“Acute Coronary Syndromes: Trials & Tribulations" Will Southern, M.D., M.S. Director of Hospitalist Services Associate Medical Director Weiler Division Hospital of Montefiore Medical DIVISION OF GENERAL INTERNAL MEDICINE
Transcript
“Acute Coronary Syndromes: Trials & Tribulations"
Will Southern, M.D., M.S.Director of Hospitalist Services
Associate Medical DirectorWeiler Division Hospital of Montefiore Medical Center
DIVISION OF GENERAL INTERNAL MEDICINE
In 25 Minutes…
● Update the most recent studies…how should they change my practice?
● How long to continue antiplatelet therapy for drug-eluting stents?
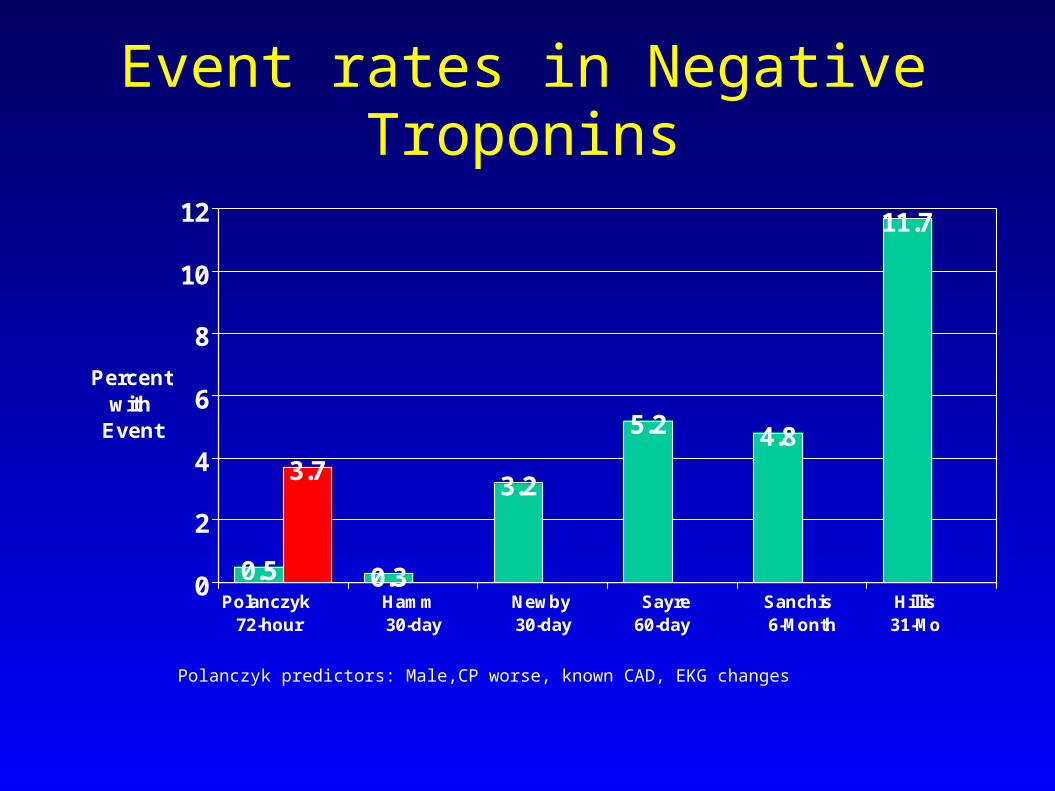
● Can I trust the Troponin? When is it safe to discharge?
● Inpatient stress test or not? Which one?
In 25 Minutes…
● Update the most recent studies…how should they change my practice?
● How long to continue antiplatelet therapy for drug-eluting stents?
● Can I trust the Troponin? When is it safe to discharge?
● Inpatient stress test or not? Which one?
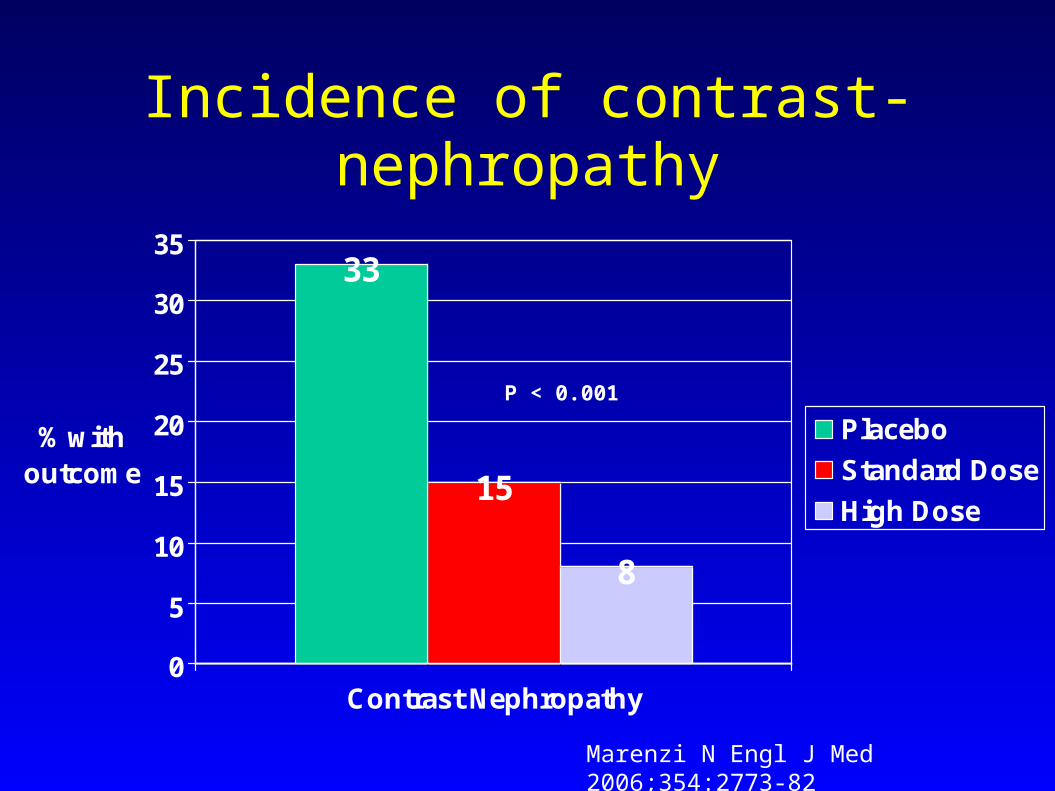
N-acetylcysteine for prevention of contrast-induced nephropathy in
primary angioplasty
Standard dose NAC(600mg IV before + 600mg PO bid x 48hrs)
vs.
High dose NAC(1200mg IV before + 1200mg PO bid x 48hrs)
vs.
Control
Marenzi N Engl J Med 2006;354:2773-82
N-acetylcysteine for prevention of contrast-induced nephropathy in
primary angioplasty
● Not blinded
● Outcomes:
1. Contrast Nephropathy: 25% increase in creatinine within 72hrs
2. Mortality, ARF (dialysis), Intubation
Marenzi N Engl J Med 2006;354:2773-82
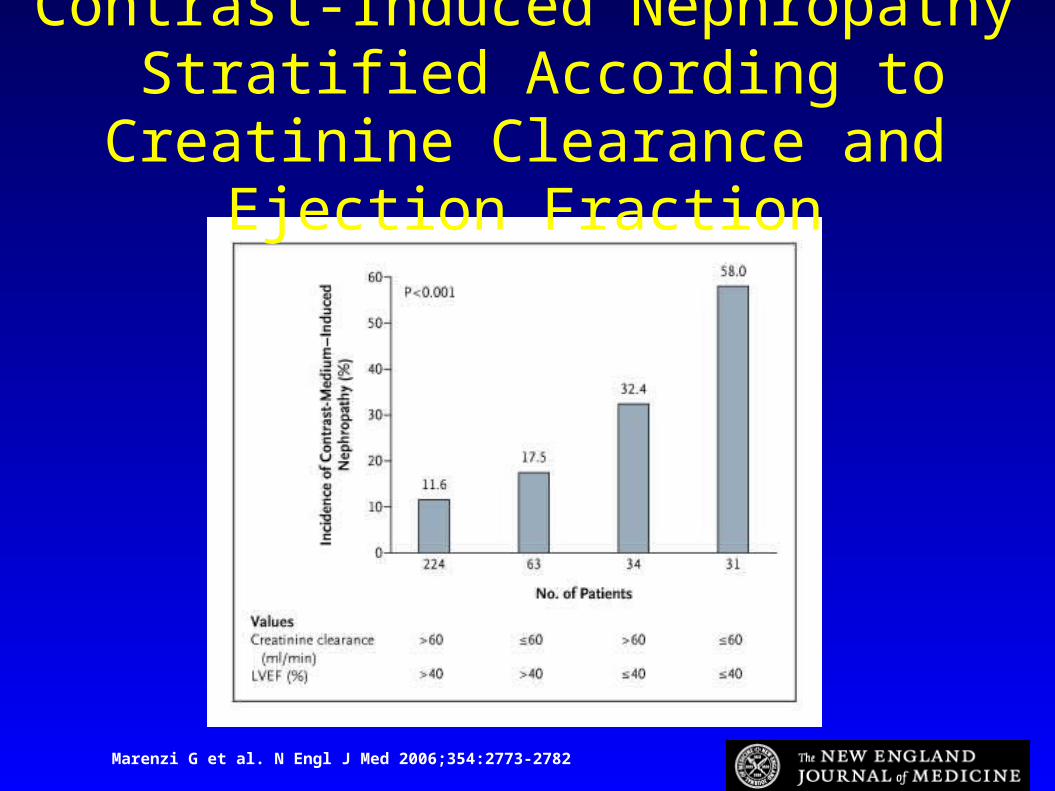
Marenzi G et al. N Engl J Med 2006;354:2773-2782
Contrast-Induced Nephropathy Stratified According to Creatinine Clearance and Ejection Fraction
Incidence of contrast-nephropathy
33
15
8
0
5
10
15
20
25
30
35
% with outcome
Contrast Nephropathy
Placebo
Standard Dose
High Dose
Marenzi N Engl J Med 2006;354:2773-82
P < 0.001
Clinical Outcomes
18
7
5
0
2
4
6
8
10
12
14
16
18
% with outcome
Composite*
Control
Standard Dose
High Dose
Marenzi N Engl J Med 2006;354:2773-82
*Mortality, Dialysis, Mech Ventilation
P = 0.001
Clinical Outcomes
5
21
8
2 2
11
43
0
2
4
6
8
10
12
% with outcome
ARF requiringHD
Intubation In-hosp Mort
Control
Standard Dose
High Dose
Marenzi N Engl J Med 2006;354:2773-82
P = 0.04 P = 0.007
P = 0.02
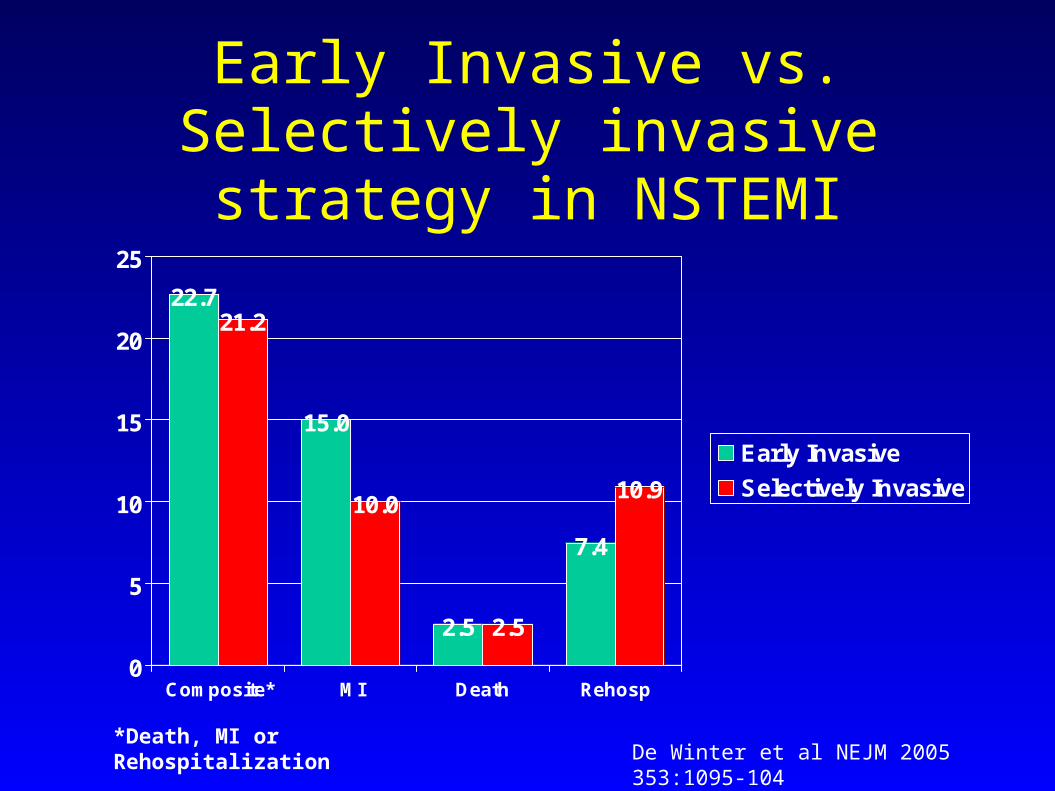
Early Invasive vs. Selectively invasive strategy in NSTEMI
● 1200 patients with elevated Troponin T and either ECG changes or known history of CAD
● Early invasive strategy: Catheterization and PCI within 24-48 hours
● Selectively invasive strategy: Catheterization if failed optimal medical therapy or clinically significant ischemia on non-invasive testing
De Winter et al NEJM 2005 353:1095-104
22.721.2
15.0
10.0
2.5 2.5
7.4
10.9
0
5
10
15
20
25
Composite* MI Death Rehosp
Early Invasive
Selectively Invasive
Early Invasive vs. Selectively invasive strategy in NSTEMI
De Winter et al NEJM 2005 353:1095-104*Death, MI or Rehospitalization
Meta-analysis of early-invasive vs. selectively invasive strategy for NSTEMI
12.2
14.4
5.5 6.07.3
9.4
0
2
4
6
8
10
12
14
16
Composite* Death MI
Early Invasive
Selectively Invasive
Mehta et al JAMA 2005;293:2908-17*Death or MI
Study showing non-inferiority of selective approach had: