Page 1
Abstract
DOES MINIMALLY INVASIVE ROBOTIC SURGICAL TREATMENT ALTER
EXERCISE TOLERANCE IN PATIENTS WITH ATRIAL FIBRILLATION AND
MITRAL REGURGITATION AT SEVEN TO ELEVEN WEEKS POST-OPERATIVE?
by Leena Jayesh Patel
July, 2009
Director: Timothy P. Gavin, Ph.D
Department of Exercise and Sport Science
In the current study, we examined if exercise tolerance was going to be reduced in atrial
fibrillation and mitral valve regurgitation patients post a minimally invasive surgery
seven to eleven weeks when compared to pre-operative. Patients that participated in this
study were diagnosed with atrial fibrillation or mitral valve regurgitation and were
previously scheduled for minimally invasive corrective surgery. Subjects were
maximally stress tested over two visits, before and after surgery. Oxygen consumption,
maximal heart rate, and maximal treadmill time were measured. They also filled out a
Physical Activity Scale for the Elderly (PASE) before and after surgery to determine their
activity levels. A paired t-test with significance level set at P ≤ 0.05 revealed that
exercise tolerance and activity levels were not found to be significantly different.
Subjects in this study were found to be asymptomatic, had mild-moderate atrial
fibrillation or mitral valve regurgitation, were younger than previously studied subjects
and were active in their daily activities up until the day of their surgery. The principle
findings of this study are: 1) patients did not have reduced exercise tolerance after
Page 2
surgery when compared to pre-operative, 2) when compared to age predicted data,
VO2MAX was not significantly different before or after surgery, and 3) there was no
change in activity levels between pre and post surgery.
Page 3
©Copyright 2009
Leena Jayesh Patel
Page 5
DOES MINIMALLY INVASIVE ROBOTIC SURGICAL TREATMENT ALTER EXERCISE TOLERANCE IN PATIENTS
WITH ATRIAL FIBRILLATION AND MITRAL REGURGITATION AT SEVEN TO ELEVEN WEEKS POST-OPERATIVE?
A Thesis
Presented to
The Faculty of the Department of Exercise and Sports Science
East Carolina University
In Partial Fulfillment of the
Requirements for the Degree of
Masters of Science in Exercise Physiology
Presented by
Leena Jayesh Patel
June 2009
Page 6
DOES MINIMALLY INVASIVE ROBOTIC SURGICAL TREATMENT ALTER EXERCISE TOLERANCE IN PATIENTS WITH ATRIAL FIBRILLATION AND
MITRAL REGURGITATION AT SEVEN TO ELEVEN WEEKS POST-OPERATIVE?
by
Leena Jayesh Patel
APPROVED BY:
DIRECTOR OF THESIS:___________________________________________________ (Dr. Timothy P. Gavin)
COMMITTEE MEMBER:__________________________________________________
(Dr. Katrina DuBose)
COMMITTEE MEMBER:__________________________________________________ (Dr. Kristina Karvinen)
COMMITTEE MEMBER:__________________________________________________
(Dr. Evelio Rodriguiz)
CHAIR OF THE DEPARTMENT OF HEALTH & HUMAN PERFORMANCE:
________________________________________________
(Dr. Stacey Altman)
DEAN OF THE GRADUATE SCHOOL:
________________________________________________ (Dr. Paul J. Gemperline)
Page 7
DEDICATION
This thesis is dedicated to my parents and my brother, for their unconditional love
and support in all my endeavors. I would not be where I am without their guidance.
Page 8
ACKNOWLEDGEMENTS
I would like to thank Dr. Gavin for his hard work, dedication, and patience with
me while I completed this thesis. In addition I would like to thank my committee
members: Dr. Karvinen, Dr. DuBose, and Dr. Rodriguez. I would also like to thank Jenn
McCartney, Jessica Van-Meter, Kandy Houmard, Gabe Dubis, Dr. Hickner, Julie Cox
and Wendy Beachum for their help. Finally I thank Dr. Stevens and Dr. Lehr for their
assistance in the testing.
Page 9
TABLE OF CONTENTS
LIST OF TABLES………………………………………………….…………………….vi
LIST OF FIGURES…………………………………..…………….……………………vii
CHAPTER I: INTRODUCTION………………………………………………….……...1
Problem Statement………………………………………………………………...2
Research Hypothesis………………………………………………………………2
Delimitations……………………………………………………………………....2
Limitations……………………………………………………………………...…2
Definition of Terms…………………………………………………………….….3
List of Acronyms………………………………………………………………….3
CHAPTER II: LITERATURE REVIEW……...…………………………………………4
Normal Function of the Heart……………………………………………………..4
Arrhythmias…………………………………………………………………….....5
Atrial Fibrillation……………………………………………………………….....6
Mitral Valve Regurgitation…………………………………………………...….11
Exercise Capacity and Exercise Tolerance………………………………………15
Surgical Treatment……………………………………………………………….17
Exercise Tolerance after Surgery………………………………………………...21
Conclusion……………………………………………………………………….23
CHAPTER III: METHODS………..……………………………………………………25
Subjects…………………………………………………………………………..25
Testing Protocol………………………………………………………………….25
Statistical Analysis……………………………………………………………….27
CHAPTER IV: RESULTS………………………………………………………………29
Page 10
Subject Characteristics…………………………………………………………...29
Exercise Tolerance……………………………………………………………….29
CHAPTER V: DISCUSSION………………………………………………………..….35
Findings………………………………………………………………………….35
Subject Characteristics…………………………………………………………...35
Effects of AF and MR on Exercise Tolerance…………………………………...37
Effect of Minimally Invasive Sugery on Exercise Tolerance……………………38
Limitations……………………………………………………………………….39
Future Projects…………………………………………………………………...39
Conclusions………………………………………………………………………40
References…………………………………………………………………………….….41
APPENDIX A: UMCIRB APPROVAL
APPENDIX B: INFORMED CONSENT
APPENDIX C: ACTIVITY QUESTIONNAIRE
APPENDIX D: TESTING PROTOCOLS
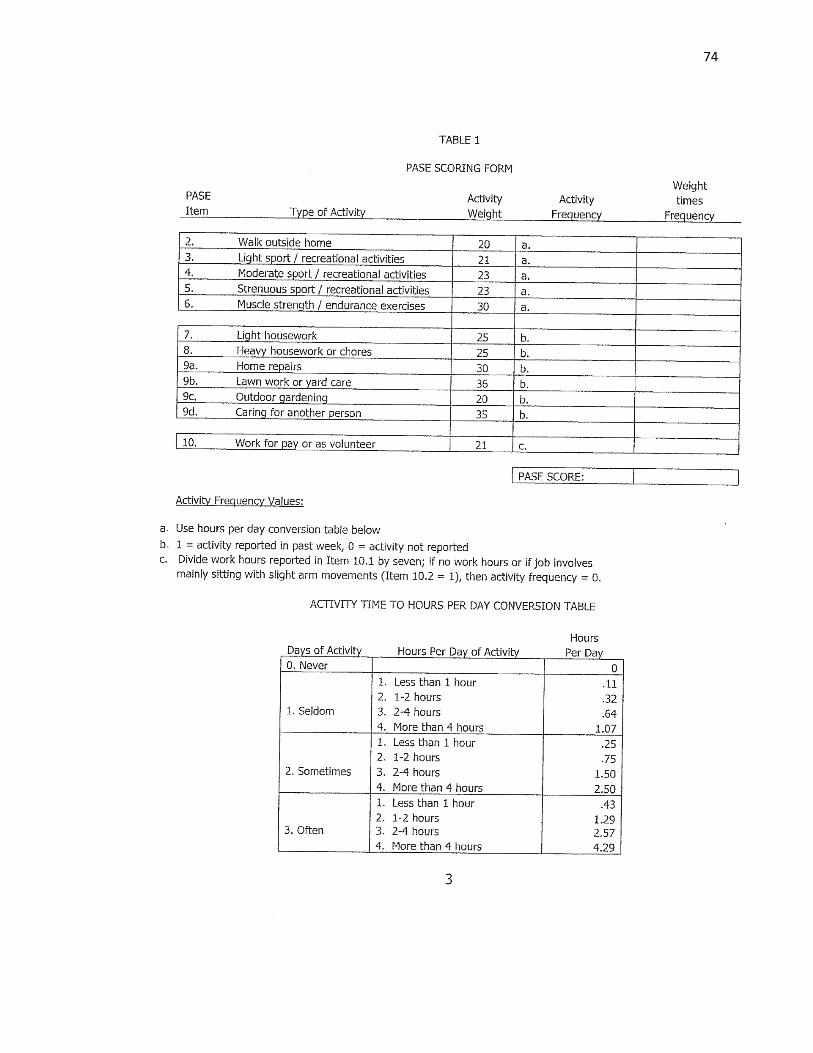
APPENDIX E: PASE SCORING FORM
Page 11
LIST OF TABLES
1. Modified Naughton Treadmill Protocol………………………………………….26
2. NYHA Classification…………………………………………………………….28
3. Individual Data Pre and Post surgery…………………………………………….29
4. Demographic and Exercise Data…………………………………………………30
Page 12
LIST OF FIGURES
1. Relative VO2max pre and post-operation compared to age predicted data………..31
2. Relative VO2max pre and post-operation compared to ACSM data………………32
Page 13
CHAPTER I
INTRODUCTION
The heart is one of the most important organs in the body. Proper functioning of
the circulatory system ensures a high quality of life. When there are problems associated
with the heart and its components, everyday activities become strenuous. Atrial
fibrillation (AF) and mitral valve regurgitation (MR) are two major types of dysfunctions
that can severely lower an individual’s quality of life.
The prevalence of AF will increase as the elderly proportion of the population
increases. It has been projected that the number of Americans with AF will increase to
more than 5.6 million during the next 50 years (Go, Hylek et al., 2001). A more recent
analysis has projected the number of adults with AF for the year 2050 to be 15.9 million,
if a continuous rise in the incidence of AF persists (Miyasaka, Barnes et al., 2006). As
individuals age, the heart begins to lose function and efficiency. When AF and MR are
present concurrently, there is a significant decrease in an individual’s quality of life,
functional status, and cardiac performance, as well as higher medical costs and a higher
risk of death (Go, Hylek et al., 2001). In many cases of AF and MR, surgical treatment is
the only remaining option. Robotically-assisted minimally invasive surgery can correct
AF and MR returning the heart to sinus rhythm and cardiac unidirectional blood flow.
Individuals in sinus rhythm have a higher quality of life and higher exercise tolerance
than AF and MR patients.
The purpose of this study was to investigate if exercise tolerance was returned to
pre-surgical capacity at 7-11 weeks post-robotic surgery to treat AF, MR and AF + MR.
Page 14
2
Problem Statement
Currently it is not known if exercise tolerance can be restored in asymptomatic
patients 7-11 weeks post robotic surgery.
Hypothesis
It was hypothesized that exercise tolerance would be reduced at 7-11 weeks post-
robotic surgery compared to pre-surgery in AF, MR and AF + MR patients.
Delimitations:
1) All subjects were men.
2) Sample size of 4 subjects.
3) Patients were not involved in a structured exercise program or participated in 30
minutes of vigorous exercise per week in the last 2 months.
4) All subjects were free of known pulmonary disease or any disease that would
result in worsened exercise capacity independent of their cardiac disease.
5) Atrial fibrillation and mitral valve regurgitation were diagnosed by physician.
6) Patients were scheduled for AF or MR surgery.
Limitations:
1) Subjects may complete questionnaires, including the PASE and Modified Baeke,
in a misleading or inaccurate manner.
2) Failure of maximal effort during VO2MAX testing could lead to underestimation of
exercise capacity workload and oxygen consumption.
Page 15
3
Definition of Terms
Exercise Capacity: The maximum ability of the body to take up and use oxygen to do
work
Maximal Oxygen Consumption (VO2MAX): quantitatively expresses an individual’s
capacity for aerobic energy production
List of Acronyms
AF: Atrial Fibrillation
MV: Mitral Valve
MVR: Mitral Valve Regurgitation
MR: Mitral Regurgitation
BMI: Body Mass Index = body mass (kg) divided by height squared (kg/m2)
PASE: Physical Activity Scale for the Elderly
NYHA: New York Heart Association
ECG: Electrocardiogram
HR: Heart Rate
BPM: beats per minute
TM: Treadmill
Page 16
CHAPTER II
REVIEW OF LITERATURE
Normal Function of the Heart
The primary function of the heart is to supply blood and nutrients. In order for
that to occur, a normal heart usually has a constant rhythm which beats between 60 to
100 times a minute. Athletes or highly trained individuals can have a resting rhythm as
low as 40 beats per minute (bpm). During each beat, or contraction, the heart expels
blood into the aorta. Each contraction is controlled by an electrical impulse traveling
through the heart. In the normal heart, these impulses occur at constant and regular
intervals. The rhythm of the heart is normally determined by a natural pacemaker called
the sinoatrial (SA) node, which is located in the posterior wall of the right atrium near the
superior vena cava. The SA node spontaneously generates action potentials at rates of
60-100 beats/minute (bpm). This intrinsic rhythm is influenced by the autonomic nerves,
with sympathetic stimulation accelerating the sinus node rate of depolarization and vagal
stimulation slowing it (Malcolm S. Thaler, 2007).
Sinus rhythm normally controls both the atrial and ventricular rhythm. Action
potentials generated by the SA node spread through the atria, depolarizing this tissue and
in turn cause atrial contraction. The impulse then travels into the ventricles via the
atrioventricular node (AV node). The purpose of the AV node is to provide a pathway
for impulses from the atria to the ventricles (Malcolm S. Thaler, 2007). There is a slight
delay in conduction from the atria to ventricles, which allows the atria to contract first
and the ventricles to fill with blood before the ventricles contract. The impulse is then
Page 17
5
picked up by specialized conduction pathways, bundle branches and Purkinje fibers, to
rapidly conduct the wave of depolarization through the ventricles to produce a ventricular
contraction. Therefore, in a normal heart, the rhythm is controlled by the SA node.
The heart consists of 4 chambers, right atrium, right ventricle, left atrium, and left
ventricle. The atriums are connected to the ventricles by valves. Between the right
atrium and right ventricle is the tricuspid valve and between the left atria and left
ventricle is the mitral valve. The right atrium collects de-oxygenated blood from the
body (via the superior and inferior vena cava), pumps it through to the right ventricle via
the tricuspid valve, and then pumps it through the pulmonary valve into the lungs.
Oxygenated blood from the lungs then returns to the left atrium, pumps through the
mitral valve into the left ventricle. Blood is then pumped to the rest of the body via the
aortic valve. The muscle wall surrounding the left ventricle is thicker compared to the
right ventricle due to the higher force needed to pump blood through the systemic
circulation.
Arrhythmias
Variations in the heart rhythm are known as arrhythmias. There are many types
of arrhythmias and they are classified according to where they originate in the heart.
Those that do not originate from the ventricles are generally called supraventricular
arrhythmias while those originating from the ventricles are called ventricular arrhythmias
(Malcolm S. Thaler, 2007). Some general arrhythmias include supraventricular
tachycardia, atrial flutter, ventricular tachycardia, and atrial fibrillation. However, these
are not the only arrhythmias, just the most common ones.
Page 18
6
Supraventricular tachycardia occurs when the atria or the AV node produces a
regular but rapid discharge. The heart has a rate of over 100bpm (usually around 130-
150bpm). Atrial flutter is generated by a reentrant circuit that runs largely around the
annulus, the ring-like structure on a heart valve where the valve leaflets are anchored, of
the tricuspid valve. Atrial depolarization occurs at such a rapid rate that discrete P waves
separated by a flat baseline are not observed (Malcolm S. Thaler, 2007). Because the
baseline continuously rises and falls, the effect produces a type of flutter wave. The rate
is usually fast (250-350 bpm) and irregular. Ventricular tachycardia occurs when fast and
regular impulses come from the ventricle and cause a very rapid heart rate. This
arrhythmia can be life-threatening and requires immediate medical attention. Lastly,
atrial fibrillation (AF), one of the most common chronic conditions (Benjamin, Wolf et
al., 1998), is caused by electrical impulses discharged at a rapid rate from many different
areas of the atria. Unlike atrial flutter, where there is a single constant signal responsible
for the flutter waves, in AF multiple reentrant circuits are unpredictably occurring
(Malcolm S. Thaler, 2007). In an ECG strip, no true P wave can be identified. This
arrhythmia also causes fast and irregular heartbeats (usually between 120-180bpm).
Atrial Fibrillation
Based on research conducted in 1995, an estimated 2.23 million Americans have
AF, with a median age of 75 years (Feinberg, Blackshear et al., 1995). The prevalence
appears to double with each decade, from 0.5% in the population aged 50-59 years to
almost 9% between ages 80-89 years, with prevalence being slightly higher in men than
women (Conway, 2002) due to the decreased amount of estrogen found in men. It has
Page 19
7
been noted that men are 50% more likely than women to develop AF (Kannel, Wolf et
al., 1998). The incidence of AF increases with advancing age, with an annual incidence
per 1000 person-years of about 3.1 cases in men and 1.9 cases in women 55 to 64 years;
also rising to 38.0 and 31.4 cases in men and women 85 to 94 years of age (Benjamin,
Levy et al., 1994).
Basic features of AF are great rapidity of atrial depolarization, irregularity of
atrial depolarization, and absence of regular atrial activity on the surface ECG (Gallagher
and Camm, 1998). Instead of one steady impulse, many impulses begin and spread
through the atria to compete for a chance to travel to the AV node. This causes a rapid
and disorganized heartbeat. Impulses in the atria can range from 300-600 bpm. The AV
node then tries to limit the number of impulses that travel to the ventricles. Even before
the ventricle has a chance to contract, another impulse may be sent. Irregular ventricular
activity is usually the result of AF, but is not necessary to identify it (Gallagher and
Camm, 1998).
There are known causes of atrial fibrillation but at times there can be no
underlying heart disease. The most common causes of AF are hypertension, coronary
artery disease, valvular disease, congestive heart failure, cardiomyopathy, and congenital
heart disease (Benjamin, Levy et al., 1994); however, atrial fibrillation can also develop
after cardiac surgery (Benjamin, Wolf et al., 1998). Obesity as a risk factor has been
controversial in the past, but there is recent data suggesting an important risk relationship
between BMI and AF development (Wang, Parise et al., 2004). Non-cardiac etiological
factors associated with atrial fibrillation include high alcohol intake, thyrotoxicosis,
Page 20
8
diabetes, chronic obstructive lung disease, infection and pulmonary embolism (Conway,
2002). Also, atrial fibrillation may be related to excessive caffeine use, stress, illegal
drugs, electrolyte, or metabolic imbalances (Kannel, Wolf et al., 1998). In extreme cases,
the cause is unknown.
Atrial fibrillation can be diagnosed through several tests. The most common tools
used to diagnose AF include an electrocardiogram (ECG) or a holter monitor (24 hour
test). An ECG records the electrical impulses traveling through the heart muscle. The
holter monitor is a small external recorder that is usually worn for one to three days. This
may be necessary because the condition often occurs sporadically.
The echocardiographic risk factors for non-rheumatic AF include left atrial
enlargement, increased left ventricular thickness, and reduced left ventricular factional
shortening (Vaziri, Larson et al., 1994) For each of these echocardiographic predictors,
AF risk increases in a continuous graded fashion (Kannel, Wolf et al., 1998). Because
AF is usually associated with an underlying heart disease, other tests may need to be
performed to fully diagnose the patient’s condition including coronary angiography,
stress test, or nuclear imaging tests.
Atrial fibrillation patients may be classified as acute or chronic, depending on
whether the arrhythmia has been present for less than or more than 48 hours (Conway,
2002). Chronic AF can be further subdivided into paroxysmal (self-terminating and
relapsing episodes), persistent (continuous episode, but susceptible to pharmacological or
electrical cardioversion) and permanent (continuous AF despite attempts at
cardioversion) (Conway, 2002). AF is highly associated with morbidity and mortality
Page 21
9
(Gillinov, 2007) because of further complications and consequences that can occur such
as systemic thromboembolism, tachycardia-induced cardiomyopathy, significant
symptoms, and poor quality of life (Ad, 2007). Because the atria are beating rapidly and
irregularly in chronic AF, blood does not flow quickly through them increasing the risk
of a blood clot. The clot can then be pumped out of the heart and travel to other parts of
the body, such as the brain. Circulating blood clots could result in a stroke. Atrial
fibrillation patients are five to seven more times likely to have a stroke (Conway, 2002;
Savelieva and Camm, 2008). Where most attributable stroke risk factors decline with
advancing age, the attributable risks for stroke associated with AF increase with age,
from 1.5% for those 50 to 59 years of age to 23.5% for those 80 to 89 years of age (Wolf,
Abbott et al., 1991). In patients between the ages 80-89, AF is the single most important
independent risk factor for stroke (Conway, 2002).
Because of the asynchronous electrical activity, there is a loss of atrial systolic
function. The loss of atrial systolic function results in a decrease in stroke volume of
about 10% in normal individuals and a greater fall at fast ventricular rates because of the
reduction in diastolic filling time (Conway, 2002). Due to the decreased pumping ability
of the heart, AF is an independent risk factor for increased mortality and it is also
commonly associated with heart failure (HF) (Conway, 2002). The prevalence of AF
among patients with HF ranges from 10% to 30% (Crijns, Tjeerdsma et al., 2000). AF is
independently associated with a 50% to 90% increase in the risk of death in men and
women consistently across the 4 decades of age studied (from 1948 to 1988) (Benjamin,
Wolf et al., 1998).
Page 22
10
Some patients have AF without any signs or symptoms, a condition known as
silent AF. If symptoms occur, they include but are not limited to heart palpitations,
fatigue, shortness of breath, exercise intolerance, dizziness, angina, and syncope (Hamer,
Blumenthal et al., 1994; Luderitz and Jung, 2000). One study surveyed AF 147 patients
and reported that 78% of patients had palpitations, 69% had fatigue, 68% had shortness
of breath, 49% had exercise intolerance, 33% had dizziness, 29% had angina, and 14%
had syncope (Jung and Luderitz, 1998).
Treatments for AF can range from pharmacological to surgical. Since there are
intrinsic cardiac causes that predispose an individual to AF, simply decreasing the risk of
cardiovascular events that induce AF will directly decrease the incidence of AF. Rhythm
and rate control medications can help return the heart to its normal sinus rhythm (Ad,
2007; Savelieva and Camm, 2008). However, side effects include increased risk of other
arrhythmias. Anticoagulants or antiplatelet therapy medications that are used to reduce
the chance of blood clots and stroke can be contraindicated in the elderly because their
use is often associated with significant morbidity (Kannel, Wolf et al., 1998). Lifestyle
changes can also be beneficial. If a patient notices that certain activities trigger AF
symptoms, such as smoking, then those activities should be limited and or avoided.
Alcohol and caffeine should be taken in moderation if there is an excess usage or even
better completely avoided. Also stimulants in cough and cold medications can promote
irregular heart rhythms.
Page 23
11
Mitral Valve Regurgitation
Atrial fibrillation is sometimes combined with other problems. One of the
common problems associated with AF is mitral valvular disease or mitral regurgitation
(MR) (Howes, Reid et al., 2001; Gillinov, 2007; Parthenakis, Patrianakos et al., 2007).
The mitral valve permits the flow of blood from the atrium to the ventricle during
ventricular diastole and prevents retrograde flow during ventricular systole. The mitral
valve consists of valvar leaflets, the annulus, tendinous cords/papillary muscles, and
subvalvar apparatus. The mitral valvar complex also includes the left atrial and left
ventricle myocardium, left atrial and left ventricle endocardium, and the aorto-mitral
curtain (Muresian, 2008). The mitral valve uses the tight systolic closure of the left
atrioventricular orifice to prevent backflow of the blood from the left ventricle into the
atrium. As blood fills the left atrium, the mitral valve remains closed until adequate
pressure is generated to open the valve. The valve permissively allows for the atria to
rapidly, forcefully, and efficiently eject the blood into the left ventricle and then the aortic
root (Muresian, 2008).
Normally, the mitral valve opens due to pressure allowing blood to flow into the
left ventricle during left atria systole. It closes at the end of atrial contraction to prevent
blood from back flowing into the atria during left ventricular systole.
The mitral valve has two leaflets that guard the opening. The opening is
surrounded by a fibrous ring known as the mitral valve annulus. These leaflets are
prevented from prolapsing into the left atrium by the tendons attached to the posterior
surface of the valve, chordae tendineae. The chordae tendineae are attached at one end to
Page 24
12
the papillary muscles and the other to the valve cusps. When the left ventricle contracts,
the intraventricular pressure forces the valve to close and prevent blood from flowing
back into the left atria. During this time, the tendons prevent the valve from opening in
the wrong directions. This prevents blood from flowing back to the left atrium. If
damage occurs to any part of the mitral valvar complex, it can hamper emptying of the
left atrium, incompetence of the mitral valvar, and/or ejection of the left ventricle
(Muresian, 2008).
Mitral regurgitation (MR) is the second most common valve disease, representing
nearly one-third of acquired left-sided valve disease (Iung, Baron et al., 2003). Mitral
regurgitation is defined as a disorder in which the heart’s mitral valve does not properly
close, causing blood to flow backward into the upper heart chamber. This causes a
decrease in forward blood flow, which in turn through negative feedback increases the
forces of cardiac contraction (Libby, 2007). The main causes of mitral regurgitation
include myxomatous (degeneration of the mitral valve), ischemic heart disease, coronary
artery disease, and Rheumatic heart disease along with several others. Mitral
regurgitation may also be caused by dysfunction or injury to the valve following a heart
attack or infection of the heart valve (infective endocarditis) which may rupture the valve
or surrounding structures, leaving an opening for blood to move backwards (Libby,
2007). The most common cause of mitral regurgitation is myxomatous degeneration of
the valve. Degeneration is more common in males and with advancing age. There is a
defect in the collagen that makes up the mitral valve which causes the leaflets and
chordae tendineae to become stretched out. The stretched out valve leaflets and chordae
Page 25
13
tendineae prevent the valve leaflets from closing properly, causing the valve leaflets to
prolapse into the left atrium causing mitral regurgitation. The most common scenario
that involved both MR and AF is found in rheumatic disease (Gillinov, 2007).
It is important to distinguish between primary and secondary (functional) MR. In
primary MR, abnormalities of one or more components of the mitral valve cause it to leak
and permit backflow which in turn results in left ventricular volume overload (Carabello,
2008). Severe prolonged primary MR can result in left ventricular remodeling,
myocardial dysfunction, pulmonary hypertension, heart failure, and death. Correction of
primary MR in a timely fashion can help to prevent these effects. In secondary MR, a
damaged left ventricle causes the mitral valve to leak and as a result makes it harder to
treat secondary MR (Carabello, 2008). In secondary MR, myocardial damage causes a
normal valve to leak, so even if MR is corrected, the underlying muscle disease will still
persist (Carabello, 2008).
Mitral regurgitation can become a chronic condition. Symptoms include but are
not limited to chest pain, cough, rapid breathing, orthopnea, palpitations, fatigue, and
light-headedness (Libby, 2007). People with mild to moderate chronic mitral valve
regurgitation may be asymptomatic. Even moderate to severe disease may never display
symptoms. If the heart weakens because of the mitral valve, symptoms of heart failure
will occur: shortness of breath with activity, extreme tiredness and weakness, and/or
edema. Acute mitral valve regurgitation is an emergency, causing severe shortness of
breath at rest, coughing, and fast heart beat.
Page 26
14
MR imposes a volume overload in the left ventricle (LV), but unlike aortic
regurgitation, it does not cause an increase in systolic blood pressure (Wisenbaugh,
Spann et al., 1984). Because of increased LV volume from MR, total stroke volume
increases, and the resulting thin left ventricular wall enhances diastolic filling (Carabello,
2008). In acute MR, afterload is actually decreased; in chronic compensated MR
afterload is normal, and in chronic decompensated MR afterload may actually be greater
than normal (Corin, Monrad et al., 1987). If the damaged mitral valve is replaced, where
some or all of the chordal attachments between the papillary muscles and valve leaflets
are maintained, it can help preserve left ventricular function and improves exercise
capacity (David, Burns et al., 1984; Madaric, Watripont et al., 2007).
To diagnose mitral valve regurgitation, one of the simplest ways is for a doctor to
feel for a thrill (vibration) over the heart when feeling the chest area (Libby, 2007).
While listening to the heart, an extra heart sound (S4 gallop) and a distinctive heart
murmur may be heard (Libby, 2007). If fluid backs up in the lungs, crackles may be
heard. Diagnostic tests include a chest x-ray, CT scan of the chest, ECG,
echocardiogram, or a cardiac catheterization. Treatment depends on the severity of the
condition symptoms. Antibiotics are prescribed for bacterial infection and to reduce the
risk of infective endocarditis. Anti-hypertensive drugs and vasodilators reduce the strain
on the heart. Anti-coagulants or anti-platelet medications prevent clot formation in
patients that also have AF. Digitalis may be used to strengthen the heartbeat, and along
with diuretics, remove excess fluid in the lungs (Libby, 2007). Patients with severe
Page 27
15
symptoms may need to be admitted to a hospital for treatment, and for severe leakages
emergency surgery may be necessary.
Exercise Capacity and Exercise Tolerance
Exercise is a physiological stress that in turn stresses the cardiovascular system.
In the healthy population, heart rate (HR) and systolic arterial pressure (SAP) increase
during exercise. Patients with AF fatigue rapidly and experience palpitations more
frequently due to exertion. Gas exchange measurement for the determination of maximal
oxygen consumption (VO2MAX), as assessed during cardiopulmonary exercise testing, has
become widely established in the routine evaluation and in risk stratification of patients.
At sub maximal exercise levels, HR in patients with AF increases more than in those with
sinus rhythm (Ueshima, Myers et al., 1993; Howes, Reid et al., 2001). Exercise tests in
AF patients are performed predominantly in order to determine if the ventricular rate is
under control by pharmacological treatment, to determine functional capacity, and to plan
rehabilitation programs (Ueshima, Myers et al., 1993).
In patients with MR, echocardiographic findings at rest, such as systolic and
diastolic left ventricular dimension, do not accurately reflect a patient’s functional status
or symptoms (Enriquez-Sarano, Tajik et al., 1994). Cardiopulmonary exercise testing is
considered the standard tool for evaluating functional status, especially in AF and MR
patients. Poor exercise capacity, reflected by a low peak oxygen consumption (peak
VO2) paired with an increased ventilatory response as indicated by a steeper slope of
ventilation to carbon dioxide production rate (VE/VCO2 slope), are strong unfavorable
predictors of outcome (De Feo, Franceschini et al., 2005).
Page 28
16
Patients with AF have a significantly reduced exercise capacity (Agostoni, Emdin
et al., 2008). One of the major characteristics of AF that decreases exercise performance
is the irregular, rapid ventricular response at rest and during exercise which may reduce
cardiac output by 10% or more (Vanhees, Schepers et al., 2000). Cardiac patients with
concomitant AF may derive less benefit from traditional cardiac rehabilitation than other
cardiac patients because of their greater reduction in exercise tolerance related to AF.
Improving exercise tolerance is very important for these patients because their exercise
capacity can be reduced from 15-20% (Atwood, Myers et al., 2007). At anaerobic
ventilator threshold, AF patients have a higher VO2 and heart rate, while sinus rhythm
patients have a higher peak exercise VO2, O2 saturation, and work load (Agostoni, Emdin
et al., 2008). The reasoning for a lower VO2 at peak but higher VO2 at anaerobic
threshold is likely related to the higher chronotropic response to exercise in AF patients
likely due to an increased sympathetic drive activated to maintain cardiac output.
Agostini et al. did not measure cardiac output during exercise; since O2 saturation was
lower, they argued it was likely that stroke volume was lower at peak exercise in AF
patients. Despite the reduction in exercise tolerance, AF patients demonstrate similar
increases in VO2MAX compared to controls (Vanhees, Schepers et al., 2000). In addition
to improvements in exercise tolerance, exercise training also is associated with improved
overall emotional health (Hegbom, Sire et al., 2006). Interestingly, men demonstrate
greater improvements in peak VO2 and peak cardiac output with exercise training than
women (Mertens and Kavanagh, 1996).
Page 29
17
The heart is a muscle and like any muscle, it gets stronger with exercise. Aerobic
exercise strengthens the heart and makes it more efficient and is generally recommended
for those with mitral valve regurgitation. Studies have shown that AF patients who
engage in regular aerobic exercise report a decline in symptoms of chest pain, fatigue,
dizziness and mood swings, and panic attacks (Bonow, Carabello et al., 2006). A person
with mitral valve regurgitation should monitor their heart rate and other symptoms and
slow down if they feel their heart racing, become lightheaded, or faint.
Mitral valve regurgitation is generally not considered to be a life threatening or a
progressive condition. It may be the most benign of the various types of heart murmurs.
However, over time, the added workload on the heart may cause shortness of breath with
exercise or it may cause an abnormal heart rhythm (Bonow, Carabello et al., 2006). The
abnormal rhythm feels like your heart is pounding, racing, or skipping in your chest. If a
valve leaflet cord breaks, the sudden regurgitation may quickly cause heart failure. There
are cases where even mild mitral valve regurgitation poses significant health problems
and in these cases valve replacement would be considered.
Surgical Treatment
If medications are ineffective or not well tolerated by AF or MR patients, then
more aggressive treatment would be required. Non-pharmacological approaches are
usually offered to symptomatic patients, and can be done either by percutaneous catheter
techniques or various surgical approaches (Ad, 2007). Procedures such as electrical
cardioversion, catheter ablation, pulmonary vein isolation, or ablation of the AV node are
the most common procedures performed. If these procedures are unsuccessful, even
Page 30
18
more aggressive treatments may be necessary. Usually surgery is recommended for
patients with chronic AF and MR since their symptoms cannot be relieved by
medications or any other procedures. There are a few options for surgical treatment as
well, but the most widely used are the robotically assisted minimally invasive mitral
valve repair with the atrial cryo-maze procedure.
The original Cox-Maze procedure was developed by James Cox in 1987 to treat
the atrial fibrillation and restore the atria to a more normal atria (Cox, 1991). Since then
a series of improvements have been made, resulting in the Cox maze III procedure. Cox
Maze III is associated with a higher incidence of sinus rhythm return, improved long-
term sinus node function, fewer pacemaker implantations, and improved long-term atrial
transport function (Ad 2007). Now considered the “gold standard,” Cox-Maze III is also
technically less demanding than the Cox-Maze I and II procedures. During the
procedure, a series of precise incisions are made in the right and left atria to interrupt the
conduction of abnormal impulses (Cox, Jaquiss et al., 1995; Gillinov, 2007). A “maze”
of new electrical pathways is created to allow electrical impulses to travel easily through
the heart. This allows for a more normal sinus impulse to reach the AV node. A recent
report demonstrated long-term results in patients having the Cox-Maze III procedure,
either as an isolated or a combined procedure, with a success rate greater than 95%
(Damiano, Gaynor et al., 2003; Prasad, Maniar et al., 2003). Another important impact
of the Cox-Maze III procedure is a reduction in the rate of cerebrovascular accidents and
transient ischemic events (Ad, 2007; Gillinov, 2007). There have been numerous
revisions to the Cox-Maze III which have reduced the complexity of the procedure, but in
Page 31
19
turn have sacrificed the completeness of the procedure and produced questionable
outcomes (Kiser, Wimmer-Greinecker et al., 2007). According to Kiser et al. (2007), the
best treatment for all types of atrial fibrillation remains the full Cox-Maze III, which
addresses both the left and right atria; and is also associated with clinical benefits in
patients with mitral valve disease (Gillinov, 2007).
Originally the Cox Maze procedure used the standard cut-and-sew method. Now
there are a variety of devices that use different energy sources that permits the surgeon to
rapidly perform corrective AF with very few suture lines (Gammie, Didolkar et al.,
2009). One of the new methods uses argon-powered cryoenergy and is known as
CryoMaze. As a treatment for atrial fibrillation, the CryoMaze procedure creates linear
cyolesions (frozen scars) in the upper chamber of the heart by applying an argon-powered
cold probe to freeze the tissue (Gammie, Laschinger et al., 2005). Freezing the tissue
creates electrical barriers, which permanently block electrical activity, thus correcting for
AF. Electrical barriers can be created in 60-90 seconds, minimizing the duration of the
procedure. It has been suggested to be safer and more efficient for the treatment of AF
(Gammie, Laschinger et al., 2005) or when combined with other cardiac operations
(Gammie, Didolkar et al., 2009). Associated with the CryoMaze are lower stroke rates in
long-term follow-up and results that are equivalent to those of the classic Cox Maze III
(Gammie, Laschinger et al., 2005). Compared with other energy sources, collateral
injury has never been reported, there is a long track record of safety, there is a greater
likelihood of a contiguous lesion, and cryotherapy is associated with a lower endocardial
thrombus volume (Gammie, Laschinger et al., 2005; Gammie, Didolkar et al., 2009).
Page 32
20
With surgery time being reduced, recovery duration is the next stage. Minimally
invasive mitral valve surgery continues to evolve as a treatment option. Studies have
been conducted showing that mitral valve procedures could be performed with a small
incision by modifying the standard sternotomy, or open chest method (Cohn, Adams et
al., 1997; Cosgrove, Sabik et al., 1998). These studies have also reported large and
successful series of endoscopic mitral valve repairs using various systems. But with the
da Vinci® Robotic system, many of the concerns of minimally invasive mitral valve
repair were addressed. The da Vinci® Robotic system allows three-dimensional
visualization of the operative field and improved surgical manipulation by the use of the
endowrists of the surgical arms (Tatooles, Pappas et al., 2004). With the introduction of
the transthoracic aortic cross clamp and the da Vinci® Surgical System, mitral valve
repair can be performed in the same manner as the standard sternotomy but with truly
limited incisions (Tatooles, Pappas et al., 2004). Advantages of minimally invasive
mitral valve surgery are reduced surgical trauma, decreased pain, fewer complications,
improved cosmesis, shorter length of stay, less bleeding and fewer pulmonary
complications, and earlier return to normal daily activity for the patient (Mohr, Onnasch
et al., 1999; Reichenspurner, Boehm et al., 2000; Felger, Chitwood et al., 2001;
Casselman, Van Slycke et al., 2003; Tatooles, Pappas et al., 2004).
On the day of surgery, electrodes are placed on the patient’s chest. The electrodes
are connected to an electrocardiogram machine which monitors the patient’s heart rhythm
and electrical activity. For the original procedure, the surgeons make an incision down
the center of the chest and then split the breastbone. This facilitates complete
Page 33
21
visualization of the heart and reduces the number of complications. However, using the
Robotic-Assisted Maze surgery only small incisions are made between the ribs. The
surgeon uses video guided instruments to manipulate a catheter and perform the
ablations. The catheter directs cryo-freeze energy to the precise areas in the heart tissue
to create lesions that block erratic electrical signals from traveling through the heart (Cox,
Jaquiss et al., 1995; Savelieva and Camm, 2008). The patterns of the incision resemble a
maze, which directs the heart’s electrical impulses straight to the heart’s lower chambers
due to scar tissue that forms. The scar tissue cannot carry electrical impulses and thus
creates a barrier to keep the electrical impulses on course.
Surgical correction of MR aims to preserve cardiac function and to improve
function status and survival (Le Tourneau, de Groote et al., 2000). Chronic MR results in
a progressive deterioration in left ventricle (LV) contractile function, although the LV
ejection fraction (EF) is maintained over a relatively long period (Starling, 1995). After
mitral valve surgery, LV contractile impairment has the ability to recover towards normal
in most patients.
Exercise tolerance after surgery
In AF patients, Cox Maze does appear to effectively prevent exercise-induced AF
(Hemels, Gu et al., 2006). In patients in whom sinus rhythm was established by Cox-
Maze, exercise-induced initiation of AF was not observed.
Exercise capacity of patients with and without heart disease that underwent the
Cox Maze procedure combined with mitral valve surgery do experience improvements in
exercise tolerance in the late phase of their recovery hypothesized to occur through the
Page 34
22
restoration of sinus rhythm (Yuda, Nakatani et al., 2004). Mitral valve surgery can
improve exercise tolerance independent of sinus rhythm abnormalities (Le Tourneau, de
Groote et al., 2000), though not all studies demonstrate such an effect (Kim, Ahn et al.,
2004).
The proper timing of surgery in asymptomatic patients remains controversial
(Madaric, Watripont et al., 2007). Usually, surgery was proposed when patients started
having symptoms. However, it has been shown that patients operated on before the
occurrence of symptoms have a better survival than patients operated on with severe
symptoms (Enriquez-Sarano, Tajik et al., 1994; Tribouilloy, Enriquez-Sarano et al.,
1999). Currently the effect of mitral valve repair (MVR) on exercise capacity and
cardiopulmonary testing in patients with little or no symptoms is relatively unknown;
however, studies have attempted to understand the mitral valve healing duration post
surgery to better access those effects.
One study looked at exercise tolerance 6 months after surgery and showed no
change in exercise tolerance despite the mitral regurgitation correction, in absence of
exercise reconditioning (Le Tourneau, de Groote et al., 2000). It is well known that
physical training improves exercise performance in patients with coronary heart disease
(Hambrecht, Walther et al. 2004) and heart failure (Belardinelli, Georgiou et al., 1999),
but it is not known how long it takes for the mitral valve to heal after mitral regurgitation
surgery in humans. Meurin et al. (2005) evaluated the safety and feasibility of early
exercise training in patients after mitral valve repair. The 251 subjects were placed in an
exercise training program that included calisthenics and endurance bicycle training for
Page 35
23
about 8 weeks. Exercise training increased both peak VO2 (22% increase) and anaerobic
threshold (16% increase) (Meurin, Iliou et al., 2005). Exercise training appears to be safe
in this population, does not have adverse effects on mitral valve function, and improves
exercise tolerance.
Madaric et al. (2007) assessed the changes in cardiopulmonary functional
capacity after minimally invasive video-assisted mitral valve repair in patients with mitral
regurgitation with mild to no symptoms. All patients were in sinus rhythm and had a
normal ejection fraction, and 80% claimed to be completely asymptomatic. They focused
on testing patients one week before surgery and 4 months after surgery and were tested
using a ramp protocol. The patients’ quality of life was also assessed during testing time
by the Euro Quality of life (EuroQol) questionnaire (Dolan, 1997). The questionnaire
was composed of 5 items: mobility, self-care, usual activity, pain or discomfort, and
anxiety or depression. Four months after surgery they found significant improvements in
VO2MAX, maximal workload, and peak oxygen pulse. Patients increased their overall
health status also. They concluded their study stating that the minimally invasive repair
improves exercise capacity of patients with severe mitral regurgitation with none to mild
symptoms.
Conclusion
Aging increases the risk of developing AF and MR, both which decrease exercise
capacity and exercise tolerance. It is imperative to examine exercise capacity post
surgery to gain a better understanding of how quickly patients can return to normal daily
activity and improvements in exercise capacity. There is no documented evidence
Page 36
24
examining the exercise capacity in patients 7-11 weeks post surgery. The aim of this
study is to measure the patients’ VO2MAX pre and 7-11 weeks post surgery to see if there
is a difference in exercise tolerance. Insight into exercise tolerance changes 7-11 weeks
post surgery can lead to quicker return to daily activity and ability to increase exercise
capacity post surgery.
Page 37
CHAPTER III
METHODS
Prior to testing, approval of methods was given by the University and Medical
Center Institutional Review Board, and conformed to the University, State of North
Carolina, and Federal mandates for standard operating procedures (Appendix A).
Subjects
Subjects diagnosed and already scheduled for treatment of AF, MR or AF+MR by
minimally invasive surgery were recruited by their physician. Any patient who was
involved in a structured exercise program or participated in 30 minutes of vigorous
exercise per week in the last 2 months was excluded. Also any other medical conditions
that would prevent patients from safely participating in this study or would result in
worsened exercise capacity independent of their cardiac disease were excluded. Once
participants were selected they had the following procedures performed before and 7-11
weeks post-surgery. Four male subjects volunteered for this study (mean age 57 years).
Testing Protocol
The testing of these patients was covered over two visits. All testing was
performed at Brody room 3S08. After informed consent was signed, on each testing day
Physical Activity Scale for the Elderly (PASE) questionnaire and the Modified Baeke
(Appendix C) was filled out by one on one interview, resting vitals were measured
(height, weight, resting blood pressure, and resting heart rate), minimum waist
circumference, and percent body fat was measured by skin folds. Skin fold locations
include chest, axilla, triceps, subscapular, abdominal, suprailium, and thigh. All
Page 38
26
measurements were done on the right side of the body and performed twice, three times if
there is a more then 2 mm discrepancy in measurements.
The questionnaire was used to quantify the amount of activity each individual did
before and after surgery. PASE questionnaire was used because it closely matched the
literature for how patients function ability was with their condition. Patients were
compared to themselves regarding changes in activity levels pre and post-surgery.
Following the resting measurements, subjects performed a physician supervised,
symptom limited, graded exercise test using the Modified Naughton treadmill test (Table
1) for determination of maximal oxygen consumption (VO2MAX). Exercise intensity
increased while minute ventilation, inhaled oxygen and exhaled carbon dioxide
concentrations of the subject were continuously monitored via ParvoMedics TrueMax
2400 Metabolic Cart (Consentius Technologies, Sandy, UT). VO2MAX is the maximum
capacity of an individual’s body to transport and utilize oxygen during incremental
exercise, which reflects the physical fitness of the individual. VO2MAX is reached when
oxygen consumption remains at steady state despite an increase in workload. Prior to and
during exercise, subjects had their blood pressure measured and a 12-lead ECG
monitored. Heart rate was monitored continuously and recorded every two minutes using
a Polar Electro heart rate monitor (Polar Electro, Washington, NY). Subjects were
encouraged to continue as long as possible. The exercise test was stopped if the subject
felt dizzy, had chest pain, had serious shortness of breath, or verbally indicated they
wanted the test to be ended. If the physician detected an abnormal heart function from
the ECG, then the test was terminated. At the end maximum time was recorded.
Page 39
27
Statistical Analysis
A paired t-test was used to determine differences in VO2MAX pre- and post-surgery
in between individuals. Significance was established at P ≤ 0.05 and data reported are
Mean ± SE.
Page 40
28
Table 1: Modified Naughton Treadmill Protocol
Time (min) Stage Speed (mph) Grade (%)
0-2 1 1.0 0
2-4 2 1.5 0
4-6 3 2.0 3.5
6-8 4 2.0 7.0
8-10 5 2.0 10.5
10-12 6 3.0 7.5
12-14 7 3.0 10.0
14-16 8 3.0 12.5
16-18 9 3.0 15.0
18-20 10 3.5 15.0
Time (min), time in minutes of the treadmill test. Speed (mph), speed, measured in miles
per hour, for each stage. Grade (%), percent incline for each stage.
Page 41
CHAPTER IV
RESULTS
Subject Characteristics
Subject characteristics are in Table 2. Four male patients completed both the pre-
and post-surgery exercise testing. Mitral valve disease was present in all patients and
surgical repair was performed. One patient had combined MR and AF and also had the
biatrial cryo-maze procedure performed. All patients had the minimally invasive robotic
surgery performed. There were no differences in HR, % body fat, waist circumference,
or treadmill time pre and post-operative (Table 4).
Exercise Tolerance
There was no change in exercise tolerance pre vs. 7-11 weeks post-operation,
therefore showing that patients did not have a reduced exercise capacity after surgery
(Table 4). Subjects also showed no significant changes in their activitity levels, treadmill
time to exhaustion and HR pre and post surgery (Table 4). When compared to Houmard
et al.’s (1998) age predicted data, the subjects’ VO2MAX were not significantly different
before or after surgery (Figure 1). However, when compared to ACSM age predicted
VO2MAX, subject’s had a significantly lower post-surgery VO2MAX (Medicine, 2005)
(Figure 2).
Page 42
30
Table 2: NYHA Classification
Class Patient Symptoms Patients
Class I (Mild) No limitation of physical activity. 4
Ordinary physical activity does not cause
undue fatigue, palpitation, or dyspnea
(shortness of breath).
Class II (Mild) Slight limitation of physical activity. 0
Comfortable at rest, but ordinary physical
activity results in fatigue, palpitation, or dyspnea.
Class III
(Moderate) Marked limitation of physical activity. 0
Comfortable at rest, but less than ordinary
activity causes fatigue, palpitation, or dyspnea.
Class IV (Severe) Unable to carry out any physical activity 0
without discomfort. Symptoms of cardiac
insufficiency at rest. If any physical activity
is undertaken, discomfort is increased.
In order to determine the best course of therapy, physicians often assess the stage of heart
failure according to the New York Heart Association (NYHA) functional classification
system. This system relates symptoms to everyday activities and the patient's quality of
life.
Page 43
31
Table 3: Individual Data Pre and Post surgery
Record Age Pre % Fat Height Weight Waist TM Time Max HR Pre-VO2MAX Pre-VO2MAX
Number (yrs) (%) (cm) (kg) (cm) (min) (bpm) (L/min) (mL/kg/min)
MR001 59 N/A 175.3 75.9 n/a 20:00 189 2.21 29.1
MR002 49 24.2 172.7 89.5 98.0 13:40 149 2.04 22.7
MR003 64 18.4 188.0 78.6 94.0 12:36 157 1.89 24.1
MR005 56 20.5 170.2 84.5 100.3 21:10 164 2.91 34.5
Record Age Post % Fat Height Weight Waist TM Time Max HR Post-VO2MAX Post-VO2MAX
Number (yrs) (%) (cm) (kg) (cm) (min) (bpm) (L/min) (mL/kg/min)
MR001 59 24.8 175.3 72.1 97.8 19:22 180 2.12 28.0
MR002 49 26.1 172.7 90 97.8 15:24 167 2.15 23.9
MR003 64 18.7 188.0 77.5 92.2 12:42 150 1.68 21.7
MR005 56 27.6 170.2 84.5 101.6 15:40 110 2.14 25.3
% Fat, percentage body fat taken using 7 site skin folds on the right side of the subject
pre- and post-operation. TM, Treadmill time to maximum exercise. Max HR, heart rate
at maximum exercise. VO2MAX, maximal oxygen consumption.
Page 44
32
Table 4: Demographic and Exercise Data
Pre-Op Post-Op P Value
Age, yrs 57 ± 3
Height, cm 176.0 ± 4.3
Mass, kg 82.2 ± 3.1 81.1 ± 3.9 0.321
Waist, cm 97.5 ± 1.5 97.3 ± 2.0 0.762
%BF 21.0 ± 1.5 24.3 ± 1.9 0.520
PASE Scores 255 ± 100 194 ± 103 0.171
TM time, sec 1012 ± 131 947 ± 82 0.539
Max HR, bpm 164.8 ± 8.6 151.8 ± 15.2 0.449
Absolute VO2MAX, (L/min) 2.26 ± 0.23 2.023 ± 0.11 0.293
Pre (Pre-Op) and post-operative (Post-Op) data. %BF, percentage body fat. PASE
Scores, Physical Activity Scale for the Elderly. TM time, maximum treadmill time to
exhaustion. Max HR, heart rate at maximum exercise. VO2MAX, absolute maximal
oxygen consumption. * - significantly different (p ≤ 0.05). Mean ±SE.
Page 45
33
Relative VO2MAX
Pre and Post-operation
Compared to age predicted data
Pre-Op Post-Op Age Predicted0
10
20
30
40
VO
2max
(mL/
kg/m
in)
Figure 1: Relative VO2MAX pre (Pre-Op) and post-operative (Post-Op) and age
predicted (Houmard, Weidner et al. 1998). One way repeated measures Anova was used
to analyze relative VO2MAX pre (Pre-Op) and post-operative (Post-Op) and age predicted
data (Houmard, Weidner et al. 1998). There were no significant differences in relative
VO2MAX between Pre-Op, Post-Op, or Age Predicted. # - significant difference between
groups. Mean ±SE.
Page 46
34
Relative VO2MAX
Pre and Post-operation
Compared to ACSM data
Pre-Op Post-Op ACSM0
10
20
30
40 #
VO
2max
(m
L/kg
/min
)
Figure 2: Relative pre (Pre-Op) and post-operative (Post-Op)VO2MAX values compared
to ACSM age predicted (Medicine 2005). One way repeated measures Anova was used
to analyze relative VO2MAX pre (Pre-Op) and post-operative (Post-Op) and ACSM age
predicted data (Medicine 2005). ACSM age predicted VO2MAX was found to be
significantly higher than post-operative values. # - significantly different than all other
groups (p ≤ 0.05). Mean ±SE.
Page 47
CHAPTER V
DISCUSSION
Findings
The principle findings of this study are: 1) patients did not have reduced exercise
tolerance after surgery when compared to pre-operative, 2) when compared to age
predicted data (Houmard, Weidner et al. 1998), VO2MAX was not significantly different
before or after surgery (Figure 1), and 3) there was no change in activity levels between
pre and post surgery (Table 4). The findings of the current study do not support the
hypothesis that exercise tolerance would be reduced 7-11 weeks post-operation.
Subject Characteristics
Patients were recruited by their physician and in this study were asymptomatic
and functional in their daily living up until the day of surgery. The NHYA
classifications, which are a functional and therapeutic classification for prescription of
physical activity for cardiac patients, showed the subjects were not in a severe condition.
All four patients were NHYA I classified, meaning they had no limitation of physical
activity and ordinary physical activity does not cause undue fatigue, palpitation, or
dyspnea (shortness of breath). They were not assisted in their daily living, those that
worked still went to work, and their daily activities were not affected by their heart
condition.
Patients came in one week to as little as 3 days before their surgery. Patients are
not seen far in advance before surgery and get surgical treatment soon after their first
exercise visit. Their post-operation stress test was done at approximately 7-11 weeks
Page 48
36
post-op, usually during their follow-up with the surgeon. Unlike previous studies that
tested severely de-conditioned patients who were unable to perform their daily activities,
the patients in the current study were completely functional and were younger (mean age
57 ± 3 compared to studies with mean ages of 70+). The current study specifically tested
patients that were not severely de-conditioned and had a very good NYHA classification.
Another study, that investigated severely de-conditioned patients who were unable to
perform their daily activities, showed that after surgery their activities levels did increase
and they were able to perform majority of their daily activities without fatigue (Le
Tourneau, de Groote et al., 2000).
Given that the current patients were sedentary post-operation and still healing
from surgery, their exercise capacity did not drop significantly from pre-operations
values. When compared to Houmard et. al’s (1998) age predicted data, there was no
significant difference. The subjects’ VO2MAX were closer to Houmard et. al’s (1998) age-
predicted data then when compared to ACSM’s age predicted VO2MAX. This is due to the
fact that as an individual ages, their VO2MAX decreases linearly and a prediction that takes
that into account is more accurate. ACSM’s data classifies individuals based on a 10 year
age predicted VO2MAX (Medicine 2005). A 50 year old male’s VO2MAX will not be the
same when he turns 59 years old and thus cannot be compared. ACSM’s data is an
average of national VO2MAX for a 10 year age range. Houmard et. al’s (1998) study
closely matches the population in this study because it represents Eastern North
Carolina’s VO2MAX values and eliminates the age gap represented in ACSM’s data.
Although the subject’s VO2MAX were closely matched with another study (Houmard,
Page 49
37
Weidner et al., 1998), only 2 subjects (MR002, MR003) had lower than normal values.
However there was no significant difference when compared to pre-operation values.
Treadmill times varied with individuals: MR001 and MR005 had lower post-operation
treadmill times, while the other two subjects MR002 and MR003 had higher post-
operation treadmill times. Overall the mean treadmill time for the subjects were no
different post-operation compared to pre-operation. All subjects continued testing until
they indicated they wanted the test to be terminated. Also subjects reached their 60%
heart rate max, which showed a true max for the patients in the current study.
There were a few factors that were controlled in this study. First patients enrolled
were already diagnosed with valvular disease, AF, or both. Second, these patients were
scheduled to have minimally invasive corrective surgery. Lastly, patients were not to
have a NYHA class of III or IV, thus causing them increased discomfort with stress
testing. Whether or not patients returned to their daily activities or if they exercised post-
surgery was not controlled.
Effects of AF and MR on Exercise Tolerance
Severe AF and MR patients have reduced exercise tolerance and an inability to
increase it due to the palpitations and fatigue associated with the disease (De Feo,
Franceschini et al. 2005; Agostoni, Emdin et al. 2008). Typically these patients cannot
perform their usual daily activity, are greatly fatigued by minimal exertion, and have a
severely reduced exercise tolerance (Agostoni, Emdin et al. 2008). Compared to
previous studies (Lewis, Irvine et al. 1988), the current subjects were asymptomatic and
did not have a severe disease progression nor a severely reduced exercise tolerance.
Page 50
38
Unlike previously treated patients that were in severe condition (Lewis, Irvine et al.
1988), the current patients were still active and performing their daily activities with little
to no help. When compared to age predicted data with no signs of CHF or other known
cardiac problem (Houmard, Weidner et al. 1998), there was no significant differences in
VO2MAX.
Effect of Minimally Invasive Sugery on Exercise Tolerance
Studies have shown that Minimally Invasive Robotic Surgery does return a
patient to normal sinus rhythm (Gammie, Laschinger et al., 2005; Gammie, Didolkar et
al., 2009) and return a patient to their daily activities 2 weeks quicker than a normal
sternotomy (Mohr, Onnasch et al., 1999; Reichenspurner, Boehm et al., 2000; Felger,
Chitwood et al., 2001). It has also been shown that treating MR and AF early, before the
condition becomes severe enough to decrease an individual’s daily activities, can return
the patient to a condition capable of increasing their exercise tolerance (Meurin, Iliou et
al., 2005). However, it is not known how soon surgical treatment should be given in MR
and AF patients. It is also unknown how soon improved exercise tolerance can be
observed (with no training).
Historically, exercise tolerance is reduced in AF and MR patients (De Feo,
Franceschini et al., 2005; Agostoni, Emdin et al., 2008) and surgical treatment improves
exercise tolerance (Le Tourneau, de Groote et al., 2000; Meurin, Iliou et al., 2005). In
AF and MR patients with reduced exercise tolerance, surgical intervention improved
exercise tolerance by 11.2% at 4 mo post-surgery (Madaric, Watripont et al., 2007).
When surgical treatment is followed with formal exercise training, peak oxygen
Page 51
39
consumption and anaerobic threshold increased 22% and 16% respectively 8 weeks post
surgery (Meurin, Iliou et al., 2005). Compared to those results, the current study found
that 7-11 weeks after surgery, with patients being sedentary, there was no difference in
exercise capacity.
Limitations
A limitation that could not be controlled was the time the patient was tested for
their post-operative visit. Because of scheduling patients coming from out of town and
unseen factors such as illness, patient’s post-operative visits varied. The post-operative
visit was between 7-11 weeks post-surgery. Three patients came in 7 weeks after surgery
with one coming in 11 weeks after surgery.
Since all testing was done at Brody, there was a limitation with measuring body
fat percentage. Instead of using a Dual Energy X-Ray Absorptiometry (DEXA) to
measure body fat, a 7-site skinfold was taken on the right side of every subject. While
the accuracy of predicting percent fat from skinfolds is approximately plus or minus 3.5%
assuming that appropriate techniques and equations have been used (Medicine, 2005),
DEXA has an accuracy of plus or minus 1-3%.
Inexperience in treadmill usage was an issue for some patients. Some patients felt
very comfortable on the treadmill, keeping hands by their sides and swinging them; while
others patients were not as accustomed to the incline of the machine and holding the side
handle bars. This could have biased exercise tolerance during the initial test toward
lower exercise tolernace pre-surgery.
Future Projects
Page 52
40
In order for a stronger finding to occur, more subjects need to be recruited and
tested. Since the patients in this study were treated fairly early in their disease
progression (NYHA classication Stage 1), a 6 month follow up in combination with an
exercise training may demonstrate significant increases in VO2MAX. If these patients
underwent an exercise training program and follow up evaluations could be done,
perhaps their VO2MAX would be higher.
Conclusions
At 7-11 weeks following minimally invasive surgery to treat MR and AF,
exercise tolerance is unchanged compared to pre-surgery. While not tested in the current
investigation, it is likely that surgical treatment involving a sternocotomy would have
decreased exercise tolerance at 7-11 weeks post-op suggesting that minimally invasive
surgery does provide significant outcomes for patients by maintaining exercise tolerance.
Historically, surgical treatment for MR and AF is associated with an improvement in
exercise tolerance which was not observed in the current investigation, however when
patients with MR and AF are tested early in disease progression (NYHA class I) there is
no significant decrement in exercise tolerance compared to age normative data and so
surgery would not be expected to improve exercise tolerance. Since the patients in the
current study were treated fairly early, they can return to daily activities quicker post
surgery and they have the potential to increase their exercise tolerance and be above age
normative data. The results of this study do not support the hypothesis that subjects’
exercise capacity and tolerance will be reduced 7-11 weeks post-operation.
Page 53
REFERENCES
Ad, N. (2007). "The Cox-Maze procedure: History, results, and predictors for failure." J
Interv Card Electrophysiol 20(3): 65-71.
Agostoni, P., M. Emdin, et al. (2008). "Permanent atrial fibrillation affects exercise
capacity in chronic heart failure patients." Eur Heart J.
Atwood, J. E., J. N. Myers, et al. (2007). "Exercise capacity in atrial fibrillation: a
substudy of the Sotalol-Amiodarone Atrial Fibrillation Efficacy Trial (SAFE-T)."
Am Heart J 153(4): 566-72.
Belardinelli, R., D. Georgiou, et al. (1999). "Randomized, controlled trial of long-term
moderate exercise training in chronic heart failure: effects on functional capacity,
quality of life, and clinical outcome." Circulation 99(9): 1173-82.
Benjamin, E. J., D. Levy, et al. (1994). "Independent risk factors for atrial fibrillation in a
population-based cohort. The Framingham Heart Study." Jama 271(11): 840-4.
Benjamin, E. J., P. A. Wolf, et al. (1998). "Impact of atrial fibrillation on the risk of
death: the Framingham Heart Study." Circulation 98(10): 946-52.
Bonow, R. O., B. A. Carabello, et al. (2006). "ACC/AHA 2006 guidelines for the
management of patients with valvular heart disease: a report of the American
College of Cardiology/American Heart Association Task Force on Practice
Guidelines (writing committee to revise the 1998 Guidelines for the Management
of Patients With Valvular Heart Disease): developed in collaboration with the
Society of Cardiovascular Anesthesiologists: endorsed by the Society for
Page 54
42
Cardiovascular Angiography and Interventions and the Society of Thoracic
Surgeons." Circulation 114(5): e84-231.
Carabello, B. A. (2008). "The current therapy for mitral regurgitation." J Am Coll Cardiol
52(5): 319-26.
Casselman, F. P., S. Van Slycke, et al. (2003). "Endoscopic mitral valve repair: feasible,
reproducible, and durable." J Thorac Cardiovasc Surg 125(2): 273-82.
Cohn, L. H., D. H. Adams, et al. (1997). "Minimally invasive cardiac valve surgery
improves patient satisfaction while reducing costs of cardiac valve replacement
and repair." Ann Surg 226(4): 421-6; discussion 427-8.
Conway, D. L., G (2002). "Atrial Fibrillation." Medicine: 140-144.
Corin, W. J., E. S. Monrad, et al. (1987). "The relationship of afterload to ejection
performance in chronic mitral regurgitation." Circulation 76(1): 59-67.
Cosgrove, D. M., 3rd, J. F. Sabik, et al. (1998). "Minimally invasive valve operations."
Ann Thorac Surg 65(6): 1535-8; discussion 1538-9.
Cox, J. L. (1991). "The surgical treatment of atrial fibrillation. IV. Surgical technique." J
Thorac Cardiovasc Surg 101(4): 584-92.
Cox, J. L., R. D. Jaquiss, et al. (1995). "Modification of the maze procedure for atrial
flutter and atrial fibrillation. II. Surgical technique of the maze III procedure." J
Thorac Cardiovasc Surg 110(2): 485-95.
Crijns, H. J., G. Tjeerdsma, et al. (2000). "Prognostic value of the presence and
development of atrial fibrillation in patients with advanced chronic heart failure."
Eur Heart J 21(15): 1238-45.
Page 55
43
Damiano, R. J., Jr., S. L. Gaynor, et al. (2003). "The long-term outcome of patients with
coronary disease and atrial fibrillation undergoing the Cox maze procedure." J
Thorac Cardiovasc Surg 126(6): 2016-21.
David, T. E., R. J. Burns, et al. (1984). "Mitral valve replacement for mitral regurgitation
with and without preservation of chordae tendineae." J Thorac Cardiovasc Surg
88(5 Pt 1): 718-25.
De Feo, S., L. Franceschini, et al. (2005). "Ischemic etiology of heart failure identifies
patients with more severely impaired exercise capacity." Int J Cardiol 104(3):
292-7.
Dolan, P. (1997). "Modeling valuations for EuroQol health states." Med Care 35(11):
1095-108.
Enriquez-Sarano, M., A. J. Tajik, et al. (1994). "Echocardiographic prediction of survival
after surgical correction of organic mitral regurgitation." Circulation 90(2): 830-7.
Feinberg, W. M., J. L. Blackshear, et al. (1995). "Prevalence, age distribution, and gender
of patients with atrial fibrillation. Analysis and implications." Arch Intern Med
155(5): 469-73.
Felger, J. E., W. R. Chitwood, Jr., et al. (2001). "Evolution of mitral valve surgery:
toward a totally endoscopic approach." Ann Thorac Surg 72(4): 1203-8;
discussion 1208-9.
Gallagher, M. M. and J. Camm (1998). "Classification of atrial fibrillation." Am J
Cardiol 82(8A): 18N-28N.
Page 56
44
Gammie, J. S., P. Didolkar, et al. (2009). "Intermediate-term outcomes of surgical atrial
fibrillation correction with the CryoMaze procedure." Ann Thorac Surg 87(5):
1452-8; discussion 1458-9.
Gammie, J. S., J. C. Laschinger, et al. (2005). "A multi-institutional experience with the
CryoMaze procedure." Ann Thorac Surg 80(3): 876-80; discussion 880.
Gillinov, M. (2007). "Atrial fibrillation surgery in nonrheumatic mitral valve disease." J
Interv Card Electrophysiol 20(3): 101-7.
Go, A. S., E. M. Hylek, et al. (2001). "Prevalence of diagnosed atrial fibrillation in
adults: national implications for rhythm management and stroke prevention: the
AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study." Jama
285(18): 2370-5.
Hambrecht, R., C. Walther, et al. (2004). "Percutaneous coronary angioplasty compared
with exercise training in patients with stable coronary artery disease: a
randomized trial." Circulation 109(11): 1371-8.
Hamer, M. E., J. A. Blumenthal, et al. (1994). "Quality-of-life assessment in patients with
paroxysmal atrial fibrillation or paroxysmal supraventricular tachycardia." Am J
Cardiol 74(8): 826-9.
Hegbom, F., S. Sire, et al. (2006). "Short-term exercise training in patients with chronic
atrial fibrillation: effects on exercise capacity, AV conduction, and quality of
life." J Cardiopulm Rehabil 26(1): 24-9.
Hemels, M. E., Y. L. Gu, et al. (2006). "Favorable long-term outcome of Maze surgery in
patients with lone atrial fibrillation." Ann Thorac Surg 81(5): 1773-9.
Page 57
45
Houmard, J. A., M. L. Weidner, et al. (1998). "Fiber type and citrate synthase activity in
the human gastrocnemius and vastus lateralis with aging." J Appl Physiol 85(4):
1337-41.
Howes, C. J., M. C. Reid, et al. (2001). "Exercise tolerance and quality of life in elderly
patients with chronic atrial fibrillation." J Cardiovasc Pharmacol Ther 6(1): 23-9.
Iung, B., G. Baron, et al. (2003). "A prospective survey of patients with valvular heart
disease in Europe: The Euro Heart Survey on Valvular Heart Disease." Eur Heart
J 24(13): 1231-43.
Jung, W. and B. Luderitz (1998). "Quality of life in patients with atrial fibrillation." J
Cardiovasc Electrophysiol 9(8 Suppl): S177-86.
Kannel, W. B., P. A. Wolf, et al. (1998). "Prevalence, incidence, prognosis, and
predisposing conditions for atrial fibrillation: population-based estimates." Am J
Cardiol 82(8A): 2N-9N.
Kim, H. J., S. J. Ahn, et al. (2004). "Cardiopulmonary exercise testing before and one
year after mitral valve repair for severe mitral regurgitation." Am J Cardiol 93(9):
1187-9.
Kiser, A. C., G. Wimmer-Greinecker, et al. (2007). "Totally extracardiac Maze procedure
performed on the beating heart." Ann Thorac Surg 84(5): 1783-5.
Le Tourneau, T., P. de Groote, et al. (2000). "Effect of mitral valve surgery on exercise
capacity, ventricular ejection fraction and neurohormonal activation in patients
with severe mitral regurgitation." J Am Coll Cardiol 36(7): 2263-9.
Page 58
46
Lewis, R. V., N. Irvine, et al. (1988). "Relationships between heart rate, exercise
tolerance and cardiac output in atrial fibrillation: the effects of treatment with
digoxin, verapamil and diltiazem." Eur Heart J 9(7): 777-81.
Libby, P. B., RO; Mann, DL; Zipes,DP (2007). Braunwald's Heart Disease: A Textbook
of Cardiovascular Medicine. St. Louis, MO, WB Saunders.
Luderitz, B. and W. Jung (2000). "Quality of life in patients with atrial fibrillation." Arch
Intern Med 160(12): 1749-57.
Madaric, J., P. Watripont, et al. (2007). "Effect of mitral valve repair on exercise
tolerance in asymptomatic patients with organic mitral regurgitation." Am Heart J
154(1): 180-5.
Malcolm S. Thaler, M. D. (2007). The Only EKG Book You'll Ever Need. Philadelphia,
PA, Lippincott Williams & Wilkins.
Medicine, A. C. o. S. (2005). ACSM's Guidelines for Exercise Testing and Prescription
7th Ed, Lea & Febiger / Lippincott Williams & Wilkins: Philadelphia.
Mertens, D. J. and T. Kavanagh (1996). "Exercise training for patients with chronic atrial
fibrillation." J Cardiopulm Rehabil 16(3): 193-6.
Meurin, P., M. C. Iliou, et al. (2005). "Early exercise training after mitral valve repair: a
multicentric prospective French study." Chest 128(3): 1638-44.
Miyasaka, Y., M. E. Barnes, et al. (2006). "Secular trends in incidence of atrial
fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the
projections for future prevalence." Circulation 114(2): 119-25.
Page 59
47
Mohr, F. W., J. F. Onnasch, et al. (1999). "The evolution of minimally invasive valve
surgery--2 year experience." Eur J Cardiothorac Surg 15(3): 233-8; discussion
238-9.
Muresian, H. (2008). "The clinical anatomy of the mitral valve." Clin Anat.
Parthenakis, F. I., A. P. Patrianakos, et al. (2007). "Atrial fibrillation is associated with
increased neurohumoral activation and reduced exercise tolerance in patients with
non-ischemic dilated cardiomyopathy." Int J Cardiol 118(2): 206-14.
Prasad, S. M., H. S. Maniar, et al. (2003). "The Cox maze III procedure for atrial
fibrillation: long-term efficacy in patients undergoing lone versus concomitant
procedures." J Thorac Cardiovasc Surg 126(6): 1822-8.
Reichenspurner, H., D. H. Boehm, et al. (2000). "Three-dimensional video and robot-
assisted port-access mitral valve operation." Ann Thorac Surg 69(4): 1176-81;
discussion 1181-2.
Savelieva, I. and J. Camm (2008). "Update on atrial fibrillation: part I." Clin Cardiol
31(2): 55-62.
Savelieva, I. and J. Camm (2008). "Update on atrial fibrillation: part II." Clin Cardiol
31(3): 102-8.
Starling, M. R. (1995). "Effects of valve surgery on left ventricular contractile function in
patients with long-term mitral regurgitation." Circulation 92(4): 811-8.
Tatooles, A. J., P. S. Pappas, et al. (2004). "Minimally invasive mitral valve repair using
the da Vinci robotic system." Ann Thorac Surg 77(6): 1978-82; discussion 1982-
4.
Page 60
48
Tribouilloy, C. M., M. Enriquez-Sarano, et al. (1999). "Impact of preoperative symptoms
on survival after surgical correction of organic mitral regurgitation: rationale for
optimizing surgical indications." Circulation 99(3): 400-5.
Ueshima, K., J. Myers, et al. (1993). "Hemodynamic determinants of exercise capacity in
chronic atrial fibrillation." Am Heart J 125(5 Pt 1): 1301-5.
Vanhees, L., D. Schepers, et al. (2000). "Exercise performance and training in cardiac
patients with atrial fibrillation." J Cardiopulm Rehabil 20(6): 346-52.
Vaziri, S. M., M. G. Larson, et al. (1994). "Echocardiographic predictors of nonrheumatic
atrial fibrillation. The Framingham Heart Study." Circulation 89(2): 724-30.
Wang, T. J., H. Parise, et al. (2004). "Obesity and the risk of new-onset atrial
fibrillation." Jama 292(20): 2471-7.
Wisenbaugh, T., J. F. Spann, et al. (1984). "Differences in myocardial performance and
load between patients with similar amounts of chronic aortic versus chronic mitral
regurgitation." J Am Coll Cardiol 3(4): 916-23.
Wolf, P. A., R. D. Abbott, et al. (1991). "Atrial fibrillation as an independent risk factor
for stroke: the Framingham Study." Stroke 22(8): 983-8.
Yuda, S., S. Nakatani, et al. (2004). "Mechanism of improvement in exercise capacity
after the maze procedure combined with mitral valve surgery." Heart 90(1): 64-9.
Page 61
APPENDIX A:
UMCIRB APPROVAL
Page 63
APPENDIX B:
INFORMED CONSENT
Page 70
APPENDIX C:
ACTIVITY QUESTIONNAIRE
Page 81
APPENDIX D:
TESTING PROTOCOLS
Page 85
APPENDIX E:
PASE SCORING FORM