Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this photo and/or video. If you don’t want your photo taken, please let us know. Thank you! DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics. .
Transcript
Video will be taken at this clinic and potentially used inProject ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow
Project ECHO to use this photo and/or video. If you don’t want your photo taken, please let us know. Thank you!
DISCLAIMER:
ECHO Nevada emphasizes patient privacy and asks participants to not share ANYProtected Health Information during ECHO clinics.
.
.
Acute Management of Agitation and Paranoia in Dementia
Alec ChangJohn Tan
Nancy Yan
.
.
Today’s focus is on acute, not chronic, management of agitation and paranoia in dementia
.
.
Agitation
• Excessive verbal or motor behavior• High potential to escalate into aggression• Exceeds “unsatisfied patient” or “having a bad day”
.
.
Your Experiences with Agitated Patients?
.
.
Where Does it Come From?Agitation can reflect a wide variety of causes:
• Medical• Delirium• Dementia (our focus today)
• Psychiatric• Mania (mood elevation) • Psychosis
• Substance Use• Amphetamine• Cocaine
• Personality • Borderline Personality Disorder
.
.
Assessment
SAFETY FIRST!
• Recognize prodrome• Assess level of threat• Involve security personnel/other staff (if necessary)• Chemical restraints (if necessary)
Trust your sense of comfort/fear
.
.
Assessment
• Try to find underlying cause (urine drug screen, labs, etc.), but safety of the patient is the most important consideration! (So don’t try to draw labs if it’s too much danger, e.g.)
.
.
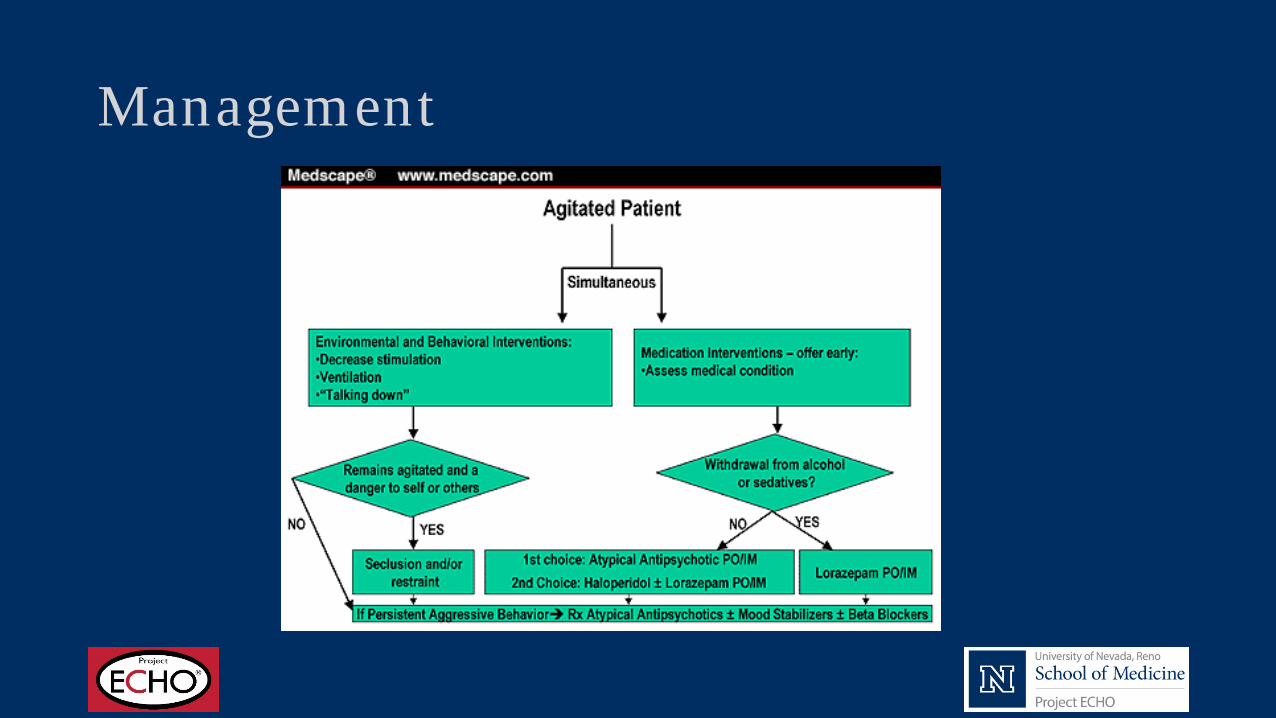
Management
.
.
Management
Create a safe environment
• Interview in quiet, non-stimulating setting• Provide sufficient space for patient, interviewer
• No barriers to leaving exam room for either party
• Avoid behaviors that can be seen as “menacing” • Standing over the patient• Staring at the patient• Touching the patient
.
.
Management
• Other non-medication interventions (talking patient down, establishing good rapport)
.
.
Management
Sometimes, chemical restraint is necessary
• Offer PO dose first• Giving options can be deescalating
• If patient remains uncooperative, administer IM • If patient poses immediate threat, administer IM
.
.
Black Box Warning
• Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death.
.
.
• However, the benefits need to be weighed against the risks of increased mortality when they are used by individuals with dementia.
• Patients with Lewy body dementia or Parkinson’s disease dementia are at increased risk for adverse effects.
• Treatment with an antipsychotic medication is indicated if a patient is agitated or combative, even in the absence of psychosis, because antipsychotics have the most support in the literature.
.
.
• APA recommends that if a risk/benefit assessment favors the use of an antipsychotic for behavioral/psychological symptoms in patients with dementia, treatment should be initiated at a low dose to be titrated up to the minimum effective dose as tolerated.
.
.
• Risk of mortality with an FGA in individuals with dementia is generally greater than the risk with an SGA
• The lack of head-to-head comparison data among antipsychotic medications on efficacy and on harms makes it difficult to designate a specific antipsychotic as being most appropriate to use as a first-line agent in treating agitation or psychosis in individuals with dementia
.
.
• Data from randomized placebo-controlled trials suggest efficacy for risperidone in treating psychosis and for risperidone, olanzapine, and aripiprazole in treating agitation.
• There was insufficient information from trials of quetiapine to determine whether it was efficacious in treating either agitation or psychosis, and it appeared to be no better than placebo in treating behavioral or psychological symptoms of dementia overall
• There is no information about the benefits or harms of asenapine, brexpiprazole, cariprazine, clozapine, iloperidone, lurasidone, paliperidone, or ziprasidone in individuals with dementia
.
.
Management
• Aripiprazole (Abilify) Antipsychotic PO or IM• Only IM approved for agitation, but no longer available in the US
.
.
Management
• Risperidone (Risperdal) Antipsychotic PO • Dose range: 0.5-1mg q1-4 hours PRN, max 3 doses
• Off label use• ODT available and may be helpful if the patient is unable to swallow.• IM not available.
.
.
Management
• Olanzapine (Zyprexa) Antipsychotic PO or IM• Dose: 10 mg IM q2-4 hours PRN, max 3 doses
• 5 mg or 7.5 mg when clinically warranted• 5mg should be considered for geriatric patients • 2.5 mg should be considered for patients who otherwise might be debilitated, be
predisposed to hypotensive reactions, or be more pharmacodynamically sensitive to olanzapine
• Assess for orthostatic hypotension prior to subsequent dosing • Side Effects
• Less potential for EPS/dystonia vs. Haldol• Metabolic syndrome (long term use) • Do not use IM Zyprexa and Ativan together: CNS and respiratory depression risk
.
.
Management
• Ziprasidone (Geodon) Antipsychotic PO or IM • Dose: 10mg IM q2 hours PRN or 20mg IM q4 hours PRN• Max Dose: 40mg/day (IM) • Side Effects
• Less potential for EPS/dystonia vs. Haloperidol• Less potential for metabolic syndrome vs. Olanzapine• QTc prolongation potential • Since there is no experience regarding the safety of administering ziprasidone
intramuscular to schizophrenic patients already taking oral ziprasidone, the practice of co-administration is not recommended.
.
.
Management
• Haloperidol (Haldol) Antipsychotic PO, IM, or IV• Dose: 0.5-10mg PO/IM/IV q1-4 hours PRN• Max Dose:
• 20mg/day IM/IV • 100mg/day PO
• Side Effects• Extrapyramidal symptoms• Acute dystonia• Neuroleptic malignant syndrome
• APA recommends that in the absence of delirium, if nonemergency antipsychotic medication treatment is indicated, haloperidol should not be used as a first-line agent
• Greater risk with haloperidol in clinical trials and cohort studies
.
.
Management
• Lorazepam (Ativan) Benzodiazepine PO, IM, or IV• Dose: 0.5-2mg PO/IM/IV q4-6 hours PRN• Max Dose: 10-12mg/day • Often given in combination with other drugs (including ones listed above,
except ziprasidone) • Side Effects:
• Respiratory depression
• Low-dose benzodiazepine may prove useful, although side effects in the elderly can be problematic
• May worsen cognition, increase the risk of falls, and put patients with sleep apnea at risk of additional respiratory depression.