BRAIN AND COGNITION 2, 205-223 (1983) Acalculia: Historical Development and Current Significance FRANCOIS BOLLER University of Pittsburgh AND JORDAN GRAFMAN University of Wisconsin Acalculia is a loss of calculating abilities occurring as a result of cerebral damage. This paper reviews the development of the notion of acalculia from an expected concomitant of aphasia or dementia to that of a sometimes autonomous disorder. Current evidence indicates that acalculia tends to occur particularly in lesions of the left posterior hemispheric areas. The ability to calculate is one of the oldest achievements of the human race. It has been said that “when a society has possessions in greater number that it can use immediately, it needs numerals” (Childe, 1973). One can give many examples of great mathematical achievements in the antiquity. For instance, it has been suggested that the stone blocks of many circles found in the British Isles, particularly those of Stonehenge (Fig. 1) erected around 1700 B.C. were used as “neolithic computers” to predict eclipses and other astronomical events thus requiring some form of arithmetic abilities (Hawkins, 1966). Some Greek philosophers attached great importance to calculation, paramount among them was Pythagoras (sixth century B.C.) who considered numbers the ruling entity of the universe. Figure 2 illustrates one instance of the Pythagorean description of reality in terms of arithmetical relationships; in this case it is applied to harmony and music. Quite independently the ancient Mayas developed a sophisticated cal- culation system (Fig. 3) which allowed them to conceive a calendar This research project was supported in part by funds of the Research and Development Service of the Veterans Administration and by a National Institutes of Health (National Institute of Aging) Program Grant PO1 AG-0370501. Send correspondence to Francois Boiler, M.D., Ph.D., Department of Neurology, University of Pittsburgh, 322 Scaife Hall, Pittsburgh, PA 15261. 205 0278-2626183 $3.00 Copyright 0 1983 by Academic Press, Inc. All rights of reproduction in any form reserved.
Transcript
BRAIN AND COGNITION 2, 205-223 (1983)
Acalculia: Historical Development and Current Significance
FRANCOIS BOLLER
University of Pittsburgh
AND
JORDAN GRAFMAN
University of Wisconsin
Acalculia is a loss of calculating abilities occurring as a result of cerebral damage. This paper reviews the development of the notion of acalculia from an expected concomitant of aphasia or dementia to that of a sometimes autonomous disorder. Current evidence indicates that acalculia tends to occur particularly in lesions of the left posterior hemispheric areas.
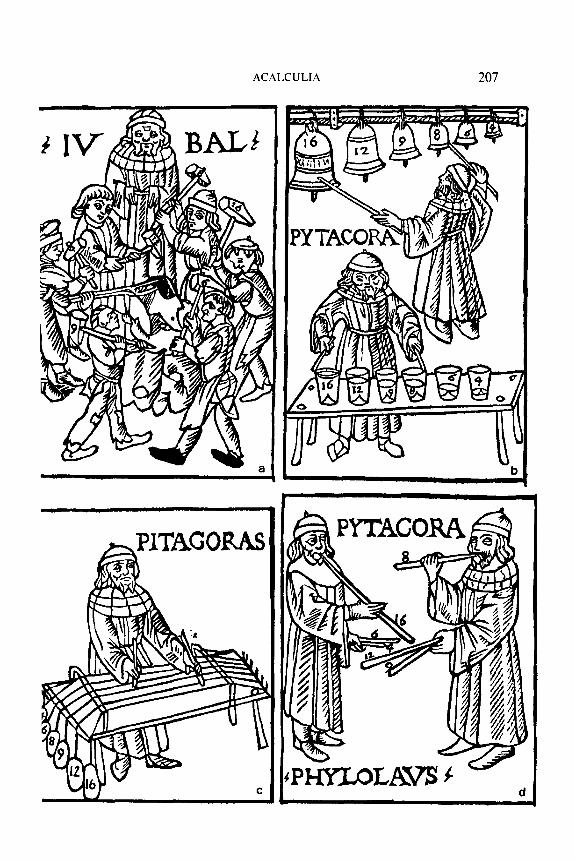
The ability to calculate is one of the oldest achievements of the human race. It has been said that “when a society has possessions in greater number that it can use immediately, it needs numerals” (Childe, 1973). One can give many examples of great mathematical achievements in the antiquity. For instance, it has been suggested that the stone blocks of many circles found in the British Isles, particularly those of Stonehenge (Fig. 1) erected around 1700 B.C. were used as “neolithic computers” to predict eclipses and other astronomical events thus requiring some form of arithmetic abilities (Hawkins, 1966). Some Greek philosophers attached great importance to calculation, paramount among them was Pythagoras (sixth century B.C.) who considered numbers the ruling entity of the universe. Figure 2 illustrates one instance of the Pythagorean description of reality in terms of arithmetical relationships; in this case it is applied to harmony and music.
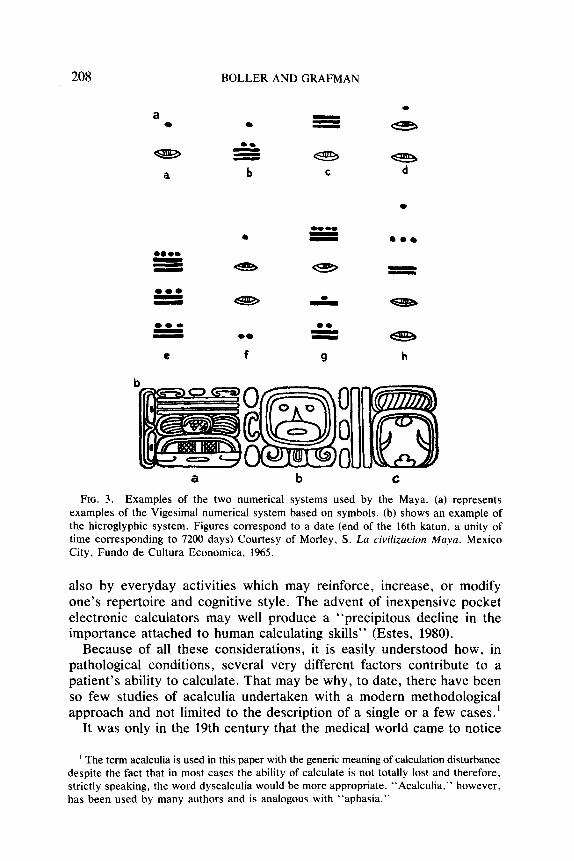
Quite independently the ancient Mayas developed a sophisticated cal- culation system (Fig. 3) which allowed them to conceive a calendar
This research project was supported in part by funds of the Research and Development Service of the Veterans Administration and by a National Institutes of Health (National Institute of Aging) Program Grant PO1 AG-0370501. Send correspondence to Francois Boiler, M.D., Ph.D., Department of Neurology, University of Pittsburgh, 322 Scaife Hall, Pittsburgh, PA 15261.
205 0278-2626183 $3.00
Copyright 0 1983 by Academic Press, Inc. All rights of reproduction in any form reserved.
206 BOLLER AND GRAFMAN
FIG. 1. Stone circle of Stonehenge in Great Britain. It has been argued that the disposition of the stones allowed precise prediction of such astronomic events as eclipses and that therefore Stonehenge represents a neolithic computer. (Courtesy of Burl, A., The Stone Circles of the British Isles. New Haven: Yale Univ. Press, 1976, by permission.)
system slightly more exact than the Julian calendar used by the Western Europeans at the time of the “discovery” of Yucatan (Morley, 1965). Despite those remarkable achievements, it would have been totally un- thinkable to test the arithmetic ability of an average population sample in the past because until fairly recently the ability to calculate remained a luxury monopolized by a restricted elite of highly educated persons and by the merchants. In some “primitive” languages, there are no words for numbers and the only way to convey some meaning of number is the use of singular, dual, and two plurals-one for few and one for many (e.g., Strehlow, 1942, 1943). Even now, it has been argued, every person has his own “arithmetic bag” (Poppelreuter, 1917), the content of which is influenced not only by hereditary abilities and cultural background but
FIG. 2. An early Renaissance illustration of the relationship between numbers and music. In the upper left comer (a) Jubal discovers the numerical ratios between the notes of the musical scale by visiting a balcksmith’s shop. Note that the hammers are weighted by presumably appropriate whole numbers. In the upper right comer (b) Pythagoras verifies these ratios by using a set of bells and again by using glasses filled with different amounts of water. In the lower left comer (c) Pythagoras confirms these numbers by using lengths of gut which are weighted to produce varying degrees of tension. In the lower right corner (d) Pythagoras and Philolaus, Pythagoras’ most famous disciple, repeat the experiment using pipes of varying length. (Originally appeared in Theorica musice by Franchino Gafori, Milano, 1492. Reproduced from Heminger, S. K., Torches of sweet harmony San Marino, CA: The Huntington Library, 1974, with permission from the publisher.)
ACALCULIA 207
208
a
-
h
a b C
FIG. 3. Examples of the two numerical systems used by the Maya. (a) represents examples of the Vigesimal numerical system based on symbols. (b) shows an example of the hieroglyphic system. Figures correspond to a date (end of the 16th katun, a unity of time corresponding to 7200 days) Courtesy of Morley, S. La civilization Maya. Mexico City, Fundo de Cultura Economica, 1965.
also by everyday activities which may reinforce, increase, or modify one’s repertoire and cognitive style. The advent of inexpensive pocket electronic calculators may well produce a “precipitous decline in the importance attached to human calculating skills” (Estes, 1980).
Because of all these considerations, it is easily understood how, in pathological conditions, several very different factors contribute to a patient’s ability to calculate. That may be why, to date, there have been so few studies of acalculia undertaken with a modern methodological approach and not limited to the description of a single or a few cases.’
It was only in the 19th century that the medical world came to notice
’ The term acalculia is used in this paper with the generic meaning of calculation disturbance despite the fact that in most cases the ability of calculate is not totally lost and therefore, strictly speaking, the word dyscalculia would be more appropriate. “Acalculia,” however, has been used by many authors and is analogous with “aphasia.”
ACALCULIA 209
impairment of higher cortical functions accompanying lesions of the cerebral hemispheres as a frequent phenomenon and as a field of study. The first to be studied was, of course, loss of language abilities (Broca, 1861). In the last decades of the 19th century, several workers interested in aphasia (e.g., Bastian, 1898) noticed that some patients had lost the ability to read and write both numbers and words, and had a severe impairment of their ability to calculate. But these deficiencies were interpreted only as an aspect of the symptom complex of aphasia. This conception cul- minated in the statement by Pierre Marie (1906) that all aphasics, like his famous cook, tend to be demented. The implication could well be drawn that an impairment or complete loss of calculation abilities is found as a normal accompaniement of aphasia.* Marie’s extremist view had many repercussions, one of which was to trigger an uproar of opposition which soon made the pendulum swing to the opposite side, culminating in the work of the Swedish neurologist Henschen (1919, 1920).
Before Henschen, several papers had described cases of acalculia. Lewandowsky and Stadelman (1908) may have been the first to report an acquired calculation disorder out of proportion with other cognitive processes. The patient was a 27-year-old shipping clerk who used to make extensive use of calculations in his daily activities. A hematoma (possibly due to an arteriovenous malformation that had bled) had been removed from his left occipital lobe. Following the operation the patient had a right homonymous hemianopsia and a short-lasting right facial weakness. He was alert, and his oral output was normal with “no anomia but increased latency in finding words.” His comprehension, repetition, and reading were normal but he had difficulty writing words spelled out loud.
The patient could read and write numbers and could use numbers, for example, to quote a price or give a date. The most striking finding on examination was that he had almost completely lost his ability to perform oral arithmetic operations such as 4 + 7 or 11 - 7; he could only do the easiest of multiplication but no division.
After noticing that their patient appeared to have normal intelligence, Lewandowsky and Stadelman point out that these calculation difficulties were probably independent from aphasia and from a disorder of inner language and/or of intelligence and were probably due to a disorder of the optic representation of numbers, “even though the patient would not admit that.”
Other cases of acquired calculation disorders were reported, before
’ Marie (1908) later denied having taken this position (“I have taken great care to declare that the aphasic disorders are not in the nature of a dementia”). Most of his contemporaries, however, interpreted him otherwise. For example, Lewandowsky and Stadelman (1908) attribute to Marie the view that “aphasia is a disorder of intelligence” and that therefore aphasic patients “usually cannot calculate and at best are always quite impaired” (p. 253).
210 BOLLER AND GRAFMAN
Henschen, by Poppelreuter (1917) Sittig (1917), and Peritz (1918). Most of these patients showed unilateral lesions located in the left retrorolandic area. Some of the cases in these series had bilateral occipital lesions. The ability to read is mentioned in 11 patients: of those, 9 were found to be alexic. Peritz specifically points to the left angular gyrus as the “calculation center”; he also states categorically that following lesions of the right hemisphere, the ability to calculate remains intact.
In Henschen’s (Fig. 4) monumental “Clinical and Anatomical Contri- butions to the Pathology of the Brain,” we find, in the fifth of eighth volumes (1920), the first systematic and complete study of the various aspects of calculation disturbances. Henschen postulated specific cortical centers for:
(a) pronunciation of numbers (left F3); (b) reading numbers (angular gyrus and fissura interparietalis); and (c) writing numbers (angular gyrus). No mention is made of the hemispheric side of the lesion for the latter
two functions. Acalculia (the word in this context is found here for the first time) is clearly related, according to him, to inability to copy (“Ako- pie”) and to agraphia for numbers. In Henschen’s opinion, this shows the great significance of the left angular gyrus. No relation is found, on the other hand, with the different types of aphasia, word blindness, word deafness, etc.
FIG. 4. Portrait of Henschen From Haymaker, W., and Schiller, F. (Eds.) The founders ofnewology Courtesy of Charles C. Thomas, Publisher, Springfield, IL: 2nd Ed., 1970.
ACALCULIA 211
Henschen is a typical example of those referred to by Sir Russel Brain (1961) as “ndive psychoanatomists”; the methods or which his conclusions are based are rather crude. That not withstanding, several points mentioned in his work are worth emphasizing. Henschen recognized that acalculia is somehow related to, but independent from aphasia; he also introduced the idea that agraphia and acalculia are associated in lesions of the left angular gyrus. As we shall see, some of his results will be confirmed by modern researchers like Hecaen and his colleagues.
In his book on aphasia, Henry Head (1962) refers to numbers and calculation only in passing. He correlated his four types of aphasia (verbal, nominal, syntactic, and semantic) with the way patients pronounce and understand digits and numbers and did not attribute specific significance to numbers in the general picture of verbal auditory tasks. As far as calculation is concerned, he states that in general it is impossible to infer the faulty mechanism which produces a wrong result. Testing calculation is therefore useless to diagnose a particular type of aphasic disturbance in a patient. In addition, calculation is highly influenced by intellectual factors.
Probably the most important among the early contributions to the problem of acalculia is that of Hans Berger, the discoverer of the EEG (Fig. 5). He (1926) pointed out the existence of two forms of acaculia. Secondary acalculia appears in patients who have an impairment of at- tention, a loss of immediate or delayed memory (as is typically the case
FIG. 5. Portrait of Hans Berger From Haymaker, W., and Schiller, F. (Eds.), The founders of neurology Courtesy of Charles C. Thomas, Publisher, Springfield, IL. 2nd Ed., 1970.
212 BOLLERANDGRAFMAN
in tumors) or a language disturbance including aphasia, alexia, and agraphia for numbers. There is also a primary or “pure” acalculia which is not clearly related to other cerebral disturbances. Berger describes 3 such cases (out of 18 reported): 2 had left occipital lesions and the third had a left temporal lesion. In all three cases, the angular gyrus was ma- croscopically and microscopically intact.
Further points of Berger’s paper are worth mentioning: (1) Rauschburg (1916) held that in children every calculation is an active act of thinking (Denkakte). Such a conclusion was reached after Rauschburg had dem- onstrated that, “in children, more and more difficult (or less simple) arithmetic problems would take more and more time for their solution” (e.g., 4 + 5 would be solved in a longer time than 4 + 1). Berger shows that for adults his principle is not true because of automatisms learned at school or in everyday life.
(2) The idea that general intelligence and logical functions on one hand and calculation ability on the other hand go puri passu may be true in the normal development and learning of calculation, however, it is con- tradicted by the unusual arithmetic ability of some mentally defective idiot savants and by the intact logical functions and severe impairment of calculation of some brain-damaged patients.
It is obvious to us, nowadays, that acalculias may be classified in different types according to their pathogenesis: most authors have, of course, realized that; nevertheless some authors (e.g., Peritz, 1918; Krapf, 1937, and in a sense Cohn, 1961, among others) have considered only their own pathogenetic theory and lumped together all acalculic defects into the same bag. On the other hand, more eclectic classifications of acalculia have also been proposed: an example can be found in an early paper of Goldstein (1919). He distinguishes two mechanisms liable to produce acalculia:
(a) An intellectual factor-which does not necessarily imply impairment of general intelligence-rather failure to understand the meaning of numbers and operations. This is associated with lesions of the “central part of the brain.” It is considered an impairment of abstraction.
(b) Mechanical factors which he unifies 30 years later under the name of learned patterns. They may be visual or motor, occipital or frontal, and may or may not produce a disturbance in calculation according to how the single patient was accustomed to calculating.
McDonald Critchley (1953) finds that impaired powers of calculation may be encountered in lesions of the right, the left, or both hemispheres. Deficits are seen more often, however, when the dominant hemisphere is affected. The lesions can be frontal, parietal, or occipital. When the lesion involves the dominant parietal lobe, some specific and recognizable features may be seen. The factors involved may be: ideational (loss of
ACALCULIA 213
the meaning of numbers), verbal (numbers may pop up inappropriately), and constructional factors.
Before coming to the review of what is perhaps the most important contribution to acalculia to date, that of Hecaen and collaborators, a brief mention should be made of authors who have put forward some interesting theory or ideas of their own:
A case report by Singer and Low (1933) is particularly interesting because of the imaginative and numerous manners in which the authors tested acalculia. Their patient was a 44-year-old male who became acalculic following accidental CO poisoning. He had some anomia, could read well (with few mistakes) and repeated well. He also disclosed some right heminattention. He was unable to do all but the simplest of mental arithmetic, made errors in counting unless objects were arranged in con- tinuous series and had problems handling any task that involved numbers. The patient also had a severe constructional apraxia. In the absence of an anatomical localization, Singer and Low concluded that “some sort of spatial element is a conspicuous factor in determining the acalculia defect.”
Karl Leonhard (1939, 1979) put particularly strong emphasis on the fact that different people follow quite different methods for calculation. Some people perform elementary calculation “automatically,” i.e., from the sound of numbers. These people will have dyscalculia following lesions of the “auditory sphere.” Other people “write in their mind” the figures involved in calculations and in these cases, dyscalculia will be associated with alexia and agraphia. Finally, a third group of persons “shape in their minds diagrams by which they carry out their calculations. In cases of constructional apraxia they are no longer able to shape these diagrams and acalculia follows.” This latter view is reminiscent of Galton’s concept of number-form (Galton, 1880; 1883) and a case of acquired disturbance in number-form has been reported by Spalding and Zangwill (1950). Others, however, (e.g., Oswald, 1960) have specifically stated that subjects with that kind of visual imaging do not use number-forms while performing calculations.
Krapf (1937) castigates other authors for their disregard of forms of acalculia which do not fit into their theory. He is referring particularly to authors who have emphasized the importance of sensory and occipital elements; but then he concentrates almost exclusively on parietal forms (“because they are more interesting from my point of view”). He em- phasizes the importance of the motor-sensory elements of calculation. This is suggested by the origin of the word itself (calculation derives from the Latin word calculus = pebble or stone), that implies the use of pebbles, by the tendency of many to use fingers etc. He divided the parietal acalculias into two forms:
214 BOLLERANDGRAFMAN
(a) Ideokinetic form: there is failure to calculate even though he knows what he is supposed to do. In Krapf s words, the patient understands the meaning of the calculating “blueprint” (Rechnungsentwur- but is unable to transform it into reality.
(b) Constructive form: a disturbance in spatial Gestalt with numbers. Krapf’s paper makes no mention of hemispheric side of lesion.
Views somewhat similar to those of Krapf have been more recently expressed by Cohn (1961). He studied 40 acalculic patients and found they made two types of errors: (1) due to impairment of what he calls memory (which includes the cases in which the symbols are not recognized), (2) due to “order disturbances”: these are seen in occipital lesions in nearly half of his series when the lesion is on the right side. “This is similar,” he said, “to the construction form of Krapf.” But he states “it is unnecessary to postulate a complex visual practic integrity disturbance to account for the observations.”
There are several examples of general psychological and neuropsy- chological concepts into which acalculia has been “integrated.” For example, the Gestaltists, such as Wertheimer (1912) considered acalculia an inability to distinguish a part from a whole. Another general conception is that of Gerstmann and his followers who introduced the concept of “body schema” to explain acalculia and the other elements of Gerstmann’s tetrad (finger agnosia, agraphia, and right-left disorientation). We won’t spend much time on this question which in itself should be the subject of another discussion. There is not much emphasis on acalculia per se in the many papers relating to the Gerstmann syndrome including recent ones against (Benton, 1961; Heimburger, De Myer, & Reitan, 1964; Poeck & Orgass, 1966, etc.) and in favor (e.g., Strub & Geschwind, 1974) of the autonomous existence of the syndrome. It is notable that among the symptoms thought to be part of Gersmann’s syndrome, acalculia was the last to be included and is certainly the one for which the relation with the concept of “body schema” appears least obvious.
In 1961, Hecaen, Angelergues, and Houillier published in the Revue Neurologique, a study of 183 patients who became acalculic following retrorolandic lesions. They classified their patients into three groups:
(1) Digit alexia and agraphia with or without alexia and agraphia. In this group, arithmetic operations are affected by the impaired writing and reading of numbers but there seems to be no other disorder. An example of agraphic acalculia is shown in Fig. 6.
(2) Spatial dyscalculia: Disorders of spatial organization for numbers. Patients in this group do not respect the rules for setting written digits in their proper order and position reminding one of Marie’s “planoto- pokinesia”; they may also have spatial neglect and spatial number inversions.
ACALCULIA 215
FIG. 6. Example of agraphia for numbers. The patient demonstrates his knowledge of the “rules” of calculation by setting the problem correctly even though, because of his agraphia, he is unable to write down numbers other than 0. Courtesy of HCcaen, Angelergues, & Houillier, Revue Neurologique 105, S-103, 1961, by permission.
(3) Disorders of the “conduct” of arithmetic operations, i.e., acalculia not clearly related to one of the impairments listed in the previous two groups. This group is said to have “anarithmetia.”
They find in their material 63 cases belonging to Group 1 (acalculia related to alexia or agraphia for numbers), 48 cases in Group 2 (spatial acalculia) and 72 in Group 3 (anarithmetia).
In a paper published the same year, Hecaen and Angelergues (1961) point out that alexia for digits and numbers is found in 84% of patients with left temporo-occipital lesions but also in 8% of right hemisphere lesions. Spatial dyscalculia is rarely found in left hemispheric lesions (4.3% of left temporal and 6.7% of left parietal lesions) but is found in 16.3% of right parietal lobe lesions and 57% of right parieto-temporo- occipital lesions, a result attributed to some “prevalent” role of parietal lobe lesions associated with that of mass effect. Finally anarithmetia is found in 53 to 62% of left hemisphere lesions but also in 6 to 15% of right hemisphere lesions. It must be pointed out that these two articles refer to acalculia found in patients with retrorolandic lesions. In a later article that presumably refers to all hemispheric lesions, Hecaen (1962) gives somehow different percentages but the fundamental fact remains that alexia and agraphia for digits is seen predominantly (but not exclusively) in left hemispheric lesions. The same is true in reverse for spatial dyscalculia which is seen mainly following right hemisphere lesions while anarithmetia is seen after lesions of either hemisphere but more often with left hem- ispheric damage. Incidentally, the 1962 article refers to “anarithmetria” instead of “anarithmetia” perhaps because of an error in translation: anarithmetia derives from arithmetic and etymologically has nothing to do with the metric system!
216 BOLLERANDGRAFMAN
The most important conclusions of Hecaen and his collaborators are the following:
(a) They confirmed the finding of Henschen that there is often a dis- sociation between language and calculation abilities.
(b) They found strong associations between alexia and agraphia for numbers and difficulty in calculation, including mental calculation.
(c) The area most frequently involved in unilateral hemispheric lesions is the parietal area.
(d) The general conclusion is that calculation is a specific function, with a high level of integration and with double hemispheric dominance.
It must be stressed that the papers by Hecaen and collaborators contain no description of methods and no precise criteria for the identification of, for example, spatial acalculia. Furthermore, there is little mention of the role played by age, education, and other factors that may have affected the premorbid calculation abilities of their patients. As pointed out by Benton (1966), this paper represents a stimulating starting point for prospective research in which an adequate technical procedure would allow a precise analysis of “various aspects of quantitative thinking and arithmetic performance.”
Barbizet, Bindefeld, Moaty, and LeGoff (1967) have studied the cal- culation ability of patients affected by severe aphasia. No detail is given on the rest of the neurological functions, but it is assumed that in all cases there was a “complete” destruction of the left hemisphere. No arithmetic operation, not even a simple addition or subtraction, was possible for any of those patients. Some, however, were able to show elementary use of the smaller numbers in tasks involving cross-motor transfer, for example, a visuo-motor task consisting of putting together on an abacus the number of counters corresponding to the number of tokens they are shown. Barbizet and his colleagues put forward the hypothesis that such “activity of elementary calculation is partially a function of the right hemisphere.”
A paper by Benson and Denckla (1969) describes two patients with clinical features of the Gerstmann’s syndrome. In both patients, the calculation disturbance appeared rather severe if only the verbal or graphic responses of the patient were taken into account. However, when presented with multiple choice answers, the patients demonstrated “intact knowledge of computational processes.” The calculation errors are, in other words, attributed to paraphasic substitutions. This report raises the methodological problem of ascertaining the very existence of calculation disturbances which might often be erroneously diagnosed, while the true defect is rather of an aphasic nature.
In a series of papers, Grewel(1952, 1962, 1969) has provided an interesting approach to the problem of acalculia. He points out that impairments of calculation may be considered the paradigm of semiotic disorders, since
ACALCULIA 217
the semiotic system involved in calculation is based on a symbolic system considerably stricter than other semiotic systems such as language.3 The semiotic system involved in calculation consists of numeration (repre- sentation of numeral quantities by words) and notation (representation by written signs). Our notation of numbers follows the Hindu system which proceeds by ones, tens, tens of tens, etc. Essential features of this system are: (1) the limitation of the number of different symbols to ten, however large the number in question; (2) the use of the zero to indicate the absence of power; (3) the principle of local value by which the value of a digit changes according to its position within a number notation. In his opinion, the disturbances we can deduce theoretically from the semantics of calculation are repeatedly seen in patients with acalculia. Following Berger, he distinguishes a primary and a secondary acalculia. He further divides primary acalculia into
-Asymbolic acalculia: inability to differentiate between or to manipulate some of the usual arithmetical symbols (digits or signs).
-Asyntactic acalculia: breakdown of the intricate semiotic-syntactic system involved in calculation. Within this group he identifies specific disorders such as a disorder of “plural digit notation” (e.g., failure to conceive the complex number notation as a unity; deterioration of the handling of the 0 in its different functions, etc.) and a disorder of written arithmetic (e.g., inability to handle a multiple-digit notation; starting additional, subtractions, or multiplications on the left side etc.)
Secondary acalculia may be due to aphasia, disorders of memory, or perseveration.
In terms of localization, Grewel mentions a frontal acalcufia in which there is allegedly a more severe disturbance in dealing with abstract than with concrete numbers. He does not think that this really happens (“it is an open question whether any number is really abstract”). He adds that in frontal lesions the intensity of acalculia parallels the general reduction of the level of productive thinking and of initiative.
Temporal acalculia is supposedly associated with a specific inability to identify sounds/numbers. This is based on the concept of a separate “auditory number centre” (Henschen, 1927), a notion that does not appear acceptable today.
In occipital acalculia, there are specific differentiations in the handling of digit symbols as well as impaired visual retention and visualization.
Grewel considers that “from a psychological point of view,” parietd acalculia is the most interesting type of acalculia, one in which spatial functions are particularly important. The importance of spatial factors in acalculia had been stressed by “many other authors.” It is interesting
3 Crewel (1952) points out that other semiotic systems include, in addition to language, maps, Morse and Braille signs, card games, chess, signal systems like semaphores or flags, etc.
218 BOLLERANDGRAFMAN
to note that many of the references that he includes in support of this point (e.g., Ehrenwald, 1931; Scheller & Seidmann, 1931; Wagner, 1932;
Conrad, 1932; Kroll & Stolban, 1933; Janota, 1938, etc.) are to authors who have written on constructional apraxia and who have remarked, in the course of their case descriptions, that written calculations are also impaired in patients with severe visuo-spatial disorders.
Grewel does not give any detail about the basis for his conclusions which appear to have been derived mainly from the literature and from clinical cases encountered here and there rather than from a systematic approach to the problem. Nevertheless, his analysis is an interesting attempt to correlate calculation disorders to the processes involved in normal calculation.
Collingnon, Leclercq, and Mahy have recently (1977) published the results of a systematic research on acalculia. Twenty-six hemisphere-damaged patients were given a series of tasks derived from the battery in use at Dr. Hecaen’s laboratory. (See Boller and Hecaen, 1979, for a complete description of the battery.) The calculation tasks included:
(1) reading and writing numbers, operation symbols and roman numerals; (2) verbal description of the shape of numbers; (3) mental and written arithmetic; (4) problems requiring use of the metric system; (5) memory for numbers and for short arithmetic opeations; (6) mental calculations involving concrete calculations, time and spatial
measurements; (7) knowledge of the concept of numbers: the longest of two numbers,
the longest of two fractions, and the meaning of the position of the digits in a number;
(8) estimation of size and amount by sight and by touch; (9) mental estimation of the size, quantity, speed, and weight of objects
named by the examiner; (10) reproduction of rhythmic sequences. They found that acalculia was present in a slightly larger percentage
of left than of right hemisphere-damaged patients (34.6 and 29.5% re- spectively) and conclude that calculation abilities rely on a series of factors that include language, body schema, finger gnosis, spatial factors, and visuo-constructive abilities. Acalculia can be divided into three forms: (1) acalculia secondary to the impairment of one specific instrument (e.g., aphasia); (2) acalculia secondary to the impairment of several instruments (e.g., aphasia, apraxia, and spatial disorders in various combinations); (3) acalculia secondary to impairment of intelligence.
It is to be noted that the authors present the percentages of various groups that failed at specific tests but that they do not tell us how many (if any) subjects performed correctly at all the tests. Since they do not seem to have included a control group, their notion of acalculia remains
ACALCLJLIA 219
poorly defined. Finally, one must keep into account that the majority (19 out of 26 patients) of their cases had tumors and that for some of them at least, increased intracranial pressure may also have played a role. Despite these methological problems, this is an important study since it is one of the very few prospective research on acalculia.
The conclusion of Collignon et al. (1977) that the majority of acalculic patients have a left hemisphere lesion is certainly in keeping with the findings of the majority of authors who have studied the problem including a research of McGee and Aten (1976) that has carefully analyzed the relationship between language and calculation disorders in aphasia. In a recent report, Leleux, Kaiser, and Lebrun (1979) have described in detail the case of a 40-year-old right-handed teacher of mathematics who became dyscalculic following removal of a right fronto-parietal hematoma. Their patient’s difficulties were certainly not limited to spatial disorders but included many aspects that would clearly be ascribed to anarithmetia. Symptoms similar to those of Leleux and colleagues’ patient have been well described in patients with left hemisphere lesions (e.g., Benson and Weir, 1972). This case brings to mind the problem discussed by Leonhard (1939, 1979): different people may use completely different systems in calculation, and they may perhaps involve different anatomical systems.
As can be seen from this review, many authors have been interested in the phenomenon of acalculia. From the earlier reports based simply on the description of isolated cases, one passes to the classification work of Berger and the clinical pathological correlations of Henschen. Later several authors put forward their own explanation or attempt of explanation to describe the mechanisms which produce acalculia. All too often, this is just an application to acalculia of an author’s general theory on aphasia and related disturbances. A recent review (Levin, 1979), correctly con- cluded that further studies are necessary to elucidate the mechanisms and regional localization of anarithmetia and (we might add) other cal- culation disorders.
An attempt to clarify some of the problems that, as pointed out in this review, have remained unsolved up to the present, is a recent prospective study of patients with calctdation disorders following focal hemispheric damage (Grafman, Passafiume, Faglioni and Boller, 1982). Following Hecaen and collaborators’ suggestion that hemisphere-damaged patients with calculation disorders can be subdivided into three groups (agraphia or alexia for numbers, spatial acalculia and anarithmetia), we wanted to evaluate further the role played by spatial disorders and by anarithmetia in subjects with impaired calculation abilities. We studied 102 subjects with demonstrated ability to read and write numbers and gave them a written calculation task. In addition, the Token Test, the Crosses Test (DeRenzi and Faglioni, 1%7), a test of constructional apraxia and Raven’s Progressive Matrices were administered to all subjects. The subjects
220 BOLLERANDGRAFMAN
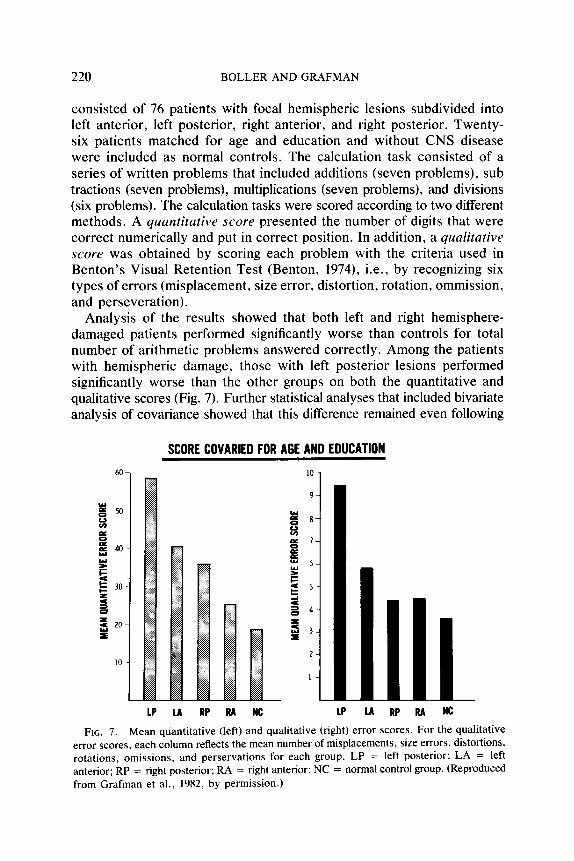
consisted of 76 patients with focal hemispheric lesions subdivided into left anterior, left posterior, right anterior, and right posterior. Twenty- six patients matched for age and education and without CNS disease were included as normal controls. The calculation task consisted of a series of written problems that included additions (seven problems), sub tractions (seven problems), multiplications (seven problems), and divisions (six problems). The calculation tasks were scored according to two different methods. A quantitative Score presented the number of digits that were correct numerically and put in correct position. In addition, a qualitative score was obtained by scoring each problem with the criteria used in Benton’s Visual Retention Test (Benton, 1974), i.e., by recognizing six types of errors (misplacement, size error, distortion, rotation, ommission, and perseveration).
Analysis of the results showed that both left and right hemisphere- damaged patients performed significantly worse than controls for total number of arithmetic problems answered correctly. Among the patients with hemispheric damage, those with left posterior lesions performed significantly worse than the other groups on both the quantitative and qualitative scores (Fig. 7). Further statistical analyses that included bivariate analysis of covariance showed that this difference remained even following
SCORE COVARIED FOR AGE AND EDUCATION
LP u RP RR WC LP LA RP RA NC
FIG. 7. Mean quantitative (left) and qualitative (right) error scores. For the qualitative error scores, each column reflects the mean number of misplacements, size errors, distortions, rotations, omissions, and perservations for each group. LP = left posterior; LA = left anterior; RP = right posterior; RA = right anterior; NC = normal control group. (Reproduced from Grafman et al., 1982, by permission.)
ACALCULIA 221
correction of the scores by the result of the Token Test, the visual-spatial tests, and Raven’s Progressive Matrices.
These results together with others reviewed here and in another recent review (Boller & Grafman, in press) strongly suggest that acalculia can indeed occur independently of dementia, aphasia, or constructional apraxia. This anarithmetia (Hecaen et al., 1961) or primary acalculia (Berger, 1926) appears particularly following left posterior lesions. Whether the dominant angular gyrus does indeed play the important role postulated by Peritz, Henschen, and Gerstmann remains to be determined by future research.
REFERENCES
Barbizet, J., Bindefeld, N., Moaty F., & Le Goff P. 1967. Persistances de possibilitts de calcul elementaire au tours des aphasies massives. Revue Neurologique, 116, 170- 178.
Bastian, H. C., 1898. A treutise on aphusiu and orher speech defects. London: Lewis. Benson, D. F., & Denckla, M. B. 1969. Verbal paraphasia as a cause of calculation
disturbances. Archives of Neurology, 21, 96-102. Benson, D. F., & Weir W. F. 1972. Acalculia: Acquired anarithmetia. Correx, 8, 465-472. Benton, A. L. 1961. The fiction of the “Gerstmann syndrome” Journal of Neurology,
Neurosurgery and Psychiatry, 24, 176- 18 1. Benton, A. L. 1966. Prohlemi di neuropsicologia. Florence: Universitaria G. Barbera. Pp.
147-159. Berger, H. 1926. Ueber Rechenstorungen bei Herderkrankungen des Grosshirns. Arch&
fiir Psychiatric und Nervenkrankheiren. 78, 238-263. Boiler F, Grafman J. Acalculia. In P. J. Vinken, G. W. Bruyn, H. L. Klawans (Eds.),
Handbook of clinical neurology. 2nd Ed. Vol. 1. (Clinical Neuropsychology J. A. M. Frederiks Ed.) Amsterdam:iNorth-Holland. In press.
Boiler, F., & Hecaen, H. 1979. L’evaluation des fonctions neuropsychologiques: Examen standard de I’unite de recherches neuropsychologiques et neurolinguistiques (U. 111) I.N.S.E.R.M. Revue de Psychologie AppliquPe, 29, 247-266.
Brain, R. 1961. The neurology of language. Bruin, 84, 145-166. Broca, P. (1861) Perte de la Parole. Bulletin de /a ,Soci&t& d’ilnthropologie. 2, 219. Childe, V. G., The dawn of European rivilizarion London: 1973. Cohn. R. 1961. Dyscalculia. Archives of Neurology, 4, 301-307. Collingnon, R., Leclercq, C., & Mahy, J. 1977. Etude de la semiologie des troubles de
calcul observes au tours des lesions corticales. Actu Neurologicu Belgicu, 77, 257- 275.
Conrad, K. 1932. Versuch einer psychologischen Analyse des Parietalsyndroms. Monafschrifi fiir Psychiutrie und Neurologie, 84, 28-97.
Critchley, M. 19.53. The purietul lobes. New York: Hafner. De Renzi, E., & Faglioni, P. 1967. The relationship between visuo-spatial impairment and
constructional apraxia. Corfex. 3, 327-342. Ehrenwald, H. 1931. Stoning der Zeitauffassung. der raumlichen Orientierung, des Zeichnens
und des Rechnens bei einem Hirnverletzten. Zeirschrifz fiir die gesamte Neuro/ogie und Psychiatric, 132, 518-569.
Estes. W. K. 1980. Is human memory obsolete? Americun Scienrisr, 68, 62-69. Galton, F. 1880. Visualized numerals. Nature (London), 21, 252-256; 323; 494-495. Galton, F. 1883. Inquiries into humun ,fuculty and its development. New York: MacMillan
co. Pp. 114-145.
222 BOLLER AND GRAFMAN
Goldstein, K. 1919. Die Behanlung, Fursorg undBequtachtung der Hirnverletzten, Leipzig: Vogel.
Grafman, J., Passafiume, D., Faghoni, P., & Boiler, F. 1982. Calculation disturbances in adults with focal hemispheric damage. Cortex 18, 37-50.
Grewel, F. 1969. The acalculias. In: Handbook of clinical neurology. p. J. Vi&en and
G. W. Bruyn (Eds.) Amsterdam: North-Holland. Vol. 4, Pp. 181-196. Grewel, F. 1952. Acalculia. Brain, 75, 397-407. Grewel, F. 1962. Disorders in the use of semiotic systems. Logos, 5, 43-50. Hawkins, G. S. 1966. Stonehenge physics. Physics Today, 19, 38-42. Head. H. 1926. Aphasia and kindred disorders of speech. Cambridge University Press,
reprint edition. New York: Hafner, Vol. 1. Pp. 328-348. HCcaen, H. 1962. Clinical symptomatology in right and left hemispheric lesions. In: V. B.
Mountcastle (Ed.), Interhemispheric relations and cerebra/ dominance. Baltimore: Johns Hopkins Press. Chap. 10. Pp. 215-243.
HCcaen, H., & Angelergues, R. 1961. Etude anatomo-clinique de 280 cas de lesions retro- rolandiques unilaterales des hemispheres certbraux. Enc~phale, 6, 533-562.
HCcaen, H., Angelergues, R., & Houillier, S. 1961. Les varietes cliniques des acalculies au tours des lesions retrorolandiques: Approche statistique du probltme. Revue Neu- rologique, 105, 85-103.
Heimburger, R. F., De Myer, W. C., & Reitan, R. M. 1964. Implications of Gerstmann’s syndrome. Journal of Neurology, Neurosurgery and Psychiatry, 27, 52-57.
Henschen, S. E. 1919. Uber Sprach, Musik, und Rechenmechanismen und ihre Lokalisationen in Grosshirn. Zeitschrift fiir die gesamte Neurologie und Psychiatric, 52, 273-298.
Henschen, S. E. 1920. Klinische und anatomische Beitriige zu Pathologic des Gehirns. Stockholm: Nordiska Bokhandeln. Vol. 5.
Henschen, S. E. 1925. Clinical and anatomical contributions on brain pathology (translated by W. F. Schaller). A.M.A. Archives of Neurology and Psychiatry, 13, 226-249.
Henschen, S. E. 1926. On the function of the right hemisphere of the brain in relation to the left in speech, music and calculation. Brain, 49, 110-123.
Henschen, S. E. 1927. Zur Lokalisation der Rechenfunktionen. Archiv fir Psychiatric und Nervenkrankheiten, 79, 375-382.
Janota, 0. 1938. Sur l’apraxie constructive et sur les troubles apparentes de I’apperception et de I’expression des rapports spatiaux. Encdphale, 2, 173-211.
Krapf, E. 1937. Ueber Akalkulie. Sweizerische Archiv fiir Neurologie und Psychiatric, 39, 330-334.
Kroll, N., & Stolban, D. 1933. Was ist konstruktive Apraxie? Zeitschrift fiir die gesamte Neurologie und Psychiatric, 148, 142-158.
Leleux, C., Kaiser, G., & Lebrun, Y. 1979. Dyscalculia in a right-handed teacher of mathematics with right cerebral damage. In Y. Lebrun and R. Hoops (Eds.), Problems of Aphasia Lisse: Swets and Zeitlinger. Chap. 6. Pp. 141-158.
Leonhard, K. 1939. Die Bedeutung optisch-r&mlicher Vorstelhtngen fur das elementaire Rechnen. Zeitschrif fiir die gesamte Neurologie und Psychiatric, 164, 321-351.
Leonhard, K. 1979. Ideokinetic aphasia and related disorders. In Y. Lebrun and R. Hoops (Eds.), Probtems of Aphasia. Lisse: Swetz and Zeitlinger. Chap. I. Pp. l-77.
Levin, H. S. 1979. The acalculias. In K. M. Heilman and E. Valenstein (Eds.), Clinical Neuropsychology. New York: Oxford Univ. Press. Chap. 5. Pp. 128-140.
Lewandowsky, M., & Stadelmann, E. 1908. Ueber einen bemerkenswerten Fall von Hirn- bluntung und tiber Rechenstorungen bei Herderkrankung des Gehims. Journal fir
Psychologie und Neurologie, 11, 249-265. MC Gee, A., & Aten, J. L. 1976. An experimental approach to the assessment of dyscalculia
in aphasia. Paper read at the Annual Meeting of the Academy of Aphasia, Victoria, British Columbia, October 1975.
ACALCULIA 223
Marie, P. 1906. La troisieme circonvolution frontale gauche ne joue aucun role special dans la function du langage. Semaine MPdicale, May 23, reprinted in Marie P., 1926. Travaux et Mcfmoires, Tome 1, Paris: Masson. Pp. 3-30. For translation, see Cole M. F., & Cole M., 1971. Pierre Murie’s papers on speech disorders. New York: Hafner.
Marie, P. 1908. Discussion de la SociCtC de Neurologie. Revue Neurologique, 16, II, 1025- 1047.
Morley, S. G. 1965. La Civilization Maya. Mexico City: Fundo de Cultura Economica. 5th edition. Pp. 306-338 (in Spanish).
Oswald, T. 1960. Number-forms and kindred visual images. Journal of General Psychology, 63, 81-88.
Peritz, G. 1918. Zur Pathopsychologie des Rechnens. Deutsche Zeitschrif fiir Nerven- heilkunde, 61, 234-340.
Poeck, K., & Orgass B. 1966. Gerstmann’s syndrome and aphasia. Cortex, 2, 421-437.
Poppelreuter, W. 1917. Die Psychischen Schaedigungen durch Kopfschuss im Kriege 1914- 1916. Leipzig: Voss.
Rauschburg, P. 1916. Die Leseschwache und Rechenschwache der Schulkinder im Lichte des Experiments. Berlin: Julius Springer.
Scheller, H., & Seidemann, H. 1931. Zur Frage der optisch-raumlichen Agnosie. Monatschrif fir Psychiatric und Neurologie, 81, 97-188.
Singer, H. D., & Low, A. A. 1933. Acalculia (Henschen): A clinical study. Archives of Neurology and Psychiatry, 29, 476-498.
Sittig, 0. 1917. Uber Storungen des Ziffernschreibens bei Aphasischen. Zeitschrifr ,fiir
Pathopsychologie, 3, 298-306. Spalding, J. M. K., & Zangwill, 0. L. 19.50. Disturbance of number-form in a case of
brain injury. Journal of Neurology, Neurosurgery and Psychiatry, 13, 24-29. Strehlow, T. 1942, 1943. Aranda Phonetics and Grammar. Oceania, 13, 71-103, 177-200,
310-361; 14, 68-90, 59-181. Strub, R., & Geschwind, N. 1974. Gerstmann syndrome without aphasia. Cortex, 10, 378-
387. Wagner, W. 1932. Uber Raumstorung. Monatschrift fur Psychiatric und Neurologie, 84,
281-307. Wertheimer, M. 1912. Uber das Denken der Nattirvolker, Zahlen und Zahlgebilde. Zeitschrift