46
Acute Diarrheal Disease Management. Dr John P George
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | johngeorge123 |
| View: | 262 times |
| Download: | 0 times |
Acute Diarrheal Disease Management.
Dr John P George
ASSESSMENT OF THE CHILD WITH DIARRHEA
1. History
• Ask the mother or other caretaker about:
• duration of diarrhea,
• number of watery stools per day,
• type of stool.
• presence of blood in the stool;
• number of episodes of vomiting;
• Abdominal Distention

ASSESSMENT OF THE CHILD WITH DIARRHEA
• pre-illness feeding practices; ? Bottle feeding
• type and amount of fluids (including breast milk) and food taken during the illness;
• drugs or other remedies taken;
• immunization history
• socioeconomic history- water source

ASSESSMENT OF THE CHILD WITH DIARRHEA
2. Physical examination
• First, check for signs and symptoms of dehydration.
• Look for these signs:
• General condition: is the child alert; restless or irritable; lethargic or unconscious?
• Are the eyes normal or sunken?
• Are tears present in the eyes?

ASSESSMENT OF THE CHILD WITH DIARRHEA
• Whether the tongue moist or not
• When water or ORS solution is offered to drink, is it taken normally or refused, taken eagerly, or is the child unable to drink owing to lethargy or coma?
• Is the child malnourished? Look for signs of malnutrition .

ASSESSMENT OF THE CHILD WITH DIARRHOEA
• Feel the child to assess:
• Skin turgor . When the skin over the abdomen is pinched and released, does it flatten immediately, slowly, or very slowly (more than 2 seconds)
• Take the child's temperature:
• Fever may be caused by severe dehydration, or by a non-intestinal infection such as malaria or pneumonia.

Estimate the fluid deficitAssessment Fluid deficit as % of body
weightFluid deficit in ml/kg body weight
Assessment Fluid deficit as % of body weight
Fluid deficit in ml/kg body weight
No signs of dehydration <5% in an infant<3% in older child
<50 ml/kg
Some dehydration 5-10% in an infant3-6% in older child
50-100ml/kg
Severe dehydration >10% in an infant>6% in older child
>100ml/kg
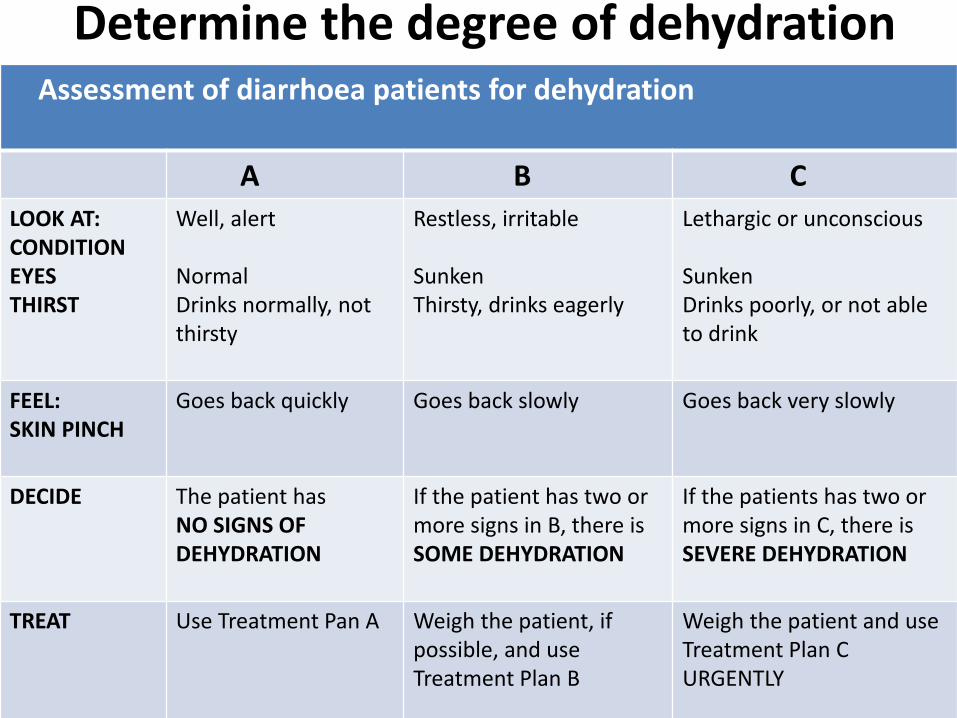
Determine the degree of dehydrationAssessment of diarrhoea patients for dehydration
A B C
LOOK AT: CONDITIONEYESTHIRST
Well, alert
NormalDrinks normally, notthirsty
Restless, irritable
SunkenThirsty, drinks eagerly
Lethargic or unconscious
SunkenDrinks poorly, or not ableto drink
FEEL: SKIN PINCH
Goes back quickly Goes back slowly Goes back very slowly
DECIDE The patient hasNO SIGNS OFDEHYDRATION
If the patient has two ormore signs in B, there isSOME DEHYDRATION
If the patients has two ormore signs in C, there isSEVERE DEHYDRATION
TREAT Use Treatment Pan A Weigh the patient, ifpossible, and useTreatment Plan B
Weigh the patient and useTreatment Plan CURGENTLY

MANAGEMENT OF ACUTE DIARRHEA
The objectives of treatment are to:
• prevent dehydration, if there are no signs of dehydration;
• treat dehydration, when it is present;
• prevent nutritional damage, by feeding during and after diarrhoea.
• Prevent spread of the enteropathogen

MANAGEMENT OF ACUTE DIARRHEA
• In select cases, determine the etiologic agent and provide specific therapy if indicated.
• reduce the duration and severity of diarrhoea, and the occurrence of future episodes, by giving supplemental zinc

Treatment Plan A
• home therapy to prevent dehydration and malnutrition
• Give the child more fluids than usual, to prevent dehydration
• Most fluids that a child normally takes can be used. It is helpful to divide suitable fluids into two groups:
• Fluids that normally contain salt, such as:• ORS solution• salted drinks (e.g. salted rice water or a salted
yoghurt drink)• vegetable or chicken soup with salt.

Treatment Plan A
• Fluids that do not contain salt, such as:
• plain water
• water in which a cereal has been cooked (e.g. unsalted rice water)
• unsalted soup
• yoghurt drinks without salt
• green coconut water
• weak tea (unsweetened)
• unsweetened fresh fruit juice.

Treatment Plan A:
• Unsuitable fluids
• A few fluids are potentially dangerous and should be avoided during diarrhoea. Especially important are drinks sweetened with sugar, which can cause osmotic diarrhoea and hypernatraemia. Some examples are:
• commercial carbonated beverages
• commercial fruit juices
• sweetened tea.

Treatment Plan A
• How much fluid to give
• The general rule is: give as much fluid as the child wants until diarrhoea stops. As a guide, after each loose stool, give:
• children under 2 years of age: 50-100 ml (a quarter to half a large cup) of fluid; give a teaspoon every 1-2 mins

Treatment Plan A
• children aged 2 up to 10 years: 100-200 ml (a half to one large cup);
• older children and adults: as much fluid as they want.
• For an older child, give frequent sips from a cup
• If the child vomits, wait for 10 mins. Then continue but more slowly ( e.g every 2-3 mins)

Treatment Plan A
• Take the child to a health worker if there are signs of dehydration or other problems
• The mother should take her child to a health worker if the child:
• starts to pass many watery stools;
• has repeated vomiting;
• becomes very thirsty;
• is eating or drinking poorly;
• develops a fever;
• has blood in the stool; or
• the child does not get better in three days

Oral Rehydration SolutionComposition of reduced (low) osmolarity ORS solution.
Grams/Litre Mmol/litre
Sodium chloride 2.6 Sodium 75 (mmol/L)
Glucose, anhydrous 13.5 Chloride 65
Potassium chloride 1.5 Glucose,anhydrous 75
Trisodium citrate, dihydrate
2.9 Potassium 20
Citrate 10
Total Osmolarity 245

Treatment Plan B:
• oral rehydration therapy for children with some dehydration
• Needs admission for observation in hospital
• ORS + Zinc(10-20mg/day)
• Amount of ORS needed for rehydration-
Weight x 75 ml given in first 4 hours
• When rehydration is complete, maintenance therapy should be started.
• Patients with mild diarrhoea usually can then be treated at home using 100 mL of ORS/kg/24 hr until the diarrhoea stops

Treatment Plan B:
• Supplementary ORS is given to replace ongoing losses from diarrhoea or emesis.10ml/kg of ORS to be given for each loose stool
• Breast-feeding should be allowed after rehydration in infants who are breast-fed; in other patients, their usual formula, milk, or feeding should be offered after rehydration

Guidelines for treating children and adults with some dehydration
Approximate Amount Of ORS to be given in 4 hours
Age Less than 4 months
4-11Months
12-23 Months
2-4 Years 5-14 Years 15 years or older
Weight Less than 5 Kg
5-7.9 Kg 8-10.9 kg 11-15.9Kg 16-29.9 Kg 30 kg or more
Volume(ml)
200-400 400-600 600-800 800-1200 1200-2200 2200-4000
Reference-THE TREATMENT OF DIARRHOEA-A manual for physicians and other senior health workers by WHO

Monitoring the progress of oral rehydration therapy
• If there are no signs of dehydration, the child should be considered fully rehydrated. When rehydration is complete:
• - the skin pinch is normal;
• - thirst has subsided;
• - urine is passed;
• - the child becomes quiet, is no longer irritable and often falls asleep.
• change to Plan A of Treatment

Monitoring the progress of oral rehydration therapy
• If the child still has signs indicating some dehydration, continue oral rehydration therapy by repeating Treatment Plan B.
• At the same time start to offer food, milk and other fluids, as described in Treatment Plan A
• continue to reassess the child frequently.

Monitoring the progress of oral rehydration therapy
• If signs of severe dehydration have appeared, intravenous (IV) therapy should be started following Treatment Plan C.
• This is very unusual, however, occurring only in children who
• drink ORS solution poorly and
• pass large watery stools frequently during the rehydration period
• frequent, severe vomiting.

Cascade for acute, mild/moderate, watery diarrhoea:
with mild/moderate dehydration.
High
↑Resources
↓
Low
Level 1
Intravenous fluids (consider) + ORT
Level 2
Nasogastric tube ORS—if persistent, vomiting
Level 3
ORT
Level 4
Home-made oral fluid: salt, sugar, and clean water
Reference: World Gastroenterology Organisation Global Guidelines Acute diarrhoea in adults and children: a global perspective

Treatment Plan C
• for patients with severe dehydration
• preferred treatment for children with severe dehydration is rapid intravenous rehydration
• Children who can drink, even poorly, should be given ORS solution by mouth until the IV drip is running.

Treatment Plan C
• In addition, all children should start to receive some ORS solution (about 5 ml/kg/h) when they can drink without difficulty, which is usually within 3-4 hours (for infants) or 1-2 hours (for older patients).
• This provides additional base and potassium, which may not be adequately supplied by the IV fluid.

Indication for IV fluids;
• Severe Dehydration with or without shock
• Persistent Vomiting
• Failure to correct or worsening of dehydration on ORT
• High purge rate
• Failure of Acceptance of ORS in dehydrated child
• Altered Sensorium/Seizures

IV Fluid Therapy
• Preferred solutions
• Ringer's Lactate Solution is the best commercially available solution.
• The concentration of potassium is low and there is no glucose to prevent hypoglycaemia
• Ringer's Lactate Solution with 5% dextrose has the added advantage of providing glucose to help prevent hypoglycaemia. If available, it is preferred to Ringer's Lactate Solution without dextrose

IV Fluid Therapy
Maintenance Fluids
• >6Yrs-12 years-%DN/2 with KCl 20 Meq/l
• >1 months-6 years- 5%DN/4 with KCl 20meq/l
• <1months 5%DN/6 with KCl 20meq/l

IV Fluid Therapy
Acceptable solution
• Normal saline (0.9% NaCl; also called isotonic or physiological saline) is often available.
• It does not contain a base to correct acidosis and does not replace potassium losses.
IV Fluid Therapy
• Unsuitable solution
• Plain glucose (dextrose) solution should not be used since it does not contain electrolytes
• and thus does not correct the electrolyte losses or the acidosis. It does not effectively correct hypovolaemia.

WHO Guidelines for intravenous treatment of children and adults with severe dehydration
Start IV fluids immediately. If the patient can drink, give ORS by mouth until the drip is set up.Give 100 ml/kgRinger's Lactate Solution divided as follows:
Age First Give 30ml/kg in Then give 70ml/kg in:
Infants 1 hour(b) 5 hours
Older 30 minutes(b) 21/2 hours
Reassess the patient every 1-2 hours. If hydration is not improving, give the IV drip more rapidly.• After six hours (infants) or three hours (older patients), evaluate the patient using the assessment chart. Then choose the appropriate Treatment Plan (A, B or C) to continue treatment.a If Ringer's Lactate Solution is not available, normal saline may be used).b Repeat once if radial pulse is still very weak or not detectable.

IV Fluid Therapy
Guideline for the total amount of fluid to be replaced in some and severe dehydration
Usual Fluid Deficit(ml/Kg)
Deficit FluidReplaced(ml/kg)
Maintenance fluid required in 8 hrs(ml/kg)
Total amount of fluid for correction of dehydration to be given in 8 hours
Some Dehydration
70-100ml 50 50 100
Severe Dehydration
120-180ml(>100<200)
100 50 150
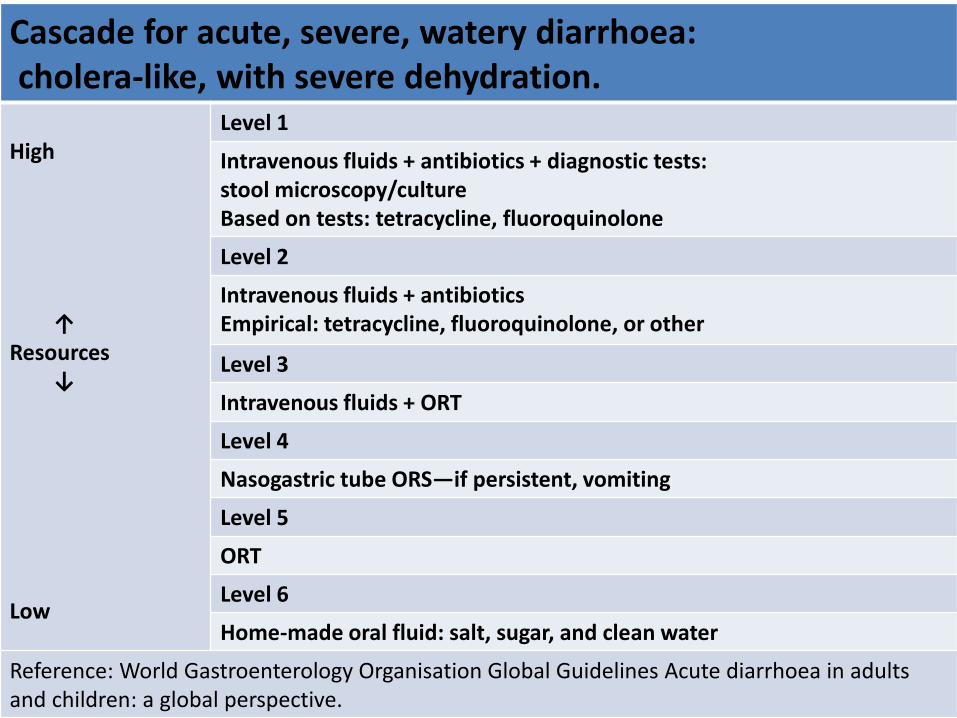
Cascade for acute, severe, watery diarrhoea:cholera-like, with severe dehydration.
High
↑Resources
↓
Low
Level 1
Intravenous fluids + antibiotics + diagnostic tests:stool microscopy/cultureBased on tests: tetracycline, fluoroquinolone
Level 2
Intravenous fluids + antibioticsEmpirical: tetracycline, fluoroquinolone, or other
Level 3
Intravenous fluids + ORT
Level 4
Nasogastric tube ORS—if persistent, vomiting
Level 5
ORT
Level 6
Home-made oral fluid: salt, sugar, and clean water
Reference: World Gastroenterology Organisation Global Guidelines Acute diarrhoea in adults and children: a global perspective.

Drug Therapy in Diarrhea.
• Definitive Indications
• Shigella Dysentry, giardiasis, infection with E.Hystolitica
• Cholera
• Septicemia, Diarrhea with systemic illness
• Moderate to severe PEM
• Immunocompromised Situations.

Drug Therapy in Diarrhea
• In dysentery, begin empirical therapy with cotrimoxazole (TMP-SMX) or ampicillin for 5 days
↓
If no improvement (disappearance of fever, less blood in stools, fewer stools, return to normal
activity) after 48 hours, change to Nalidixicacid for 5 days
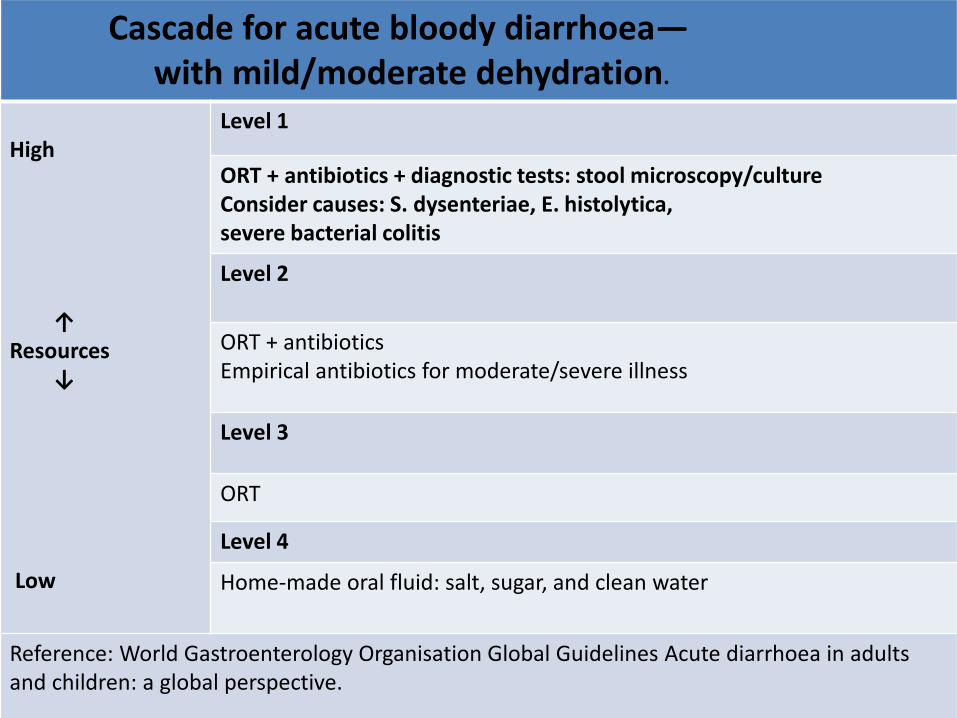
Cascade for acute bloody diarrhoea—with mild/moderate dehydration.
High
↑Resources
↓
Low
Level 1
ORT + antibiotics + diagnostic tests: stool microscopy/cultureConsider causes: S. dysenteriae, E. histolytica,severe bacterial colitis
Level 2
ORT + antibioticsEmpirical antibiotics for moderate/severe illness
Level 3
ORT
Level 4
Home-made oral fluid: salt, sugar, and clean water
Reference: World Gastroenterology Organisation Global Guidelines Acute diarrhoea in adults and children: a global perspective.

Drug Therapy in DiarrheaCause Antibiotics of Choice Alternatives
Cholera DoxycyclineSingle dose of 6mg/kg POor
TetracyclineChildren: 12.5 mg/kg4 times a day x 3 days
ErythromycinChildren: 12.5 mg/kg4 times a day x 3 days
Shigella dysentery CiprofloxacinChildren: 15 mg/kg2 times a day x 3 days
PivmecillinamChildren: 20 mg/kg4 times a day x 5 days
CeftriaxoneChildren: 50-100 mg/kgonce a day IM x 2 to 5 day

Drug Therapy in Diarrhea
Cause Antibiotics of Choice Alternatives
Amoebiasis MetronidazoleChildren: 10 mg/kg3 times a day x 5 days (10days for severe disease)
Giardiasis AlbendazoleChildren: 400 mgonce a day x 5 days
Metronidazole15 mg/kg/24 hr divided tidPO for 5 days

Zinc Therapy
• Zinc has been identified to play a critical role in metalloenzymes, polyribosomes, the cell membrane, and cellular function, leading to the belief that it also plays a central role in cellular growth and in the function of the immune system.
• Intestinal zinc losses during diarrheaaggravate pre existing zinc deficiency.

Probiotics
• commonly used probiotic bacteria include Lactobacillus, Bifidobacteria and the yeast Saccharomyces boullardii.
• probiotics offer innumerable benefits to the host by alleviating symptoms of lactose intolerance.

Probiotics
Uses if Probiotics:
• They are also known to prevent
• acute diarrhea,
• traveler’s diarrhea,
• antibiotic associated diarrhea,
• Rotaviral diarrhea
• probiotics don’t work the same in everyone. Probiotics may be more effective in older people than in younger ones.

Probiotics
• Conclusions of the IAP National Task Force for use of probiotics in diarrhea, May 2006
• The group recommended that there is presently insufficient evidence to recommend probiotics in the treatment of acute diarrhea in our settings as:
• Almost all the studies till now were done in developed countries.
• It may not be possible to extrapolate the findings of these studies to our setting where the breast feeding rates are high and the microbial colonization of the gut is different

AntiSecretory Drugs.
• Rececodotil -Enkephalinase inhibitor preventing the breaking down of endogenous encephalins in GI tract. It decreases intestinal hypersecretion but not motility.
• Currently not indicated for acute diarhoealdisease.
• It should await more evidence from well designed RCT done in our settings.

AntidiarrhoealDrugs
• These agents, though commonly used, have no practical benefit and are never indicated for the treatment of acute diarrhoea in children.
• Adsorbents -e.g. kaolin, activated charcoal, cholestyramine
• Antimotility drugs e.g. loperamidehydrochloride, tincture of opium, codeine.

References
• Nelson Textbook of Pediatrics 19th edition
• IAP text Book of Peadiatrics• THE TREATMENT OF DIARRHOEA-A manual for
physicians and other senior health workers by WHO
• IAP Guidelines 2006 on Management of Acute Diarrhea
• World Gastroenterology Organisation Global Guidelines
• Acute diarrhea in adults and children: a global perspective February 2012.

















