67
Acute stroke treatment Tim Harrington
| Date post: | 20-Jan-2016 |
| Category: |
Documents |
| Upload: | andrea-kennedy |
| View: | 217 times |
| Download: | 0 times |

Acute stroke treatment
Tim Harrington

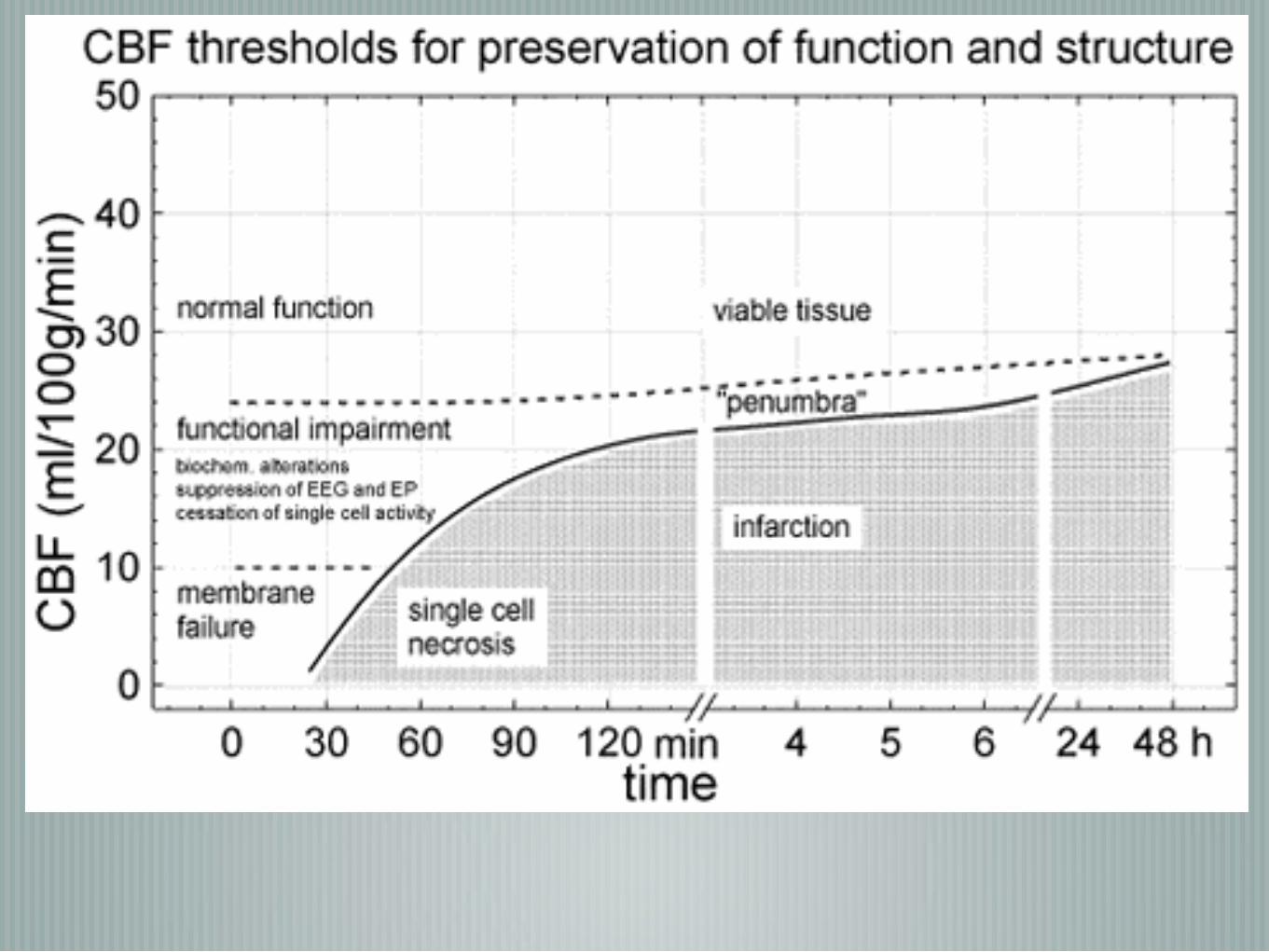
Important conceptsAll time loss/wastage results in further neuronal loss/poorer outcome
The rate at which neuronal loss occurs is highly variable
variations in COW and pial collaterals
Penumbra- injured but resurrectable brain
Patient selection is critical and is still controversial
CTP not reliable, MRP not readily available
IV and IA have differing strengths and weaknesses

Variability and reversibility of focal cerebral ischaemia in unanesthetized monkeys
Cromwell RM et alStroke lab, Uni of MassachusettsNeurology October 198131(10):1295-1302
‘neurologic improvement was common after the release of occlusion. …frequent with 30-min and 4-hour occlusions
…was observed even after 16 hours’

CONCEPTS
INFARCT CORE
ISCHAEMIC PENUMBRA

concepts
Core of irreversible injury
Penumbra sustained by peripheral collaterals: potentially salvageable with prompt institution of appropriate therapy

QuickTime™ and aH.264 decompressor
are needed to see this picture.

Aims
Recannalisation
Minimal delay
Minimal Cx- nb sICH
Optimise physiological parameters to minimise cerebral compromise
What do we know?
Most of morbidity and mortality comes from large vessel occlusions -46% of stroke involve large vessel occlusions and these have a poor prognosis (eg Basilar or ICA occlusion have 4.5 fold ↑ risk of death and 3 fold ↓risk of good outcome)-Smith WS et al Stroke 2009
Recanalisation associated with good outcome- 58 vs 25% Rha Stroke 2007
Higher rates of recanalisation with arterial embolectomy than IV tPA especially in the vessels that IV tPA is ineffective


Neuronal loss
32,000 neurones/min Average
Individual rates are highly variable and depend mainly on
quality/quantity of pial and other collateral
other drivers of perfusion such as BP
Time
A protocol that allows up to 4.5hrs does not mean that much time should be used up
Procedural time is often one of the least important delays in achieving recannalisation


TimeA successful acute stroke program will address delays throughout the treatment pathway
Public information re nature of stroke and urgency
Ambulance diversion to stroke centres
Rapid triage and informing of relevant teams
Imaging urgency
Parallel arrangement of consent, ICU, aneasthetics, bloods whilst waiting for other steps

IV Thrombolysis
Almost 20yrs old and still only <20% being treated in western countries- bolus + 1hr infusion
Only requires NCCT for triage
many contraindications- mainly re bleeding risk
not effective in large vessels
newer agents more fibrin specific eg Tenectoplase
Advanced imaging hoping to improve pt selection

IV Thrombolysis38% good outcome in NINDS in strokes selected for small size by clinical stroke score
recannalisation <10% in ICA, <25% in M1
Approx 9% sICH
Tenectoplase- ↑recannalisation, ↑neurological improvement Parsons et al
rtPA approved to 4.5hrs

Patient selection
Time is a poor surrogate for knowing an individual’s pathophysiology
Assessing ‘penumbra’
CTA and CTP whilst not having full validation proving to be useful tools and readily available- adds about 15min to NCCT

NECT
Haemorrhage
Cytotoxic oedema
Dense MCA sign

Lentiform nucleus

Insular stripe
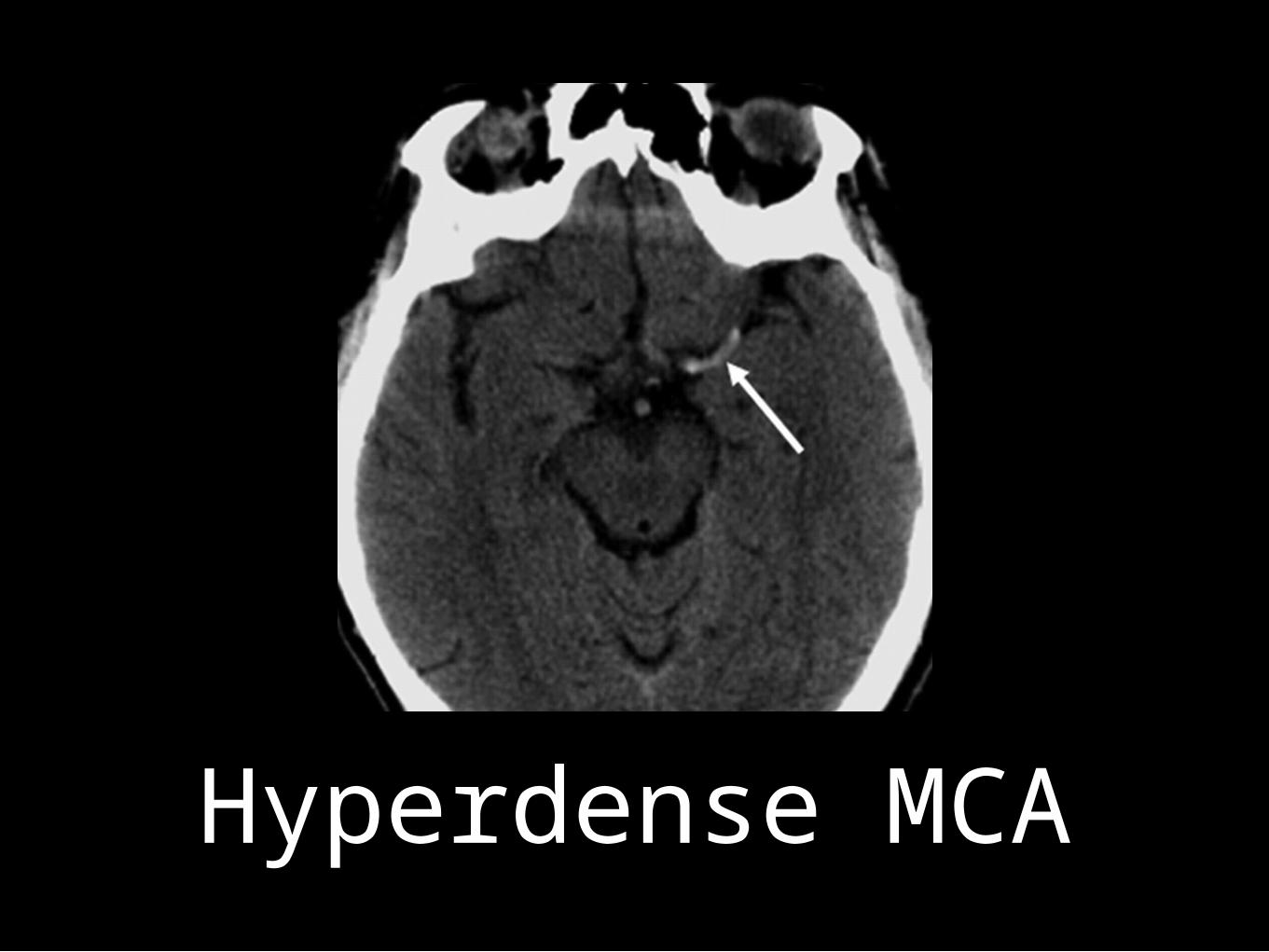
Hyperdense MCA

MRI
DWI measures “water motion”
Ischaemia: normal cellular ion pumps (eg Na-K) fail
Shift of water from extracellular to intracellular space
Cytotoxic oedema
Restricted diffusion


CT perfusion
Can be used to measure perfusion parameters
CBV
CBF
MTT

cerebral blood volume
Volume of blood per unit of brain tissue
4-5mL/100g

cerebral blood flow
Blood flow per unit of brain tissue per minute
50-60mL/100g/min

MEAN TRANSIT TIME
Time difference between arterial inflow and venous outflow
CEREBRAL ISCHAEMIA
Decreased CBF
Cerebral autoregulation
Capillary dilatation
CAPILLARY DILATATION
Increased CBV
Increased MTT

CRITICAL CBF LOSS
Normally 20%
Failure of autoregulation
Reduction in CBV
Reduction in CBF

Imaging the core
MRI DWI
Visible hypo-attenuation of NECT rarely reverses
CBV abnormality on Perfusion
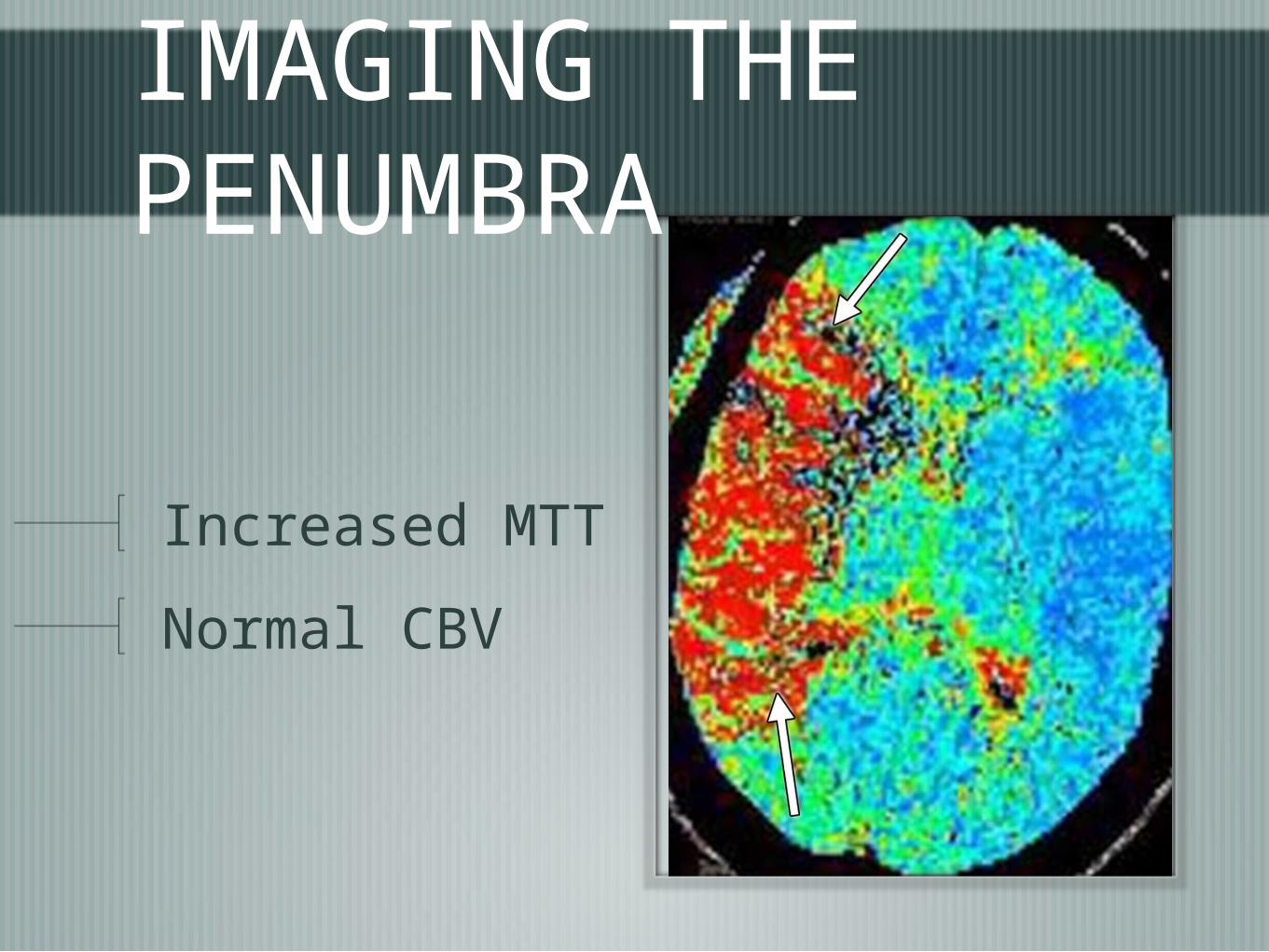
IMAGING THE PENUMBRA
Increased MTT
Normal CBV

CTA
Site of occlusion
length of occlusion
Tandem lesions- ICA source of embolus
Access issues
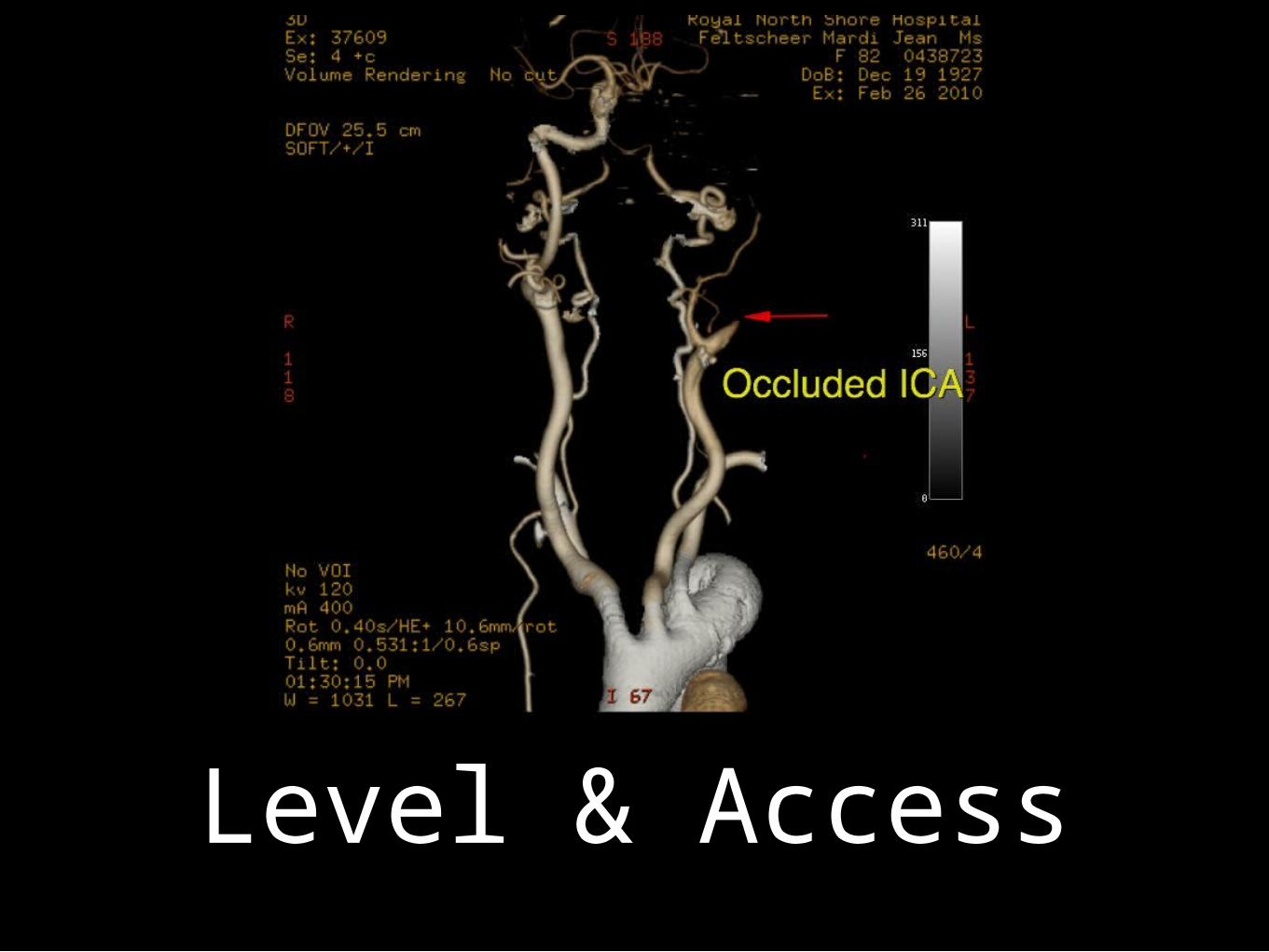
Level & Access
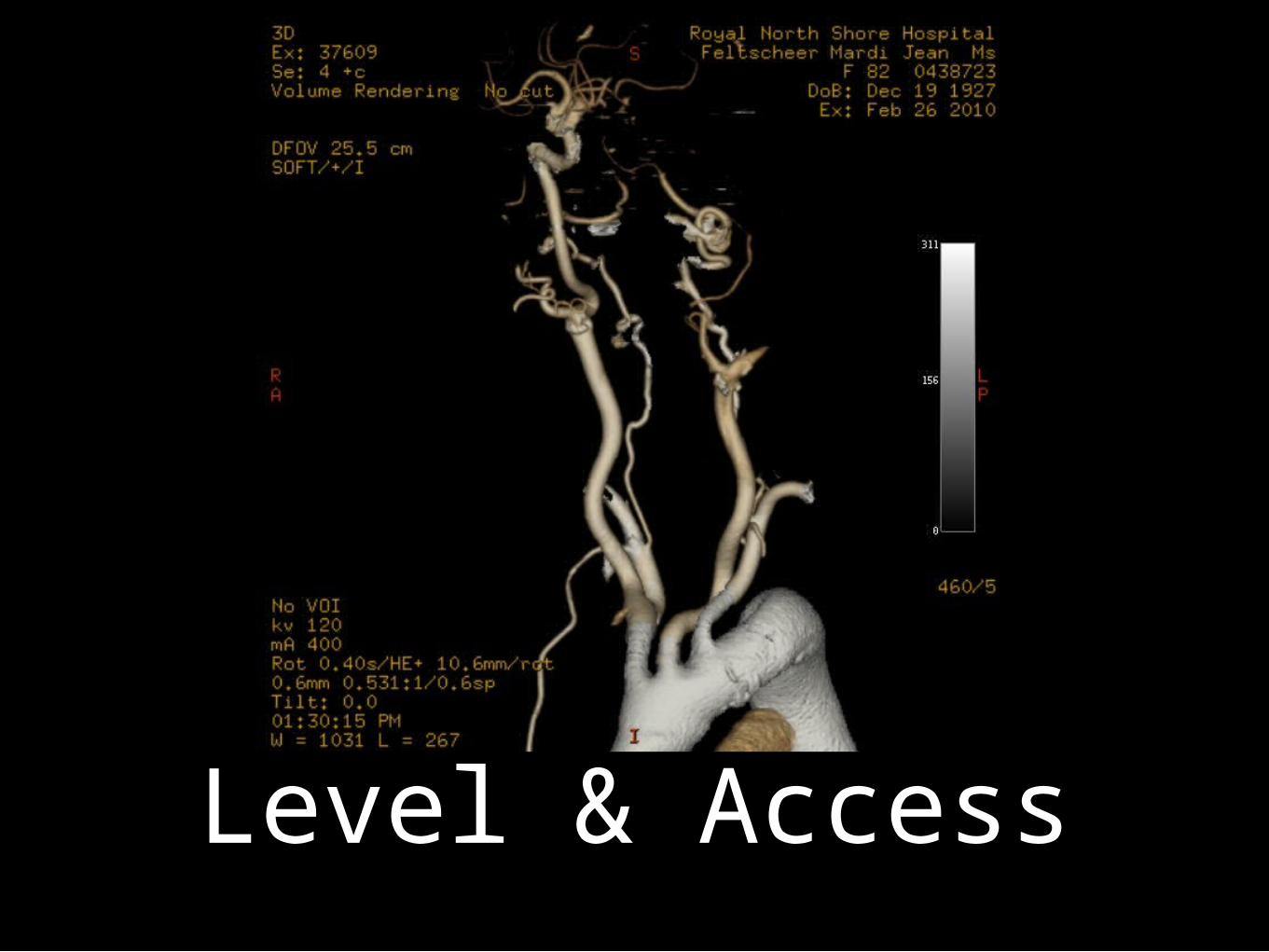
Level & Access

Imaging Core
CBV or DWI
Poor chance of good outcome if >25ml
Almost no chance of good outcome if >70ml
Severe perfusion changes predicts ICH TTP >14sec

Poor collateral/CTP 2hrs

Poor collaterals/CTP

Poor collaterals/CTP
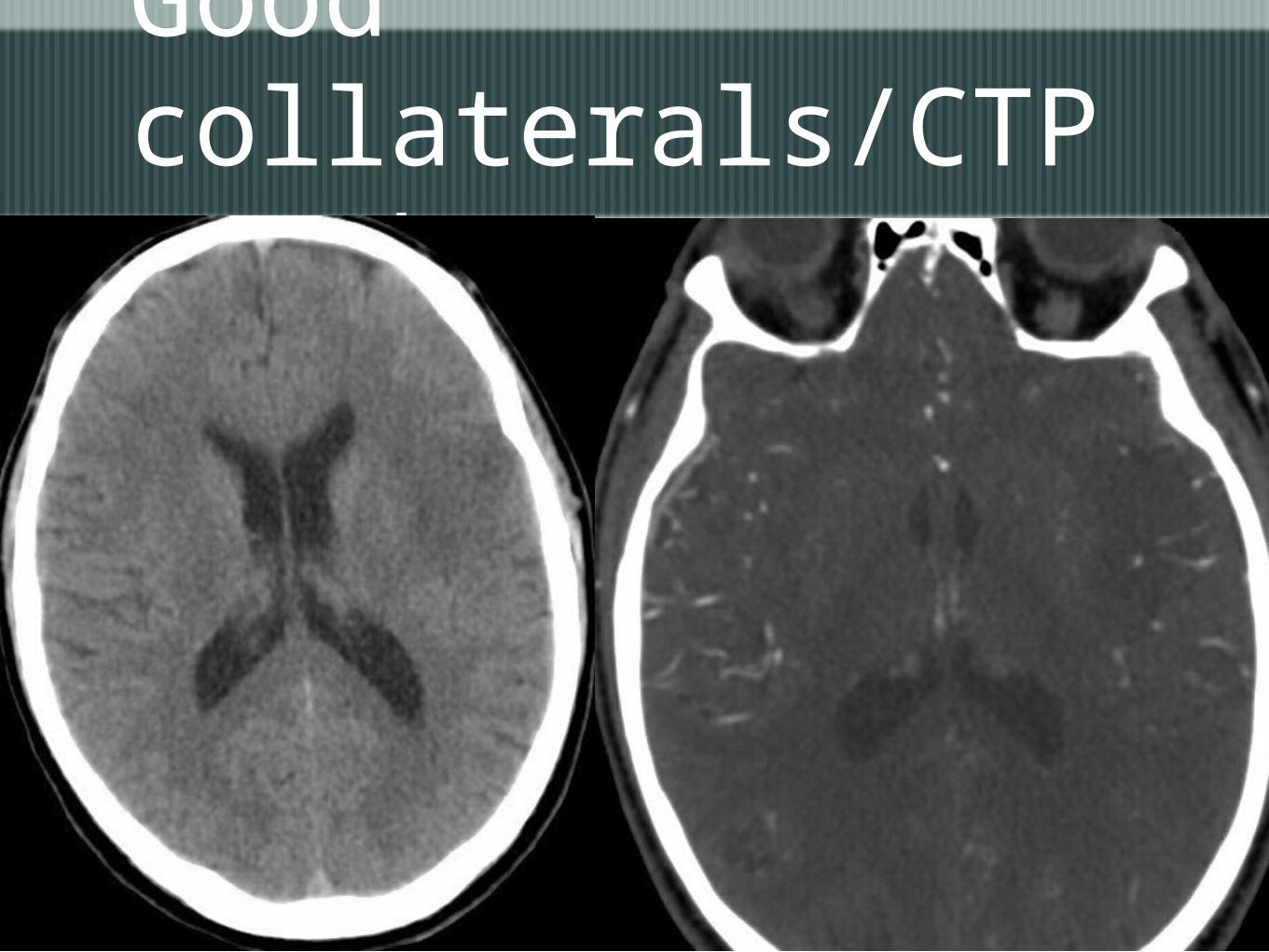
Good collaterals/CTP at 8hrs
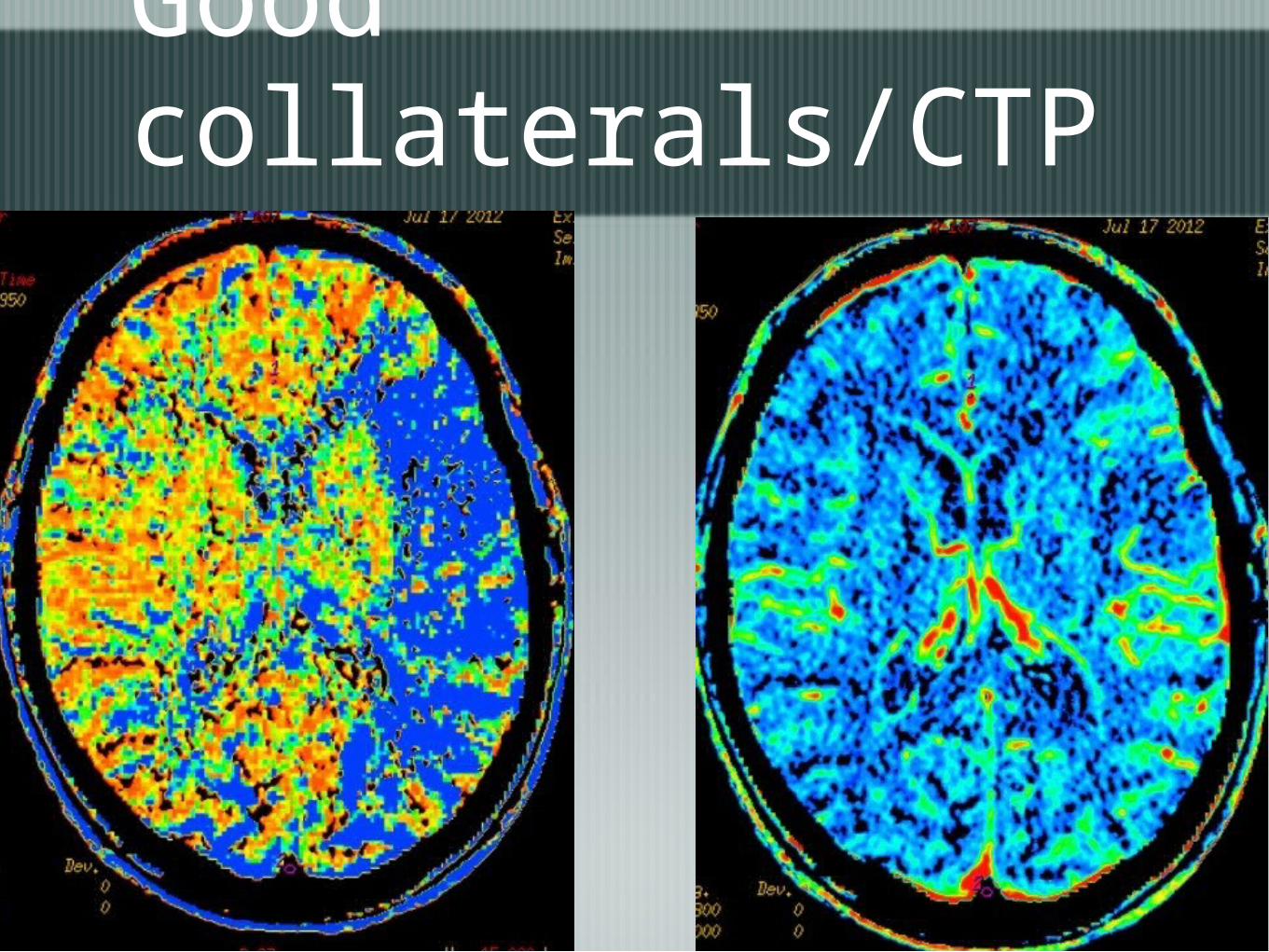
Good collaterals/CTP at 8hrs
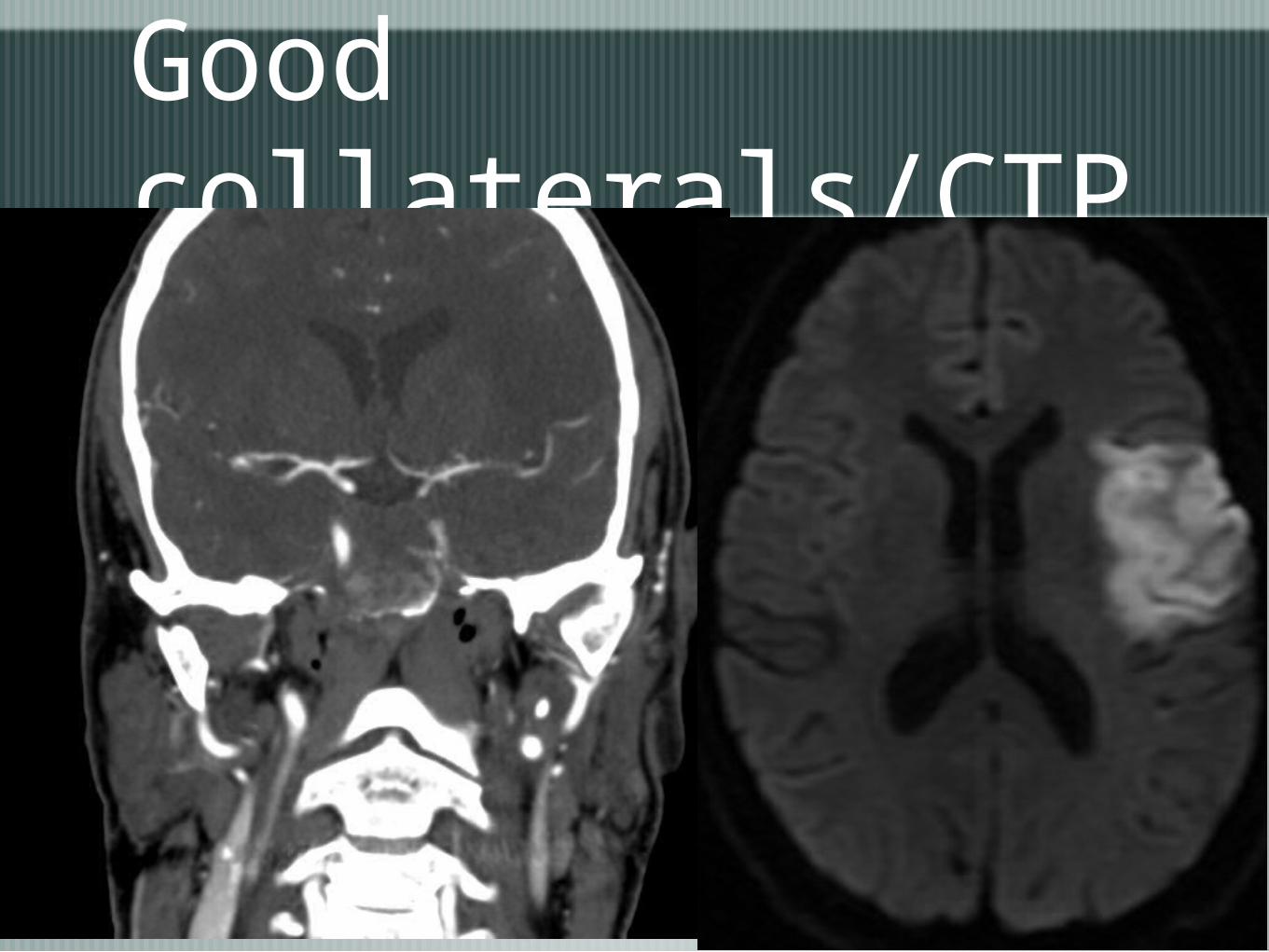
Good collaterals/CTP

IA therapy/embolectomy
Stentriever- Solitaire, Trevo, others
Direct aspiration- Penumbra
Combination of above

44554455

44664466
What do we know?iv tPA fails to recannalise in most
large vessel occlusions-25% success in M1,10% for ICA
Most patients do not receive iv tPA- at best 20% - time and other exclusions
Imaging can select gps with salvageable brain beyond 3-4.5hr time window Abou-Chebl A Stroke 2010
Efficacy?
Recannalisation rates of 80-90%
Average times to recann. of 40min
Frequent single pass recann-average no of passes 1.8

Outcomes
Miteff F- mRS≤2 in 56% ant circ’n 16pts
Galimanis A et al-623 pts prospective-48.9%
Soize S et al-36pts prospective- 63.9%
STAR- prospective registry multinational -58%

83yo female
SUDDEN COLLAPSE
DYSPHASIA

QuickTime™ and aMotion JPEG OpenDML decompressor
are needed to see this picture.
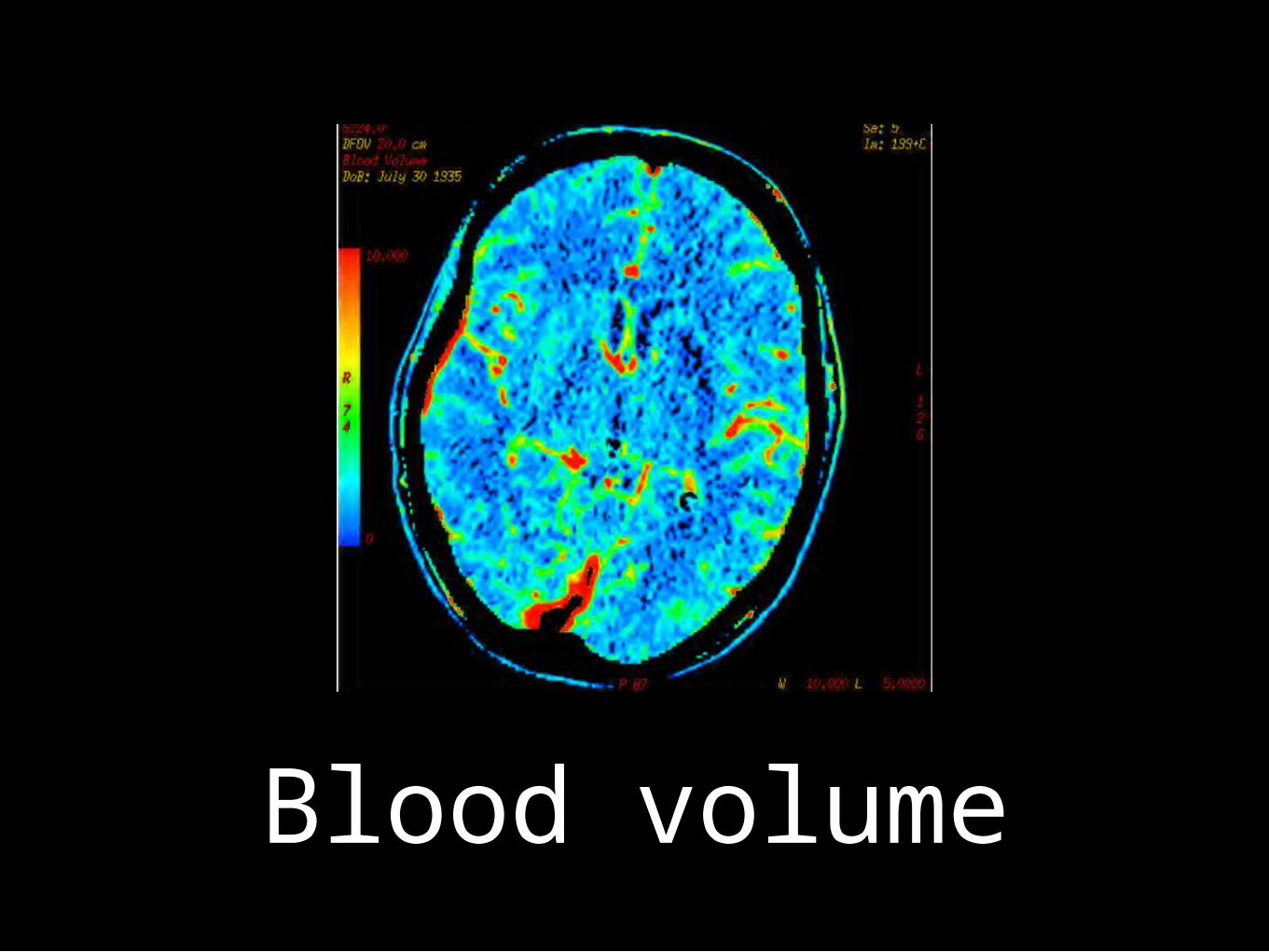
Blood volume

Mean transit time

QuickTime™ and aH.264 decompressor
are needed to see this picture.

QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.

QuickTime™ and aH.264 decompressor
are needed to see this picture.

PROCEDURE TIME: 15 MIN
SINGLE PASS


QuickTime™ and aMotion JPEG OpenDML decompressor
are needed to see this picture.
IV vs IA
IMS 111 failed but wrong devices used with unacceptable delays
Randomised trials in US , Europe and Aus
Evolving Protocol
Clinical then CT work-up
NCCT,CTA,CTP
IV rTPA in those suitable
Endovascular immediately in those with large vessel occlusion

Treatment selectionIV tPA has limit on size of vessel/thrombus it can dissolve
longer than 8mm embolus has 0 recann
should have occurred within 1hr of injection
Quick and no skill in delivery, can be used after limited imaging( NCCT as per NINDS)
‘drip and ship’ model

Treatment selectionArterial treatment restricted to large vessels
ICA, M1/2,Basilar
these are most morbid strokes
Technical issues/skill important
access difficult in elderly- ?restrict to <80yrs
Not interfered with by prior tPA and not limited by tPA limitations

Treatment synergyIV and IA are not really the competitors they are made out to be
Interested in different vessels
Extend IA- IV vs IV plus IA, similar UK/European studies
IMS 111- poor devices and prolonged delays in IA Rx

Treatment selectionIV thrombolysis- rTPA, tenectoplase
IA
stentriever
aspiration
IA thrombolysis

Thank You

















