Page 1
ORIGINAL ARTICLES
Acupuncture for Treating Common Side EffectsAssociated With Breast Cancer Treatment:
A Systematic Review
Stephanie Dos Santos, MSc,1 Nancy Hill, MSc,1 Ashley Morgan, MSc,1 Jenna Smith, MSc,1
Carolyn Thai, MSc,1 and Oren Cheifetz, MSc2
ABSTRACT
Background: Although breast cancer treatment is associated with improved survival rates, it is also associated
with numerous side effects, which can decrease overall quality of life for patients. Recent research indicates
acupuncture may be useful in decreasing the incidence and duration of some side effects associated with cancer
treatment.
Objective: To assess the evidence surrounding the role of acupuncture in treating side effects associated with
breast cancer treatment.
Design: Systematic review based on search of PubMed, EMBASE (1996 to 2009 week 17), AMED (1985 to
April 2009), and Ovid MEDLINE (1996 to April 2009) databases for relevant studies published up to April
2009. Authors of recent studies were contacted to determine if additional studies were taking place. Fourteen
articles were independently appraised by 4 blinded reviewers.
Results: Twelve studies met inclusion criteria: 9 investigated effects of traditional acupuncture and 3 addressed
electroacupuncture. Seven different side effects were examined (hot flashes, fatigue, pain, dyspnea, psycho-
logical well-being, decreased range of motion with lymphedema, and emesis). The findings support the po-
tential use of traditional acupuncture to decrease hot flashes, fatigue, and pain, whereas electroacupuncture may
be useful in treating emesis and hot flashes. There is a paucity of high-quality evidence to support the use of
acupuncture to treat dyspnea, emesis, and decreased range of motion with lymphedema or to improve psy-
chological well-being.
Conclusion: Current evidence suggests that traditional acupuncture may be useful in reducing hot flashes,
fatigue, and pain, whereas electroacupuncture may be useful in treating emesis and hot flashes. Due to limi-
tations in study designs and heterogeneity in treatment protocols, results should be viewed with caution and
combined with clinical reasoning.
Key Words: Acupuncture, Electroacupuncture, Breast Cancer, Side Effects
INTRODUCTION
Breast cancer is a life-threatening disease that
affects approximately 22,460 individuals in Canada
each year.1 Breast cancer is defined as cancer that has a site
of origin in tissues of the breast, usually occurring in the
ducts or lobules.1 Medical treatment is known to increase
survival rates in women with breast cancer but can also
1McMaster University, Hamilton, Ontario, Canada.2Hamilton Health Sciences, Hematology=Oncology Program, Hamilton, Ontario, Canada.
MEDICAL ACUPUNCTUREVolume 22, Number 2, 2010# Mary Ann Liebert, Inc.DOI: 10.1089=acu.2009.0730
81
Page 2
cause many harmful side effects.2-7 Such side effects
include, but are not limited to, nausea, vomiting, myelo-
suppression, fatigue, cognitive dysfunction, pain, and ac-
celerated menopause.3-5,8-10 Premature menopause can, in
turn, lead to night sweats, hot flashes, and sexual dysfunc-
tion.11,12 Due to the negative impact these side effects may
have on quality of life, appropriate treatment to control these
symptoms is recommended.12
Acupuncture is defined as ‘‘a therapeutic and=or pre-
ventive medical procedure performed by the insertion of one
or more specially manufactured solid metallic needle(s) into
specific location(s) on the body.’’13(p39) Since its introduc-
tion to the Western world from ancient China, acupuncture
has evolved to include various forms, including electro-
acupuncture (EA).14,15 Despite this, traditional Chinese
acupuncture is still the most prevalent theoretical frame-
work guiding acupuncture practice today.14,15
Adverse effects of acupuncture rarely occur. The risk of a
serious adverse reaction is approximately 0.05 per 10,000
treatments.16 Reported side effects range from local skin
irritation to pneumothorax and death and can include central
nervous system injury, infection (most commonly hepatitis
B), and extreme drowsiness.14-17 Although the overall in-
cidence of these side effects is very small, they can be
avoided if proper precautions are taken,14-16 such as using
appropriate sterile techniques and ensuring adequate acu-
puncturist training.17
Recent research has found that acupuncture may aid in
reducing the side effects of cancer treatment.18-20 The pur-
pose of this systematic review was to determine the effec-
tiveness of acupuncture as a treatment to manage the
common side effects in patients receiving treatment for
breast cancer.
METHODS
Data Source Location and Selection
PubMed, EMBASE (1996 to 2009 week 17), AMED
(1985 to April 2009), and Ovid MEDLINE (1996 to April
2009) databases were searched for relevant studies pub-
lished up to and including April 2009. Using the search
terms ‘‘[(acupuncture OR dry needle OR dry needling)
AND breast AND (cancer OR malignancy OR metastasis
OR neoplasm)],’’ 18 articles were found. Studies were in-
cluded if (1) the full article was accessible electronically or
in hard copy, (2) research was conducted using a primary
study design in the form of a randomized controlled trial
(RCT) or high-quality case series, (3) subjects included
those who had a primary diagnosis of breast cancer, (4) they
involved adult subjects (�18 years of age) with breast
cancer at any point during treatment for their disease,
(5) interventions included acupuncture with or without
electrical stimulation, and (6) acupuncture was used alone
or in combination with other forms of treatment as the
studied intervention. Studies were excluded if (1) the con-
trol group also received acupuncture or (2) acupressure was
used as the sole treatment in the intervention group. Nine
articles matched the inclusion=exclusion criteria, while the
other 9 articles did not.
After the initial search, references of retrieved articles
were reviewed. Five additional articles were found in this
manner. Thereafter, authors of the most recent articles were
contacted to inquire about any current research that might
contribute to or significantly alter any of the conclusions
made in this review. Responses from authors in Norway and
New York confirmed that all available studies had been
located, thereby ending the literature search. No language
restrictions were made; articles written in languages other
than English were translated, after which inclusion was
determined. In total, 14 articles were included for review.
Hard copies of all articles were retrieved and read in full.
Data Extraction and Synthesis
Following the search and collection of relevant research
studies by 2 reviewers ( J.S., O.C.), articles were given to
blinded reviewers for critical appraisal using the PEDro
scale, an 11-item scale initially developed to evaluate the
quality of RCTs in research relevant to physiotherapy
practice.21 This scale considers 2 aspects of the studies’
quality: internal validity and external validity.22 Scores can
range from 0-10 with higher scores representing better
methodological quality.21 Along with rating RCTs, this
scale has been previously used to evaluate other primary
clinical trial designs22,23; however, total scores are lower
due to the lack of subject randomization involved in these
designs. Past research has found the reliability of this rating
scale to be high when evaluating RCTs.21 This scale is not
used to evaluate systematic reviews or clinical practice
guidelines.21
Four reviewers (S.D., N.H., A.M., and C.T.) appraised
these articles in pairs. Each pair received and reviewed a
total of 7 articles. Disagreements among reviewers within
each pairing were resolved through discussion. Once all
critical appraisals were completed, 2 studies were elimi-
nated due to methodological issues: a retrospective chart
review narrating heterogeneous treatments and a case series
providing insufficient description of the intervention to al-
low for inclusion. Therefore, the following results include
10 RCTs and 2 case series. Interrater reliability of the
PEDro scale was determined by exchanging 2 articles be-
tween all 4 reviewers and comparing results. Interrater re-
liability was calculated using percentage agreement by
dividing the number of similar item scores (a) by the max-
imum possible PEDro score from both articles (b) and
then multiplying by 100 (a=b � 100). For this systematic
review, percentage agreement was calculated to be 95%
(19=20�100).
82 DOS SANTOS ET AL.
Page 3
Ta
bl
e1
.S
um
ma
ry
of
PE
Dr
oS
ca
le
sa
nd
Me
th
od
ol
og
ic
al
Qu
al
it
yfo
ra
ll
In
cl
ud
ed
St
ud
ie
s
So
urc
e
Ove
rall
PE
Dro
Sco
re*
Ra
nd
om
all
oca
tio
n
Co
nce
ale
d
all
oca
tio
n
Gro
up
s
sim
ila
r
Su
bje
ct
bli
nd
ing
Th
era
pis
t
bli
nd
ing
Ass
esso
r
bli
nd
ing
<1
5%
Dro
po
uts
Inte
nti
on
totr
eat
Bet
wee
n-g
rou
p
com
pa
riso
n
Va
ria
bil
ity
da
ta
Ho
tfl
ash
es
Den
get
al,2
52
00
78=1
0Y
esY
esN
oY
esN
oY
esY
esY
esY
esY
es
Fri
sket
al,2
82
00
84=1
0Y
esN
oY
esN
oN
oN
oN
oN
oY
esY
es
Her
vik
and
Mja
lan
d,2
42
00
89=1
0Y
esY
esY
esY
esN
oY
esY
esY
esY
esY
es
Ned
stra
nd
etal
,27
20
05
4=1
0Y
esY
esY
esN
oN
oN
oN
oN
oN
oY
es
Tu
km
ach
i,2
62
00
03=1
0N
oN
oN
oN
oN
oN
oY
esY
esN
oY
es
Fa
tig
ue
Mo
lass
ioti
set
al,2
92
00
77=1
0Y
esY
esN
oY
esN
oY
esN
oY
esY
esY
es
Pa
in Ali
mi
etal
,30
20
03
8=1
0Y
esY
esY
esY
esN
oY
esY
esN
oY
esY
es
Cre
wet
al,3
12
00
73=1
0Y
esN
oY
esN
oN
oN
oY
esN
oN
oN
o
Dy
spn
ea
Vic
ker
set
al,3
22
00
59=1
0Y
esY
esY
esY
esN
oY
esY
esY
esY
esY
es
Psy
cho
log
ica
lw
ell-
bei
ng
Ned
stra
nd
etal
,33
20
06
5=1
0Y
esY
esN
oN
oN
oN
oN
oY
esY
esY
es
Ra
ng
eo
fm
oti
on
an
dly
mp
hed
ema
Ale
man
dG
urg
el,3
42
00
82=1
0N
oN
oN
oN
oN
oN
oY
esN
oN
oY
es
Em
esis
Sh
enet
al,3
52
00
08=1
0Y
esY
esY
esN
oN
oY
esY
esY
esY
esY
es
*T
he
PE
Dro
scal
eis
an1
1-i
tem
scal
ed
evel
op
edto
eval
uat
eth
eq
ual
ity
of
rand
om
ized
con
tro
lled
tria
lsin
rese
arch
rele
van
tto
ph
ysi
oth
erap
yp
ract
ice.
21
83
Page 4
Ta
bl
e2
.S
um
ma
ry
of
Ac
upu
nc
tu
re
Tr
ea
tm
en
tfo
rIn
cl
ud
ed
St
ud
ie
s
So
urc
e(L
oca
tio
n)
Typ
eo
f
acu
pu
nct
ure
Du
rati
on
of
each
acu
pu
nct
ure
sess
ion
,m
in
No
.o
f
acu
pu
nct
ure
sess
ion
s
No
.o
f
po
ints
use
dS
pec
ific
po
ints
Ele
ctro
acu
pu
nct
ure
pa
ram
eter
s
Ho
tfl
ash
es
Den
get
al2
52
00
7
(US
A)
Tra
dit
ion
al2
08
19
DU
14
,G
B2
0,
BL
13
,P
C7
,
HT
6,
KI
7,
ST
36
,S
P6
,E
arS
hen
Men
,E
arsy
mp
ath
etic
po
int
NA
Fri
sket
al2
82
00
8
(Sw
eden
)
Ele
ctro
acu
pu
nct
ure
30
14
12
BL
15
,B
L2
3,
BL
32
bil
ater
ally
;
GV
20
,H
T7
,P
C6
,L
R3
,
SP
6,
SP
9u
nil
ater
ally
Sti
mu
late
dat
2H
zat
BL
23
and
BL
32
bil
ater
ally
Her
vik
and
Mja
lan
d,2
42
00
8
(No
rway
)
Tra
dit
ion
al3
01
58
LR
3,
GB
20
,L
U7
,K
I3
,S
P6
,
RE
N4
,P
C7
,L
R8
un
ilat
eral
ly
NA
Ned
stra
nd
etal
27
20
05
(Sw
eden
)
Ele
ctro
acu
pu
nct
ure
30
14
12
BL
15
,B
L2
3,
BL
32
bil
ater
ally
;
HT
7,
SP
6,
SP
9,
LR
3,
PC
6,
GV
20
un
ilat
eral
ly
Lo
w-b
urs
t2
-Hz
AC
curr
ent
to
elic
ita
no
np
ain
ful
loca
l
mu
scle
con
trac
tio
nat
BL
23
and
BL
32
bil
ater
ally
Tu
km
ach
i,2
6
20
00
(UK
)
Tra
dit
ion
al2
0–
30
6–
14
6-1
0p
oin
ts
sele
cted
fro
m
10
cho
sen
po
ints
BL
62
,L
R1
4,
KI
3,
HT
7,
TE
6,
SP
6,
LI
11
,S
T3
6,
GV
20
,
LI
4u
nil
ater
ally
NA
Fa
tig
ue
Mo
lass
ioti
set
al2
9
20
07
(UK
)
Tra
dit
ion
al2
06
6L
I4
,S
P6
,S
T3
6b
ilat
eral
lyN
A
Pa
in
Ali
mi
etal
30
20
03
(Fra
nce
)
Au
ricu
lar
acu
pu
nct
ure
Un
til
nee
dle
sfe
ll
ou
t(a
ver
age,
12
day
s)
2S
elec
ted
bas
edo
n
elec
tro
der
mal
resp
on
se
(av
erag
e,
6p
oin
ts)
NA
NA
84
Page 5
Cre
wet
al3
1
20
07
(US
A)
Tra
dit
ion
alan
d
auri
cula
r
30
12
6st
and
ard
ized
po
ints
plu
s
spec
ific
po
ints
for
up
to3
of
the
pat
ien
t’s
mo
stp
ain
ful
area
s(s
ho
uld
er,
wri
st,
fin
ger
s,
lum
bar
area
,
hip
,o
rk
nee
)
Sta
nd
ard
ized
po
ints
:T
B5
,G
B4
1,
GB
34
,L
I4
,S
T4
1,
KI
3
NA
Dy
spn
ea
Vic
ker
set
al3
2
20
05
(US
A)
Tra
dit
ion
al1
51
14
RE
N6
,S
tern
alp
oin
tsO
RR
EN
17
un
ilat
eral
ly;
LU
1,
LU
7,
ST
36
,K
I6
,A
uri
cula
rlu
ng
po
int,
Au
ricu
lar
kid
ney
po
int
bil
ater
ally
NA
Psy
cho
log
ica
lw
ell-
bei
ng
Ned
stra
nd
etal
33
20
06
(Sw
eden
)
Ele
ctro
acu
pu
nct
ure
30
14
12
BL
15
,B
L2
3,
BL
32
bil
ater
ally
;
HT
7,
SP
6,
SP
9,
LR
3,
PC
6,
GV
20
un
ilat
eral
ly
Lo
w-b
urs
t2
-Hz
AC
curr
ent
toel
icit
an
on
pai
nfu
llo
cal
mu
scle
con
trac
tio
nat
BL
23
and
BL
32
bil
ater
ally
Ra
ng
eo
fm
oti
on
an
dly
mp
hed
ema
Ale
man
dG
urg
el,3
4
20
08
(Bra
zil)
Tra
dit
ion
al3
02
41
1C
V1
2,
CV
3,
CV
2,
LI
15
,T
E1
4,
LU
5,
TE
5,
LI
4,
ST
36
,S
P9
,
SP
6u
nil
ater
ally
NA
Em
esis
Sh
enet
al3
5
20
00
(US
A)
Ele
ctro
acu
pu
nct
ure
20
44
PC
6,
ST
36
bil
ater
ally
Fre
qu
ency
2–
10
Hz,
pu
lse
wid
th
0.5
–0
.7m
illi
seco
nd
s,cu
rren
t
<2
6m
A,
var
iab
leD
C
NA
indic
ates
no
tap
pli
cab
le.
85
Page 6
RESULTS
Overall, 12 studies met the inclusion criteria and were
included in this systematic review, 5 of which were of higher
methodological quality (i.e., rated as Pedro score 8=10 or
greater) (Table 1).24-35 The specific parameters of acupunc-
ture treatment varied widely between studies (Table 2), as did
the outcome measures, and for this reason a meta-analysis
was not possible. Specific details of each study can be found
in Table 3. The following is a summary of each study’s
findings grouped according to the 8 primary outcomes in-
vestigated: hot flashes, fatigue, pain, dyspnea, psychological
well-being, range of motion and lymphedema, and emesis.
Hot Flashes
A large portion of the current evidence surrounding the
use of acupuncture in women with or recovering from breast
cancer is related to vasomotor symptoms, more specifically,
hot flashes. (The terms hot flash and hot flush were used
interchangeably between studies despite a common defini-
tion.) Five studies analyzing this symptom were included
for analysis, 2 of which were high-quality RCTs.
Three of the included studies investigated the effects of
traditional acupuncture on hot flash frequency. An RCT by
Hervik and Mjaland24 investigated the effectiveness of
traditional acupuncture in 59 women following breast can-
cer surgery. The mean number of hot flashes occurring
during both day and night was significantly reduced in the
traditional acupuncture group up to 12 weeks following
treatment.24 In the sham acupuncture group, a significant
reduction in hot flashes at night was found during treatment,
but at 12 weeks’ follow-up this effect was almost com-
pletely reversed.24 Differences between groups were sig-
nificant during treatment and at follow-up.
In another RCT, Deng et al25 compared the effects of
traditional acupuncture with placebo acupuncture on hot
flash frequency in 72 women undergoing treatment for
breast cancer. Although the true acupuncture group was
associated with 0.8 less hot flashes per day than the placebo
group at 6 weeks, this difference did not reach statistical
significance.25 This study also used a crossover design in
which women in the sham acupuncture group received true
acupuncture treatment after the initial study period.25 The
sham group experienced a further decrease in hot flash
frequency after receiving the true acupuncture protocol.25
Both groups continued to display decreased frequency of
hot flashes at 20 weeks.
Tukmachi26 investigated traditional acupuncture as a
treatment option for hot flashes in 22 patients with breast
cancer in a case series. In addition to acupuncture, partici-
pants were given lifestyle and diet advice to help reduce hot
flashes. Hot flash frequency during the day and night was
found to decrease significantly at the end of treatment and at
3-5 weeks.26
The remaining 2 studies investigated the efficacy of EA in
treating hot flashes. Nedstrand et al27 conducted an RCT
comparing the effects of EA with that of applied relaxation
therapy in 38 women who had completed breast cancer
treatment. Scores on the Kupperman Index (a scale used to
assess 11 menopausal symptoms) significantly improved in
both groups after 12 weeks of treatment and was maintained
at 6 months’ follow-up.27 No between-group comparisons
were made.
Frisk et al28 conducted an RCT comparing the effects of
12 weeks of EA with hormone therapy on hot flash fre-
quency and associated distress in 45 women who were ex-
periencing vasomotor symptoms due to previous cancer
treatment. Although the EA group experienced significant
decreases in hot flash frequency and distress at all time
points (12 weeks, 12 months, and 24 months), the authors
found a significant difference in favor of hormone therapy
for both hot flash frequency and distress at 12 months fol-
lowing treatment.28
Fatigue
Molassiotis et al29 conducted a pilot RCT to investigate
the effects of acupuncture and acupressure on cancer-related
fatigue in 47 patients. At the end of the 2-week intervention
period, both the acupuncture and acupressure group dem-
onstrated significant improvements on 4 of the 5 Multi-
dimensional Fatigue Inventory (MFI) subscales, most
notably the general fatigue subscale, while the sham acu-
puncture group did not.29 The improvements on this sub-
scale were significantly greater in the acupuncture group;
however, this difference did not remain statistically signif-
icant after 2 weeks of follow-up.29
Pain
Alimi et al30 investigated the effects of auricular acu-
puncture for the treatment of cancer pain in 90 patients
through an RCT.30 At trial days 30 and 60, the auricular
acupuncture group demonstrated a significant improvement
in pain scores compared with the placebo auricular acu-
puncture and placebo auricular seed groups.30 It is unknown
how long these effects were maintained because there was
no long-term follow up in this study.
Crew et al31 investigated the effects of traditional acu-
puncture on pain in 21 patients with breast cancer using a
crossover study design. After the initial 6 weeks, patients
undergoing acupuncture reported improvements in joint
stiffness, pain, physical function, and quality of life, while
the observation group reported worsening of symptoms.31
The immediate acupuncture group did not maintain im-
provements after 6 weeks of observation, while the delayed
acupuncture group demonstrated improvements after re-
ceiving 6 weeks of acupuncture.31 No between-group
comparisons were made.
86 DOS SANTOS ET AL.
Page 7
Ta
bl
e3
.O
ut
co
me
so
f1
2S
tu
die
sIn
cl
ud
ed
in
th
eF
in
al
Re
vie
w
So
urc
e
Sa
mp
lesi
ze
an
dd
eta
ils
Fo
llo
w-u
pIn
clu
sio
ncr
iter
iaT
rea
tmen
tg
rou
pC
om
pa
riso
ng
rou
pO
utc
om
em
easu
res
Ma
inre
sult
s
Ho
tfl
ash
es
Den
get
al2
5
20
07
N¼
72
Mea
n
(ran
ge)
age,
55
(48
-59
)y
20
wee
ks
Fem
ale;
rece
ivin
g
trea
tmen
tfo
rb
reas
t
can
cer;
Kar
no
fsk
y
per
form
ance
sco
re
>6
0;
aver
age
of�
3h
ot
flas
hes
per
day
du
rin
ga
1-w
eek
bas
elin
ed
iary
Tru
eac
up
un
ctu
re
gro
up
(n¼
42
):
acu
pu
nct
ure
2x=w
eek
,fo
r4
wee
ks;
Sh
amac
up
un
ctu
re
gro
up
rece
ived
the
tru
eac
up
un
ctu
re
trea
tmen
t2
wee
ks
afte
rco
mp
leti
ng
sham
trea
tmen
t
Sh
amac
up
un
ctu
re
gro
up
(n¼
30
):
retr
acta
ble
nee
dle
s
pla
ced
afe
w
cen
tim
eter
saw
ay
fro
mth
ep
oin
tsu
sed
inth
etr
ue
acu
pu
nct
ure
gro
up
2x=w
eek
,fo
r4
wee
ks
Dai
lyd
iary
reco
rdin
go
fh
ot
flas
hfr
equ
ency
At
6w
eeks
mea
nN
o.
of
hot
flas
hes=day
dec
reas
edfr
om
8.7�
3.9
to6.2�
4.2
for
true
acupunct
ure
and
from
10.0�
6.1
to7.6�
5.7
for
sham
.T
rue
acupunct
ure
gro
up
exper
ience
d0.8
less
hot
flas
hes=day
(not
stat
isti
call
ysi
gnifi
cant)
Sham
gro
up
exper
ience
da
furt
her
dec
reas
ein
the
num
ber
of
hot
flas
hes=
day
afte
rcr
oss
ing
over
to
true
acupunct
ure
trea
tmen
t
Both
gro
ups
conti
nued
a
dec
reas
ein
dai
lyhot
flas
hes
at20
wee
ks
post
foll
ow
-up
Fri
sket
al2
8
20
08
N¼
45
Mea
nag
e,
EA
:5
6.5
y
HT
:5
3.4
y
24
mo
nth
sF
emal
e;co
mp
lete
d
trea
tmen
tfo
rb
reas
t
can
cer
insi
tu,
T1
and
T2
tum
ors
wit
h�
4
lym
ph
no
des
po
siti
ve
for
met
asta
sis;
no
rep
ort
edsi
gn
so
f
recu
rren
ceo
r
vas
om
oto
rsy
mp
tom
s
req
uir
ing
trea
tmen
t
Ele
ctro
acu
pu
nct
ure
(EA
)g
rou
p
(n¼
27
):E
A
2x=w
eek
for
2w
eek
sfo
llo
wed
by
1x=w
eek
for
10
wee
ks
Ho
rmo
ne
ther
apy
(HT
)
gro
up
(n¼
18
):
ind
ivid
ual
lych
ose
n
by
ag
yn
eco
log
ist
Dai
lylo
go
fh
ot
flas
hfr
equ
ency
and
dis
turb
ance
(0–
10
)
KI
At
end
of
trea
tmen
td
ecre
ase
inm
edia
nN
o.
of
ho
t
flas
hes
:E
A9
.6to
4.3
(P<
.00
1),
HT
6.6
to0
.0
(P¼
.00
1)
and
ind
istr
ess:
EA
5.5
to2
.4(P<
.00
1),
HT
5.0
to0
.00
(P¼
.00
1)
At
12
mo
nth
sH
Tg
rou
ph
ad
sig
nifi
can
tly
dec
reas
edh
ot
flas
hfr
equ
ency
,
dis
turb
ance
,an
dK
Isc
ore
s
vs
EA
gro
up
EA
had
sig
nifi
can
td
ecre
ases
inN
o.
of
ho
tfl
ash
esin
foll
ow
-up
,an
dsi
gn
ifica
nt
dec
reas
ein
dis
tres
sat
12
wee
ks,
12
and
24
mo
nth
s
(co
nti
nu
ed)
87
Page 8
Ta
bl
e3
.(C
on
tin
ue
d)
So
urc
e
Sa
mp
lesi
ze
an
dd
eta
ils
Fo
llo
w-u
pIn
clu
sio
ncr
iter
iaT
rea
tmen
tg
rou
pC
om
pa
riso
ng
rou
pO
utc
om
em
easu
res
Ma
inre
sult
s
Her
vik
and
Mja
lan
d,2
4
20
08
N¼
59
Mea
nag
e,
TA
:
53
.6�
6.4
y
SA
: 52
.3�
6.9
y
12
wee
ks
Fem
ale;
po
stm
eno
pau
sal;
tam
ox
ifen
for�
3
mo
nth
s;co
mp
lain
ing
of
ho
tfl
ash
esaf
ter
bre
ast
can
cer
surg
ery
;
com
ple
ted
any
po
sto
per
ativ
era
dia
tio
n
and=o
rch
emo
ther
apy
Tra
dit
ion
al
acu
pu
nct
ure
gro
up
(n¼
30
):
acu
pu
nct
ure
2x=w
eek
for
5
wee
ks,
then
1x=w
eek
for
ano
ther
5w
eek
s
Sh
amac
up
un
ctu
re
gro
up
(n¼
29
):
sham
acu
pu
nct
ure
at
4p
oin
tsb
ilat
eral
ly
far
away
fro
mtr
ue
po
ints
2x=w
eek
for
5w
eek
s,th
en
1x=w
eek
for
ano
ther
5w
eek
s
KI
Rec
ord
edN
o.
of
ho
tfl
ash
esat
day
and
nig
ht
No
.o
fh
ot
flas
hes
du
rin
gth
e
day
was
red
uce
db
y5
0%
(P<
.00
1)
wit
htr
ue
acu
pu
nct
ure
,w
ith
afu
rth
er
30
%re
du
ctio
n(P<
.01
7)
du
rin
gfo
llo
w-u
p
No
sig
nifi
can
tch
ang
esin
sham
gro
up
No
.o
fh
ot
flas
hes
atn
igh
tin
the
tru
eac
up
un
ctu
reg
rou
p
was
red
uce
db
y6
0%
(P<
.00
1)
wit
ha
furt
her
30
%re
du
ctio
n(P<
.00
6)
du
rin
gfo
llo
w-u
p
No
.o
fh
ot
flas
hes
atn
igh
tin
sham
gro
up
sig
nifi
can
tly
red
uce
db
y2
5%
(P¼
.01
)
du
rin
gtr
eatm
ent,
no
lon
ger
sig
nifi
can
tan
dal
mo
st
enti
rely
rev
erse
dd
uri
ng
foll
ow
-up
(P¼
.22
)
Ned
stra
nd
etal
27
20
05
N¼
38
Mea
n
(ran
ge)
age:
53
(30
-64
)y
6m
on
ths
Fem
ale;
men
op
ausa
l;
com
ple
ted
trea
tmen
tfo
r
bre
ast
can
cer
(ex
cep
t
tam
ox
ifen
,st
ill
on
go
ing
in8
wo
men
);m
od
erat
e
tose
ver
ev
aso
mo
tor
sym
pto
ms;�
2h
ot
flas
hes=2
4h
ou
rs
EA
gro
up
(n¼
19
):E
A
2x=w
eek
for
2
wee
ks,
then
1x=w
eek
for
10
wee
ks
Ap
pli
edre
lax
atio
n
gro
up
(n¼
19
):
rela
xat
ion
trai
nin
g
insm
all
gro
up
s,1
-
ho
ur
sess
ion
s
1x=w
eek
for
12
wee
ks
plu
sd
aily
self
-ad
min
iste
red
sess
ion
s
Lo
gb
oo
ko
fN
o.
of
ho
tfl
ash
es
KI
No
.o
fh
ot
flas
hes
dec
reas
ed
sig
nifi
can
tly
vs
bas
elin
ein
bo
thg
rou
ps
afte
rtr
eatm
ent
and
at6
mo
nth
s(P<
.00
1)
KI
sco
resi
gn
ifica
ntl
yre
du
ced
afte
rtr
eatm
ent
inb
oth
gro
up
san
dre
mai
ned
un
chan
ged
at6
mo
nth
s
Tu
km
ach
i,2
6
20
00
N¼
22
Mea
n
(ran
ge)
age:
50
(38
-59
)y
3–
5w
eek
sD
iag
no
sed
wit
hb
reas
t
can
cer;
refe
rred
for
acu
pu
nct
ure
trea
tmen
t
of
ho
tfl
ash
esth
at
dis
turb
edsl
eep
and
soci
alac
tiv
itie
s
Tra
dit
ion
al
acu
pu
nct
ure
2x=w
eek
for
up
to7
wee
ks
No
ne
Ho
tfl
ash
dia
ryA
ver
age
No
.o
fh
ot
flas
hes=d
aysi
gn
ifica
ntl
y
red
uce
dd
uri
ng
the
day
fro
m1
4.3
2at
bas
elin
eto
1.4
1af
ter
last
trea
tmen
t,
and
atn
igh
tfr
om
6.9
5to
0.8
6(P<
.00
1)
Red
uct
ion
sm
ain
tain
edat
foll
ow
-up
and
stil
l
sig
nifi
can
tco
mp
ared
wit
h
bas
elin
e(P<
.00
1)
88
Page 9
Fa
tig
ue
Mo
lass
ioti
s
etal
29
20
07
N¼
47
Mea
n(r
ang
e)
age:
53
.4
(20
–76
)y
2w
eek
sA
du
lts
dia
gn
ose
dw
ith
any
typ
eo
fca
nce
r;
com
ple
ted
chem
oth
erap
y�
1
mo
nth
bef
ore
;sc
ore
of
�5
on
MF
I;an
tici
pat
ed
surv
ival>
3m
on
ths;
no
tsc
hed
ule
dto
rece
ive
any
mo
re
can
cer
trea
tmen
ts
du
rin
gth
est
ud
yp
erio
d
Acu
pu
nct
ure
gro
up
(n¼
15
):
acu
pu
nct
ure
3x=
wee
k,
for
2
wee
ks
(fem
ale:
n¼
9,
bre
ast
can
cer:
n¼
4)
Acu
pre
ssu
reg
rou
p
(n¼
16
):se
lf-
acu
pre
ssu
refo
r1
min
ute=d
ayat
each
acu
pu
nct
ure
gro
up
po
int
for
2w
eek
s
(fem
ale:
n¼
12
,
bre
ast
can
cer:
n¼
6)
Sh
amac
up
ress
ure
gro
up
(n¼
16
):se
lf-
acu
pre
ssu
reat
pla
ceb
op
oin
tsin
the
sam
em
ann
eras
the
acu
pre
ssu
reg
rou
p
(fem
ale:
n¼
11
,
bre
ast
can
cer:
n¼
5)
MF
IF
atig
ue
sco
res
sig
nifi
can
tly
imp
rov
edin
the
trea
tmen
t
gro
up
sin
4=5
of
the
MF
I
sub
scal
es:
gen
eral
fati
gu
e
(P<
.00
1),
ph
ysi
cal
fati
gu
e
(P¼
.01
6),
acti
vit
y
(P¼
.04
),an
dm
oti
vat
ion
(P¼
.02
4)
atth
een
do
f
trea
tmen
t
Aft
ertr
eatm
ent
acu
pu
nct
ure
gro
up
had
sig
nifi
can
tly
hig
her
imp
rov
emen
t(3
6%
)
ing
ener
alfa
tig
ue
vs
acu
pre
ssu
re(1
9%
)an
d
sham
(0.6
%)
gro
up
s
Imp
rov
emen
tsre
mai
ned
at2
wee
ks
bu
tn
ot
asla
rge
(22
%,
15
%,
and
7%
,
resp
ecti
vel
y);
acu
pu
nct
ure
no
lon
ger
sig
nifi
can
tly
dif
fere
nt
Acu
pu
nct
ure
gro
up
also
had
sig
nifi
can
tly
hig
her
imp
rov
emen
tin
men
tal
fati
gu
eth
anth
eo
ther
gro
up
sat
the
end
of
trea
tmen
t
Pa
in
Ali
mi
etal
30
20
03
N¼
90
Mea
n(r
ang
e)
age:
57
(37
–84
)y
Var
iab
le
bas
edo
n
wh
enth
e
nee
dle
so
r
seed
sfe
ll
off
Ad
ult
sre
qu
irin
gtr
eatm
ent
for
chro
nic
per
iph
eral
or
cen
tral
neu
rop
ath
ic
pai
nar
isin
gaf
ter
trea
tmen
to
fca
nce
r;
pai
nV
AS
val
ue�
30
des
pit
ean
alg
esic
trea
tmen
tfo
r�
1m
on
th
bef
ore
Au
ricu
lar
acu
pu
nct
ure
gro
up
(n¼
29
):2
cou
rses
of
auri
cula
r
acu
pu
nct
ure
ov
er
*2
mo
nth
sat
po
ints
wh
ere
an
elec
tro
der
mal
sig
nal
had
bee
nd
etec
ted
(fem
ale:
n¼
20
,b
reas
t
can
cer:
n¼
16
)
Pla
ceb
oau
ricu
lar
acu
pu
nct
ure
gro
up
(n¼
30
):sa
me
as
auri
cula
rg
rou
pat
pla
ceb
op
oin
ts
(fem
ale:
n¼
27
,
bre
ast
can
cer:
n¼
14
)
Pla
ceb
oau
ricu
lar
seed
gro
up
(n¼
31
):
sam
eas
auri
cula
r
wit
hse
eds
at
pla
ceb
op
oin
ts
(fem
ale:
n¼
23
,
bre
ast
can
cer:
n¼
15
)
Pai
no
nV
AS
At
day
30
,p
ain
sco
res
wer
e
sig
nifi
can
tly
low
erin
the
auri
cula
rac
upunct
ure
gro
up
(mea
n�
SD
,
44�
19
)th
anin
eith
erth
e
pla
ceb
o(5
4�
25
)o
rse
ed
(56�
19
)g
rou
ps
(P¼
.02
)
At
day
60
,p
ain
sco
res
wer
e
sig
nifi
can
tly
low
erin
the
auri
cula
rac
upunct
ure
gro
up
(37�
19
)th
anin
eith
erth
ep
lace
bo
(55�
24
)o
rth
ese
edg
rou
p
(58�
20
)(P<
.00
1)
(co
nti
nu
ed)
89
Page 10
Ta
bl
e3
.(C
on
tin
ue
d)
So
urc
e
Sa
mp
lesi
zea
nd
det
ail
sF
oll
ow
-up
Incl
usi
on
crit
eria
Tre
atm
ent
gro
up
Co
mp
ari
son
gro
up
Ou
tco
me
mea
sure
sM
ain
resu
lts
Cre
wet
al3
1
20
07
N¼
21
Mea
n(r
ang
e)ag
e:
59
(46
–7
3)
y
Cro
sso
ver
stu
dy
Fem
ale;
po
stm
eno
pau
sal;
his
tory
of
stag
eI,
II,
or
IIIa
ho
rmo
ne
rece
pto
r–
po
siti
ve
bre
ast
can
cer;
curr
entl
yta
kin
gth
ird
-
gen
erat
ion
aro
mat
ase
inh
ibit
or
for
the
pas
t6
mo
nth
s
Imm
edia
te
acu
pu
nct
ure
gro
up
(n¼
no
tsp
ecifi
ed):
trad
itio
nal
and
auri
cula
r
acu
pu
nct
ure
2x=w
eek
,fo
r6
wee
ks,
foll
ow
edb
y
6w
eek
so
f
ob
serv
atio
n
Del
ayed
acu
pu
nct
ure
gro
up
(n¼
no
t
spec
ified
):o
bse
rved
for
6w
eek
s,th
en
rece
ived
trad
itio
nal
and
auri
cula
r
acu
pu
nct
ure
2x=w
eek
,fo
r6
wee
ks
BP
I-S
F
WO
MA
C
FA
CT
-G
Tel
eph
on
e
inte
rvie
ws
Fro
m0
–6
wee
ks,
the
imm
edia
teg
rou
pre
po
rted
imp
rov
emen
tsin
join
t
stif
fnes
san
dp
ain
,p
hy
sica
l
fun
ctio
n,
and
qu
alit
yo
fli
fe
bu
tth
ese
imp
rov
emen
ts
did
no
tla
st
Del
ayed
gro
up
rep
ort
ed
wo
rsen
ing
of
sym
pto
ms
for
firs
t6
wee
ks,
foll
ow
edb
y
rep
ort
edim
pro
vem
ent
wit
h
the
init
iati
on
of
acu
pu
nct
ure
Bo
thg
rou
ps
had
sig
nifi
can
t
imp
rov
emen
tsin
wo
rst
pai
n(P¼
.00
8),
pai
n
sev
erit
y(P¼
.02
2),
and
pai
n-r
elat
edin
terf
eren
ce
(P¼
.01
5)
on
BP
I-S
Fas
wel
las
on
the
WO
MA
C
fun
ctio
nsu
bsc
ale
(P¼
.01
9)
and
the
FA
CT
-Gp
hy
sica
l
wel
l-b
ein
gsu
bsc
ale
(P¼
.03
)
Dy
spn
ea
Vic
ker
s
etal
32
20
05
N¼
47
Mea
n(S
D)
age:
tru
eac
up
un
ctu
re,
63
(12
.8);
sham
,6
7
(11
.4)
y
1w
eek
�1
8y
ears
;d
iag
no
sed
wit
hb
reas
to
rlu
ng
can
cer;
com
pla
ints
of
short
nes
sof
bre
ath;
gra
de
2o
rg
reat
ero
n
Am
eric
anT
ho
raci
c
So
ciet
yB
reat
hle
ssn
ess
scal
e
Tru
eac
up
un
ctu
re
gro
up
(n¼
25
):1
sess
ion
of
acu
pu
nct
ure
foll
ow
edb
y
trea
tmen
tw
ith
acu
pre
ssu
rest
ud
s1
ho
ur
po
stn
eed
le
rem
ov
al(f
emal
e:
n¼
15
,b
reas
t
can
cer:
n¼
5)
Ad
vis
edto
app
ly
pre
ssu
reto
each
stu
d
atle
ast
2x=d
ayfo
r
1-2
min
ute
s
Sh
amac
up
un
ctu
re
gro
up
(n¼
22
):
retr
acta
ble
nee
dle
s
atp
lace
bo
po
ints
foll
ow
edb
yp
lace
bo
acu
pre
ssu
rest
ud
s
(fem
ale:
n¼
13
,
bre
ast
can
cer
n¼
4)
Ad
vis
edto
app
ly
pre
ssu
reto
the
pla
ceb
ost
ud
sin
the
sam
em
ann
eras
tru
e
acu
pu
nct
ure
gro
up
Lev
elo
fd
ysp
nea
rate
do
na
0-1
0
scal
e;
dai
lyd
ysp
nea
dia
ry
Bo
thg
rou
ps
sig
nifi
can
tly
imp
rov
edim
med
iate
ly
afte
rtr
eatm
ent
(P¼
.00
3)
bu
tn
osi
gn
ifica
nt
dif
fere
nce
sb
etw
een
gro
up
s
Dy
spn
easc
ore
ssl
igh
tly
hig
her
intr
ue
acu
pu
nct
ure
gro
up
bo
thim
med
iate
ly
foll
ow
ing
acu
pu
nct
ure
and
1w
eek
foll
ow
-up
90
Page 11
Psy
cho
log
ica
lw
ell-
bei
ng
Ned
stra
nd
etal
33
20
06
N¼
38
Mea
n(r
ang
e)ag
e:
53
(30
–6
4)
y
6m
on
ths
Fem
ale;>
6m
on
ths
sin
ce
last
men
stru
atio
n;
des
irin
gtr
eatm
ent
for
vas
om
oto
rsy
mp
tom
s;
>2
ho
tfl
ash
es=d
ay,
ho
t
flas
hes
con
sid
ered
sev
ere
eno
ug
hto
req
uir
etr
eatm
ent
EA
gro
up
(n¼
19
):E
A
2x=w
eek
for
the
firs
t
2w
eek
s,th
en
1x=w
eek
for
10
wee
ks
Ap
pli
edre
lax
atio
n
gro
up
(n¼
19
):
rela
xat
ion
trai
nin
g
insm
all
gro
up
s,1
-
ho
ur
sess
ion
1x=w
eek
for
12
wee
ks
plu
sd
aily
self
-ad
min
iste
red
sess
ion
s
KI
VA
S
SC
L
Mo
od
Sca
le
At
6m
on
ths
KI,
VA
S,
and
SC
Lsc
ore
sd
ecre
ased
sig
nifi
can
tly
fro
m
bas
elin
ein
bo
thg
rou
ps
(P<
.00
1)
EA
had
sig
nifi
can
t
imp
rov
emen
tin
mo
od
fro
mb
asel
ine
to
end
of
foll
ow
-up
(P<
.05
)
No
sig
nifi
can
td
iffe
ren
ces
bet
wee
ng
rou
ps
[no
te:
this
stu
dy
also
rep
ort
ed
dat
are
gar
din
gh
ot
flas
hes
wh
ich
was
also
rep
ort
ed
else
wh
ere,
see
Ned
stra
nd
20
05
abo
ve]
Ra
ng
eo
fm
oti
on
an
dly
mp
hed
ema
Ale
man
d
Gu
rgel
,34
20
08
N¼
29
Mea
n(r
ang
e)ag
e:
61
.9
(43
-92
)y
No
ne
Fem
ale;
un
der
go
ne
un
ilat
eral
bre
ast
can
cer
surg
ery
wit
hax
illa
ry
lym
ph
no
de
dis
sect
ion
�6
mo
nth
sb
efo
re;
lym
ph
edem
aan
d=o
r
rest
rict
ion
of�
208
in
sho
uld
erab
du
ctio
no
r
flex
ion
on
surg
ical
sid
e
Acu
pu
nct
ure
con
tral
ater
alto
surg
ical
sid
ew
eek
ly
for
24
wee
ks
(*6
mo
nth
s)
No
ne
Ly
mp
hed
ema
deg
ree
and
mea
sure
men
t
Sh
ou
lder
RO
M
VA
S
Sh
ou
lder
RO
Min
abd
uct
ion
imp
rov
edsi
gn
ifica
ntl
yin
thir
dm
on
th(P¼
.00
2)
and
flex
ion
insi
xth
mo
nth
(P<
.00
1),
reac
hed
no
rmal
val
ues
by
end
of
trea
tmen
t
Hea
vin
ess
and
tig
htn
ess
in
the
affe
cted
up
per
lim
b
sig
nifi
can
tly
imp
rov
ed
fro
mb
asel
ine
toen
do
f
trea
tmen
t(P<
.00
1)
Deg
ree
of
lym
ph
edem
ara
tin
g
sig
nifi
can
tly
imp
rov
ed
fro
mb
asel
ine
toen
do
f
trea
tmen
t
(P¼
.01
6)
No
sig
nifi
can
tch
ang
esin
lym
ph
edem
a
mea
sure
men
ts
(co
nti
nu
ed)
91
Page 12
Ta
bl
e3
.(C
on
tin
ue
d)
So
urc
e
Sa
mp
lesi
ze
an
dd
eta
ils
Fo
llo
w-u
pIn
clu
sio
ncr
iter
iaT
rea
tmen
tg
rou
pC
om
pa
riso
ng
rou
pO
utc
om
em
easu
res
Ma
inre
sult
s
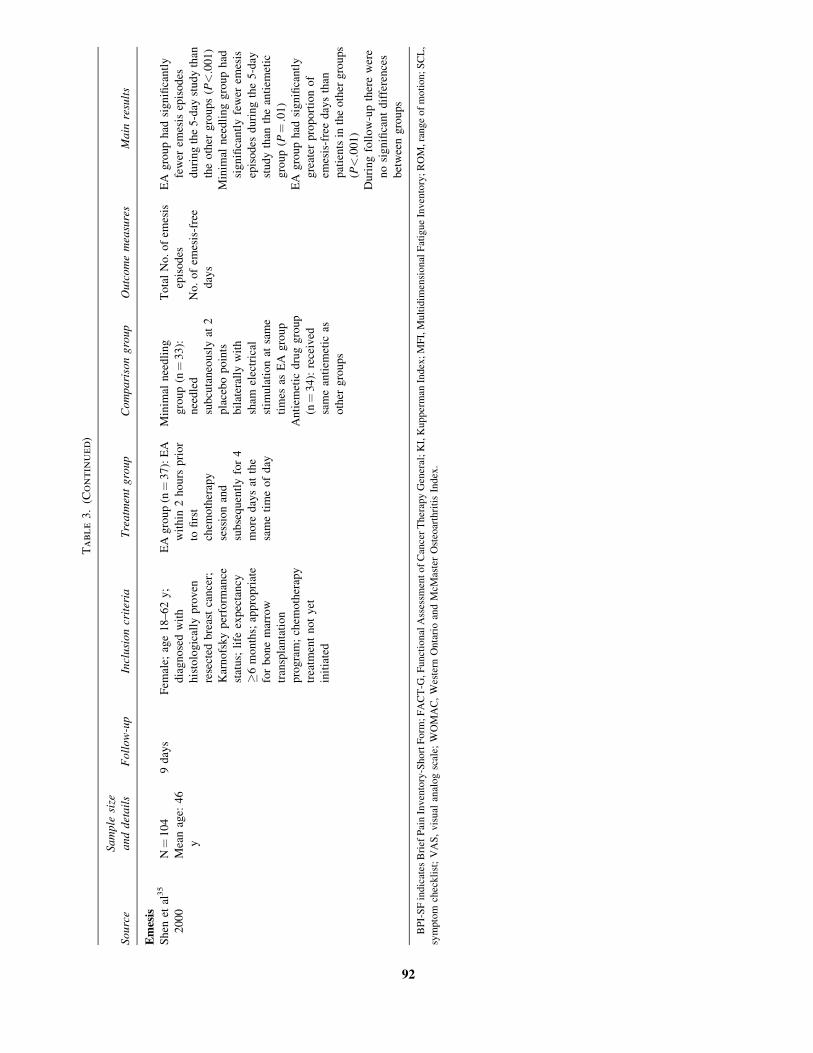
Em
esis
Sh
enet
al3
5
20
00
N¼
10
4
Mea
nag
e:4
6
y
9d
ays
Fem
ale;
age
18
–6
2y
;
dia
gn
ose
dw
ith
his
tolo
gic
ally
pro
ven
rese
cted
bre
ast
can
cer;
Kar
no
fsk
yp
erfo
rman
ce
stat
us;
life
exp
ecta
ncy
�6
mo
nth
s;ap
pro
pri
ate
for
bo
ne
mar
row
tran
spla
nta
tio
n
pro
gra
m;
chem
oth
erap
y
trea
tmen
tn
ot
yet
init
iate
d
EA
gro
up
(n¼
37
):E
A
wit
hin
2h
ou
rsp
rio
r
tofi
rst
chem
oth
erap
y
sess
ion
and
sub
seq
uen
tly
for
4
mo
red
ays
atth
e
sam
eti
me
of
day
Min
imal
nee
dli
ng
gro
up
(n¼
33
):
nee
dle
d
sub
cuta
neo
usl
yat
2
pla
ceb
op
oin
ts
bil
ater
ally
wit
h
sham
elec
tric
al
stim
ula
tio
nat
sam
e
tim
esas
EA
gro
up
An
tiem
etic
dru
gg
rou
p
(n¼
34
):re
ceiv
ed
sam
ean
tiem
etic
as
oth
erg
rou
ps
To
tal
No
.o
fem
esis
epis
od
es
No
.o
fem
esis
-fre
e
day
s
EA
gro
up
had
sig
nifi
can
tly
few
erem
esis
epis
od
es
du
rin
gth
e5
-day
stu
dy
than
the
oth
erg
rou
ps
(P<
.00
1)
Min
imal
nee
dli
ng
gro
up
had
sig
nifi
can
tly
few
erem
esis
epis
od
esd
uri
ng
the
5-d
ay
stu
dy
than
the
anti
emet
ic
gro
up
(P¼
.01
)
EA
gro
up
had
sig
nifi
can
tly
gre
ater
pro
po
rtio
no
f
emes
is-f
ree
day
sth
an
pat
ien
tsin
the
oth
erg
rou
ps
(P<
.00
1)
Du
rin
gfo
llo
w-u
pth
ere
wer
e
no
sig
nifi
can
td
iffe
ren
ces
bet
wee
ng
rou
ps
BP
I-S
Fin
dic
ates
Bri
efP
ain
Inv
ento
ry-S
ho
rtF
orm
;F
AC
T-G
,F
unct
ion
alA
sses
smen
to
fC
ance
rT
her
apy
Gen
eral
;K
I,K
up
per
man
Ind
ex;
MF
I,M
ult
idim
ensi
on
alF
atig
ue
Inv
ento
ry;
RO
M,ra
ng
eo
fm
oti
on
;S
CL
,
sym
pto
mch
eckli
st;
VA
S,
vis
ual
anal
og
scal
e;W
OM
AC
,W
este
rnO
nta
rio
and
McM
aste
rO
steo
arth
riti
sIn
dex
.
92
Page 13
Dyspnea
One RCT conducted by Vickers et al32 investigated the
role of a single session of acupuncture, followed by acu-
pressure, in dyspnea management of 47 patients with ad-
vanced lung or breast cancer. Significant improvements
were noted in both the true and placebo acupuncture=acupressure groups; however, no significant between-group
differences were found.
Psychological Well-being
A second paper by Nedstrand et al33 reported the effects
of EA compared with applied relaxation on psychological
well-being in 38 women experiencing hot flashes due to
breast cancer treatment. The authors found a significant
improvement in mood (as measured by a mood scale) from
baseline to the end of follow-up at 6 months in the EA
group.33 There were no significant differences between
groups.
ROM and Lymphedema
Alem and Gurgel34 investigated the effects of acupunc-
ture on range of motion and lymphedema in 29 women after
breast cancer surgery through a case series. Range of
shoulder flexion and abduction, degree of lymphedema
(visual inspection and palpation), and visual analog scale
ratings of perceived feelings of heaviness or tightness all
demonstrated significant improvement after traditional
acupuncture treatment.34
Emesis
Shen et al35 investigated the effects of EA on emesis in
104 women with breast cancer in an RCT. The EA group
experienced significantly fewer episodes of emesis and a
greater proportion of emesis-free days compared with the
other 2 groups over the course of the trial.35 The minimal
needling group also had significantly fewer episodes of
emesis than the control group. At 9 days’ follow-up,
however, differences between groups were no longer sig-
nificant.
DISCUSSION
Of the 12 studies included for analyses, 2 different types
of acupuncture were considered: traditional acupuncture
and EA. Seven cancer-related outcomes were assessed: hot
flashes, fatigue, pain, dyspnea, psychological well-being,
decreased range of motion with lymphedema, and emesis.
Six studies assessing hot flashes, fatigue, pain, dyspnea, and
emesis had a PEDro score of 8=10 or higher. While acu-
pressure was not explicitly analyzed, 2 studies identified in
our search used acupressure either adjunctively or in com-
parison with traditional acupuncture.
Traditional Acupuncture
The effects of traditional acupuncture on vasomotor
symptoms were analyzed through 3 studies. Hervik et al24
found statistically significant improvements in reducing hot
flash frequency, with effects persisting 12 weeks following
treatment. Deng et al25 also found an improvement in hot
flashes with traditional acupuncture; however, results were
not statistically significant. Tukmachi26 found statistically
significant improvements in the reduction of hot flash fre-
quency; however, the study was of low methodological
quality. This study failed to use a true control group or
specify the details of the lifestyle and diet advice included in
the intervention, and the independent effects of each on hot
flashes.26 Overall, these results are consistent with a review
investigating the role of acupuncture in cancer care, which
concluded that acupuncture demonstrated positive effects
on reducing vasomotor symptoms, while its long-term ef-
ficacy is questionable.36 The North American Menopause
Society’s Position Statement does not currently recommend
acupuncture for the treatment of menopause-associated
vasomotor symptoms, stating there are currently insufficient
clinical trials to merit its use.37 Therefore, while individual
trials have shown that traditional acupuncture is effective at
reducing hot flash frequency and intensity in women with
breast cancer, further studies are recommended to
strengthen findings and assess long-term efficacy.
Based on the results of one high-quality RCT by
Molassiotis et al,29 traditional acupuncture was found to
have positive short-term effects on fatigue. It is question-
able, however, whether a placebo effect may have occurred
due to the increased attention the acupuncture group re-
ceived in comparison with the other treatment groups.
Furthermore, the authors of this study noted that patients in
the acupuncture group may not have received a sufficient
number of treatments to allow for sustained benefits, and for
this reason, future research involving longer treatment pe-
riods are recommended. Also, the results of this study must
be applied with caution to patients with breast cancer be-
cause participants had a heterogeneous sample of cancer
diagnoses, only 32% of which represented breast cancer.29
The results from this study are consistent with a review that
concluded there is little evidence to suggest that the benefits
of acupuncture for cancer-related fatigue last over time.36
Therefore, while its long-term effects are questionable,
traditional acupuncture may be appropriate to explore as a
component of multidimensional care for temporarily ame-
liorating fatigue due to breast cancer treatment.
The effects of acupuncture on pain were analyzed in 2
studies. Alimi et al30 concluded that auricular acupuncture
was effective at reducing neuropathic pain; however, no
long-term follow-up was conducted to assess if these effects
were maintained over time. The results of a study conducted
by Crew et al31 also indicated that traditional acupuncture
was effective at decreasing pain in patients with breast
BREAST CANCER TREATMENT 93
Page 14
cancer for a short duration; however, the study was of lower
methodological quality and included a small sample size.
This study’s lack of a placebo control group and failure to
retain positive findings following treatment indicate that the
positive results could be due to a placebo effect. Therefore,
while there is some evidence to suggest that traditional
acupuncture may improve pain due to breast cancer, future
studies are recommended to strengthen these findings, es-
pecially in regard to its long-term use. This conclusion is
supported by systematic reviews.38,39 While further re-
search needs to be conducted, acupuncture may be consid-
ered an alternative treatment option for patients who refuse
to use narcotics and desire a less sedating and constipating
alternative to relieve pain.38
With respect to dyspnea, Vickers et al32 found that a
single session of traditional acupuncture, followed by acu-
pressure, was no better at reducing symptoms than placebo.
The study was of high methodological quality; however, the
treatment protocol implemented in this study was not re-
flective of typical clinical practice, as standard acupuncture
treatment typically involves more than one session. Fur-
thermore, the majority of the patients in this study had a
diagnosis of lung cancer, which limits the generalizability of
these findings to the breast cancer population. Overall, the
study’s findings are consistent with a review concluding that
results have not yet confirmed the efficacy of acupuncture in
reducing symptoms of dyspnea in patients with breast can-
cer, thereby rendering a need for further research in this
area.36
Lastly, positive effects were noted in 2 separate studies by
Nedstrand et al33 and Alem and Gurgel34 examining psy-
chological well-being and decreased range of motion with
lymphedema, respectively. The results of these studies must
be considered with caution since they both demonstrated
poor research methodologies, lack of comparison groups,
inadequate=absent follow-ups, and=or failure to retain
positive effects over time. Further research is therefore
needed to assess the role of traditional acupuncture in
treating these symptoms in people with breast cancer. This
conclusion is consistent with reviews noting that there are
insufficient data to support the use of acupuncture to im-
prove psychological well-being.36,39 No systematic reviews
were found to address the use of acupuncture in treating
decreased range of motion and lymphedema.
Electroacupuncture
With respect to EA, 2 outcomes were considered: emesis
and hot flashes. Based on the results of one study, which was
of high methodological quality, EA may be useful for re-
ducing emesis associated with chemotherapy treatment in
patients with breast cancer.35 The benefits demonstrated in
this study, however, were only sustained for a short 5-day
period during which the treatment was implemented. The
effect of longer EA trials has yet to be determined. These
findings are consistent with a systematic review.40 In that
review, however, many of the trials analyzed used EA in
conjunction with antiemetic medications that are now out-
dated, whereas trials including current antiemetic drug
routines showed nonsignificant effects.40 Therefore, while
positive effects have been demonstrated with the use of EA
in relieving emesis due to chemotherapy, there exists a
further need for research surrounding its use, especially in
regard to its long-term effects and use with concurrent
medications.
With respect to hot flashes, Nedstrand et al27 and Frisk
et al28 found the use of EA had significant long-term effects
on hot flash frequency and levels of associated distress.
However, neither of the studies utilized a true control group.
Nedstrand et al found that EA and applied relaxation therapy
were both effective in significantly decreasing hot flashes in
women with breast cancer, although there were insufficient
participants to make between-group comparisons of treat-
ment effects. The results from this study should also be in-
terpreted with caution due to the small sample size and high
dropout rates.27 Frisk et al28 indicated that although EAmay
have positive effects on hot flashes, the effects of hormone
therapy are superior. The results of this study, however, were
also limited by a small sample size and missing long-term
data.28 Therefore, while the limited evidence suggests that
EA is effective at reducing hot flashes in women following
breast cancer treatment, further research is needed to deter-
mine if it is more effective than other available treatment
options. No other systematic reviews addressing the role of
EA on hot flashes could be found within existing literature to
affirm or refute this conclusion.
Acupressure
While the use of acupressure in treating side effects of
breast cancer therapy was not explicitly analyzed in this
systematic review, 2 studies were identified in our search
that used acupressure in their studies as either adjuncts or
comparisons with traditional acupuncture.29,32 Two out-
comes were considered in these studies: dyspnea and fa-
tigue. The evidence presented in these studies did not fully
support the use of acupressure alone to decrease either of
these symptoms, and when compared with traditional acu-
puncture, was found to be inferior. These conclusions are
consistent with the results of the 2009 Cochrane Group
systematic review on nonpharmacological interventions for
dyspnea,41 whereas no systematic reviews were found per-
taining to the use of acupressure to ameliorate fatigue.
Furthermore, no additional clinical studies implementing
acupressure for relief of fatigue could be found to make
comparisons or draw additional conclusions. Overall, fur-
ther research needs to be conducted to determine the role of
acupressure alone or in combination with traditional acu-
puncture in ameliorating dyspnea and fatigue because there
is currently insufficient evidence to merit its use.
94 DOS SANTOS ET AL.
Page 15
Mechanism of Action
Although acupuncture was found to be effective in re-
lieving some symptoms related to breast cancer, its mecha-
nism of action is not yet fully understood. Western medicine
has been slow to accept acupuncture due to uncertainty re-
garding its mechanism of action. While several theories have
been proposed, the most widely accepted theory states that
stimulation of acupoints causes the release of natural en-
dogenous opioids and neurotransmitters, such as seroto-
nin.42,43 It is proposed that acupuncture modulates pain
perception by activating A-d and C afferent fibers in muscle,
signaling the spinal cord to release neurotransmitters.42 The
release of neurotransmitters such as serotonin and dopamine
leads to presynaptic and postsynaptic inhibition, which, in
turn, alter symptoms, such as pain and nausea, or release
other chemicals that influence the immune system.42,43 These
biochemical changes, while not entirely understood, may in
turn stimulate the body’s healing abilities and promote
physical and emotional well-being.43
Study Limitations
This systematic review was the first to examine the ef-
fects of acupuncture specific to the breast cancer population.
The generalized findings presented above have been based
on a limited number of studies found in the literature. In
addition, many of these studies were found to have meth-
odological flaws, as discussed throughout this review.
Overall, due to heterogeneity in treatment protocols, study
populations, outcome measures, and length of follow-up, it
is difficult to draw definite conclusions surrounding the use
of acupuncture in treating side effects due to breast cancer
treatments. Therefore, at this time, only recommendations
can be made.
Clinical Implications
In summary, the role of acupuncture in the relief of side
effects associated with breast cancer treatment is still un-
clear due to both an overall lack of studies and numerous
methodological flaws found in existing studies. Overall, the
use of traditional acupuncture may be beneficial in ame-
liorating symptoms such as hot flashes, fatigue, and pain,
whereas EA may be useful in treating emesis and hot fla-
shes. Because existing evidence surrounding the use of
acupuncture is still limited and often inconclusive, it is re-
commended that clinicians use acupuncture as an adjunct to
other forms of therapy and not necessarily as a sole form of
treatment. When implementing acupuncture in one’s prac-
tice, a clinician must make a case-by-case decision as to
whether or not their client is appropriate. Therefore, evi-
dence presented in this review should be used in conjunction
with a clinician’s experience and clinical reasoning to guide
one’s practice in determining when acupuncture should be
used.
CONCLUSIONS
The purpose of this systematic review was to determine
the effectiveness of acupuncture as a treatment option for
common side effects associated with breast cancer treat-
ment. Overall, the results of this review support the potential
use of traditional acupuncture to decrease hot flashes, fa-
tigue, and pain, whereas EA may be useful in treating
emesis and hot flashes. There is, as of yet, a paucity of high-
quality evidence to support the use of acupuncture to ame-
liorate dyspnea, emesis, and decreased range of motion with
lymphedema or to improve psychological well-being. While
the use of acupressure was not explicitly analyzed in this
systematic review, 2 studies investigated the role of acu-
pressure as either adjuncts or comparisons with traditional
acupuncture. While definitive conclusions cannot be made,
overall the evidence presented in these 2 studies did not
support the use of acupressure to decrease dyspnea or fa-
tigue, and was actually found to be inferior when compared
with traditional acupuncture. Concerns regarding the
methodological rigor of existing studies, however, encour-
age the reader to accept these findings with caution.
Therefore, the results of this study, combined with clinician
discretion, should guide a clinician’s decision on whether to
use acupuncture in treatment.
Recommendations for future research are 3-fold. First,
studies with strong methodological rigor are needed to as-
sess the true effect of acupuncture on symptoms related to
breast cancer treatment by utilizing homogeneous sample
populations, adequate sample sizes, and true comparison
groups. Second, studies need to assess the long-term effi-
cacy of acupuncture by including longer follow-up periods.
Lastly, studies assessing the role of acupuncture as part of a
multimodal treatment intervention must clearly specify
acupuncture intervention parameters, as well as the com-
ponents of any adjunct treatment. Once these elements are
addressed in future studies, stronger recommendations re-
garding the role of acupuncture in ameliorating side effects
associated with breast cancer treatment can be made. In the
interim, the results of this study suggest that acupuncture
may be used as an adjunct to existing treatment to amelio-
rate several side effects associated with breast cancer
treatment and ultimately improve quality of life.
DISCLOSURE STATEMENT
No competing financial interests exist.
REFERENCES
1. Breast Cancer Information. Breast Cancer Society of
Canada. http:==www.bcsc.ca=menu.php?list¼518&page¼44.
Accessed July 7, 2009.
BREAST CANCER TREATMENT 95
Page 16
2. Early Breast Cancer Trialists’ Collaborative Group. Poly-
chemotherapy for early breast cancer: an overview of the
randomised trials. Lancet. 1998;352:930–942.
3. Treatment Side Effects. BREASTCANCER.ORG. 2009.
http:==www.breastcancer.org=treatment=side_effects=. Ac-
cessed June 4, 2009.
4. Tchen N, Juffs HG, Downie FP, et al. Cognitive function, fatigue,
and menopausal symptoms in women receiving adjuvant che-
motherapy for breast cancer. J Clin Oncol. 2003;21:4175–4183.
5. Goodwin PJ, Ennis M, Pritchard KI, Trudeau M, Hood N.
Risk of menopause during the first year after breast cancer
diagnosis. J Clin Oncol. 1999;17:2365–2370.
6. Early Breast Cancer Trialists’ Collaborative Group. Effects of
chemotherapy and hormonal therapy for early breast cancer
on recurrence and 15-year survival: an overview of the ran-
domized trials. Lancet. 2005;365:1687–1717.
7. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA
Cancer J Clin. 2008;58:71–96.
8. Weis J, Poppelreuter M, Bartsch HH. Cognitive deficits as long-
term side-effects of adjuvant therapy in breast cancer patients:
‘subjective’ complaints and ‘objective’ neuropsychological test
results. Psycho-Oncology. 2009;18:775–782.
9. Kayl AE, Meyers CA. Side-effects of chemotherapy and
quality of life in ovarian and breast cancer patients. Curr Opin
Obstet Gynecol. 2006;18(1):24–28.
10. Buijs C, de Vries EGE, Mourits MJE, Willemse PHB. The
influence of endocrine treatments for breast cancer on health-
related quality of life. Cancer Treat Rev. 2008;34:640–655.
11. Knobf MT. Natural menopause and ovarian toxicity associa-
tion with breast cancer therapy. Oncol Nurs Forum.
1998;25:1519–1532.
12. Molina JR, Barton DL, Loprinzi CL. Chemotherapy-induced
ovarian failure: manifestations and management. Drug Saf.
2005;28:401–416.
13. Rotchford JK, Kobrin LE. The importance of a modern and
comprehensive definition for acupuncture in clinical research:
preliminary perspectives. Medical Acupuncture. 2002;13(3):
38–40.
14. Rotchford JK. Overview: adverse events of acupuncture.
Medical Acupuncture. 1999;11(2):32–35.
15. Acupuncture. National Cancer Institute. 2008. http:==wwwcancer.gov=cancertopics=pdq=cam=acupuncture=health
professional=allpages#Section_4. Accessed June 5, 2009.
16. White A. A cumulative review of the range and incidence of
significant adverse events associated with acupuncture. Acu-
punct Med. 2004;22(3):122–133.
17. Kaptchuk TJ. Acupuncture: theory, efficacy and practice. Ann
Intern Med. 2002;136:374–383.
18. Weidong L. Acupuncture for side effects of chemoradiation
therapy in cancer patients. Semin Oncol Nurs. 2005;21(3):
190–195.
19. Deng G, Vickers A, Simon Yeung K, Cassileth BR. Acu-
puncture: integration into cancer care. J Soc Integr Oncol.
2006;4(2):86–92.
20. Cohen AJ, Menter A, Hale L. Acupuncture: role in compre-
hensive cancer care—a primer for the oncologist and review
of the literature. Integr Cancer Ther. 2005;4(2):131–143.
21. Maher CG, Sherrington C, Herbert RD, Moseley AM,
Elkins M. Reliability of the PEDro scale for rating quality
of randomized controlled trials. Phys Ther. 2003;83(8):713–
721.
22. PEDro. Physiotherapy evidence database. http:==www.pedro.
fhs.usyd.edu.au=. Accessed February 24, 2009.
23. Psychological database for brain impairment treatment efficacy.
http:==www.psycbite.com=. Accessed February 22, 2009.
24. Hervik J, Mjaland O. Acupuncture for the treatment of hot
flashes in breast cancer patients, a randomized controlled trial
[Epub ahead of print]. Breast Cancer Res Treat. 2008.
25. Deng G, Vickers A, Yeung S, et al. Randomized, controlled
trial of acupuncture for the treatment of hot flashes in breast
cancer patients. J Clin Oncol. 2007;25(35):5584–5590.
26. Tukmachi. Treatment of hot flushes in breast cancer patients
with acupuncture. Acupunct Med. 2000;18(1):22–27.
27. Nedstrand E, Wijma K, Wyon Y, Hammar M. Vasomotor
symptoms decrease in women with breast cancer randomized
to treatment with applied relaxation or electro-acupuncture: a
preliminary study. Climacteric. 2005;8(3):243–250.
28. Frisk J, Carlhall S, Kallstrom AC, Lindh-Astrand L, Mal-
mstrom A, Hammar M. Long term follow-up of acupuncture
and hormone therapy on hot flushes in women with breast
cancer: a prospective, randomized, controlled multicenter
trial. Climacteric. 2008;11(2):166–174.
29. Molassiotis A, Sylt P, Diggins H. The management of cancer-
related fatigue after chemotherapy with acupuncture and
acupressure: a randomised controlled trial. Complement Ther
Med. 2007;15(4):228–237.
30. Alimi D, Rubino C, Pichard-Leandri E, Fermand-Brule S,
Dubreuil-Lemaire ML, Hill C. Analgesic effect of auricular
acupuncture for cancer pain: a randomized, blinded controlled
trial. J Clin Oncol. 2003;21(22):4120–4126.
31. Crew KD, Capodice JL, Greenlee H, et al. Pilot study of
acupuncture for the treatment of joint symptoms related to
adjuvant aromatase inhibitor therapy in postmenopausal
breast cancer patients. J Cancer Surviv. 2007;1(4):283–291.
32. Vickers AJ, Feinstein MB, Deng GE, Cassileth BR. Acu-
puncture for dyspnea in advanced cancer: a randomized, pla-
cebo-controlled pilot trial. BMC Palliat Care. 2005;4:5–12.
33. Nedstrand E, Wyon Y, Hammar M, Wijma K. Psychological
well-being improves in women with breast cancer after
treatment with applied relaxation or electro-acupuncture for
vasomotor symptom. J Psychosom Obstet Gynaecol. 2006;
27(4):193–199.
34. Alem M, Gurgel MS. Acupuncture in the rehabilitation of
women after breast cancer surgery—a case series. Acupunct
Med. 2008;26(2):86–93.
35. Shen J, Wenger N, Glaspy J, et al. Electroacupuncture for
control of myeloablative chemotherapy-induced emesis: a
randomized controlled trial. JAMA. 2000;284(21):2755–2761.
36. Cohen AJ, Menter A, Hale L. Acupuncture: role in com-
prehensive cancer care—a primer for the oncologist and
review of the literature. Integr Cancer Ther. 2005;4(2):
131–143.
37. The North American Menopause Society. Treatment of
menopause-associated vasomotor symptoms: position state-
ment of The North American Menopause Society. Meno-
pause. 2004;11(1):11–33.
38. Lee H, Schmidt K, Ernst E. Acupuncture for the relief of cancer-
related pain: a systematic review. Eur J Pain. 2007;9(4):437–444.
96 DOS SANTOS ET AL.
Page 17
39. Weidong L. Acupuncture for side effects of chemoradiation
therapy in cancer patients. Semin Oncol Nurs. 2005;21(3):
190–195.
40. Ezzo J, Vickers A, Richardson MA, et al. Acupuncture-point
stimulation for chemotherapy-induced nausea and vomiting.
J Clin Oncol. 2005;23(28):7188–7198.
41. Bausewein C, Booth S, Gysels M, Higginson IJ. Non-phar-
macological interventions for breathlessness in advanced
stages of malignant and non-malignant diseases. Cochrane
Database Syst Rev. 2008;2.
42. Wang SM, Kain ZN, White P. Acupuncture analgesia, I: the
scientific basis. Anesth Analg. 2008;106(2):602–610.
43. Collins KB, Thomas DJ. Acupuncture and acupressure for the
management of chemotherapy–induced nausea and vomiting.
J Am Acad Nurse Pract. 2004;16(2):76–80.
Address correspondence to:
Oren Cheifetz, MSc
Clinical Specialist - Physiotherapy
CIHR Strategic Training Fellow in Rehabilitation Research
Hematology=Oncology Program
Henderson Campus, Ward C4
Hamilton Health Sciences
711 Concession Street
Hamilton, On L8V 1C3
Canada
E-mail: [email protected]
BREAST CANCER TREATMENT 97