27
Acyanotic Congenital Heart Disease Dr David Coleman Consultant Paediatric Cardiologist Our Lady’s Children’s Hospital, Crumlin Dublin
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | freddy-severn |
| View: | 226 times |
| Download: | 2 times |
Acyanotic Congenital Heart
Disease
Dr David Coleman
Consultant Paediatric CardiologistOur Lady’s Children’s Hospital, Crumlin
Dublin
Common Shunt Lesions
♥ Ventricular septal defect (VSD)
♥ Atrial septal defect (ASD)
♥ Patent ductus arteriosus (PDA)
* All 3 lesions can lead to Eisenmenger’s Syndrome if a large lesion is not detected and treated early enough
Common Stenotic Lesions
♥ Pulmonary stenosis (PS)
♥ Aortic stenosis (AS)
♥ Coarctation of the aorta (CoA)

VSD’s
♥ Commonest form of CHD
♥ Commonest types:membranous (perimembranous)
~75%muscular
♥ Can be single or multiple


VSD’s
♥ Symptoms relate to the degree of shunt (VSD size, pulmonary vascular resistance)
if small: no symptoms
if large (high pulmonary blood flow, CHF):tachypnoeadyspnoeaslow feeding failure to thrivesweating

VSD’s
♥ Exam (smaller VSD):pinknormal pulsesnormal S1 and S2± systolic thrillharsh pansystolic murmur
LLSE
♥ ECG: normal (smaller VSD)or LVH ± RVH (larger VSD)

VSD’s
♥ Larger defect:
MDM @ apex (mitral flow murmur)
narrowly split S2 and loud P2
± S3
CXR: cardiomegaly increased pulmonary
vascularity

VSD’s
♥ Treatment options:
Nil (spontaneous closure)
Surgical closure
Device closure

ASD’s
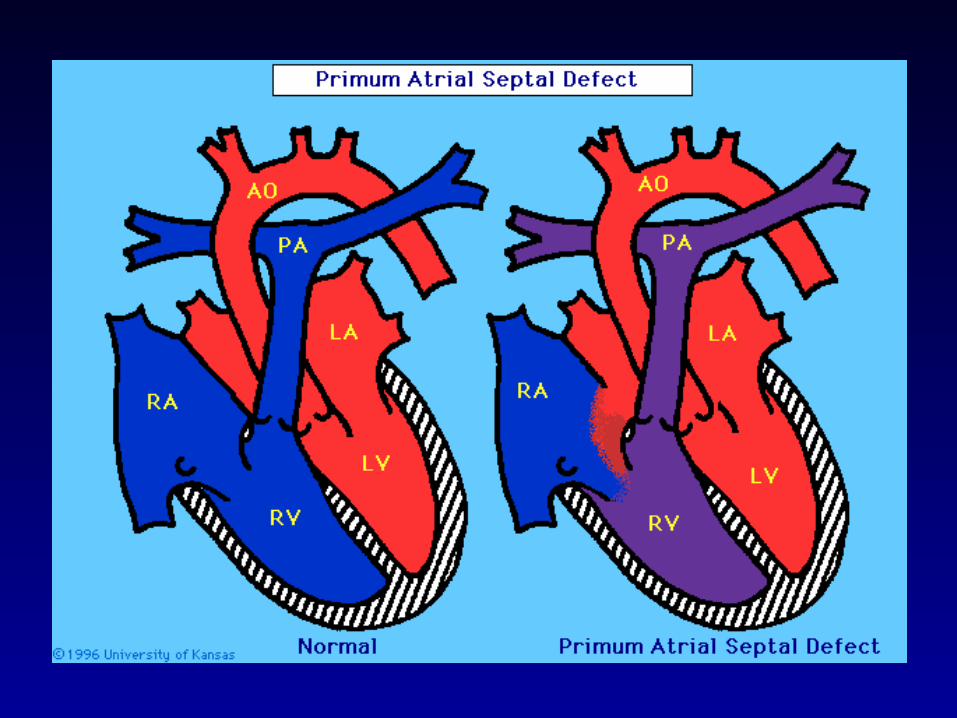
♥ Three types: secundumprimumsinus venosus
♥ Commonest: secundum
♥ Primum: a form of atrioventricular septal (canal) defect

Secundum ASD
♥ Usually no symptoms in childhood
♥ Exam: pinknormal pulseswide ± ‘fixed’ split S2soft ESM @ ULSE
♥ ECG: incomplete RBBB (95%)
♥ CXR: often normal sometimes pulmonary
plethora

Secundum ASD
♥ Haemodynamic significance of ASD is assessed to decide if closure appropriate
♥ Usually closed age 3-5 years (earlier if symptomatic) or when diagnosed if later
♥ Two options for closure:surgery - suture or patchinterventional catheter - device
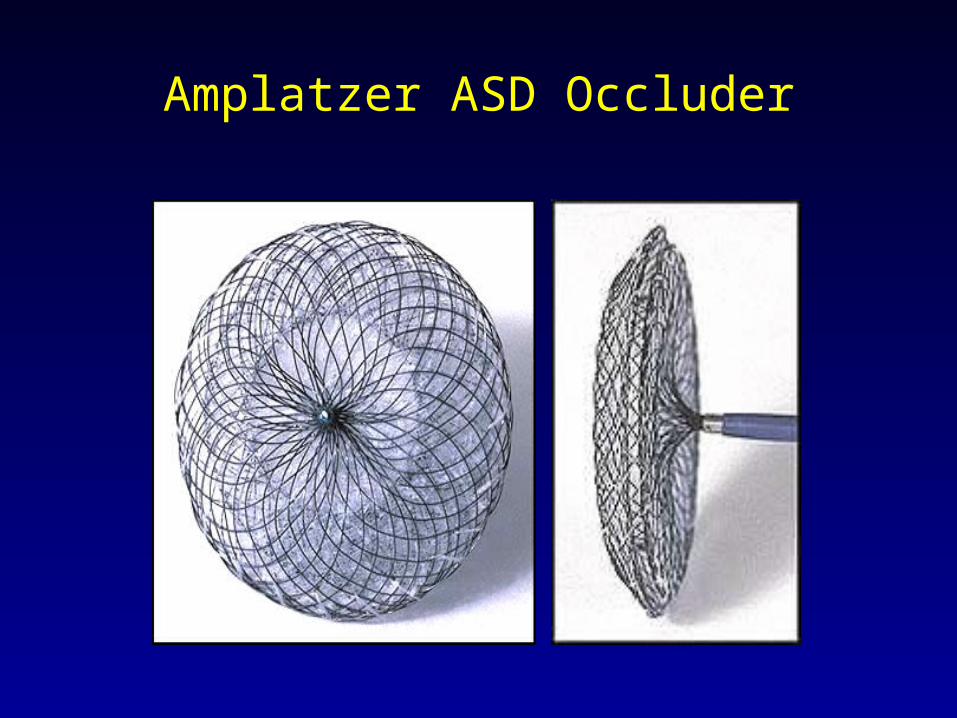
Amplatzer ASD Occluder

PDA
♥ CHF symptoms if large ductus in very young infant, otherwise often asymptomatic
♥ Exam: pinkfull volume pulsesharsh systolic (1st few weeks) or continuous ‘machinery’
murmur loudest under left clavicle
♥ ECG: normal (small PDA)LVH ± RVH (large PDA)


PDA
♥ CXR: ± cardiomegaly, pulm plethora
♥ Options for closure:
surgery - ligationinterventional catheter - coil(s) or
device
Pulmonary Stenosis
♥ Usually asymptomatic
♥ Exam: pinknormal pulses± systolic ejection clickESM loudest @ ULSE if severe, S2 widely split (not
fixed)

Pulmonary Stenosis
♥ ECG:RAD, RVH
♥ CXR: normal ± prominent MPA (post-stenotic dilatation)
♥ Treatment of valvar PS (moderate/severe):balloon valvuloplasty preferreduncommonly surgical
valvotomy

Aortic Stenosis
♥ Often asymptomatic; otherwise SOB, syncope or chest pain on exertion
♥ Exam: pinksmall volume pulse, small pulse pressure± LV lift± systolic thrill (suprasternal, URSE)± systolic ejection clickharsh ESM loudest @ URSE & radiating to carotidsif severe, narrow split S2 (even reversed)


Aortic Stenosis
♥ ECG:normal (mild AS)LVH ± strain (more severe AS)
♥ CXR: often normal± dilated ascending aorta
♥ Treatment of valvar AS (moderate/severe):balloon valvuloplastysurgical valvotomy
Coarctation of the Aorta
♥ CHF in neonate if severe CoA;often asymptomatic in older child
♥ Exam: pinkreduced or absent femoral
pulsessoft systolic murmur mid LSE and/or mid left back
♥ ECG:RVH in 1st few months of life,LVH if older


Coarctation of the Aorta
♥ CXR: cardiomegalyevidence of CHFrib notching (older child)
♥ Treatment:surgery for ‘native’ CoAballoon angioplasty for re-
CoA
!['Overview of the Palliative Care Service at Our Lady’s Children’s Hospital, Crumlin' (Presentation at the Maternity and Neonatal Network Meeting, April 2015) [MNN 12]](https://static.documents.pub/doc/80x56/58ecee1d1a28abad6b8b46d1/overview-of-the-palliative-care-service-at-our-ladys-childrens.jpg)
















