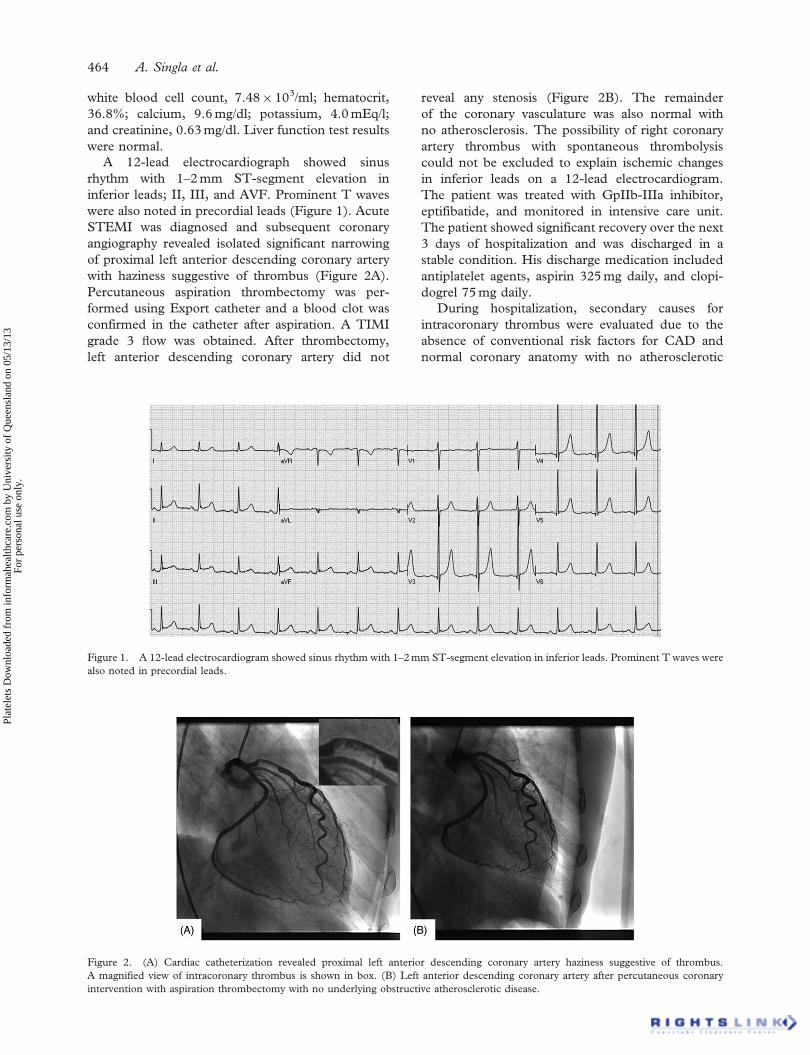
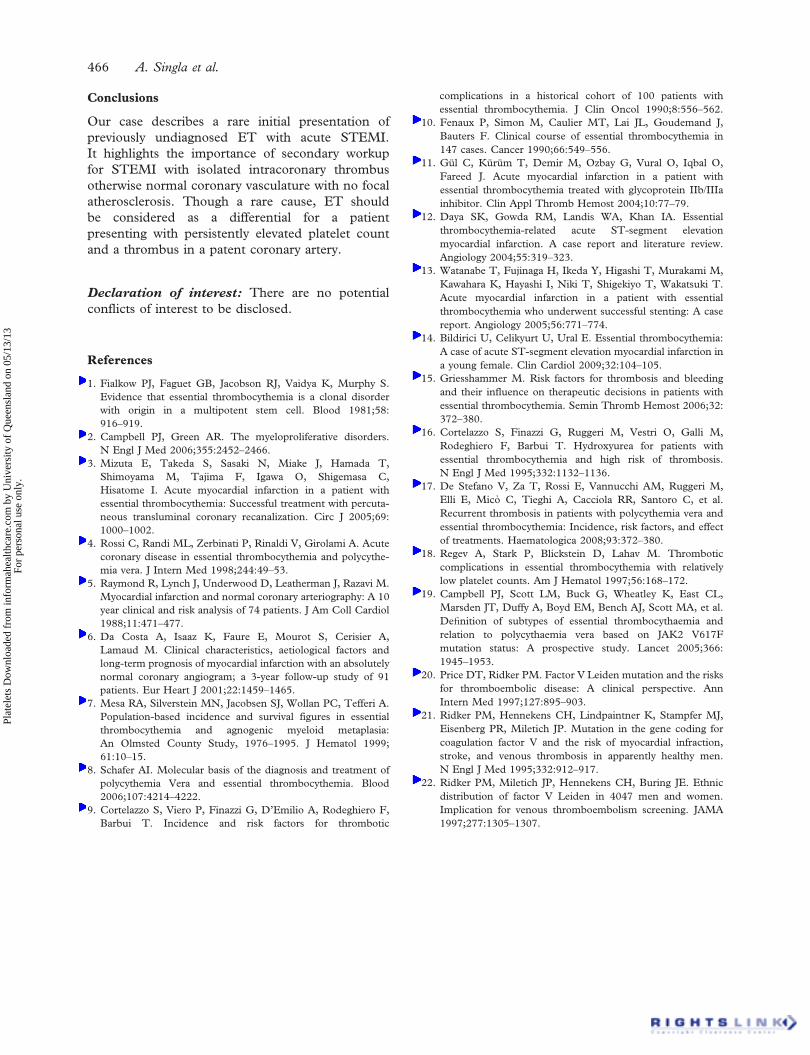
Platelets, September 2012; 23(6): 463–466 Copyright ß 2012 Informa UK Ltd. ISSN: 0953-7104 print/1369-1635 online DOI: 10.3109/09537104.2011.640966 ORIGINAL ARTICLE Acute ST-segment elevation myocardial infarction: A rare initial presentation of previously undiagnosed essential thrombocythemia ANAND SINGLA, DINESH JAGASIA, MUKESH GARG, PHILIP A LOWRY, & DWIGHT STAPLETON Guthrie Clinic, One Guthrie Square, Sayre, PA, USA Abstract Essential thrombocythemia (ET) is a myeloproliferative disorder characterized by hemorrhagic and thrombotic complications. We describe a rare case of ST-segment elevation myocardial infarction (STEMI) in a patient with previously undiagnosed ET, confirmed by gene mutation. A 68-year-old man presented with severe acute chest pain and was diagnosed with STEMI. Primary coronary angiography showed severe stenosis with thrombus in the proximal left anterior descending coronary artery. Percutaneous aspiration thrombectomy was performed with no residual stenosis. The patient was discharged on antiplatelet agents, aspirin, and clopidogrel. Further investigations for intracoronary thrombus with no underlying atherosclerotic disease revealed positive Janus kinase 2 (JAK2) V617F gene mutation, and this was consistent with a diagnosis of ET with elevated platelet count. This case describes a rare initial presentation of previously undiagnosed ET with acute STEMI and highlights the potential importance of secondary workup for non-atherosclerotic causes of STEMI with isolated intracoronary thrombus otherwise normal coronary vasculature with no focal atherosclerosis. Keywords: Essential thrombocythemia, ST-segment elevation myocardial infarction Introduction Essential thrombocythemia (ET) is a myeloprolifera- tive disorder characterized by pathological clonal proliferation of megakaryocytes with persistently elevated platelet count [1, 2]. The clinical manifesta- tions of ET include hemorrhagic and thrombotic complications. Recent studies have demonstrated that thrombotic complications, especially thrombus in the cerebral, coronary, and peripheral arteries, are more frequent than hemorrhages in patients with ET [3]. The incidence of acute coronary events in patients with ET has been reported as high as 9.4% [4]. In the medical literature, few cases of acute myocardial infraction (AMI) have been reported in association with ET. Here, we report a rare case of ST-segment elevation myocardial infarction (STEMI) as the first clinical presentation of pre- viously undiagnosed ET, with positive Janus kinase 2 (JAK2) V617F gene mutation. Case discussion A 68-year-old Caucasian man with no significant past medical history presented to the emergency room reporting chest pain. His symptoms of severe, crushing, non-radiating, and retrosternal chest pain started 2 hours before he came to the emergency room. He reported no history of cardiac problems, was not taking any cardiac medications, and had no family history suggesting any cardiac diseases. Physical examination revealed moderate distress and diaphoresis. His pulse was 88 beats per minute, his blood pressure was 128/84 mm Hg, and his respiratory rate was 18 breaths per minute with 98% oxygen saturation on room air. Auscultation revealed normal S1 and S2 heart sounds with no murmur or gallop. His chest was clear to auscultation on both sides. Cardiac markers suggested cardiac ischemia; troponin I peaked at 3.13 ng/ml. He had thrombo- cytosis at the time of admission (platelet count ¼ 539 10 3 /l). Other laboratory values were Correspondence: Anand Singla, Fellow, Cardiovascular Diseases, Department of Cardiology, Guthrie Clinic/Robert Packer Hospital, One Guthrie Square, Sayre, PA 18840, USA. Tel: 570-882-2331. Fax: 570-887-2290. E-mail: [email protected](received 5 October 2011; revised 28 October 2011; accepted 9 November 2011) Platelets Downloaded from informahealthcare.com by University of Queensland on 05/13/13 For personal use only.
Transcript
Platelets, September 2012; 23(6): 463–466
Copyright � 2012 Informa UK Ltd.
ISSN: 0953-7104 print/1369-1635 online
DOI: 10.3109/09537104.2011.640966
ORIGINAL ARTICLE
Acute ST-segment elevation myocardial infarction: A rare initialpresentation of previously undiagnosed essential thrombocythemia
ANAND SINGLA, DINESH JAGASIA, MUKESH GARG, PHILIP A LOWRY,
& DWIGHT STAPLETON
Guthrie Clinic, One Guthrie Square, Sayre, PA, USA
AbstractEssential thrombocythemia (ET) is a myeloproliferative disorder characterized by hemorrhagic and thromboticcomplications. We describe a rare case of ST-segment elevation myocardial infarction (STEMI) in a patient with previouslyundiagnosed ET, confirmed by gene mutation. A 68-year-old man presented with severe acute chest pain and was diagnosedwith STEMI. Primary coronary angiography showed severe stenosis with thrombus in the proximal left anterior descendingcoronary artery. Percutaneous aspiration thrombectomy was performed with no residual stenosis. The patient wasdischarged on antiplatelet agents, aspirin, and clopidogrel. Further investigations for intracoronary thrombus with nounderlying atherosclerotic disease revealed positive Janus kinase 2 (JAK2) V617F gene mutation, and this was consistentwith a diagnosis of ET with elevated platelet count. This case describes a rare initial presentation of previously undiagnosedET with acute STEMI and highlights the potential importance of secondary workup for non-atherosclerotic causes ofSTEMI with isolated intracoronary thrombus otherwise normal coronary vasculature with no focal atherosclerosis.