Acute and Chronic Pulmonary Function Changes in Allergic Bronchopulmonary Aspergillosis DAVID NICHOLS, M.D.* GUILLERMO A. DOPICO, M.D. SHELDON BRAUN. M.D. STEPHEN IMBEAU, M.D. MARY E. PETERS, M.D. JOHN RANKIN. M.D. Madison, Wisconsin From the Departments of Medicine and Pre- ventive Medicine, University of Wisconsin Center for Health Sciences, Madison, Wisconsin. This study was supported by Specialized Center of Research (SCOR) Grant No. HL 15389 and training grant HL 07016 from the National Heart, Lune. and Blood Institute. NIH. Requests for -~~~-“. reprints should be addres&d to Dr.G. A.doPico, 600 Highland Avenue, Madison, Wisconsin 53792. Manuscript accepted June 6.1979. * Present address: 6501 Bolton Road, Ft. Smith, Arkansas 72903. Pulmonary functions of patients with allergic bronchopulmonary aspergillosis were studied during an acute episode (n = 6) during a mean follow-up period of 44 months (range four months-14.6 years) (n = 16); and for any correlation between duration of ABPA and asthma with the total lung capacity (helium dilution), 1 second forced expiratory volume (FEV& vital capacity, 1 second forced expiratory volume-forced vital capacity ratio (FEV#VC per cent) and diffusing capacity of carbon monoxide (DkCO) (single breath) for the entire group (n = 22). All patients were treated with corticosteroids (inter- mittent or continuous) and bronchodilators. For the 16 patients, slopes using linear regression analysis were determined from the function as per cent predicted versus time in months from diagnosis and then analyzed for significance. Significant functional loss was shown in three of 16 patients for FEVI, two of 16 patients for vital capacity, one of 16 patients for FEV&VC per cent, none of 10 patients for DLCO and one of 10 patients for total lung capacity. No significant corre- lation between actual DL:CO, total lung capacity, FEVI,vital capacity, FEV#VC per cent and the duration of asthma or allergic broncho- pulmonary aspergillosis was found by multiple regression analysis correcting for age and smoking (mean 4.24 years; range 0.3 to 14.6 years). Roentgenographic criteria and blood eosinophiiia were used to define a “flare” of allergic bronchopulmonary aspergillosis. The six patients during a flare showed a significant reduction in total lung capacity Q <O.OOl), vital capacity Q <0.05), FJWI (P <O.Ol) and DLCO (P <O.OOl) which uniformly returned to baseline values during steroid therapy, The FEV#VC per cent remained unaltered. These findings, contrary to suggestions in the literature, indicate that in the majority of our patients there was no significant progressive functional de- terioration after diagnosis. However, during acute episodes of allergic bronchopulmonary aspergillosis, transient reduction of volumes and DL:CO were uniformly present. Allergic bronchopulmonary aspergillosis is thought to represent a hypersensitivity lung disease to species of the fungus Aspergillus, chiefly A. fumigatus [l]. This disease is found among patients with bronchial asthma and is characterized by recurrent episodes of pul- monary infiltrates with eosinophilia [l], the presence of a proximal saccular type of bronchiectasis [z] and evidence of an immunologic response to the fungus. The latter takes the form of specific elevations, in immunoglobulin E (IgE) serum precipitins, and skin test sensitivity of an immediate and delayed type [l]. Allergic bronchopulmonary aspergillosis is only one of several diseases due to Aspergillus that occurs in man [3,4] and was first described by Henson, Moon and October 1979 The American Journal of Medicine Volume 67 631
Transcript
Acute and Chronic Pulmonary Function Changes in Allergic Bronchopulmonary Aspergillosis
DAVID NICHOLS, M.D.*
GUILLERMO A. DOPICO, M.D.
SHELDON BRAUN. M.D.
STEPHEN IMBEAU, M.D.
MARY E. PETERS, M.D.
JOHN RANKIN. M.D.
Madison, Wisconsin
From the Departments of Medicine and Pre- ventive Medicine, University of Wisconsin Center for Health Sciences, Madison, Wisconsin. This study was supported by Specialized Center of Research (SCOR) Grant No. HL 15389 and training grant HL 07016 from the National Heart, Lune. and Blood Institute. NIH. Requests for -~~~-“.
reprints should be addres&d to Dr. G. A. doPico, 600 Highland Avenue, Madison, Wisconsin 53792. Manuscript accepted June 6.1979.
* Present address: 6501 Bolton Road, Ft. Smith, Arkansas 72903.
Pulmonary functions of patients with allergic bronchopulmonary aspergillosis were studied during an acute episode (n = 6) during a mean follow-up period of 44 months (range four months-14.6 years) (n = 16); and for any correlation between duration of ABPA and asthma with the total lung capacity (helium dilution), 1 second forced expiratory volume (FEV& vital capacity, 1 second forced expiratory volume-forced vital capacity ratio (FEV#VC per cent) and diffusing capacity of carbon monoxide (DkCO) (single breath) for the entire group (n = 22). All patients were treated with corticosteroids (inter- mittent or continuous) and bronchodilators. For the 16 patients, slopes using linear regression analysis were determined from the function as per cent predicted versus time in months from diagnosis and then analyzed for significance. Significant functional loss was shown in three of 16 patients for FEVI, two of 16 patients for vital capacity, one of 16 patients for FEV&VC per cent, none of 10 patients for DLCO and one of 10 patients for total lung capacity. No significant corre- lation between actual DL:CO, total lung capacity, FEVI, vital capacity, FEV#VC per cent and the duration of asthma or allergic broncho- pulmonary aspergillosis was found by multiple regression analysis correcting for age and smoking (mean 4.24 years; range 0.3 to 14.6 years). Roentgenographic criteria and blood eosinophiiia were used to define a “flare” of allergic bronchopulmonary aspergillosis. The six patients during a flare showed a significant reduction in total lung capacity Q <O.OOl), vital capacity Q <0.05), FJWI (P <O.Ol) and DLCO (P <O.OOl) which uniformly returned to baseline values during steroid therapy, The FEV#VC per cent remained unaltered. These findings, contrary to suggestions in the literature, indicate that in the majority of our patients there was no significant progressive functional de- terioration after diagnosis. However, during acute episodes of allergic bronchopulmonary aspergillosis, transient reduction of volumes and DL:CO were uniformly present.
Allergic bronchopulmonary aspergillosis is thought to represent a hypersensitivity lung disease to species of the fungus Aspergillus, chiefly A. fumigatus [l]. This disease is found among patients with bronchial asthma and is characterized by recurrent episodes of pul- monary infiltrates with eosinophilia [l], the presence of a proximal saccular type of bronchiectasis [z] and evidence of an immunologic response to the fungus. The latter takes the form of specific elevations, in immunoglobulin E (IgE) serum precipitins, and skin test sensitivity of an immediate and delayed type [l]. Allergic bronchopulmonary aspergillosis is only one of several diseases due to Aspergillus that occurs in man [3,4] and was first described by Henson, Moon and
October 1979 The American Journal of Medicine Volume 67 631
PULMONARY FUNCTION IN ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS-NICHOLS ET AL.
TABLE I Clinical Information on 23 Patients with Allergic Bronchopulmonary Asperglllosls (ABPA)
Plummer in 1952 [5]. Although first described and ap- parently more common in Great Britain, increasing re- ports of experience with this disease have been coming from North America and India [6-91. Particular em- phasis in the literature has been placed on case reports [lo-121, diagnostic criteria [1,3,8], roentgenographic features [2,13,14], immunology [1,15-171 and the pa- thology of the disease [18,19]. Pulmonary function, al- though included in the case reports [3,10,11,12] and in some patient series [1,7,20,21], has been limited largely to that measured during clinically quiescent periods. Any longitudinal data have been in the form of a re- gression analysis at the end of a follow-up period [2O]. The majority of these patient series are reported from Great Britain and, largely, from the same group of in- vestigators [1,20,21]. Studies have been published con- trasting allergic bronchopulmonary aspergillosis with simple bronchial asthma [22,23].
The purpose of this study was to describe our patient population with allergic bronchopulmonary aspergil- losis with particular emphasis on the changes in pul- monary function that occurred during the acute phase of the illness, and the more permanent changes which may have occurred over the course of follow-up. This latter aspect of the study was approached utilizing two different methods. First, a linear regression analysis
correcting for age and smoking habits was performed on the pulmonary function data collected at the time of the last follow-up. Second, the individual function data collected periodically over the course of follow-up were analyzed.
MATERIALS AND METHODS Patient Population. Twenty-three patients with the diagnosis
of allergic bronchopulmonary aspergillosis were studied [Table I). Twelve were male and 11 female, with a mean age of 37.9 years (range 14 to 63 years]. The average age at the onset of asthma was nine years (range 0.5 to 53 years]. The average duration of ABPA after the diagnosis was 4.2 years (range 0.3 to 14.8 years]. Because several of these patients most certainly had the disease prior to the actual time of diagnosis, the first date of a recorded pulmonary infiltrate was also ascertained and used in the analysis. The mean time since this first infil- trate was seven years (range 0.3 to 23 years). Eight of the 23 patients smoked (range 1 to 45 pack years). Three patients in this series had undergone resective pulmonary surgery prior to the diagnosis. Diagnostic Criteria. All patients met sufficiently the diag- nostic criteria in the literature 111: (1) history of recurrent pul- monary infiltrates, (2) blood eosinophilia (greater than 500 cells/cc), (3) history of asthma, (41 serum precipitins to A. fu- migatus, (5) dual skin test reactivity to Aspergillus species, (6) elevated serum IgE levels, (7) sputum culture of Aspergillus
632 October 1979 The American Journal of Medicine Volume 67
PULMONARY FUNCTION IN ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS-NICHOLS ET AL.
TABLE II Pulmonary Function Data (Baseline*) on 23 Patients with Allergic Bronchopulmonary Aspergillosis
NOTE: TLC = total lung capacity; VC = vital capacity; RV:TLC = residual volume to total lung capacity: FEV, = 1 second forced expiratory volume: FEV,:FVC = 1 second forced expiratory volume to forced vital capacity; DLco = diffusing capacity of carbon monoxide; DL:VA = diffusing capacity to alveolar volume. l Time closest to diagnosis and clinically asymptomatic. t Pulmonary surgery performed. t No data available.
and (a) a bronchogram with proximal saccular bronchiectasis. Although unusual, the absence of asthma in one patient (Case 15) has been previously reported by McCarthy [lo]. All the other diagnostic criteria were present in this patient, including the proximal saccular bronchiectasis described by Gadding to be pathognomonic [z]. Sputum cultures were not uniformly positive as reported by others [a]. The variation we found in blood eosinophilia and IgE levels may be due to effects of steroid therapy and disease activity [8,17]. Definition of a Flare. A “flare” was defined as the presence of a roentgenographic change (atelectasis. alveolar infiltrate] associated with blood eosinophilia (greater than 500 cells/cc) and clinical symptoms (wheeze, cough, sputum plugs or fever). Therapy. All patients with allergic bronchopulmonary as- pergillosis were treated with corticosteroids on either a con- tinuous or an intermittent basis. For an acute episode, the dose of corticosteroid was 30 to 60 mg of prednisone daily, tapering over a two to three week period. For continuous use, a 15 to 20 mg dose of prednisone on alternate days was used. Broncho- spasm was controlled as needed with various bronchodilators including corticosteroids. Pulmonary Functions. Spirometry was performed in the usual manner on a Collins 13.5 liter water seal spirometer or a Vitalograph bellows spirometer. A favorable comparison of these two instruments has been previously reported [24]. The best of three trials was used in all cases. The predicted values
were taken from Morris et al. [25] for adults and from Dickman et al. for children and adolescents [26]. All values of forced expiratory flow between 25 and 75 per cent of vital capacity were made from the water seal spirometer. Total lung capacity was determined by the single breath helium dilution method, and the norma values for adults were taken from Needham et al. [27] and for children and adolescents from Polgar et al. [28]. Diffusing capacity for carbon monoxide (DLco) and ratio of diffusing capacity to alveolar volume were determined by the single breath method of Ogilvie et al. [29] and the mean of three determinations was used. The predicted values were taken from Ogilvie et al. [29]. Closing volume was performed by the nitrogen method, and normal values were taken from McCarthy et al. [30]. Flow volume loops were performed on a wedge spirometer, and normal values for maximal instan- taneous flows at 50 and 75 per cent of vital capacity (irm,,50 and 9,,,75) were taken from Bass [31]. Chest Roentgenography. Chest roentgenograms obtained on the same day as the pulmonary function tests were read by an independent radiologist and classified as to alveolar infiltra- tion, bronchial plugging or obstructive atelectasis. The radi- ologist had no prior knowledge of the pulmonary function.
RESULTS The baseline pulmonary functions of our 23 patients are
presented in Table II. These values were obtained during an asymptomatic time which was as close to the
October 1978 The American Journal of Medicine Volume 67 633
PULMONARY FUNCTION IN ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS-NICHOLS ET AL.
t
“C -
2C- FE”(F”C% H
_ DL’CO H P7 2
1 I I I a I I, I I, I, I I, 1 I I I I I I, I, I
0 8 , , , ,
16 24 32 40 48 56
MONTHS FROM DIAGNOSIS
ATELECTASIS o o o o o
PLUGGING + ++ f +
100 INFlLTRATlON 0 00 0 0
“!I I
MONTHS FROM DIAGNOSIS
ATETELECTASIS +
PLUGGING + INFILTRATION +
120
0 0 16 24 32 40 48 56 64 12
MONTHS FROM DIAGNOSIS MONTHS FROM DIAGNOSIS
Figure 1. Individual pulmonary function and roentgenographic data during the follow-up period.
actual time of diagnosis as possible. Lung volumes were generally well preserved as shown by a vital capacity of greater than 80 per cent predicted in 19 of 23 patients, and a total lung capacity of greater than 80 per cent predicted in 18 of 23 patients. There was mild evidence for hyperinflation as evidenced by residual volume to total lung capacity ratio being greater than 40 per cent in seven of 22 patients. DLco exceeded 100 per cent of the predicted value in 12 of 22 patients. A DLco of less than 80 per cent of predicted was found in only seven of 22 patients. Airway obstruction as measured by the FEV1:FVC per cent was not severe in any of these pa- tients. In all patients, the value was above 50 per cent. In seven of nine patients with normal FEV1:FVC, per cent evidence of airways obstruction by reduced Vmaxso and a forced expiratory flow of 25 to 75 per cent was found, whereas in three of nine the closing voIume was abnormal.
Figure 1 displays examples of the changes in pul- monary functions seen in individual patients during the follow-up period. The values of FEV1, vital capacity, and DLco as per cent of predicted values and the simple ratio of FEVl:FVC, per cent are plotted against time
expressed in months since diagnosis. Some patients show frequent, transient fluctuations in function (Figure la, b and c) whereas others remain fairly constant [Figure Id] showing minimal change. Since lung vol- umes are&own to have an effect upon DLco [29], it was understandable to see vital capacity and DL:CO vary directly as in Figure la and c. However, when linear regression slopes were used to look for positive corre- lation between DL:CO and alveolar volume, only four of 14 patients showed significant correlation. This sug- gested that changes in diffusion were multifactorial and not simply related to volume changes in all instances.
Every time there was a roentgenographic infiltrate or atelectasis there were decrements in diffusion capacity and lung volumes (Figure la, b and d). At times, how- ever, there was evidence of the same functional change without the roentgenographic abnormality (Figure la). Bronchial plugging was seen to occur without any changes in the pulmonary functions (Figure 1).
Six patients who met the criteria of a’flare were ex- amined as a group. Each patient’s functions were com- pared to a previous set obtained during a clinically asymptomatic time. Using a two tailed t test the total lung
634 October 1979 The American Journal of Medicine Volume 67
PIJLMONARY FUNCTION IN ALLERGIC BRONCHOPIjLMONARY ASPERGILLOSIS-NICHOLS ET AL.
FLARE Vs BASELINE n=6 mean values
p<.o1
n I r/
TLC vc FEVl
FLARE Vs BASELINE n=6 mean values
ezl El
FLARE
BASELINE
l-54 $45 v E 36
a
P NS 27 r
El 18
- L
9
DL/VA DL co Iml/mm/mmHq~
81
72
63 1
P NS
FEV,/FVC X
1 I-
, /’
IOOr 1’ / / /’
go- /’ s / b
/
d /’ .60- ,/
A A
2 / A A
E c -. A
c 70- b
. . *
$ -.
z ‘.
f 60- ‘-.a b -.
NON SIGNIFICANT SLOPE ‘.
‘.
50 _ 95 % CONFIDENCE LIMITS t--j .-. .
1111111111111 120
r
I I I1 I1 I / 0 IO 20 30 40 %--’ 60
MONTHS SINCE OX
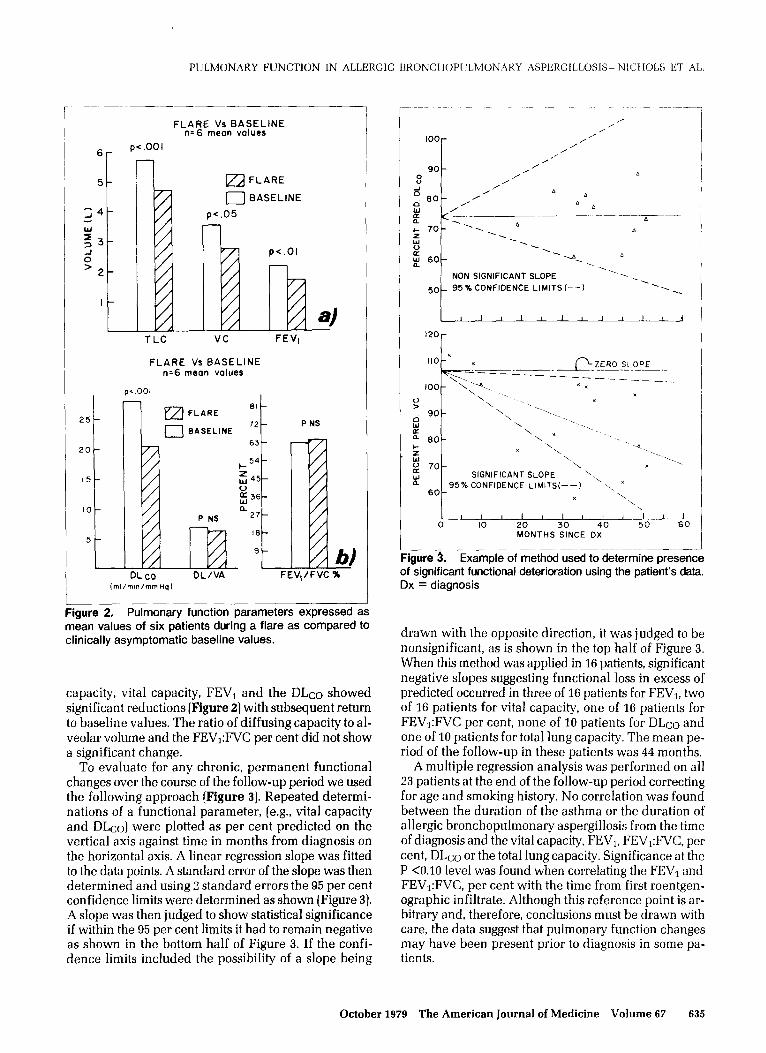
Igure 3. Example of method used to determine presence of significant functional deterioration using the patient’s data. Dx = diagnosis
Figure 2. Pulmonary function parameters expressed as mean values of six patients during a flare as compared to clinically asymptomatic baseline values.
capacity, vital capacity, FEVl and the DLco showed significant reductions (Figure 2) with subsequent return to baseline values. The ratio of diffusing capacity to al- veolar volume and the FEV1:FVC per cent did not show a significant change.
To evaluate for any chronic, permanent functional changes over the course of the follow-up period we used the following approach (Figure 3). Repeated determi- nations of a functional parameter, [e.g., vital capacity and DLco) were plotted as per cent predicted on the vertical axis against time in months from diagnosis on the horizontal axis. A linear regression slope was fitted to the data points. A standard error of the slope was then determined and using 2 standard errors the 95 per cent confidence limits were determined as shown (Figure 3). A slope was then judged to show statistical significance if within the 95 per cent limits it had to remain negative as shown in the bottom half of Figure 3. If the confi- dence limits included the possibility of a slope being
drawn with the opposite direction, it was judged to be nonsignificant, as is shown in the top half of Figure 3. When this method was applied in 16 patients, significant negative slopes suggesting functional loss in excess of predicted occurred in three of 16 patients for FEV1, two of 16 patients for vital capacity, one of 16 patients for FEV,:FVC per cent, none of 10 patients for DLco and one of 10 patients for total lung capacity. The mean pe- riod of the follow-up in these patients was 44 months.
A multiple regression analysis was performed on all 23 patients at the end of the follow-up period correcting for age and smoking history. No correlation was found between the duration of the asthma or the duration of allergic bronchopulmonary aspergillosis from the time of diagnosis and the vital capacity, FEV1, FEVi:FVC, per cent, DLeo or the total lung capacity. Significance at the P <O.lO level was found when correlating the FEVl and FEV1:FVC, per cent with the time from first roentgen- ographic infiltrate. Although this reference point is ar- bitrary and, therefore, conclusions must be drawn with care, the data suggest that pulmonary function changes may have been present prior to diagnosis in some pa- tients.
October 1979 The American Journal of Medicine Volume 67 635
PULMONARY FUNCTION IN ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS-NICHOLS ET AL.
COMMENTS
Patients with allergic bronchopulmonary aspergillosis can have normal pulmonary function, evidence of fixed airway obstruction with normal DLco or fixed airway obstruction with a reduced DLco. Patients with chronic bronchiectasis are known to show progressive fixed airway obstruction’ and reduced DLco [32-341. Con- versely, in patients with asthma airway obstruction is generally more reversible and single breath DLco is normal to increased [35,36]. Similar to the findings of Khan et al. [7], airways obstruction in our patients was mild to moderate-none of the patients had a FEV1:FVC below 50 per cent-and was generally milder than that reported by others [1,20,21]. Malo et al. [20], with the use of helium-oxygen flow volume loops, suggested that most obstruction was in the larger central airways; however, in nine of their patients with a normal FEV1, an abnormal iT max5~ suggested small airways involve- ment. Similarly in seven of nine of our patients who had an FEV1:FVC < 0.69, we found abnormalities of \i,,, 50, closing volume or forced expiratory flow 25 to 75 per cent suggestive of small airways abnormality. Such small airways disease has been reported by Landau et al. [33] in chronic bronchiectasis based on abnormal flow volume loops and frequently dependent compli- ance. Differences in airways obstruction have been used to separate patients with allergic bronchopulmonary aspergillosis from those with asthma [22,23].
sion distribution due to areas of atelectasis pneumonitis, and peribronchial and bronchial abnormalities.
During acute flares of allergic bronchopulmonary aspergillosis the characteristic changes in pulmonary function are reductions in volume (total lung capacity, vital capacity, FEV1) and DLco. These changes are all seen to be transient and, usually, fully reversible to previous baseline values, they were noted to occur each time the chest film showed evidence of atelectasis or alveolar infiltration. However, they were also seen to occur on occasion when the chest film showed no ab- normalities, suggesting that, although characteristic of a flare, the functional changes may not be specific. The only transient roentgenographic change seen to occur without evidence of functional change was focal bron- chial plugging.
Lung volumes in our patients were generally pre- served and showed only mild hyperinflation whereas others have reported hyperinflation in the majority of patients [1,20].
Like measurements of airway obstruction, DLco varies in patients with allergic bronchopulmonary as- pergillosis [1,20,21]. Since patients with bronchial asthma are reported to have normal to increased DLco values [35,36], and patients with bronchiectasis gener- ally have a reduced diffusing capacity [32-341, the DLco values in allergic bronchopulmonary aspergillosis provide important information. A chronically reduced diffusing capacity has been reported as a distinguishing feature between patients with allergic bronchopulmo- nary aspergillosis and patients with bronchial asthma [22,23]. We believe that the presence of a fixed reduction in DLco reflects severity of disease and probably re- flects an increased amount of bronchiectasis or chronic pneumonitis. The reduction in DLco can also be tran- sient in these patients and then is usually associated with an acute “flare.” Such reductions contrast sharply with the increases seen during.status asthmaticus [35,36] and may represent a process unique to allergic broncho- pulmonary aspergillosis such as pneumonitis. We have been able to correlate the reduction in DLco to volume changes in some patients, but in others volume is not the complete explanation. We conclude, therefore, that changes in diffusing capacity are due to multifactorial causes, such as the reduced alveolar volume, increased diffusion pathway, and altered ventilation and perfu-
McCarthy and Pepys [l] have suggested that in some patients allergic bronchopulmonary aspergillosis is a rapidly progressive disease which leads to the devel- opment of fixed airway obstruction and a reduction in diffusion capacity, but they do not offer evidence of this progressive change in the form of longitudinal pulmo- nary function data. Malo et al. [ZO] examined their pa- tient population with simple linear regression analysis and reported a reduction in FE&, V,,,50, FVC, vital capacity and DLco directly related to age and the pa- tient’s age when the diagnosis of aspergillosis was made. Furthermore, they report a direct correlation between reduced DLco and FVC, and the duration of allergic bronchopulmonary aspergillosis. It is important to point out that no correction was made in their study for smoking habits or age, Our longitudinal data suggested no clear evidence of functional deterioration in all pa- tients over the course of follow-up. We have been un- able to confirm any correlation with the duration of disease and functional impairment after correcting for age and smoking. Our data indicate progressive disease in a minority of patients. Safirstein et al. [21] also suggest that little change occurred in their five year follow-up but did not present the longitudinal data.
In summary we have shown that only a minority of our patients have had progressive functional deterio- ration. It must be emphasized, however, that we, like others, have not been able to describe the natural history of allergic bronchopulmonary aspergillosis because of the therapy employed in these patients. We would fur- ther suggest that because of the side effects of cortico- steroid therapy, and the finding that some patients do very well without corticosteroids, further study of the natural history of allergic bronchopulmonary asperg- illosis and therapeutic regimens would be helpful.
ACKNOWLEDGMENT
We are grateful to Dr. Helen Dickie and Dr. Charles Reed for their valuable collaboration and advice: Dr. Anastasios Tsiatis for his advice in the statistical analysis and to Jean Vaughn and Elaine Holms for their tech- nical assistance.
636 October 1979 The American Journal of Medicine Volume 67
Henson KFW, Moon AJ, Plummer NS: Bronchopulmonary aspergillosis-a review and a report of eight new cases. Thorax 7: 317.1952.
6. Sandhu RS, Mishra SK, Randhawa HS, et al.: Allergic bronchopulmonary aspergillosis in India. Stand J Respir Dis 53: 289,1972.
7. Khan ZU, Sandhu RS, Randhawa HS, et al.: Allergic bron- chopulmonary aspergillosis. A study of 46 cases with spe- cial reference to laboratory aspects. Stand J Respir Dis 57: 73, 1976.
8.
9.
10.
11.
12.
Imbeau S, Cohen M. Reeb CE: Allergic bronchopulmonary asoerEillosis in infants. Am I Dis Child 131: 1127.1977.
HoehneJH, Reeb CE, Dickie hA: Allergic bronchopulmo- nary aspergillosis is not rare. Chest 63: 177, 1973.
McCarthy DS: Bronchiectasis in allergic bronchopulmonary asoeraillosis. Proc R Sot Med 61: 5.1968.
Huseby: KO: Serial studies in a case of pulmonary asperg- illosis. Dis Chest 51: 327, 1967.
13. Malo JL, Pepys J, Simon G: Studies in chronic allergic bron- chopulmonary aspergillosis 2: radiological findings. Thorax 32: 262, 1977.
14. McCarthy DS, Simon G, Hargreave FE: Radiological ap- pearances in allergic bronchopulmonary aspergillosis. Clin Radio1 21: 366, 1970.
15. Malo JL, Longbottom J. Mitchell J. et al.: Studies in chronic allergic bronchopulmonary aspergillosis. 3. immunological findings. Thorax 32: 269,1977.
Turner-Warwick M, Citron K, Carroll K. et al.: Immunologic lung disease due to aspergillus. Chest 68: 346.1975.
Katzenstein A, Liebow A, Freedman P: Bronchocentric granulomatosis, mucoid impaction and hypersensitivity reactions to fungi. Am Rev Respir Dis 111: 497, 1975.
19. Merkow L, Epstein S, Sebransky H, et al.: The pathogenesis
PULMONARY FUNCTION IN ALLERGIC BRONCHOPZJLMONARY ASPERGILLOSISm-NICHOLS ET AL.
REFERENCES
of experimental pulmonary aspergillosis. Am J Path01 62: 57, 1971.
20.
21.
22.
23.
24.
25.
27.
28.
Malo JL, Hawkins R, Pepys J: Studies in chronic allergic bronchopulmonarv asperpillosis. I. Clinical and phvsio- logical findings. Thorax 3% 254, 1977.
. ”
Safirstein BH, D’Souza M, Simon G, et al.: Five year fol- low-up of allergic bronchopulmonary aspergillosis. Am Rev Respir Dis 108: 450.1973.
Malo J, Inouye T, Hawkins R, et al.: Studies in chronic allergic bronchopulmonary aspergillosis. 4. comparison with a group of asthmatics. Thorax 32: 275,1977.
Biagi RW, Bapot BN: Pulmonary function in aspergillus- sensitive asthma patients. Br J Clin Prac 24: 470,197O.
Wever A, Britton M. Hughes D: Evaluation of two spirome- ters. A comparative study of the steal wells and the vital- ograph spirometers. Chest 70: 244.1976.
Morris JF, Koski A, Johnson LC: Spirometric standards for healthy non-smoking adults. Am Rev Respir Dis 103: 57, 1971.
Needham C, Rogan M, McDonald I: Normal standard for lung volumes, intrapulmonary gas-mixing and maximum breathing capacity. Thorax 9: 313,1954.
Polgar G, Promadhat V: Pulmonary Function Testing in Children: Techniques and Standards. Philadelphia, W.B. Saunders Co., 1971, Table 44. P 254.
29. Ogilvie CM, Forster R, Blakemore W, et al.: A standardized breath holding techniaue for the clinical measurement of the diffusing capacity bf the lung for carbon monoxide. J Clin Invest 36: 1, 1957.
30. McCarthy DS, Spencer R, Greene R. et al.: Measurement of “closing volume” as a simple and sensitive test for early detection of small airways disease. Am j Med 52: 747, 1972.
31. Bass H: The flow volume loop: normal standards and ab- normalities in chronic obstructive pulmonary disease. Chest 63: 171,1973.
32. Pande J, Jain B, Gupta G, et al.: Pulmonary ventilation and gas exchange in bronchiectasis. Thorax 26: 727,1971.
33. Landau L, Phelan P, Williams H: Ventilatory mechanics in patients with bronchiectasis starting in childhood. Thorax 29: 304. 1974.
34. Cherniack N, Carton R: Factors associated with respiratory insufficiency in bronchiectasis. Am J Med 41: 562, 1966.
35. Ohman J, Schmidt-Nowara W. Lawrence M, et al.: The dif- fusing capacity in asthma. Am Rev Respir Dis 107: 932, 1973.
36. Weitzman RH, Wilson AF: Diffusing capacity and over-all ventilation: perfusion in asthma. Am I Med 57: 767, 1974.
October 1979 The American Journal of Medicine Volume 67 637