We report flow cytometric characterization of surface CD26 expression in 271 peripheral blood samples from 154 patients evaluated for the presence of a T-cell lymphoproliferative disorder, primarily mycosis
fungoides/Sézary syndrome (MF/SS). The presence of morphologically identifiable tumor cells on peripheralblood smears was the criterion for lymphomatousinvolvement. In 66 of 69 samples from 28 patients, weidentified an abnormal CD26–/dim T-cell populationthat was distinct from the variable CD26 expressionseen in normal peripheral blood T cells. This
population was CD26– in 23 patients and weaklyCD26+ in 5 patients. CD7 was more variably expressed in MF/SS tumor cells, allowing recognition of a distinct,quantifiable abnormal T-cell population in only 34 of 69 involved samples. An increased CD4/CD8 ratio and lower surface expression of CD4 in tumor cells alsohelped separate the CD26–/dim atypical population for quantification. In 35 blood samples from other types of T-cell tumors, tumor cells in 10 of 11 morphologicallyinvolved cases showed absent/dim CD26. Althoughcapable of detecting abnormalities in most cases of
MF/SS, CD7 expression does not provide as clear a
separation of the neoplastic population and can bereplaced by CD26 staining in routine peripheral blood
flow cytometric screening of MF/SS patients.
Mycosis fungoides (MF) is a cutaneous lymphomacomposed of CD4+ T cells with a skin-homing phenotype. Arelated disorder, Sézary syndrome (SS), is characterized bymanifestation as a diffuse erythrodermic rash with substantialnumbers of circulating tumor cells. A subset of patients withtypical MF also develop SS when the disease progresses. Thepresence of peripheral blood involvement in MF is a negativeprognostic factor. 1,2 Molecular studies have detected evidenceof clonal T cells in the peripheral blood in many patients withMF, likely representing the circulation of small numbers of tumor cells. 2-5 However, the clinical significance of such low-level peripheral blood involvement, detected only by poly-
merase chain reaction analysis, is unclear given the presenceof such clones in patients with clinically localized cutaneousdisease. 6
MF/SS in blood has a variety of morphologic appear-ances, including small irregular cells, markedly convolutedclassic “Sézary” lymphocytes, and larger nucleolated forms.Because of this variable appearance, accurate enumeration of tumor cells by manual differential can be difficult. For thesereasons, flow cytometric analysis is used routinely in manycenters to identify circulating MF cells in peripheral blood.Diagnostic criteria have included absolute increases in CD4+T cells, an elevation of the CD4/CD8 ratio, and increases in
the number of CD7– T cells. 7-11 However, all of these parame-ters also can be increased in the peripheral blood in nonneo-plastic conditions, including inflammatory dermatoses,hindering the definitive diagnosis of MF/SS or other T-celltumors. 8,9,11 CD26 is a well-characterized surface proteolyticenzyme that is expressed in the majority of lymphocytes inperipheral blood. 12 We report that absent or dim CD26expression is a feature of almost all cases of MF and can beused to allow more sensitive flow cytometric detection andquantitation of tumors cells than the use of CD7.
We analyzed 271 consecutive peripheral blood samples(from 154 patients) submitted for evaluation of involvementby a T-cell lymphoproliferative disorder to the immunologylaboratory at the University of Texas–M.D. Anderson CancerCenter, Houston, during a 5-month study period (4 monthscontinuous with 1 subsequent month of follow-up). In 83%of the cases, correlation was made with the morphologicfindings in peripheral blood smears or bone marrow aspiratesprepared from a sample from the same day. For theremaining cases, comparison was made with peripheralblood smears from other dates, usually within a week of theanalyzed cytometry sample. Lymphoma cells, defined aseither Sézary cells with markedly convoluted nuclearcontours or enlarged (nucleolated) lymphocytes, were quan-titated by 100-cell manual differential by one of us (D.J.).Serial samples from the same patient were examined, whenavailable, to establish the characteristic morphologic featuresof each patient’s tumor.
Diagnoses of patients were MF (94), SS (11, 1 in remis-sion), nodal peripheral T-cell lymphoma (12), cutaneousanaplastic large cell lymphoma (3), cutaneous T-cell lym-phoma, not otherwise specified (6), CD8+ leukemia/ lymphoma (2), natural killer cell lymphoma (2), large gran-ular lymphocyte (LGL) leukemia (2), atypical cutaneousinfiltrate/rule out MF (10), and chronic dermatitis (12). Finaldiagnoses in all cases were based on overall morphologicand immunophenotypic findings in bone marrow, blood, andtissue samples using criteria from the updated World Health
Organization classification.13
Cases with primary skininvolvement by a CD4+, epidermotropic T-cell tumor werediagnosed as MF or as Sézary leukemia if there was anerythrodermic rash and substantial peripheral blood involve-ment (tumor cells >500/µL). The diagnosis of “atypical cuta-neous lymphoid infiltrate” was used for cases with clinicalfeatures suggestive of MF and/or the presence of a clonal T-cell receptor rearrangement by molecular analysis but equiv-ocal histologic findings. At our institution during this period,we typically performed analysis of peripheral blood samplesfor all patients with systemic T-cell lymphoma and patientswith cutaneous findings suggestive of MF.
Three-color flow cytometric analysis was performed onsamples following a standard cell lysis method using mousemonoclonal antibodies directed against CD45 (peridin-chlorophyll-a-protein [PerCP]-conjugated), as well asvarious combinations of CD26 (fluorescein isothiocyanate[FITC]-conjugated, IgG2a clone L272), CD3 (FITC orphycoerythrin [PE]), CD4 (PE), CD5 (PE), CD7 (FITC),CD8 (FITC or PE), and CD19. All antibodies were fromBecton Dickinson, San Jose, CA, unless otherwise stated,and analysis was performed using FACScan or FACSCaliber
cytometers (Becton Dickinson). Ten control samples fromhealthy blood donors were used to establish the range of CD26 and CD7 expression in T-cell populations. In casesother than MF, additional antibodies (particularly CD56,CD57, and T-cell receptor-gamma/delta) were used in 4-color analysis to determine the final diagnosis. Negativestaining levels were set by comparison with an isotypecontrol antibody. Statistical analysis was performed using theFisher exact and the Student t tests and Pearson correlationcoefficient measures with Stats Direct Software (Camcode,Ashwell, England).
For all samples, analysis was limited to lymphocytes byusing a manual gating strategy based on forward/side scatterand side scatter/CD45-PerCP staining properties. Contami-nation of the lymphocyte gate by monocytes was assessed byCD45-PerCP/CD14-PE staining. The CD26 and CD7staining patterns were analyzed by eye using the CD4-PE/CD26-FITC, CD3-PE/CD26-FITC, CD4-PE/CD7-FITC,and CD3-PE/CD7-FITC dot-plot cytograms. For some cases,cluster analysis was performed using CellQuest and Paint-a-Gate software (Becton Dickinson). Criteria for an abnormalCD7 or CD26 tumor population included the presence of aCD4+ T-cell population that was clearly separable from thenormal spectrum of variably positive reactive lymphocytes.
Results
CD26 and CD7 Expression in Normal Peripheral BloodLymphocytes
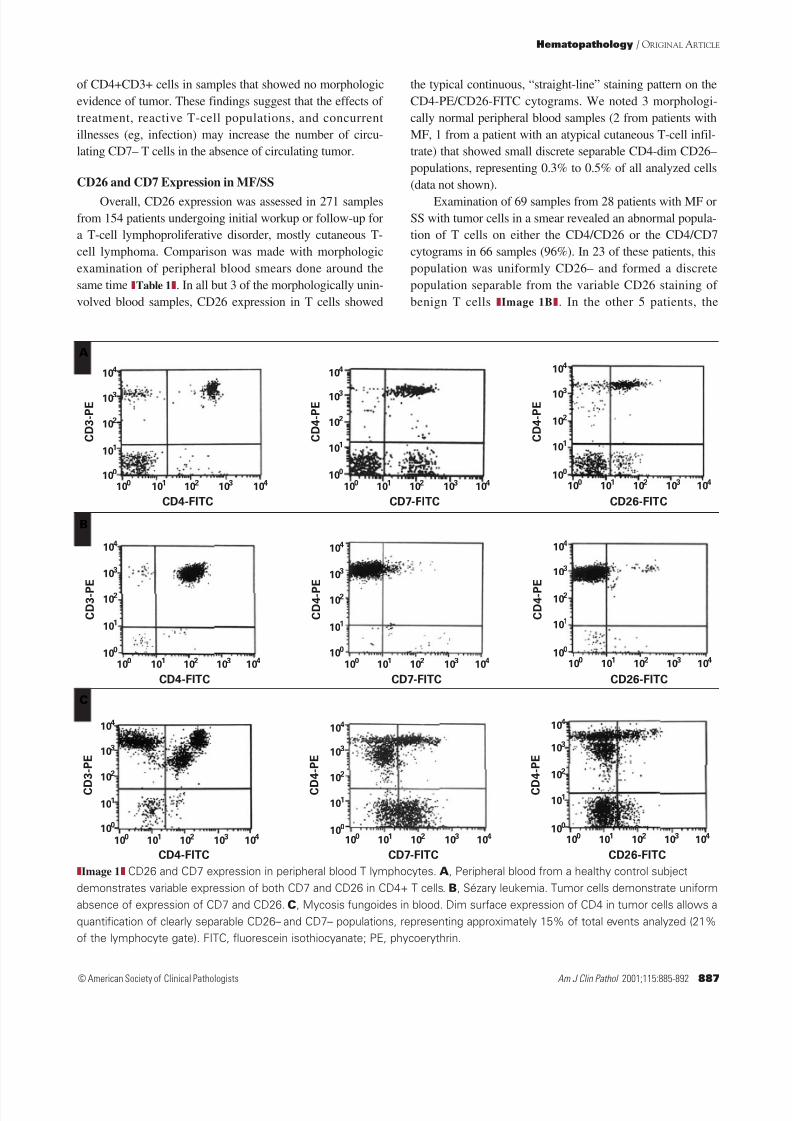
In peripheral blood from 10 healthy control subjects,there was a spectrum of CD26 expression in both CD4+ andCD8+ T cells Image 1A . As shown on the CD4/CD26cytograms, CD26 positivity ranged between 56% and 86%of the CD3+CD4+ T-cell population (mean ± SD, 77% ±8%). Normal CD8+ lymphocytes showed similar variablesurface CD26 expression, with a range of 24% to 80%showing positive staining (mean ± SD, 52% ± 13% [notshown]). CD3+CD56+ T cells also showed variable CD26expression (range, 25%-90%) but CD56+CD3– natural killercells were typically CD26– (up to 10% could be weaklypositive). Variation in the percentage of CD26+ peripheral
blood T cells in different samples likely was affected by thedegree of activation of the normal lymphocyte populations, acharacteristic feature of CD26 expression in mature T cells. 14
CD7 expression in nonneoplastic T cells was assessed in19 normal control samples and showed variable positivity of both CD4+ and CD8+ T cells (Image 1A). CD7 expressionwas seen in 73% to 97% of CD4+CD3+ T cells (mean ± SD,85% ± 6%) in the samples from healthy control subjects.CD7 expression was more variable on CD4+ T cells in studypatients than in control subjects, ranging from 61% to 89%
of CD4+CD3+ cells in samples that showed no morphologicevidence of tumor. These findings suggest that the effects of treatment, reactive T-cell populations, and concurrentillnesses (eg, infection) may increase the number of circu-lating CD7– T cells in the absence of circulating tumor.
CD26 and CD7 Expression in MF/SS
Overall, CD26 expression was assessed in 271 samplesfrom 154 patients undergoing initial workup or follow-up fora T-cell lymphoproliferative disorder, mostly cutaneous T-cell lymphoma. Comparison was made with morphologicexamination of peripheral blood smears done around thesame time Table 1 . In all but 3 of the morphologically unin-volved blood samples, CD26 expression in T cells showed
the typical continuous, “straight-line” staining pattern on theCD4-PE/CD26-FITC cytograms. We noted 3 morphologi-cally normal peripheral blood samples (2 from patients withMF, 1 from a patient with an atypical cutaneous T-cell infil-trate) that showed small discrete separable CD4-dim CD26–populations, representing 0.3% to 0.5% of all analyzed cells(data not shown).
Examination of 69 samples from 28 patients with MF orSS with tumor cells in a smear revealed an abnormal popula-tion of T cells on either the CD4/CD26 or the CD4/CD7cytograms in 66 samples (96%). In 23 of these patients, thispopulation was uniformly CD26– and formed a discretepopulation separable from the variable CD26 staining of benign T cells Image 1B . In the other 5 patients, the
Image 1 CD26 and CD7 expression in peripheral blood T lymphocytes. A , Peripheral blood from a healthy control subjectdemonstrates variable expression of both CD7 and CD26 in CD4+ T cells . B, Sézary leukemia. Tumor cells demonstrate uniformabsence of expression of CD7 and CD26. C , Mycosis fungoides in blood. Dim surface expression of CD4 in tumor cells allows aquantification of clearly separable CD26– and CD7– populations, representing approximately 15% of total events analyzed (21%of the lymphocyte gate). FITC, fluorescein isothiocyanate; PE, phycoerythrin.
abnormal population was weakly CD26+ but was separablefrom the normal T-cell population because of lower surfaceexpression of CD4. Only 3 morphologically atypical bloodsamples (all from patients in the patch/plaque stage of MF)did not show a discrete abnormal population on theCD4/CD26 (or CD3/CD26) cytograms. Two samples wereinvolved minimally, showing 1% and 3% identifiable tumorcells, respectively, on manual differential counts of thesmear. The remaining smear had rare lymphocytes (<0.1% of cells) suggestive of Sézary cells. Comparing MF/SS,dermatitis, and atypical cutaneous lymphoid lesions, therewas a strong association between the identification of a sepa-
rable CD26–/dim population and identifiable tumor cells onthe peripheral smear ( P < .0001).
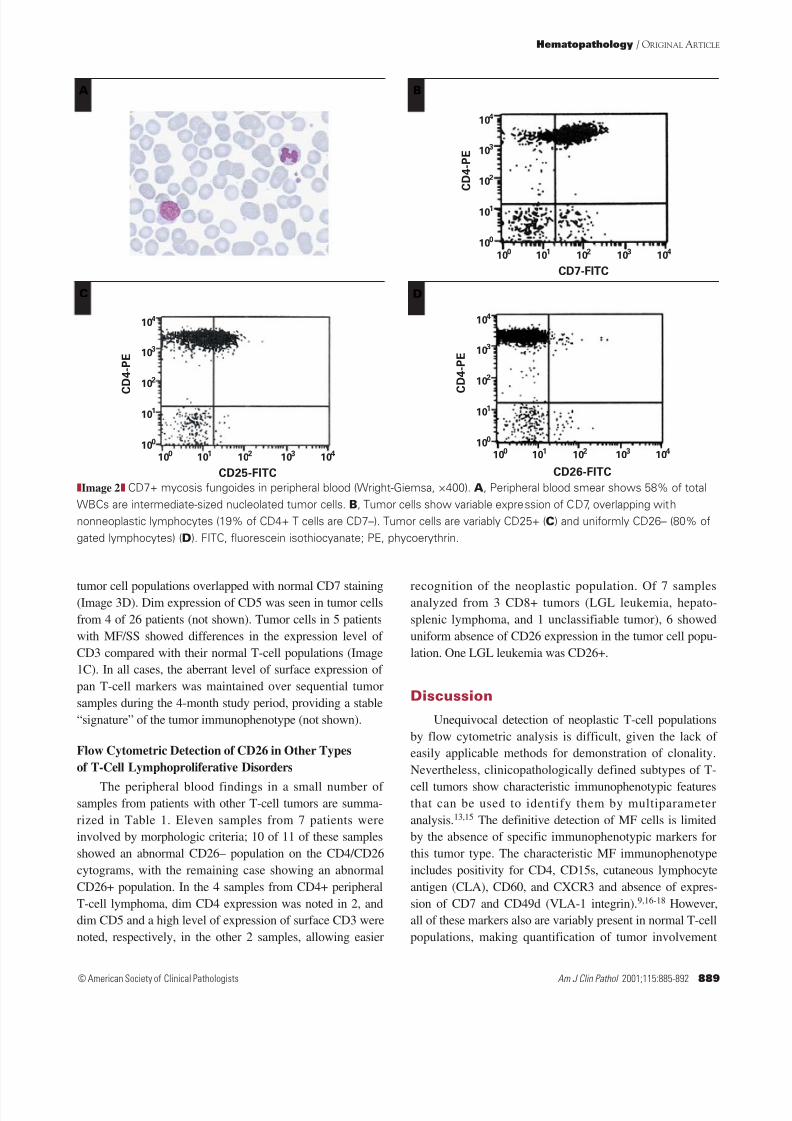
In contrast, CD7 was expressed more variably onMF/SS tumor cells. Overall, 34 (49%) of 69 involved bloodsamples from 28 patients with MF/SS had a separable,quantifiable abnormal T-cell population identified by exami-nation of the CD4/CD7 cytograms Image 1C . In theremaining cases, it was not possible to separate theabnormal population from the nonneoplastic lymphocytesbecause of variability in CD7 staining Image 2 . The exis-tence of an abnormal (neoplastic) population in these casesusually could be inferred (but not quantified) by relative
increases in the number of CD7– T cells. CD4/CD26 dualstaining allowed separation of the abnormal T-cell popula-tion in all of these cases. There was a single sample inwhich an abnormal population detected by examination of CD4/CD7 cytograms was not clearly seen by CD4/CD26staining. Overall, 10 of 28 patients with MF/SS showedabnormal (tumor) T-cell populations that were variably oruniformly CD7+. In 3 patients, there were variations in theexpression of CD7 in the presumed tumor cells betweensamples obtained on different dates.
Serial analyses of peripheral blood samples frompatients with MF/SS undergoing treatment showed variationsin the numbers of tumor cells counted on smears that paral-leled variations in the size of the abnormal populationdetected by CD4/CD26 surface staining. Especially intumors undergoing therapy, morphologic counts tended tounderestimate the percentages of tumor cells presentcompared with the flow cytometric detection. However, largechanges in the number of the abnormal CD26–/dim T-cellpopulations detected by the flow cytometric method wereparalleled by the findings on the smears. Thus, the CD26–population likely represents the neoplastic population in
MF/SS.
Expression of Other T-Cell Markers in MF/SS
Other flow cytometric features seen in involved samplesfrom patients with MF/SS are summarized in Table 1.Analysis of the CD3+ T-cell population revealed a CD4/CD8ratio greater than 5 in at least 1 sample from 23 of 28patients with MF/SS but in only 3 of 139 uninvolved samples(P < .0001). This ratio was elevated more frequently inuntreated patients and was less often elevated in patients withMF/SS undergoing systemic therapy. It therefore was lessuseful for detecting low-level lymphomatous involvement.
Lower level expression of CD4 (compared with the levelon nonneoplastic T cells) was seen on tumor cells from 14 of 28 patients (Image 1C). Tumor cells in 3 cases showedcomplete absence of CD4 on some tumor cells. In 2 of thecases, correlation of the results of skin biopsy findings withcluster analysis of the peripheral blood flow cytometric datarevealed that this absence of CD4 was associated with thetransformed large cell population within the tumor Image 3
(other data not shown). CD7 staining in these cases wasconfusing to interpret since variable staining of different
MF, mycosis fungoides; PB, peripheral blood; PTCL, peripheral T-cell lymphoma; SS, Sézary syndrome,* Data are given as number with finding/total (percentage) unless otherwise indicated.† Antigen loss detected in only a subset of the tumor cell population.‡ Abnormal population represented 1% of all analyzed cells.
8/14/2019 Absence of CD26 Expression is a Useful Marker for T-Cell Lymphoma in PB
tumor cell populations overlapped with normal CD7 staining(Image 3D). Dim expression of CD5 was seen in tumor cellsfrom 4 of 26 patients (not shown). Tumor cells in 5 patientswith MF/SS showed differences in the expression level of CD3 compared with their normal T-cell populations (Image1C). In all cases, the aberrant level of surface expression of pan T-cell markers was maintained over sequential tumorsamples during the 4-month study period, providing a stable“signature” of the tumor immunophenotype (not shown).
Flow Cytometric Detection of CD26 in Other Typesof T-Cell Lymphoproliferative Disorders
The peripheral blood findings in a small number of samples from patients with other T-cell tumors are summa-rized in Table 1. Eleven samples from 7 patients wereinvolved by morphologic criteria; 10 of 11 of these samplesshowed an abnormal CD26– population on the CD4/CD26cytograms, with the remaining case showing an abnormalCD26+ population. In the 4 samples from CD4+ peripheralT-cell lymphoma, dim CD4 expression was noted in 2, anddim CD5 and a high level of expression of surface CD3 werenoted, respectively, in the other 2 samples, allowing easier
recognition of the neoplastic population. Of 7 samplesanalyzed from 3 CD8+ tumors (LGL leukemia, hepato-splenic lymphoma, and 1 unclassifiable tumor), 6 showeduniform absence of CD26 expression in the tumor cell popu-lation. One LGL leukemia was CD26+.
Discussion
Unequivocal detection of neoplastic T-cell populationsby flow cytometric analysis is difficult, given the lack of easily applicable methods for demonstration of clonality.Nevertheless, clinicopathologically defined subtypes of T-
cell tumors show characteristic immunophenotypic featuresthat can be used to identify them by multiparameteranalysis. 13,15 The definitive detection of MF cells is limitedby the absence of specific immunophenotypic markers forthis tumor type. The characteristic MF immunophenotypeincludes positivity for CD4, CD15s, cutaneous lymphocyteantigen (CLA), CD60, and CXCR3 and absence of expres-sion of CD7 and CD49d (VLA-1 integrin). 9,16-18 However,all of these markers also are variably present in normal T-cellpopulations, making quantification of tumor involvement
Image 2 CD7+ mycosis fungoides in peripheral blood (Wright-Giemsa, ×400). A , Peripheral blood smear shows 58% of totalWBCs are intermediate-sized nucleolated tumor cells. B, Tumor cells show variable expression of CD7, overlapping withnonneoplastic lymphocytes (19% of CD4+ T cells are CD7–). Tumor cells are variably CD25+ ( C ) and uniformly CD26– (80% ofgated lymphocytes) ( D ). FITC, fluorescein isothiocyanate; PE, phycoerythrin.
8/14/2019 Absence of CD26 Expression is a Useful Marker for T-Cell Lymphoma in PB
difficult. We showed that absence of expression of CD26also is highly characteristic of MF/SS tumor cells and that anabnormal CD26– population correlates with the presence of
morphologically identifiable tumor cells in the peripheralblood (96% sensitivity, 98% specificity).
The best-studied MF-associated marker is CLA, anadhesion molecule that mediates the cutaneous localizationof skin-homing lymphocytes. 19 CLA is expressed in mostskin-homing T cells and almost all MF tumor cells withinskin, as well as in a small subset of circulating benignlymphocytes, especially in patients with chronicdermatitis. 20-23 However, MF/cutaneous T-cell lymphoma(CTCL) tumor cells tend to shed CLA expression outside the
skin microenvironment, and there is not a good correlationbetween the number of CLA-positive cells in the blood andthe number of Sézary cells counted or the degree of lymph
node involvement in MF. 10 Molecular analysis of sorted cellpopulations has demonstrated that circulating MF tumorcells are present in both the CLA-positive and the CLA-negative populations. This result is supported by the labilityof CLA expression noted on T cells in culture. 24 Thus, CLAis unlikely to be a highly sensitive antigen for detection of circulating MF cells.
The most commonly used method for detection of cuta-neous lymphoma circulating in peripheral blood is theabsence of CD7 expression on CD4+ T cells. In normal T
Image 3 Mycosis fungoides with dim or absent surface CD4 expression. A , Skin biopsy specimen demonstrates a superficialdermal infiltrate of large neoplastic cells (H&E, ×200), which are mostly CD4– by cryostat section immunohistochemistry (inset,×1,000). B, Peripheral blood smear reveals that 62% of the lymphocytes are enlarged with prominent nucleoli and irregularnuclear contours (Wright-Giemsa, ×1,000). C , Flow cytometric analysis of peripheral blood demonstrates 73% of the gated
lymphocytes are CD3+ T cells, highlighted in color on the scattergram (other cells are shaded in gray). D , CD3/CD7 cytogramshows variable CD7 expression, mimicking the typical distribution in normal T cells. E , CD4/CD3 cytogram demonstrates 2abnormal populations, CD4 dim (green) and CD4– (red) and a normal CD4+ population (blue). The CD4– population has a largercell size on the scattergram, consistent with tumor cells. F, CD4/CD26 cytogram shows complete absence of CD26 expressionin both abnormal (tumor) populations with variable CD26 expression in normal T cells (blue). In panels not shown, CD19+ B cellsrepresented 25% of gated lymphocytes; CD56+ natural killer cells and CD8+ T cells each made up 0.5% of the lymphoid gate.FITC, fluorescein isothiocyanate; FSC, forward scatter; PE, phycoerythrin; PerCP, peridin-chlorophyll-a-protein; SSC, side scatter.
8/14/2019 Absence of CD26 Expression is a Useful Marker for T-Cell Lymphoma in PB
cells, CD7 is low or absent in most skin-homing lympho-cytes and in a variable number of circulating T cells. 8,11,25 Ithas been reported that the size of the CD7– T-cell populationcorrelates with the extent of disease in MF/CTCL. 4,10
However, as described, approximately 50% of MF/CTCLcases show variable CD7 expression, making tumor cellsdifficult to distinguish from normal and nonneoplastic reac-tive T-cell populations. 7-9,26 We found that unless the MFtumor cells show lower surface expression of CD4 (or CD3or CD5), it is difficult to separate them definitively fromnormal T cells by cluster analysis with CD7 staining. Incontrast, the reproducible low or negative expression of CD26 in MF usually creates a separable discrete cluster of tumor cells that can be recognized.
CD26 (also known as dipeptidyl peptidase IV) is awidely expressed cell surface proteolytic enzyme related tocellular activation that is expressed in the majority of circu-lating T cells. 27 As shown herein, CD26 is expressed vari-ably in most CD4+ circulating T cells, and it is expressed athighest levels on the activated memory-helper T-cell subset,but also is expressed at varying levels in CD8+ and immatureT-cell populations. 12,28 Absence of CD26 expression hasbeen reported in small numbers of other T-cell tumor types,including adult T-cell leukemia/lymphoma and MF inskin. 9,29-31 Whether CD26 will prove useful for the detectionof T-cell tumor cells other than MF/SS requires further study.In a small number of cases, we noted absence of CD26expression in blood involvement in 5 patients with peripheralT-cell lymphoma and 3 patients with CD8+ tumors. Previ-ously, small studies have demonstrated that CD26 expression
is associated with certain tumor types—anaplastic large celllymphoma, precursor T-lymphoblastic lymphoma, andhepatosplenic lymphoma—that we did not study. 31,32 Ourstudy supports the use of CD26, in place of or in addition toCD7, as part of the routine panel for flow cytometric detec-tion of neoplastic T cells in MF/SS.
From the 1 Division of Pathology and Laboratory Medicine and the Departments of 2 Lymphoma and 3 Dermatology, the Universityof Texas–M.D. Anderson Cancer Center, Houston.
Address reprint requests to Dr Jones: Dept of Hemato- pathology, Box 72, 1515 Holcombe Blvd, Houston TX 77030.
Acknowledgments: We thank Louise Huck, Linda Powers,and the entire staff of the M.D. Anderson Cancer Center
Immunology and Flow Cytometry Laboratory for their assistancein this work. We thank John T. Manning, MD, for critical reviewof the manuscript.
References1. Bakels V, van Oostveen JW, Gordijn RL, et al. Frequency and
prognostic significance of clonal T-cell receptor beta–generearrangements in the peripheral blood of patients withmycosis fungoides. Arch Dermatol. 1992;128:1602-1607.
2. Fraser-Andrews EA, Woolford AJ, Russell-Jones R, et al.Detection of a peripheral blood t cell clone is an independentprognostic marker in mycosis fungoides. J Invest Dermatol.2000;114:117-121.
3. Dommann SN, Dommann-Scherrer CC, Dours-ZimmermannMT, et al. Clonal disease in extracutaneous compartments incutaneous T-cell lymphomas: a comparative study betweencutaneous T-cell lymphomas and pseudo lymphomas. ArchDermatol Res. 1996;288:163-167.
4. Laetsch B, Haffner AC, Dobbeling U, et al. CD4+/CD7– Tcell frequency and polymerase chain reaction–based clonalityassay correlate with stage in cutaneous T cell lymphomas.
J Invest Dermatol. 2000;114:107-111.5. Muche JM, Lukowsky A, Asadullah K, et al. Demonstration
of frequent occurrence of clonal T cells in the peripheralblood of patients with primary cutaneous T-cell lymphoma.Blood. 1997;90:1636-1642.
6. Muche JM, Lukowsky A, Heim J, et al. Demonstration of frequent occurrence of clonal T cells in the peripheral bloodbut not in the skin of patients with small plaque parapsoriasis.Blood. 1999;94:1409-1417.
7. Bogen SA, Pelley D, Charif M, et al. Immunophenotypicidentification of Sézary cells in peripheral blood. Am J Clin
Pathol. 1996;106:739-748.8. Harmon CB, Witzig TE, Katzmann JA, et al. Detection of
circulating T cells with CD4+CD7– immunophenotype inpatients with benign and malignant lymphoproliferativedermatoses. J Am Acad Dermatol. 1996;35:404-410.
9. Scala E, Russo G, Cadoni S, et al. Skewed expression of activation, differentiation and homing-related antigens incirculating cells from patients with cutaneous T celllymphoma associated with CD7– T helper lymphocytesexpansion. J Invest Dermatol. 1999;113:622-627.
10. Borowitz MJ, Weidner A, Olsen EA, et al. Abnormalities of circulating T-cell subpopulations in patients with cutaneousT-cell lymphoma: cutaneous lymphocyte-associated antigenexpression on T cells correlates with extent of disease.Leukemia. 1993;7:859-863.
11. Moll M, Reinhold U, Kukel S, et al. CD7-negative helper Tcells accumulate in inflammatory skin lesions. J InvestDermatol. 1994;102:328-332.
12. Dang NH, Torimoto Y, Shimamura K, et al. 1F7 (CD26): amarker of thymic maturation involved in the differentialregulation of the CD3 and CD2 pathways of humanthymocyte activation. J Immunol. 1991;147:2825-2832.
13. Harris NL, Jaffe ES, Diebold J, et al. World HealthOrganization classification of neoplastic diseases of thehematopoietic and lymphoid tissues: report of the ClinicalAdvisory Committee meeting, Airlie House, Virginia,
November 1997. J Clin Oncol. 1999;17:3835-3849.14. Dang NH, Torimoto Y, Sugita K, et al. Cell surface
modulation of CD26 by anti-1F7 monoclonal antibody:analysis of surface expression and human T cell activation.
J Immunol. 1990;145:3963-3971.15. Jones D, O’Hara C, Kraus M, et al. Expression pattern of T-
cell–associated chemokine receptors and their chemokinescorrelates with specific subtypes of T-cell non-Hodgkinlymphoma. Blood. 2000;96:685-690.
16. Bank I, Rapman E, Shapiro R, et al. The epidermotropicmycosis fungoides associated alpha1beta1 integrin (VLA-1,CD49a/CD29) is primarily a collagen IV receptor onmalignant T cells. J Cutan Pathol. 1999;26:65-71.
17. Lu D, Duvic M, Medeiros LJ, et al. The T-cell chemokinereceptor CXCR3 is expressed highly in low-grade mycosisfungoides. Am J Clin Pathol. 2001;115:413-421.
18. Kamarashev J, Burg G, Kempf W, et al. Comparative analysisof histological and immunohistological features in mycosisfungoides and Sézary syndrome. J Cutan Pathol. 1998;25:407-412.
19. Fuhlbrigge RC, Kieffer JD, Armerding D, et al. Cutaneouslymphocyte antigen is a specialized form of PSGL-1 expressedon skin-homing T cells. Nature. 1997;389:978-981.
20. Picker LJ, Michie SA, Rott LS, et al. A unique phenotype of
skin-associated lymphocytes in humans: preferentialexpression of the HECA-452 epitope by benign andmalignant T cells at cutaneous sites. Am J Pathol.1990;136:1053-1068.
21. Dworzak MN, Froschl G, Printz D, et al. Skin-associatedlymphocytes in the peripheral blood of patients with atopicdermatitis: signs of subset expansion and stimulation. J AllergyClin Immunol. 1999;103:901-906.
22. Jones D, Benjamin RJ, Shahsafaei A, et al. The chemokinereceptor CXCR3 is expressed in a subset of B-cell lymphomasand is a marker of B-cell chronic lymphocytic leukemia.Blood. 2000;95:627-632.
23. Santamaria Babi LF, Picker LJ, Perez Soler MT, et al.Circulating allergen-reactive T cells from patients with atopicdermatitis and allergic contact dermatitis express the skin-selective homing receptor, the cutaneous lymphocyte-associated antigen. J Exp Med. 1995;181:1935-1940.
24. Armerding D, Kupper TS. Functional cutaneous lymphocyteantigen can be induced in essentially all peripheral blood Tlymphocytes. Int Arch Allergy Immunol. 1999;119:212-222.
25. Reinhold U, Pawelec G, Fratila A, et al. Phenotypic andfunctional characterization of tumor infiltrating lymphocytesin mycosis fungoides: continuous growth of CD4+ CD45R+T- cell clones with suppressor-inducer activity. J InvestDermatol. 1990;94:304-309.
26. Schiavon V, Roth P, Bolton WE, et al. Lymphocytes subsets innormal individuals: analysis by four color immunofluorescenceand flow cytometry on whole blood. Tissue Antigens.1996;48(4 pt 1):312-318.
27. Buhling F, Kunz D, Reinhold D, et al. Expression andfunctional role of dipeptidyl peptidase IV (CD26) on humannatural killer cells. Nat Immun. 1994;13:270-279.
28. Ruiz P, Zacharievich N, Shenkin M. Multicolor cytoenzymatic
evaluation of dipeptidyl peptidase IV (CD26) function innormal and neoplastic human T-lymphocyte populations. ClinDiagn Lab Immunol. 1998;5:362-368.
29. Ruiz P, Mailhot S, Delgado P, et al. CD26 expression anddipeptidyl peptidase IV activity in an aggressive hepatosplenicT-cell lymphoma. Cytometry. 1998;34:30-35.
30. Kondo S, Kotani T, Tamura K, et al. Expression of CD26/dipeptidyl peptidase IV in adult T cell leukemia/lymphoma(ATLL). Leuk Res. 1996;20:357-363.
31. Carbone A, Cozzi M, Gloghini A, et al. CD26/dipeptidylpeptidase IV expression in human lymphomas is restricted toCD30-positive anaplastic large cell and a subset of T-cell non-Hodgkin’s lymphomas. Hum Pathol. 1994;25:1360-1365.
32. Klobusicka M, Babusikova O. CD26 and DPP IV expressionin T acute lymphoblastic leukemia cells: immunocyto-chemistry and enzyme cytochemistry. Gen Physiol Biophys.1999;18(suppl 1):34-37.