30
Abdominal Compartment Syndrome John Hartley Academic Surgical Unit The University of Hull
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | homer-bryce-gregory |
| View: | 244 times |
| Download: | 1 times |

Abdominal Compartment Syndrome
John Hartley
Academic Surgical Unit
The University of Hull
Abdominal Compartment Syndrome (ACS)
Definition
“The adverse physiological consequences of
an acute elevation in intra-abdominal pressure”- Oliguria- Increased airway pressures- Reduced cardiac output
Abdominal Compartment Syndrome
Historical background
The perils of elevated intra-abdominal pressure…• 1890’s elevation of IAP caused death in animal
models• 1911 cardiovascular effects of raised IAP
identified• 1913 effects of raised IAP on renal function• 1980’s abdominal decompression for IAP
Abdominal Compartment Syndrome
Acute elevation IAP >30mmHgPost-op
Acute elevation IAP >30mmHgPost-op
Oliguria in 11 ptsOliguria in 11 pts
7 ptsRe-exploration Decompression
7 ptsRe-exploration Decompression
4 pts Not re-explored
4 pts Not re-explored
Immediate diuresisImmediate diuresisRenal failure
and diedRenal failure
and died
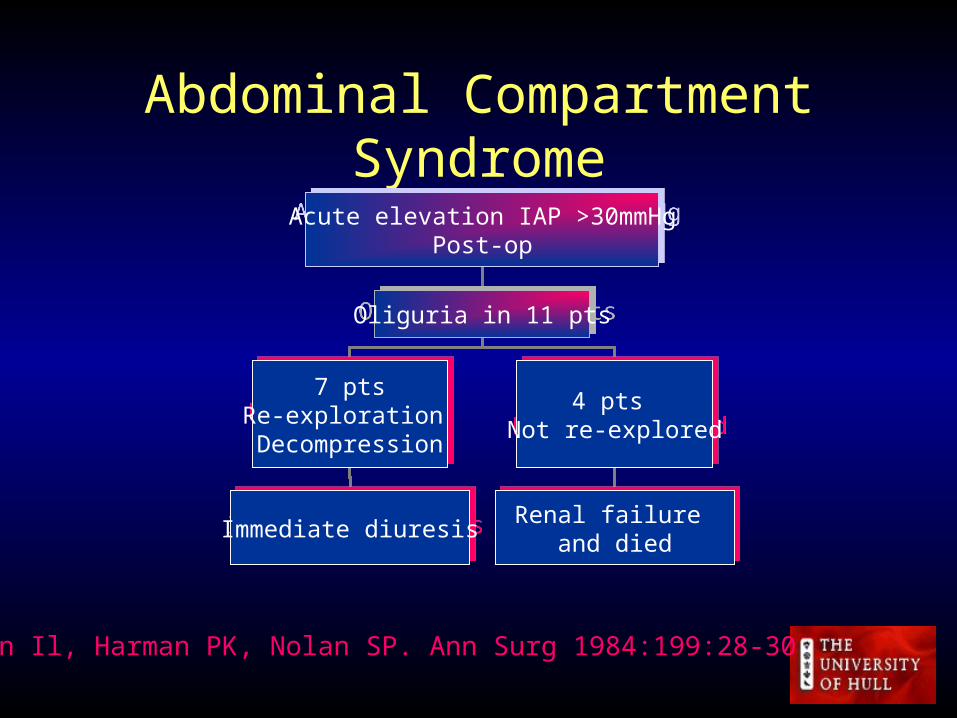
Kron Il, Harman PK, Nolan SP. Ann Surg 1984:199:28-30

Abdominal Compartment Syndrome
abdominal pressure abdominal pressure
Compression of kidneysCompression of kidneys Venous return Venous return Intrathoracic pressures Intrathoracic pressures
Renal blood flow Urine output
Renal blood flow Urine output
CO VEDV SV SVR
Oxygen delivery
CO VEDV SV SVR
Oxygen delivery
Hypoxaemia Airway pressures
Compliance PA pressures CVP readings
Hypoxaemia Airway pressures
Compliance PA pressures CVP readings
ICP
Pathophysiology
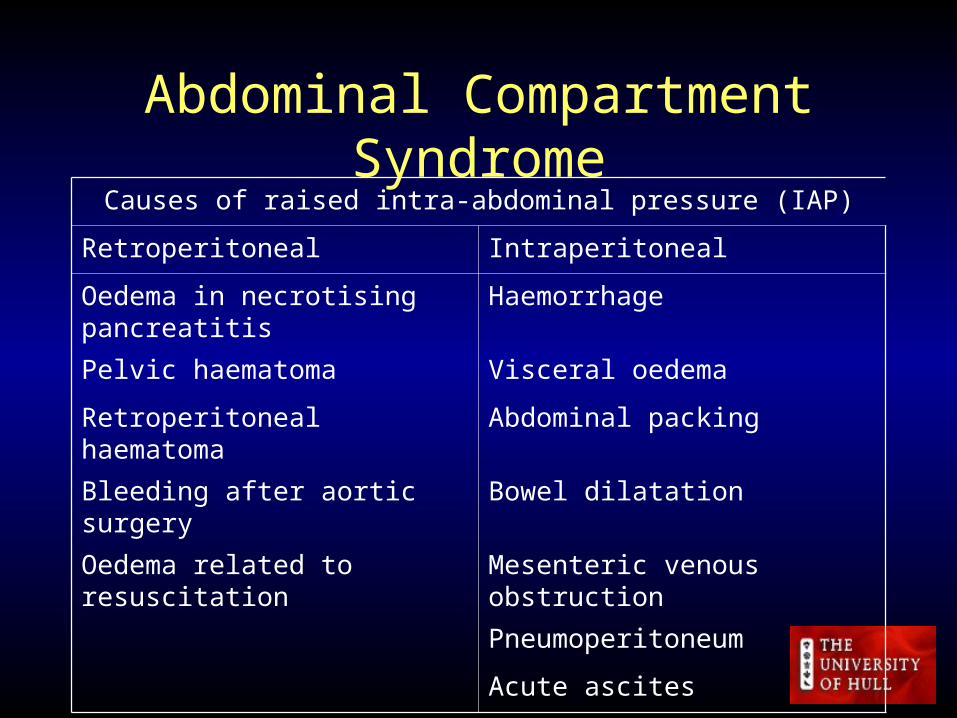
Abdominal Compartment SyndromeCauses of raised intra-abdominal pressure (IAP)
Retroperitoneal Intraperitoneal
Oedema in necrotising pancreatitis Haemorrhage
Pelvic haematoma Visceral oedema
Retroperitoneal haematoma Abdominal packing
Bleeding after aortic surgery Bowel dilatation
Oedema related to resuscitation Mesenteric venous obstruction
Pneumoperitoneum
Acute ascites
Abdominal Compartment Syndrome
At risk patients
• Major trauma
• Damage control surgery
• Laparotomy for bleeding, ischaemia etc
• Re-laparotomy for postoperative complications
• Massive volume resuscitation
Abdominal Compartment Syndrome
Clinical features• Abdominal distension• ELEVATED IAP• Consequent organ dysfunction
Importance• Decompression can reverse abnormal physiology• Probable fatal progression if left untreated

Abdominal Compartment Syndrome
Measurement of IAP
• Indirect assessment of IAP by bladder pressure
• 50-100ml saline into bladder
• Manometer readings from symphysis pubis

Abdominal Compartment Syndrome
Problems• What value of IAP should cause concern?• Level beyond which ACS is irreversible?• ABSOLUTE IAP UNHELPFUL
– >20mmHg significant in all pts– >15mmHg significant in many– >12mmHg significant in some
Malbrain ML. Intensive Care Med 1999;25:1453-58

Abdominal Compartment Syndrome
Survey of British practice• 137 of 207 hospitals (66.2% response)• 1.5% (n=2) no knowledge of ACS• Some measurement IAP 76% (n=104)• Upon suspicion of ACS 93% (n=97)• No consensus on frequency of measurement or indication
for decompression
Ravishankar N, Hunter J.Br J Anaesth 2005;94:763-6

Abdominal Compartment Syndrome
Incidence• Prospective measurement of IAP in 9 months
admissions to trauma ICU• 15 of 706 pts IAH (2%)• 6 of 15 pts with IAH developed ACS (1%)• 50% mortality in ACS and 2 of 9 with IAH
Hong JJ, Cohn SM, Perez JM et al Br J Surg2002;89:591-6
Abdominal Compartment Syndrome
Abdominal decompression• Reversal of abnormal parameters in approx 80%• Mean survival approx. 50%• Intervention too late?• Inevitable SIRS and MOF?• PREVENTION BETTER THAN CURE
Sugrue MD’Amour S. J Trauma 2001;51:419
Abdominal Compartment Syndrome
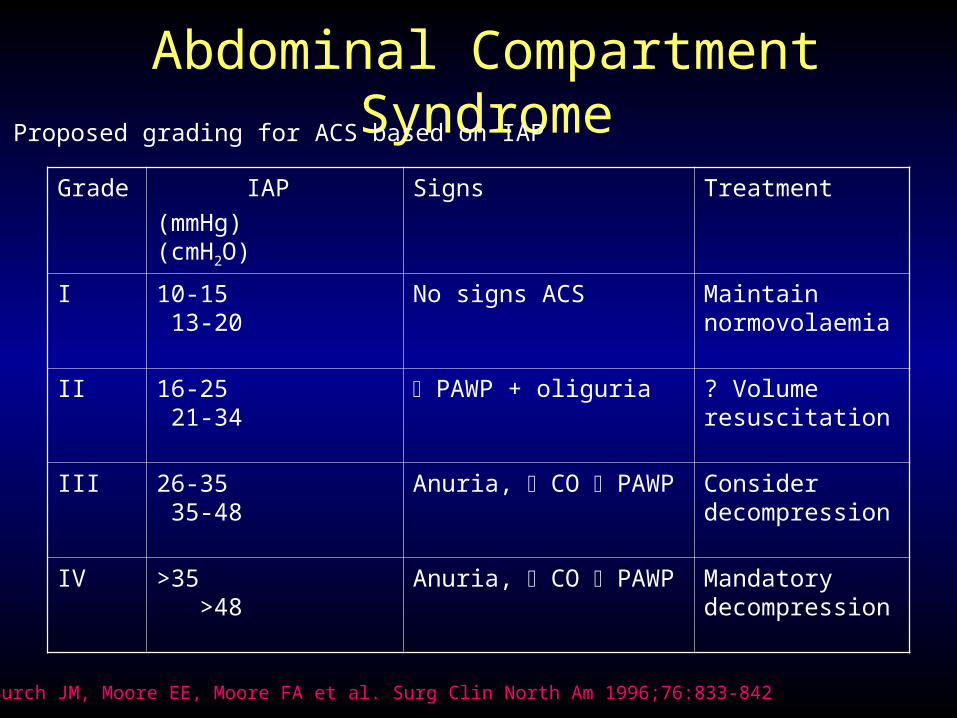
Grade IAP
(mmHg) (cmH2O)
Signs Treatment
I 10-15 13-20 No signs ACS Maintain normovolaemia
II 16-25 21-34 PAWP + oliguria ? Volume resuscitation
III 26-35 35-48 Anuria, CO PAWP Consider decompression
IV >35 >48 Anuria, CO PAWP Mandatory decompression
Proposed grading for ACS based on IAP
Burch JM, Moore EE, Moore FA et al. Surg Clin North Am 1996;76:833-842

Abdominal Compartment Syndrome

Abdominal Compartment Syndrome
Conclusions
• Concept of ACS important
• True incidence and significance unclear
• Increasing awareness and measurement of IAP may lead to:
- Better understanding of pathophysiology
- Evidence based management

Abdominal Compartment Syndrome
• World Society on Abdominal
Compartment Syndrome
• www.wsacs.org
• Antwerp 24th-27th March 2007
Abdominal Compartment Syndrome
Renal effects• IAP 15-20mmHg RBF and GFR with anuria when
>30mmHg• No effect of stenting• Parenchymal compression and renal vascular resistance• Reversible by decompression
Harman PK, Kron IL, McLachlan HD et al Ann Surg1982;196:594-7

Abdominal Compartment Syndrome
Gut and hepatic effects splanchnic and hepatic blood flow flow in animal models with IAP>10mmHg• Ischaemia at >40mmHg• Gastric mucosal acidosis with IAP improves
with decompressionIvatury RR, Porter JM, Simon RJ et al J Trauma1998,44:1016-21
Abdominal Compartment Syndrome
Other means of detection• CT changes
- Narrowing of IVC- Direct renal compression- Bowel wall thickening- “Rounded abdomen”
• Splanchnic hypoperfusion and acidosis• Abdominal perfusion pressure
Abdominal Compartment Syndrome
Management of ACS – the issues
• Indication for decompression
• Timing of decompression
• “point of no return”
• Subsequent laparostomy management
Abdominal compartment syndrome
• Definition
• The adverse physiological consequences that occur as a result of an acute increase in IAP
Abdominal compartment syndrome
• Management of ACS
• Indication for decompression
• Timing of decompression
• “point of no return”
• Subsequent laparostomy management
Abdominal Compartment Syndrome
Effects of intra-abdominal hypertension (IAH)
• Gut and hepatic effects
• Renal effects
• Cardiovascular effects
• Respiratory effects
• CNS
• Abdo wall
Abdominal Compartment Syndrome
Cardiovascular effects venous return by compression of IVC and
portal vein intra-thoracic pressure, LV compliance,
cardiac contractility and CO peripheral oxygen delivery
Abdominal Compartment Syndrome
Respiratory effects
• Elevation of diaphragm, thoracic volume and compliance, intra-pleural pressure
airway pressures to maintain ventilation
• Compressive atelectasis and V/Q mismatch, hypoxia, hypercarbia, acidosis
Abdominal Compartment Syndrome
• Acute elevation of IAP above 30mmHg caused oliguria in 11 postoperative pts
• Re-exploration and decompression in 7 pts resulted in immediate diuresis.
• 4 pts not re-explored developed renal failure and died.• If IAP > 25mmHg in the early post period is assoc. with
oliguria and normal blood pressure and cardiac index, the patient should undergo re-exploration and decompression of the abdomenKron Il, Harman PK, Nolan SP. Ann Surg 1984:199:28-30

Abdominal Compartment Syndrome
CNS effects• Impaired venous return and cerebral pooling intra-cranial pressure
Ertel W, Oberholzer A, Platz A et al Crit CareMed 2000; 28:1747-53

Abdominal Compartment Syndrome
Early detection
• Survey trauma surgeons USA
• 6% measured IAP routinely
• 59% selectively
Mayberry JC, Goldman RK, Mullins RJ.
J Trauma 1999;47:509-513
















![Abdominal Compartment Syndrome (ACS); · developing intra-abdominal hypertension and abdominal compartment syndrome. Acta Anaesthesiol Scand.58,1267–1275. [PubMed] 13. Kim IB, Prowle](https://static.documents.pub/doc/80x56/6004869f58479d049b555e4b/abdominal-compartment-syndrome-acs-developing-intra-abdominal-hypertension-and.jpg)
