bring fragrance and meaning to life, they are a gift of God and we the
gardeners to meet their needs, we provide the best to them by proper care,
nourishment, love, attention and good health.3
Todays children are citizens of tomorrow and to have a strong shouldered
man, a child should be free from mortality. Mahler who was the Director general of
the WHO in 1984 stated that “children are a priceless resources and a nation which
neglects them does so at its peril”. Healthy children are the greatest resource and pride
of the nation, the children ought to be healthy and happy to become productive adults
of the future. To give them happy and healthy childhood we must safe guard their
total health right from the beginning.4
Oral health is an integral component of primary school children’s health and
well-being. The overall health, well being, education and development ofchildren,
families and communities can be affected by oral health.4
Dental caries and periodontal disease, the most commonly seen oral disease
show striking geographic variation, socioeconomic patterns and severity of
distribution all over the World 1-5 Number of factors have been put forward to
explain the variation in prevalence and severity of dental caries and periodontal
disease that can be found between developing and technically developed countries,
but also between rural and urban communities. Additionally, there is marked
variability in the pattern of many disease between different socio-economic groups in
Page 23
23
the same country. In recent studies, socio-economic factors have been identified as
predisposing factors in the development of both dental caries and periodontal disease
6-9. Low income and poor education have been reported to influence periodontal
status 10. Reseach in industrialized countries has revealed that children of high
social class families experience less caries than those of lower social classes 11 .
However, this relationship appears to be reversed in the developing countries 3.
Hence an attempt has been made to determine the relationship of oral hygiene status
and dental caries experience with socio-economic status in Davangere, India.5
Though there has been considerable improvement in the oral health of children
in the last few decades, dental caries (tooth decay) still remains one of the most
commonly occurring oral health problems in the children all over the
globe.Unfortunately,many children are afflicted with dentalcaries at an early age.
Even those as young as12 months Decay at this age usually beginsin the deciduous
maxillary incisors but canlater progress to involve primary molars andcanines. Those
affected often suffer froma reduced oral health-related quality of lifewhen contrasted
with their caries-free peers (1,2). Children with rampant dental cariesmay also have
other associated health problems, ranging from local infections to oralpain that
manifests as difficulty eating andsleeping, reduced growth and altered behavior (2,3).
Primary tooth decay does not discriminate. It crosses ethnic and cultural groupingsbut
is generally concentrated among disadvantagedpopulations (4-7). Furthermore, there
is mounting evidence indicating thatchildren who exhibit ECC are more likely tohave
an increased caries experience along thecontinuum of childhood (8-14).6
An especially virulent form of caries is early childhood caries (ECC), affecting
infants and toddlers from 12 to 18 months of age. However, if appropriate measures
Page 24
24
are applied early enough (beginning during pregnancy and infancy), this painful
condition can be prevented (Douglass, Douglass, & Silk, 2004; Finn & Wolpin,
2005). The first dental examination is now recommended between six months and one
year of age (AAPD, 2010c), but this is often unrealistic, especially among the poor
and underinsured. Therefore, there is a huge need for preventive efforts by nurses and
other health care providers who care for infants and young children. The purpose of
this article is to review the literature on the risk factors and prevention strategies for
ECC, and to discuss the role of nurses in preventing this disease process.7
The use of resin pit and fissure sealants has been shown to be an effective
barrier method of preventing caries in pits and fissures over a wide range of studies in
recent decades. Improvements in dental materials have increased retention and
improved technique sensitivity in high caries risk patients. A formal meta-analysis has
demonstrated their efficacy.8
Parents have a major role in preventing dentaldiseases in their children. In
addition, they have amajor role in any preventive measure. Parents'knowledge about
different preventive methodshas been studied previously. Children generally spend
most of their time with parents and guardians, especially mothers, even when they
attend primary-schools or nurseries. These early years involve "primary socialization"
during which the earliest childhood routines and habits are acquired. These include
dietary habits and healthy behaviours established as norms in the home and are
dependent on the knowledge and behaviour of parents and elder siblings. Studies have
reported that poor attitude of parents toward oral health of infants and young children
Page 25
25
are associated with increased caries prevalence (Hind and Gregory, 1995).9
It has been found that the more positive is the parents' attitudes toward
dentistry, the better will be the dental health of their children.Young children's oral
health maintenance and outcomes are influenced by their parent's knowledge beliefs
and practices, which affect oral hygiene and healthy eating habits. Without basic
knowledge of caries risk factors, importance of the deciduous teeth and oral
maintenance, it is difficult to employ effective disease preventive strategies. Parent's
knowledge and positive attitude toward good dental care are very important in the
preventive cycle of dental caries.10
NEED FOR THE STUDY:-
Dental caries can be traced to be as old as civilization with its evidence seen
even in skeletal remnants of prehistoric humans.Dental caries remains the most
common disease affecting humans. Tooth decay is one of the most common of all
disorders, second only to the common cold. It usually occurs in children and young
adults but can affect any person.Numerous studies have reviewed the effectiveness of
different preventive measures in different populations. In spite of these studies,
children still suffer from high cariesincidence. In western countries, the prevalence of
dental caries is low compared to developing countries.11
In 1979, the World Health Assembly adopted a resolution calling for
attainment of "Health for all" by the year 2000. In line with this, the FDI
recommended the establishment of specific oral health schedule on the time scale. Of
the WHO goals for global oral health, the first goal is that 50% of 5-6 years old
Page 26
26
children should be caries free and the second goal is that the global average should
not be more than 3 decayed, missing, or filled teeth at 12 years of age.12
Worldwide, most children and an estimated ninety percent of adults have
experienced caries, with the disease most prevalent in Latin American countries,
countries in the Middle East, and South Asia, and least prevalent in China. In the
United States, dental caries is the most common chronic childhood disease, being at
least five times more common than asthma. It is the primary pathological cause of
tooth loss in children.13
The number of cases has decreased in some developed countries, and this
decline is usually attributed to increasingly better oral hygiene practices and
preventive measures such as fluoride treatment. Nonetheless, countries that have
experienced an overall decrease in cases of tooth decay continue to have a disparity in
the distribution of the disease. Among children in the United States and Europe,
twenty percent of the population endures sixty to eighty percent of cases of dental
carries’ similarly skewed distribution of the disease is found throughout the world
with some children having none or very few caries and others having a high number.
Australia, Nepal, and Sweden have a low incidence of cases of dental caries among
children, whereas cases are more numerous in Costa Rica and Slovakia.14
In 1940, the prevalence of dental caries in India was 55.5% and it rose to 68%
in the 1960s. The prevalence of these diseases is continuously increasing with change
in dietary habit of peoples and increased consumption of sugar. The prevalence of
dental caries is approximately 60% – 65% in India.15
There is a dearth of information on the oral health of pre-school children in
India. Very few data are available on the oral health of pre-school children. Data from
Page 27
27
NOHS 2000 reported a mean Decayed Missing Filled Teeth (DMFT) of 1.40, which
is quite highcompared to that of developed countries in Europe, North America and
Australia Dental caries is a transmissible infectious disease in which Streptococcus
mutans0 is generally considered to be the main etiological agent. Studies using
phenotyping and/or genotyping methods strongly suggest that mother is the major
primary source of infection for children. Improper feeding practices by
mothers/caregivers increase the risk for the development of early childhood caries in
infants and toddlers, by promoting the early establishment of S. mutans in the oral
cavity.16
Young children's oral health maintenance and outcomes are influenced by
their parent's knowledge and beliefs, which affect oral hygiene and healthy eating
habits. Without basic knowledge of caries risk factors, importance of the deciduous
teeth and oral maintenance, it is difficult to employ effective disease preventive
strategies. Parent's knowledge and positive attitude toward good dental care are very
important in the preventive cycle of dental caries.17
Researches showed that the degree to which mothers understand oral health
issues is significantly related to better oral health in their children. In addition,
mothers' knowledge about oral health had an important impact on their children's
future oral health-related practices.18
Based on several literatures and the personal experience of the investigator, it
was found that, mothers lack of knowledge and practices towards dental hygiene
contribute to the high prevalence of dental caries in primary school children.
Page 28
28
Knowledge and practices modifiable factors. It can better modified through health
education and structured teaching programmes. Childhood Caries can be prevented by
successfully educating primary caregivers children about this disease and by thus
motivating them to engage in positive oral health promotion efforts. Researches
showed that the degree to which mothers understand oral health issues is significantly
related to better oral health in their children. In addition, mothers' knowledge about
oral health had an important impact on their children's future oral health-related
practices.19
Hence the investigator felt the need to investigate the effectiveness of a
planned teaching programme on knowledge and practices of dental hygiene on
prevention of dental carries.
Page 30
30
OBJECTIVES
This chapter deals with the statement of the problem, objectives of the study,
operational definitions, assumptions, hypothesis of the study and conceptual
framework which provides a frame of reference. The statement of the study is as
follows
STATEMENT OF THE PROBLEM:
“A study to evaluate the effectiveness of planned teaching programme
regarding knowledge and attitude on prevention of dental caries among mothers of
primary school children at AnekalDistrict Bangalore.”
OBJECTIVES OF THE STUDY;
The objective of the study were to,
1. To assess the pre and post test level of knowledge on prevention of dental caries.
2. To assess the pre test practice on prevention of dental caries
3. To introduce the structured teaching program regarding prevention of dental
caries.
4. To find out the difference between the pre test and post test knowledge on
prevention of dental caries.
5. To find out the difference between the pre test and post test attitude on prevention
of dental caries.
6. To find out the association between the pre tests knowledge on prevention of
dental caries among mothers of primary school children with their demographic
variables.
Page 31
31
OPERATIONAL DEFINITIONS;
1. Evaluate
It refers to the careful appraisal, judgement or examining.
2. Effectiveness
It refers to the degree to which objectives are achieved and the extent to which
targeted problems are solved.
3. Planned Teaching Programme
It refers to the educational programme which is prior planned in an organized
manner.
4. Knowledge
It refers to the intellectual capacity of the mother.
5. Attitude
It refers to the way or manner in which the mother performs in relation to her
child oral hygiene.
6. Prevention
It refers to the measures intended to the protect the child from dental caries.
7. Dental Caries
It refers to the irreversible tooth decay or cavity due to bacterial infection.
Page 32
32
8. Primary school children
It refers to the school children whose age is below 11 years of old.
9. Primay school children mother
It refers to the correct response or judgment of the Mothers of primary school
children on dental hygiene in prevention of dental caries which will be elicited by
administering self administered close ended Knowledge questionnaire.
HYPOTHESIS
H 1 – There will be a significant difference between the pre test and post test
knowledge on prevention of dental caries among mothers of primary school children.
H 2 - There will be a significant association between the pre test and post test
knowledge on prevention of dental caries among mothers of primary school children
with their secured demographic variables.
H 3 - There will be a significant association between the pre test and post test
attitude on prevention of dental caries among mothers of primary school children with
their secured demographic variables.
DELIMITATIONS:
1. The study is delimited to the mothers of primary school children residing at
Anekal District Banglore.
2. The study is delimited to assess the knowledge and attitude on prevention of
dental caries among mothers of primary school children.
Page 33
33
INCLUSION CRITERIA
1. Mothers of primary school children aged between 21- 40 years at selected areas of
Anekal District Bangalore.
2. Mothers of primary school children those who are willing to participate in the
study.
3. Mothers of primary school children who can able to read and write Kannada or
English.
EXCLUSION CRITERIA ;
1. Mothers of primary school children who have already attended IEC package on
dental hygiene.
2. Mothers of primary school children those who are not available during the data
collection period.
3. Mothers of children those who are not studying in primary school.
ASSUMPTIONS ;
1. The mothers of primary school children may have knowledge on prevention of
dental caries.
2. The mothers of primary school children having unfortunable attitude in prevention
of dental caries.
3. Structured teaching programme on prevention of dental caries may enhance the
knowledge and attitude of mothers of primary school children.
Page 34
34
CONCEPTUAL FRAMEWORK:
Conceptual framework acts as building block for the research study. The
overall purpose of framework is to make the scientific finding, meaningful and
generalized. It provides a certain framework of reference for clinical practice,
education and research. Framework can guide the researcher’s undertaking of not only
‘what’ of natural phenomena but also ‘why’ of their occurrence. They also give
direction for relevant questions to practical problems. Conceptual framework is
defined as the frame of reference that serves to guide a research study and is
developed from theories, findings from a variety of other research studies, and the
authors personal experiences and values.
A conceptual model is a group of concepts that are broadly defined and
systematically organized to provide a focus, a rationale, and a tool for the integration
and interpretation of information.20 Conceptual model refers to set of values, beliefs
and preferences for research approach. Conceptual framework plays several
interrelated roles in the progress of science. There overall purpose is to make
scientific meaningful and generalisable. Conceptual frame work is a theoretical
approach to the study of the problem which is scientifically based on the emphasis,
the section arrangement and clarification of the concepts, dealing with the study.
According to Fowcet (1980) a conceptual framework can be defined as set of
concepts and those, assumptions that integrate in to a meaningful configuration.
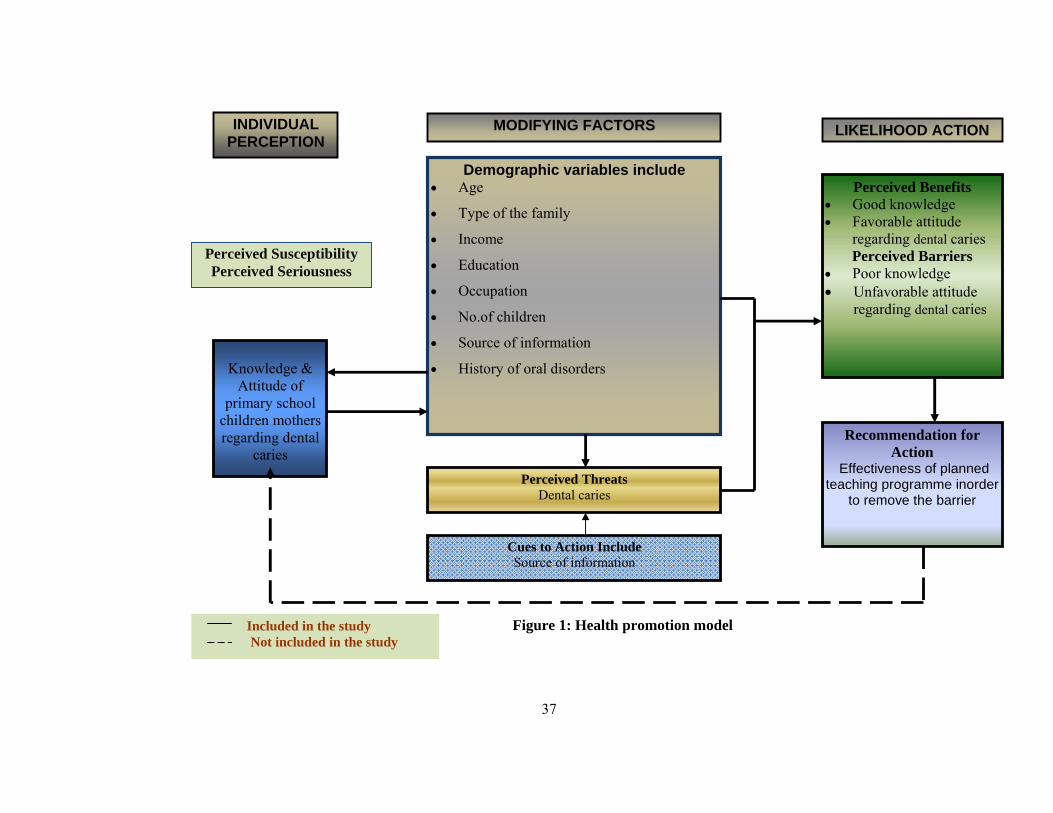
The conceptual frame work chosen for this study is based on the Health
promotion Model. The Pender’s health promotional model about that affects health
promotion behaviour practice. Persons have to initiate and do active roles and this
Page 35
35
behavior is goal directed for raising health and good living. The Pender’s health
promotion model first appears in nursing literature in early 1980s and later the revised
health promotion model appears in 1996. In revised health promotional model, Pender
represents that raising health status and avoiding illness are the major motivational
significance in health promotional behavioral practice.
The model comprised of three primary components, including
Client cognitive-Individual perceptions (perceptual factors)
Modifying factors
Participating in health promoting behaviours( likelihood of initiating or engaging
in action)
Individual Perceptions
Perceived susceptibility: An individual’s estimated probability if encountering a
specific health problem.
Perceived seriousness: The degree of concern on experiences created by the
thought of problem or disease associated with a given health condition. In the
present study perceived susceptibility and perceived seriousness referred to the
problem perceived by the primary school children mothers related to knowledge
and attitude towards dental caries.
Perceived threat: The combined impact of perceived susceptibility and perceived
seriousness refers to the study subjects i.e. primary school children mothers. To
identify the perceived threat, to assess their knowledge and attitude through pre-
tested instrument developed for the study.
Page 36
36
Modifying Factors
A category of variable within the health promotional model is considered to be
of major motivational significance. Furthermore, these variables constitute a critical
care for intervention as they are subject to modification
These include a variety of selected demographic, socio-psychological and
structural factors that predispose the above factors of the primary school children
mothers age, type of the family, family income, education, occupation, number of children,
source of information, history of oral disorders.
The Likelihood of Action
It is the positive difference between perceived benefits and perceived barriers.
In this study perceived benefits is belief about effectiveness of planned teaching
programme recommended action such as adequate knowledge about and positive
attitude towards dental caries acceptances. Perceived barriers are hindrances to
engaging in actions include poor knowledge regarding dental caries and negative
attitude of primary school children mothers towards dental caries.
Likelihood of taking recommendations:
In this study likelihood of taking recommended action is the effectiveness of
planned teaching programme about dental caries in order to remove barrier to action
i.e., poor knowledge and unfavourable attitude towards dental caries.
Feed back: It refers to monitoring and evaluating health promotion activity. This is
not included in the study.
Page 37
37
INDIVIDUAL PERCEPTION
MODIFYING FACTORS LIKELIHOOD ACTION
Knowledge &
Attitude of primary school
children mothers regarding dental
caries
Perceived Susceptibility Perceived Seriousness
Demographic variables include • Age
• Type of the family
• Income
• Education
• Occupation
• No.of children
• Source of information
• History of oral disorders
Perceived Threats Dental caries
Cues to Action Include Source of information
Perceived Benefits • Good knowledge • Favorable attitude
regarding dental caries Perceived Barriers
• Poor knowledge • Unfavorable attitude
regarding dental caries
Recommendation for Action
Effectiveness of planned teaching programme inorder
to remove the barrier
Included in the study Not included in the study
Figure 1: Health promotion model
Page 39
39
REVIEW OF LITERATURE
A review of literature on the research topic makes research familiar with the
existing studies and provides information which helps to focus on a particular
problem and laid foundation up on base knowledge it creates accurate picture of
foundation on the subject. Review of literature done for the study is arranged under
the following headings.
Studies related to dental caries in primary school children
Studies related to mother’s knowledge and attitude on dental caries
Studies related to preventive measures of dental caries in primary school
children
Studies related to effectiveness of planned teaching programme
Studies related to dental caries in primary school children
A cross sectional study was conducted to describe the occurrence of dental
caries and periodontal conditions among standards three and four primary school
children in Morogoro municipality. A total of 1,297 standards three and four children
in five primary schools randomly selected from a list of 36 primary schools. Dental
caries and periodontal status were recorded using the criteria described in the WHO
manual for Oral health Surveys, Basic Methods (1997). Analysis and interpretation
showed that seventy six percent of the children were caries free. No fillings were
encountered. Remaining 29 % 0f the sample were affected with dental caries.20
A study was conducted to describe the Prevalence of dental caries in Italian
primary schoolchildren living in rural and urban areas. The number of surveyed
children were 5413, 8359, 8362 and 5026 in the 6-, 7-, 8- and 9-year-old groups
Page 40
40
respectively. Analysis and interpretation of results showed that the percentages of
children positive for caries were 39.5, 48.3, 54.4 and 60.8 respectively21
A study was conducted to determine the prevalence, severity, and pattern of
dental caries in 6 to 7-year-old children in military primary schools in Jeddah city,
Saudi Arabia. A random sample of 300 children (6 to 7-year-olds) was drawn from
six schools. Clinical examinations were carried out. Caries were diagnosed using the
British Association for the Study of Community Dentistry (BASCD) criteria. Analysis
and interpretation of the results showed that Caries were diagnosed in 288 (96%) of
the children, and only 4% were clinically caries free22
A cross-sectional study of patients referred for a tooth extraction in
one dental surgery in south-east London. Statistical methods consisted of logistic and
ordinal regressions to model the likelihood of exposure to oral health promotion and
of obtaining higher levels of knowledge of oral health issues, respectively. Linear
regression was used to model the level of oral health and knowledge of oral health. In
our observational study, 34% of the patients reported exposure to a settings-based oral
health education programme: Sure Start (5%), NHS (7%) and other (22%). This
exposure was not influenced by age or gender, but an association with education was
detected. Although oral health promotion was not found to influence the actual
knowledge of oral health issues, it was found to influence some oral health-
related attitudes and perceptions.23
A study was conducted in Hawaii for analyzing and a social ecology model
was used to frame the discussion, recognizing family and community influences
on children's oral health. The context of oral health in early childhood contributes to
Page 41
41
the changes in the concept vulnerability. The attributes are closely related to family
and community factors and identified as limited parental income, parental education,
community-based services and fluoride; and exposure to poor parental habits, parental
neglect and harmful toxins. The primary antecedent is identified as a form of limited
protection from exposure to various circumstances.24
A study was conducted in Greece to provide a review of the
existing literature on early childhood caries (ECC) with particular reference on the
nomenclature, case definition, epidemiology, etiology and risk assessment. An
electronic search was used to identify and critically review papers that have been
published and are pertinent to the above issues, evaluate and compile the reported
evidence. The term ECC has been adopted to more accurately describe dental
caries that affects primary dentitions, replacing previously used terminology that
associated the disease with the nursing habit. Suggested ECC case definition uses
caries patterns as defining criteria, however, further refinement to include different
clinical expressions of a varying severity is necessary. Significant percentages of
preschool child populations are affected by ECC today, with the disease concentrating
disproportionately in deprived families. Early colonization by mutants streptococci
(MS) is associated with increased ECC development, with bacteria being transmitted
in both vertical and horizontal ways. Dietary factors related to sugar consumption
predispose to early MS colonization and establishment and increase the risk for ECC
development, being part of the causal chain. Inappropriate bottle and breast-feeding
behaviors also increase the risk, without showing a direct causal relationship. High
risk children belong to ethnic minority groups and to low income families with poor
parental behaviors and attitudes.25
Page 42
42
Studies related to mother’s knowledge and attitude on dental caries
A study was conducted to identify the knowledge of mothers regarding dental
hygiene. Results revealed that 26.7% of mothers of primary school children who
brought their children for extractions of teeth under general anaesthesia to a dental
school did not know how to prevent caries in their children26
A study was conducted to identify the Knowledge of practices on dental
hygiene of primary school children with dental carries. Samples of 139 mothers were
surveyed. Results revealed that 100 out of 139 mothers admitted giving their children
sweets to reward them for good behaviour, to pacify the child, or for no specific
reason27
A study concerning the prevention of caries demonstrated that 80% of the
mothers answered that tooth brushing can prevent dental decay. However, only 46%
of these respondents believed that fluoride could prevent decay. Few mothers
mentioned flossing when asked about oral hygiene practice in their households28
A study was conducted to explore mothers'/guardians' knowledge about how
to promote their children's oral health. Data were collected from 105 mothers/female
guardians.Results revealed that that mothers with lower incomes (under $1000 per
month) had less knowledge concerning the utilization of health care services than
mothers with higher incomes29
A study was conducted in lioyd to determine the effectiveness of providing
free toothpaste containing either 1450 or 440 ppm F on caries experience in 5-year-
old children living in areas with different levels of material deprivation. Toothpaste
containing either 440 or 1450 ppm F and dental health literature posted at 3-month
Page 43
43
intervals and toothbrush provided annually from the age of 1-5 years. Comparison
group received no intervention. A total of 3467 children were included in the final
data analysis. The Townsend index was found to be useful in identifying groups
of children with increased caries risk. Overall, participants in the programmed using
the high-fluoride toothpaste had significantly (P < 0.002) less caries than the
comparison group with similar absolute reductions in mean dmft for the most- and
least-deprived groups. Relative to the comparison group the association between
deprivation and dental caries was changed so that in the most-deprived quartile those
using the low-fluoride toothpaste tended to have less dental caries than the
comparison group whereas in the least deprived they tended to have more. This
difference in the association (slope) was statistically significant (P < 0.05). Provision
of both low- and high-fluoride toothpaste appeared to reduce the risk of extractions
for participants in the most-deprived quartile (P < 0.05).30
A study was conducted in north Carolina to review the evidence for
effectiveness of five possible physician interventions- (1) screening and risk
assessment, (2) referral, (3) provision of dietary supplemental fluoride, (4) application
of fluoride varnish, and (5) counseling-for the prevention of dental caries for the U.S.
Preventive Services Task Force. For most key questions related to the five
interventions, the evidence for primary care clinician effectiveness was rated as poor
owing to the scarcity of studies. Ten surveys of physicians' knowledge and behavior
about fluoride supplementation provided fair evidence, suggesting that
supplementation decisions were often made without consideration of other fluoride
exposures. Reviews of the dental literature identified fair evidence supporting the
effectiveness of both fluoride supplements and varnish, although information
Page 44
44
describing effectiveness and adverse outcomes of supplementation with the most
recent dosage schedule is not available31
A study was conducted to assess the knowledge, attitudes and practices of
caregivers in Kuwait in relation to the oral health of preschool children. Subjects and
Methods: Questionnaires with multiple-choice questions were distributed to 334
caregivers of children under the age of 6 years attending vaccination centers in
Kuwait. For each question, one of the multiple-choice answers was consistent with the
consensus in the pediatric dental literature in relation to early
childhood caries prevention, and was considered to be correct. The χ(2) test,
independent t test, ANOVA, and stepwise linear regression were used to assess the
associations between the variables in question and p ≤ 0.05 was accepted as
statistically significant. Results: Of the 334 participants, 234 (70%) were between 20
and 40 years of age with a high school diploma or higher degree and had between 2
and 5 children. The mean knowledge score was 4.68 ± 1.87, the mean attitude score
was 4.34 ± 0.88 and the mean practice score was 2.45 ± 0.99. Major weaknesses were
reported in infant oral health-related concepts. Mothers had better knowledge than
other caregivers (p < 0.001). Higher education was significantly associated with
better knowledge (p = 0.003) and better practices (p = 0.017). In addition, knowledge,
attitude and level of education were positively and significantly associated with
practices (p < 0.005). Conclusions: Our study showed that caregivers had
weak knowledge and practice in relation to the oral health of preschool
children. Mothers and caregivers with higher education had better knowledge and
practices. Education and attitude appeared to be favorable indicators of the caregivers'
practices with regard to the oral health of their preschool children.32
Page 45
45
Studies related to preventive measures of dental caries in primary school
children
The paper provides a literature review focused on the current methodological
approach to psychosocial and behavioural factors (socioeconomic and demographic
status, education level, health-related attitudes, risk behaviour, stress, oral health and
quality of life) and oral-health indicators (DMFT--Decayed, Missing and Filled teeth;
CPI--Community Periodontal Index, proportion of edentulous subjects, proportion of
subjects in need for dental treatment and SiC Index--Significant Caries Index). The
selected factors are recognized as additional factors associated with oral health and a
detailed investigation thereof represents a novel approach to the prevention of dental
caries and periodontal diseases. The paper also specifies the type of research that is
needed in this branch of the preventive dentistry33
Relatively few health education interventions directed at preventive health
behaviors and management of chronic illness among Native Americans have been
reported in the literature. This article provides a selective review of health education
interventions among Native Americans that address the prevention and management
of chronic illnesses/conditions as well as preventive health behaviors. For each
intervention included in the review, a description of its cultural relevance, sample,
design, and evaluation is provided. Limitations are noted, as well as implications for
research and practice.34
This literature review reports the history and the current market of oral home-
care products. It provides information extending from the products used by our
Page 46
46
ancestors to those currently available, as well as on the changes in the supply and
consumption of these products. Although the scientific knowledge about oral diseases
has improved greatly in recent years, our ancestors had already been concerned with
cleaning their teeth. A variety of rudimentary products and devices were used since
before recorded history, like chewing sticks, tree twigs, bird feathers, animal bones,
tooth powder and home-made mouth rinses. Today, due to technological
improvements of the cosmetic industry and market competition, home-use oral care
products available in the marketplace offer a great variety of options. An increase in
the consumption of oral care products has been observed in the last decades.
Estimates show that Latin America observed a 12% increase in hygiene and beauty
products sales between 2002 and 2003, whereas the observed global rate was
approximately 2%. A significant increase in the per capita consumption of toothpaste,
toothbrush, mouthrinse and dental floss has been estimated from 1992 to 2002,
respectively at rates of 38.3%, 138.3%, 618.8% and 177.2%. Pertaining to this
increased supply and consumption of oral care products, some related questions
remain unanswered, like the occurrence of changes in disease behavior due to the use
of new compounds, their actual efficacy and correct indications, and the extent of the
benefits to oral health35
A study was to determine the associations between changes in self-reported
tooth brushing frequency and the knowledge and attitudes related to oral health. The
study population consisted of all fifth and sixth graders who started the 2001-2002
school year in Pori (n = 1,691); of these, 1,362 were monitored throughout the 3.4-yr
study. Data were gathered by questionnaires before, in the middle, and after the
follow-up, which was divided into two periods. Associations between changes in
Page 47
47
tooth brushing frequency, sum score of knowledge items, and sum scores of items in
attitudinal factors were studied. The attitudinal factor structure was determined by
principal component analyses. The associations were evaluated using mean values
and general linear models for repeated measures. Tooth brushing frequency and
knowledge and attitudes related to oral health improved among the same children
during the study, with the changes usually taking place in the same time-period. In
different time-periods, different children's tooth brushing and oral health-related
knowledge and attitudes improved. Based on our results, changes in knowledge,
attitudes, and behavior are related, but children are ready for change at different times.
Therefore, oral health promotion should be designed to be a continuous process rather
than a short-term intervention.36
A study was conducted in 5-yr double-blind fluoridated milk study has been
completed and, following baseline stratification, 94 children aged 4 1/2/5 1/2 yr were
allocated to the test group and 93 to the control. Each subject received 200 ml school
milk daily, identification between the test and control plastic packs being by colour-
coding alone with the former containing 1.5 mgF- giving a potential topical benefit of
approximately 7 ppmF- per school day. After 5 yr, 50 of the test children remained
and 56 of the controls. While the mean DMFT incremental data relating to permanent
teeth was always in favour of the test group, it was not until the fourth year that a
significant difference was obtained (P less than 0.01) between the fluoridated group
(mean, 1.65) and the non-fluoridated group (mean, 2.56). For permanent teeth which
were unerupted at baseline, the mean DMFS differences increased to 39.6% at the
same time and to 48.0% by the fifth year. No benefit was noted for previously erupted
primary teeth. Cavitation was less in the test group throughout the study. When the
Page 48
48
third, fourth and fifth year DMFT reductions obtained were compared with previously
published artificial water fluoridated data where children were of comparable age at
the onset of water adjustment, similar caries inhibition data were noted.37
A study was conducted for the prevalence of dental caries in 3,6, 9, 12 and 15-
year-old school children of Chandigarh, selected on a randomized basis was evaluated
using Moller's criteria (1966) and correlated with the various risk factors. The mean
deft was found to be 4.0 ± 3.6 in 6 year old and 4.61 ± 3.14 in 9 year old, whereas the
mean DMFT in 12 and 15 year old was found to be 3.03 ± 2.52 and 3.82 ± 2.85
respectively. The high prevalence of dental caries in these children was attributed to
the lack of use of fluoride toothpaste (80% children), lack of knowledge about
etiology of dental caries (98%) and frequency of sugar exposures up to more than five
times per day (30%).38
A cross-sectional study of 1000 preschool children was conducted in Saddar
town, Karachi. Two-stage cluster sampling was used to select the sample. At first
stage, eight clusters were selected randomly from total 11 clusters. In second stage,
from the eight selected clusters, preschools were identified and children between 3- to
6-years age group were assessed for dental caries. Caries prevalence was 51% with a
mean dmft score being 2.08 (±2.97) of which decayed teeth constituted 1.95. The
mean dmft of males was 2.3 (±3.08) and of females was 1.90 (±2.90). The mean dmft
of 3, 4, 5 and 6- year olds was 1.65, 2.11, 2.16 and 3.11 respectively. A significant
association was found between dental caries and following variables: age group of 4-
years (p-value ² 0.029, RR = 1.248, 95% Bias corrected CI 0.029-0.437) and 5-years (p-
Page 49
49
value ² 0.009, RR = 1.545, 95% Bias corrected CI 0.047-0.739), presence of dental
plaque (p-value ² 0.003, RR = 0.744, 95% Bias corrected CI (-0.433)-(-0.169)), poor
oral hygiene (p-value ² 0.000, RR = 0.661, 95% Bias corrected CI (-0.532)-(-0.284)), as
well as consumption of non-sweetened milk (p-value ² 0.049, RR = 1.232, 95% Bias
corrected CI 0.061-0.36739
Studies related to effectiveness of planned teaching programme on dental caries
A study was conducted for variations in tooth eruption patterns are supposed
to have multifactorial reasons and etiologic factors to explain variation in caries are
unsatisfactory. Prevalence of caries is comparatively higher in the children of
developing countries than that of the children of same age in developed countries.
Indian studies on the dental caries mostly in children related to prevalence and
treatment. However, nutritional effect on dental caries on Indian school going
children is yet to be carried out in eastern India. This study investigated the
prevalence of dental caries in permanent teeth and nutritional status among the 544
School going children (girls) of 6 - 19 years age group of Bengalee ethnicity of West
Bengal, India. Caries was recorded based on DMFT index following basic guidelines
for Oral Health Surveys guideline (WHO). Nutritional status was obtained using BMI
and classification of nutritional status was achieved using the standards of WHO and
CDC growth charts include an age- and sex-specific BMI reference for children aged
2 - 20 year. The overall prevalence of dental caries was 44.5% and mean DMFT was
0.45 ? 1.57. Nutritional status demonstrated, about 30% and 6.69% of schools going
girls were underweight and overweight respectively. Occurrence of dental caries was
Page 50
50
found in all permanent teeth among the girls of underweight and normal according to
their BMI-for age status. Furthermore, a significant association (p < 0.05) with
occurrence of dental caries among the underweight girls has been found compared to
that of the overweight and normal. This study indicates a close relationship between
nutritional status and dental caries in this region.40
The study was a community-based, randomized, controlled trial in
schoolchildren aged 6-7 years with untreated dental caries. Participants were
randomly assigned to early (test) or regular (control) dental treatment. The primary
outcome was Weight-for-age Z-score. Secondary outcomes were Height-for-age and
BMI-for-age Z-scores, dental pain, dental sepsis, satisfaction with teeth and child’s
appetite. 86 children were randomly assigned to test (42 children) and control (44)
groups. Mean duration of follow-up was 34.8 (±1.1) weeks. There were insignificant
improvements in anthropometric outcomes between the groups after treatment of
caries. However, treated children had significantly less pain experience (P = 0.006)
(OR 0.09, [0.01-0.51]) and higher satisfaction with teeth (P = 0.001) (OR 9.91, [2.68-
36.51]) compared to controls. Controls had significantly poorer appetites (P = 0.01)
(OR 2.9, [1.24-6.82]) compared to treated children. All treated children were free of
clinical dental sepsis whereas 20% (9 of 44) of controls who were free of sepsis at
baseline had sepsis at follow-up.41
A study was conducted in Birmingham to determine the oral health status of
minority ethnic groups is a critical issue for practitioners in today's multicultural
society. The National Dental Health survey, conducted by the OPCS, provides
Page 51
51
baseline information on the oral health and oral health related behavior of the
population in the United Kingdom but not specifically relating to the minority ethnic
communities. To date, little is known concerning oral health status and self-reported
oral health related behaviors among minority ethnic communities in this country.
Following a review of the published literature, this paper will address two questions:
how has ethnicity been used as a variable by dental researchers and, what is known of
the oral health status of minority ethnic groups Other background variables are
considered which might explain the differences in oral health status between these
communities and the indigenous population, and recommendations are made
concerning further research in this area42
A study was to compare the changes in children's oral health-related behavior,
knowledge, and attitudes obtained using an oral health-promotion approach, a risk-
strategy and promotion approach, and reference area, and to report changes in the
behavior of children between the experimental and the control groups of a randomized
clinical trial (RCT). The study population consisted of all fifth and sixth graders who
started the 2001-2002 school year in Pori, Finland (n = 1,691), where the RCT and
program of oral health promotion were implemented for 3.4 yr. Children with at least
one active caries lesion were randomly assigned to experimental (n = 250) and control
(n = 247) groups. Children in Rauma (n = 807) acted as the reference. Changes in
children's self-reported behavior, knowledge, and attitudes were compared between
groups. The subjects in the oral health-promotion group and in the risk-strategy and
promotion group in Pori tended to show greater improvement in most of their oral
health-related behaviors than those in the reference group, and children in the RCT
experimental group showed greater improvement in most of their oral health-related
Page 52
52
behaviors than those in the RCT control group. Children can be helped to improve
their oral health-related behavior by intervention, including oral hygiene and dietary
counseling, or by implementing a multilevel-approach oral health-promotion
program.4
Page 53
53
METHODOLOGY
Research methodology organizes all the components of the study deals with
the type of research approach used, the setting of the study, the population, sampling
technique, sample selection, the inclusion and exclusion criteria, the development of
Page 54
54
the tool, collection of data, pilot study, procedure of data collection and plan for data
analysis.
RESEARCH APPROACH
The selection of research approach is the basic procedure for the conduction of
research enquiry. A research approach tells us so as to what data to collect and how to
analyze it. It also suggests possible conclusions to be drawn from the data. In view of
the nature of the problem selected for the study and the objectives to be accomplished,
a evaluate approach was considered as the best way to preparation of planned
teaching programme regarding dental caries among primary school children
mothers.Evaluate method was used in this study.
RESEARCH DESIGN
The research design refers to the researcher’s overall plan for obtaining
answers to the research question and its spells out strategies that the researcher
adopted to develop information that is accurate, objective and interpretable.
A evaluate design is used as a research design by the use of one group pre test
post test design in this study as there is a need to conduct pre test and post test of the
knowledge and attitude of primary school children mothers regarding
dental caries.
RESEARCH SETTINGS
Research Setting refers to the area where the study is conducted. It is the
physical location and condition in which data collection takes place in a study. The
Page 55
55
study was conducted in Anekal Taluk st. philomena’s high school selected for the
study on the basis of:
Feasibility of conducting the study
Availability of the samples
POPULATION
Population is the entire aggregation of the cases that meet a designed set of
criteria. In the present study, the populations were primary school children mothers
for attending the PTP in st.philomena’s high school, Anekal, Bengaluru.
SAMPLE
Sample consists of the subject of the population selected to participate in a
research study. In the present study primary school children mothers are selected as
target population or samples of the study.
SAMPLE SIZE
The total sample size of the study consists of 60 primary school children
mothers.
SAMPLING TECHNIQUE;
Sampling refers to the process of selecting the portion of population to
represent the entire population. Subjects were selected from the sampling frame to
achieve non probability purposive sampling technique. In the present study non
probability purposive sampling technique was adopted for 60 primary school children
mothers.
Page 56
56
CRITERIA FOR SAMPLING TECHNIQUE ;
The sampling frame structured by the researcher included the following criteria.
Inclusive Criteria
1. Mothers of primary school children aged between 21- 40 years at selected areas
of Anekal District Bangalore.
2. Mothers of primary school children those who are willing to participate in the
study.
3. Mothers of primary school children who can able to read and write Kannada or
English.
Exclusion criteria
1. Mothers of primary school children who have already attended IEC package on
dental caries.
2. Mothers of primary school children those who are not available during the data
collection period.
3. Mothers of children those who are not studying in primary school.
DATA COLLECTION INSTRUMENTS
Method of data collection includes selection and development of tool, for validity and
reliability and pretesting by administering on few samples, data collection procedure.
SELECTION OF TOOL
Page 57
57
Tool is the instrument used by the researcher to collect the data. A structured
knowledge questionnaire and attitude rating scale was selected based on the objective
of the study as it was considered the best instrument to elicit the responses from the
participnts.
DEVELOPMENT OF TOOL
Based on the objectives of the study, a structured knowledge questionnaire and
attitude rating scales were prepared in order to assess the knowledge and attitude of
primary school children mothers regarding dental caries. After extensive and
systematic review, the investigator has developed the structured knowledge
questionnaire and attitude rating scale.
SOURCES OF TOOL CONSTRUCTION
• Review of literature from books, journals, news paper and on-line source reports
and other publications.
• Discussion with the experts, who included Child health nursing, Statistician, and
refined the investigator’s ideas about the tool preparation.
DESCRIPTION OF TOOL
• The tool consists of a structured knowledge questionnaire and 3 point attitude
scale (likert’s type). It is divided into 3 parts, they are as follows
Part I: The investigator constructed the tool to collect the Socio - demographic data
of the study subjects. It consists of demographic variables.
Page 58
58
Part II: Investigator prepared structured knowledge questionnaire containing 24
knowledge questions regarding denal caries.
• Each correct response was given with score of ‘one’ and wrong answer was given
a score of ‘zero’. The maximum score was 24 and minimum score is Zero. The
respondents were given the questionnaires and placed a tick ( ) to their correct
response.
Part III: Investigator prepared attitude rating scale regarding dental caries consisting
of 16 statements, Attitude statements were given with the range score of 0 to 2 marks.
The maximum score was 32 and minimum score was 0. The respondents were asked
to put a tick ( ) mark to their response.
THE FOLLOWING STEPS WERE UNDERTAKEN FOR PREPARING TOOL
1. CONTENT VALIDITY
Content validity refers to the degree to which an instrument measures what it is
intended to measure. The prepared instrument along with the objectives, blue print
and criteria check list was submitted to 10 experts comprising of in the field of Child
Health Nursing(7), Statistician (1), Paediatrist (1) and Language expert(1) for
establishing the content validity. The tool was modified as per suggestions of the
experts and the final tool was constructed. Later the tool was translated into the local
language, Kannada, without changing the meaning of the tool and it was edited by a
Kannada expert.
2. RELIABILITY
Page 59
59
Reliability of the research instrument was defined as the extent to which the
instrument yields the same results in repeated measures. It was then concerned with
the consistency, accuracy, precision, stability, equivalence and homogeneity.51
The tool after validation was subjected to test for its reliability. The structured
interview schedule was tested for reliability by administering it to 6 primary school
children mothers in Aekal st.philomena’s high school, Bangalore. The reliability of
the tool was computed by using split half Karl Pearson’s correlation formula (raw
score method).
N ∑ XY – (∑ X) (∑ Y)
r1/2 = ------------------------------------------------------
√ [N ∑ X2 - (∑ X) 2] [N ∑ Y2 – (∑ Y)2]
And Spearman Brawn prophecy formula was used.
2 r
rII=
1+ r
rII — reliability co-efficient of correlation of whole test
r — reliability co-efficient of correlation of half test
The reliability co-efficient on knowledge was found to be 0.72 revealing the
tool is feasible for administration for the main study. Since the knowledge reliability
co-efficient is r > 0.84. The tool was found to be reliable and feasible for the main
study.
Page 60
60
The reliability co-efficient on attitude was found to be 0.70 revealing the tool
is feasible for administration for the main study. Since the knowledge reliability co-
efficient is r > 0.82. The tool was found to be reliable and feasible for the main study.
PILOT STUDY
“Pilot study is a small scale version, or trial run, done in preparation for a major
Study”.after obtaining formal administrative permission from Anekal st.philomena’s
high school, The pilot study was conducted from 15.09.12-16.09.12
DATA COLLECTION PROCEDURE
Prior to data collection, permission was obtained from the concerned
authority. The participants were informed about the purpose of the study and written
consent was taken from them. Knowledge and attitude was assessed by using
structured questionnaire on selected primary school children mothers.
THE PLAN FOR DATA ANALYSIS
The data collected from the participant were grouped and analyzed with the
help of statistical analysis. The data analysis was planned to include descriptive and
inferential statistics
DEVELOPMENT OF INFORMATION BOOKLET
The PTP on dental caries and preventive health behavior was developed for the
primary school children mothers in st.philomena’s high school anekal, Bangalore
Page 61
61
The steps involved in the development of PTP were,
1. Preparation of the first draft of PTP
2. Development of attitude scale criteria
3. Pre test of PTP
4. Preparation of the final draft of PTP
Preparation of the first draft of PTP
The PTP was developed according to the objective prepared, the investigator
prepared the overall plan of the PTP and a.v aids, after reviewing the available of
literatures and consulting the experts.
Development of check list criteria
An evaluation criterion was prepared for the content validity of the PTP for
assessing the appropriateness, adequacy, accuracy for formulation of the objectives,
selection and organization of the content, presentation language, feasibility and
practicability.
Pre test of planned teaching programme
Pre testing of the PTP was done by administering the structured questionnaire
to the primary school children mothers in anekal st.philomena’s high school,
Bangaslore
Preparation of the final draft of PTP
The PTP covered the following content are,
Introduction
Page 62
62
Anatomy and physiology of teeth
Definition of dental caries
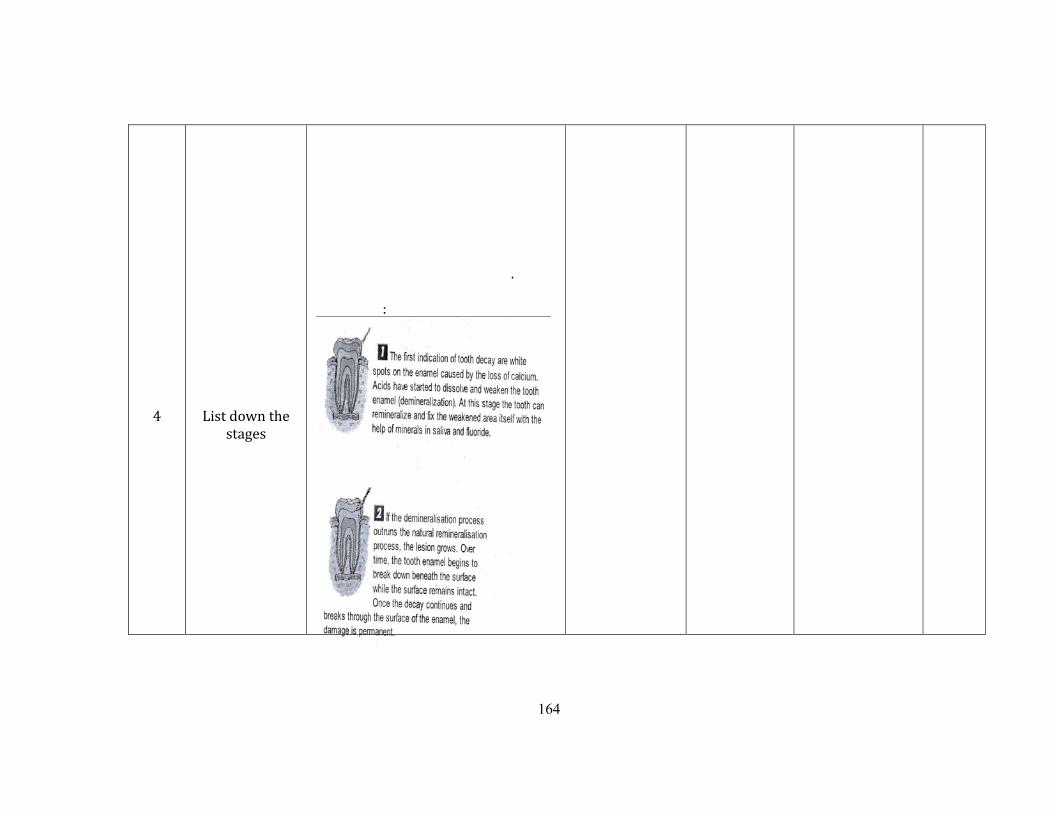
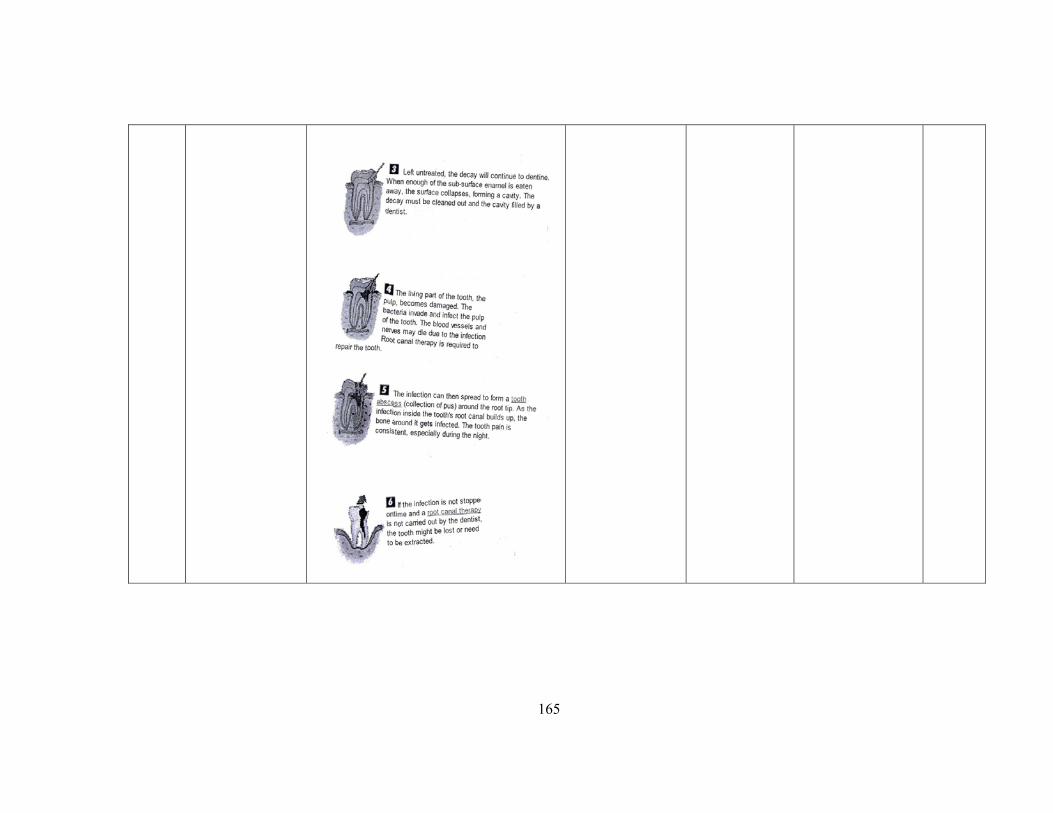
Stages of dental caries
Pathological mechanism
Signs and symptoms
Diagnostic evaluation
Complication
Prevention
The final draft of PTP was prepared based on the suggestions of the experts after
ensuring the validity of the findings of the pre test
Page 63
63
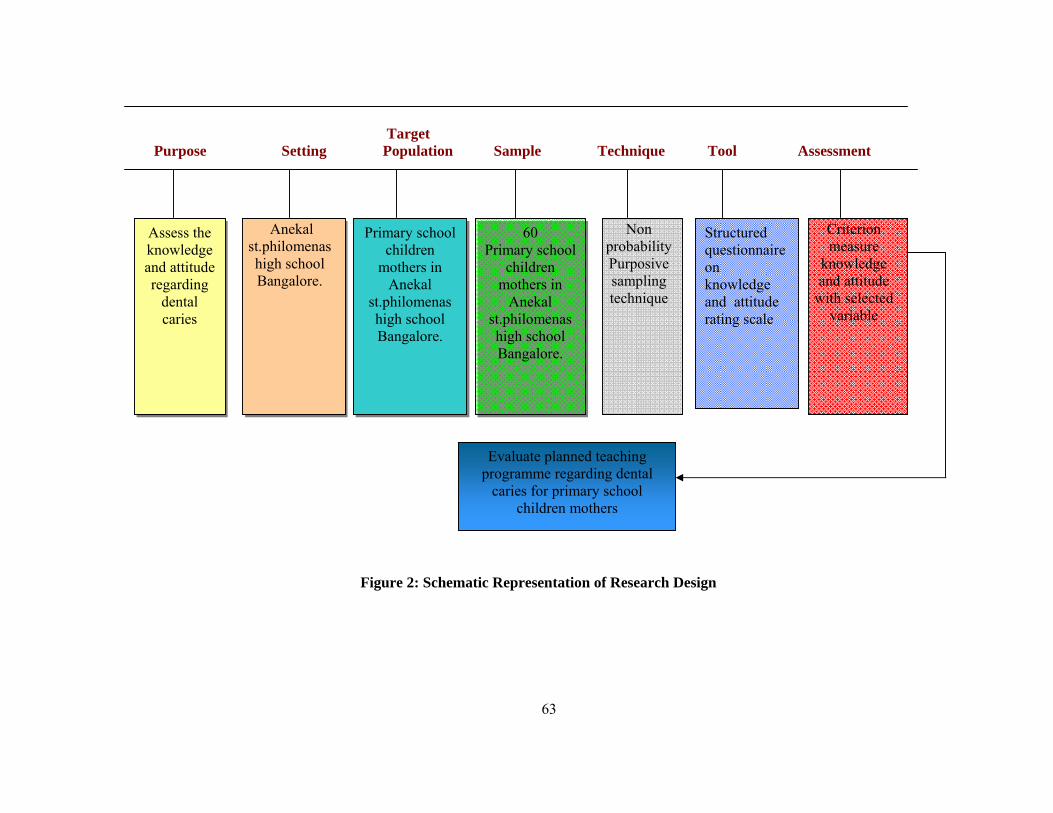
Target Purpose Setting Population Sample Technique Tool Assessment
Figure 2: Schematic Representation of Research Design
Assess the knowledge and attitude regarding
dental caries
Anekal st.philomenas high school Bangalore.
Primary school children
mothers in Anekal
st.philomenas high school Bangalore.
60 Primary school
children mothers in
Anekal st.philomenas high school Bangalore.
Non probability Purposive sampling technique
Criterion measure
knowledge and attitude
with selected variable
Structured questionnaire on knowledge and attitude rating scale
Evaluate planned teaching programme regarding dental
caries for primary school children mothers
Page 65
65
RESULT
Analyzing collected data for the purposes of summarizing information to make
it more usable and/or making generalizations about a population based on a sample
drawn from that population.
This chapter deals with analysis and interpretation of data collected from 60
primary school children mothers regarding dental caries keeping in a view the
objectives of the study use evaluate research approach which was adopted to assess
the knowledge and attitude of the primary school children mothers regarding dental
caries
The data was collected from the respondents before conducting the planned
teaching programme. The collected information was organized, tabulated, analyzed
and interpreted using descriptive and inferential statistics. Analysis was done based on
the objectives and hypothesis of the study.
PRESENTATION OF THE DATA:
The data were presented under the following headings.
Section I : Assessment of knowledge regarding dental caries.
Section II : Assessment of attitude towards dental caries.
Section I11 : Association between pre test and post test of knowledge with
demographic variables.
Section 1V : Relation between knowledge and attitude scores with
Demographic variables.
Section V : Correlation of pre test and post test scores.
Page 66
66
SECTION I
Socio-demographic data
Findings related to socio- demographic variables as described in the study are
age, type of the family, family income, education, occupation, number of children,
source of information, history of oral disorders.
Table 5.1
Frequency and percentage distribution according to age
SL.NO Age (in yrs) Frequency Percentage
1. Below 20 12 12%
2. 21-25 25 25%
3. 26-30 10 10%
4. Above 30 13 13%
TOTAL 60 60%
FIGURE 3: DISTRIBUTION OF RESPONDENTS BY AGE
Page 67
67
The above table shows that out of 60 subjects, 12% were in age group of
below 2 0 yrs,25% were 21 to 25 yrs, 10% were 26 to 30 yrs and 13% in above 30
yrs of age group. The above table shows that majority of the primary school children
mothers were 21-25yrs
Table 5.2
Frequency and percentage distribution according to education.
SL.No Education Frequency Percentage
1. Illiterate 0 0%
2. Up to SSLC 38 38%
3. PUC 14 14%
4. Graduation and above 8 8%
TOTAL 60 60%
Page 68
68
The above table denotes that out of 60 primary school children mothers, 38%
have SSLC, 14% have PUC education and 8% have graduation and above education.
It is observed that majority of primary school children mothers have upto SSLC
education
Table-5.3
Frequency and percentage distribution of according to occupation
SL. No Occupation Frequency Percentage
1. Home maker 18 18%
2. Cooli worker 25 25%
3. Govt employee 10 10%
4. Private employee 7 7%
TOTAL 60 60%
The above table shows that out of 60 primary school children mothers 18%
were home maker, 25% were cooli workers, 10% were govt employes and 7% were
DIDTRIBUTION BASED ON OCCUPATION
Page 69
69
private employees. It is observed that majority of primary school children mothers are
cooli workers
Table-5.4
Frequency and percentage distribution according to Income per month(in
rupees)
SL.No Income Frequency Percentage
1. 1001-2000 0 0
2. 2001-3000 0 0
3. 3001-4000 37 37%
4. 4001 and above 23 23%
TOTAL 60 60%
FIGURE 6: DISTRIBUTION OF RESPONDENTS BY MONTHLY INCOME
The above table shows that out of 60 subjects, 37% were from the income
group of Rs3001-4000 and 23% were from income group of 4001 and above. The
above table shows that majority of them are from income group of Rs 3001-4000.
Page 70
70
The above table shows that out of 60 subjects, 37% were from the income group of
Rs3001-4000 and 23% were from income group of 4001 and above. The above table
shows that majority of them are from income group ofRs 3001-4000.
Table-5.5
Frequency and percentage distribution according to number of children
SL.No No. of children Frequency Percentage
1. 2 18 18%
2. 1 16 16%
3. 3 12 12%
4. Twins 14 14%
TOTAL 60 60%
FIGURE 7: DISTRIBUTION OF RESPONDENTS BY NUMBER OF
CHILDREN
Page 71
71
The above table denotes that out of 60 subjects, 18% were have 2 children,
16% were have 1 child, 12% were have 3 children and 14% were have twins. The
above table shows that majority of them were have 2 children.
Table-5.6
Frequency and percentage distribution according to history of oral disorders.
SL.No Oral disorders Frequency Percentage
1. Mouth ulcer 18 18%
2. Oral sores 16 16%
3. Dental caries 26 26%
TOTAL 60 60%
FIGURE 8: DISTRIBUTION OF RESPONDENTS BY THE HISTORY OF
ORAL DISORDERS
Page 72
72
The above table denotes that out of 60 primary school children mothers, 18%
have oral ulcers, 16% of them have oral sores, 26% of them have dental caries. The
above table shows that majority of them are having mouth ulcers.
Table-5.7
Frequency and percentage distribution according to type of family
SL.No Type of family Frequency Percentage
1. Nuclear 36 36%
2. Joint 16 16%
3. Extended 8 8%
TOTAL 60 60%
FIGURE 9: DISTRIBUTION OF RESPONDENTS BY TYPE OF FAMILY
Page 73
73
The above table denotes that out of 60 primary school children mothers, 36% were
from nuclear family, 16% were from joint family, 8% were from extended family.
The above table shows that majority of them were from nuclear family
Table -5.8
Frequency and percentage distribution according to sources of information
FIGURE 11: DISTRIBUTION OF RESPONDENTS BY SOURCES OF
INFORMATION
SL.No Sources of information Frequency Percentage
1. Mass media 14 14%
2. Friends 13 13%
3. Relatives 10 9%
4. Parents 7 7%
5. Health personel 17 17%
TOTAL 60 60%
Page 74
74
The above table denotes that out of 60 primary school children mothers, 14%
got information from mass media, 13% of them got from friends,9% got from
Relatives and 7% got from parents and.17% got information from health personels.
The above table shows that majority of them got sources of information from health
personnels.
SECTION-II
Findings related to assessment of knowledge regarding dental caries
It deals with the Item wise analysis of primary school children mothers. The
structured questionnaire is used for collecting and analyzing the data. The structured
questionnaire consists of 24 questions related to dental caries. The total scores allotted
were 24. The knowledge assessment is divided in to 3 levels.
Inadequate - below 50%
Moderate - 51-75%
Adequate - above 76%
Table-5.9
Frequency and percentage distribution of primary school children mothers
according to their knowledge assessment
SL.No Level of
knowledge
Frequency Percentage
1. Inadequate 78.3 78.3%
2. Moderate 18.3 18.3%
3. Adequate 3.3 3.3%
Page 75
75
Table 5.10
Aspect wise Mean Knowledge Score related to dental caries
Knowledge Score
No Knowledge No. of questions
Maximum score Mean
Mean (%)
SD (%)
1 dental caries 24 24 23.5 97.96% 13.56
This denotes that the mean of the knowledge score is 23.5, mean % is 97.96
and the Standard deviation is 13.56.
TABLE- 5:11
Aspect wise Mean, S.D and mean% score for the knowledge level
No
AREA
NO OF
ITEMS
MAX
SCORE
MEAN
MEAN
SD
1 Dental
caries
4 4 26 650 1.5
2 stages 4 4 24.8 618.8 1.3
3 Signs and
symptoms
5 5 22.2 444 1.5
4 complication 5 5 22.6 452 1.2
5 prevention 6 6 23.3 388.9 1.8
Table-5-1 Reveals Aspects wise Mean knowledge score of respondents on
dental caries. Regarding introduction to dental caries the mean knowledge score was
Page 76
76
26 & S.D was 1.5, In the aspect of stages the mean knowledge score was 24.8 & S.D
Score was 1.3, regarding signs and symptoms the mean knowledge score was 22.2,
and SD was 1.5, regarding complication the mean knowledge score was 22.6 and SD
was 1.2, regarding dental caries the knowledge score was 3,3 and SD was1.8.
SECTION-III
Findings related to assessment of attitude regarding dental caries
It deals with the Item wise analysis of primary school children mothers. The 3
point Likert’s scale is used for collecting and analyzing the data. This consists of 8
positive and 8 negative statements related to dental hygiene. The total scores allotted
were 32
Table5.12
Aspect wise Mean, Mean% and standard deviation of attitude Scores related to
dental caries
N=60
Score No
Attitude
Aspects Statements
maximum
score Mean Mean (%) SD
I Positive
statements
8 16 6.72 83.96% 10.77
II Negative
statements
8 16 6.37 79.63% 10.02
Combined 16 32 12.63 78.96 11.83
Page 77
77
It reveals that in the positive statements, the mean attitude score was 6.72,
and in the negative statements mean attitude score was 6.37. The combined mean
attitude score is 12.63 and SD
Table5.13
Frequency and percentage distribution of primary school children mothers
according to their Attitude assessment
SL.No Degree of attitude Frequency Percentage
1. Positive
11.7 11.7%
2. Negative 73.3 73.3%
3. Neutral 15 15%
This shows that41% of respondents possessed Negative attitude.17%
possessed neutral and 2% possessed positive attitude.
SECTION IV
Findings related to association between pre test and post test knowledge levels of
primary school children mothers regarding dental caries.
This section deals about the association between knowledge score with the
demographic variables.
Page 78
78
Table 5.14
Association between demographic variables and pre test post test Knowledge
Level of Respondents on dental caries
N=60
Sl
No.
DEMOGRA
PHIC
VARIABLE
S
frequency ≤MEDI
AN
Value
>MED
IAN
Value
X2 DF P
VALU
E
REM
ARK
S
Below 20 7 5
21-25 2 1 4
26-30 5 6
1 Age
Above 30 8 5
9.25 3 7.815 S
Uneducated 0 0
Up to SSLC 27 11
PUC 8 6
Graduation 5 3
2 Education
Postgraduate 3 1
1.078 4 9.488 NS
House wife 13 5
Cooli worker 17 8
Government
employee
6 4
3 Occupation
Private
employee
4 3
0.793 3 7.815 NS
1001-2000 0 0
2001-3000 0 0
3001-5000 24 13
4 Monthly
income
>5000 16 7
0.149 3 7.815 NS
2 15 3
1 9 7
3 10 2
5 Number of
children
twins 6 8
7.95 3 7.815 S
Page 79
79
NS: NON SIGNIFICANT S:SIGNIFICANT AT 5% LEVEL
Data is presented in the table indicated, association between demographic
variables and pre test post test knowledge level of respondents regarding dental caries.
There exists a significant association between knowledge score on dental caries
among primary school children mothers and the selected demographic variable such
as age, education,income, occupation,number of children,history of dental disorders,
type of family, and source of information found.
6 History of
oral
disorders
Mouth ulcers 10 8 5.568 2 5.991 S
Oral sores 9 7
Dental caries 21 5
Type of
family
Nuclear
family
28 8 5.998 2 5.991 S
Joint family
7 9
Extended
family
5 3
Sources of
information
Mass media
10 3 7.080 4 9.488 NS
Friends
5 8
Relatives
7 2
Parents
6 1
Health
personnels
12 5
Page 80
80
SECTION V
Findings related to association between pre test post test attitude and
demographic variables
Table 5.15
Association between demographic variables and pre test post test attitude Level
of Respondents on dental caries,
no DEMOGRAP
HIC
VARIABLES
frequency ≤ME
DIA
N
value
>MEDI
AN
value
X2 DF P
VAL
UE
RE
MA
RKS
Below 20 0 8
21-25 14 5
26-30 18 4
1 Age
Above 30 8 3
18.72 3 7.815 S
Uneducated 0 0
Up to SSLC 15 7
PUC 17 9
Graduation 5 3
. Education
Postgraduate 3 1
0.2053 4 9.488 NS
House wife 23 8
Cooli worker 7 6
Government
employee
5 2
3. Occupation
Private employee 5 4
2.33 3 7.815 NS
1001-2000 0 0
2001-3000 0 0
3001-5000 25 10
4. Monthly
income
>5000
15 10
0.878 3 7.815 NS
Page 81
81
NS: NON SIGNIFICANT S:SIGNIFICANT AT 5% LEVEL
Data is presented in the table in`icated, association between demographic
variables and pre test post test attitude level of respondents regarding dental caries.
There exists a significant association between attitude score on dental caries among
primary school children mothers and the selected demographic variable such as
age,number of children,history of dental disorders,type of family education,
occupation, monthly income and source of information found.
2 18 6
1 15 5
3 3 4
5. Number of
children
twins 4 5
5.75 3 7.815 NS
Mouth ulcer 11 13
Oral sores 9 5
6. History of
dental
disorders Dental caries 20 2
10.508 2 5.991 S
Nuclear family 25 20
Joint family 9 10
7.
Type of family
Extended family 6 18
0.565 2 5.991 NS
Mass media
6
7 23.73 4 9.488 S
Relative
15 1
Parent
10 3
8. Sources of
information
Health personnels
7 2
Page 82
82
SECTION VI
Findings related to Correlation between knowledge score and attitude score
regarding dental caries
This deals with the findings related with the correlation between knowledge
score and attitude score.
Table 5.16
Distribution of Respondents and Relationship between Knowledge and Attitude
Scores
N=60
Knowledge Attitude
Category Number Percent Category Number Percent
Inadequate 78.3 78.3 Negative 73.3 73.3
Moderate 18.3 18.3 Neutral 11.7 11.7
Adequate 3.4 3.4 Positive 15 15.0
Combined 100 100.0 Combined 100 100.0
Page 83
83
It represents that 78.3% of the respondents had the inadequate knowledge;
18.3% of the respondents had moderate knowledge and 3.4% had adequate
knowledge regarding dental caries. With respect to attitude towards dental caries
73.3% of the respondents possessed Negative attitude, 11.7% of the respondents’
possessed neutral attitude and 15 % possessed positive attitude regarding dental
caries.
Table 5.17
Correlation between pre test and post test scores
This shows that mean of the pre test score is 23.5 and post test mean is
12.6.The standard deviation of pre test score is 13.6 and standard deviation of post test
score is 11.8. The correlation between pre test score and post test score is + 0.894274.
This proved the pre test score and post test scores are highly correlated with each
other.
ITEMS MEAN STANDARD
DEVIATION
CORRELATION
Pre test 23.51 13.56
Post test 12.63 11.83
0.894274
Page 85
85
DISCUSSION
A report of findings is never sufficient to convey their significance. The
meaning that researchers give to the results plays a rightful and important role in the
report. The discussion section is devoted to a thoughtful and insightful analysis of the
finding, leading to a discussion of their home and theoretical utility. The findings of
the study have been discussed with reference to the objectives and hypothesis stated.54
The aim of the present study was to assess the knowledge and attitude of the
primary school children mothers regarding dental caries those who are in
st.philomena’s high school, Bengaluru. A total of 60 primary school children mothers
from st.philomena’s high school children were selected for the study by using non
probability purposive sampling method. Structured questionnaire for knowledge and
rating scales for attitude was given to all the subjects.
The findings are discussed under the demographic characteristics and objectives.
Description of demographic characteristics of the sample
Findings of the revealed that majority of the subjects were (25%) in the age
group of 21- 25years, majority of the subjects (38%) had upto SSLC education and
majority of the respondents (25%) were coolie worker. 37% of the family income falls
between Rs. 3001 -4000. Majority of respondents were have 2 children (18%).26%of
the samples have mouth ulcer, 36% samples were from nuclear family. Majority of
them got information from health personnels about dental caries.
Page 86
86
A study conducted by kosika K, chowska A and przybos A (2005) on attitude
of primary school children mothers towards dental caries related to the study of forms
and preparation and preference. Samples were the 275 primary school children
mothers in Puck high school in Warsaw was assessed in the period of July 2003 to
February 2004.This revealed that the dental caries was very popular among better
educated women from big cities, while those with lower education from small cities
and villages.44
A study by Schröcksna H, Kunziky V, Brezinka C and Oberaigner W(2004)
cited in Australia. Samples were 265 primary school children mothers.So dental caries
is considered to be a safe method for a healthy teeth. This study proved that attitude of
the women was depending upon the educational level. 45
Similarly in present study demographic data included were Age,
Occupation,no.of children, Income, type of family and Source of information.
The first objective of the study was to assess the knowledge of primary school
children mothers regarding dental caries.
In this study the results revealed that out of 60 primary school children
mothers 73.3 (73.3%) had inadequate knowledge, 11.7(11.7%) women had
moderately knowledge and 15 of the primary school children mothers had adequate
knowledge regarding dental caries. These findings are supported by the following
study.
Page 87
87
A study was conducted by Made RM, Fourur MJ(2005) bon women's
experience of giving adequate care for their family. This study aimed to give
importance to women's experiences and knowledge of dental caries. The sample was
five women from a large urban region in New Zealand, who give adequate care for
their family, at home and in hospital. The knowledge increases their confidence to for
giving care for their family. Women's knowledge contributes an important part in this
study.46
The second objective of this study was to determine the attitude of the primary
school children mothers regarding dental caries.
In present study results revealed that out of 60 primary school children
mothers, 78.3 (78.3%) women had negative attitude, 18.3(17%) and 3.4 (3.4%) had
positive attitude, towards dental caries.
A study was conducted by Halsm and Holloway IM(1995) to examine primary
school children mothers experiences in dental caries. This was an exploratory study
and setting of the study was a peadiatric unit of a local general hospital set in a semi-
rural location in England. Nine women were participated in this study. This study
concluded that all women participated in the study had a positive attitude towards
dental caries.47
The Third of objective of the study was to find out the correlation between the
pre test post test knowledge & attitude of primary school children mothers
regarding dental caries.
Page 88
88
The correlation between pre test post test knowledge score and attitude score
regarding dental caries is 0.883574.So this is highly correlated with each other.
A study by Richard H conducted in London (2004) to assess the awareness of
primary school children mothers regarding dental caries. This study showed the
knowledge and attitude of primary school children mothers regarding dental caries. A
sample of 189 mothers who were experienced dental care taken for this survey. Most
women desired dental hygiene and dental caries as they have inadequate knowledge
and attitude.48
The fourth objective of the study was to find out the association between the pre
test post test knowledge and attitude scores with selected demographic variables.
1. Knowledge scores
The significance associations of knowledge with the selected demographic
variables in this study are age,education, occupation,no.of children,history of
dental disorders,type of family, and source of information.
Age - The value of X2 found significant at the level of 5% (X2 = 9.248 at P>0.05
level).
Occupation – The value of X2 found non significant at the level of 5%(X2 = 0.793 at
P<0.05 level).
Education- The value of X2 found to be statistically non significant at the level of 5%
(X2 = 1.078 at P<0.05 level).
Number of children- The value of X2 found to be statistically significant at the level
of 5% (X2 = at 5.568 P>0.05 level).
Page 89
89
Religion- The value of X2 found to be statistically significant at the level of 5% (X2 =
7.968 at P>0.05 level).
Source of information-The value of X2 found to be statistically significant at the level
of 5%(X2 = 7.0808 at P>0.05 level).
A study conducted by Julett, Burns(2008)for assessessing the knowledge and
attitude of women related to their information about dental caries. This study cited at
High field, United Kingdom and samples were 3146 primary school children
mothers.The fact is that adequate dental care is carried out according to their sources
of information.49
2. Attitude Scores
The significance association of attitude with the selected demographic
variables in this study are Age, Education,Occupation,number of children,history of
dental disorders and source of information.
Age- The value of X2 found to be statistically significant at the level of 5%. (X2
=18.72 at P>0.05 level).
Education- The value of X2 found to be statistically non significant at the level of 5%.
(X2 = 0.205 at P<0.05 level).
Occupation- The value of X2 found to be statistically non significant at the level of
5%. (X2 =2.33 at P<0.05 level).
Number of children- The value of X2 found to be statistically non significant at the
level of 5%. (X2 =5.75 at P<0.05 level).
History of dental disorders- The value of X2 found to be statistically significant at the
level of 5%. (X2 = 10.51 at P>0.05 level).
Page 90
90
Source of information -The value of X2 found to be statistically significant at the level
of 5%. (X2 = 23.73 at P>0.05 level).
A study was conducted by R Dällenbch , .Martens (2003) to identify Pros and
cons and the attitude of primary school children mothers towards dental caries. This
was conducted in Basel, Switzerland. This study showed that the primary school
children mothers needed all the information to develop good attitude from the
professionals. so the information have a significant role in developing good attitude
towards dental caries. 50
Page 92
92
CONCLUSION
On the basis of findings of the study the below set conclusions were drown. It
also brings about the limitations of study in to practice. The implications are given on
the various aspects like nursing education, nursing practice, nursing administrations
and it also gives insight in to the future studies.
Many studies show that there is a lack of knowledge and negative attitude
regarding dental caries among primary school children mothers. Planned teaching
programme is the one of the best method to improve knowledge and attitude
regarding dental caries among primary school children mothers.
The knowledge and attitude of primary school children mothers regarding
dental caries was inadequate and negative when assessed. So planned teaching
programme was given to maintain the adequate knowledge and positive attitude.
The study was based on the Pender’s health belief model (1996). It is one of
the most widely used models to explain why people do or do not take preventive
health actions.
Implications of the Study
The findings of the study have implications in the field of nursing practice,
nursing education, nursing administration and nursing research.
Page 93
93
1. Nursing Practice
• Nursing professionals working in the community as well as in the hospital
should educate regarding dental caries for reducing the dental problems.
• Nursing professionals play a key role in enhancement of knowledge of dental
caries, which could change the attitude and practice towards the dental
hygiene and dental caries
2. Nursing Education
• Nursing education is to bring changes in the behaviour of people so as to
prepare them to play their roles effectively as an individual and as a good
responsible citizen.
• As a nurse educator, there are abundant opportunities for nursing professionals
to educate the primary school children mother as well as to the married
women regarding dental hygiene and dental caries
• The study emphasizes significance of short term in service education
programmes for nurses and peripheral health workers to educate for adopting
dental caries
3. Nursing Administration
• Nursing administration is to organise and direct human and material resources
to achieve desired nursing outcomes.
• The nursing administrator can take part in developing protocols, regarding the
health education programmes and strategies for primary school children
mothers regarding dental caries
Page 94
94
• The nursing administrator can mobilize the available resource personnel
towards the health education of primary school children mothers regarding
dental caries
• The nurse administrators should explore their potentials and encourage
innovative ideas in the preparation of appropriate teaching material. She
should organize sufficient manpower; money and material for disseminating
health information.
4. Nursing Research
• Nursing research is to explore new solutions and remedies for overcome the
health related problems of dental caries
• This study helps nurse researchers to educate the primary school mothers to
participate in adopting this alternative method according to their demographic,
socio-economic, cultural and political characteristics.
• Nurses should come forward to carryout studies on dental caries and publish
them for the benefit of public and nursing fraternity. The public and private
agencies should also encourage research in this field through materials and
funds.
Limitations of the Study
• The study is limited only primary school children mothers in selected high
school.
• The sample size was limited to 60 primary school children mothers.
• The study period is 4-6 weeks only.
Page 95
95
Recommendations
On the basis of the findings of the study following recommendations have been
made:
• A similar study can be replicated on a large sample to generalize the findings.
• A quasi-experimental study can be undertaken with a control group for
effective comparison of the result.
• A study can be conducted by including additional demographic variables.
• Manuals, self-instruction module may be developed in areas of dental caries
among primary school children mothers.
• A study can be carried out to evaluate the efficiency of various teaching
strategies like SIM, pamphlets, leaflets and computer-assisted instruction on
dental caries.
Page 97
97
SUMMARY
This chapter presents the summary of the study, its discussion, conclusion, its
nursing implications and recommendations.
• This is a descriptive study on assessing the knowledge and attitude of primary
school children mothers regarding dental caries. A sample of 60 primary
school children mothers was selected by using non probability purposive
sampling. It was concluded that primary school children mothers have
inadequate knowledge and negative attitude regarding dental caries.
OBJECTIVES OF THE STUDY:-
The objectives of the study to:
1. To assess the pre and post test level of knowledge on prevention of dental caries.
2. To assess the pre test practice on prevention of dental caries
3. To introduce the structured teaching program regarding prevention of dental
caries.
4. To find out the difference between the pre test and post test knowledge on
prevention of dental caries.
5. To find out the difference between the pre test and post test attitude on prevention
of dental caries.
6. To find out the association between the pre tests knowledge on prevention of
dental caries among mothers of primary school children with their demographic
variables.
Page 98
98
HYPOTHESIS:-
H 1 – There will be a significant difference between the pre test and post test
knowledge on prevention of dental caries among mothers of primary school children.
H 2 - There will be a significant association between the pre test knowledge on
prevention of dental caries among mothers of primary school children with their
secured demographic variables.
H 3 - There will be a significant association between the pre test and post test
attitude on prevention of dental caries among mothers of primary school children with
their secured demographic variables.
CONCEPTUAL FRAME WORK:-
The investigator selected conceptual framework was based on the Pender’s
health belief model (1996). It is one of the most widely used models to explain why
people do or do not take preventive health actions.
STUDY SETTINGS:-
The study was conducted at Anekal st.philomena’s high school on the month
of November 2012.The study was a descriptive survey type. The data was collected
from 60 samples through Non probability Purposive sampling technique. It was
conducted during the period of 15-10-2012 to 20-10-2012.
The sample of this study comprised of 60 primary school children mothers at
Anekal st.philomena’s high school. Non Purposive sampling technique was used to
draw the sample for the study.
Page 99
99
The tool developed and used for the data collection. 7 experts validated the
content validity of the tool and the tool was found to be reliable and feasible. The
reliability of the knowledge tool was established by Karl Pearson coefficient of
correlation and that was .85 and attitude tool reliability was .64.
Pilot study was conducted as a part of the major study, tool proved to be
comprehensive, feasible and acceptable. After obtaining written permission from
concerned authorities, the main study data was collected by using structured
knowledge questionnaire and 3 point likert’s attitude scale from 25th November to 30th
November 2011.
The tool used for assessment consists of
SECTION-A
Demographic variables which include Age,number of children, Education, Occupation,
Income,history of dental problems, Type of family, Sources of information.
SECTION-B
Knowledge questionnaire regarding dental caries which consist of 24items ,
SECTION-C
3 point likert’s Attitude scale regarding dental caries consist of 16 items. It includes 8
positive and 8 negative attitude statements.
The data gathered were analyzed and interpreted according to objectives.
Descriptive statistics like mean, and standard deviation. And inferential statistics like
χ2-test were included to test the hypothesis at different levels of significance and the
data obtained are presented in the graphical form.
Page 100
100
Major findings of the study
The following conclusions were drawn on the basis of the findings of the study:
Finding related to demographics characteristics
• Majority of the subjects were (25.0%) in the age group of 21-25years followed by
13.0% in above 30 years and 12.0% in below 20 age group.
• Majority of the subjects (38.0%) had SSLC education followed by 14% had PUC
education as educational status.
• Majority of the respondents (25.0%) were Coolie workers.
• Most of the respondents (37.0%) had family income between ’3001 - 4000.
• Majority of respondents were have 2 children (18.0%).
• Majority of respondents were have mouth ulcer (26.0%).
• Majority of respondents were from nuclear family (36.0%)
• Majority of respondents got information from(17%) health personnels.
Finding related to knowledge and attitude of primary school children
mothers
• In this study out of 60 primary school children mothers, 73.3(73.3%) had
inadequate knowledge, 11.7(11.7%) women had moderately knowledge and
15(15%) of the primary school children mothers had adequate knowledge
regarding dental caries. The respondent’s mean knowledge score is 97.96%.
• In this study out of 60 primary school children mothers, 78.3 (78.3%) women had
negative attitude,18.3(18.3%) women had neutral attitude and 3.4 (3.4%) had
Page 101
101
positive attitude towards dental caries. The respondent’s mean attitude level
showed is 78.96% .
Finding related to association of pre test post test knowledge and attitude
scores of primary school children mothers with selected demographics
variables
• There is a significant association between Age and knowledge at the level of 5%
(X2 =9.25 at P>0.05 level).
• There is no significant association between Occupation and knowledge at the level
of 5% (X2 = 0.793 at P<0.05 level).
• There is no significant association between Education and knowledge at the level
of 5% (X2 = 1.078 at P<0.05 level).
• There is a significant association between number of children and knowledge at
the level of 5% (X2 = 5.568 at P>0.05 level).
• There is a significant association between Type of family and knowledge at the
level of 5% (X2 = 5.993 at P>0.05 level).
• There is a significant association between history of dental problems and
knowledge at the level of 5% (X2 = 7.862 at P>0.05 level).
• There is no significant association between Source of information and knowledge
at the level of 5%(X2 = 7.08at P<0.05 level).
Finding related to correlation between pre test post test knowledge and
attitude scores of primary school children mothers regarding dental caries
Page 102
102
There is a positive significant relationship between knowledge and attitude of
respondents on dental caries (r = +.0.883574).So this is highly correlated with each
other.
Page 103
103
LIST OF REFERENCES
Page 104
104
1. Filstrup SL, Briskie D, da Fonseca M, Lawrence L,Wandera A, Inglehart MR.
Early childhood caries and quality of life: child and parent perspectives.
PediatrDent 2003;25:431-440.
2. Low W, Tan S, Schwartz S. The effect of severe caries on the quality of life in
young children.PediatrDent 1999;21:325-326
3. Acs G, Lodolini G, Kaminsky S, Cisneros GJ. Effectof nursing caries on body
weight in a pediatric population.Pediatr Dent 1992;14:302-305.
4. Milnes AR. Description and epidemiology of nursing caries. J Public Health Dent
1996;56:38-50.
5. Downer MC. The 1993 national survey of children’s dental health. Br Dent J
1995;178:407-412.
6. Hallett KB, O’Rourke PK. Social and behavioural determinants of early childhood
caries. Aust Dent J 2003;48:27-33.
7. Jose B, King NM. Early childhood caries lesions in preschool children in Kerala,
India.Pediatr Dent 2003;25:594-600.
8. Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth:
an eight-year cohort study. J Dent Res 2002;81:561-566.
9. Kaste LM, Marianos D, Chang R, Phipps KR. The assessment of nursing caries
and its relationship to high caries in the permanent dentition. J Public Health Dent
1992;52:64-68.
10. Johnsen DC, Gerstenmaier JH, DiSantis TA, Berkowitz RJ. Susceptibility of
nursing-caries children to future approximal molar decay.Pediatr Dent 1986;8:
168-170.
11. al Shalan TA, Erickson PR, Hardie NA.Primary incisor decay before age 4 as a
risk factor for future dental caries.Pediatr Dent 1997;19:37-41.
Page 105
105
12. Peretz B, Ram D, AzoE, Efrat Y. Preschool caries as an indicator of future caries:
a longitudinal study. PediatrDent 2003;25:114-118.
13. Holbrook WP, de Soet JJ, de Graaff J. Prediction of dental caries in pre-school
children. Caries Res 1993;27:424-430.
14. Sclavos S, Porter S, Kim SW. Future caries development in children with nursing
bottle caries. J Pedod1988;13:1-10.
15. Holm AK. Caries in pre-school children: international trends. J Dent 1990;291-5.
16. Hinds K, Gregory JR. National diet and nutrition survey: Children aged 11/2 to 4
½ years. Report of dental survey.Vol. 2. London: HMSO; 1995.
17. 17.Friedman LA, Mackler IG, Hoggard GJ, French CI. A comparison of perceived
and actual dental needs of a selected group of children in Texas. Community Dent
Oral Epidemiol1976;4:89-93.
18. Finlayson TL, Siefert K, Ismail AI, Sohn W. Maternal self-efficacy and 1-5 year
old children's brushing habits. Community Dent Oral Epidemiol 2007;35:272-81.
19. National Oral Health Policy: JIDA 1986;58:397-401.
20. Chawla H.S: Dental health promotion, reaching the needy: JIDA 1985;57:387-
95.
21. Oral health, ICMR Bulletin, 1994;24:4.
22. National Oral Health Survey. Dental Council of India, New Delhi: 2002 -03.
23. Holm AK. Caries in pre-school children: international trends. J Dent 1990;291-5.
24. Berkowitz RJ. Mutans streptococci acquisition and transmission.Peadiatr Dent
2006;28:106-9.
25. Dental caries and periodontal conditions among primary school children in
Morogoro municipality, Tanzania. Kikwilu EN, Mandari GJ 2002
Page 106
106
26. Institute of Dental Research, First Faculty of Medicine, Charles University,
General Teaching Hospital, Prague, Czech Republic. [email protected]
27. Department of Health Behavior and Health Education, University of Michigan,
Ann Arbor 48109-2029.
28. Department of Social and Preventive Dentistry, School of Dentistry, Federal
University of Rio Grande do Sul, Porto Alegre, RS, Brazil.
29. Department of Community Dentistry, Institute of Dentistry, University of Oulu,
Oulu, Finland. [email protected]
30. Tewari A, Chawla HS. A study of prevalence of dental caries in an urban area of
India, Chandigarh. J Indian Dent Assoc 1977;49:231-7
31. Department of Community Dentistry, Dr, Ishrat Ul Ebad Khan Institute of Oral
Health Sciences, DUHS, Rafiqui Shaheed Road, Karachi, Pakistan.
[email protected]
32. Alvarez, J. O., Eguren, J. C, Caceda, J. & Navia, J. M. (1990). The effect of
nutritional status on the age distribution of dental caries in the primary teeth.
Journal of Dental Research, 69, 1564-1566. doi:10.1177/00220345900690090501
33. CDC Data & Statistics | Feature: Untreated Dental Caries (Cavities) in Children
Ages 2-19, United States [Internet]. [cited 2012 Feb 25].
34. Available from: http://www.cdc.gov/Features/dsUntreatedCavitiesKids/
35. US Department of Health and Human Services. Agency for Health Care Policy
and Research. Acute Pain Management: operative or medical procedures and
trauma. Rockville (MD): The Agency; 1993. Clinical Practice Guideline No.1.
AHCPR Publication No. 92-0023. p.107.
Page 107
107
36. Pitts NB, Nugent ZJ, Davies JA. The Scottish Health Boards’ Dental
Epidemiological Programme Report of the 1997/98 survey of 5 year old children.
Dundee: University of Dundee, 1998.
37. Pitts NB, Nugent ZJ, Smith PA. The Scottish Health Boards’ Dental
Epidemiological Programme Report of the 1998/99 survey of 14 year old children.
Dundee: University of Dundee, 1999.
38. Pitts NB, Binnie V, Gerrish AC, Mackenzie NM, Watkins TR. Dental Caries in
Children. Scottish Needs Assessment Programme Report. 1994, Scottish Forum
for Public Health, Glasgow.
39. Pitts NB, Binnie V, Gerrish AC, Stevenson J. Dental Caries in Children (Update).
Scottish Needs Assessment Programme Report. 1998, Scottish Forum for Public
Health, Glasgow.
40. Field MJ, Lohr KN (editors) Clinical practice guidelines: directions for a new
program. Washington (DC): National Academy Press; 1990. Committee to Advise
the Public Health Service on Clinical Practice Guidelines, Institute of Medicine
41. Scottish Intercollegiate Guidelines Network. SIGN guidelines: an introduction to
SIGN methodology for the development of evidence-based clinical guidelines.
Edinburgh: SIGN; 1999 (SIGN publication no. 39).
42. Disney JA, Graves RC, Stamm JW, Bohannan HM, Abernathy JR, Zack DD. The
University of North Carolina Caries Risk Assessment Study: further developments
in caries risk prediction. Community Dent Oral Epidemiol 1992; 20: 64-75.
43. Faculty of General Dental Practitioners (UK) Working Party. Selection Criteria
for Dental Radiography. London: Faculty of General Dental Practitioners (UK)
The Royal College of Surgeons of England, 1998.
Page 108
108
44. Seppa L, Hausen H, Pollanen L, Helasharju K, Karkkainen S. Past caries
recordings made in Public Dental Clinics as predictors of caries prevalence in
early adolescence. Community Dent Oral Epidemiol 1989; 17: 277-81.
45. Stecksen-Blicks C, Gustafsson L. Impact of oral hygiene and use of fluorides on
caries increment in children during one year. Community Dent Oral Epidemiol
1986; 14: 185-9.
46. Hackett AF, Rugg-Gunn AJ, Appleton DR. Sugar consumption of Northumbrian
children aged 11-14 years. Nutr Health 1987; 5: 19-23.
47. Serra Majem L, Garcia Closas R, Ramon JM, Manau C, Cuenca E, Krasse B.
Dietary habits and dental caries in a population of Spanish schoolchildren with
low levels of caries experience. Caries Res 1993; 27: 488-94.
48. Gustaffson BE, Quensel CE, Lanke LS, Lundquist C, Grahnen H, Bonow BE,
Krasse B. The Vipeholm dental caries study. The effect of different levels of
carbohydrate intake on caries activity in 436 individuals observed for five years.
Acta Odont Scand 1954; 11: 232-364.
49. Newbrun E. Frequent sugar intake - then and now: interpretation of the main
results. Scand J Dent Res 1989; 97: 103-9.
Page 110
110
LIST OF ANNEXURES
Sl.No
Annexure Page. No
1 Letter seeking permission for conducting the study 110
2 Certificate of content validity 111
3 Letter seeking experts opinion for the content validity of the tool
used for the study 112-113
4 Scoring key 114-115
5 Tool for data collection 116-173
6 Blue print of the tool 174
7 Letter requesting permission to conduct the piolot study 175
8 Letter granting permission to conduct piolot study 176
9 Letter requesting permission to conduct the main study 177
10 Letter granting permission to conduct main study 178
11 Letter seeking consent of the subjects for participation in the study 179
12 List of experts who validated the tool 180
13 Certificate of editing 181
Page 111
111
ANNEXURE-I
LETTER SEEKING PERMISSION FOR CONDUCTING THE STUDY
Ref. No: - Date:-
To,
The principal,
St.philomena’s high school,
Anekal,
Bangalore-562106
Respected Sir\Madam,
Sub: - Letter seeking permission for conducting the study.
Ms Anju Appukuttan is a student of Msc Nursing in our college. She is
conducting a study on “A study to evaluate the effectiveness of planned teaching
programme regarding knowledge and attitude on prevention of dental caries among
mothers of primary school children at AnekalDistrict Bangalore.’’
This is for her research project to submit to Rajiv Gandhi University of Health
Sciences in partial fulfillment of University requirement for the award of Master of
Nursing degree. We request you to kindly accord permission to conduct the study at
selected setting.
Thanking you,
Yours Faithfully
(PRINCIPAL)
Date :-
Place :-
Page 112
112
ANNEXURE- II
CERTIFICATE OF CONTENT VALIDITY
This is to certify that the tool developed by Ms Anju Appukuttan, second year
Msc nursing student of Spurthy college of Nursing, Marasur gate, Anekal Taluk,
Bangalore for my study “A study to evaluate the effectiveness of planned teaching
programme regarding knowledge and attitude on prevention of dental caries among
mothers of primary school children at AnekalDistrict Bangalore.” is validated by the
undersigned and can proceed with this tool to conduct main study.
Place
Date Signature of the expert.
Page 113
113
ANNEXURE- III
LETTER SEEKING EXPERTS OPINION FOR THE CONTENT VALIDITY
OF THE TOOL USED FOR THE STUDY
From
Ms. Anju Appukuttan
II Year M.Sc.Nursing
Spurthy College of Nursing,
Bangalore – 562106
To
_______________________________
_______________________________
_______________________________
Forwarded Through
Principal
Spurthy College of Nursing,
Bangalore – 562106
Respected Sir/Madam,
Sub: - Expert opinion for content validation of Research tool.
I am Anju Appukuttan postgraduate student in child health Nursing studying
at Spurthy College of Nursing, Bengaluru. For the partial fulfillment of the course I
have undertaken a research project. I have selected the below mentioned topic for the
research project to be submitted to Rajiv Gandhi University of Health Sciences,
Bengaluru.
“A study to evaluate the effectiveness of planned teaching programme regarding
knowledge and attitude on prevention of dental caries among mothers of
primary school children at AnekalDistrict Bangalore.’’
I hereby have enclosed the following documents for your kind reference.
1. Structured interview schedule to assess the knowledge
2. 3-Point attitude scale to assess the attitude
3. Lesson plan
4. Answer keys
5. Criteria checklist for content validation
6. Certificate of content validity
Page 115
115
ANNEXURE 1V
SCORING KEY
Respected Madam/ Sir,
Kindly go through the items in the enclosed tool and place a tick mark (√)
against each item in the column provided indicating your opinion best. There are 5
columns, namely Strongly Agree (SA), Agree (A), Neutral (N), Disagree (DA) and
Strongly Disagree (SDA). If there are any suggestions, please mention them in the
remarks column.
Q.NO SA A N DA
SDA REMARKS
TOOL –I: PART –I :DEMOGRAPHIC PROFORMA 1.
2.
3.
4.
5.
6.
7.
8.
PART -II : KNOWLEGDE STRUCTURED QUESTIONNAIRE FOR ASSESSING THE KNOWLEGDE OF PRIMARY SCHOOL CHILDREN MOTHERS REGARDING DENTAL HYGIENE AND DENTAL CARIES. 1.
2.
3.
4.
5.
6.
Page 116
116
Q.NO SA A N DA
SDA REMARKS
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
Page 117
117
ANNEXURE – V
TOOLS FOR DATA COLLECTION
STRUCTURED KNOWLEDGE QUESTIONNAIRE
Questionnaire includes multiple choice questions.
Part-I
Consists of ten items related to demographic variable of primary school children
mothers attending planned teaching programme at Anekal st.philomena’s high school.
Part -II
Consists of twenty four items on knowledge of primary school children mothers attending planned teaching programme at Anekal st.philomena’s high school regarding dental hygiene and dental care.
PART –I Dear participant,
This questionnaire is related to the demographic variables. I am here with requesting you to answer all the questions. This information will be treated as confidential. Kindly put tick marks in the appropriate information or encircle the most appropriate answer.
Sample code no:
DEMOGRAPHIC PROFILE
1. Age a. Below 20 yrs ( ) b. 21 yrs -25 yrs ( ) c. 26 yrs -30 yrs ( ) d. Above 30 yrs ( )
2. Educational status of the mother a. Illiterate ( ) b. Up to SSLC ( ) c. PUC ( )
Page 118
118
d. Graduate ( ) e. Postgraduate ( )
3. Type of family
a. Nuclear family ( ) b. Joint family ( ) c. Extended family ( )
4. Family income per month
a. Rs 1001- 2000 ( ) b. Rs 2001-3000 ( ) c. Rs 3001- 4000 ( ) d. Rs > 4000 ( )
5. Occupation of the mother
a. Home maker ( ) b. Cooli worker ( ) c. Government employee ( ) d. Private employee ( )
6. Number of children
a. 2 ( ) b. 1 ( ) c. 3 ( ) d. twins ( )
7. Sources of information a. Mass media ( ) b. Friends ( ) c. Relative ( ) d. Parents ( ) e. Health personal ( )
8. History of oral disorders
a. Mouth ulcer ( ) b. Dental caries ( ) c. Oral sores ( )
Page 119
119
PART- 11
STRUCTURED INTERVIEW SHEDULE ON DENTAL HYGIENE AND
DENTAL CARIES
Kindly read the following questions, Select the correct answer
according to you and put tick marks or encircle them. Please note that it is important
to respond to all questions. This questionnaire is to assess the knowledge regarding
dental hygiene and dental caries.
1. DENTAL CARIES otherwise called
a. Glossitis ( )
b. Gingivitis ( )
c. Tooth decay ( )
d. Tooth extraction ( )
2. THE STUDYOF DENTAL CARIES IS
a. Cariology ( )
b. Cardiology ( )
c. Radiology ( )
d. Ophthalmology ( )
3. DENTAL CARIES is caused by
a. Streptococcus pneumonia ( )
b. Streptococcus aureus ( )
c. Streptococcus mutans ( )
d. Staphylococcus ( )
Page 120
120
4. Inner layer of tooth is
a. Dentist ( )
b. Dentine ( )
c. Dental caries ( )
d. Periosteum ( )
5. Root canal therapy means
a. Removal of tooth ( )
b. Opening of tooth ( )
c. Repair the tooth ( )
d. Cutting of tooth ( )
6. Pathological changes in dental caries
a. De-mineralization ( )
b. Enlargement of tooth ( )
c. Bleeding from gums ( )
d. Pus collection to the teeth ( )
7. Sign’s & symptoms of dental caries is
a. Xerostomia ( )
b. Xereothalmia ( )
c. Sneezing ( )
d. Hair fall & joint pain ( )
Page 121
121
8. Primary sign of dental caries
a. Black spot on the teeth ( )
b. White spot on the teeth ( )
c. Toothache ( )
d. Bad colour ( )
9. The diagnostic evaluation for DENTAL CARIES includes
a. Chest x-ray ( )
b. Intra oral radiographs ( )
c. Ophthalmoscopy ( )
d. All the above ( )
10. Use of Electronic caries detector
a. Measure demenerslisation ( )
b. Measurement of symptoms ( )
c. Detect tooth colour ( )
d. Check glossitis ( )
11. Complication of DENTAL CARIES is
a. Tycodeties ( )
b. Congestive heart failure ( )
c. Caveenous sinus thrombosis ( )
d. Tonsilities ( )
Page 122
122
12. Measures to prevent dental caries
a. Advice for hand washing ( )
b. Wearing mask ( )
c. Oral hygine ( )
d. Playing out side ( )
13. Flossing means
a. Removal of teeth ( )
b. Cleaning between teeth ( )
c. Removal of enamel ( )
d. Removal of membrane ( )
14. Plague can be prevented by
a. Good oral hygine ( )
b. Advise for mouth wash ( )
c. Advise for hand wash ( )
d. Fissure sealant ( )
15. Fluoride protects against
a. Infection ( )
b. Inflammation ( )
c. Dental caries ( )
d. Gingiivities ( )
Page 123
123
16. For dietary modification
a. Sugar intake is increased ( )
b. Sugar intake is decreased ( )
c. Fiber rich diet ( )
d. Green leafy vegetables ( )
17. Use of Topical fluoride
a. Protect the surface layer of teeth ( )
b. Protect the inner layer of the teeth ( )
c. Treat stomatitis ( )
d. Remove bacteria ( )
18. To prevent decay by
a. Increase flow of saliva ( )
b. Use antibiotics ( )
c. Use tooth paste ( )
d. Use mouthwash ( )
19. Rich source of fluoride is
a. Water ( )
b. Tooth paste ( )
c. Food ( )
d. Vegetables ( )
Page 124
124
20. Filling is the measure to
a. Repair damage caused by caries ( )
b. Remove caries ( )
c. Increase circulation ( )
d. Decrease bleeding ( )
21. Drug of choice for dental caries
a. Bronchodialator ( )
b. Antepyratics ( )
c. Bronchoconstrutor ( )
d. Antibiotics ( )
22. treatment provided for cavity in the pulp is called
a. Filling ( )
b. Root canal ( )
c. Drug ( )
d. Extraction ( )
23. Which one of the following should avoided in the home
a. Cold drinks ( )
b. Exercise ( )
c. Tobacco smoke ( )
d. Daily brush ( )
Page 125
125
24. Re mineralization factors are
a. Fats ( )
b. Calcium ( )
c. Protein ( )
d. Vitamins ( )
Page 126
126
PART–III
ATTITUDE SCALE Instructions:
Kindly read the following questions. Select the correct answer according to
you and put tick marks. Please note that is important to respond to all questions. This
questionnaire is to assess the attitude regarding dental hygiene.
Sl No Attitude Statement
Agree
Disagree
1. dental caries is a bacterial infection
2. Outer layer of tooth contain calcium
3. Enamel protect the inner layer of the teeth
4. Sugar and carbohydrates will cause dental caries
5. Bad breath is the symptom of dental caries
6. Flurides will protect the tooth against dental caries
7. Root canal treatment is the one of the dental caries treatment
8. Cold drinks will cause dental caries
9. Chewy sticky food is the best food which are eaten during
dental caries
10. Brushing is important for oral health
11. Tooth abcess means collection of pus
12. Antibiotics drugs using for dental caries
13. Intra oral radiographs is the one of the diagnostic evaluation
for dental caries
14. Leedwing’s angina is the one of the complication for dental
caries
15. Flossing means cleaning between teeth
16. Reduce intake of cariogenic food will give good oral health
Page 127
127
SCORING KEYS
Question No. Answer
1 c
2 a
3 c
4 b
5 c
6 a
7 a
8 b
9 b
10 c
11 d
12 b
13 b
14 c
15 a
16 b
17 c
18 d
19 b
20 b
Question No. Answer
21 a
22 c
23 a 24 b
Page 128
128
ATTITUDE SCORES
Statement No. A D 1 1 0 2 0 1 3 1 0 4 0 1 5 1 0 6 0 1 7 1 0 8 0 1 9 1 0 10 0 1 11 1 0 12 0 1 13 1 0 14 0 1 15 1 0 16 0 1
Page 129
129
SUBMITTED TO SUBMITTED BY MRS.PUSHPAKUMARI K MS.ANJU APPUKUTTAN ASSOCIATE PROFESSOR 2ND YEAR MSc NURSING CHN DEPARTMENT S.C.O.N S.C.O.N
Page 130
130
LESSON PLAN Topic:Dental caries
Group: primary school children mothers
Place:st.philomena’s high school
Duration: 45 Minutes
Method of teaching: planned teaching programme
Audio -visual aids: LCD Projector
No of participants: 60
General objectives:
The primary school children mothers should acquire knowledge and understand the dental caries and the
importance of oral hygiene and to develop desirable skills in applying this knowledge in home.
Page 131
131
Specific objectives:
Primary school children mothers will be able to
• Define dental caries
• Stages of dental caries
• Causes of dental caries
• Pathological mechanism
• Diagnostic evaluation
• complication
• preventive measures of dental caries
Introduction :
Good morning to all, I am final year MSc (N) student of spurthy college of nursing Bangalore .I am going to teach
regarding dental caries and dental hygiene, it’s a care have to teach to the family members.
Page 132
132
TIME SPECIFIC OBJECTIVE
CONTENT TEACHER’S ACTIVITY
LEARNER;S ACTIVITY
AV AIDS
EVALUATION
3 min
Explain the introduction of dental caries
Introduction: Dental caries also known as tooth decay or a cavity is an infection, bacterial in origin, that causes demineralization and destruction of the bald tissue (enamel, dentin and cemetum)usually by production of acid by bacterial fermentation of the food debris accumulated on the surface. If demonetization exceeds saliva and other remineralization factors such as from calcium and fluoridated tooth pastes, these hard tissues progressively break down producing dental cares .today caries remain one of the most common diseases throughout the world .cardiology is the study of dental caries.
Teacher introduces the topic of dental
caries
Listening What is meant by dental caries
Page 133
133
3 Min
ANATOMY & PHYSIOLOGY The outer hard layer of the tooth contains large amounts of calcium and is very hard. In fact of it is the hardest structure that can be formed by the body. The tooth enamel has no blood supply and can therefore also not heal itself once it has been damaged it is literally a dead layer of cells.
Teacher explain the
listening
Chart
What are the different parts of teeth
Page 134
134
The enamel protects the inner somewhat softer, more porous inner layer of the tooth, called dentine. The detain is the living part of the tooth and is directly linked to the nerve inside the tooth. The nerve runs in a canal, called the root canal deep within the tooth. The root canal is literally a cavity in the root of every tooth.it contains not only the nerve but also the blood vessels which provide the dentine with nutrients and oxygen & keep it alive
Page 135
135
2 Min 3 Min
Define dental caries
DEFINITION Dental caries is an irreversible microbial disease of the calcified tissues of the teeth, characterized by de‐mineralization of inorganic portion & destruction of organic substance of the tooth, which often leads to cavitation CAUSES BACTERIA Streptococcus mutans‐83% children’s are affected Lactobacilli Actinomycesviscosus SUGAR Sugar can be found in all carbohydrates foods, such as bread, potatoes, banana’s and breakfast and cereals. Plague + sugar + acid The bacteria in the plague use the sugar as a source of energy food. The bacteria digest the sugar and by products are exerted. these by products are very sticky and acidic and cause a fall in the mouth’s PH Time if the plague is not allowed to lie on the tooth surface for any length of time, no decay will result
Teacher defines Dental caries
Understanding causes of Dental
caries
Listening
Listening
Flash card
chart
What is the meaning of dental caries
What are the causes of dental caries
Page 136
136
4 Min
List down the stages
Thus cleaning your teeth soon after eating will decrease the amount of time these factors have to cause dental caries. STAGES:
Teacher listening out the dental caries
Listening
Pamphlet
What are the stages of dental caries
Page 138
138
3 Min
Identify pathologic mechanism
PHATHALOGIC MECHANISM Fermentation of dietary sugars by oral microorganism De‐mineralization Re‐ mineralization Further demineralization & cavitations initiation/formation of caries.
Listening out pathologic mechanism
Listening
Explain the pathologic mechanism
3 Min
Enumerate the signs and symptoms
SIGN & SYMPTOMS White spot on the skin Toothache Visible pits or holes in the teeth discoloration of teeth Bad breath Foul tastes Xerostomia Brown spot is spear
Teacher discuss about the signs and symptoms of dental caries
Listening
What are the signs and
symptoms of dental caries.
Page 139
139
4 Min
Explain the diagnostic evaluation of dental caries
DIAGNOSIS: History taking Physical examination Visual examination Intra oral radiographs Electronic causes detectors
Teacher explains in details about diagnosis
Listening
Chart
What are
the diagnosis of dental caries
2 Min 2 min
List out the complaints of dental caries
List out the prevention of dental caries
COMPLICATIONS: Cavernous sinus thrombosis Leedwig’s angina PREVENTION: ORAL HYGIENE It is important that the plague should be effectively removed even brushing two or three times pee day is not good enough if you
Teacher list out the complaints
Teacher discuss about the
prevention of dental caries
Listening
listening
Flash card
What are the
complaints of dental caries
What are the
prevention of dental caries
Page 140
140
4 Min
Use the correct technique Flossing is also essential in the removal of plague it is the only effective way cleaning between teeth. Fissure sealants: The sealing of the grooves on top of the premolars and molars as soon as their crown except fully through the gun, prevents them from becoming clogged with food particles sealants are then plastic like coating applied to the chewing surfaces of the molars. thus coating prevents the accumulation of the plague on the unalienable surfaces Older people may also benefit from the use of fissure sealants.
Page 141
141
1 Min 2 Min 2 min
FLUROIDS: To protect teeth against dental caries TOPICAL FLUROIDS: Helps to protect the surface layer of the teeth. It is mainly found in tooth pastes & mouth wash DIET: Chewy, sticky foods are best as a past of a meal rather than snacks Encourage to take sucrose intake
Selective counseling Reduce intake of cariogenic food Reduce long time use of baby bottles
Page 142
142
4 Min
TREATMENT Fluoride treatment Treated with high concentrations of fluorides resulting in the arrest of caries & remineralisation of the tooth enamel Filling It is used to repair the damage caused by carries Root canal treatment If the infection has reached the pulp, then root canal treatment is sued Some of the restrictive materials include porcelain, composite resin gold and dental amalgam Tooth extraction can also be the treatment of extreme decay In some cases, endodontic therapy can be necessary to presence the tooth Decayed methanol from an affected tooth can be removed with the help of a dental hand piece like a drill
Page 143
143
Early treatment is generally less painful. If a cavity is so extensive that there is no space to place the restrictive material, then a crown is needed, crown are made of porcelain or gold & fused to a metal In severe cases, anesthesia such as laughing gas (eg: nitrous oxide)or other medicine are given before the treatment
2 Min
Home treatment for toothache If you have sensitivity to cold drinks, try using tooth paste made for sensitive teeth Avoid alcoholic beverages such as wine The other condition you can attempt to treat at home is dull ache and pressure in your upper teeth & jaw
Page 144
144
2 Min
SUMMARY: In today’s class I disused about definition of dental causes stages, causes, pathology, signs & symptoms, diagnostic evaluation, complication, prevention & management of dental causes like oral hygiene, dietary modification, avoid cold drinks etc. It is very important to protect them by giving good personal hygiene, food, & cross infection CONCLUSION: This is knowledge about dental caries will help to mothers to know about home care & to improve the dental hygiene of primary school children. This knowledge also helps to education others to build up healthy children & healthy nation
Page 145
145
BIBLIOGRAPHY
Page 146
146
KANNADA TOOL VERSION
���-I
������ �������,
� ������������ �������� ������
����������. ���� ���� ������������ ���������
���� ����� ����. � ����������� ����� ����
����������������. �������� ������ �����������
���� ��������� ���� ���� ������ ��������
���������� �������������.
����� ������ �������:
�������������� ����������
1. ������ a. 20 ������ ����� (
) b. 21 ���� -25 ���������� (
) c. 26 ���� -30 ���������� (
) d. 30 ������ ����� (
)
2. ����� ��������� ������ a. ��������� (
) b. ���.���.���.��. ����� (
) c. ������ ( ) d. ���� ������ (
) e. �������������
( )
3. ������� ���������� a. ��� ������ (
) b. ������� ������ (
)
Page 147
147
c. ������� ������ ( )
4. �������� ������ ���� a. �� 1001 - 2000 (
) b. �� 2001-3000 ( ) c. �� 3001- 4000 ( ) d. �� > 4000 ( )
5. ����� ��������
a. ������ ( ) b. ���� ������� ( ) c. ������� ���� (
) d. ����� ���� ( )
6. ����� ������
a. 2 ( ) b. 1 ( ) c. 3 ( ) d. ���� ( )
7. ������ ���
a. ���� ��������� ( )
b. ���������� ( )
c. ������� ( ) d. ������ ( ) e. ��������� ��������
( )
8. ����� ����������� ������ a. ���� ������ (
) b. ��� ���� (
) c. ���� ������ (
)
���-II
Page 148
148
������ �������� ����� ��� ���� ����� �������� ������������ ����������
�������� ������ ������������� ���,
����� ������ ������ ���������� ��������� ����� ���� ��������� ���� ���� ��������� �������������. ����� ������������ �������������� ����� ��������� �������� ������. � ������������ ������ �������� ����� ������ ���� ����� ����� ���������� ��������.
1. ��� ���� ����������� ���
a. ������ ������ fAf«n¸ï ( ) b. ������������ ( ) c. ����� ( )
2. ��� ���� ������ a. PÉjAiÉƯÉÆf ( ) b. ���� ( ) c. ������������� ( ) d. ������������� ( )
3. ������ �� ������ ���� ����������� a. ����������������� ������������ ( ) b. ������������������ ����� ( ) c. ������������������ ªÀÄÄl£ïì ( ) d. ������������������ ( )
4. ������ �� ��� a. ��������� ( )
Page 149
149
b. ��� ������ ( ) c. ��� ���� ( ) d. ¥ÉÇÃjAiÉÆùAiÀÄä ( )
5. ���� ������ ��������� ���� a. ������ ���������� ( ) b. ������ ������� ( ) c. ������ ������� ( ) d. ������ ��������� ( )
6. ��� ���� ����� ���������� ������������� a. ��‐��������� ( ) b. ������ ���������� ( ) c. ������� ���� ��������� ( ) d. ���������� ����� ������ ( )
7. ����� � & �������� ��� ���� �������� a. EgÉÆmÉÆ«ÄAiÀÄ ( ) b. EgÉÆÃxÀ°äAiÀÄ ( ) c. �������� ( ) d. ����� ��� ����� ����� ������ ( )
8. ��� ���� �������� ������ a. ������� ����� ����� ������ ( ) b. ���������� ����� ������ ( ) c. ����������� ( )
Page 150
150
d. ����� ���� ( )
9. ��� ���� ���� �������������� �������������� ��������������
a. ���� ��� ‐ ���� ( ) b. ����� ����� ��������������������� ( ) c. M¥ÀܯÉÆäøÉÆÌæ ( ) d. ������ ����� ( )
10. ������������� ��������� ��������� ���� a. ���� ����������� ( ) b. ������������ ���� ( ) c. ������ ���� ����� ( ) d. ������ ������ ���������� ( )
11. ��� ���� ��� ������ a. låPÉÆÃrlå¸ï ( ) b. ���� ����� ���� ������ ( ) c. ������ ������������� ( ) d. ��������� ������ ( )
12. ��� ���� ��������� ������� a. �������� ����������� �� ���� ( ) b. ������ ������ ( ) c. ����� ��������� ( ) d. ������ ���������� ( )
Page 151
151
13. ¥sÁè¹AUï �������� a. ������� ���������� ( ) b. ������ ����� �������������� ( ) c. ������ �������������� ( ) d. ������ ���������� ( )
14. ������� ��������������� a. ������ ����� ��������� ( ) b. �������� �� ���� ( ) c. �������� �������� �� ���� ( ) d. ������������ ���� ( )
15. ����������� ������������ a. ������ ( ) b. ������ ( ) c. ��� ���� ( ) d. fAf«n¸ï ( )
16. ���� �������� a. ������� ������ ������������� ( ) b. ������ ������ ����� ��� ( ) c. ������ ������ ���� ( ) d. ����� ����� ��������� ( )
17. �������� ��������� ���� a. ������ �������� �������� �������� ( ) b. ������� �� ��� ������� ( )
Page 152
152
c. ������������� �������� ( ) d. ������������� ���������� ( )
18. ������ ���������������� ��������� a. ������� ����� ������ ( ) b. ������������ ���� ( ) c. ������ ������� ���� ( ) d. �������� ����� ( )
19. ����������� ������ ��� a. ����� ( ) b. ������� ( ) c. ���� ( ) d. ��������� ( )
20. ������ ���� a. ����� ���� ����������� ������� ���� ( ) b. ����� ���� ���������� ( ) c. ����������� ��������� ( ) d. ��������� �������������� ( )
21. ��� ���� ������ ����� a. ����������� ( ) b. JAn¥ÀågÁnPÀì ( ) c. §æAPÉÆPÀAlÄlgï ( ) d. ������������� ( )
Page 153
153
22. ����������� ��������� ������� �������� ���� �������������
a. ����� ( ) b. ���� ������ ( ) c. ���� ( ) d. ������������ ( )
23. ������ ���� �������� ���������� �������� a. ���� ��������� ( ) b. ������� ( ) c. ������ ����� ( ) d. �������� ���� ( )
24. �������������� ������ a. ���������� ( ) b. ���������� ( ) c. ������� ���� ������ ( ) d. ����������� ( )
���-III ������� �������
��������:
�������� ������ ������������� ���. �����
������ ������ ���������� ��������� ����� ����
��������� ����. ����� ������������
�������������� ����� �������� ������. �
������������ ������ �������� ����� ������
���������� ��������.
Page 154
154
Sl No ������ �������
������������
�����
��
1. ��� ���� ������������� �������
2. ������ �������� ��� ����������
�������������
3. ������� �� �������� �������� ������
4. ������ �����
��������������������� ��� ����
�������������
5. ����� ������� ��� ���� � �����
6. �������������� ��� ���� �������
����� ������������
7. ���� ������ ��������� ��� ����
��������� ����
8. ���� ��������� ��� ����
�������������
9. ���� ������� ���� ��� ���� �������� �������� ��� ����� ����
10. ������������� ����� �������� �����
11. ������ ������ ����� ������ ����
12. ��� ���� ���� ����� ����������
������
13. ����� ����� ���������������������
��� ���� ������� ��������� ��������
14. �������� � ������ ��� ���� ����
������ ��������
15. ������ ����� �������������� ����
16. ���� ����� ���� ����� ������ �����
����� �������� ����������
Page 155
155
�������� �������� ���� ��������. ������ ������ ����. ���� ������������ ������������ ���������� 2 ��� ����� ������� �������� ¹.JZï.£ï ����� S.C.O.N S.C.O.N
Page 156
156
����� �������� ����: ��� ���� ����� ������ �������� �����: �������� ���� ����� �������� ������� ¸ÉAmï ¦ü¯ÉÆëģÁ
��������� ����: 45 �������� ������� �����: ������� ��� ��������� ����� ����� ����� AIDS: ������� ���������� 60: �������������� ������ ����� ����������: �������� ���� ����� �������� ���������� ����� ������ ��������
����� ������ ���� ���� ����� ��������� ����������������
Page 157
157
���������������� ����� �������� � ���������� �������������
����������� ���������� ��������������� ��������.
��������� ����������:
�������� ���� ����� �������� ��������������
• ��� ���� �������
��� ���� ��� • ������
��� ���� ��� • �������
• ���������������� ��������
• �������������� ��������������
• ������
��� ���� ��� • �������� �������
• ������ ��������
�����:
����� ���� ���������, ���� �������� �������� spurthy �������� �������
(���) ���������� ����� ����� am. ���� ��� ���� ����� ������ ��������
Page 158
158
����� ��������� �����������������, ��� ������ ������� ���������
������ ������������� �������.
��� ��������� ������ ���� �������
��������
�����������
��������
��� �����
����������
3 �����
��� ���� �����
�������
�����: ��� ���� ���� ������������ ���� ���� ��������� ������ ������� ����������� ����� �������� ��������� ��� ������������� �������, (������, ��������� ����� cemetum) ����������� �������� ����� ��������� ���� �������� ������������� �������������� �����
������ ��� ���� ����� ���������
����
����� ��� ���� ��������
Page 159
159
�������� ���� . ����������� ������ ����� ���������� ����� ���������������� ������ ���������� ���� ��� �������������� ������ ����������, � ������ ��������� ������� ������ ������� ���������� ������������. ���� ��������� ������������ ������ ������� �������� ���� ����������. ����������� ��� ���� ������������.
Page 160
160
3
�����
����� ������� ����� ����� ������� ������ �������� ���� �������� ���������� ������ ������� �������� ����� ������ ����. ��� ���������� ������ ��������� ���� ����������. ������ ����� ������� ���� ������� ����� ��� ������� ����������� ���� ��� ����������� ���� �������� �� �����
������ ��������
�����
�����
������ �����
������ ������
Page 161
161
��������� ����������. ������, ������ �� ������ �������, ������ ����������� ����� ����� ������������ ��������� �������������. ��������� ������ ����� ��������� ����� �������� ������ ���� �� ����� ���. ��, ������ ����������� ������ ���� ����� ���� ������ ���. ���� ������ ��� �� ���� ������������ ����� ��������������� ��������� ����������� ���� ��� ����������������� ��� ��������� ����� �������� ������� ������ ������ ���� ������� ��������
Page 162
162
2
����� 3
�����
Define dental caries
��������� ��� ���� ����������� ��������������� ������������� ������ ����� �������� ������� �������� ����� ������ ��‐��������� ���� ������� calcified �������� ���� ����������� ������������� ��������������, ������� ������������� ������������������ mutans ‐83% ������ ������������������� ����������������� ��������������� Viscosus ������ ������ ������ ����� ����������������� �������, ��������, �����������, ���� ����� ����� ����� ��������.
������ ���������
�� ��� ����
��� ���� ���������
��� �������
�����
�����
����������
�����
��� ���� ���� ���
��� ���� ������� ������
Page 163
163
������� + ������ + ���� ������������� ������������� ����� ����� ���� ������� ������ ����. ������������� ������ ���������� ����� ���������� ������������ ������������. � ���� ������������� ������ ������� ����� ������� ����� ������� ���� �������� ������ �������� ����� ������ ������������������ ����� ����� PH ����� ����� ������������, ������� ������ �������������
Page 164
164
4
�����
List down the stages
�������� ������ ���� ���� ����� ����� �������������� � ������ ��� ���� ��������� �������� ��� ����������� �����������������. ������:
������ ��� ���� ��� ������
������
������
��� ���� ��������
� ����
��
Page 166
166
3
�����
���������������
�����������
��������
���������� �������� ����� ������������ ������ ����� ������ ��������� ��‐��������� ��� ��������� �������� ����������� & ��������������� ������� / ��������� ������.
���������
� ��������
��� ������
������
��������
�� �������� �������
3 �����
��������� �����
������������� �����
������ ����� �������� ����� ����� ���� ������ ����������� ������� ����� ������ ������ ����� ���� ������� ����� ����� ���� ������� Xerostomia ������ ������ ��� �����
������ ���
���� ���������
�� ����� ��������
������
���
���� �����������
������.
Page 167
167
4
�����
��� ����
��������������
��������������
�������
�����: ������ �������������� ����� �������� ��������� ����� ����� ��������������������� ����������� ������� ���������
������ ������������ �����
����������
������������
������
Chart
What are the diagnosis of dental caries
2
����� 2
�����
��� ���� ���������
� ��� �����
��� ���� ��������� ��� �����
���������: Cavernous ������ ������������� �������� � ������ ���: ����� ���������
���������� ���
������ �����
������ ��� ����
��������� �����
��������
������
������
����������
��� ���� ��������
�� ����
��
��� ���� ��������� ������
Page 168
168
��� ������� �������������� ��� ���� ���� ���� ���� ��� ��� ������������� ����������������� �������������� ����� �����
4
�����
������ ���������� ���� flossing �� ������ ����� �������������� ����� ���������� ����������� ������� ������������������� ��������. ������ ����: ����� ���� ������ ������ ����������� ����������� ��� ���� ���������� ����� ���� ����� ��������� � ��������, ���� ��������� ��������� ���������� ������ ���������� ���� ���� �������� ������ ����� �������������� ���������� ���������
Page 169
169
������������ ����������. ������� ����� ������������������ ����������� ����� ������� ����������� ������������� ���� ���� �� ������ ������ �������� ��������������������.
1
����� 2
����� 2
�����
�����������: ��� ���� ������� ����� �������� ������ �����������: ������ �������� �������� �������� ������������. ��� ��������� ������ ���������� ����� ���� ����������� ������������ ����: ���, ������� ������� ����� ���� ���� ����
Page 170
170
������ �������� ������ ��������� ���������� ������ ������ �������������� ���� ���� ���� ����� ���� ������ ����� ������� ��� �����
4
�����
�������� ����������� �������� ������ ���� ����� remineralisation �������� ���������� �������������� ����������� �������� ����� ��� ���������� ��������� ������� ����� ������������
Page 171
171
���� ������ ��������� ������� ������ ������� �����, ���� ���� ������ ��������� ��������� ��� ��������� ����� ����������� �������, �������� ��� ����� ����� ��� ������������� ������� ����� ��� ������ ������ �������� �������� ����� ������������, Endodontic �������� �������� ������ ������������� �������� ����� ����� ������
Page 172
172
������� ���� ������ ���� ������ ��� ����� �������� ���������� ������� ���������� ����������� ����� ����������. ����� ��������� ����������� ������ ������� �������� ����, ����� ����� ������ ����� ���� ������ ���������, ������ ������������� ���� ��������� ����� ������ �� ����������������� ����������� ������������, ��������� ������� ���� (���: �������� ��������) ���� �������� ���� ��� ����������
Page 173
173
���������� ���������� ����������
2
�����
����������� ����� �������� ����� ������� ������������ �������������� �����������, ������� ����� ����� ������ ������� ����� ���������� ��������� ����� ���� ��������������� ����������� ������� ����� �������� ��������� ����������� ��� ����������� ����� ������ �������� ����� ���� ����� ���� ������������ ����� �����
Page 174
174
2
�����
������: ����� ���� ���� ��� ������� ���������, �������, ���������������, ��������� ����� �������������, ����������� ����������, ������, ������������ ����� ����� ���������, ���� ��������� ������ ������ ������ ��������� ���������� ����� ��������, ���� ��������� ������� �������� ��� ������ ��� ����� ����� ��������� ���������, ����, ����� ���� ������� ������ ���� ��������:
Page 175
175
� ��� ���� ����� ���������� ���� ������ ����� ������� ����� �������� ���� ����� ������ �������� ��������� ���������� ���� �����. � ���������� �� ����������� ������ ����� ���������� ������� ��������� ������ ������� ����
Page 176
176
ANNEXURE – VI
BLUE PRINT OF THE TOOL - II
Sl. No Items/Content
Question Numbers
Total Questions
Percentage(%)
1 Information regarding dental caries
1-24 24 100%
Total
24
24
100%
Blue Print for Attitude Statement
SL. NO Attitude Statements Item number Total
number Percentage
(%)
1. Positive statements
1,3,5,7,9,11,13,15, 8 50
2. Negative statements
2,4,6,8,10,12,14,16 8 50
Total
16 16 100
Page 177
177
ANNEXURE – VII
LETTER SEEKING PERMISSION FOR CONDUCTING PILOT STUDY
From
Ms.Anju Appukuttan,
II year M.Sc. Nursing,
Spurthy College of Nursing,
Bangalore-562106.
To
The pricipal,
Spurthy Pre University college,
Marasur
Bangalore -562106.
Respected Sir\Madam,
Sub: Seeking permission to conduct a pilot study.
With reference to the above subject, I am Anju Appukuttan II year M.Sc.
Nursing student of Spurthy College of Nursing with a specialization in child health
nursing. I have to conduct a research study for the partial fulfillment of the course on
a topic “A study to evaluate the effectiveness of planned teaching programme
regarding knowledge and attitude on prevention of dental caries among
mothers of primary school children at AnekalDistrict Bangalore”.
I request you to kindly give the necessary permission for conducting study at
selected setting.
Thanking You,
Yours faithfully,
Date:
Place: (MS ANJU APPUKUTTAN )
Page 179
179
ANNEXURE – 1X LETTER SEEKING PERMISSION FOR CONDUCTING MAIN STUDY
From
Ms.Anju appukuttan
II year M.Sc. Nursing,
Spurthy College of Nursing,
Bangalore-562106.
To
The Pricipal,
Spurthy college of nursing,
Marasur
Bangalore -562106.
Respected Sir,
Sub: Seeking permission to conducting study.
With reference to the above subject, I am Anju appukuttan, II year M.Sc.
Nursing student of Spurthy College of Nursing with a specialization in child health
nursing would like to bring to your kind notice that I have to conduct a research study
for the partial fulfillment of the course on a topic “A study to evaluate the
effectiveness of planned teaching programme regarding knowledge and attitude
on prevention of dental caries among mothers of primary school children at
AnekalDistrict Bangalore.”
In this regard, I need permission from the principals of Spurthy College of
Nursing and stphilomena’s high school. Hence I request you to communicate with the
principal for getting permission for conducting this at selected setting.
Thanking You,
Yours faithfully,
Date:
Place: (MS.ANJU APPUKUTTAN)
Page 181
181
ANNEXURE – XI
LETTER SEEKING CONSENT OF THE SUBJECTS FOR PARTICIPATION
IN STUDY
Dear participant,
I am a final year MSc.(N) student of Spurthy College of Nursing, Marasur
Gate, Bangalore. As a partial fulfillment of the course, I have selected the below
mentioned topic for research work.
“A study to evaluate the effectiveness of planned teaching programme regarding
knowledge and attitude on prevention of dental caries among mothers of
primary school children at AnekalDistrict Bangalore.”
I request you to respond to the given questionnaire with the most appropriate
responses. Kindly do not leave any question unattended. The information given by
you will be kept confidential and used only for the study purpose.
Thanking you, yours faithfully
(ANJU APPUKUTTAN)
Page 182
182
ANNEXURE X11
LIST OF EXPERTS
1. Dr.Ramareddy
Peadiatrician
Maruthi hospital
Banglore
2. Mrs.Nirmala Florence
H.o.d
M sc peadiatrics
K.T.G College of Nursing
3. Mrs. D.Kalaichelvi
Principal and h o d
Department of paediatrics
National college of nursing
Banglore
4. Mrs.Jayavanitha
Msc paediatrics
Professor
Nightingale college of nursing
5. Mrs.Sathyavathi
Associate professor peadiatric nursing
National college of nursing
Banglore
6. Mr.Bhaskar Raj
Statistician