28
Morganella 2/6/2017 Subhas Chandra Aryal 1
| Date post: | 16-Jan-2017 |
| Category: |
Education |
| Upload: | subhas-chandra-aryal |
| View: | 164 times |
| Download: | 0 times |
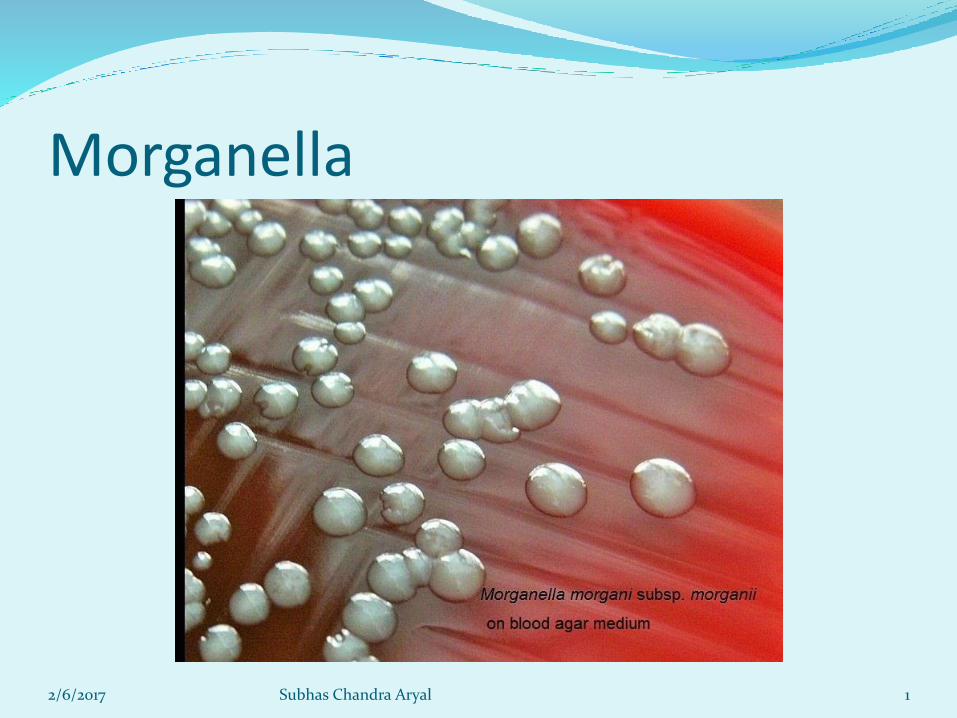
Morganella
2/6/2017 Subhas Chandra Aryal 1

Classification Phylum: Proteobacteria
Class: Gammaproteobacteria
Order: Enterobacteriales
Family: Enterobacteriaceae
Genus: Morganella
Species: morganii
Sub species: morganii (trehalose non-fermenter)
Biogroups: A,B,C,D
Sub species: sibonii(trehalose fermenter)
Biogroups : E,F,G
2/6/2017 Subhas Chandra Aryal 2
Subspecies further divided in to biogroups Four biogroups ( A, B, C, and D) of M. morganii
subspecies morganii Based largely on the ability of strains to form lysine or
ornithine decarboxylase or both or neither.
Biogroup A is ODC+/LDC-, Biogroup B ODC+/LDC+,Biogroup C is ODC-/LDC-, Biogroup D is ODC-/LDC+,
Three biogroups (E, F, and G)of M. morganiisubspecies sibonii Based on the ability of strains to produce lysine or
ornithine decarboxylase or both, and indole and grow inthe presence of KCN
Biogroup E is ODC+/LDC+, Biogroup F is ODC-/LDCvariable, and Biogroup G is ODC+/LDC-
2/6/2017 Subhas Chandra Aryal 3
Genus name: named after the British bacteriologist H. de R. Morgan, who first studied this organism.
G + C content of the DNA is 50 mol%.
HABITAT Intestinal and feces pathogen of man, other mammals, and
reptiles. MACROSCOPIC APPEARANCE Some Morganella strains appear hemolytic when cultured
on Blood Agar, while others produce a reddish-brown pigmentation.
METABOLIC PROPERTIES Facultatively anaerobic. Chemoorganotrophic, having both
fermentative and respiratory type metabolism. Acid production from mannose, but gas is not produced.
2/6/2017 Subhas Chandra Aryal 4

MICROSCOPIC APPEARANCE Gram Stain: Gram-negative.
Morphology: Straight rods.
Size: 0.6-0.7 micrometers by 1.0-1.7 µm.
Motility: Motile by peritrichous flagella (less than 30 ˚c) and nonmotile (above 30°C), swarming does not occur.
Capsules: None.
Spores: None.
Other: Originally classified in the genus Proteus as Proteus morganii .
2/6/2017 Subhas Chandra Aryal 5
KEY BIOCHEMICAL REACTIONS Oxidase-negative.
Catalase-positive.
Urease-positive.
Indole-positive.
Voges-Proskauer-positive.
Simmons-Citrate-negative.
Methyl-Red-positive.
H 2 S-negative.
Phenylalanine deaminase:positive.
Ornithine-decarboxylase-positive.
Produces acid from mannose.
2/6/2017 Subhas Chandra Aryal 6
RECOMMENDED MEDIA
For culture: Tryptic Soy Agar (TSA), Blood Agar 5%.
For selective isolation: MacConkey Agar, EMB Agar, Selenite Broth, Tetrathionate Broth.
For maintenance: Tryptic Soy Agar for short-term maintenance and lyophilization for long-term preservation.
INCUBATION
Temperature: 35 degrees C. Time: 18-24 hours. Atmosphere: Aerobic.
2/6/2017 Subhas Chandra Aryal 7

Fermentation of carbohydrates • Acidify glucose, usually with gas formation,
and mannose
• Do not acidify lactose, sucrose, salicin,mannitol, xylose, adonitol, or inositol.
• Because of an inability to acidify sucrose andlactose, M. morganii strains form colorlesscolonies on MacConkey, eosin-methyleneblue, xylose-lysine-deoxycholate, andSalmonella-Shigella agars.
2/6/2017 Subhas Chandra Aryal 8
IntroductionMorganella morganii
Are small, Gram-negative, motile bacilli, but unlike Proteus species do not produce swarming on solid media.
Oxidase negative; catalase, indole, citrate and urease positive.
They are facultatively anaerobic and non-encapsulated found in the feces and intestines of humans, dogs, and other mammals.
Grow on blood agar or on Mac-Conkey agar.
Ferments glucose and mannose but not lactose.
Decarboxylate ornithine, hydrolyze urease, and reduce nitrates.
Do not liquefy gelatin and do not produce hydrogen sulfide.
2/6/2017 Subhas Chandra Aryal 9
It is known to be a causative organism of opportunistic infections in the respiratory tract, the urinary tract, and in wound infections.
It can cause devastating infections in the neonates and postoperative stages, especially in diabetic patients .
The risk of infection is particulary high when a patient becomes neutropenic( neutrophils) as a result of myelosuppressive (bonemarrow suppresion) chemotherapy .
Massive hemolysis can be associated with bacterial infection and has been reported mainly in cases of Clostridial or Vibrio sepsis .
2/6/2017 Subhas Chandra Aryal 10

History The first isolation of this bacteria was done by a man named Castellani
in 1905, and he named it Bacterium columbensea.
In 1906 when Morgan came across this bacteria while studying summer infantaile diarrhea .
he was unaware that it was indeed the same bacteria that was found by Castellani. Morgan described this as a non-lactose fermenting bacteria - different from the other Bacillus type bacteria. He named this Morgan's Bacillus .
It was later named, in 1919, Bacillus morganii by Winslow.
Years later, Rauss performed further evaluation of the bacteria and realized it was very similar to the Proteus group and although there were marked differences, he renamed the bacteria Proteus morganii.
2/6/2017 Subhas Chandra Aryal 11
History....contdFinally in 1943, Fulton made the connection that the
bacteria Proteus morganii was in fact the same bacteria discovered by Castellani in 1905 and he proposed a new genus name of Morganella. The species would be called M. morganii and Castellani's species would be called M. columbensis. M. morganii was unable to ferment lactose or sucrose but was able to produce indole.
In 1962, Ewing found the M. columbensis was actually E. coli, which left M. morganii as the only species in the genus. This led Ewing to disregard the genus and relate moganii to the Proteus genus.
2/6/2017 Subhas Chandra Aryal 12

Finally in 1976, morganii was put in its rightful place in the genus of Morganella.
The differentiation between the two genera was finally made by Brenner using DNA-DNA hybridization, which showed less than 20% homology between P. morganii and Proteus. The differences were further backed by the ability for trehalose fermentation (O'Hara et al., 2000).
Morganella is also distinguishable from the genus Proteusby the lysine iron agar test and by the ability of the genus Proteus to differentiate in to swarmer cells when colonizing a new habitat (Manos & Belas, 2006).
2/6/2017 Subhas Chandra Aryal 13

Clinical manifestations GI diarrhoea Sepsis(presence of pus forming bacteria or their toxins in blood or
tissues) Pneumonia Wound infections Pericarditis(inflammation of pericardium)
Chorioaminonitis (inflammation of the fetal membranes (amnion and chorion)
Endophthalmitis (purulent inflammation of the intraocular fluids)
Empyema (collection of pus in body cavity) Spontaneous bacterial peritonitis (inflamation of peritoneum) CNS infections Ear and sinus infections
2/6/2017 Subhas Chandra Aryal 14

Genome structure
.M. morganii has a complete genome sequence (3,826,919-bp) with a G+C content of 51.15%
3,565 protein-coding sequences
Genes encoding for drug resistance are ;
ampC-ampR, MBL, Tellurite resistance operon, and Tetracycline resistance
blaCTX-M, blaSHV, blaTEM, blaOXA
2/6/2017 Subhas Chandra Aryal 15

VIRULENCE FACTORS Adhesins
Hemolysin Calcium-dependent The hemolysin is serologically and functionally identical to E.
coli hemolysin HlyA and is associated with high virulence of strains for mice and chick embryos
Urease Constitutively produced Active at acidic pH, promote colonization of intestinal
epithelium protecting against the acidity of stomach
Other enzymes
2/6/2017 Subhas Chandra Aryal 16

PATHOGENICITY There is considerable evidence that Morganella
species play a pathogenic role in urinary tract infections, particularly for those of nosocomial origin. It is an opportunistic secondary invaders rather than a primary pathogen at other sites and has been isolated from bacteremias, respiratory tract, and wound infections.
2/6/2017 Subhas Chandra Aryal 17
Type IV pili: adheres to hosts The ability of Morganella to cause infections in the urinary tract may be
due to the MR/K hemagglutinin that enhances adherence to urinary catheters . Additionally, Morganella produces a urease that predisposes to encrustation of urinary catheters .
The Morganella urease also can be activated at a low pH, which may enhance the bacterial survival at low pH. This can have many adverse effects including the formation of stones causing renal damage, and it can also lead to a urinary tract infection (Manos & Belas, 2006).
Morganella species may also produce a hemolysin, which enhances virulence by lysing erythrocytes due to the formation of hydrophilic pores in the cell wall .
Due to its highly mobile state, Morganella is able to rapidly colonize the gut. Coupled with enlargement of the Peyer’s patches in the gut and specific IgA responses, it is able to change the environment of the host very quickly.
2/6/2017 Subhas Chandra Aryal 18
Risk factors for M. morganiiinfection include the following
Prior exposure to ampicillin and other beta-lactamantibiotics
Diabetes mellitus
Advanced age
Surgical procedures
Perinatal exposure
Abscesses or soft tissue infections following snakebite
2/6/2017 Subhas Chandra Aryal 19
Antibiotic tests Susceptible to Resistant to
Cefepime
Imipenem
Meropenem
Piperacillin
Aminoglycosides
Ceftazidime
Other 3rd generation
cephalosporins
2/6/2017 Subhas Chandra Aryal 20
Laboratory diagnosis Specimens: faeces,urine, wound and ear discharges Diagnosis: culture Identification of M. morganii is made by recovery of small,
non-fermenting colonies, oxidase-negative, catalase and indole-positive gram-negative rods on blood agar or MacConkey agar.
M. morganii ferments glucose and mannose but not lactose.
M morganii is motile(at tempr below 30°C), facultativelyanaerobic, and nonencapsulated, and it hydrolyzes urease and reduces nitrates.
Unlike Proteus species, swarming does not occur. M. morganii urinary tract infections are often associated
with an alkaline urine pH.2/6/2017 Subhas Chandra Aryal 21

Culture on phenylalanine deaminase agar medium : + Production of green colour (Phenylpyruvic acid thus formed reacts with ferric chloride producing a green colored compound thus turning the medium dark green).
Mac-Conkey agar: flat, colorless 2 to 3 mm non-lactose fermenting colonies.
Sheep-blood agar: flat, colorless 2 to 3 mm colonies, no swarming, Some strains appear hemolytic, while others produce a reddish-brown pigmentation.
Eosin-methylene Blue Agar (EMB): colorless or light purple colonies.
Triple Sugar Iron Agar (TSI): Yellow butt, red slant (K/A) = ferments glucose only, no H2S,no gas
Catalase: +Oxidase: -IMViC: +++-
2/6/2017 Subhas Chandra Aryal 22

ANTIMICROBIAL THERAPY The antibiotic of choice depends upon the site of infection, the
nature of the host and the local pattern and prevalence of resistance.
Bacteremia: A third-generation cephalosporin , aminoglycoside +cephalosporin::a course of at least 2 weeks appears reasonable.
Urinary Tract Infection:oral quinolones like ciprofloxacin, third generation cephalosporins and trimethoprim-sulfamethoxazole.
Wound Infection:a broad-spectrum agent such as piperacillin-tazobactam, third generation cephalosporins like ceftriaxone, cefipime or a quinolone with an antianaerobic drug.
For infections caused by an ESBL-producing strain, the drug of choice is generally a carbapenem.
2/6/2017 Subhas Chandra Aryal 23

Intra-abdominal Infection: Broad-spectrum antibiotic such as piperacillin-tazobactam are the first choice; other options include the use of third generation cephalosporins like ceftriaxone, cefipime or a fluoroquinolone.
Neonatal Infections: a third generation cephalosporin such as cefotaxime and an aminoglycoside.
Underlying Diseases: treatment of other diseases The third-generation cephalosporins ceftriaxone, cefotaxime, and
ceftazidime are more active against Morganella, with MIC90s ranging from 0.03 to 32 mg/mL .The MICs for cefotaxime and ceftazidime are 0.015 and 0.06 mg/mL for inducible strains but 4 and 8 mg/mL for constitutive hyperproducers, respectively.
Trimethoprim-sulfamethoxazole is also active against some Morganella (MIC50s-0.06 mg/mL; MIC90s 16 mg/mL)
The fluroquinolones are highly active against Morganella, with the MIC90s for most isolates below 0.25 mg/mL
2/6/2017 Subhas Chandra Aryal 24
VACCINES
There are no vaccines in development against Morganella.
2/6/2017 Subhas Chandra Aryal 25
PREVENTION OR INFECTION CONTROL MEASURES
• Checking of rectal conlonizers of this organism, vigorous handwahingpractices, use of contact isolation for infected or colonized patients could prevent the spread of antimicrobial resistance and ESBL producers.
• Hospital policy regarding antibiotic use may play important role in scenarios when multiple clones of ESBL producers are present in hospital.
2/6/2017 Subhas Chandra Aryal 26
References Chen et al ,2012, Whole-genome sequencing and identification
of Morganella morganii KT pathogenicity-related genes,BMCgenomics, licensee BioMed Central Ltd.
Monas j and belas R (2006), prokaryotes ,www.yumphu.com/articles ,(6),245-269.
Parija SC,(2012) textbook of microbiology and immunology,2nd
edition, A division of Reed Elsevier India private ltd., India . O’Hara, C. M., Brenner, F. W. & Miller, J. M.
(2000).Classification,identification, and clinical significance of Proteus,Providencia, and Morganella.Clin Microbiol Rev 13,534–546.
Patil AB, Nadagir SD, Lakshminarayana SA, and Syeda FM. (2012), Morganella morganii, subspecies morganii, biogroup A: An unusual causative pathogen of brain abscess, J Neurosci Rural Pract. 3(3): 370–372.
https://microbewiki.kenyon.edu/index.php/Morganella_marganaii
2/6/2017 Subhas Chandra Aryal 27
2/6/2017 Subhas Chandra Aryal 28

















