58
ACT 48: AN ACT CREATING A UNIVERSAL AND UNIFIED HEALTH CARE SYSTEM- UPDATE 2012 Harry Chen, MD, Commissioner of Health
| Date post: | 15-Dec-2015 |
| Category: |
Documents |
| Upload: | max-suarez |
| View: | 215 times |
| Download: | 0 times |

ACT 48: AN ACT CREATING A UNIVERSAL AND UNIFIED HEALTH CARE SYSTEM- UPDATE 2012
Harry Chen, MD, Commissioner of Health
Why our health care system is broken
It’s too costly and contains no mechanism for cost control.
It is funded in a manner which is unfair, inefficient and inequitable.
Too many people are uncovered (47,000) and underinsured (160,000)
And it doesn’t provide Vermonters with the best value for the health care dollars we spend.
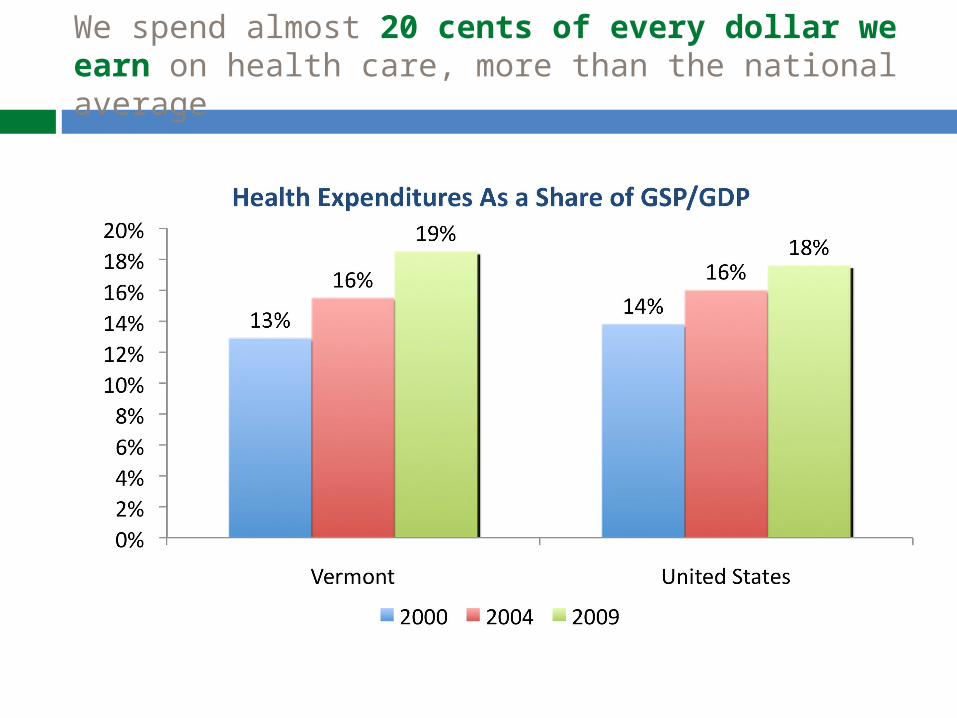
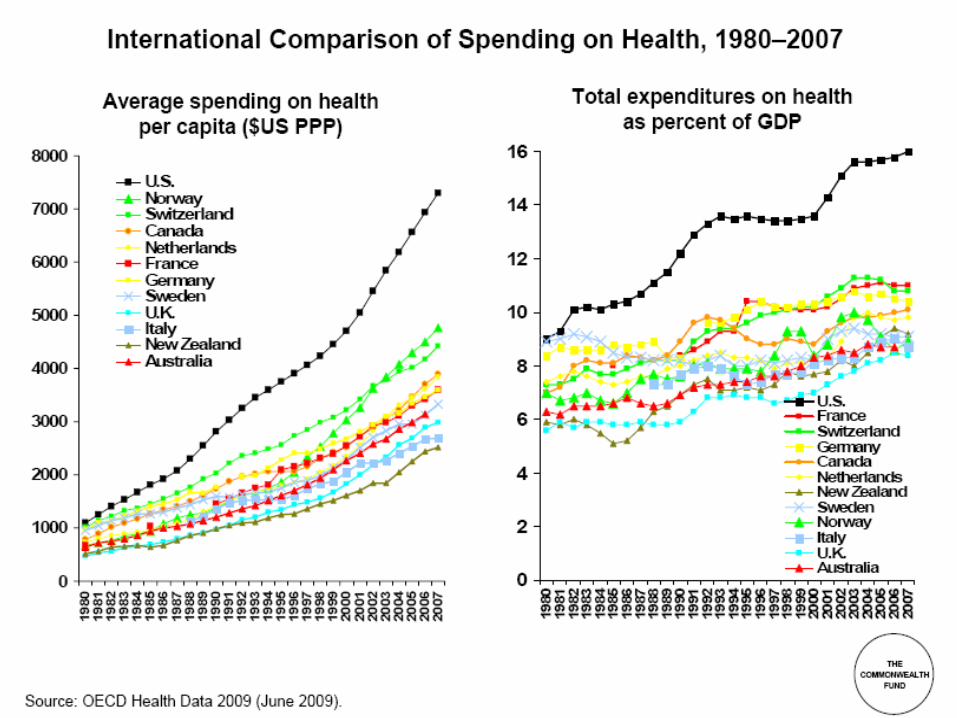
We spend almost 20 cents of every dollar we earn on health care, more than the national average
The Opportunity of Health Care Reform
Cover all Vermonters regardless of age income, or employment status
Preserve quality and patient choice
Separate health care from employment
Lower health care spending
Improve health
Create jobs and economic opportunities
Goals
A sustainable budget for health care in Vermont
Achieve and maintain a reasonable rate of growth in overall spending closer to economic growth
Quality maintained or improved and health improved
Changes in health care payment and delivery that are necessary to support these goals

What did Act 48 do?
Green Mountain Care Board Cost containment Payment reform Workforce development Oversight of almost all aspects of health policy
Vermont Health Benefit Exchange Reorganizes purchasing of health insurance Allows many uninsured Vermonters to get tax credits
for coverage Detailed Planning for Green Mountain Care (single
payer) Operational planning Financing plan
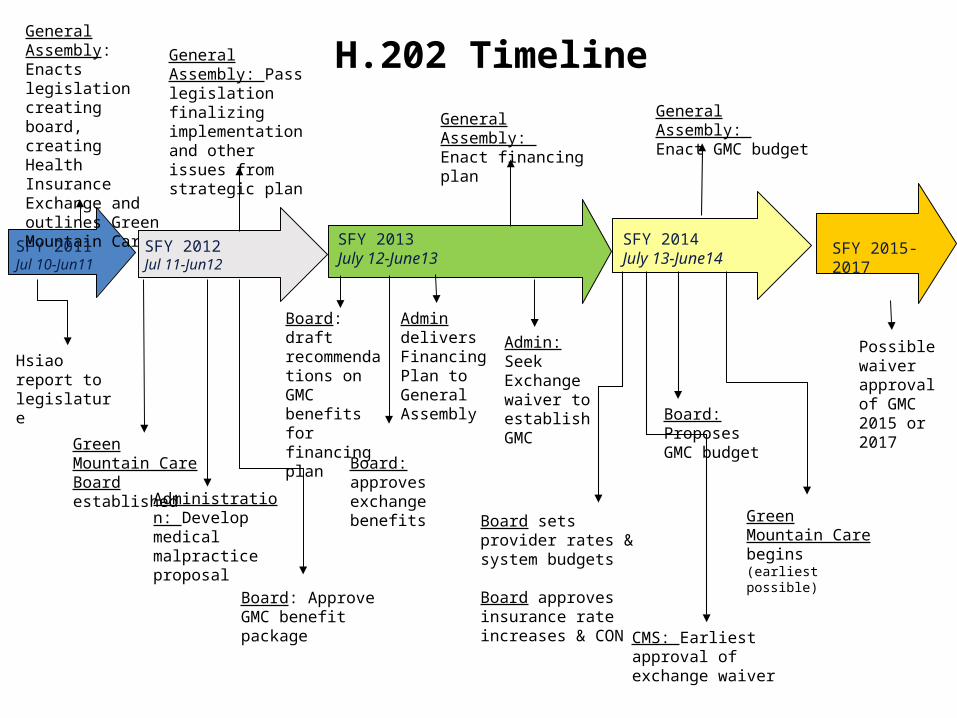
H.202 Timeline
CMS: Earliest approval of exchange waiver
SFY 2013July 12-June13
Admin delivers Financing Plan toGeneral Assembly
Board: draft recommendations on GMC benefits for financing plan
Board: approves exchange benefits
General Assembly: Enact financing plan
Admin: Seek Exchange waiver to establish GMC
Green Mountain Care begins (earliest possible)
Board sets provider rates & system budgets
Board approves insurance rate increases & CON
SFY 2014July 13-June14
General Assembly: Enact GMC budget
Board: Proposes GMC budget
SFY 2015-2017
Possible waiver approval of GMC 2015 or 2017
General Assembly:Enacts legislation creating board, creating Health Insurance Exchange and outlines Green Mountain Care
SFY 2011Jul 10-Jun11
Hsiao report to legislature
Administration: Develop medical malpractice proposal
Green Mountain Care Board established
General Assembly: Pass legislation finalizing implementation and other issues from strategic plan
SFY 2012Jul 11-Jun12
Board: Approve GMC benefit package
Health Care Reform Timeline
10
Green Mountain Care Board: Who are they?
11
5 members, appointed by the Governor with advice and consent of the Senate
Chairwoman Anya Rader Wallack, Ph.D. of Calais
Al Gobeille, of Shelburne Karen Hein, M.D. of Jacksonville Con Hogan of Plainfield Allan Ramsay, M.D. of Essex Junction
04/18/23 12
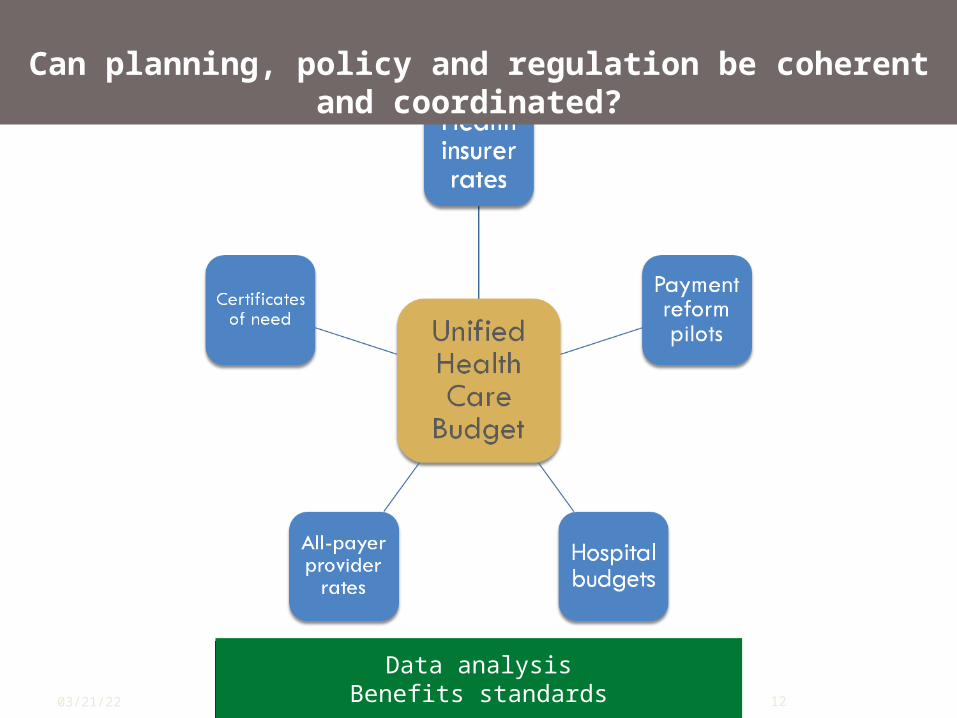
Data analysisBenefits standards
Data analysisBenefits standards
Can planning, policy and regulation be coherent and coordinated?
More steps along the way …
2014 – Vermont Health Benefit Exchange Provides new federal tax credits to cover
uninsured Vermonters Administrative structure for the single
payer Upon availability of federal waiver (2017
at latest) Vermont implements single payer
“Health Benefit Exchange”
14
A mechanism for purchasing health insurance
Simplifies shopping – like Expedia Standardizes insurance options “Qualifies” health plans Administers new federal tax credits Provides guidance and quality ratings to
people shopping If state doesn’t develop, feds will
15
Who is eligible to buy insurance in the Exchange?
Open to all citizens and legal immigrants who live in Vermont (except those in prison)
Open to small employers that offer coverage to all full-time employeesSmall employer = up to 50 employees in 2014; 100 employees in 2016
In 2017, states may choose to include large employers, too.

16
What are they buying?
Qualified health plans: Provide “essential health benefits” Are certified by the Exchange as meeting certain standards
and requirements Are offered by Vermont-licensed insurers who agree to offer
at least gold and silver level plans
17
Uninsured individuals with income under 400% FPL (and no access to an employer plan) are eligible for premium tax credits for enrolling in plans through the Exchange
Tax credit amounts are based on income
Individuals under 250% also receive reductions in cost-sharing (including deductibles and co-pays)
Why buy in the Exchange?Tax Credits and Cost-Sharing Subsidies
Why do we need an Exchange ?
Individual tax credits are available only through the Exchange
Funds to design and build the Exchange and revamp our eligibility, enrollment and claims processing for Medicaid to serve a larger population
Reduced complexity of insurance purchasing Federal limitations on waiver Potential for single claims processing
mechanism
19
Exchange Internal Timeline/Activities Summer-Fall 2012
Finalize outreach & education plan and Navigator Program Present GMCB with Essential Health Benefits and Plan Design
recommendations Develop scope of work and contract for IT system integrator
(SI) Develop informational Exchange website (shell) Explore and finalize wellness offerings through Exchange --
offerings and quality measures in line with Healthy Vermonters 2020 and Blueprint for Health
Begin CMS Design Reviews (federal requirements & oversight)
Winter-Spring 2013o Submit sustainability and transition plans to state
legislatureo Lay the groundwork for outreach, Navigator program, and
internal/external training o SI work ongoing
Vermont Health Benefit Exchange
HIX Internal Timeline
Summer 2013o Full-scale launch of outreach campaign o System testing o Train Navigators, call-center staff, state support
staff, and grass-roots advocates October-January 2013
o Open Enrollment on Exchange website o Navigators providing enrollment assistance in the
fieldo Call-center up and running
January 1, 2014o Exchange health coverage active
Vermont Health Benefit Exchange
New: Proposed Visual Identity
Vermont Health Benefit Exchange
The visual identity of the Exchange will be a public face of health reform in Vermont. A range of possible names, taglines, logos, color schemes and images were developed. Then, focus groups of Vermonters – including both individuals and small business owners – were asked to give feedback and discuss their reactions. This is the result.
Green Mountain Care (single payer)
23
Occurs after Affordable Care Act waiver and other requirements are met
All Vermonters covered by virtue of residency
Legislative concerns re: in-migration of people for benefits
Penalties for falsifying residency De-coupled from employment
What about the financing?
Report to the legislature in 2013two financing plans:
one with continued private premiums one with all public financing
Maximize federal funds and spread costs fairly Many issues to be resolved:
What will the overall costs/savings be? How much federal $ will we get? How do we deal with cross-border issues? How are public and private coverage integrated? How do we incorporate self-insured employers?
25
December 14, 2011
HEALTH CARE REFORM FINANCING:LISTENING SESSION
Listening Session’s Purpose Legislature Passed Act 48, An Act Relating to
a Universal and Unified Health System Act 48 requires financing plans to be presented
in 2013 Public input is important & necessary to inform
the financing plans o “The state must ensure public participation in the
design, implementation, evaluation, and accountability mechanisms of the health care system.” –ACT 48
Listening sessions provide an opportunity to express preferences for the type of principles and funding sources that will help shape the financing plans due in 2013
27
Organization of the Session
Principles of a Health Care Finance System What are
principles and why are they important?
Discuss in small groups
Express preferences
Potential Funding Sources Funding generally Payers and funding
sources Health care
expenditures and state revenues
Small group exercise
28
Examples of Principles for a Financing System
Example principle: Equity Revenue system should take into account ability to
payo Example, progressive federal & state income tax
Example principle: Exportability Taxes should be paid by non-residents when
possibleo Example, Alaska receives 83% revenue from oil
royalties
Example principle: Stability Relies on a balanced variety of revenue sources
o Example, Vermont’s revenue mix is among most balanced in Nation
29
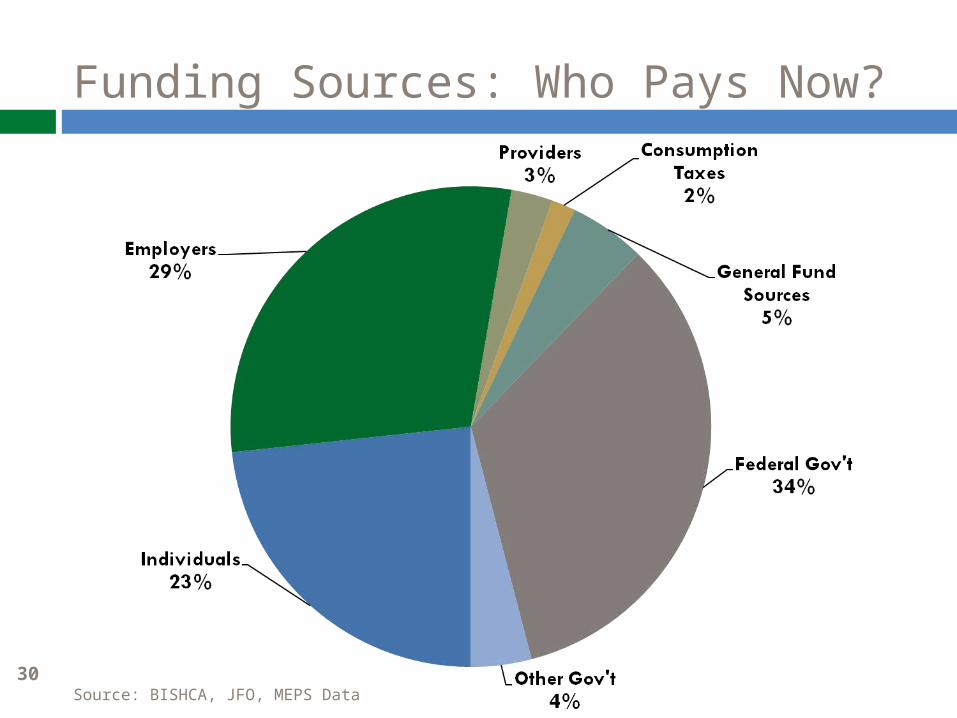
Funding Sources: Who Pays Now?
Source: BISHCA, JFO, MEPS Data30
Potential Funding for Health Care Financing System
Individuals: beneficiary premiums Individuals: out of pocket spending for
services General tax on businesses Payroll tax, both businesses and
individuals Income tax Property tax Consumption taxes
31
Benefits Listening Sessions May – June 2012
GREEN MOUNTAIN CARE: VERMONT’S HEALTH CARE REFORM
Listening Session’s Purpose
Public input is important and necessary to inform the design of the benefits
“The state must ensure public participation in the design, implementation, evaluation, and accountability mechanisms of the health care system.” –ACT 48
Listening sessions provide an opportunity to express preferences that will help shape the benefits for Green Mountain Care
33
GMC Benefits: focus for today
34
35
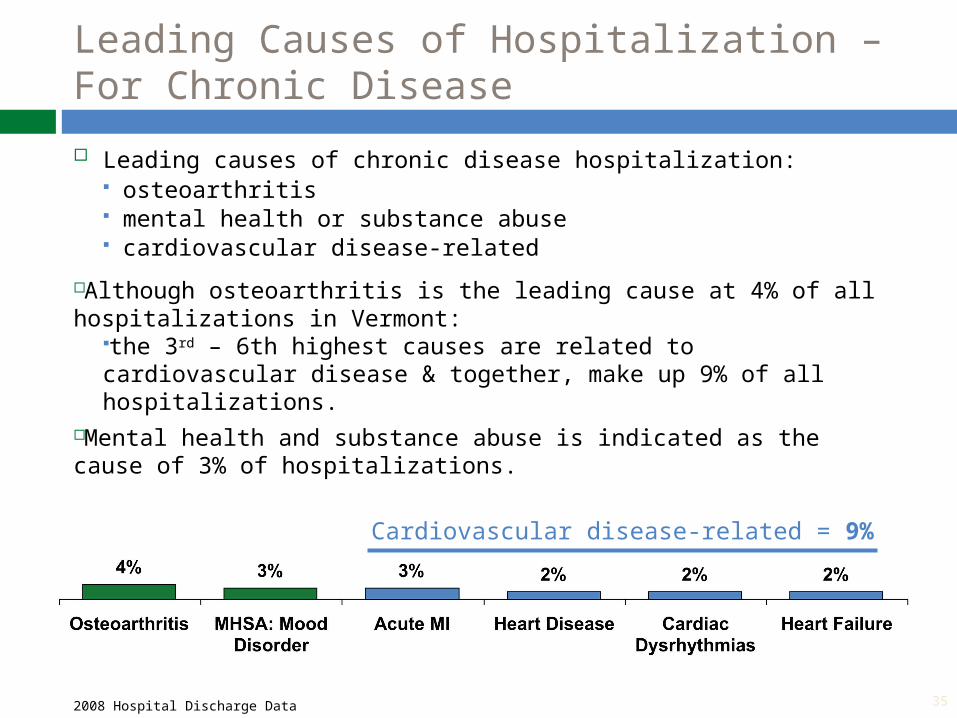
Leading Causes of Hospitalization – For Chronic Disease
Leading causes of chronic disease hospitalization: osteoarthritis mental health or substance abuse cardiovascular disease-related
Although osteoarthritis is the leading cause at 4% of all hospitalizations in Vermont:
the 3rd – 6th highest causes are related to cardiovascular disease & together, make up 9% of all hospitalizations.
Mental health and substance abuse is indicated as the cause of 3% of hospitalizations.
2008 Hospital Discharge Data
Cardiovascular disease-related = 9%
36
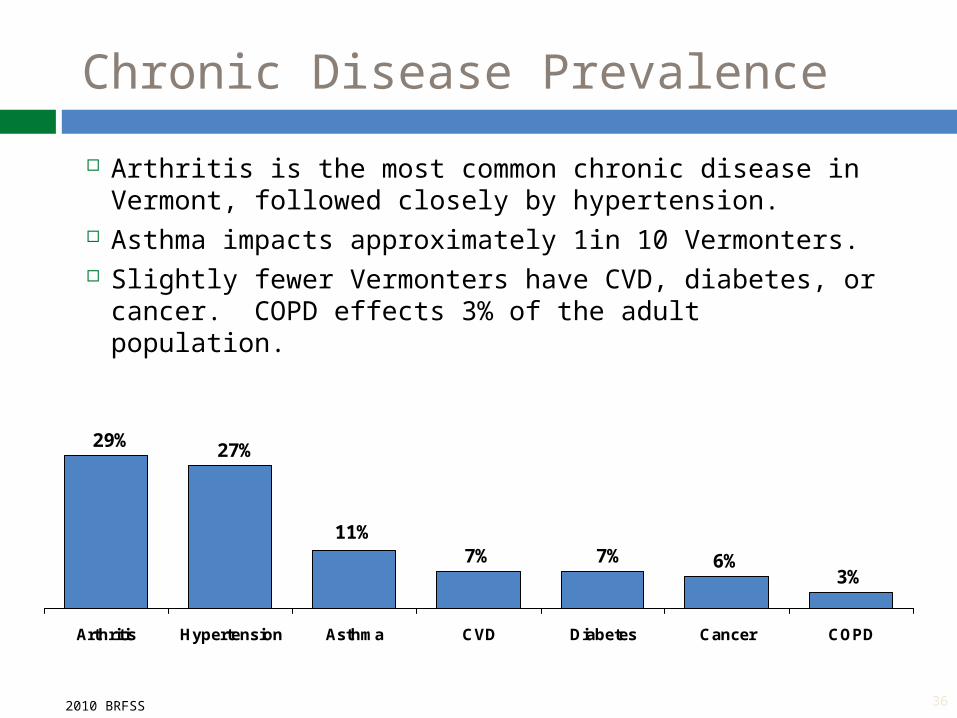
Chronic Disease Prevalence
6%3%
11%
27%
7%
29%
7%
Arthritis Hypertension Asthma CVD Diabetes Cancer COPD
2010 BRFSS
Arthritis is the most common chronic disease in Vermont, followed closely by hypertension.
Asthma impacts approximately 1in 10 Vermonters. Slightly fewer Vermonters have CVD, diabetes, or
cancer. COPD effects 3% of the adult population.
Coverage and Cost are Connected
In a universal system, everyone is covered and everyone pays into the system
What are our priorities as a community? How do we decide what care to pay for? While ensuring people get what they need Promoting health and wellness
37
Shift the Emphasis of Care
In the US health care system there is not enough focus on and utilization of preventative medicine and chronic disease management, which improve health outcomes and curb escalating health costs
Studies have shown that prevention can: prevent chronic diseases (such as type II
diabetes) Chronic disease management can:
prevent avoidable Emergency Dept visits, improve outcomes, prevent the need for invasive surgeries, and save lives
40
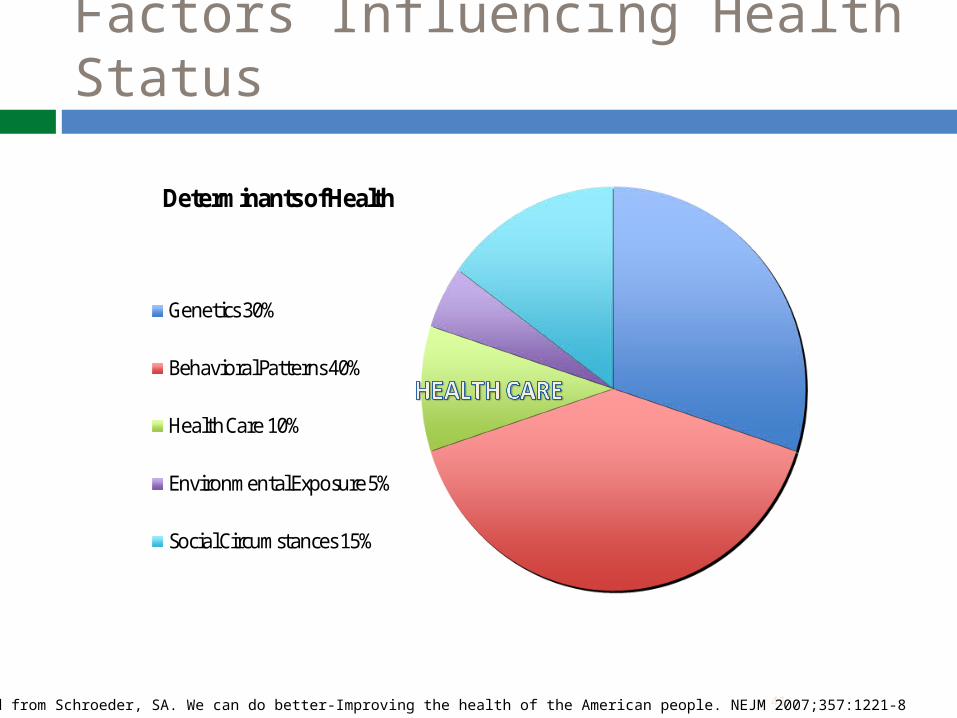
Factors Influencing Health Status
Determinants of Health
Genetics 30%
Behavioral Patterns 40%
Health Care 10%
Environmental Exposure 5%
Social Circumstances 15%
41Adapted from Schroeder, SA. We can do better-Improving the health of the American people. NEJM 2007;357:1221-8
Act 171: 2012 Health Reform Bill
Insurance market reforms compliant with the federal Affordable Care Act
Integration of Medicaid with the Exchange: Global Commitment, Dual-Eligibles, and other waivers
Creation of a viable and dynamic exchange that supports Vermont's health care reform goals
Refinement of the functions of the Green Mountain Care Board- CON, hospital budgets, rate review
Malpractice Reform
Exchange/Insurance Compliance with ACA
Employers in the Vermont Health Benefit Exchange 2014: 50 or fewer 2016: 100 or fewer
Allows bronze plans and dental plans to be sold with QHPs. Merges individual and small group
Provides parameters about Navigators and Brokers GMCB must approve a full range of cost-sharing
structures in the Exchange for each actuarial value and allow insurers to offer wellness rewards and discounts
“
Malpractice Reform
• Certificate of Merit • Pre-suit mediation • Medical malpractice reform
report
44
Begins Feb. 2013
Begins Feb. 2013
Health Reform: Building on a Strong Base Blueprint for Health Vermont Information Technology
Leaders Medicaid Global Commitment Waiver
Coverage Expansion “MCO Investments”
Federally Qualified Health Centers
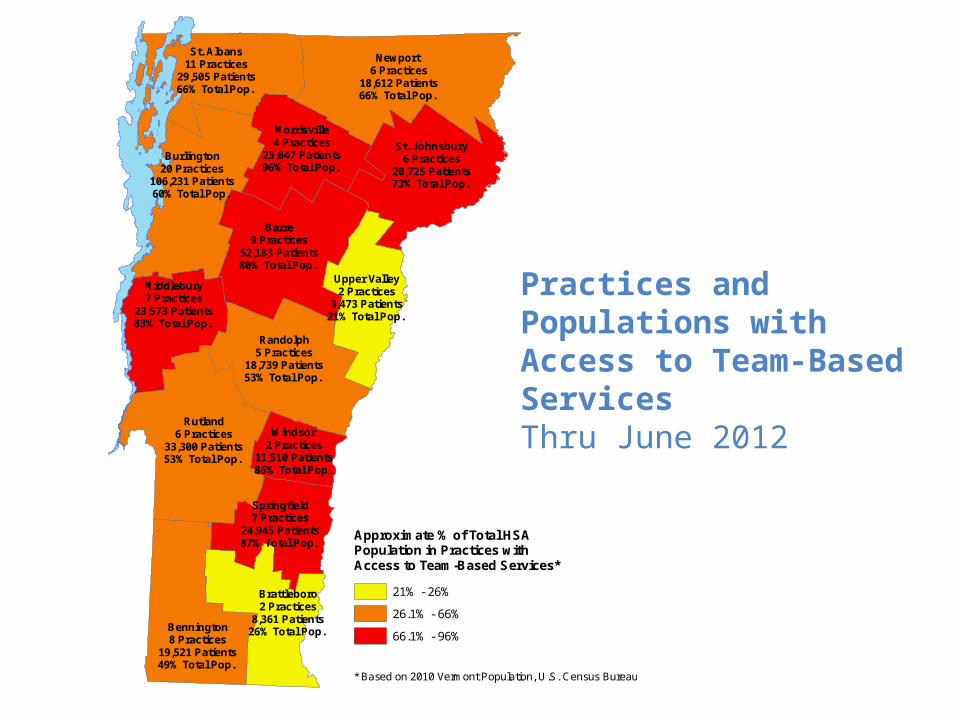
Practices and Populations with Access to Team-Based ServicesThru June 2012
* Based on 2010 Vermont Population, U.S. Census Bureau
Approximate % of Total HSA Population in Practices with Access to Team-Based Services*
21% - 26%
26.1% - 66%
66.1% - 96%
Newport6 Practices
18,612 Patients66% Total Pop.
Rutland6 Practices
33,300 Patients53% Total Pop.
Burlington20 Practices
106,231 Patients60% Total Pop.
Barre9 Practices
52,183 Patients80% Total Pop.
Randolph5 Practices
18,739 Patients53% Total Pop.
St. Johnsbury6 Practices
20,725 Patients73% Total Pop.
Bennington8 Practices
19,521 Patients49% Total Pop.
St. Albans11 Practices
29,505 Patients66% Total Pop.
Middlebury7 Practices
23,573 Patients83% Total Pop.
Brattleboro2 Practices
8,361 Patients26% Total Pop.
Morrisville4 Practices
25,047 Patients96% Total Pop.
Upper Valley2 Practices
3,473 Patients21% Total Pop.
Springfield7 Practices
24,945 Patients87% Total Pop.
Windsor2 Practices
11,510 Patients86% Total Pop.
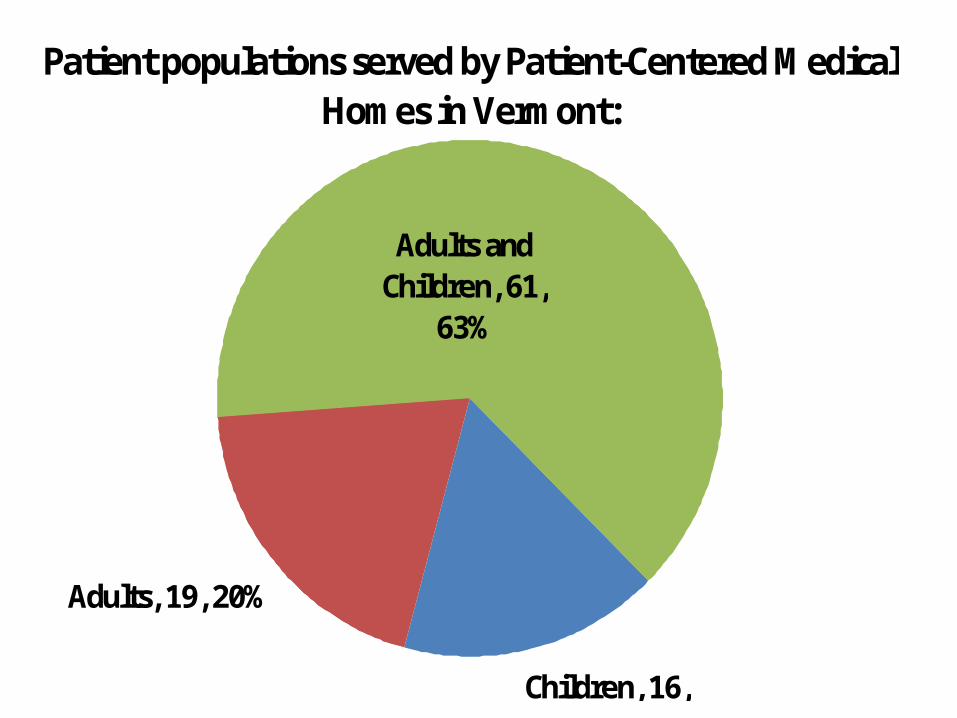
Patient populations served by Patient-Centered Medical Homes in Vermont:
Children, 16, 17%
Adults, 19, 20%
Adults and Children, 61,
63%
49
Current Payment Systems Do Not Support High Quality Cost Effective Patient Care
Volume based – (FFS, DRG’s, Per diems)
Encourages visits and procedures
Does not encourage efficiency, quality, coordination or value.
New payment methods must be balanced to address utilization, cost, quality and patient experience (value)
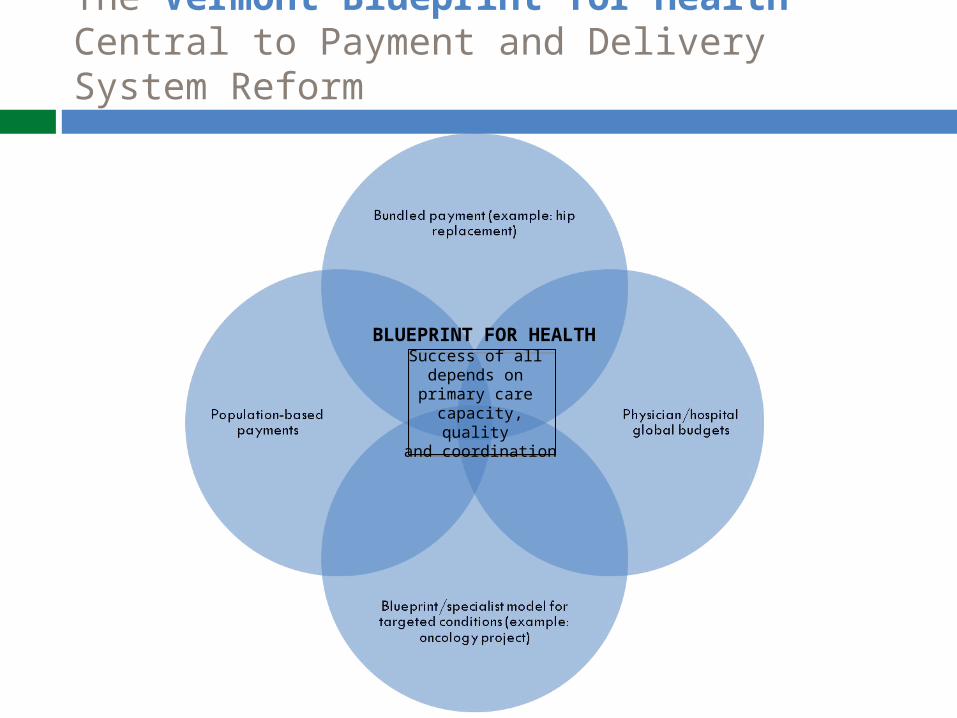
The Vermont Blueprint for Health Central to Payment and Delivery System Reform
Success of all depends on primary care
capacity, quality and coordination
BLUEPRINT FOR HEALTH
Payment reform goals
52
Shared Interests: PCPs, Specialists, Hospitals, Community-Based Services
Intense Focus on high risk/high cost patients Better coordination of care
Mental Health and Substance Abuse Services, Home Health, SNFs/NHs
Four dimensions of performance (balanced) Reduce growth of total cost of care Reduce avoidable utilization Improve adherence to standards of care
(condition specific) Measure patient experience
What about Washington?
Supreme Court Decision Individual mandate survived as a tax. Medicaid expansion is optional. Are we done with court challenges?
2012 Elections Congress could repeal ACA. New President could ???
ACA Waiver for Green Mountain Care 2017 is earliest date in law. Anything sooner would require legislation.
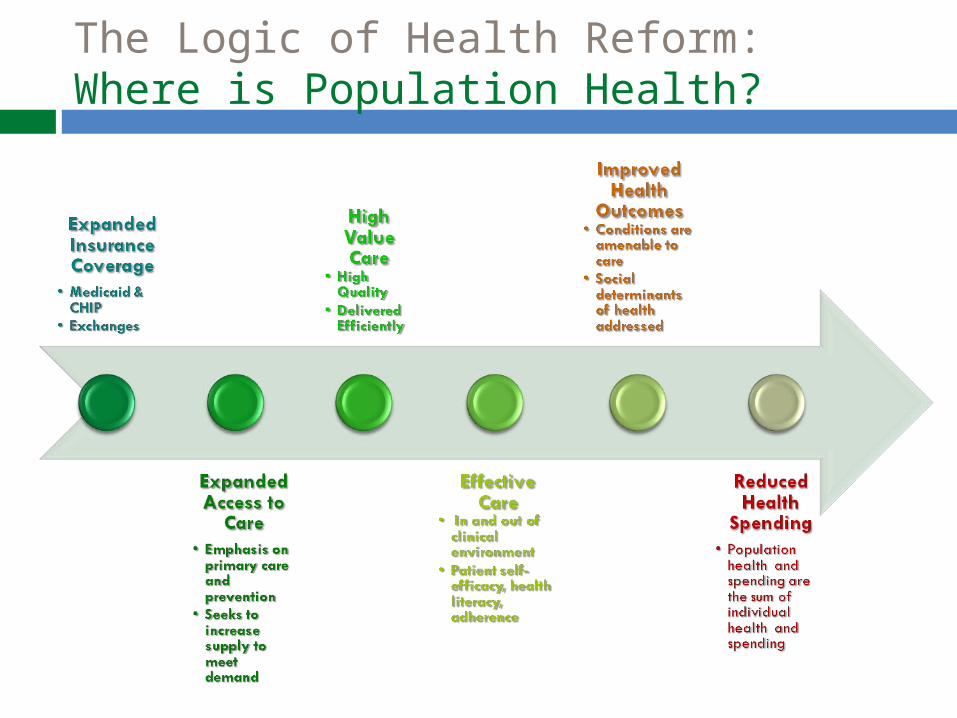
The Logic of Health Reform: Where is Population Health?

The Best Opportunity To Maximize Health
Leverage the Far Larger Personal Health System to Achieve Population
Health Goals
NOT TO SCALE
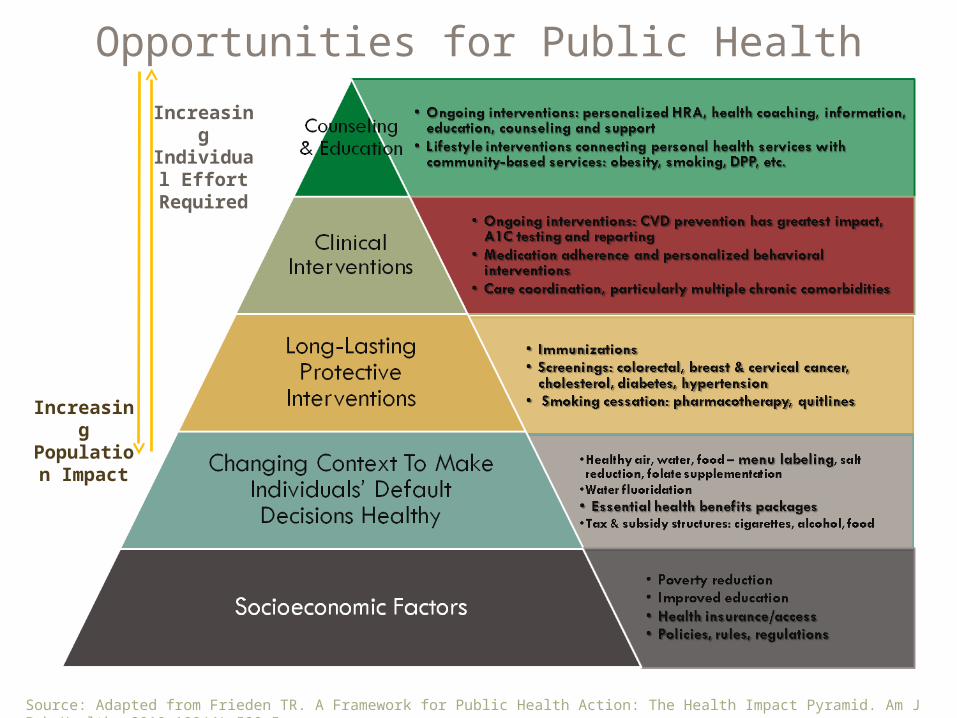
Increasing
Individual Effort
Required
Increasing
Population Impact
Source: Adapted from Frieden TR. A Framework for Public Health Action: The Health Impact Pyramid. Am J Pub Health. 2010;100(4):590-5.
Opportunities for Public Health
The finish line
Health care is a right – all Vermonters are covered
Health care costs are sustainable – closer to our rate of economic growth
Providers are paid fairly Everybody pays their fair share Vermont is the best place to do business Vermont is the best place to practice
medicine Vermont is the healthiest place to live
Summary
Act 48 creates a responsible plan for health care reform that includes opportunities for Vermonters to participate. We are making progress toward that goal.
Without reform, costs will grow faster and system will continue to erode.
With reform, we can cover all Vermonters, achieve substantial cost savings and improve overall health.
— Dr. Martin Luther King Jr., 1966
"Of all the forms of inequality, injustice in health care is the most shocking and inhumane."



![Hermione Granger’s Act of Equality in Harry Potter Saga Movies · Potter and The Order of the Phoenix [6], Harry Potter and the Half-Blood Prince [7], Harry Potter and The Deathly](https://static.documents.pub/doc/80x56/612191065eaeea66235041c8/hermione-grangeras-act-of-equality-in-harry-potter-saga-movies-potter-and-the.jpg)













