48
By: Dr.Wesam Abdelaziz
| Date post: | 22-Jan-2018 |
| Category: |
Health & Medicine |
| Upload: | melkholy |
| View: | 132 times |
| Download: | 4 times |
By: Dr.Wesam Abdelaziz

Early Signs of a critically ill patient
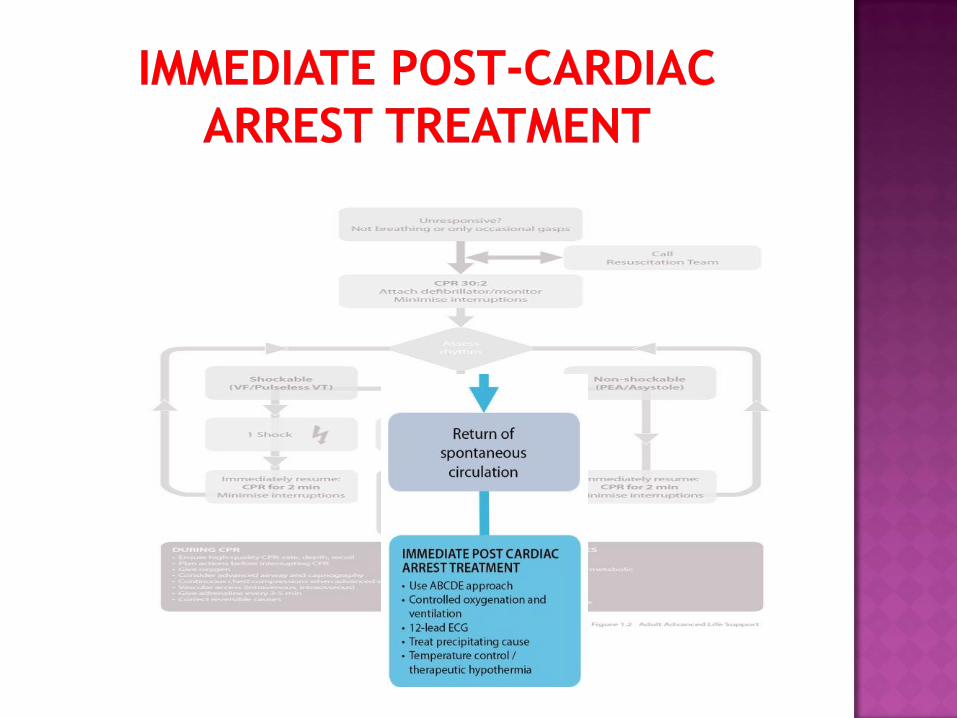
Initial management of a critically ill
patient
ABCDE Approach
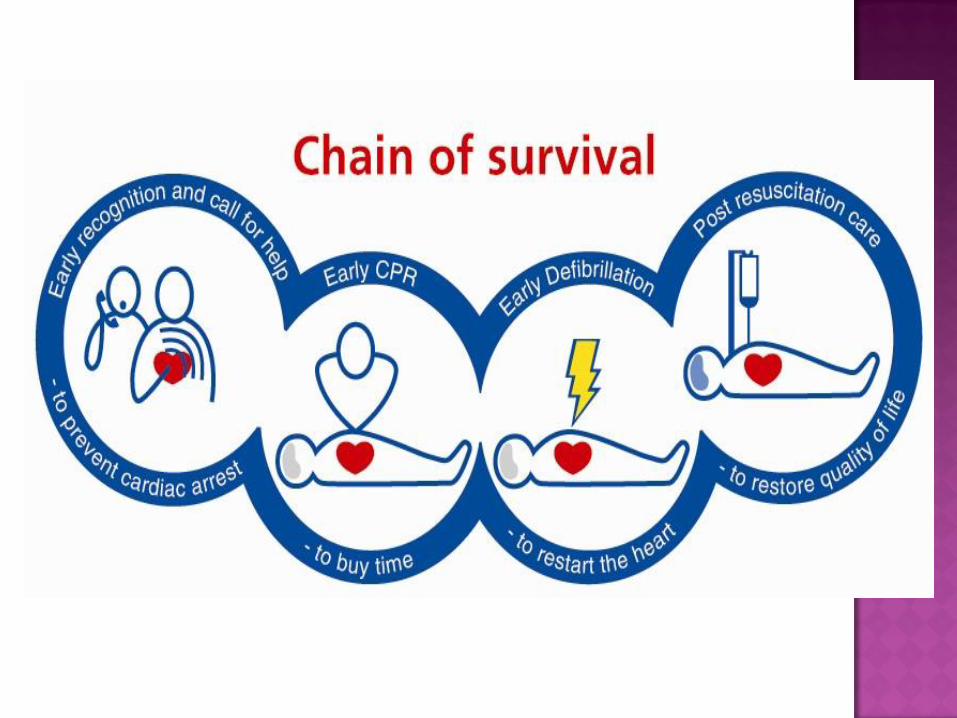
Most cardiac arrest cases are predictable
Hypoxia and Hypotension are the most
common causes
Medical Emergency Team (MET)
A: Airway
B: Breathing
C: Circulation
D: Disability
E: Exposure
Safety
Treat life-threatening problems
Assess effects of treatment/interventions
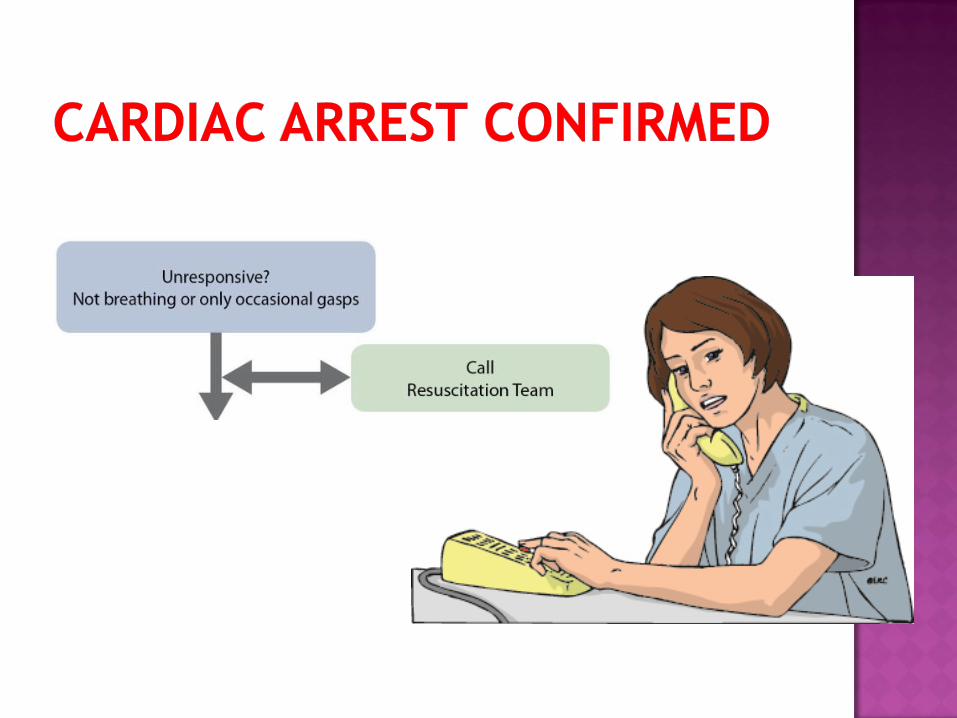
Call for help early
Continuous assessment is very important
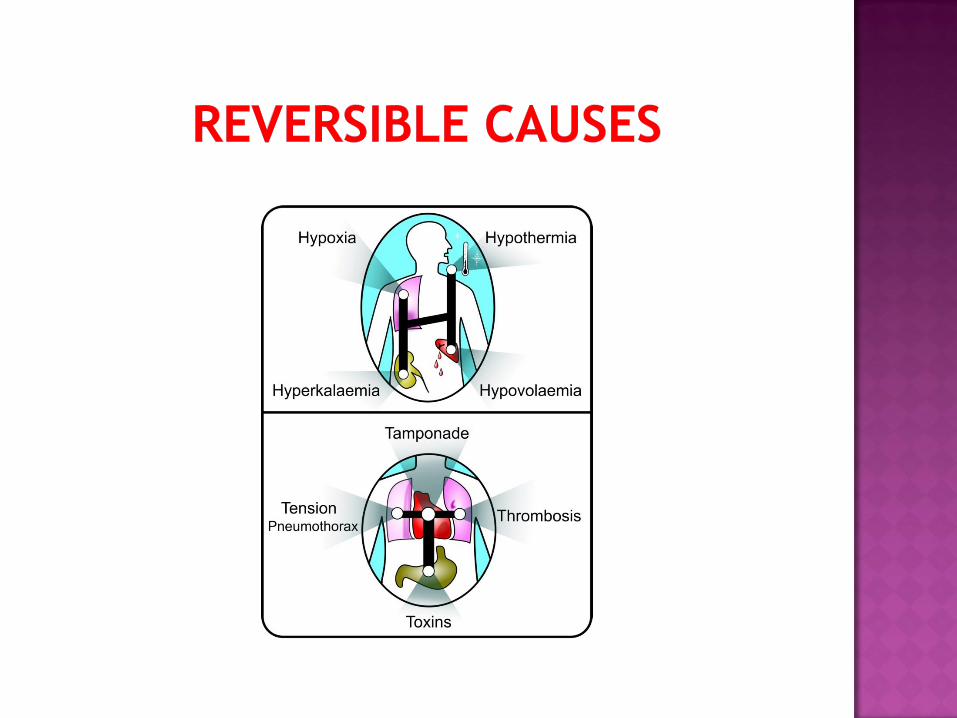
Causes of airway obstruction:
1. CNS depression
2. Blood
3. Vomit
4. Foreign body
5. Trauma
Talking means patent airway
Difficulty breathing, distressed, choking
Shortness of breath
Noisy breathing Stridor, wheeze, gurgling
See-saw respiratory pattern, accessory muscles
Head Tilt and chin lift
Jaw thrust if Trauma
Oro-pharyngeal Airway
Naso-pharyngeal Airway
Suction
Laryngeal Mask Airway (LMA)
Endotracheal tube
Oxygen

Causes if breathing problems:
Decreased respiratory drive
CNS depression
Decreased respiratory effort
Muscle weakness
Nerve damage
Restrictive chest
defect
Pain from fractured
ribs
Lung disorders
Pneumothorax
Hemothorax
Infection
COPD
Asthma
Pulmonary
embolus
ARDS
Inspection:
• Respiratory Rate
• Chest expansion
• Working accessory
muscle
• Deformity
Palpation:
• Tenderness
• Surgical emphysema
• Crepitus
Percussion:
• Dullness or hyper-
resonance
Auscultation:
• For breath sounds and
equality

Open Airway
Oxygen Supply
Treat Underlying Problem:
Bronchodilator Nebulizer is wheezy chest
Needle Thoracocentesis if Tension Pneumothorax
Assisted Ventilation if inadequate breathing
Causes of circulation problems:
Primary
Acute coronary syndromes
Arrhythmias
Hypertensive disease
Valve disease
Drugs
Inherited cardiac diseases
Electrolyte/acid base
abnormalities
Secondary
Aasphyxia
Hypoxemia
Blood loss
Hypothermia
Septic shock
Pulse :
Central & peripheral
Rate, Rhythm, Equality
Blood pressure
Peripheral perfusion - capillary refill time ( < 2 sec)
Organ perfusion
– Chest pain, mental state, urine output
Look at the patient : Pallor, Bleeding
Airway ,Oxygen
Breathing
IV/IO access, take bloods
Treat cause : ACS
Fluid challenge
Monitor
Recognition: AVPU
A: Alert
V: Responsive to verbal Stimuli
P: Responsive to Painful stimuli
U: Unresponsive
Pupils
Blood glucose
Normally is 4 mmol/ L (70 mg/dl)
Treatment:
ABC
Treat underlying
Cause:
Check for drug chart

Remove clothes to enable examination
e.g. injuries, bleeding, rashes
Avoid heat loss
Maintain dignity
Indication of complete Exposure
• Consult Specialist and Admission
• Investigations
• Continuous Assessment


Follow the ABCDE in assessment of any
patient.
Assess and re-assess all the time.
Don’t delay Calling senior Help


Basic Life Support
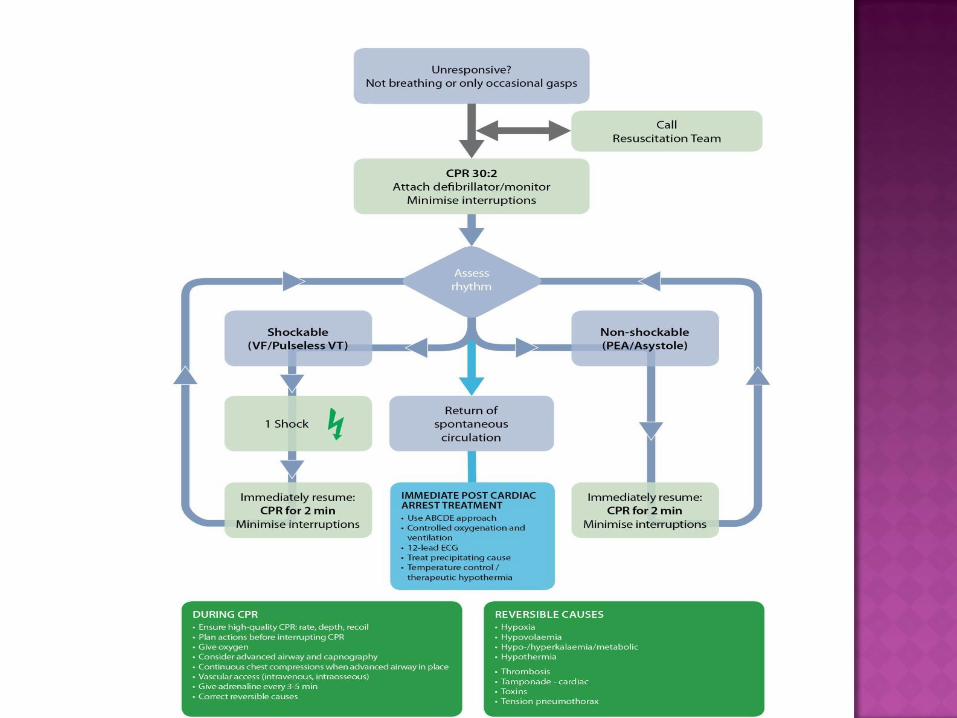
The ALS algorithm
Treatment of shockable and non-shockable rhythms
Potentially reversible causes of cardiac arrest
Role of resuscitation team
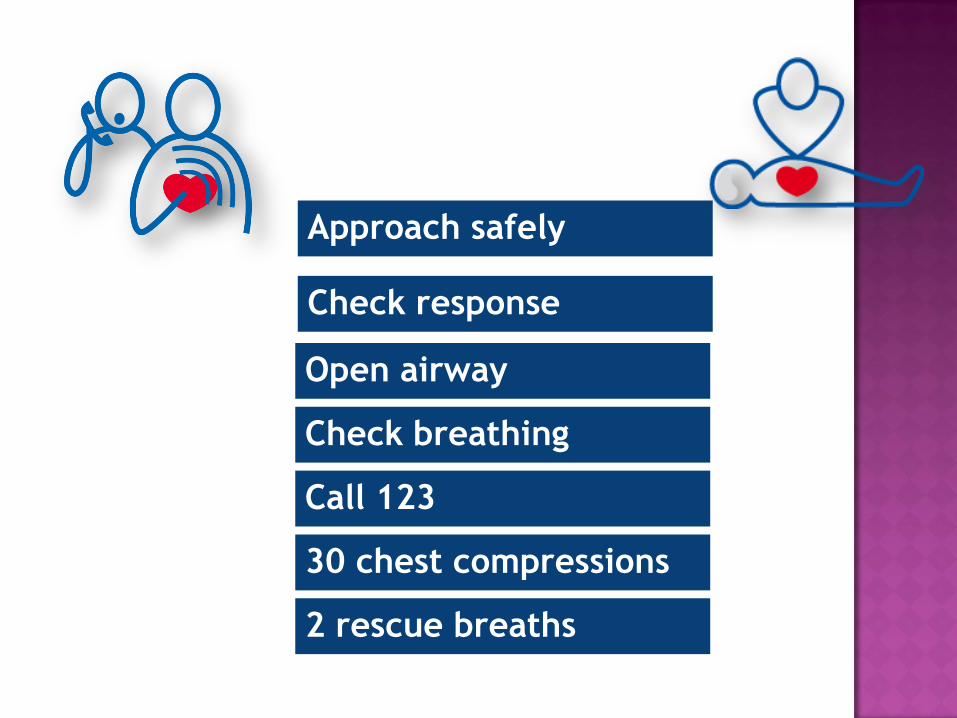
Approach safely
Check response
Open airway
Check breathing
Call 123
30 chest compressions
2 rescue breaths

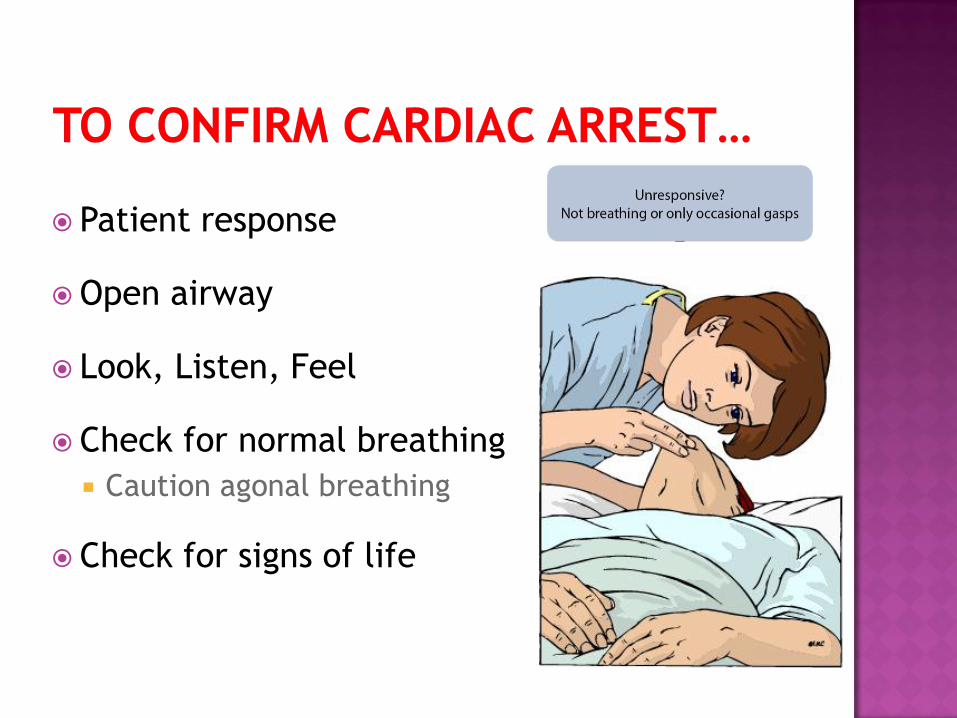
Patient response
Open airway
Look, Listen, Feel
Check for normal breathing
Caution agonal breathing
Check for signs of life
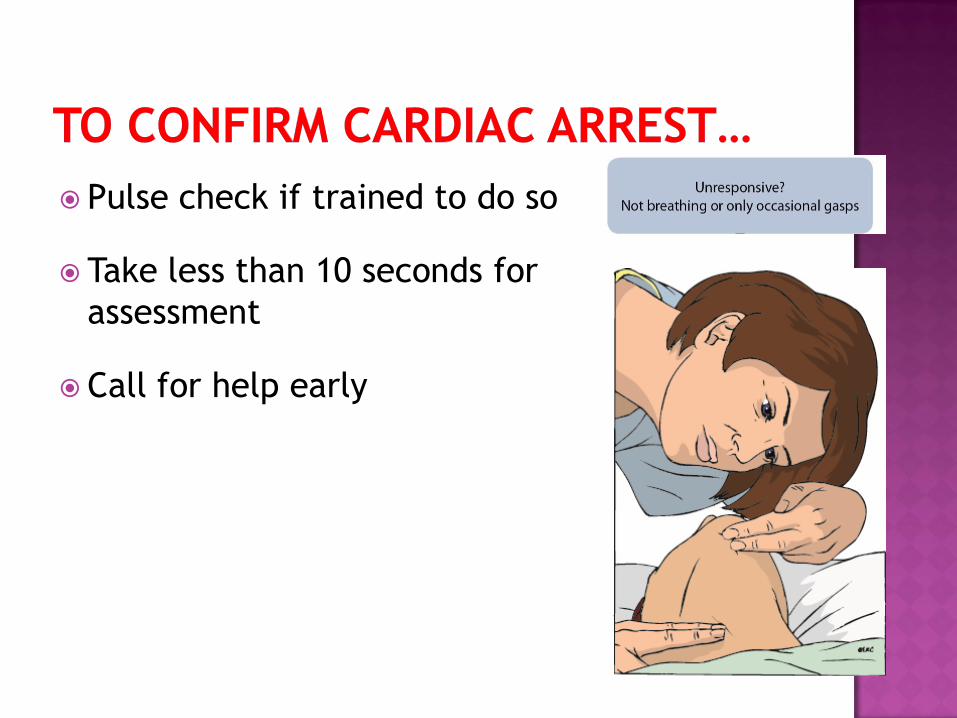
Pulse check if trained to do so
Take less than 10 seconds for
assessment
Call for help early
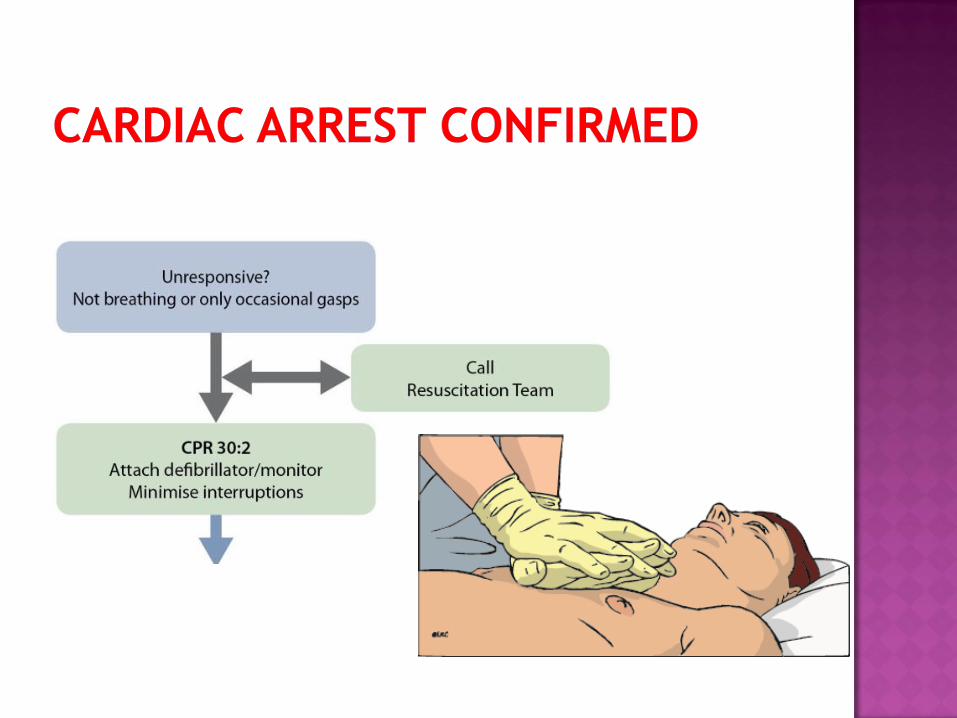
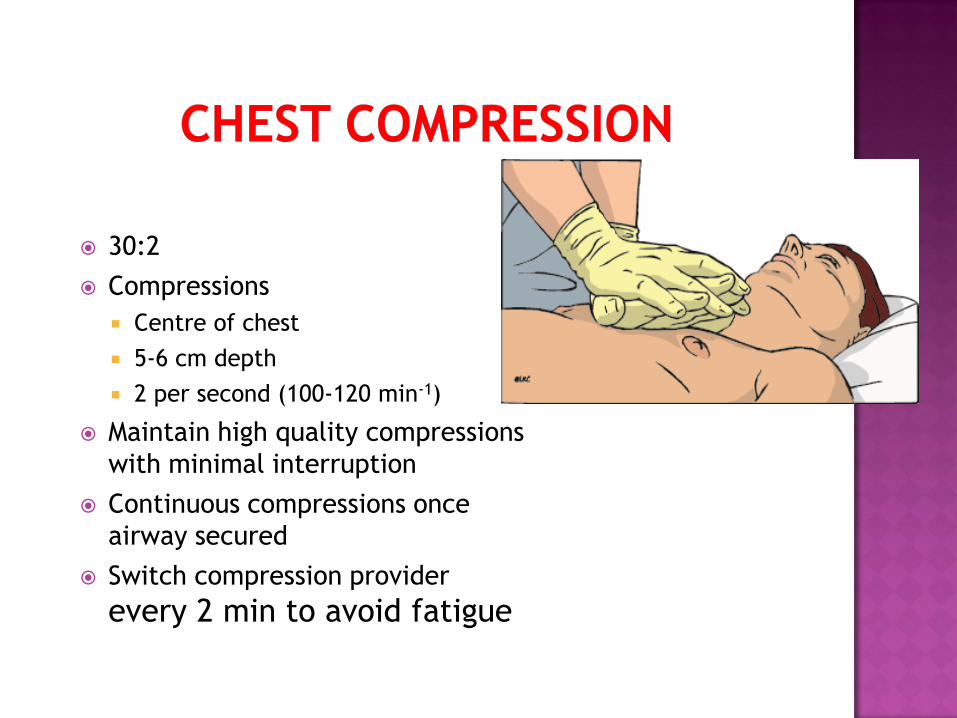
30:2
Compressions
Centre of chest
5-6 cm depth
2 per second (100-120 min-1)
Maintain high quality compressions
with minimal interruption
Continuous compressions once
airway secured
Switch compression provider
every 2 min to avoid fatigue
Team Means:
Monitor
Skilled Persons
Drugs
Start With Monitor
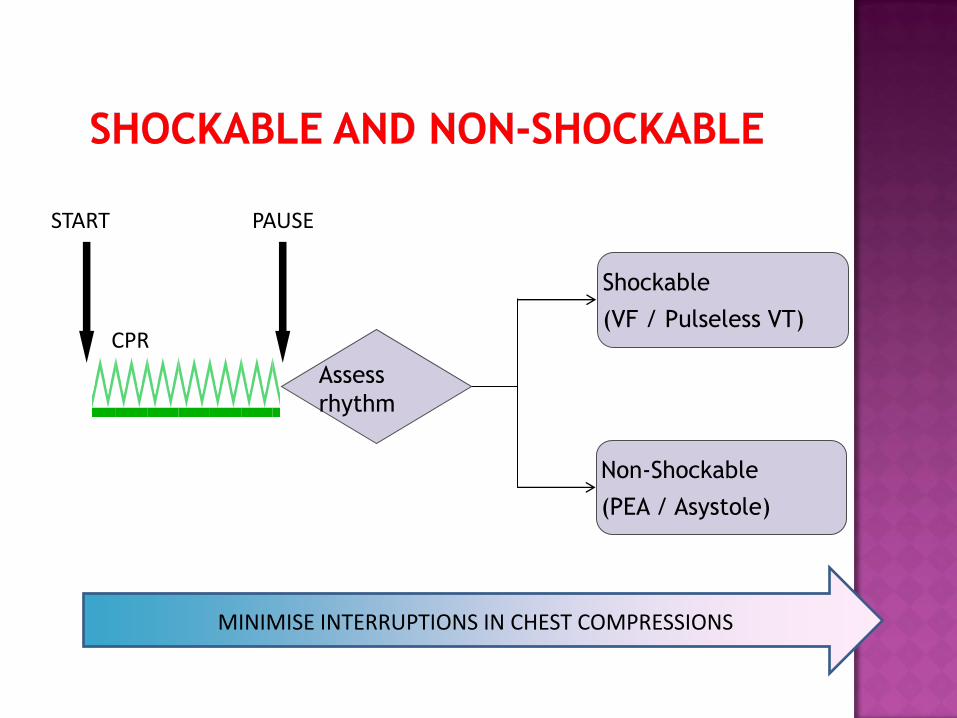
MINIMISE INTERRUPTIONS IN CHEST COMPRESSIONS
START PAUSE
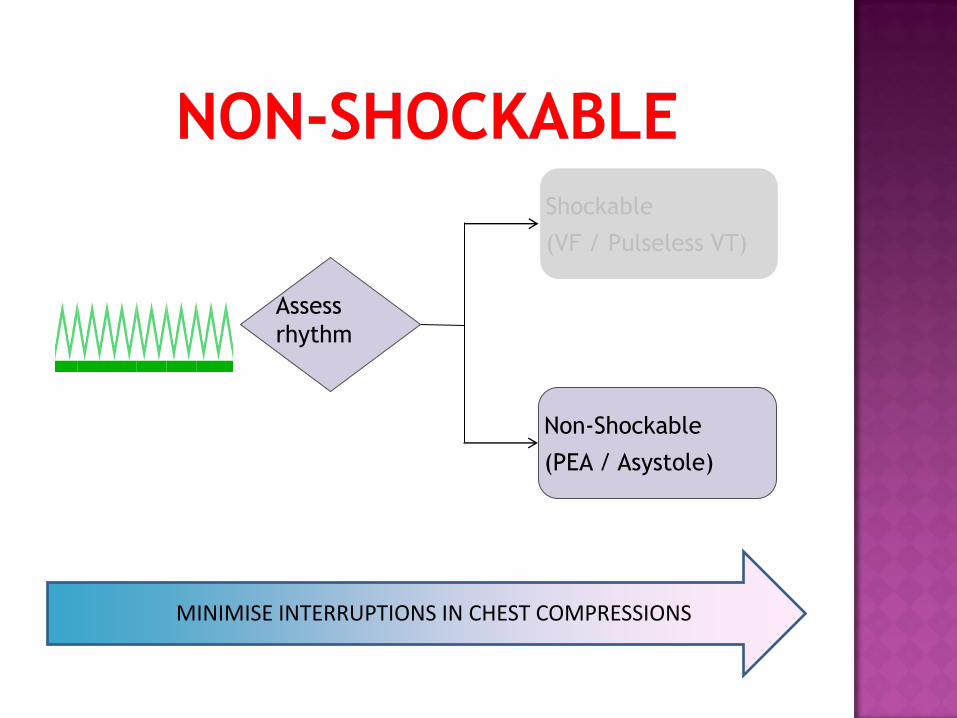
Assess
rhythm
Shockable
(VF / Pulseless VT)
Non-Shockable
(PEA / Asystole)
CPR
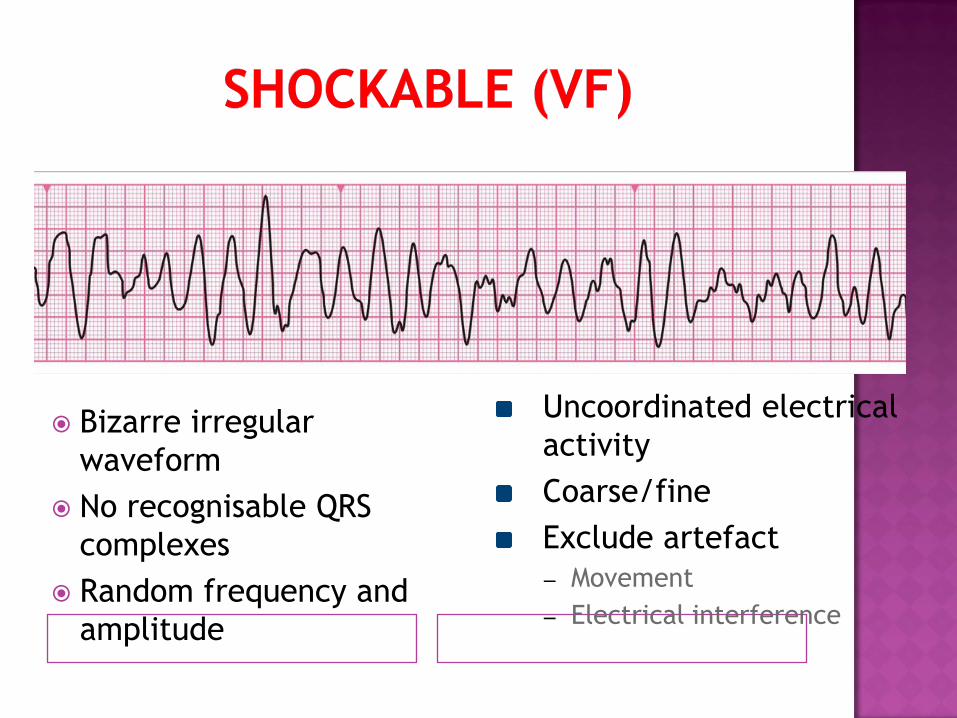
Bizarre irregular
waveform
No recognisable QRS
complexes
Random frequency and
amplitude
Uncoordinated electrical
activity
Coarse/fine
Exclude artefact
– Movement
– Electrical interference
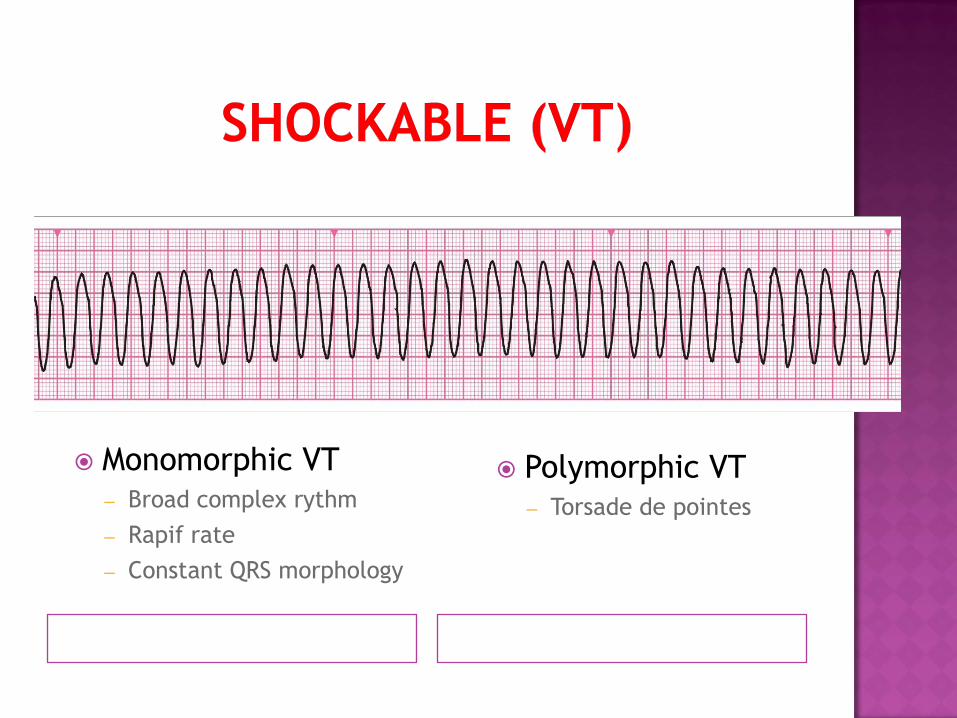
Monomorphic VT – Broad complex rythm
– Rapif rate
– Constant QRS morphology
Polymorphic VT – Torsade de pointes
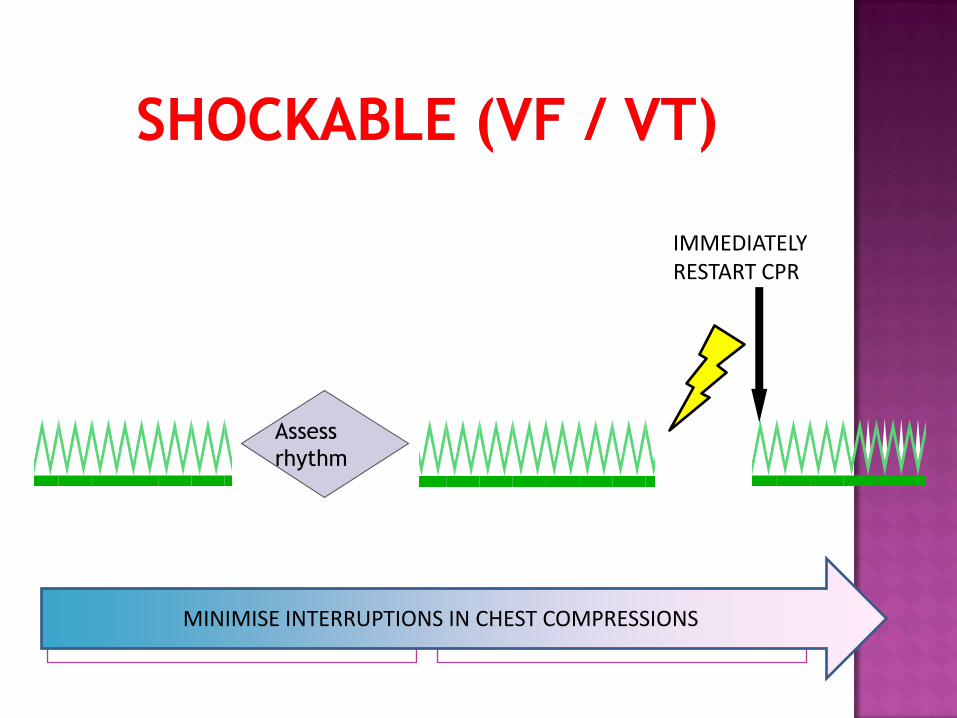
MINIMISE INTERRUPTIONS IN CHEST COMPRESSIONS
Assess
rhythm
IMMEDIATELY RESTART CPR
MINIMISE INTERRUPTIONS IN CHEST COMPRESSIONS
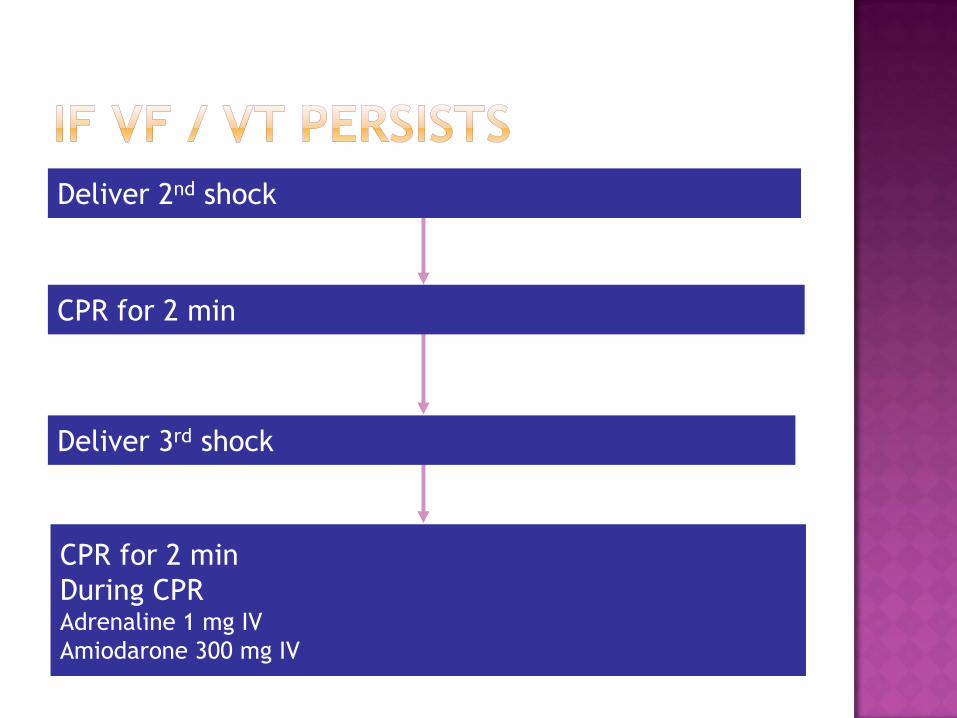
CPR for 2 min
CPR for 2 min
During CPR Adrenaline 1 mg IV
Amiodarone 300 mg IV
Deliver 2nd shock
Deliver 3rd shock
Assess
rhythm
Shockable
(VF / Pulseless VT)
Non-Shockable
(PEA / Asystole)
MINIMISE INTERRUPTIONS IN CHEST COMPRESSIONS
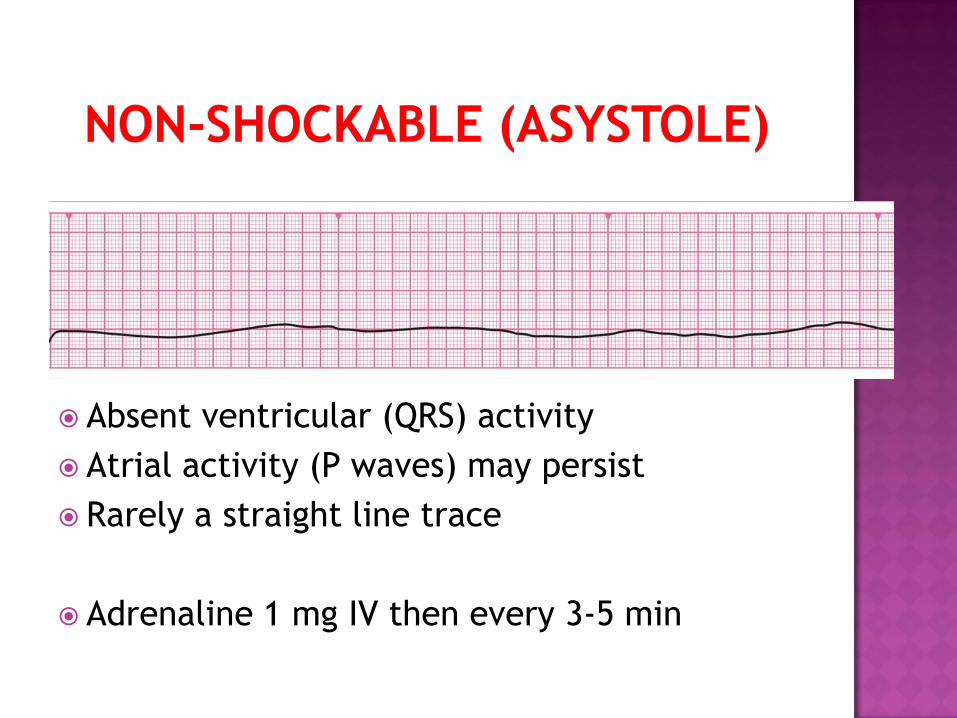
Absent ventricular (QRS) activity
Atrial activity (P waves) may persist
Rarely a straight line trace
Adrenaline 1 mg IV then every 3-5 min
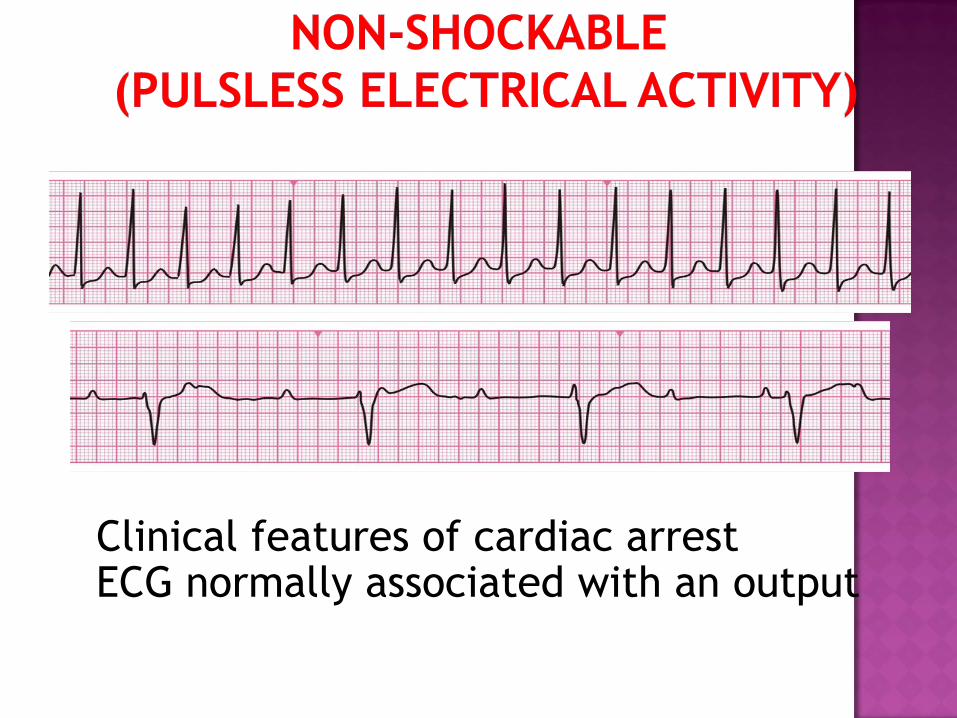
Clinical features of cardiac arrest ECG normally associated with an output
Adrenaline 1 mg IV every 3-5 min
Continue chest compression and ventillation
Assesment of rhythm every 2 minutes

Any questions

















