news September / October 2013 Healthy Albertans through excellence in pharmacy practice If a husband asks for his wife’s prescription receipts, can you give them to him? What can you tell the police when they investigate a forgery? Can you email drug information to a patient? Read on to find out. The Health Information Act (HIA) sets out the rules for the collection, use and disclosure of health information by custodians. The Act is designed to enable, not restrict, the flow of health information among health providers within a patient’s circle of care. However, it must balance the need for privacy against the need for use and disclosure, so it is a complex document. This can make it challenging to put into practice. We’re here to help clear things up. What it all boils down to is this: The special section starting on page 7 has the essentials you need to practice safely, effectively, and responsibly. We’ll look at: n Best practices for collecting information, n When and to whom you can disclose information without consent, and n Resources and references to put the answers at your fingertips. IN THIS ISSUE... Quality Pharmacy Practice 2 n Small town or big city: Chat, Check, and Chart is working 4 n Practice Profile: Taking off with travel medicine Partners in Practice 5 n Preceptors: Thank you! 6 n ACP and CPSA partner to identify high risk patients n Technician bridging program delivery to go national n In memory Health information: Handle with care 7 n How is privacy protected in Alberta? 8 n What ACP Standards apply? 9 n The 3 HIA concepts you must understand 16 n HIA in a nutshell Health information: Handle with care How to protect patient privacy and yourself 1. Office of the Information and Privacy Commissioner of Alberta, Health Information – A Personal Matter: A Practical Guide to the Health Information Act, p. 16 PRIME DIRECTIVE Collect, use, and disclose the least amount of information necessary and preserve the highest degree of patient anonymity possible to carry out the intended purpose. 1
Transcript
newsSeptember / October 2013
Healthy Albertansthrough excellencein pharmacy practice
If a husband asks for his wife’s prescription receipts, can you give them to him? Whatcan you tell the police when they investigate a forgery? Can you email druginformation to a patient? Read on to find out.
The Health Information Act (HIA) sets out the rules for the collection, use and disclosureof health information by custodians.
The Act is designed to enable, not restrict, the flow of health information among healthproviders within a patient’s circle of care. However, it must balance the need forprivacy against the need for use and disclosure, so it is a complex document. This canmake it challenging to put into practice. We’re here to help clear things up.
What it all boils down to is this:
The special section starting on page 7 has the essentials you need to practice safely,effectively, and responsibly. We’ll look at:
n Best practices for collecting information,
n When and to whom you can disclose information without consent, and
n Resources and references to put the answers at your fingertips.
IN THIS ISSUE...Quality Pharmacy Practice
2 n Small town or big city: Chat,Check, and Chart is working
4 n Practice Profile: Taking offwith travel medicine
Partners in Practice
5 n Preceptors: Thank you!
6 n ACP and CPSA partner toidentify high risk patients
n Technician bridging programdelivery to go national
n In memory
Health information: Handle with care
7 n How is privacy protected inAlberta?
8 n What ACP Standards apply?
9 n The 3 HIA concepts you mustunderstand
16 n HIA in a nutshell
Healthinformation: Handle with careHow to protect patient privacy and yourself
1. Office of the Information and Privacy Commissioner of Alberta, Health Information – A Personal Matter: A Practical Guide to theHealth Information Act, p. 16
PRIME DIRECTIVECollect, use, and disclose the least amount of information
necessary and preserve the highest degree of patientanonymity possible to carry out the intended purpose.1
aφnews is published six times per yearby the Alberta College of Pharmacists.Send submissions for publication [email protected].
The deadline for submissions for theNovember/December 2013 issue is Oct. 10.
Alberta College of Pharmacists1100, 8215 - 112 Street NWEdmonton AB T6G 2C8780-990-0321 / 1-877-227-3838Fax: 780-990-0328
President: Kelly OlstadPresident Elect: Brad WillseyExecutive Member at Large: Clayton BraunPast President: Kaye Moran
Councillors:Brad Willsey, District 1Clayton Braun, District 2Rick Hackman, District 3Taciana Pereira, District 3Krystal Wynnyk, District 3Kelly Olstad, District 4Kamal Dullat, District 5Kaye Moran, District 5Kelly Boparai, Pharmacy Technician
Public members:Vi BeckerBob KruchtenPat Matusko
Pharmacy technician observer:Robin Burns
You can contact council members by emailvia our website under About ACP/ Council,or by using the search feature to locatethem by name.
Staff DirectoryAll staff are available at 780-990-0321 or 1-877-227-3838 or by fax at 780-990-0328.
Their email addresses are available onour website at pharmacists.ab.ca underContact Us.
Registrar: Greg EberhartDeputy Registrar: Dale CooneyComplaints Director: James KrempienPractice Development Director:
Debbie LeeProfessional Practice Director: Shao LeePharmacy Practice Consultants:
Tom Curr, Monty Stanowich, Jennifer Voice
Operations and Finance Director: Lynn Paulitsch
Registration and Competence Director:Heather Baker
Registration Manager: Linda HagenCommunications Director: Karen Mills
pharmacists.ab.ca
news
When you walk into Thorhild’s lonepharmacy, you will meet Darrel Coma, awell-spoken, knowledgeable member ofAlberta’s pharmacy community for over27 years.
Chat, Check, and Chart was introducedto Darrel as a method to encouragedocumentation and assessment withincommunity practice. Darrel embracedit and has integrated the method intohis practice.
This tool allows Darrel to dig deeper intopatient history and make sureprescriptions are appropriate, effective,and safe. It also allows for a personalizedway of assessing patients.
By using Chat, Check, and Chart, Darrelcan get to know his patients and makethem feel at ease talking about healthconcerns or potential side effects. “Chat,Check, and Chart uses open endedquestions that get patients talking.
“Chat, Check, and Chart has given me theconfidence to chart and document everypatient, complete medication reviews, aswell as unearth new challenges. It ismaking me a better health careprovider.” He is now aiming to furtherhis education and obtain his additionalprescribing authorization.
Darrel believes Chat, Check, and Chart is atool every pharmacist should use.“Pharmacists have a lot to offer and thisincrease in dialogue will create arelationship between the public and theirpharmacists that is vital in a changinghealth system. This will also aid inbridging patient therapy betweendoctors and pharmacists, allowing forcontinuous care.”
2
QualityPharmacyPractice
Small town or big city: Chat,Check, and Chart is working
Digging deeper in the small town
Approximately 90 km south ofDarrel’s drugstore, Salam Shartoohworks in a bustling Edmontonpharmacy. With a revolving door ofpatients who have a multitude ofneeds and prescription types, she hasfound patient documentation andassessment a challenge.
To help with that, an ACP practiceconsultant recommended she try Chat,Check, and Chart. Salam began slowlyby entering basic DAP notes, startingwith one patient per day. It was noteasy for Salam at first to embrace andapply Chat, Check, and Chart, but shepersevered. She has now been usingthis method for over a year and hasexcelled in her practice.
Salam is a foreign trained pharmacistwho has been practising in Alberta forthree years. By implementing Chat,Check, and Chart, she has gainedconfidence as a pharmacist, and isnow training her team members to usethe method.
Salam believes that by using the threequestions to evaluate the appropriatenessof therapy, she has been able to detectunknown or unlisted allergies, a patient’suse of other medications, as well ashealth conditions.
Salam now easily integrates Chat,Check, and Chart into her dailypractice. “This is fundamental to thepractice and I recommend everypharmacy use it in every scenario. Itimproves quality practice and overallpatient safety.”
aφnews – September / October 2013 3
Building confidence in the big city
What is Chat, Check,and Chart?Chat, Check, and Chart wasdesigned to give pharmacistspractical tools that could beincorporated into everydaypractice. This three year oldinitiative, developed by ACP’sShao Lee and U of A ProfessorLisa Guirguis, encouragespharmacists to ask the “rightquestions” when consulting witha patient.
Chat, Check, and Chart is made upof three key tools.
1. Chat asks a pharmacist toreview a specific set ofquestions and document theresponses in order to gainunderstanding of a patient’spurpose for medication, theoverall direction of the therapy, and the monitoring of the therapy.
2. Check has four key questionsfor a pharmacist to considerand evaluate in regards to theappropriateness of the therapy.
3. Chart allows for an efficientDAP.
Find Chat, Check, and Charttoolcards and worksheets on theACP website under PracticeResources > Info sheets & posters.
Jason KmetOwner, Polaris Travel Clinic and Pharmacy, Airdrie
Anticoagulation pharmacist, Foothills Medical Centre, Calgary
Inpatient pharmacist, Peter Lougheed Centre, Calgary
Twenty years in, Jason Kmet still showsthe enthusiasm and energy of a newpharmacy graduate. He constantly seeksout ways to keep his own practice andthe profession growing. This January, hebrought many of his experiences andpassions together when he opened hisPolaris Travel Clinic and Pharmacy.
“Because of the new practice privilegesthat pharmacists have, I've set up adedicated clinical practice primarilyfocused on travel health,” explains Jason.“I received my additional prescribingand injection authorizations in 2008. Ithink I was one of the first to have bothdesignations. Thanks to these changesand expansion of practice that ACP hasenabled, I set up the clinical practice thatI currently provide.”
Jason’s work in anticoagulationprompted him to participate in the 2007pilot for additional prescribingauthorization. “The anticoagulation clinicis basically an outpatient clinic, so weneed to manage patients’ INRs, changedoses, and respond to refill requests allthe time. I saw how useful prescribingwould be.”
At about the same time, he developed aninterest in travel medicine. He went on toobtain his Certificate in Travel Healthfrom the International Society of TravelMedicine in 2009. “It’s so important tomake sure you are confident in yourknowledge, and can back up yourdecisions with evidence,” Jason reasons.“Certification really helps with that.”
He then worked at another travel clinicto hone his skills and in January, tookover a former doctor’s office and madethe leap to clinic ownership. “It doesn’tlook like a typical pharmacy at all. I’vekept all the patient interview rooms, sowe can assess and counsel patients in aprivate, uninterrupted setting. It’s alsodifferent from your typical pharmacy inthat all the patients feel great when theycome in. They’re all excited about thetrips they are planning.”
The clinic is open four days a week, andJason still works some shifts at theanticoagulation and inpatient pharmacy.“In fact,” he laughs, “I used myprescribing authorization in all threeclinics in one week!”
Jason is connecting with thephysicians and other pharmacies inthe area. “I’ve had really goodresponse from the physicians. I makesure to fax each patient’s physician,telling them what I injected orprescribed, including my reasons fortreatment. Keeping them informed hashelped build relationships.”
Amidst juggling work in three clinics,pharmacy ownership, and relationshipbuilding, Jason keeps current byreading as much as possible, attendingconferences, and connecting withcolleagues. He observes that,“pharmacy is always dynamic, nomatter what area you are interested in,so you have to keep up.”
A new clinic, expanding skills, and anenergetic approach to his career – what agreat way for Jason to celebrate his 20thyear in practice!
Jason’s tip for success“Open yourself up to possibilities andlook around. Doors do open up. Andkeep current so that you’re prepared forthose opportunities.”
ResourcesInternational Society of Travel Medicine:www.istm.org
Alberta Association of Travel HealthProfessionals: www.aathp.com
aφnews – September / October 2013 4
practice profile: Taking off with travel medicine
aφnews – September / October 2013 5
Partnersin Practice
Preceptors: Thank you!
I am exceptionally proud of how the pharmacy community in Albertacontinued to contribute substantially to the experiential program of theFaculty of Pharmacy and Pharmaceutical Sciences during the past year despitethe unprecedented economic challenges it faced. Over 220 community andinstitutional pharmacy practice sites volunteered to accept our first-, second-and fourth-year students. Over 500 pharmacists served as preceptors for oneor more of these students. In addition, pharmacists across Alberta haveembraced our PharmD program and we are pleased with the quality andquantity of sites that will be available to our students starting in the winter of2014. Our preceptors are integral members of our Faculty and with theirsupport and involvement, we continue to graduate the very best pharmacistsin Canada. My sincere thanks to everyone who participated in our program.Your contributions are essential to what we do, and greatly appreciated.
James P. Kehrer, Dean
From L to R: Pauline Yeung (Institutional Preceptor), Serena Westad (Student), RachaelHeisler (Institutional Preceptor ), Stollery Children’s Hospital, U of A; Jill Yates (CommunityPreceptor) Save-on-Foods #6678, Sherwood Park, Jasmine Mah (Student)
Preceptor recognition The Faculty would like to recognize andthank all preceptors for theircontribution to their program in2012/13. Please visit the Faculty website (www.pharm.ualberta.ca/Experiential_Education.aspx) to view the list ofpreceptors who precepted studentsover the last academic year.
Preceptor facultyposition open To acknowledge the important role ofpreceptors as part of the Faculty, aformal appointment structure within theUniversity has been created. There aretwo positions: Clinical Preceptor andClinical Academic Colleague (CAC).
The CAC position designates thosepreceptors who consistently preceptstudents. The CAC is a three-year termappointment that provides preceptorswith online access to the Universitylibrary, access to the Faculty Club andrecreational facilities, as well as LRTaccess in Edmonton between SouthCampus and Churchill stations when aONEcard is obtained.
The preceptor homepage(www.pharm.ualberta.ca/en/Experiential_Education/Preceptors.aspx) outlinesdirections for requesting thisappointment. The U of A welcomes alleligible preceptors to nominatethemselves for this faculty appointment.
Preceptor of the Year recipients 2013 Congratulations to the winners of the Preceptor of the Year award for community andinstitutional preceptors for fourth year placements – Pharmacy 425.
ACP and the College of Physicians &Surgeons of Alberta (CPSA) arecollaborating to identify potential highrisk patients and notify involvedpharmacists and physicians.
Patients who are:
n receiving daily OME (oral morphineequivalent) doses greater than 600 mgand
n seeing more than two physicians and
n attending more than two pharmaciesin a three-month period
will be identified using TriplicatePrescription Program (TPP) data.
All the prescribing physicians anddispensing pharmacists will receive anadvisory letter from their college.
The combination of high opioid dosesand attending multiple physicians andpharmacists is worrisome and we willalert the health providers of this concernso that appropriate clinical decisions canbe considered for these patients.
The prescribing may not beinappropriate, but in general CPSA
would recommend that physicians havestrategies to manage opioid prescribingwith firm boundaries to minimize therisk of harm.
ACP recommends that if pharmacistsidentify or become aware of issuesconcerning these prescriptions, theycollaborate with the physicians involvedin their patients' care. Tools to helpmanage high risk patients will beincluded in the letter to the physiciansand pharmacists of these patients.
Some of these patients identified willbe struggling with an addictiondisorder and getting appropriatetreatment will be important toconsider in their management. Furtherinformation on addiction services inAlberta can be found at:https://myhealth.alberta.ca/Pages/default.aspx
We began this process in mid-Augustand hope that this information will helpphysicians and pharmacists to managethese high risk patients collaborativelyand with appropriate strategies in place.
�
�In memory...� Violet May Cornett-Ching diedon June 25, 2013 at the age of 89. Shegraduated from Pharmacy at the U of A in 1948 and got her start as apharmacist in Turner Valley. She spentthe majority of her career in Calgary.
� Iris Farries (nee Maximchuk)died on Oct. 23, 2012 at the age of 80.Iris graduated from the U of A Facultyof Pharmacy in 1955. She served manyclients in several Edmontondrugstores and enjoyed a stimulatingand caring career.
� Rita Diana Forest died on Apr. 10, 2013 at the age of 69. Dianareceived her pharmacy degree fromthe U of A in 1967. She had anadventurous practice in both Albertaand Manitoba. One job required her totravel from Winnipeg to Portage LaPrairie and back each day by bus – an80 mile trip. She nearly died when abullet passed by her left ear during anarmed pharmacy robbery. She alsofailed to convince one drugstoreowner that it was dangerous to smokein a storage room full of canisterscontaining pure oxygen. There neverwas an explosion but Diana had manytense moments when the ownerdisappeared for a smoke. She retired(intact and relieved) in 2002.
� Roger Powlik died onJuly 2, 2013 at the age of 74. Rogergraduated in pharmacy from the U of A in 1960. He practisedpharmacy for 40 years in southernAlberta. For a time he was the owner of Dalbrent Pharmacy inCalgary NW.
� Norman Sproule died on July 9, 2013 at the age of 94. After twoyears of schooling, Norman enlistedwith the army in 1942 and serveduntil returning to his education wherehe achieved his degree as apharmacist in 1947. Norman workedalongside and built his career with hisfather at Sproule Drugs and laterpurchased and operated Shipley Druguntil his retirement in 1986.
aφnews – September / October 2013 6
ACP and CPSA partner toidentify high risk patients
To ensure national consistency,NAPRA, the National Association ofPharmacy Regulatory Authorities, willtake over the administration of thebridging program this fall.
National program is equivalent tothe current program
All courses will be consideredequivalent, regardless of when orwhere they were completed. Coursenames and learning objectives have
not changed. There is no need toretake any courses.
Candidates who have already takensome bridging courses may take theremaining course(s) in the nationalprogram without duplicating ormissing any information.
For more information, visit the ACPwebsite and go to Registration &Licensure > Technicians > Bridgingcourse availability.
Technician bridging programdelivery going national
aφnews – September / October 2013 7
Alberta has three privacy laws:2
1. the Freedom of Information andProtection of Privacy Act for thepublic sector,
2. the Health Information Act for thehealth sector, and
3. the Personal Information Protection Actfor the private sector.
All three Acts require that you limitany collection, use or disclosure ofpersonal information or healthinformation to only what you need toachieve the purpose of the collection,use or disclosure.
Health Information Act (HIA)The HIA applies to health information inthe custody or control of custodians.Custodians include pharmacists,pharmacy technicians, Alberta Health,Alberta Health Services, CovenantHealth, nursing homes, ambulanceoperators, physicians, registered nursesand certain other health professionals.The HIA authorizes custodians to collect,use, and disclose health information forthe purposes of providing healthservices.
Why do you need to know about theHealth Information Act? So that youknow…
n What the law expects you to do toadequately protect health information.
n How to deal with requests for healthinformation from patients and thirdparties.
n When consent is required.
n When you may and when you mustwithhold information.
n What records must be created andstored.
n You are in no danger of aninvestigation by the PrivacyCommissioner and disciplinaryactions from your employer if youcomply with the HIA requirements.
SpecialSection
Healthinformation:Handle with care
What is health information?The HIA definition of health information (s.1(1)) covers anyinformation about an individual that is collected and recordedwhen a health service is provided.
The Act defines two types of health information:
1. Diagnostic, treatment, and care information
2. Registration information
How is privacy protected in Alberta?
2. Excerpted from Office of the Information and Privacy Commissioner of Alberta, “Privacy Emergency Kit,” http://www.oipc.ab.ca/pages/Resources/PrivacyEmergencyKit.aspx (July 23, 2013)
�
aφnews – September / October 2013 8
Sections in the Standards of Practicefor Pharmacists and PharmacyTechnicians, Standards for theOperation of Licensed Pharmacies, andCode of Ethics provide guidance forhandling health information.
The Code of Ethics outlines theframework for your professionalbehaviour. Principle 4 states that whenhandling personal patient information,unless otherwise authorized by law,you must:
n Inform each patient about the usethat will be made of the patient’spersonal information.
n Disclose a patient’s personalinformation only pursuant to thepatient’s consent or for the purpose ofproviding care to the patient.
n Inform the patient to whom and forwhat purpose the patient’s personalinformation will be disclosed.
n Use information obtained in thecourse of professional practiceonly for the purposes for which itwas obtained.
n Seek only information that isnecessary to make informed decisionsabout the patient’s health and thetreatment alternatives that align withthe patient’s treatment goals.
n Protect each patient’s privacy duringany consultation.
Principle 2 gives direction for specifictypes of patients, and patient access toinformation:
n Respect the autonomy of a patientwho is a minor and who is able tomake decisions about the patient’shealth and health care and is able toconsent to care.
n Respect the intentions of a patientwho is not competent where thoseintentions were expressed before thepatient became incompetent (e.g.,through directions provided in a
personal directive or through theappointment of an agent under anadvance directive).
n Give each patient access toinformation in that patient’s recordunless restricted by law or unless it isnot in the patient’s best interest.
The Standards of Practice forPharmacists and Pharmacy Techniciansindicate:
n The types of information thepharmacist needs to providepharmaceutical care (s.3 and 6), and
n The information needed for thepatient record. (s. 18 and Appendix A)
The Standards for the Operation ofLicensed Pharmacies indicate:
n The required environments for saferecord storage and patient services(s. 5), and
n Rules for record keeping (s. 8).
What ACP Standards apply?
Health information: Handle with care
aφnews – September / October 2013 9
Custodians are individuals ororganizations in the health system thathave custody of, or control over, healthinformation. They are the “gatekeepers”of health information.
Custodians are authorized to use healthinformation for:
n Providing health services.
n Determining or verifying a person’seligibility to obtain health services.
n Conducting investigations, disciplinehearings, inspections, etc. relating tomembers of a health profession.
n Conducting ethically approvedresearch or data matching.
n Providing health service providereducation.
n Carrying out specific purposesidentified in other legislation (e.g.,Hospitals Act).
n Internal management, includingplanning, resource allocation, policydevelopment, quality improvement,monitoring, auditing, reporting, andbilling for health services.
Custodians are responsible forensuring that health information iscollected, protected, used anddisclosed appropriately.
Affiliates are “individuals employed bythe custodian.” If you provide serviceson behalf of another designatedcustodian such as a communitypharmacy licensee, Alberta HealthServices, a nursing home, or anotherhealth professional, you are consideredan affiliate of that custodian.
n Custodians are responsible forensuring their affiliates handle healthinformation appropriately.
Note: ACP is not a custodian (that is whywe can’t release individually identifyinginformation in our forgery alerts).
1. Custodian vs. affiliate
The 3 HIA concepts you must understand
Each registrant of the Alberta College of Pharmacists is acustodian under HIA, except when they are an employee /agent or affiliate of another custodian (e.g., a staff pharmacistor pharmacy technician at a community pharmacy or AHS isconsidered an affiliate).
continued on page 10
aφnews – September / October 2013 10
Jeff is a staff pharmacist at a Fort McMurray community pharmacy.
When a pharmacist is employed by a licensed pharmacy, the pharmacist is considered anaffiliate of the pharmacy licensee (the custodian).
Is Jeff a custodian or anaffiliate at the pharmacy?
Barry, a pharmacy licensee, is contracted by an oil company to come to their site and administer fluimmunizations to their employees.
Is Barry the custodianor an affiliate of theoil company?
The oil company is not a custodian under the definition in the Act, so the oil company is notsubject to the Act. Because the company is not a custodian, Barry could not be an affiliateunder the Act despite being employed by the company.
This means Barry is the custodian and so is responsible for the privacy policies andprocedures and the protection of all records related to the services he provides.
The head office manages the storage of records for the pharmacy where Serena works.
No. The pharmacy licensee is the custodian of this health information. If the corporationprovides information management, processing or storage services for the pharmacypractice, it would be providing services as an affiliate as well, and specifically as aninformation manager, which has a distinct status under HIA s.66.
Is the head office of thepharmacy chain thecustodian?
What is a health service?A service that is provided toan individual for any of thefollowing purposes:
n Protecting, promoting ormaintaining physical andmental health
n Preventing illness
n Diagnosing and treatingillness
n Rehabilitation
n Caring for the healthneeds of the ill, disabledinjured or dying
TEST YOURSELF: Custodian vs. affiliate
Health information: Handle with care
Consent of the individual is neitherrequired nor adequate for you to collecthealth information from them for one ofthe authorized purposes. Rememberthough, only collect what is needed todo the job, no more.
Authorized purposes forcollecting, using and disclosinghealth information withoutconsent within the circle ofcare (HIA s.27)
n Providing health services;
n Verifying eligibility to receive ahealth service;
n Investigations, practice reviews,or inspections of a healthprofessional;
n Research that has beenapproved by a designatedresearch ethics board;
n To facilitate health serviceprovider education;
n For a purpose authorized bystatute; or
n To support internalmanagement, includingplanning, resource allocation,policy development, qualityimprovement, monitoring,audit, evaluation, reporting,processing payments, orhuman resource management.
2. Collection
aφnews – September / October 2013 11
3. Standards of Practice for Pharmacists and Pharmacy Technicians
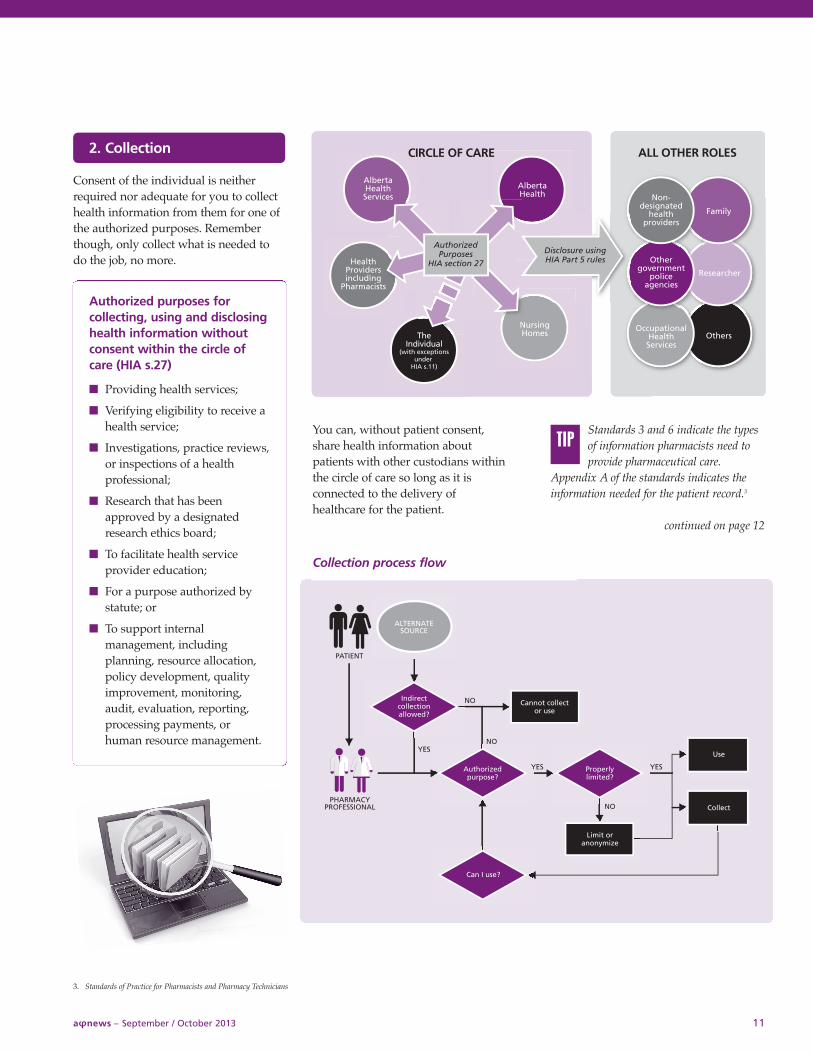
You can, without patient consent,share health information aboutpatients with other custodians withinthe circle of care so long as it isconnected to the delivery ofhealthcare for the patient.
Standards 3 and 6 indicate the typesof information pharmacists need toprovide pharmaceutical care.
Appendix A of the standards indicates theinformation needed for the patient record.3
continued on page 12
TIP
AlbertaHealthServices
AlbertaHealth Non-
designatedhealth
providersFamily
Othergovernment
policeagencies
Researcher
OccupationalHealthServices
Others
HealthProvidersincluding
Pharmacists
TheIndividual
(with exceptionsunder
HIA s.11)
NursingHomes
AuthorizedPurposes
HIA section 27
Disclosure usingHIA Part 5 rules
CIRCLE OF CARE ALL OTHER ROLES
Collection process flow
aφnews – September / October 2013 12
True or False: I can collect health information about a patient from family members to fill a prescription.
This is an indirect collection and is allowable if:
n The patient is incapacitated and not reasonably able topresent and fill their prescriptions themselves, or
n The family member is an authorized representative (e.g.,parent of a minor).
Otherwise, you will need some reasonable indication that thepatient has authorized the family member to provide you withtheir health information.
True or False: The patient’s personal health number is required as part of patient demographics.
n HIA s.21 specifically authorizes custodians to requirecollection of the PHN.
n HIA Regulation s.7.1 requires you to provide a patient’sPHN to Alberta Health as part of a dispensing record.
In all cases, you need to notify patients of your authority torequire their PHN. You can do this with ACP’s PatientInformation Collection Poster (available under Practice Resourceson the ACP website.)
True or False: I should not serve patients who refuse to provide their personal health number.
If, after proper notification, an individual is still apprehensiveabout providing their PHN, explain to them that having theirPHN is important to:
n Uniquely identify their record within the pharmacy and thehealth system;
n Ensure that their drug therapy information is entered onlyon their record;
n Ensure their drug therapy information is accessible to otherhealthcare professionals, through their EHR, if they becomeill and cannot speak (e.g., stroke or unconscious from anauto accident); and
n Serve as one more step you are taking to keep them safe.
It depends
True
Health information: Handle with care
Get from the patient, the first timethey are present, the names ofothers who might provide or
receive information on their behalf.Otherwise, the fact that the patient iscovered by the family member’s healthinsurance may be a good indicator thatthe person is acting on the patient’s behalf.If there are any doubts, contact the patientdirectly before completing the collection.
TEST YOURSELF: Collection conundrums
False If the individual refuses to providetheir PHN, despite your explanation,DO NOT refuse professional servicesunless not having the PHN preventsyou from having information thatyou need to provide the healthservice. Proceed to provide theservices as you normally would, anddo your best to ensure that theirdrug therapy information is enteredon the correct record.
Once health information is collected, you are not free to use it for any purpose. You must only access information for patients to whom you are providing services;you can’t just “check on” family, friends, or others. Also, pharmacies cannot repurposeinformation collected for health services for use in marketing campaigns.
TIP
aφnews – September / October 2013 13
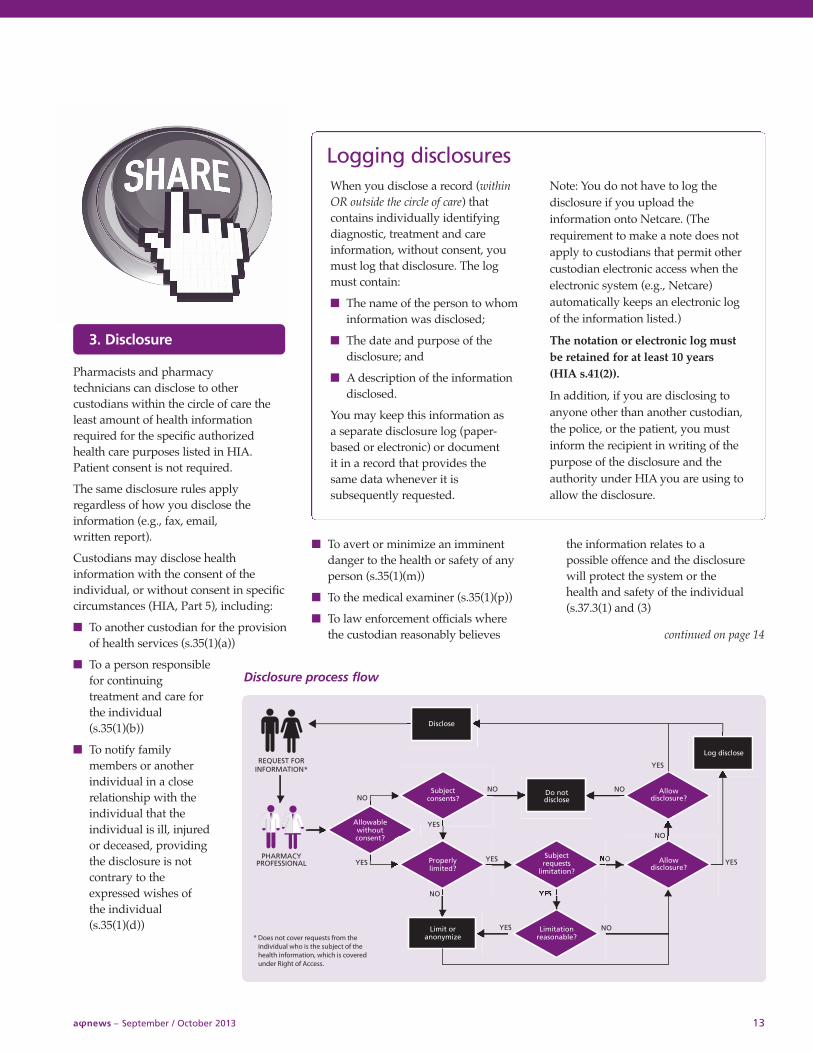
Pharmacists and pharmacytechnicians can disclose to othercustodians within the circle of care theleast amount of health informationrequired for the specific authorizedhealth care purposes listed in HIA.Patient consent is not required.
The same disclosure rules applyregardless of how you disclose theinformation (e.g., fax, email, written report).
Custodians may disclose healthinformation with the consent of theindividual, or without consent in specificcircumstances (HIA, Part 5), including:
n To another custodian for the provisionof health services (s.35(1)(a))
n To a person responsiblefor continuingtreatment and care forthe individual(s.35(1)(b))
n To notify familymembers or anotherindividual in a closerelationship with theindividual that theindividual is ill, injuredor deceased, providingthe disclosure is notcontrary to theexpressed wishes ofthe individual(s.35(1)(d))
n To avert or minimize an imminentdanger to the health or safety of anyperson (s.35(1)(m))
n To the medical examiner (s.35(1)(p))
n To law enforcement officials wherethe custodian reasonably believes
the information relates to apossible offence and the disclosurewill protect the system or thehealth and safety of the individual(s.37.3(1) and (3)
continued on page 14
3. Disclosure
Disclosure process flow
Logging disclosures When you disclose a record (withinOR outside the circle of care) thatcontains individually identifyingdiagnostic, treatment and careinformation, without consent, youmust log that disclosure. The logmust contain:
n The name of the person to whominformation was disclosed;
n The date and purpose of thedisclosure; and
n A description of the informationdisclosed.
You may keep this information asa separate disclosure log (paper-based or electronic) or documentit in a record that provides thesame data whenever it issubsequently requested.
Note: You do not have to log thedisclosure if you upload theinformation onto Netcare. (Therequirement to make a note does notapply to custodians that permit othercustodian electronic access when theelectronic system (e.g., Netcare)automatically keeps an electronic logof the information listed.)
The notation or electronic log mustbe retained for at least 10 years(HIA s.41(2)).
In addition, if you are disclosing toanyone other than another custodian,the police, or the patient, you mustinform the recipient in writing of thepurpose of the disclosure and theauthority under HIA you are using toallow the disclosure.
aφnews – September / October 2013 14
TEST YOURSELF: Disclosure scenarios
Scenario 1: Request for copies of prescriptions
Prescription receipts for income tax purposes contain individually identifying diagnostic,treatment and care information and registration information. This information may be disclosedon the tax receipt if:
n Each family member has consented to the disclosure (s.34), or
n The authorized representative of a family member has authorized Mary to act on their behalf toaccess the information (s.33 and 104).
So, in this scenario, the following disclosure decisions would apply:
Robert (7 years old) - You may disclose because, as the parent, Mary is his authorizedrepresentative (s.104(1)(c)).
John (husband) - You would have to obtain John’s consent for Mary to access his healthinformation (s.104(1)(i)).
Cathy (16 years old) - You would use your discretion since Cathy probably understands the natureof consenting and the consequences of exercising that right or power (s.104(1)(b)). An example ofsuch a situation would be if Cathy was taking oral contraceptives and her mother was not awareof this. Providing the information to her mother would be a judgment call and you shoulddocument your rationale for your decision.
Rose (her mother) - Mary states that she has a power of attorney for Rose. You could disclose toMary if she presented evidence of the power of attorney to you.
If all of the disclosures are to the individual or their authorized representative, a disclosurenotation and notice to recipient is not required. If a disclosure is done with the individual’sconsent, a notice to recipient (s.42) would be required.
As always, document the disclosure unless it was to an authorized representative, and keep it forat least 10 years.
Consent note: Verbal consent, or other alternatives such as implied or opt-out consent, is not valid underHIA; consent must be written.
Consent must also be informed. For example, before asking patients to sign consent forms, you must ensureyou provide them with enough information about the disclosure consent request so that they can understandthe request.
Scenario 2: A forgery
You may disclose health information to a police service without the individual’s consent if youreasonably believe that the information disclosed relates to the possible commission of an offenceunder a statute of Alberta or Canada and will either:
n Detect, limit or prevent fraudulent use or abuse of the health system (HIA s.37.1), or
n Protect the health or safety of an individual (HIA s.37.3).
You may disclose the following individually identifiable information:
n The individual’s name, birth date, and personal health number;
n The nature of any injury or illness of the individual;
n The date on which a health service was sought or received;
n The locations where the health service was sought or received; and
n The name of any drug provided or prescribed to the individual, and the date the drug wasprovided or prescribed.
Log the disclosure and keep on the patient’s record for at least 10 years.
How does HIAapply to thisscenario?
Mary Smith comesinto your pharmacy torequest copies ofprescription receipts forincome tax purposesfor her entire family(husband John,daughter Cathy(16 years old), sonRobert (7 years old)and her mother Rose(87 years old andliving with the family).
How does HIAapply to thisscenario?
You suspect a forgedprescription. Whatinformation can youdisclose to the police?
Health information: Handle with care
aφnews – September / October 2013 15
Scenario 3: Request to not disclose to another health provider
You must consider any expressed wishes of the patient when deciding whether and what todisclose, even as part of the Alberta EHR, together with any factors that you think are important.
For instance, a patient might ask to ensure that her ex-husband, who is a physician, does not knowthat she is taking medications and therefore does not want you to submit her information to PIN(even though the physician would be prohibited from accessing the file). If the physician is stillpractising, and considering the circumstances described by the patient, this might seem reasonable.
In other circumstances, it may be your judgment that not disclosing health information toother health providers is too much of a risk to the safety of the patient or the ability of ahealthcare professional to provide appropriate health services, including circumstances of amedical emergency.
In the end, the decision to disclose is still yours to make in spite of the objections of thepatients, and you should document the rationale for your decision. (NOTE: You must stillupload ALL prescription transaction data to PIN, even if you and the patient agree that itshould not be disclosed.)
Alberta Netcare has developed procedures, criteria and scripts for masking information. Healthproviders may still “lift the mask” or can apply to rescind masking applied to records of theirpatients as required for specific reasons documented in the system.
How does HIAapply to thisscenario?
One of your patientsexplicitly requests thatsome or all of theirhealth information notbe disclosed to anotherhealth provider underany circumstances.
What do you do?
Available on the ACP website, underPractice Resources:
n Patient information collection poster
n Patient privacy poster
n Health Information – A PersonalMatter: A Practical Guide to theHealth Information Act
Helping pharmacists andpharmacy techniciansunderstand the Health
Information Act: Privacy andconfidentiality guidelines
This is the “go to” resource forunderstanding how the HIAapplies to pharmacy.
The easy-to-read explanations,examples, and real-life scenarioswill help you confidently deal withhealth information in transactionswith patients, third parties, andother healthcare professionals.
Privacy resources
NEW
To prevent disclosure through careless actions:
n Remove all labelling before dispensing medication that was previously prepared for, but not picked up by,another patient.
• Simply blacking out the original label with marker often does not render the informationunreadable. It can also heighten the receiving patient’s curiousity, raise doubts about the safety ofthe medication, and diminish confidence in your pharmacy’s handling of patient information.
n Remember that disclosure of just basic facts such as the location of the patient or some detail about theirclinical condition, may be sufficient to identify them to a family member or acquaintance.
Canadian Publication Agreement Number: 40008642
Return undeliverable Canadian addresses to:Alberta College of Pharmacists1100, 8215 - 112 Street NW, Edmonton, AB T6G 2C8news
aφnews – September / October 2013 16
Controlling the sharing of healthinformation can seem daunting. But ifyou follow the Prime Directive (seethe front cover) and keep thefollowing concepts in mind, you’ll beon solid footing.
General rulesn Only collect, use or disclose what is
needed to do the job, no more.
n Collect directly from the individualwhenever possible.
n Only provide information to thosewith a need to know.
n Provide anonymous informationwhenever possible.
n Safeguard the health informationyou hold.
Use of health informationwithout consentCustodians can use health informationwithout consent for:
n Providing and determining eligibilityfor health services;
n Conducting formal investigations orauthorized research;
n Providing health service providereducation;
n Managing internal operations such asplanning and allocating resources,quality improvement, evaluation, andobtaining payment for services.
Disclosure of healthinformation without consentCustodians can disclose withoutconsent to:
n Another custodian or successor of acustodian;
n Continuing treatment and careproviders;
n Family members in certaincircumstances;
n Authorized representatives ofindividuals;
n Health professional bodies, auditors,and quality assurance committees;
n Researchers subject to ethics review;
n Entities authorized to obtaininformation required by otherlegislation, e.g., courts and subpoenas;
n Police when investigating a lifethreatening injury to the individual;and
n Another custodian or police toprevent fraud or detect abuse ofhealth services;
n Any person to avert or minimize animminent danger.
HIA in a nutshell 4
ACP emails and newsletters are official methods of notification to pharmacists andpharmacy technicians licensed by the college. In addition to providing you with timelyinformation that could affect your practice, college emails serve in administrativehearings as proof of notification. Make sure you get the information you need topractice legally and safely by reading college newsletters and ensuring ACP emails arenot blocked by your system.!
4. Adapted from The Health Information Act At a Glance For Custodians, produced by the Office of the Information and Privacy Commissioner of Alberta, 2012