ACCURACY OF COMPUTER- AIDED IMPLANT PLACEMENT N. Van Assche, M. Vercruyssen, W. Coucke, W. Teughels, R. Jacobs and M. Quirynen Clin. Oral Implants Res. 23 (Suppl. 6), 2012, 112–123 AAMIR ZAHID GODIL FIRST YEAR P.G. DEPARTMENT OF PROSTHODONTICS M.A.R.D.C.
Transcript
ACCURACY OF COMPUTER-
AIDED IMPLANT PLACEMENT
N. Van Assche, M. Vercruyssen, W. Coucke,
W. Teughels, R. Jacobs and M. QuirynenClin. Oral Implants Res. 23 (Suppl. 6), 2012, 112–123
• ADVANTAGES AND DISADVANTAGES OF FLAPLESS GUIDED SURGERY
• CLINICAL CASE
• RESEARCHES AND REVIEWS
• CONCLUSION
• CRITIQUE
INTRODUCTION
GUIDED IMPLANT SURGERY• During the last decade, special attention was given to a “prosthesis
driven” implant placement, to optimize the aesthetic outcome of
the final restoration with optimal loading conditions and good
access for cleaning.
• Three-dimensional imaging (showing the alveolar bone in relation to
the ideal tooth position), obtainable with relative low radiation
dosages especially when CBCT are used (Loubele et al. 2009;
Pauwels et al. 2012) in combination with planning software opened
the possibility for preoperative planning and proper
communication among the patient, the surgeon and the
prosthodontist.
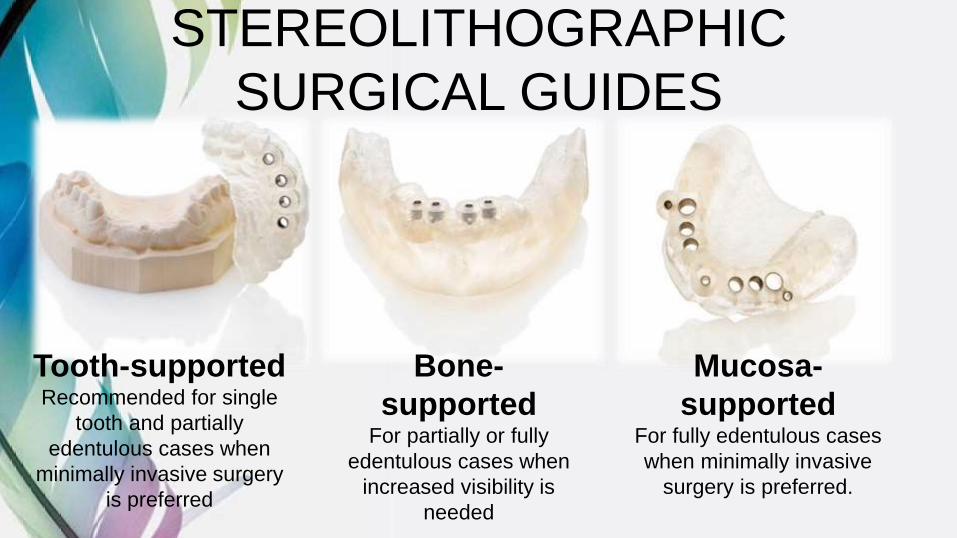
STEREOLITHOGRAPHIC
SURGICAL GUIDES
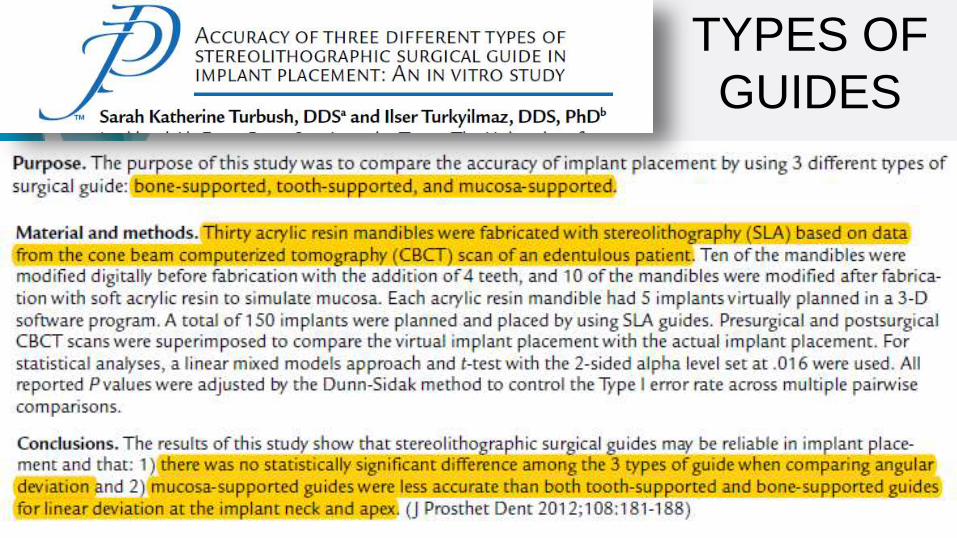
Tooth-supportedRecommended for single
tooth and partially
edentulous cases when
minimally invasive surgery
is preferred
Bone-
supportedFor partially or fully
edentulous cases when
increased visibility is
needed
Mucosa-
supportedFor fully edentulous cases
when minimally invasive
surgery is preferred.
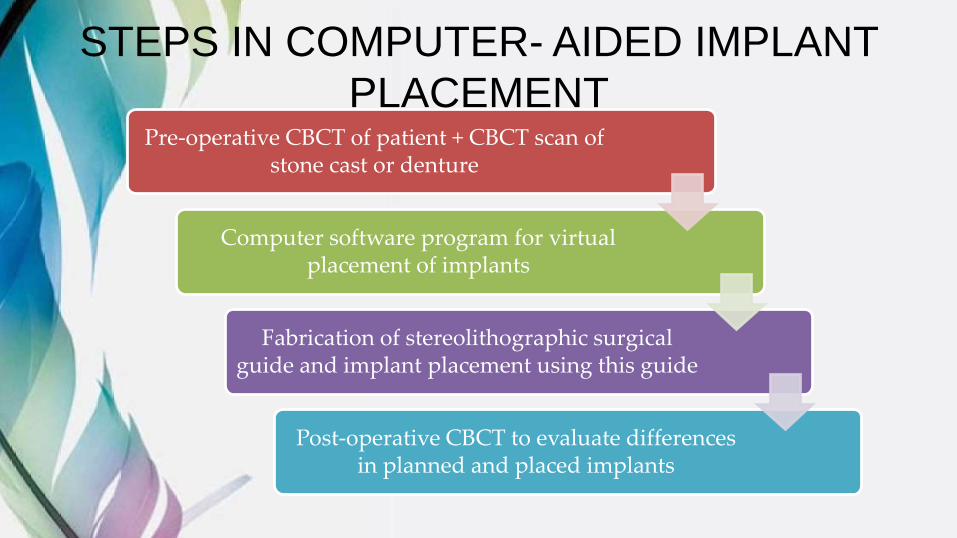
STEPS IN COMPUTER- AIDED IMPLANT
PLACEMENTPre-operative CBCT of patient + CBCT scan of
stone cast or denture
Computer software program for virtual placement of implants
Fabrication of stereolithographic surgical guide and implant placement using this guide
Post-operative CBCT to evaluate differences in planned and placed implants
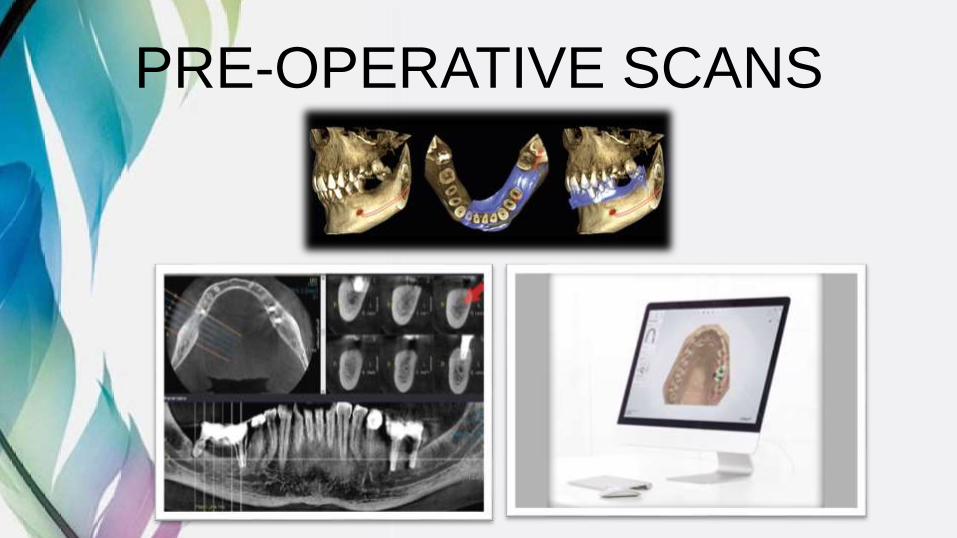
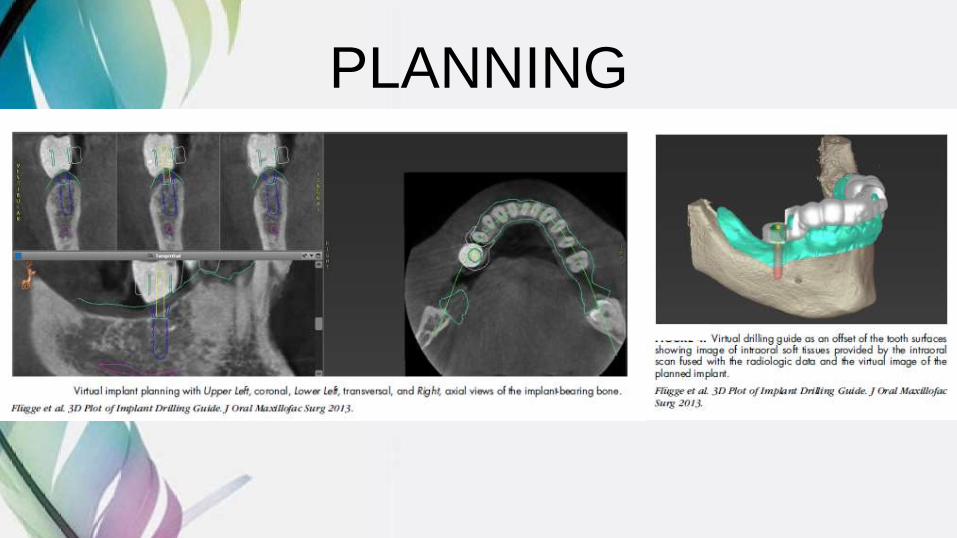
PRE-OPERATIVE SCANS
PLANNING
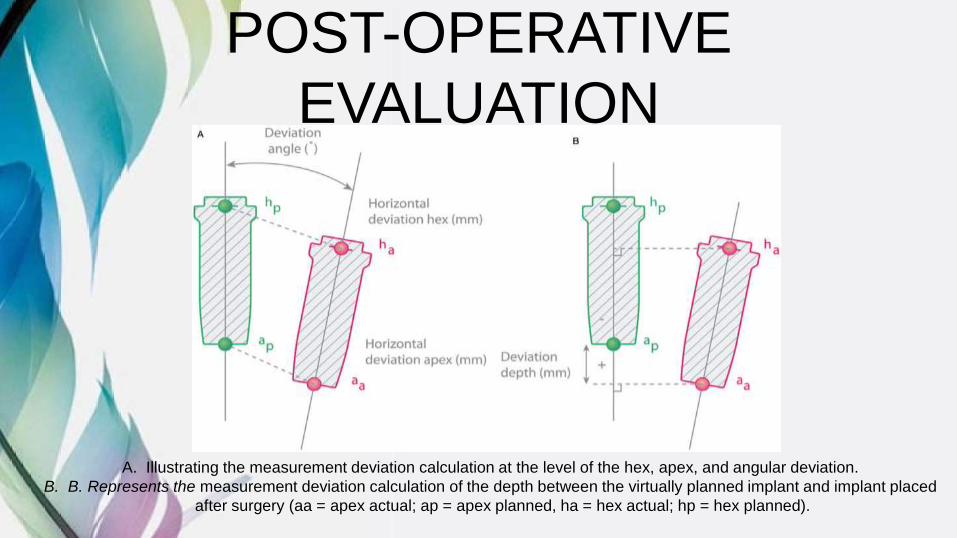
POST-OPERATIVE
EVALUATION
A. Illustrating the measurement deviation calculation at the level of the hex, apex, and angular deviation.
B. B. Represents the measurement deviation calculation of the depth between the virtually planned implant and implant placed
after surgery (aa = apex actual; ap = apex planned, ha = hex actual; hp = hex planned).
ADVANTAGES OF FLAPLESS
GUIDED SURGERY
Facilitated surgical
procedure
Reduced surgical
intervention time
Reduced postoperative complications
Treatment of medically
compromised
Avoiding bone grafting
procedures
Facilitated immediate
loading protocol
D'haese J, Van De Velde T, Komiyama AI, Hultin M, De Bruyn H. Accuracy and Complications
Using Computer‐Designed Stereolithographic Surgical Guides for Oral Rehabilitation by Means of
Dental Implants: A Review of the Literature. Clinical implant dentistry and related research. 2012
Jun 1;14(3):321-35.
DISADVANTAGES OF FLAPLESS
GUIDED SURGERYLack of visibility
and tactile control during surgical
procedure
Insufficient mouth opening
jeopardizes surgical procedure
Risk of damaging vital anatomical
structures
D'haese J, Van De Velde T, Komiyama AI, Hultin M, De Bruyn H. Accuracy and Complications
Using Computer‐Designed Stereolithographic Surgical Guides for Oral Rehabilitation by Means of
Dental Implants: A Review of the Literature. Clinical implant dentistry and related research. 2012
Jun 1;14(3):321-35.
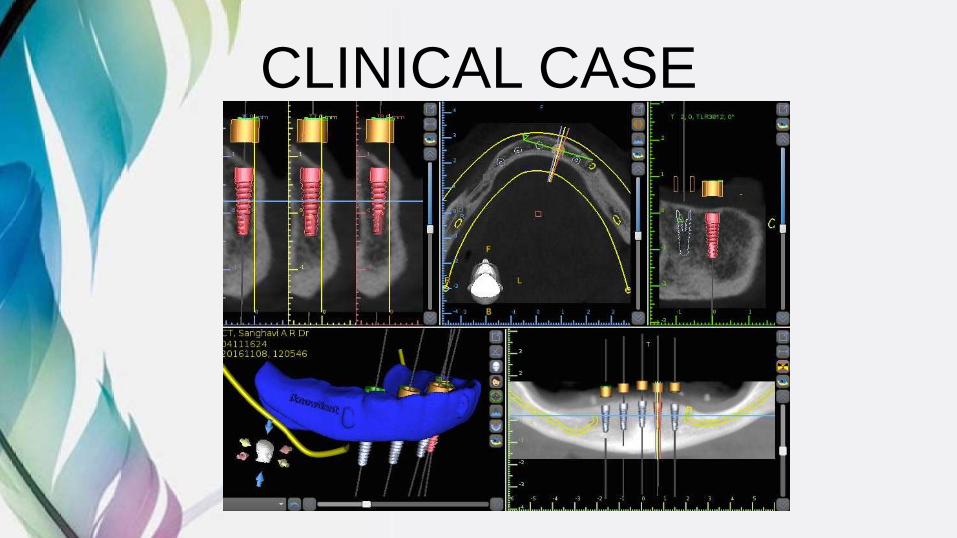
CLINICAL CASE
RESEARCHES AND
REVIEWSPAIN EXPERIENCED AND SURGICAL TRAUMA
FOR RESORBED RIDGES
DURATION OF TREATMENT AND COST-EFFECTIVENESS
COMPLICATIONS
ALL ON FOUR AND ALL ON SIX
EXPERIENCED V/S INEXPERIENCED SURGEONS
TYPES OF GUIDES
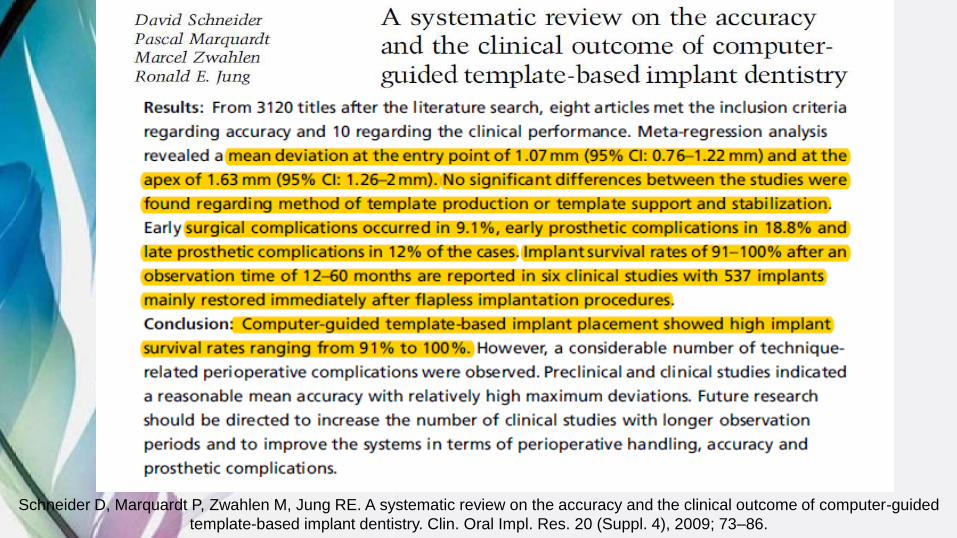
SYSTEMATIC REVIEW
FROM THE CHOSEN ARTICLE
PAIN EXPERIENCED
Good scores were
reported on patient
comfort and pain
after surgery and
patient satisfaction
with oral functions
after 3–12 months
(Steenberghe et al. 2005;
Nikzad & Azari 2010;
Abad-Gallegos et al.
2011)Hultin M, Svensson KG, Trulsson M.
Clinical advantages of computer‐guided
implant placement: a systematic review.
Clinical oral implants research. 2012 Oct
1;23(s6):124-35.
Fortin et al. 2006; Nkenke et al.
2007; Arisan et al. 2010• Statistically significant reduction in immediate
postoperative pain, use of analgesics, swelling, edema, hematoma, hemorrhage, and trismuswhen flapless guided surgery was performed.
• Arisan et al. (2010) also compared guided flapless surgery with guided open flap surgery and demonstrated consistently better outcome measures for the flapless guided technique
FOR RESORBED RIDGES
• The study by Barter (2010) was based on patients previously treated with extensive onlay bone grafting of severely resorbed maxillas.
• They reported 98% implant survival rate and 100% prosthesis survival rate after more than 4 years.
Barter, S. (2010) Computer-aided implant placement in the reconstruction of a severely resorbed maxilla-a 5-year clinical study. The International Journal of Periodontics & Restorative Dentistry 30: 627–637.
DURATION OF TREATMENT AND COST-EFFECTIVENESS
• Arisan et al (2010) found the flapless guided surgery technique to be significantly faster (24 min) compared to both open flap guided surgery (61 min) and conventional surgery (69 min).
• No study has reported on cost-effectiveness measurements.
Arisan et al. (2010). “Accuracy of two stereolithographic guide systems for computer-aided implant placement:
Hultin M, Svensson KG, Trulsson M. Clinical advantages of computer‐guided implant placement: a
systematic review. Clinical oral implants research. 2012 Oct 1;23(s6):124-35.
COMPLICATIONS
• The most common surgical complication was fracture of the surgical guide
• Implant survival after 1 year ranged between 89 and 100% (study mean 97%) and the corresponding prosthesis survival between 62 and 100% (study mean 95%).
• No obvious difference in implant survival rate was observed between studies using an immediate or delayed loading protocol
ALL-O
N-F
OU
R A
ND
AL
L-O
N-S
IX
Van de Wiele G, Teughels W, Vercruyssen M, Coucke W, Temmerman A, Quirynen M. The accuracy of guided surgery via mucosa-
supported stereolithographic surgical templates in the hands of surgeons with little experience. Clin. Oral Impl. Res. 00, 2014, 1–6
EXPERIENCED V/S INEXPERIENCED
SURGEONS
TYPES OF
GUIDES
Schneider D, Marquardt P, Zwahlen M, Jung RE. A systematic review on the accuracy and the clinical outcome of computer-guided