American Dietetic Association Standards of Practice
and Standards of Professional Performance forRegistered Dietitians (Generalist, Specialty, Advanced)
in Sports DieteticsThe American Dietetic Association Dietitians in Sports, Cardiovascular, and Wellness Nutrition Dietetic
Practice Group: Patricia L. Steinmuller, MS, RD, CSSD; Nanna L. Meyer, PhD, RD, CSSD; Laura J. Kruskall, PhD, RD, CSSD, FACSM; Melinda M. Manore, PhD, RD, CSSD, FACSM;
Nancy R. Rodriguez, PhD, RD, CSSD; Michele Macedonio, MS, RD, CSSD, FACSM; Randy L. Bird, MS, RD, CSSD, CSCS; Jacqueline R. Berning, PhD, RD, CSSD; and ADA Quality
Management Committee
The Sports, Cardiovascular, andWellness Nutrition Dietetic Prac-tice Group (SCAN DPG) of the
American Dietetic Association (ADA),under the guidance of the ADA QualityManagement Committee, has devel-oped Standards of Practice (SOP) andStandards of Professional Performance(SOPP) for Registered Dietitians (RDs)in Sports Dietetics (See the Web siteexclusive Figures 1, 2, and 3, at www.
adajournal.org). These documents arebuilt upon the ADA Revised 2008 SOPfor RDs in Nutrition Care and SOPPfor RDs (1). As part of ADA’s Scope of Dietetics Practice Framework (2), the2008 SOP in Nutrition Care and SOPPfor RDs, and ADA’s Code of Ethics (3),guide the practice and performance of RDs in all settings. The concept of scope of practice is fluid (4), changing inresponse to the expansion of knowl-edge, the health care environment, andtechnology. Recognizing advancementsin the practice of sports dietetics, theCommission on Dietetic Registration(CDR) established the Board CertifiedSpecialist in Sports Dietetics (CSSD)credential in 2006.
The 2008 SOP for RDs in NutritionCare and the SOPP for RDs are theresult of a review and update of the2005 ADA SOP in Nutrition Care andUpdated SOPP (5). The SOP in Nutri-
tion Care address the four steps of theNutrition Care Process (NCP) and ac-tivities related to patient/client careduring the NCP (6). They are designedto promote the provision of safe, effec-tive, and efficient food and nutritionservices, facilitate evidence-based prac-tice, and serve as a professional evalu-ation resource, enabling RDs to assesstheir current level of practice in meet-ing the Standards and to determine thetraining required for advancement to ahigher level of practice. The SOPP areauthoritative statements that describe
a competent level of behavior in theprofessional role. Categorized behav-iors that correlate with professionalperformance are divided into six sepa-rate standards. Together, the SOP andSOPP comprehensively depict the min-imum expectation for competent pa-tient/client care and professional be-havior for RDs.
SCAN DPG advocates that the afore-mentioned standards also be used toenhance recognition of the skills andexpertise of sports dietitians, educate
RDs and others about the CSSD cer-tification, guide the development of continuing education materials andprograms, and conduct and publishoutcomes research.
The indicators for the SOP andSOPP for RDs in Sports Dieteticswere developed with input and con-sensus of content experts represent-ing diverse practice and geographicperspectives and were reviewed andapproved by the Executive Commit-tee of the SCAN DPG, the Scope of Dietetics Practice Framework Sub-
Committee, and ADA’s Quality Man-agement Committee. A 2005 job anal-ysis survey for sports dietitiansconducted by CDR provided informa-tion to support the standards devel-oped for sports dietitians. These stan-dards are a guide for self-evaluationand improving practice, a means of identifying areas for professional de-
velopment, and a tool for demonstrat-ing competence in delivering sportsnutrition services.
Three levels of practice in sports di-
Approved November 2008 by the Quality Management Committee of the American Dietetic Association House of Delegates and the Executive Com-mittee of the Sports, Cardiovascular, and Wellness Nutrition Dietetic Prac-tice Group (SCAN DPG) of the American Dietetic Association. Scheduledreview date: March 2014. Questions regarding the Standards of Practice and Standards of Professional Performance for RDs in Sports Dietetics may beaddressed to Sharon McCauley, MS, MBA, RD, FADA, Director of Quality Management at ADA at [email protected] ; or Cecily Byrne , MS, RD, Manager of Quality Management at ADA at [email protected].
etetics care, generalist, specialty andadvanced, are defined. An entry-levelpractitioner has less than 3 years of registered practice experience anddemonstrates a competent level of die-tetics practice and professional perfor-mance. A general practitioner (or
generalist) is an individual whose prac-tice includes responsibilities across sev-eral areas of practice including, but notlimited to, more than one of the follow-ing: community, clinical, consultationand business, research, education, andfood and nutrition management. Aspecialty practitioner is an individ-ual who concentrates on one aspect of the profession of dietetics. This spe-cialty may or may not have a credentialand additional certification, but it oftenhas expanded roles beyond entry levelpractice. An advanced practitioner
has acquired the expert knowledgebase, complex decision-making skills,and competencies for expanded prac-tice, the characteristics of which areshaped by the context in which he orshe practices. Advanced practitionersmay have expanded or specialty rolesor both. Advanced practice may or maynot include additional certification.Generally, the practice is more com-plex, and the practitioner has a higherdegree of professional autonomy andresponsibility. In addition, it is recog-nized that sports dietetics care is mosteffectively undertaken with a multidis-
ciplinary focus and at a level beyondthat practiced by an entry-level RD.
These standards, along with the ADA’s Code of Ethics (3), answer thequestions: “Why is an RD uniquelyqualified to provide sports nutritionservices?” and “What knowledge,skills and competencies does an RDneed to demonstrate for the provisionof safe, effective, and quality sportsdietetics care at the generalist, spe-cialty, and advanced levels?” Thesestandards incorporate the principlesof ADA’s NCP. The outcomes (eg,
health of physically active people, en-ergy and fluid balance, appropriatefueling and hydration for trainingand competition, achieving and main-taining appropriate body weight andbody compositions goals, facilitatingathlete compliance with rules andregulations of sports organizationsregarding sport/dietary supplements)to be monitored and evaluated are theoutcomes of dietetics professionalspracticing in sports dietetics relatedto each step of the NCP along with
professional practices outlined in theSOPP.
Other practice guidelines that buildon the NCP are evidence-based sportnutrition guidelines, the establishedmedical nutrition therapy (MNT) pro-tocols for general dietetics care, and
best practice as determined by thosewith clinical expertise and extensiveexperience in sports dietetics in a
variety of settings. While these stan-dards are intended to serve as a pro-fession evaluation resource, the MNTprotocols are established practicetools that provide the specific contentto use with a patient/client when pro-
viding nutrition care using the NCP.These standards cover the continuumof care that primarily takes place inan outpatient setting and can be ex-tended to interactions with the sports
science researchers and medicine pro- viders, support staff (eg, coaches, ad-ministration), and/or other healthprofessionals. MNT protocols are tobe used when the athlete or activeindividual (patient/client) requirestreatment for a nutrition-related dis-ease or condition that is negativelyaffecting overall health or perfor-mance.
OVERVIEW
Public interest in nutrition and exer-cise has dramatically increased over
the last 20 years. This interest hasbeen fueled by factors such as the ris-ing incidence of obesity and chronicdisease and recognition that nutritionis integral to health and sport perfor-mance. With 66% of the US adult pop-ulation estimated to be overweight orobese, it is not surprising the interestin nutrition and exercise has in-creased (7,8). The role physical activ-ity plays in preventing weight gain,promoting weight loss, and prevent-ing weight gain subsequent to weightloss is well documented (9-11). The
importance of physical activity andnutrition for attaining optimal weightand overall health has also been high-lighted in a number of recent US De-partment of Health and Human Ser-
vices (DHHS) and US Department of Agriculture documents. These in-clude the Dietary Guidelines for Americans 2005 (12); Healthy People2010 (13), with 11 goals specific tonutrition and exercise; and the 2008Physical Activity Guidelines AdvisoryCommittee Report (14). The Physical
Activity Guidelines Report is the firstreport ever issued by the US govern-ment specifically for the Americanpublic with regard to the health ben-efits of physical activity that is accom-panied by a summary of the sciencesupporting these recommendations.
In addition, the Food and NutritionBoard issued Dietary Reference In-takes (DRIs) for energy intake, which,for the first time, specifically includesrecommendations for the level of physical activity required for weightmaintenance and weight loss (15).
Obesity and many chronic diseases(eg, cardiovascular disease, hyperten-sion, diabetes, and some cancers) areassociated with physical inactivityand poor dietary habits (16). RDs,especially those who are skilled innutrition, exercise, and weight man-
agement, are needed to assist indi- viduals, communities, organizations,and governments in realizing the
value of an integrative approach tonutrition and physical activity in pro-moting overall health and wellness.In addition, there is great interest inutilizing the interactions of food, nu-trition, and physical activity to de-
velop behavioral strategies that canreduce the risk of chronic diseases.For individuals interested in recre-ational sports and fitness, sports die-titians provide counseling in what,how much, and when to eat to main-
tain good health, appropriate bodyweight and composition, and to prop-erly fuel the body for activities en-
joyed by this population. Correspond-ingly, interest in the purportedbenefits of widely promoted sportsfoods, drinks, dietary supplements,popular diets, and quick-fix exerciseplans continues to grow. Sports dieti-tians provide sound food and nutri-tion advice appropriate for an individ-ual’s current level of fitness and sport/ physical activities, assist individualsin evaluating sports foods, drinks,
and dietary supplements, and helpclients meet their goals for healthybody weight and physical activity orsport.
For competitive or elite athletes,sports nutrition guidance can enhancetraining capacity, improve exercise per-formance, reduce the risk of injury, pro-mote appropriate body weight andcomposition, and strengthen the im-mune system. Applying sound nutri-tion strategies can also facilitate re-covery from strenuous exercise by
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 545
refueling and rehydrating the body,providing nutrients to build and re-pair muscles, and preparing athletesfor the next training session or com-petition. This is especially importantfor competitive athletes who competemultiple times per day or participate
in tournaments and for individualswho engage in strenuous, repetitiveexercise training one or more timesper day.
Proper nutrition can help speed thehealing process for injured athletes.Recovery from muscle or bone injuriesor from surgery requires extra energyand nutrients, including protein, vita-mins, and minerals. Sound nutritioncontributes to appropriate manage-ment of body weight and body compo-sition. Utilizing individualized ap-proaches to weight maintenance,
weight/muscle gain, or weight losscan significantly improve health andreduce stress. Sports dietitians edu-cate athletes regarding individual-ized menu planning, recipe modifica-tion, grocery shopping, and foodpreparation and storage. In addition,sports dietitians educate on the use of sports foods, drinks, and dietary sup-plements in compliance with the rulesand regulations of sports organiza-tions and governing bodies, such asthe National Federation of HighSchool Associations (NFHS), the Na-tional Collegiate Athletic Association
(NCAA), the US Olympic Committee(USOC), the United States Anti-Dop-ing Agency (USADA), the World Anti-Doping Agency (WADA), and profes-sional sports organizations such asthe Major League Baseball (MLB),the National Basketball Association(NBA), and the National FootballLeague (NFL).
A strong body of research evidencedemonstrating these benefits hasbeen compiled over the last 2 decades(17-19). This research has provided afoundation for evidenced-based gov-
ernment reports and position papersproviding specific nutrition guide-lines for individuals participating instrenuous exercise. Examples are thefollowing: the joint position paper onNutrition and Athletic Performanceby the ADA, the American College of Sports Medicine (ACSM), and the Di-etitians of Canada (20-24). In addi-tion, there are numerous reports bythe Committee on Military NutritionResearch (CMNR) of the Institute of Medicine (IOM) emphasizing the im-
portance of nutrition for soldiers per-forming high levels of physical exer-tion in harsh environments (25-28).Without question, the application of sports nutrition principles plays a vi-tal role in exercise training and per-formance, weight management, and
maintaining health of the athlete.The field is advanced by ongoing re-search in sports nutrition.
The sports dietitian working withathletes and active individuals inpractice settings needs to develop theappropriate knowledge, skills, andcompetencies to provide safe and ef-fective care. In addition, every effortis taken to assure confidentiality andcompliance with the regulations andstandards of the Health InsurancePortability and Accountability Act of 1996 (HIPPA). To provide sports nu-
trition guidance that addresses thediverse needs of athletes and activeindividuals, the sports dietitian mustpossess a breadth of knowledge andskills that can be applied to variedand complex situations. The key tooptimal nutrition for athletes is indi-
vidualization. The sports dietitianmust recognize the demands of theathletes’ annual training and compe-tition plans as well as the specificneeds of other patients/clients andwork to meet those needs with a per-sonalized approach. Patients or cli-ents deserve individualized and spe-
cific nutritional guidance related tooptimizing body weight and composi-tion; recommendations for energy,nutrient, and fluid intake before, dur-ing, and after exercise; guidance inplanning, selection, and preparationof meals and snacks; and use of sportsfoods, drinks, and dietary supple-ments in a variety of settings, includ-ing traveling for competitions.
The sports dietitian delivers nutri-tion information specific to varioussports or activities and has a thor-ough understanding of how energy
and nutrient needs change during the various phases of training and compe-tition. Equally important is the abil-ity to effectively educate athletes,coaches, athletic trainers, and othersregarding compliance with the rulesand regulations of sports organiza-tions (eg, NCAA, NFHS, USOC,USADA, WADA, MLB, NBA, NFL)specific to sports foods, drinks, anddietary supplements. To integrate nu-trition effectively into the athlete’sannual training and competition plan,
the sports dietitian works closely withcoaches, physiologists, and other mem-bers of the multidisciplinary team.Once an individual’s nutrient needs areestablished, the sports dietitian devel-ops a plan for the patient or client tomeet those nutritional goals with ap-
propriate quantity; quality; and timingof food, fluid, and intake of dietarysupplements when appropriate. Dailyschedule demands, environmental fac-tors, and cultural influences shouldalso be considered. Finally, in additionto performance outcomes, it is essentialfor sports dietitians to provide servicesthat promote the overall health andwellness of the athlete or active indi-
vidual.Sports dietitians have traditionally
worked with elite and recreationalathletes who are members of colle-
giate, club, and professional sportteams and in settings such as healthclubs, corporate wellness centers, andOlympic training centers. Sports die-titians are also being recruited towork with the military, military affil-iates and with occupational groupssuch as police and fire fighters wherehuman performance as well as phys-ical fitness is required. Moreover, de-mand is growing for sports dietitiansto be employed in a number of areas,such as private companies specializ-ing in sport performance by parentsfor their children’s health or sport
performance, and to work with ath-letes who have disabilities and otherspecial needs. Sports dietitians arealso hired as consultants by research-ers to assist in selecting appropriateassessment methods such as dietaryintake, nutritional status, energy ex-penditure, and body composition. Theclinical skills of sports dietitians areincreasingly required to provide MNTfor active and athletic patients or cli-ents diagnosed with medical condi-tions (eg, diabetes, gluten intoler-ance, food allergies, Crohn’s disease)
and in situations such as post–cancertreatment and post-bariatric surgery.Clearly, sports dietetics is a growingand demanding new field of study andpractice that requires the integrationof nutrition science and exercise prin-ciples and corresponding researchinto a variety of settings where activeand athletic populations participatein sports or workers engage in physi-cally demanding occupations.
One’s level of physical fitness andsport performance is determined by a
number of factors including geneticcharacteristics that influence physicalabilities, appropriate exercise trainingaimed at optimizing physical potential,and developing specific skills and dietbehaviors. Appropriate food choices canlead to improved performance and abil-
ity to train, while inadequate nutritionpractices can be detrimental to healthand performance outcomes. Beyond un-derstanding how research findings innutrition and exercise sciences aretranslated into nutrition guidelines forathletes and active individuals of allsports, ages, sexes, and competitive lev-els, sports dietitians must integratethese guidelines into the provision of high-quality sports dietetics care.
ADA SOP AND SOPP FOR RDs(GENERALIST, SPECIALTY, AND
ADVANCED) IN SPORTS DIETETICS
The sports dietitian uses the ADA SOPand SOPP (Generalist, Specialty, and
Advanced) for RDs in Sports Dietetics(see the Web site exclusive Figures 1, 2,and 3 at www.adajournal.org) to:
● identify the competencies needed toprovide sports dietetics care;
● self-assess whether they have theappropriate skill and knowledgebase to provide safe and effectivesports dietetics care for their levelof practice;
● identify the areas in which additionalknowledge and skills are needed topractice at the generalist, specialty,or advanced level of sports dieteticspractice;
● provide a foundation for public andprofessional accountability in sportsdietetics care;
● assist management in the planningof sports dietetics services and re-sources;
● enhance professional identity andcommunicate the nature of sportsdietetics;
● guide the development of sports di-etetics-related education programs,
job descriptions, and career path-ways; and
● assist preceptors in teaching stu-dents and interns the competenciesand skills needed to work in sportsdietetics and the understanding of the full scope of this profession.
CDR launched the CSSD certifica-tion for RDs in 2006. Members of theSCAN DPG assisted CDR in writing a
job analysis survey for sports dieti-tians and contributed to developingthe certification. A sports dietitianwho is a CSSD has met minimumpractice experience requirements andhas successfully completed the CSSDexamination. Eligibility criteria for
the credential, applications, andother information are available fromCDR (www.cdrnet.org). A sports die-titian’s job description, consistentwith specialty level practice, devel-oped by SCAN members is publishedin Job Descriptions: Models for the Dietetics Profession, 2nd ed, 2008(29). The CSSD certification, ADAsports dietitian job description, andthe SOP and SOPP for RDs in SportsDietetics are components of a systemthat assists sports dietitians in gaug-ing their level of practice and provid-
ing a pathway for advancement bydefining sports dietetics practice, doc-umenting skill levels, and establish-ing benchmarks. During the develop-ment of these standards, severalissues unique to nutrition interven-tion in sports dietetics settings wereidentified.
● Principles of exercise science andexercise physiology are integratedinto the application of the sportsdietetics care.
● A nutrition approach matched tothe athlete’s annual training andcompetition plan is an essentialcomponent of sports dietetics care.
● Exercise/athletic performance para-meters are considered in the man-agement of body weight and bodycomposition of the target population.
Application to Practice
Indicators described as specialty levelof practice designations in this docu-ment are not equivalent to the CSSDcertification. Rather, the CSSD desig-nation refers to an RD who has devel-
oped sports dietetics nutrition knowl-edge, skill, and application beyondthe entry-level or the generalist prac-titioner. An RD who has earned theCSSD certification is an example of an RD who has demonstrated, at aminimum, specialty level skills aspresented in this document.
The Dreyfus model (30) identifieslevels of proficiency (novice, specialist,advanced) during the acquisition anddevelopment of knowledge and skills.This model is helpful in understand-
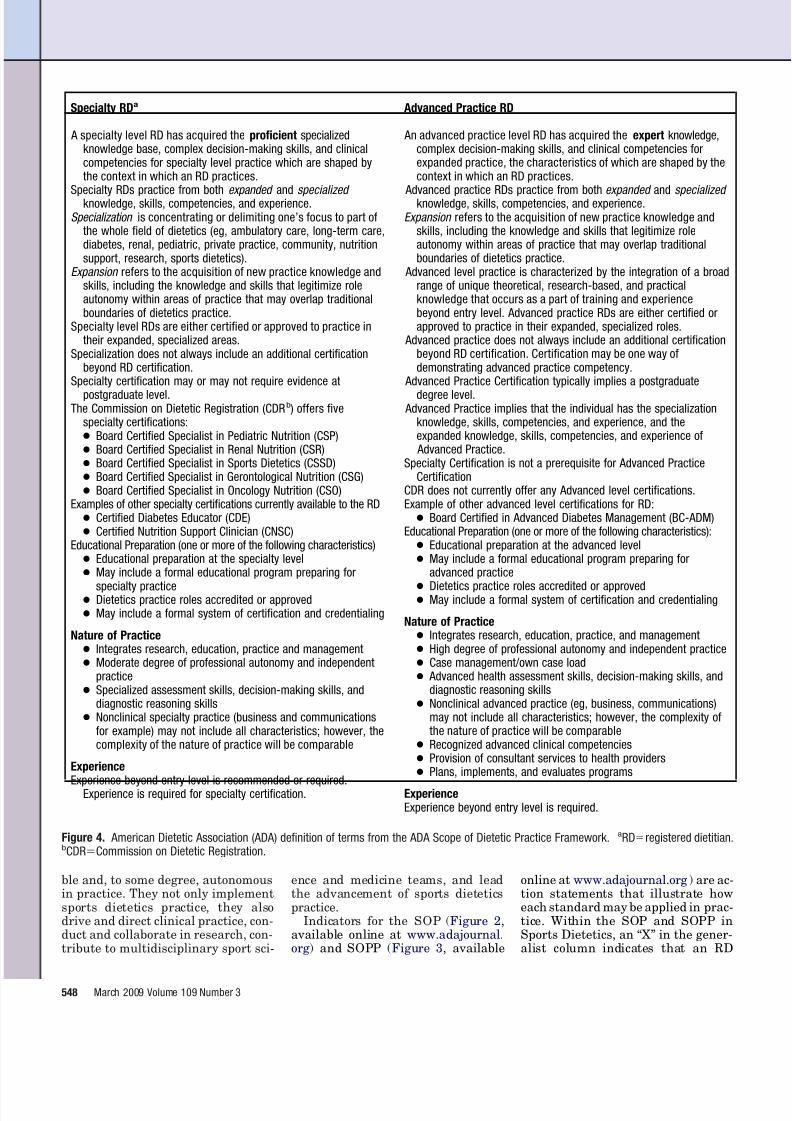
ing the levels of practice described inthe SOP and SOPP in Sports Dietet-ics. In ADA SOP and SOPP, thestages are represented as generalist,specialty, and advanced practice lev-els (Figure 4).
All RDs, even those with significant
experience in other practice areas, be-gin at the Novice level (generalistlevel) when practicing in a new set-ting. At the Novice level (generalistlevel), the RD in sports dietetics islearning the principles that underpinthe practice and is developing skillsfor effective sports dietetics practice.This RD, who may be an experiencedRD or may be new to the profession,has a breadth of knowledge in nutri-tion overall and may have specialty oradvanced knowledge/practice in an-other area. However, the RD new to
the specialty of sports dietetics mayexperience a steep learning curve dueto the wide range in demands posedby different sports and their special-ized annual training and competitionplans, the need for individualizedsports dietetics approaches, and thecomplexity of sports dietetics services.
At the Proficiency stage (specialtylevel), the RD has developed a deeperunderstanding of sports dietetics careand is much better equipped to applyevidence-based guidelines and bestpractices. This RD is also able to mod-ify practice according to unique situ-
ations (eg, integrating environmentalfactors such as heat, cold and altitudein the evaluation of an athlete’s en-ergy, fluid, and nutrient needs).
At the Expert stage (advanced prac-tice level), the RD thinks criticallyabout sports dietetics, demonstrates amore intuitive understanding of sports dietetics care and practice, anddisplays a range of highly developedclinical and technical skills (whichmay include but is not limited to per-forming sports-directed nutrition as-sessment) and formulates judgments
acquired through a combination of ex-perience and education. Essentially,practice at the advanced level re-quires the application of composite di-etetics knowledge, with practitionersdrawing not only on their clinical ex-perience, but also on the experience of the sports dietitians in various disci-plines and practice settings. Experts,with their extensive experience andability to see the significance andmeaning of sports dietetics within acontextual whole, are fluid and flexi-
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 547
ble and, to some degree, autonomousin practice. They not only implementsports dietetics practice, they alsodrive and direct clinical practice, con-duct and collaborate in research, con-tribute to multidisciplinary sport sci-
ence and medicine teams, and leadthe advancement of sports dieteticspractice.
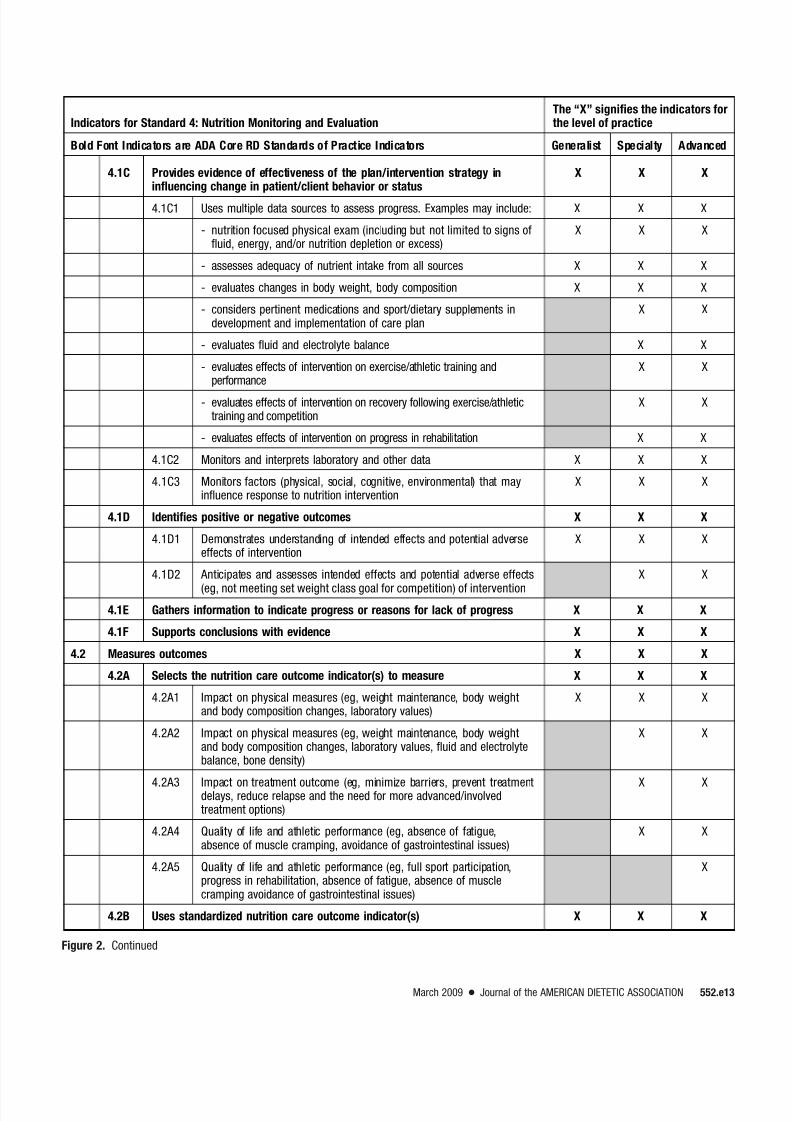
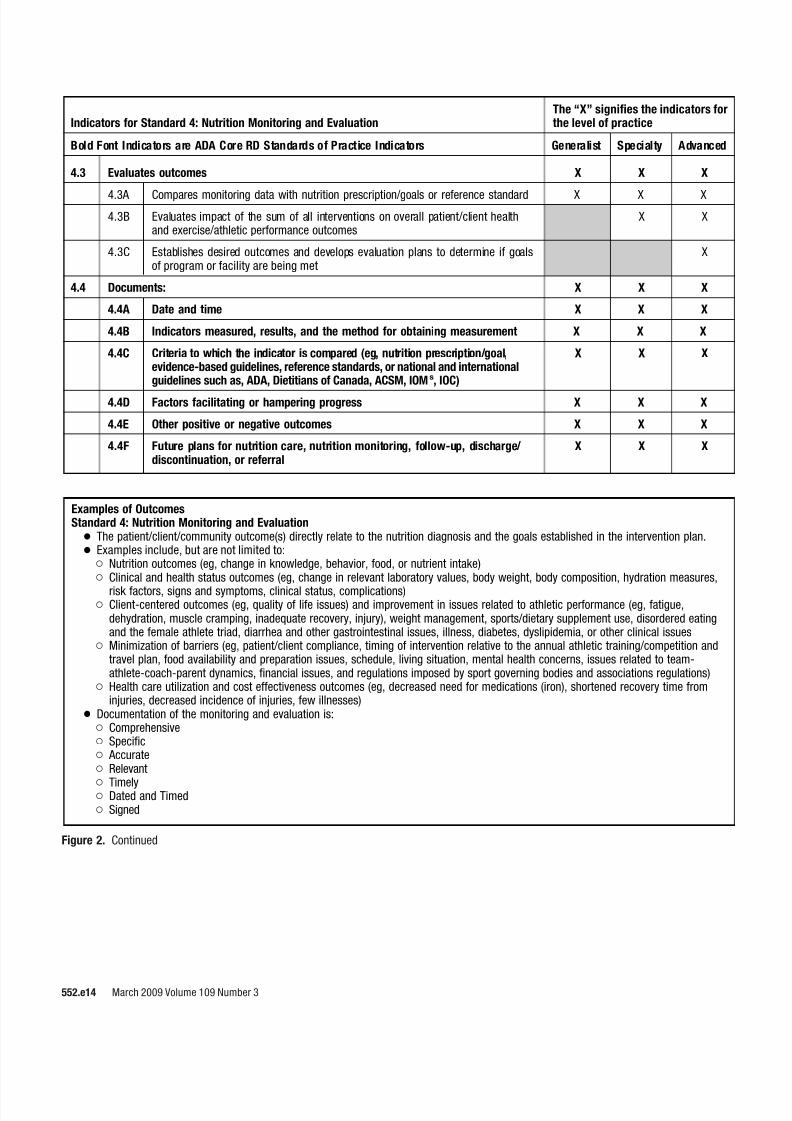
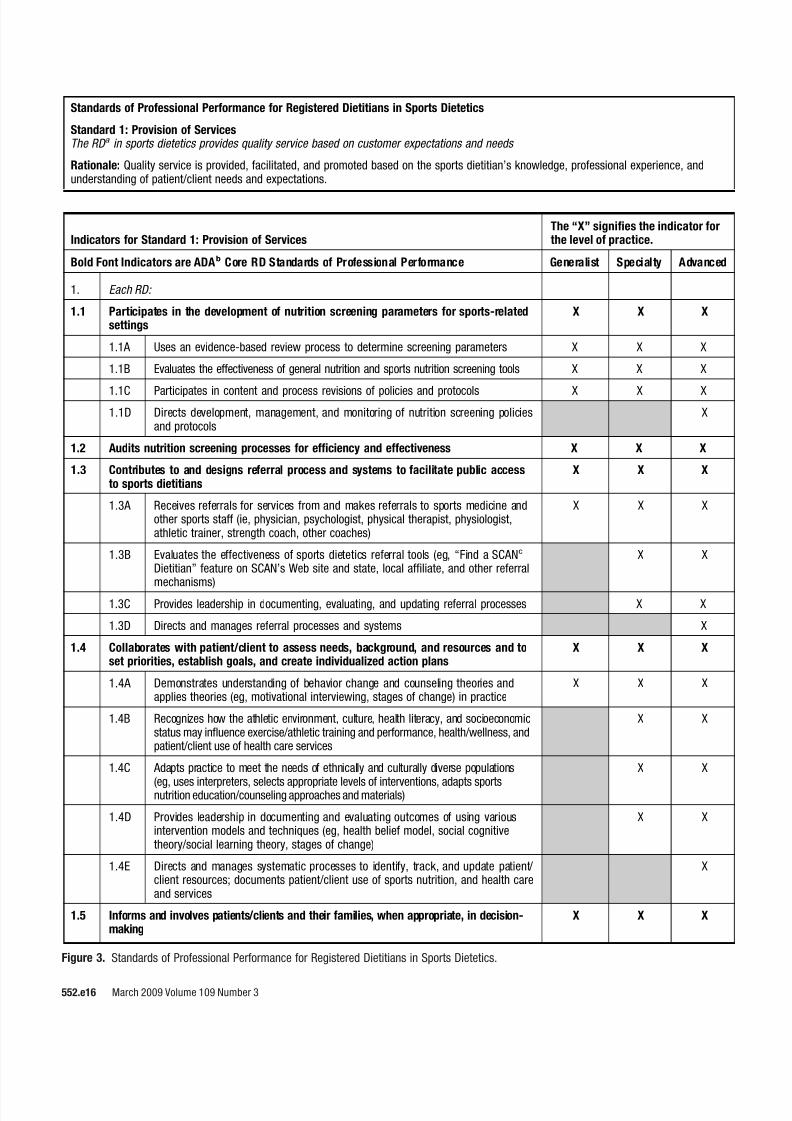
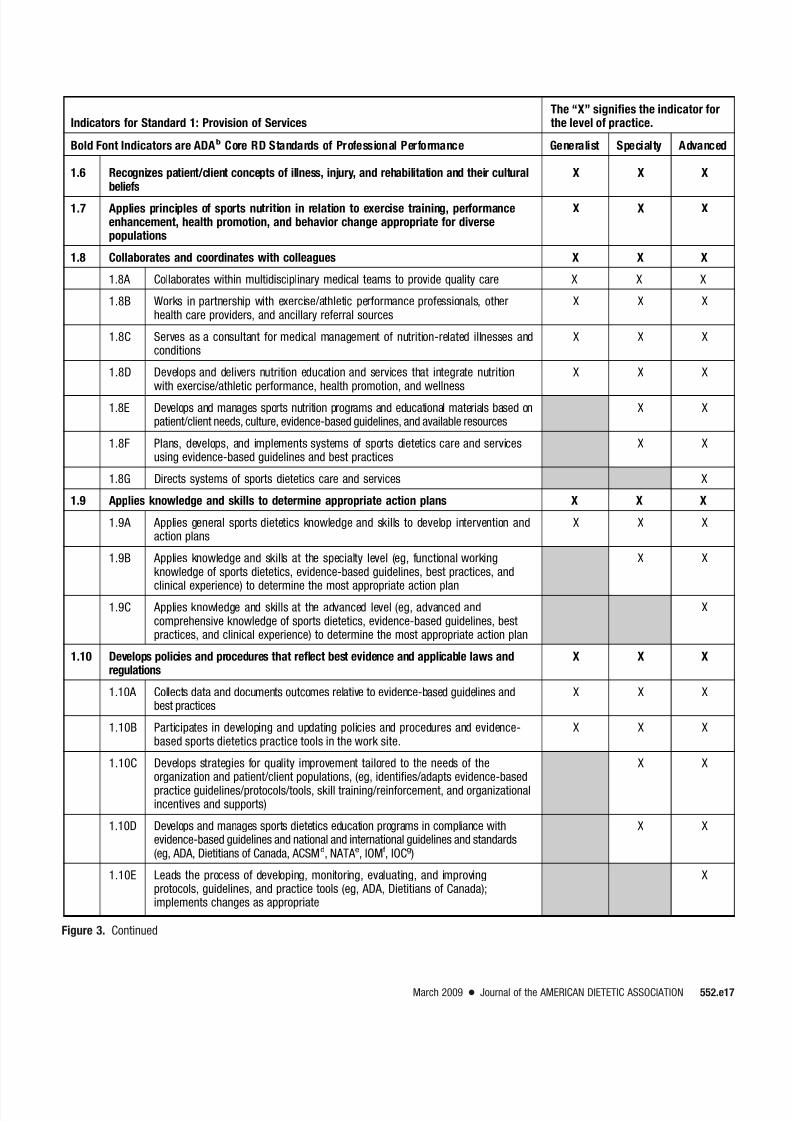
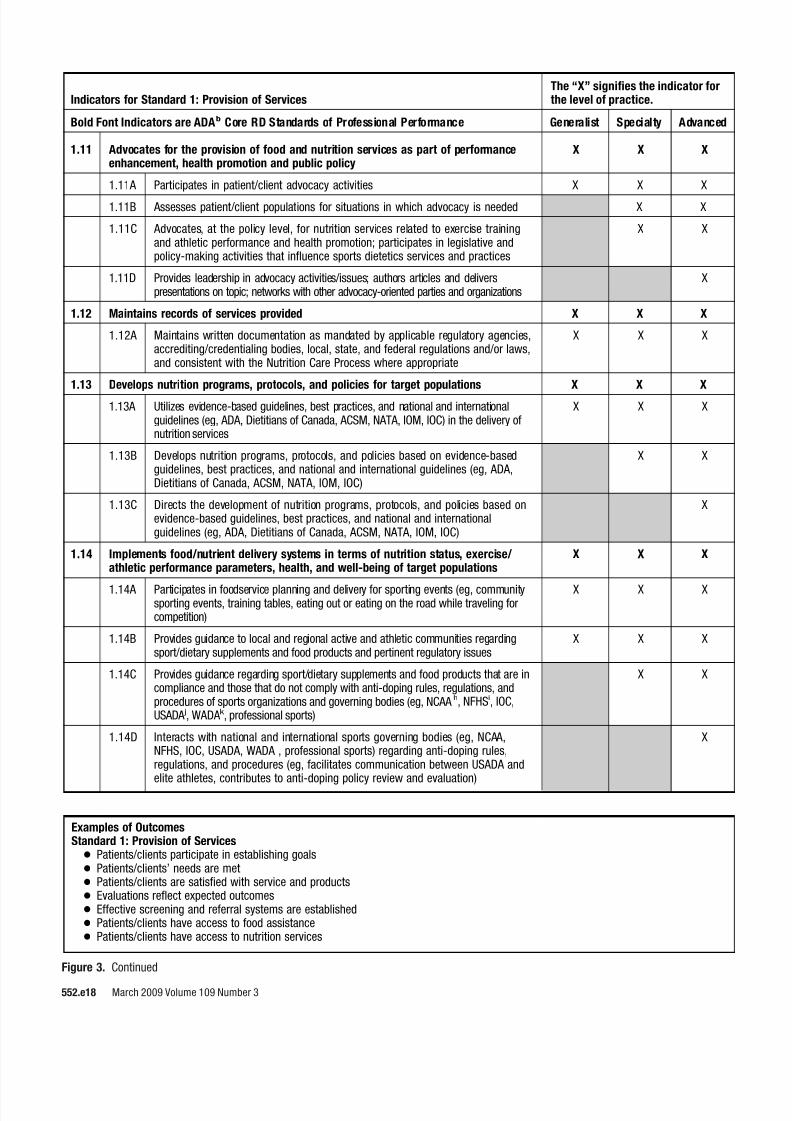
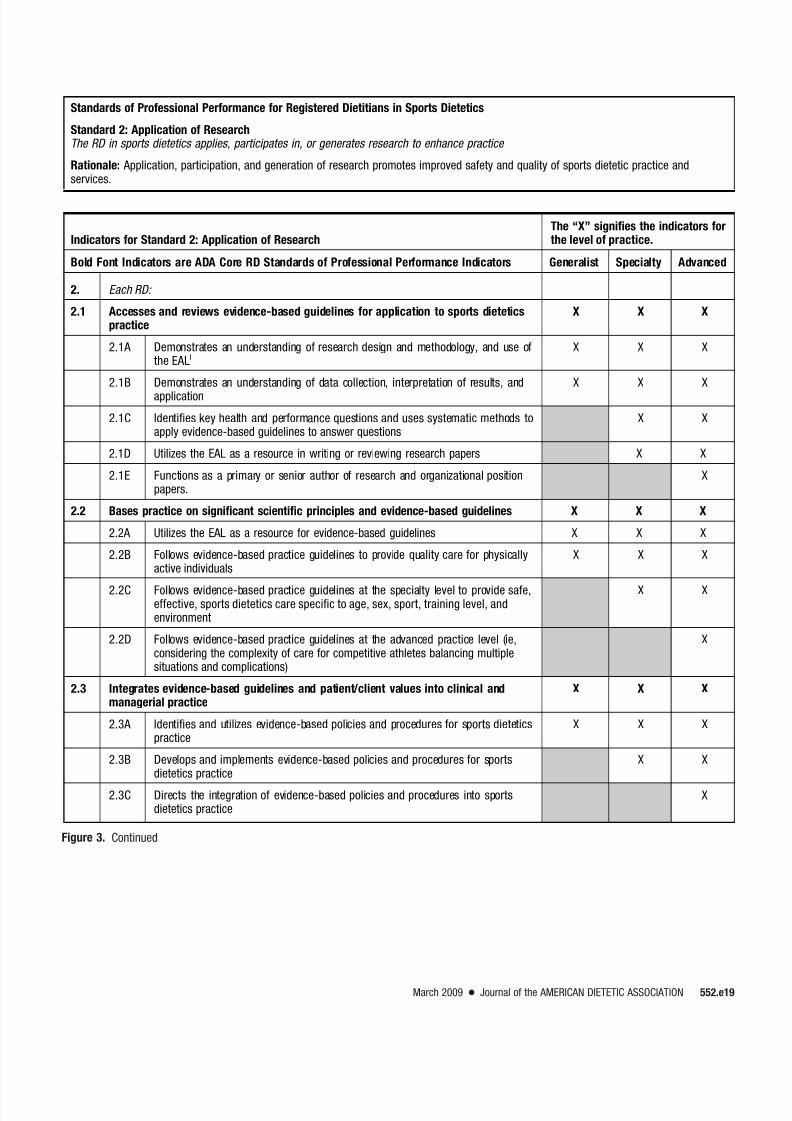
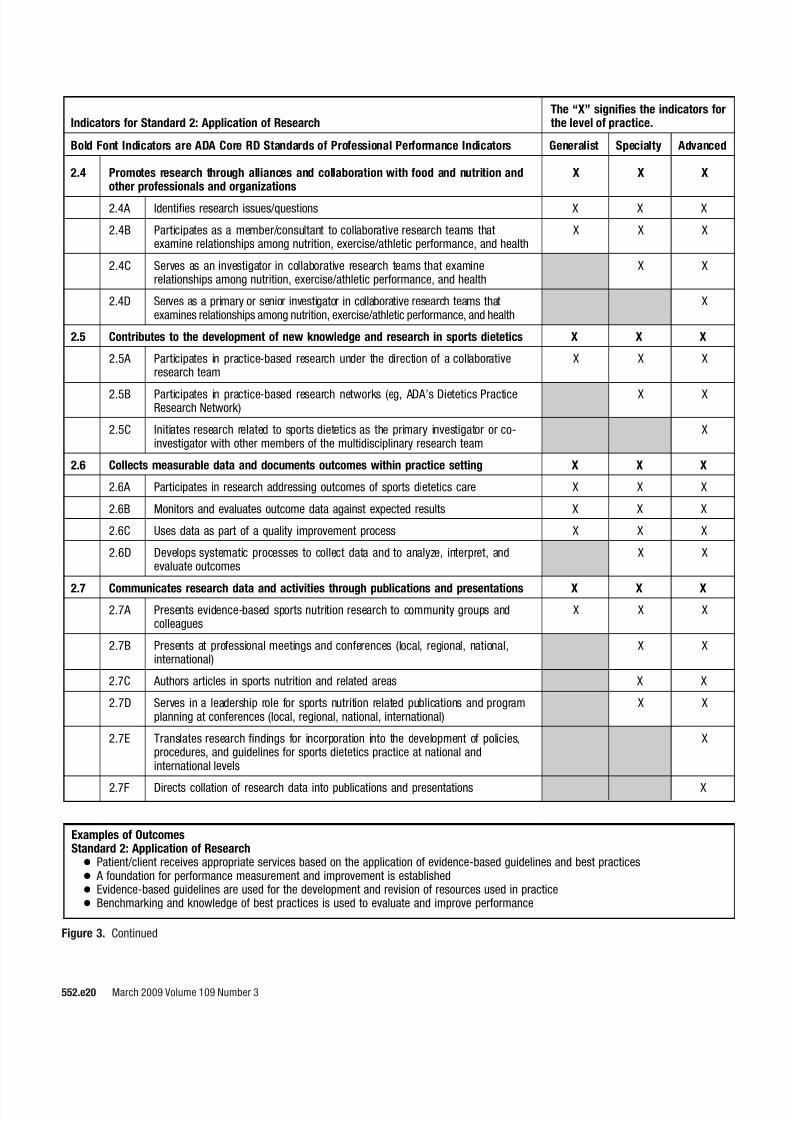
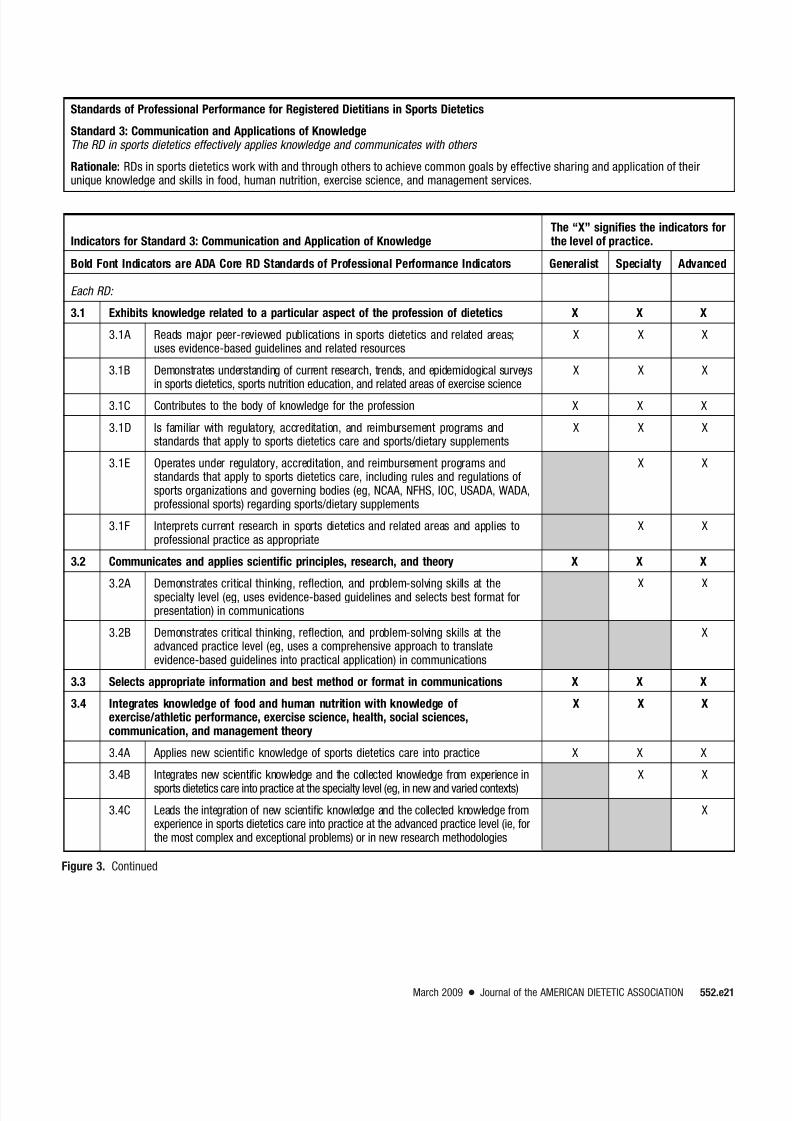
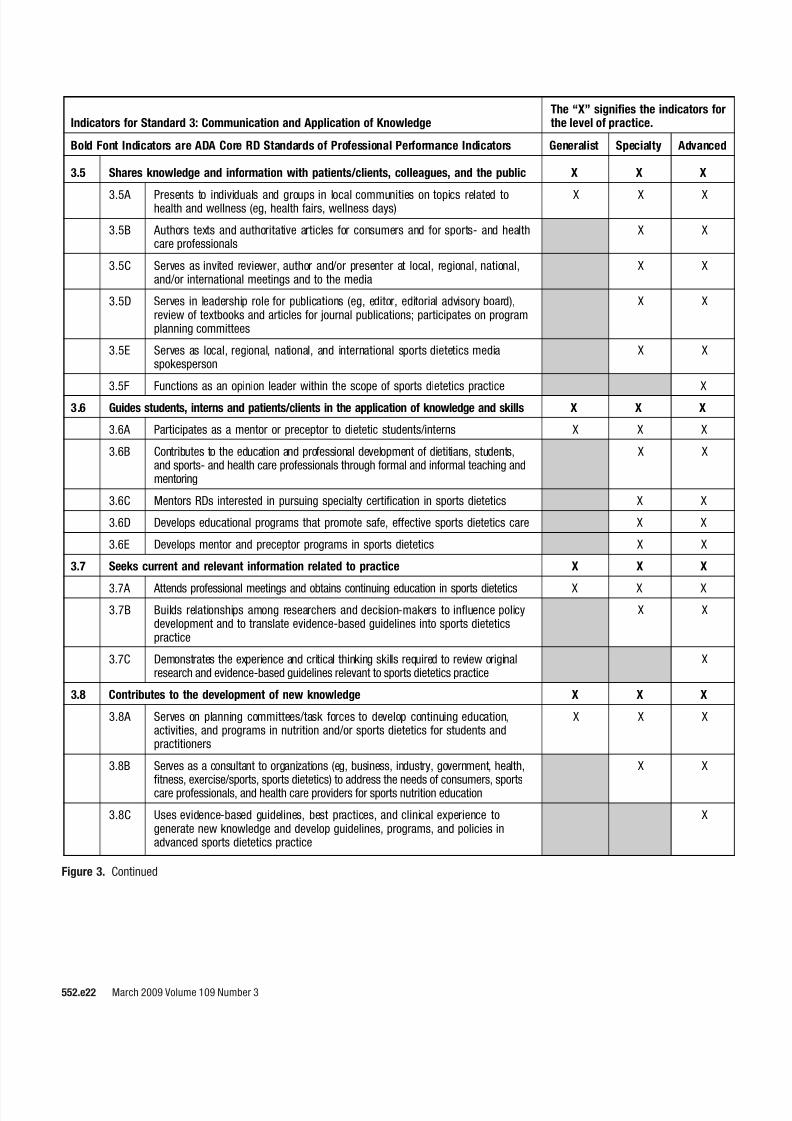
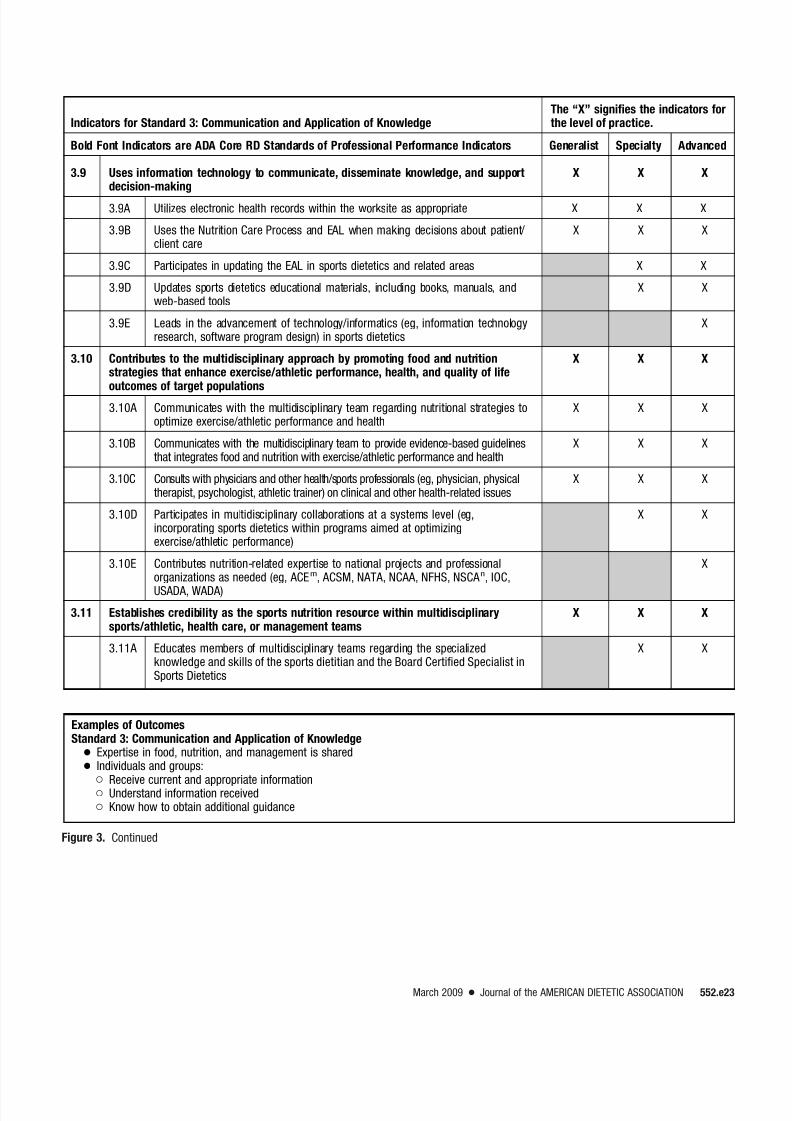
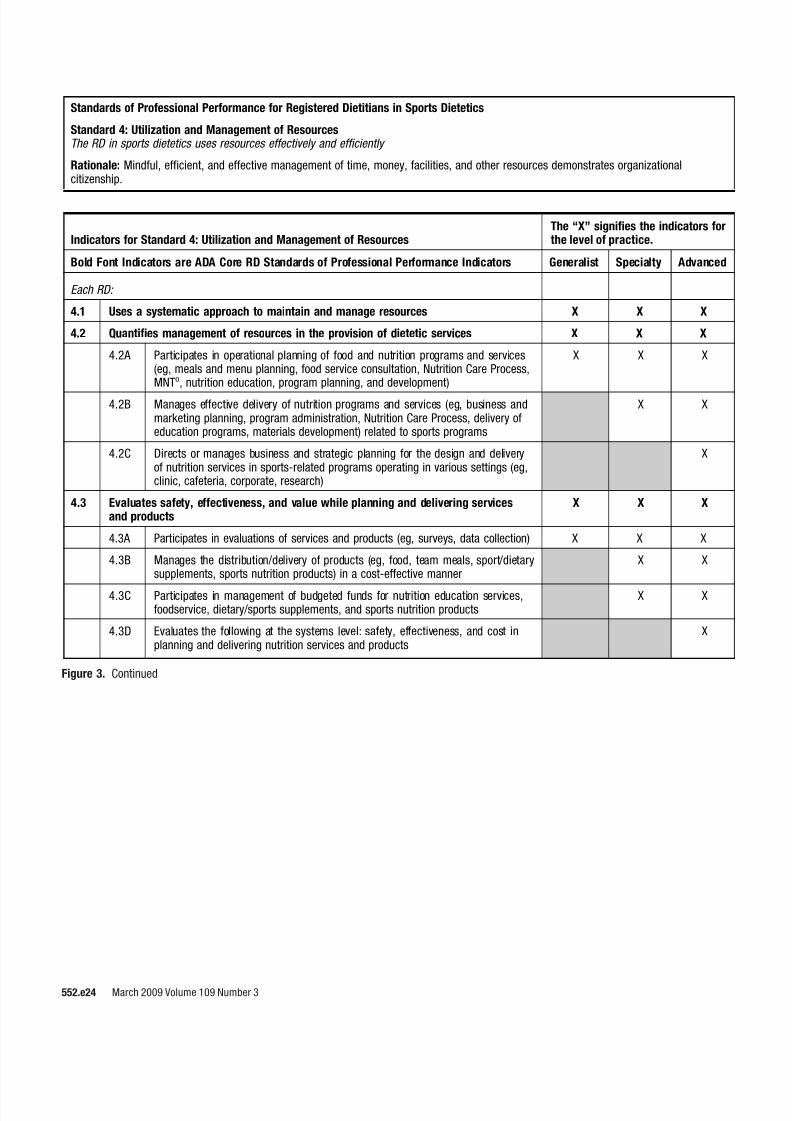
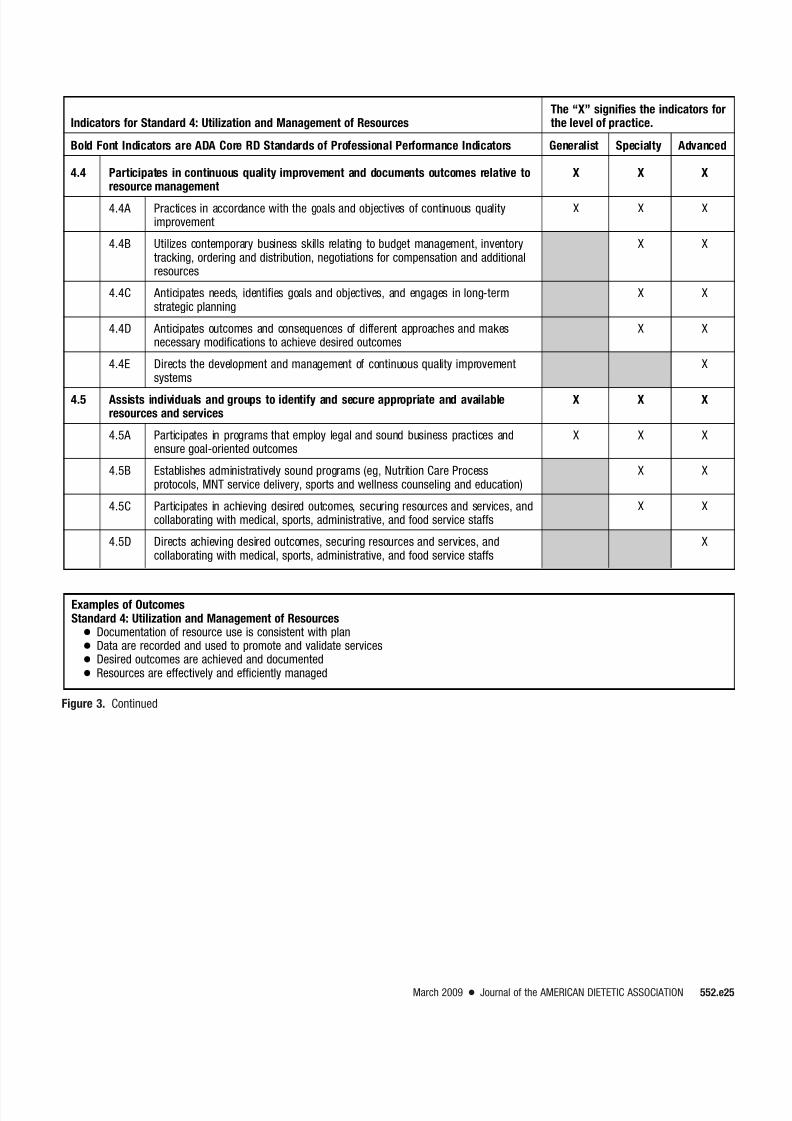
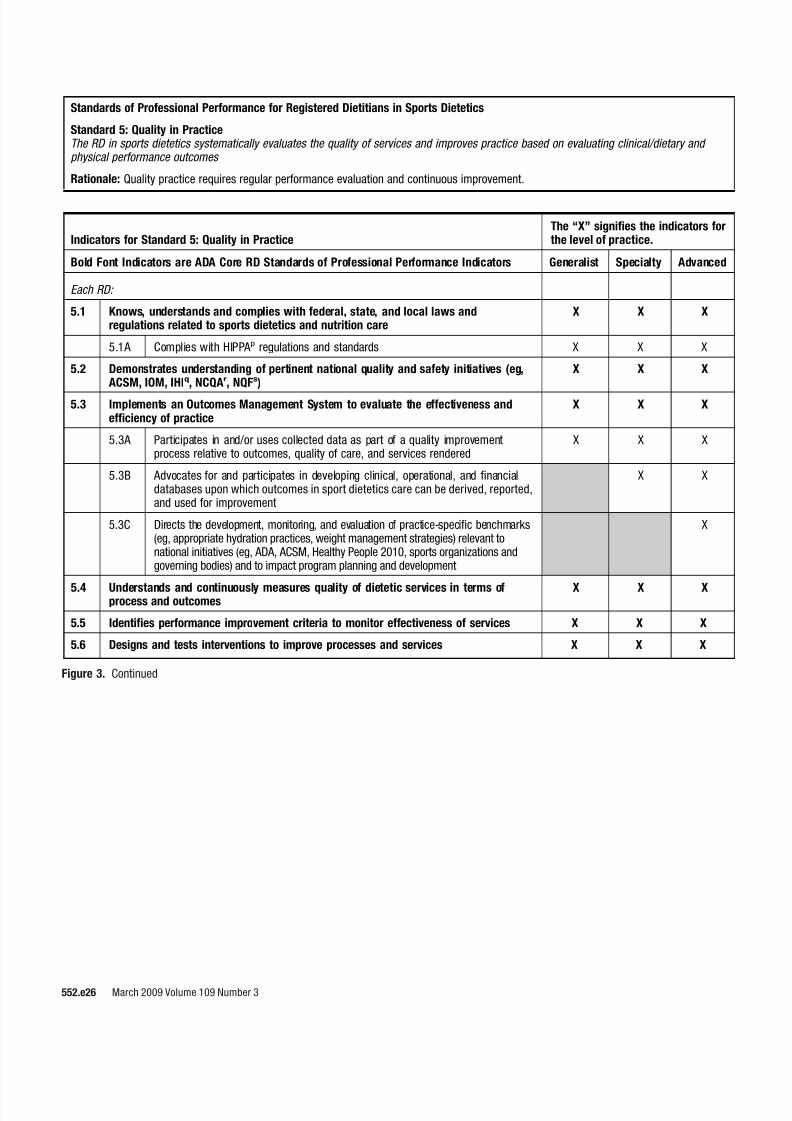
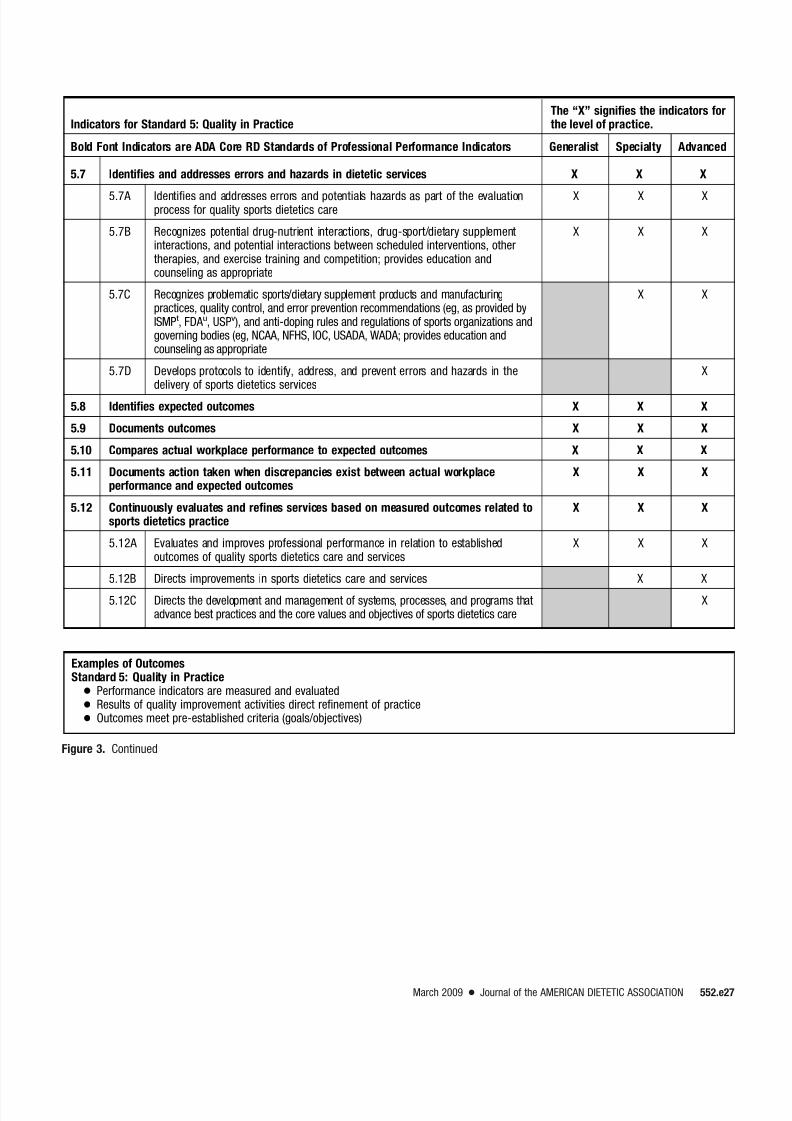
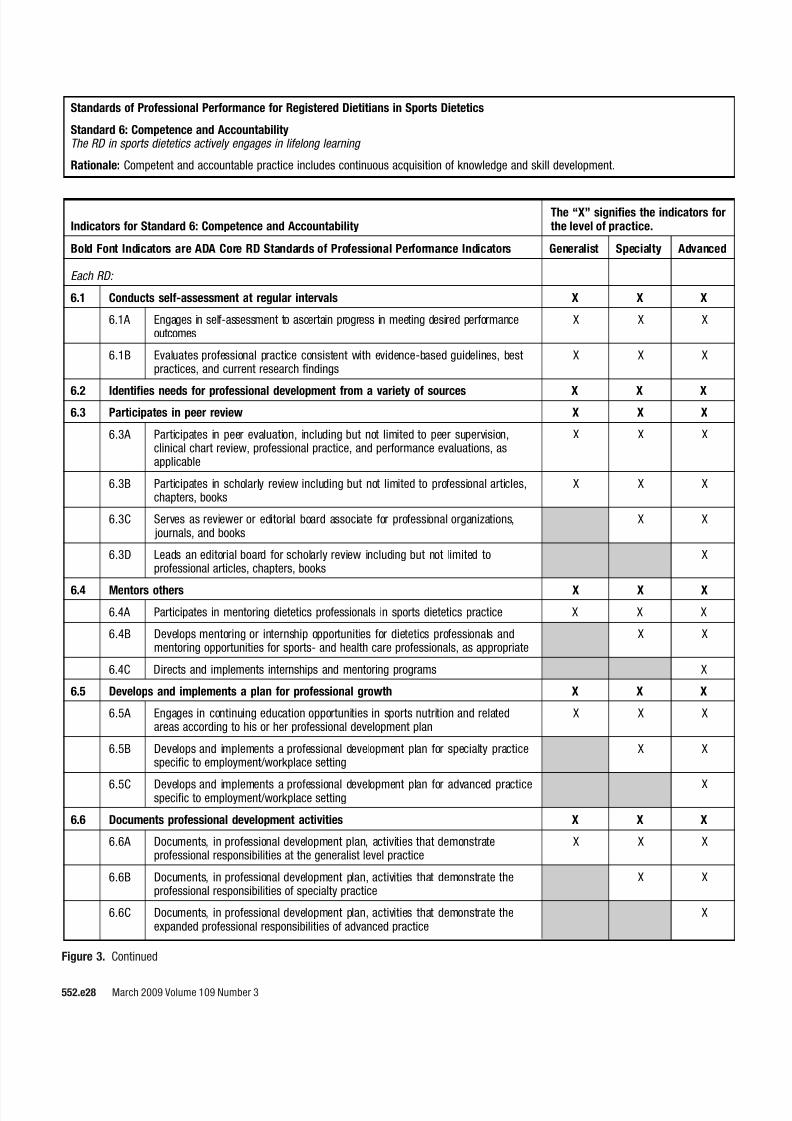
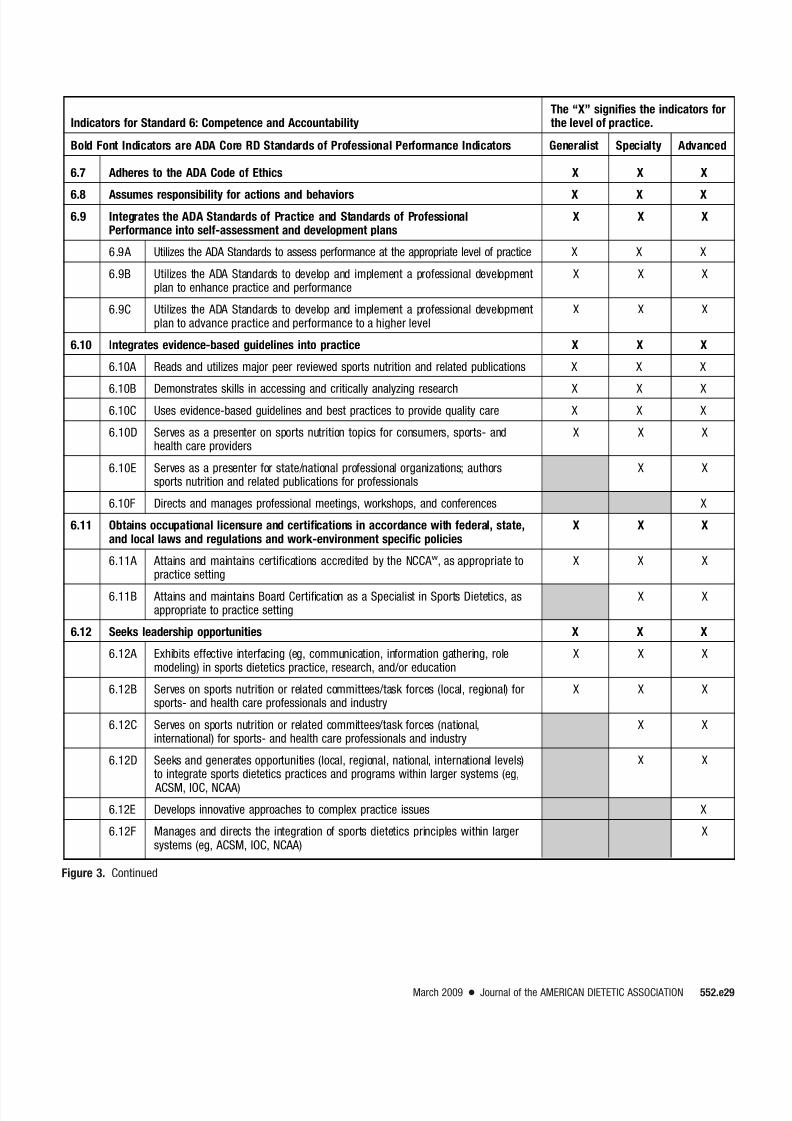
Indicators for the SOP (Figure 2,available online at www.adajournal.org) and SOPP (Figure 3, available
online at www.adajournal.org) are ac-tion statements that illustrate howeach standard may be applied in prac-tice. Within the SOP and SOPP inSports Dietetics, an “X” in the gener-alist column indicates that an RD
Specialty RDa Advanced Practice RD
A specialty level RD has acquired the proficient specializedknowledge base, complex decision-making skills, and clinicalcompetencies for specialty level practice which are shaped bythe context in which an RD practices.
Specialty RDs practice from both expanded and specialized knowledge, skills, competencies, and experience.
Specialization is concentrating or delimiting one’s focus to part ofthe whole field of dietetics (eg, ambulatory care, long-term care,diabetes, renal, pediatric, private practice, community, nutritionsupport, research, sports dietetics).
Expansion refers to the acquisition of new practice knowledge andskills, including the knowledge and skills that legitimize roleautonomy within areas of practice that may overlap traditionalboundaries of dietetics practice.
Specialty level RDs are either certified or approved to practice intheir expanded, specialized areas.
Specialization does not always include an additional certificationbeyond RD certification.
Specialty certification may or may not require evidence at
postgraduate level.The Commission on Dietetic Registration (CDRb) offers five
specialty certifications:● Board Certified Specialist in Pediatric Nutrition (CSP)● Board Certified Specialist in Renal Nutrition (CSR)● Board Certified Specialist in Sports Dietetics (CSSD)● Board Certified Specialist in Gerontological Nutrition (CSG)● Board Certified Specialist in Oncology Nutrition (CSO)
Examples of other specialty certifications currently available to the RD● Certified Diabetes Educator (CDE)● Certified Nutrition Support Clinician (CNSC)
Educational Preparation (one or more of the following characteristics)● Educational preparation at the specialty level● May include a formal educational program preparing for
specialty practice● Dietetics practice roles accredited or approved● May include a formal system of certification and credentialing
Nature of Practice● Integrates research, education, practice and management● Moderate degree of professional autonomy and independent
practice● Specialized assessment skills, decision-making skills, and
diagnostic reasoning skills● Nonclinical specialty practice (business and communications
for example) may not include all characteristics; however, thecomplexity of the nature of practice will be comparable
Experience
Experience beyond entry level is recommended or required.Experience is required for specialty certification.
An advanced practice level RD has acquired the expert knowledge,complex decision-making skills, and clinical competencies forexpanded practice, the characteristics of which are shaped by thecontext in which an RD practices.
Advanced practice RDs practice from both expanded and specialized knowledge, skills, competencies, and experience.
Expansion refers to the acquisition of new practice knowledge andskills, including the knowledge and skills that legitimize roleautonomy within areas of practice that may overlap traditionalboundaries of dietetics practice.
Advanced level practice is characterized by the integration of a broadrange of unique theoretical, research-based, and practicalknowledge that occurs as a part of training and experiencebeyond entry level. Advanced practice RDs are either certified orapproved to practice in their expanded, specialized roles.
Advanced practice does not always include an additional certificationbeyond RD certification. Certification may be one way ofdemonstrating advanced practice competency.
Advanced Practice Certification typically implies a postgraduate
degree level. Advanced Practice implies that the individual has the specialization
knowledge, skills, competencies, and experience, and theexpanded knowledge, skills, competencies, and experience of
Advanced Practice.Specialty Certification is not a prerequisite for Advanced Practice
CertificationCDR does not currently offer any Advanced level certifications.Example of other advanced level certifications for RD:● Board Certified in Advanced Diabetes Management (BC-ADM)
Educational Preparation (one or more of the following characteristics):● Educational preparation at the advanced level● May include a formal educational program preparing for
advanced practice●
Dietetics practice roles accredited or approved● May include a formal system of certification and credentialing
Nature of Practice● Integrates research, education, practice, and management● High degree of professional autonomy and independent practice● Case management/own case load● Advanced health assessment skills, decision-making skills, and
diagnostic reasoning skills● Nonclinical advanced practice (eg, business, communications)
may not include all characteristics; however, the complexity ofthe nature of practice will be comparable
● Recognized advanced clinical competencies● Provision of consultant services to health providers● Plans, implements, and evaluates programs
ExperienceExperience beyond entry level is required.
Figure 4. American Dietetic Association (ADA) definition of terms from the ADA Scope of Dietetic Practice Framework. aRDregistered dietitian.bCDRCommission on Dietetic Registration.
who is caring for patients or clients isexpected to complete this activityand/or seek assistance to learn how toperform at the level of the standard.The generalist in sports dieteticscould be an entry level RD or an ex-perienced RD who has newly as-sumed responsibility to providesports dietetics care of active or ath-letic patients or clients. The general-
ist could also be an experienced indi- vidual who has changed the focus of his or her sports dietetics practice toanother group (eg, children to adult)or to another specialty (eg, endurancesports to strength/power sports) (seeFigure 4). An “X” in the specialty col-umn indicates that an RD who per-forms at this level has a deeper un-derstanding of sports dietetics andhas the ability to modify therapy tomeet the needs of patients/clients in
various situations (eg, caring for ayoung athlete who is participating in
preseason conditioning and is suffer-ing from dehydration; helping an ath-lete with hypoglycemia to choose theright foods and fluids at the righttime before, during, and after exer-cise). An “X” in the advanced columnindicates that the RD who performsat this level possesses a comprehen-sive understanding of sports dieteticsand exercise physiology and a highlydeveloped range of skills and judg-ments acquired through a combina-tion of experience and education.
Bolded standards and indicatorsoriginate from ADA’s 2008 SOP inNutrition Care and SOPP for RDs (1)and should apply to RDs in all threecategories. Several unbolded indica-tors are identified as applicable to alllevels of practice. Where “X”s areplaced in all three categories of prac-tice, it is understood that all RDs insports dietetics are accountable for
practice within each of these indica-tors. However, the depth with whichan RD performs each activity will in-crease as the individual moves be-yond the generalist level. Level of practice considerations warrant thata holistic view of the SOP and SOPPfor RDs in Sports Dietetics be taken.It is the totality of individual practicethat defines the level of practice andnot any one indicator or standard.
RDs should review the SOP andSOPP in Sports Dietetics at regular in-tervals to evaluate their sports nutri-
tion knowledge, skill, and competence.Regular self-evaluation is importantbecause it helps identify opportunitiesto improve and/or enhance practiceand professional performance. This ap-praisal also enables sports dietitians tobetter utilize CDR’s Professional Devel-opment Portfolio for self-assessment,planning, improvement, and commit-ment to lifelong learning (31). Thesestandards may be used in each of thefive steps in the Professional Develop-mental Portfolio process (Figure 5).
RDs are encouraged to pursue addi-tional training, regardless of practicesetting, to expand their personal scopeof sports dietetics. Individuals are ex-pected to practice only at the level atwhich they are competent, and this will
vary depending on education, trainingand experience (32). Sports dietitiansare encouraged to pursue additionalknowledge and skill training regard-
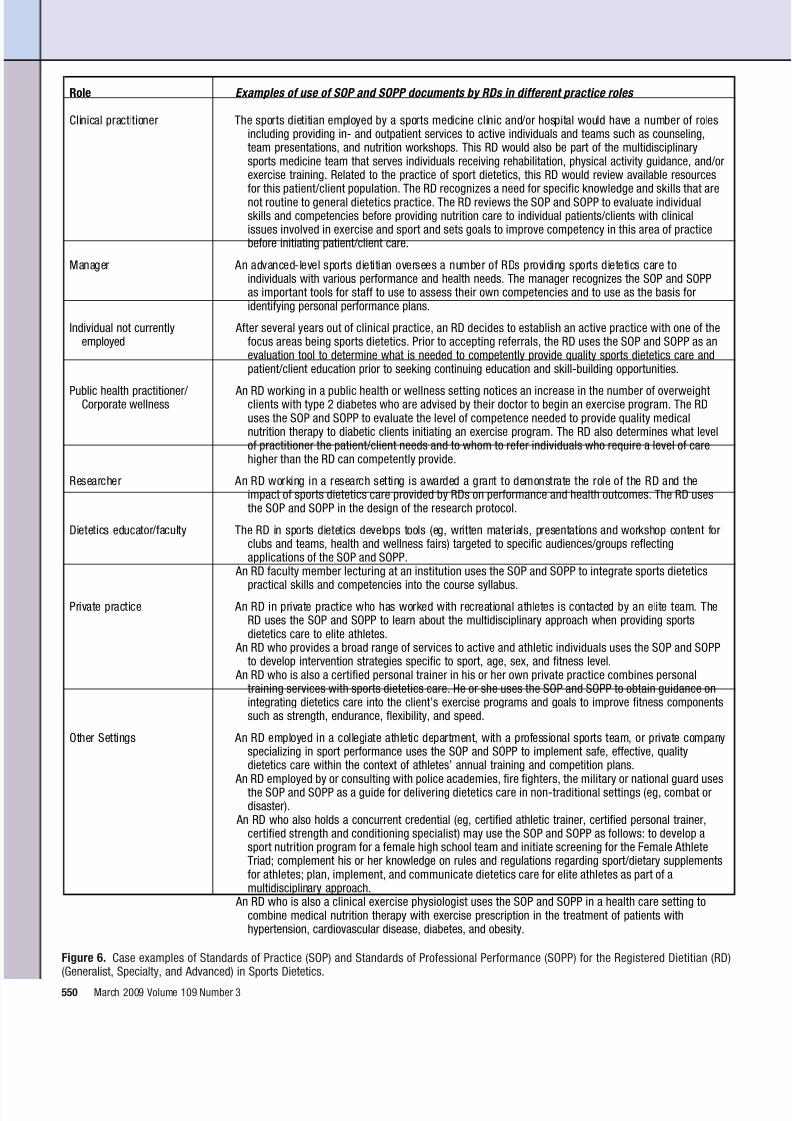
less of practice setting and to pursueCSSD certification to promote consis-tency in practice and performance andcontinuous quality improvement. SeeFigure 6 for case examples of how RDsin different roles, at different levels of practice, may use the SOP and SOPPin Sports Dietetics.
In some instances, components of the SOP and SOPP in Sports Dietet-ics do not specifically differentiate be-tween specialty and advanced levelpractice. In these areas, it was theconsensus of the content experts that
the distinctions are subtle—capturedin the knowledge, experience, and in-tuition demonstrated in the context of practice at the advanced level, whichcombines dimensions of understand-ing, performance, and value as an in-tegrated whole (33). A wealth of un-tapped knowledge is embedded in theexperience, discernment, and practiceof advanced-level sports dietetics prac-titioners. The knowledge and skills ac-quired through practice will continu-ally expand and mature. They will be
How to Use the Standards of Practice and Standards of Professional Performance for Registered Dietitians (Generalist, Specialty,and Advanced) in Sports Dietetics as part of the Professional Development Portfolio Processa
niatniamroecitcarpruoydnapxeoteraslaogruoyrehtehwdnaecitcarpfoleveltnerrucruoyssess A tcefleR.1your current level of practice. Review the Standards of Practice and Standards of ProfessionalPerformance document to determine what you want your future practice to be, and assess yourstrengths and areas for improvement. These documents can help you set short- and long-termprofessional goals.
2. Conduct learning needsassessment
Once you have identified your future practice goals, you can review the Standards of Practice andStandards of Professional performance document to assess your current knowledge, skills,behaviors, and define what continuing professional education is required to achieve the desiredlevel of practice.
3. Develop learning plan Based on your review of the Standards of Practice and Standards of Professional Performance, youcan develop a plan to address your learning needs as they relate to your desired level of practice.
4. Implement learning plan As you implement your learning plan, keep reviewing the Standards of Practice and Standards ofProfessional Performance document to re-assess knowledge, skills, and behaviors and yourdesired level of practice.
5. Evaluate learning planprocess
Once you achieve your goals and reach or maintain your desired level of practice, it is important tocontinue to review the Standards of Practice and Standards of Professional Performance documentto re-assess knowledge, skills, and behaviors and your desired level of practice.
Figure 5. Application of the Commission on Dietetic Registration Professional Development Portfolio process. aThe Commission on DieteticRegistration Professional Development Portfolio process is divided into five interdependent steps that build sequentially upon the previous stepduring each 5-year recertification cycle and succeeding cycles.
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 549
Role Examples of use of SOP and SOPP documents by RDs in different practice roles
Clinical practitioner The sports dietitian employed by a sports medicine clinic and/or hospital would have a number of rolesincluding providing in- and outpatient services to active individuals and teams such as counseling,team presentations, and nutrition workshops. This RD would also be part of the multidisciplinarysports medicine team that serves individuals receiving rehabilitation, physical activity guidance, and/orexercise training. Related to the practice of sport dietetics, this RD would review available resourcesfor this patient/client population. The RD recognizes a need for specific knowledge and skills that arenot routine to general dietetics practice. The RD reviews the SOP and SOPP to evaluate individualskills and competencies before providing nutrition care to individual patients/clients with clinicalissues involved in exercise and sport and sets goals to improve competency in this area of practicebefore initiating patient/client care.
Manager An advanced-level sports dietitian oversees a number of RDs providing sports dietetics care toindividuals with various performance and health needs. The manager recognizes the SOP and SOPPas important tools for staff to use to assess their own competencies and to use as the basis foridentifying personal performance plans.
Individual not currentlyemployed
After several years out of clinical practice, an RD decides to establish an active practice with one of thefocus areas being sports dietetics. Prior to accepting referrals, the RD uses the SOP and SOPP as anevaluation tool to determine what is needed to competently provide quality sports dietetics care andpatient/client education prior to seeking continuing education and skill-building opportunities.
Public health practitioner/ Corporate wellness
An RD working in a public health or wellness setting notices an increase in the number of overweightclients with type 2 diabetes who are advised by their doctor to begin an exercise program. The RDuses the SOP and SOPP to evaluate the level of competence needed to provide quality medicalnutrition therapy to diabetic clients initiating an exercise program. The RD also determines what levelof practitioner the patient/client needs and to whom to refer individuals who require a level of carehigher than the RD can competently provide.
Researcher An RD working in a research setting is awarded a grant to demonstrate the role of the RD and theimpact of sports dietetics care provided by RDs on performance and health outcomes. The RD usesthe SOP and SOPP in the design of the research protocol.
Dietetics educator/faculty The RD in sports dietetics develops tools (eg, written materials, presentations and workshop content forclubs and teams, health and wellness fairs) targeted to specific audiences/groups reflectingapplications of the SOP and SOPP.
An RD faculty member lecturing at an institution uses the SOP and SOPP to integrate sports dietetics
practical skills and competencies into the course syllabus.Private practice An RD in private practice who has worked with recreational athletes is contacted by an elite team. The
RD uses the SOP and SOPP to learn about the multidisciplinary approach when providing sportsdietetics care to elite athletes.
An RD who provides a broad range of services to active and athletic individuals uses the SOP and SOPPto develop intervention strategies specific to sport, age, sex, and fitness level.
An RD who is also a certified personal trainer in his or her own private practice combines personaltraining services with sports dietetics care. He or she uses the SOP and SOPP to obtain guidance onintegrating dietetics care into the client’s exercise programs and goals to improve fitness componentssuch as strength, endurance, flexibility, and speed.
Other Settings An RD employed in a collegiate athletic department, with a professional sports team, or private companyspecializing in sport performance uses the SOP and SOPP to implement safe, effective, qualitydietetics care within the context of athletes’ annual training and competition plans.
An RD employed by or consulting with police academies, fire fighters, the military or national guard usesthe SOP and SOPP as a guide for delivering dietetics care in non-traditional settings (eg, combat ordisaster).
An RD who also holds a concurrent credential (eg, certified athletic trainer, certified personal trainer,certified strength and conditioning specialist) may use the SOP and SOPP as follows: to develop asport nutrition program for a female high school team and initiate screening for the Female AthleteTriad; complement his or her knowledge on rules and regulations regarding sport/dietary supplementsfor athletes; plan, implement, and communicate dietetics care for elite athletes as part of amultidisciplinary approach.
An RD who is also a clinical exercise physiologist uses the SOP and SOPP in a health care setting tocombine medical nutrition therapy with exercise prescription in the treatment of patients withhypertension, cardiovascular disease, diabetes, and obesity.
Figure 6. Case examples of Standards of Practice (SOP) and Standards of Professional Performance (SOPP) for the Registered Dietitian (RD)(Generalist, Specialty, and Advanced) in Sports Dietetics.
captured in refined indicators as ad- vanced-level RDs systematically recordtheir own experience using the conceptof clinical exemplars. The experiencedpractitioner observes clinical events,analyzes them to make new connec-tions between events and ideas, and
produces a synthesized whole. Clinicalexemplars provide outstanding modelsof the actions of individual sports dieti-tians in clinical settings and the profes-sional activities that have enhancedpatient or client care. They include abrief description of the need for actionand the process used to change the out-come (34-36).
FUTURE DIRECTIONS
The SOP and SOPP for RDs in SportsDietetics are innovative and dynamic
documents. Future revisions will re-flect changes in practice, dietetics ed-ucation programs, and outcomes of practice audits. The authors acknowl-edge that the three practice levels re-quire more clarity and differentiationin content and role delineation andthat competency statements that bet-ter characterize differences amongthe practice levels are needed. Cre-ation of this clarity, differentiation,and definition are the challenges of today’s sports dietitians to betterserve tomorrow’s practitioners andtheir patients, clients, and customers.
SUMMARY
The SOP and SOPP for RDs in SportsDietetics are key resources for RDs atall knowledge and performance levels.These standards can and should beused by RDs in daily practice to consis-tently improve and appropriately dem-onstrate competency and value asproviders of safe and effective sportsdietetics care. These standards alsoserve as a professional resource for self-evaluation and professional develop-
ment for RDs specializing in sports di-etetics practice. The development andevaluation process is dynamic. Just asthe professional’s self-evaluation andcontinuing education process is an on-going cycle, these standards are also awork-in-progress and will be reviewedand updated on a regular basis. Cur-rent and future initiatives of ADA willprovide information to use in these up-dates and in further clarifying anddocumenting the specific roles and re-sponsibilities of RDs at each level of
practice. As a quality initiative of ADAand the SCAN DPG, these standardsare an application of continuous qual-ity improvement and represent an im-portant collaborative endeavor.
1. American Dietetic Association Revised 2008standards of practice for registered dieti-tians in nutrition care; standards of profes-sional performance for registered dietitians;standards of practice for dietetic techni-cians, registered, in nutrition care; and stan-dards of professional performance for die-tetic technicians, registered. J Am Diet Assoc. 2008;108:1538-1542e9.
2. O’Sullivan-Maillet J, Skates J, Pritchett E.Scope of dietetics practice framework. J Am Diet Assoc. 2005;105:634-640.
3. Code of ethics for the profession of dietetics.
J Am Diet Assoc. 1999:99:109-113.4. Visocan B, Swift J. Understanding and us-
ing the scope of dietetics practice frame-work: A step-wise approach. J Am Diet As-soc. 2006;106:459-463.
5. Kieselhorst K, Skates J, Pritchett E. Amer-ican Dietetic Association: Standards of prac-tice in nutrition care and updated standardsof professional performance. J Am Diet As-soc. 2005;105:641-645.
6. Lacey K, Pritchett E. Nutrition care processand model: ADA adapts road map to qualitycare and outcomes management. J Am Diet Assoc. 2003;103:1061-1072.
7. Prevalence of overweight and obesity amongadults: United States, 2003-2004. Centers for
Disease Control and Prevention, NationalCenter for Health Statistics Web site. April2006. http://www.cdc.gov/nchs/products/pubs/ pubd/hestats/overweight/overwght_adult_03.htm. Accessed September 2008.
8. Galusky DA, Gillespie C, Kuester SA, Mokdad AH, Cogswell ME, Philip CM. State-specificprevalence of obesity among adults—UnitedStates, 2007. MMWR Weekly. 2008;57:765-
768.9. Jakicic JM, Clark K, Coleman E, Donnelly
JE, Foreyt J, Melanson E, Volek J, Volpe SL. American College of Sports Medicine Posi-tion Stand. Appropriate intervention strate-gies for weight loss and prevention of weightregain for adults. Med Sci Sports Exerc.2001;33:2145-2156.
10. Amati F, Dube JJ, Shay C, Goodpaster BH.Separate and combined effects of exercisetraining and weight loss on exercise effi-ciency and substrate oxidation. J Appl Physiol. 2008;105:825-831.
11. Donnelly JE, Blair SN, Jakicic JM, ManoreMM, Rankin JW, Smith BK. Update of the2001 American College of Sports Medicine(ACSM) Position Stand. Appropriate inter-
vention strategies for weight loss and pre- vention of weight regain for adults. Med Sci Sports Exerc. 2009;41:459-478.
12. Dietary Guidelines for Americans, 2005. Ex-ecutive summary. Washington, DC: US De-partment of Health and Human Services,US Department of Agriculture Web site.2005. http://www.health.gov/dietaryguidelines/ dga2005/document/html/executivesummary.htm. Accessed September 2008.
13. Healthy People 2010: The cornerstone forprevention. Office of Disease Preventionand Health Promotion, US Department of Health and Human Services Web site. 2005.http://www.healthypeople.gov/Publications.
Accessed September 2008.14. Physical Activity Guidelines Advisory Com-
mittee, Physical Activity Guidelines Advi-
sory Committee Report, 2008. Washington,DC: US Department of Health and HumanServices, 2008.
15. Institute of Medicine (IOM), Food and Nu-trition Board, National Academy of Science. Dietary Reference Intakes for Energy, Carbo-hydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients).Washington, DC: National Academies Press;2005.
16. National Diabetes Fact Sheet, 2007. US De-partment of Health and Human Services,Centers for Disease Control and PreventionWeb site. 2007. http://www.cdc.gov/diabetes/ pubs/factsheet07.htm. Accessed September2008.
17. Burke L. Practical Sports Nutrition. Cham-paign, IL: Human Kinetics, 2007.
18. Burke L, Deakin V. Clinical Sports Nutri-tion, 3rd ed. North Ryde, NSW, Australia:McGraw-Hill Australia; 2006.
19. Manore MM, Meyer N, Thompson J. Sport Nutrition for Health and Performance, 2nded. Champaign, IL: Human Kinetics; June2009.
20. Rodriguez NR, DiMarco NM, Langley S. Po-sition of the American Dietetic Association,Dietitians of Canada, and the American Col-lege of Sports Medicine: Nutrition and ath-letic performance. J Am Diet Assoc. 2009;109:509-527.
21. Nattiv A, Loucks AB, Manore MM, SanbornCF, Sundgot-Borgen J, Warren M. AmericanCollege of Sports Medicine position stand.
These standards have been formu-lated to be used for individual self-evaluation and the development of practice guidelines, but not for in-stitutional credentialing or for ad-
verse or exclusionary decisions re-garding privileging, employment
opportunities or benefits, disciplin-ary actions, or determinations of negligence or misconduct. Thesestandards do not constitute medi-cal or other professional advice,and should not be taken as such.The information presented in thesestandards is not a substitute forthe exercise of professional judg-ment by the health care profes-sional. The use of the standards forany other purpose than that forwhich they were formulated mustbe undertaken within the sole au-thority and discretion of the user.
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 551
The female athlete triad. Med Sci Sports Exerc. Oct 2007;39:1867-1882.
22. Sawka MN, Burke LM, Eichner ER,Maughan RJ, Montain, SJ. American Col-lege of Sports Medicine (ACSM) positionstand: Exercise and fluid replacement. Med Sci Sports Exerc. 2007;39:377-390.
23. Bonci CM, Bonci LJ, Granger LR, JohnsonCL, Malina, RM, Milne LW, Ryan RR,
Vanderbunt EM. National Athletic Trainers’ Association position statement: Preventing,detecting, and managing disordered eatingin athletes. J Athletic Training. 2008;43:80-108.
24. Casa DJ, Armstrong LE, Hillman SK, Mon-tain SJ, Reiff RV, Rich BSE, Roberts WO,Stone JA. National Athletic Trainers’ Asso-ciation position statement: Fluid replace-ment for athletes. J Athletic Training. 2000;35:212-224.
25. Committee on Metabolic Monitoring for Mil-itary Field Applications (Vanderveen JE,Bistrian BR, Caldwell JA, Dwyer JT, Erd-man JW, Lane HW, Manore MM, MorganWP, O’Neil PM, Sternberg EM, Tepper BJ,Thayer J, authors). Monitoring Metabolic Status: Predicting Decrements in Physiolog-ical and Cognitive Performance. StandingCommittee on Military Nutrition Research,Institute of Medicine. Washington, DC: Na-tional Academies Press; 2004.
26. Committee on Optimization of NutrientComposition of Military Rations for Short-Term, High-Stress Situations (Erdman JW,Bistrian BR, Clarkson PM, Dwyer JT, KleinBP, Lane HW, Manore MM, O’Neil PM, Rus-sell RM, Tepper BJ, Tipton KD, Yates AA,authors). Nutrient Composition of Rations for Short-Term, High-Intensity Combat Op- erations. Standing Committee on MilitaryNutrition Research, Food and NutritionBoard, Institute of Medicine. Washington,DC: National Academies Press; 2005.
27. Committee on Mineral Requirements for
Cognitive and Physical Performance by Mil-itary Personnel (Russel RM, Beard JL, BeckM, Bistrian BR, Cannon JG, Combs GF, Dw-yer JT, Erdman JW, Haymes EM, Hunt JR,Lane HW, Penland JG, Percival SS, WeaverCM, authors). Mineral Requirements of Mil-itary Personnel. Levels Needed for Cognitiveand Physical Performance During GarrisonTraining. Standing Committee on MilitaryNutrition Research, Food and NutritionBoard, Institute of Medicine. Washington,DC: National Academies Press; 2006.
28. Committee on Dietary Supplement Use byMilitary Personnel (Greenwood MRC, Ander-son C, Bistrian B, Erdman JW, Franke WC,Jeffery E, Kanarek RB,Keen CL,Mahady GB,Miller SA, Myer EF, Rankin JW, authors).Use of Dietary Supplements by Military Per-
sonnel. Standing Committee on Military Nu-trition Research, Food and Nutrition Board,Institute of Medicine. Washington, DC: Na-tional Academies Press; 2008.
29. Job Descriptions: Models for the Dietetics Profession, 2nd ed. Chicago, IL: AmericanDietetic Association; 2008.
30. Dreyfus HL, Dreyfus SE. Mind over Ma-chine: The Power of Human Intuitive Exper-tise in the Era of the Computer. New York,NY: Free Press; 1986.
31. Weddle DO. The Professional DevelopmentPortfolio Process: Setting goals for creden-tialing. J Am Diet Assoc. 2002;102:1439-1444.
32. Gates G. Ethics opinion: Dietetics profes-
sionals are ethically obligated to maintainpersonal competence in practice. J Am Diet Assoc. 2003;103:633-635.
33. Chambers DW, Gilmore CJ, Maillet JO,Mitchell BE. Another look at competency-based education in dietetics. J Am Diet As-soc. 1996;96:614-617.
34. Clark N, Coleman C, Figure K, Mailhot T,Zeigler J. 2003. Food for trans-Atlantic row-
ers: A menu planning model and case study. Int J Sport Nutr Exerc Metab. 2003;13:227-242.
35. Stout A. Fueling and weight managementstrategies in sport. Practice applications. J Am Diet Assoc. 2007;107:1475-1479.
36. Quatromoni PA. Clinical observations fromnutrition services in college athletics. Per-spectives in practice. J Am Diet Assoc. 2008;108:689-694.
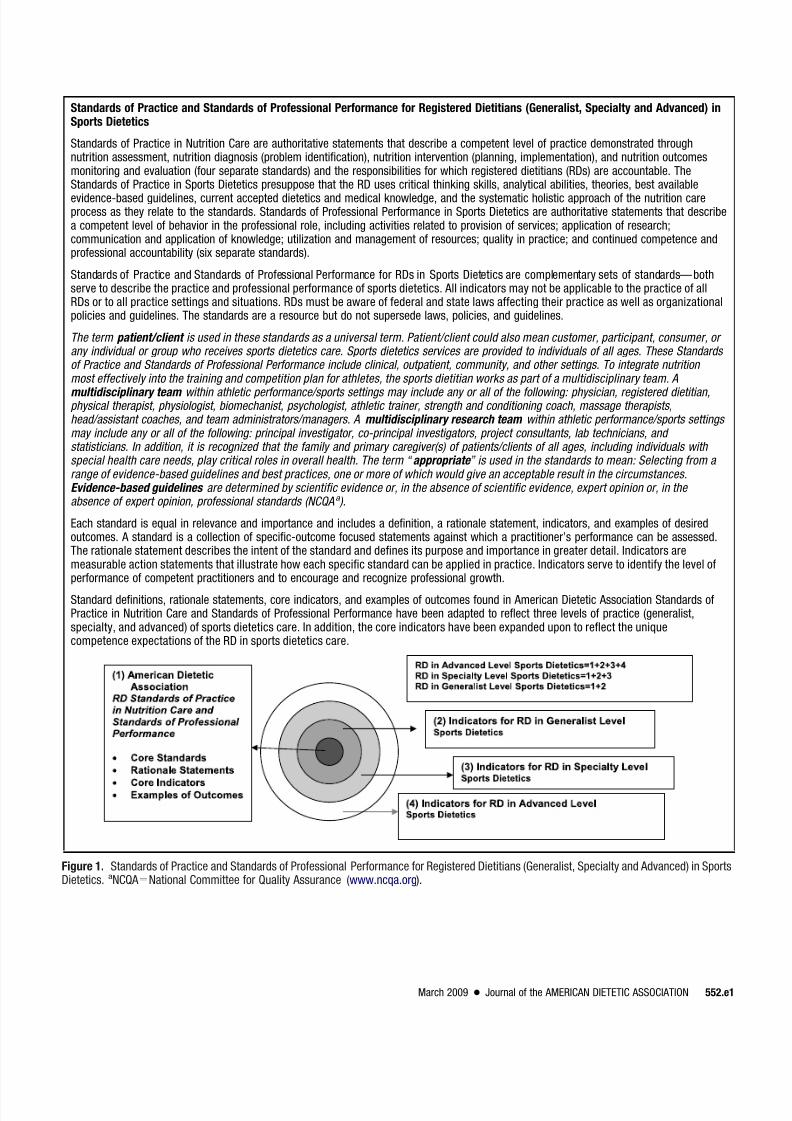
Standards of Practice and Standards of Professional Performance for Registered Dietitians (Generalist, Specialty and Advanced) inSports Dietetics
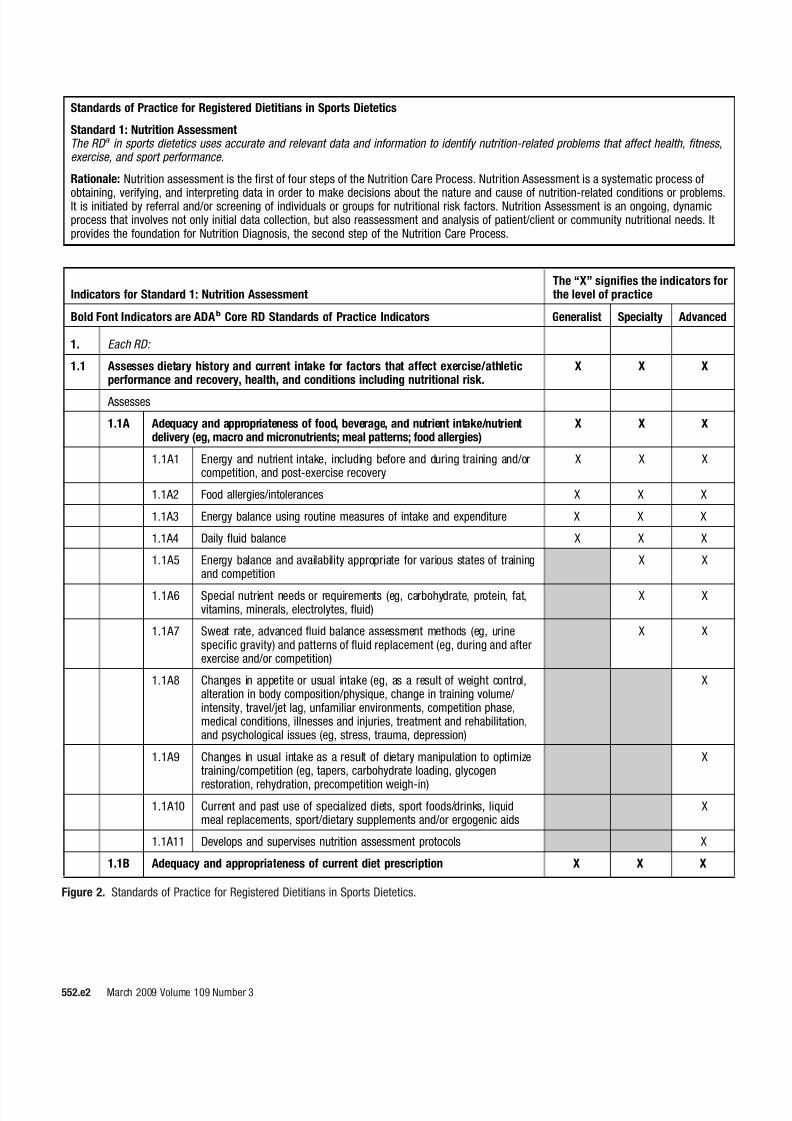
Standards of Practice in Nutrition Care are authoritative statements that describe a competent level of practice demonstrated throughnutrition assessment, nutrition diagnosis (problem identification), nutrition intervention (planning, implementation), and nutrition outcomesmonitoring and evaluation (four separate standards) and the responsibilities for which registered dietitians (RDs) are accountable. TheStandards of Practice in Sports Dietetics presuppose that the RD uses critical thinking skills, analytical abilities, theories, best available
evidence-based guidelines, current accepted dietetics and medical knowledge, and the systematic holistic approach of the nutrition careprocess as they relate to the standards. Standards of Professional Performance in Sports Dietetics are authoritative statements that describea competent level of behavior in the professional role, including activities related to provision of services; application of research;communication and application of knowledge; utilization and management of resources; quality in practice; and continued competence andprofessional accountability (six separate standards).
Standards of Practice and Standards of Professional Performance for RDs in Sports Dietetics are complementary sets of standards— bothserve to describe the practice and professional performance of sports dietetics. All indicators may not be applicable to the practice of allRDs or to all practice settings and situations. RDs must be aware of federal and state laws affecting their practice as well as organizationalpolicies and guidelines. The standards are a resource but do not supersede laws, policies, and guidelines.
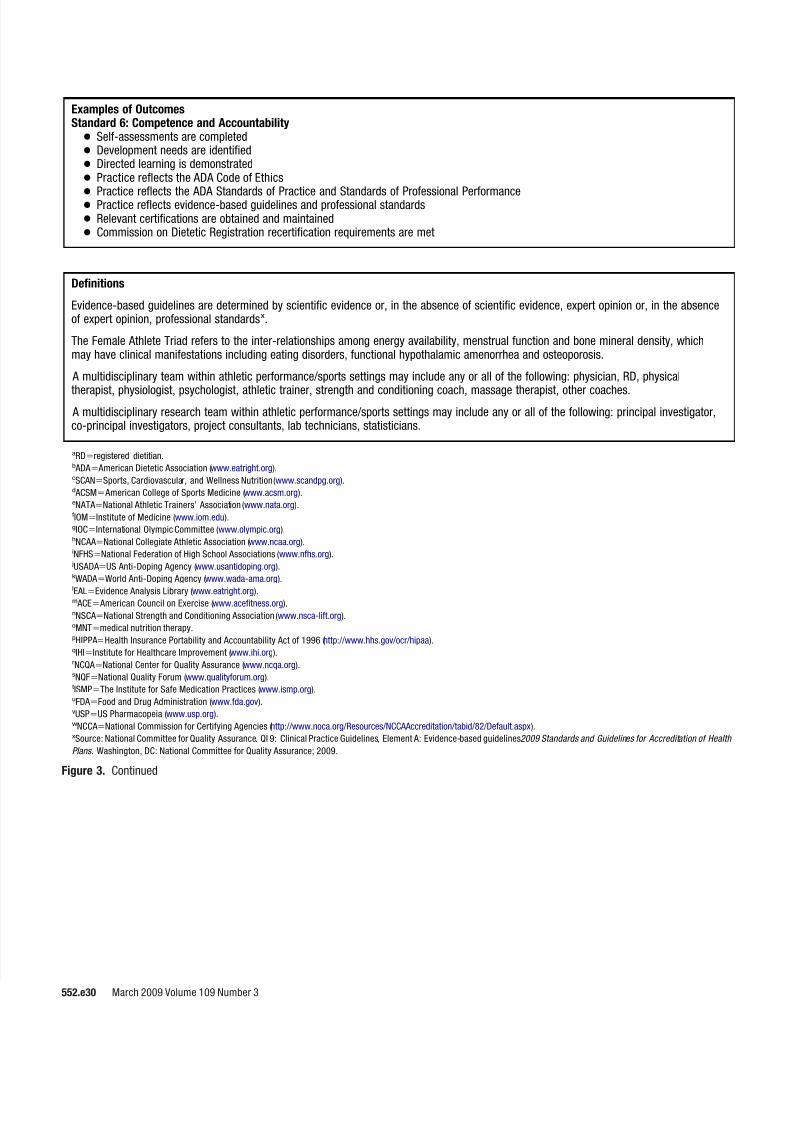
The term patient/client is used in these standards as a universal term. Patient/client could also mean customer, participant, consumer, or any individual or group who receives sports dietetics care. Sports dietetics services are provided to individuals of all ages. These Standards of Practice and Standards of Professional Performance include clinical, outpatient, community, and other settings. To integrate nutrition most effectively into the training and competition plan for athletes, the sports dietitian works as part of a multidisciplinary team. A
multidisciplinary team within athletic performance/sports settings may include any or all of the following: physician, registered dietitian,physical therapist, physiologist, biomechanist, psychologist, athletic trainer, strength and conditioning coach, massage therapists,head/assistant coaches, and team administrators/managers. A multidisciplinary research team within athletic performance/sports settings may include any or all of the following: principal investigator, co-principal investigators, project consultants, lab technicians, and statisticians. In addition, it is recognized that the family and primary caregiver(s) of patients/clients of all ages, including individuals with special health care needs, play critical roles in overall health. The term “ appropriate ” is used in the standards to mean: Selecting from a range of evidence-based guidelines and best practices, one or more of which would give an acceptable result in the circumstances.Evidence-based guidelines are determined by scientific evidence or, in the absence of scientific evidence, expert opinion or, in the absence of expert opinion, professional standards (NCQA a ).
Each standard is equal in relevance and importance and includes a definition, a rationale statement, indicators, and examples of desiredoutcomes. A standard is a collection of specific-outcome focused statements against which a practitioner’s performance can be assessed.The rationale statement describes the intent of the standard and defines its purpose and importance in greater detail. Indicators aremeasurable action statements that illustrate how each specific standard can be applied in practice. Indicators serve to identify the level ofperformance of competent practitioners and to encourage and recognize professional growth.
Standard definitions, rationale statements, core indicators, and examples of outcomes found in American Dietetic Association Standards ofPractice in Nutrition Care and Standards of Professional Performance have been adapted to reflect three levels of practice (generalist,specialty, and advanced) of sports dietetics care. In addition, the core indicators have been expanded upon to reflect the uniquecompetence expectations of the RD in sports dietetics care.
Figure 1. Standards of Practice and Standards of Professional Performance for Registered Dietitians (Generalist, Specialty and Advanced) in SportsDietetics. aNCQA National Committee for Quality Assurance (www.ncqa.org).
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e1
Indicators for Standard 1: Nutrition AssessmentThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADAb Core RD Standards of Practice Indicators Generalist Specialty Advanced
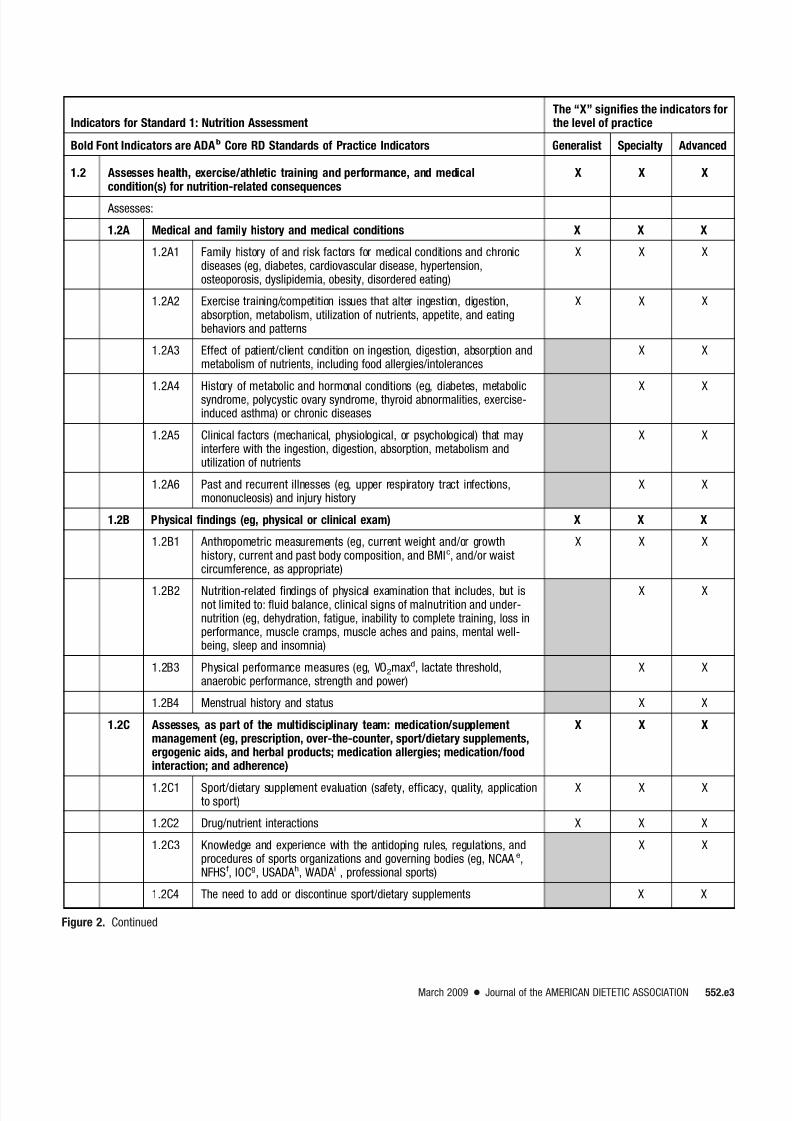
1.2 Assesses health, exercise/athletic training and performance, and medicalcondition(s) for nutrition-related consequences
X X X
Assesses:
1.2A Medical and family history and medical conditions X X X
1.2A1 Family history of and risk factors for medical conditions and chronicdiseases (eg, diabetes, cardiovascular disease, hypertension,osteoporosis, dyslipidemia, obesity, disordered eating)
X X X
1.2A2 Exercise training/competition issues that alter ingestion, digestion,absorption, metabolism, utilization of nutrients, appetite, and eatingbehaviors and patterns
X X X
1.2A3 Effect of patient/client condition on ingestion, digestion, absorption andmetabolism of nutrients, including food allergies/intolerances
X X
1.2A4 History of metabolic and hormonal conditions (eg, diabetes, metabolicsyndrome, polycystic ovary syndrome, thyroid abnormalities, exercise-induced asthma) or chronic diseases
X X
1.2A5 Clinical factors (mechanical, physiological, or psychological) that mayinterfere with the ingestion, digestion, absorption, metabolism andutilization of nutrients
X X
1.2A6 Past and recurrent illnesses (eg, upper respiratory tract infections,mononucleosis) and injury history
X X
1.2B Physical findings (eg, physical or clinical exam) X X X
1.2B1 Anthropometric measurements (eg, current weight and/or growthhistory, current and past body composition, and BMIc, and/or waistcircumference, as appropriate)
X X X
1.2B2 Nutrition-related findings of physical examination that includes, but isnot limited to: fluid balance, clinical signs of malnutrition and under-nutrition (eg, dehydration, fatigue, inability to complete training, loss inperformance, muscle cramps, muscle aches and pains, mental well-being, sleep and insomnia)
1.2C Assesses, as part of the multidisciplinary team: medication/supplementmanagement (eg, prescription, over-the-counter, sport/dietary supplements,ergogenic aids, and herbal products; medication allergies; medication/foodinteraction; and adherence)
1.2C3 Knowledge and experience with the antidoping rules, regulations, andprocedures of sports organizations and governing bodies (eg, NCAA e,NFHSf, IOCg, USADA h, WADA i , professional sports)
X X
1.2C4 The need to add or discontinue sport/dietary supplements X X
Figure 2. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e3
Indicators for Standard 1: Nutrition AssessmentThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADAb Core RD Standards of Practice Indicators Generalist Specialty Advanced
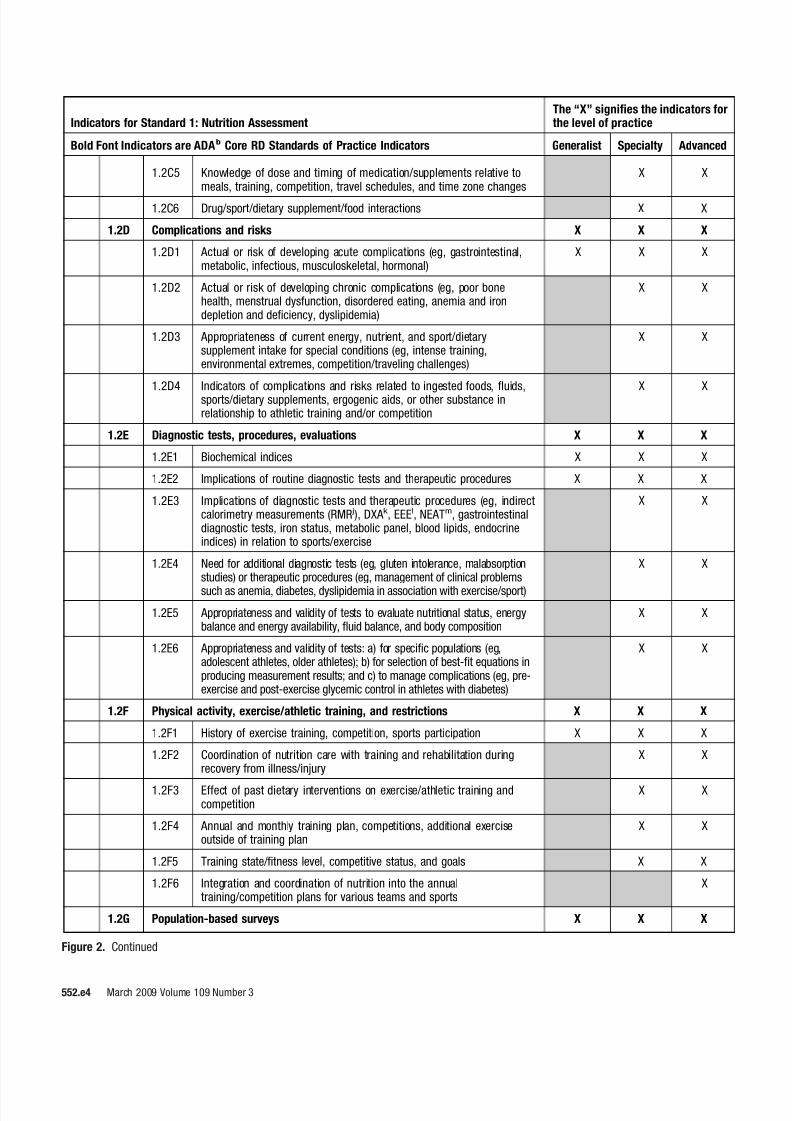
1.2C5 Knowledge of dose and timing of medication/supplements relative tomeals, training, competition, travel schedules, and time zone changes
X X
1.2C6 Drug/sport/dietary supplement/food interactions X X
1.2D Complications and risks X X X
1.2D1 Actual or risk of developing acute complications (eg, gastrointestinal,metabolic, infectious, musculoskeletal, hormonal)
X X X
1.2D2 Actual or risk of developing chronic complications (eg, poor bonehealth, menstrual dysfunction, disordered eating, anemia and irondepletion and deficiency, dyslipidemia)
X X
1.2D3 Appropriateness of current energy, nutrient, and sport/dietarysupplement intake for special conditions (eg, intense training,environmental extremes, competition/traveling challenges)
X X
1.2D4 Indicators of complications and risks related to ingested foods, fluids,sports/dietary supplements, ergogenic aids, or other substance inrelationship to athletic training and/or competition
X X
1.2E Diagnostic tests, procedures, evaluations X X X
1.2E1 Biochemical indices X X X
1.2E2 Implications of routine diagnostic tests and therapeutic procedures X X X
1.2E3 Implications of diagnostic tests and therapeutic procedures (eg, indirectcalorimetry measurements (RMR j), DXA k , EEEl, NEATm, gastrointestinaldiagnostic tests, iron status, metabolic panel, blood lipids, endocrineindices) in relation to sports/exercise
X X
1.2E4 Need for additional diagnostic tests (eg, gluten intolerance, malabsorptionstudies) or therapeutic procedures (eg, management of clinical problems
such as anemia, diabetes, dyslipidemia in association with exercise/sport)
X X
1.2E5 Appropriateness and validity of tests to evaluate nutritional status, energybalance and energy availability, fluid balance, and body composition
X X
1.2E6 Appropriateness and validity of tests: a) for specific populations (eg,adolescent athletes, older athletes); b) for selection of best-fit equations inproducing measurement results; and c) to manage complications (eg, pre-exercise and post-exercise glycemic control in athletes with diabetes)
X X
1.2F Physical activity, exercise/athletic training, and restrictions X X X
1.2F1 History of exercise training, competition, sports participation X X X
1.2F2 Coordination of nutrition care with training and rehabilitation duringrecovery from illness/injury
X X
1.2F3 Effect of past dietary interventions on exercise/athletic training andcompetition
X X
1.2F4 Annual and monthly training plan, competitions, additional exerciseoutside of training plan
X X
1.2F5 Training state/fitness level, competitive status, and goals X X
1.2F6 Integration and coordination of nutrition into the annualtraining/competition plans for various teams and sports
Indicators for Standard 1: Nutrition AssessmentThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADAb Core RD Standards of Practice Indicators Generalist Specialty Advanced
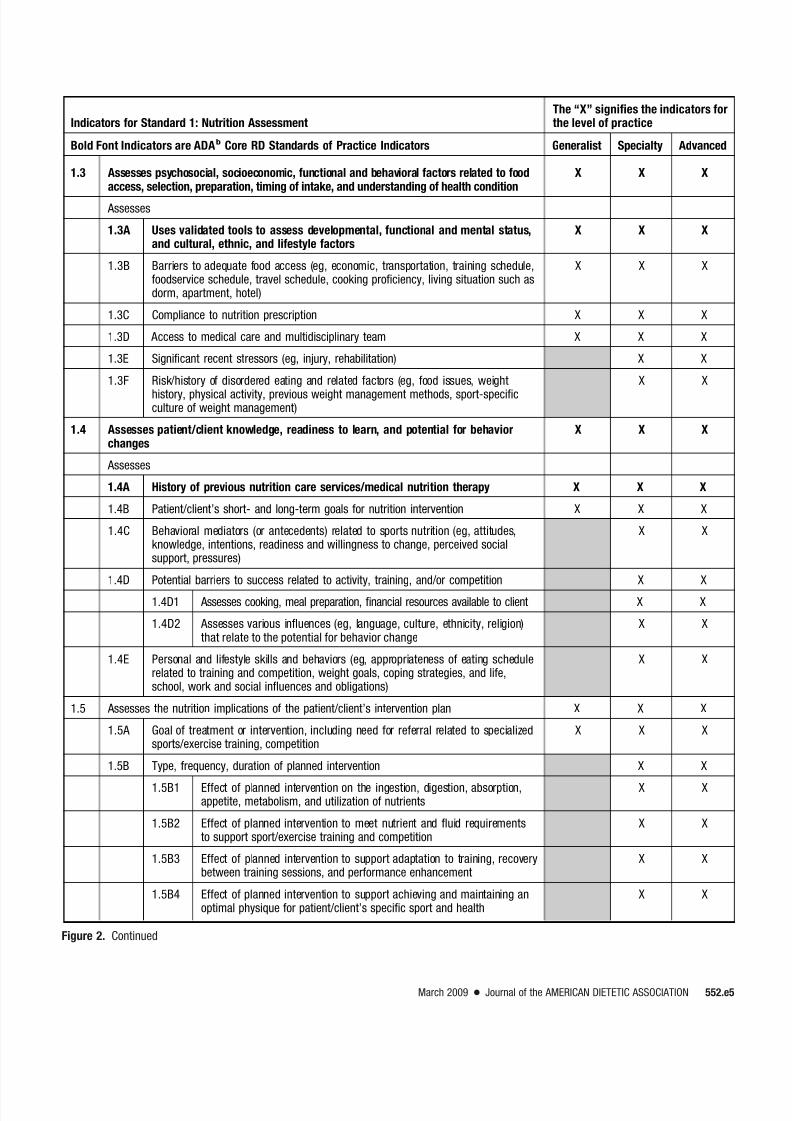
1.3 Assesses psychosocial, socioeconomic, functional and behavioral factors related to foodaccess, selection, preparation, timing of intake, and understanding of health condition
X X X
Assesses
1.3A Uses validated tools to assess developmental, functional and mental status,and cultural, ethnic, and lifestyle factors
X X X
1.3B Barriers to adequate food access (eg, economic, transportation, training schedule,foodservice schedule, travel schedule, cooking proficiency, living situation such asdorm, apartment, hotel)
X X X
1.3C Compliance to nutrition prescription X X X
1.3D Access to medical care and multidisciplinary team X X X
1.3E Significant recent stressors (eg, injury, rehabilitation) X X
1.3F Risk/history of disordered eating and related factors (eg, food issues, weight
1.4 Assesses patient/client knowledge, readiness to learn, and potential for behaviorchanges
X X X
Assesses
1.4A History of previous nutrition care services/medical nutrition therapy X X X
1.4B Patient/client’s short- and long-term goals for nutrition intervention X X X
1.4C Behavioral mediators (or antecedents) related to sports nutrition (eg, attitudes,knowledge, intentions, readiness and willingness to change, perceived socialsupport, pressures)
X X
1.4D Potential barriers to success related to activity, training, and/or competition X X
1.4D1 Assesses cooking, meal preparation, financial resources available to client X X
1.4D2 Assesses various influences (eg, language, culture, ethnicity, religion)that relate to the potential for behavior change
X X
1.4E Personal and lifestyle skills and behaviors (eg, appropriateness of eating schedulerelated to training and competition, weight goals, coping strategies, and life,school, work and social influences and obligations)
X X
1.5 Assesses the nutrition implications of the patient/client’s intervention plan X X X
1.5A Goal of treatment or intervention, including need for referral related to specializedsports/exercise training, competition
X X X
1.5B Type, frequency, duration of planned intervention X X
1.5B1 Effect of planned intervention on the ingestion, digestion, absorption,appetite, metabolism, and utilization of nutrients
X X
1.5B2 Effect of planned intervention to meet nutrient and fluid requirementsto support sport/exercise training and competition
X X
1.5B3 Effect of planned intervention to support adaptation to training, recoverybetween training sessions, and performance enhancement
X X
1.5B4 Effect of planned intervention to support achieving and maintaining anoptimal physique for patient/client’s specific sport and health
X X
Figure 2. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e5
Indicators for Standard 1: Nutrition AssessmentThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADAb Core RD Standards of Practice Indicators Generalist Specialty Advanced
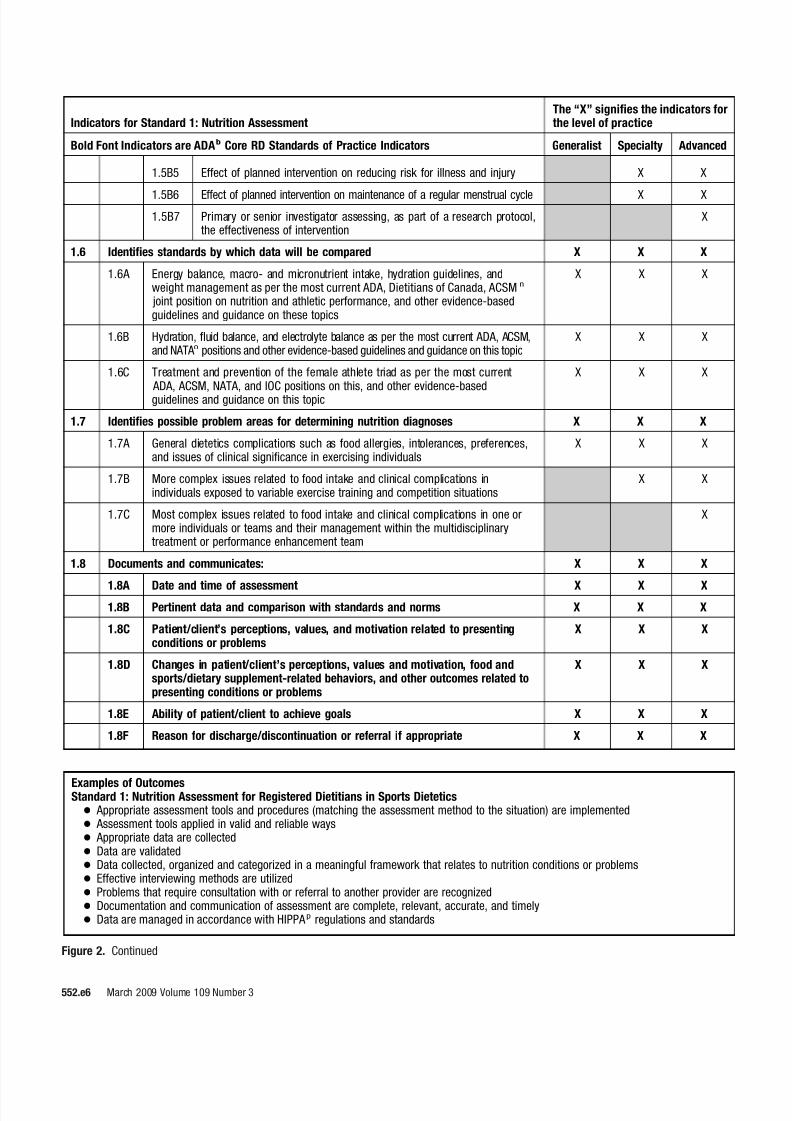
1.5B5 Effect of planned intervention on reducing risk for illness and injury X X
1.5B6 Effect of planned intervention on maintenance of a regular menstrual cycle X X
1.5B7 Primary or senior investigator assessing, as part of a research protocol,the effectiveness of intervention
X
1.6 Identifies standards by which data will be compared X X X
1.6A Energy balance, macro- and micronutrient intake, hydration guidelines, andweight management as per the most current ADA, Dietitians of Canada, ACSM n
joint position on nutrition and athletic performance, and other evidence-basedguidelines and guidance on these topics
X X X
1.6B Hydration, fluid balance, and electrolyte balance as per the most current ADA, ACSM,and NATA o positions and other evidence-based guidelines and guidance on this topic
X X X
1.6C Treatment and prevention of the female athlete triad as per the most current ADA, ACSM, NATA, and IOC positions on this, and other evidence-basedguidelines and guidance on this topic
X X X
1.7 Identifies possible problem areas for determining nutrition diagnoses X X X
1.7A General dietetics complications such as food allergies, intolerances, preferences,and issues of clinical significance in exercising individuals
X X X
1.7B More complex issues related to food intake and clinical complications inindividuals exposed to variable exercise training and competition situations
X X
1.7C Most complex issues related to food intake and clinical complications in one ormore individuals or teams and their management within the multidisciplinarytreatment or performance enhancement team
X
1.8 Documents and communicates: X X X
1.8A Date and time of assessment X X X1.8B Pertinent data and comparison with standards and norms X X X
1.8C Patient/client’s perceptions, values, and motivation related to presentingconditions or problems
X X X
1.8D Changes in patient/client’s perceptions, values and motivation, food andsports/dietary supplement-related behaviors, and other outcomes related topresenting conditions or problems
X X X
1.8E Ability of patient/client to achieve goals X X X
1.8F Reason for discharge/discontinuation or referral if appropriate X X X
Examples of OutcomesStandard 1: Nutrition Assessment for Registered Dietitians in Sports Dietetics● Appropriate assessment tools and procedures (matching the assessment method to the situation) are implemented● Assessment tools applied in valid and reliable ways● Appropriate data are collected● Data are validated● Data collected, organized and categorized in a meaningful framework that relates to nutrition conditions or problems● Effective interviewing methods are utilized● Problems that require consultation with or referral to another provider are recognized● Documentation and communication of assessment are complete, relevant, accurate, and timely● Data are managed in accordance with HIPPA p regulations and standards
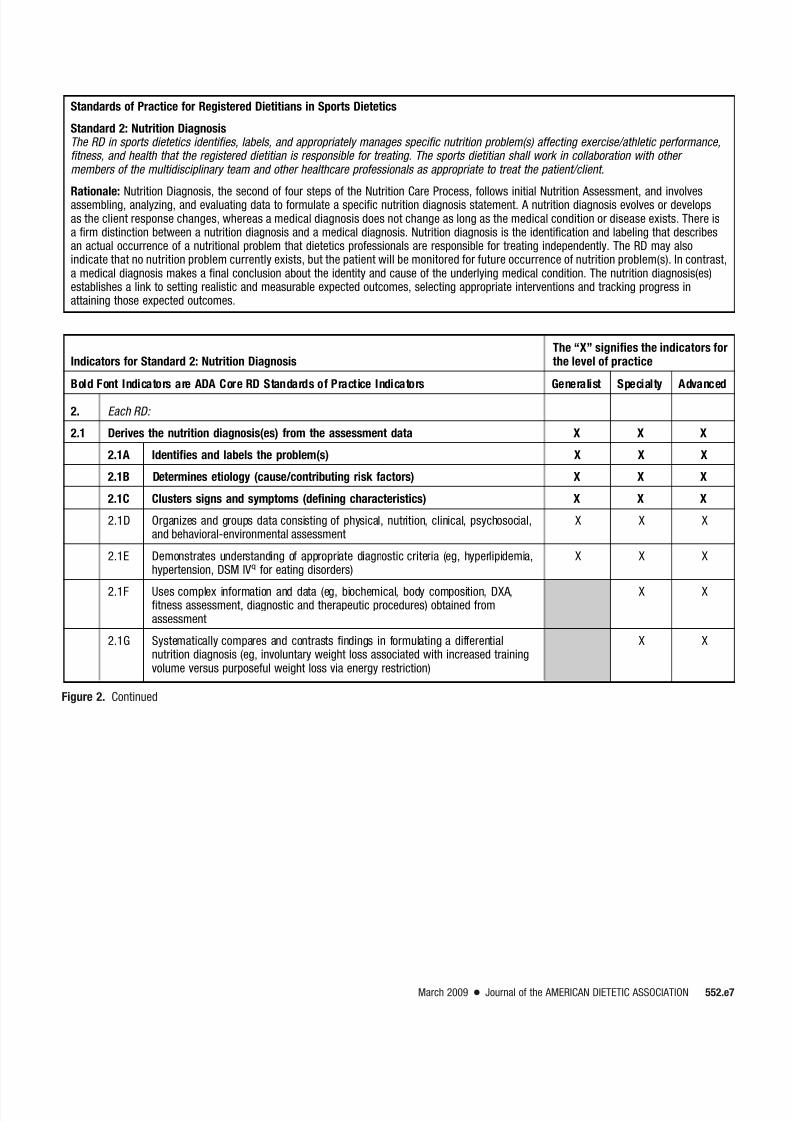
Standards of Practice for Registered Dietitians in Sports Dietetics
Standard 2: Nutrition DiagnosisThe RD in sports dietetics identifies, labels, and appropriately manages specific nutrition problem(s) affecting exercise/athletic performance,fitness, and health that the registered dietitian is responsible for treating. The sports dietitian shall work in collaboration with other members of the multidisciplinary team and other healthcare professionals as appropriate to treat the patient/client.
Rationale: Nutrition Diagnosis, the second of four steps of the Nutrition Care Process, follows initial Nutrition Assessment, and involvesassembling, analyzing, and evaluating data to formulate a specific nutrition diagnosis statement. A nutrition diagnosis evolves or developsas the client response changes, whereas a medical diagnosis does not change as long as the medical condition or disease exists. There isa firm distinction between a nutrition diagnosis and a medical diagnosis. Nutrition diagnosis is the identification and labeling that describesan actual occurrence of a nutritional problem that dietetics professionals are responsible for treating independently. The RD may alsoindicate that no nutrition problem currently exists, but the patient will be monitored for future occurrence of nutrition problem(s). In contrast,a medical diagnosis makes a final conclusion about the identity and cause of the underlying medical condition. The nutrition diagnosis(es)establishes a link to setting realistic and measurable expected outcomes, selecting appropriate interventions and tracking progress inattaining those expected outcomes.
Indicators for Standard 2: Nutrition DiagnosisThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
2. Each RD:
2.1 Derives the nutrition diagnosis(es) from the assessment data X X X
2.1A Identifies and labels the problem(s) X X X
2.1B Determines etiology (cause/contributing risk factors) X X X
2.1C Clusters signs and symptoms (defining characteristics) X X X
2.1D Organizes and groups data consisting of physical, nutrition, clinical, psychosocial,and behavioral-environmental assessment
X X X
2.1E Demonstrates understanding of appropriate diagnostic criteria (eg, hyperlipidemia,hypertension, DSM IVq for eating disorders)
X X X
2.1F Uses complex information and data (eg, biochemical, body composition, DXA,fitness assessment, diagnostic and therapeutic procedures) obtained fromassessment
X X
2.1G Systematically compares and contrasts findings in formulating a differentialnutrition diagnosis (eg, involuntary weight loss associated with increased trainingvolume versus purposeful weight loss via energy restriction)
X X
Figure 2. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e7
Indicators for Standard 2: Nutrition DiagnosisThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
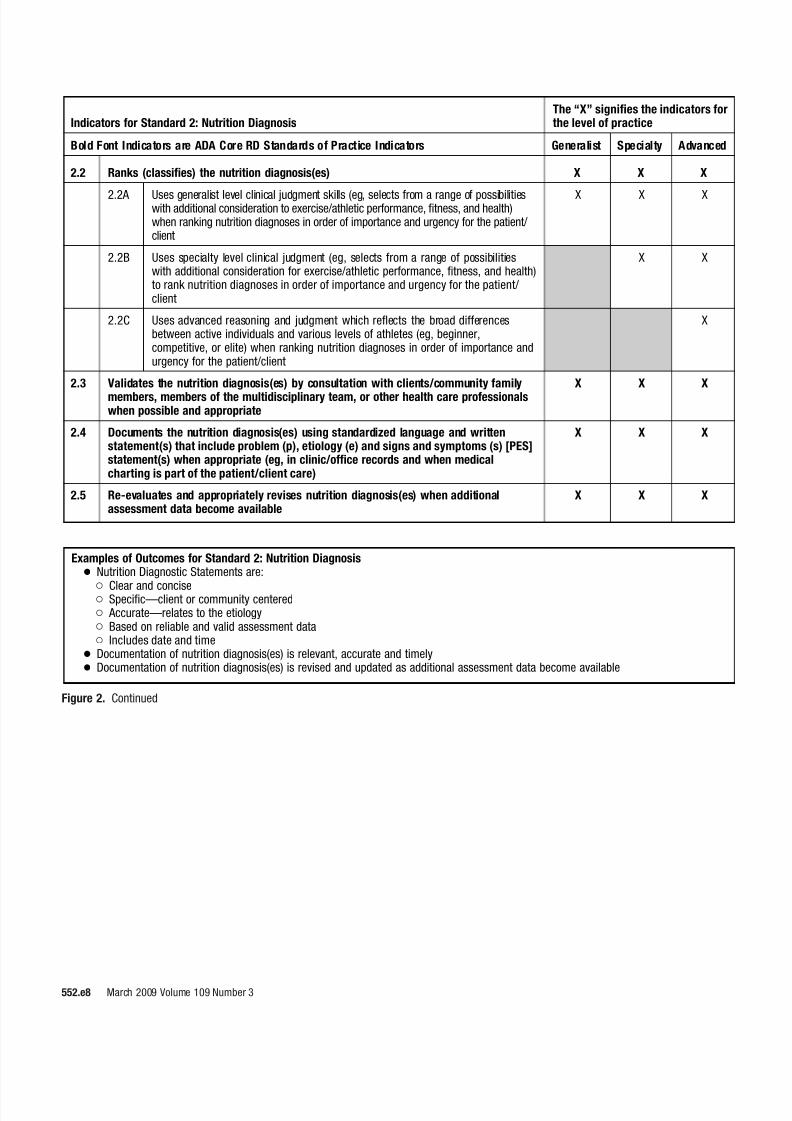
2.2 Ranks (classifies) the nutrition diagnosis(es) X X X
2.2A Uses generalist level clinical judgment skills (eg, selects from a range of possibilitieswith additional consideration to exercise/athletic performance, fitness, and health)when ranking nutrition diagnoses in order of importance and urgency for the patient/ client
X X X
2.2B Uses specialty level clinical judgment (eg, selects from a range of possibilitieswith additional consideration for exercise/athletic performance, fitness, and health)to rank nutrition diagnoses in order of importance and urgency for the patient/ client
X X
2.2C Uses advanced reasoning and judgment which reflects the broad differencesbetween active individuals and various levels of athletes (eg, beginner,competitive, or elite) when ranking nutrition diagnoses in order of importance andurgency for the patient/client
X
2.3 Validates the nutrition diagnosis(es) by consultation with clients/community family
members, members of the multidisciplinary team, or other health care professionalswhen possible and appropriate
X X X
2.4 Documents the nutrition diagnosis(es) using standardized language and writtenstatement(s) that include problem (p), etiology (e) and signs and symptoms (s) [PES]statement(s) when appropriate (eg, in clinic/office records and when medicalcharting is part of the patient/client care)
X X X
2.5 Re-evaluates and appropriately revises nutrition diagnosis(es) when additionalassessment data become available
X X X
Examples of Outcomes for Standard 2: Nutrition Diagnosis● Nutrition Diagnostic Statements are:
Clear and concise Specific—client or community centered Accurate—relates to the etiology Based on reliable and valid assessment data Includes date and time
● Documentation of nutrition diagnosis(es) is relevant, accurate and timely● Documentation of nutrition diagnosis(es) is revised and updated as additional assessment data become available
Standards of Practice for Registered Dietitians in Sports Dietetics
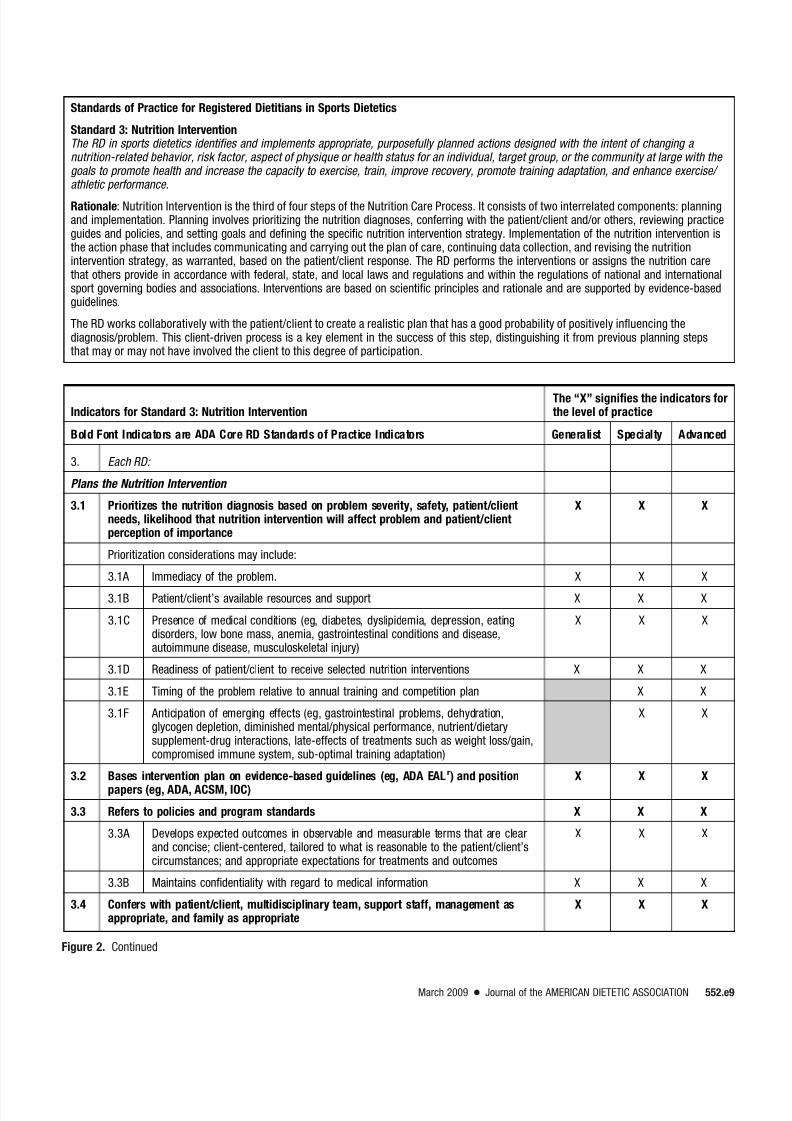
Standard 3: Nutrition InterventionThe RD in sports dietetics identifies and implements appropriate, purposefully planned actions designed with the intent of changing a nutrition-related behavior, risk factor, aspect of physique or health status for an individual, target group, or the community at large with the goals to promote health and increase the capacity to exercise, train, improve recovery, promote training adaptation, and enhance exercise/ athletic performance.
Rationale: Nutrition Intervention is the third of four steps of the Nutrition Care Process. It consists of two interrelated components: planningand implementation. Planning involves prioritizing the nutrition diagnoses, conferring with the patient/client and/or others, reviewing practiceguides and policies, and setting goals and defining the specific nutrition intervention strategy. Implementation of the nutrition intervention isthe action phase that includes communicating and carrying out the plan of care, continuing data collection, and revising the nutritionintervention strategy, as warranted, based on the patient/client response. The RD performs the interventions or assigns the nutrition carethat others provide in accordance with federal, state, and local laws and regulations and within the regulations of national and internationalsport governing bodies and associations. Interventions are based on scientific principles and rationale and are supported by evidence-basedguidelines.
The RD works collaboratively with the patient/client to create a realistic plan that has a good probability of positively influencing thediagnosis/problem. This client-driven process is a key element in the success of this step, distinguishing it from previous planning stepsthat may or may not have involved the client to this degree of participation.
Indicators for Standard 3: Nutrition InterventionThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
3. Each RD:
Plans the Nutrition Intervention
3.1 Prioritizes the nutrition diagnosis based on problem severity, safety, patient/clientneeds, likelihood that nutrition intervention will affect problem and patient/clientperception of importance
X X X
Prioritization considerations may include:
3.1A Immediacy of the problem. X X X
3.1B Patient/client’s available resources and support X X X
3.1C Presence of medical conditions (eg, diabetes, dyslipidemia, depression, eatingdisorders, low bone mass, anemia, gastrointestinal conditions and disease,autoimmune disease, musculoskeletal injury)
X X X
3.1D Readiness of patient/client to receive selected nutrition interventions X X X
3.1E Timing of the problem relative to annual training and competition plan X X
3.1F Anticipation of emerging effects (eg, gastrointestinal problems, dehydration,glycogen depletion, diminished mental/physical performance, nutrient/dietarysupplement-drug interactions, late-effects of treatments such as weight loss/gain,compromised immune system, sub-optimal training adaptation)
X X
3.2 Bases intervention plan on evidence-based guidelines (eg, ADA EALr) and position
papers (eg, ADA, ACSM, IOC)
X X X
3.3 Refers to policies and program standards X X X
3.3A Develops expected outcomes in observable and measurable terms that are clearand concise; client-centered, tailored to what is reasonable to the patient/client’scircumstances; and appropriate expectations for treatments and outcomes
X X X
3.3B Maintains confidentiality with regard to medical information X X X
3.4 Confers with patient/client, multidisciplinary team, support staff, management asappropriate, and family as appropriate
X X X
Figure 2. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e9
Indicators for Standard 3: Nutrition InterventionThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
3.5 Determines patient/client-focused goals and expected outcomes X X X
Considerations of the intervention plan may expand but is not limited to include:
3.5A Plans intervention to address current issues (eg, fatigue; dehydration; musclecramping; inadequate recovery, exercise/athletic performance improvement andtraining adaptation; diarrhea and other gastrointestinal issues; illness; injury;eating disorder and female athlete triad; dietary and sports/dietary supplementuse, or other clinical issues)
X X
3.5B Anticipates barriers to successful implementation (eg, patient/client compliance,timing of intervention relative to annual training/competition and travel plans, foodavailability and preparation issues, financial issues, regulations of sport governingbodies and associations, issues related to team-athlete-coach-family dynamics)
X X
3.5D Anticipates issues related to off-season/transition weight change, detraining, andscheduled and unscheduled breaks in training such as holidays)
X X
3.5E Anticipates ways to minimize barriers and other issues, prevent treatment delays,reduce relapse, and reduce the need for more advanced/involved treatment options
X X
3.6 Details the nutrition prescription X X X
3.6A Considers the educational needs of the patient/client, including cultural competency X X X
3.6B Selects specific intervention strategies that are focused on the etiology of theproblem, that are effective, and based on evidence, best practices, professionalexperience, and time constraints (ie, sufficient time to make meaningful changesbefore a competition deadline)
X X
3.7 Defines time and frequency of nutrition intervention X X X
3.8 Utilizes standardized language for describing interventions X X X
3.9 Identifies resources and/or referrals needed X X X
Implements the Nutrition Intervention
3.10 Collaborates with colleagues X X X
3.10A Participates in communications within the multidisciplinary team and/orperformance enhancement team
X X X
3.10B Collaborates with the multidisciplinary team and/or performance enhancement team X X
3.10C Directs the multidisciplinary team and/or performance enhancement team X
3.11 Communicates the nutrition intervention plan to the referring physician,multidisciplinary team, and/or patient/client
X X X
3.12 Initiates the nutrition intervention plan X X X
3.12A Utilizes appropriate behavior change theories (eg, motivational interviewing,behavior modification, modeling) to facilitate self-management self-care strategies X X X
3.12B Uses critical thinking and synthesis skills to guide decision-making incomplicated, unpredictable, and dynamic situations
X
3.13 Continues data collection X X X
3.14 Individualizes nutrition intervention X X X
3.14A Uses a variety of educational approaches, tools, and materials as appropriate X X X
3.14B Adapts general nutrition educational tools to individualized learning style andmethod of communication and culture of the sport
Indicators for Standard 3: Nutrition InterventionThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
3.14C Uses critical thinking and synthesis skills for combining multiple interventionapproaches as appropriate
X X
3.14D Draws on experiential knowledge and current body of scientific evidence aboutthe patient/client population to individualize the strategy for complex interventions
X
3.15 Monitors, follows-up, and verifies that nutrition intervention is occurring X X X
3.15A Communicates with multidisciplinary team and/or performance enhancement teamto verify progress
X X X
3.15B Collaborates with multidisciplinary team and/or performance enhancement teamto verify progress and adjust strategies
X X
3.15C Directs the integration of the athlete’s progress within the multidisciplinary teamand/or performance enhancement team
X
3.16 Adjusts nutrition intervention plan, if needed, as response occurs X X X
3.16A Adjusts nutrition intervention (eg, general energy balance, macro- and micronutrientneeds, hydrations guidelines) according to annual training/competition plan
X X X
3.16B Adjusts nutrition intervention (eg, energy balance, macro- and micronutrientneeds, hydrations guidelines for high intensity training and recovery, meetingweight class goals, adjusting to environmental extremes) according to annualtraining/competition plan
X X
3.17 Documents X X X
3.17A Date and time X X X
3.17B Specific treatment goals and expected outcomes X X X
3.17C Recommended interventions X X X
3.17D Adjustments to the plan and justifications X X X
3.17E Client/community receptivity X X X
3.17F Referrals made and resources used X X X
3.17G Other information relevant to providing care and monitoring progress over time X X X
3.17H Plans for follow-up and frequency of care X X X
3.17I Rationale for discharge/discontinuation or referral if appropriate X X X
Examples of Outcomes for Standard 3: Nutrition Intervention● Appropriate prioritizing and setting of goals/expected outcomes● Appropriate nutrition plan or prescription is developed● Interdisciplinary connections are established● Nutrition interventions are delivered and actions are carried out● Documentation of nutrition intervention is: Comprehensive Specific Accurate Relevant Timely Dated and Timed
● Documentation of nutrition intervention is revised and updated
Figure 2. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e11
Standards of Practice for Registered Dietitians in Sports Dietetics
Standard 4: Nutrition Monitoring and EvaluationThe RD in sports dietetics monitors and evaluates outcome(s) directly related to the nutrition diagnosis and the goals established in the prescribed intervention plan. This will assist in determining if the goals or expected outcomes of nutrition care are being met. Through monitoring and evaluation, the RD uses pertinent outcome indicators (markers) that are relevant to the patient/client-defined needs, nutrition diagnosis, and nutrition goals. Progress should be monitored, measured, and evaluated on a timely, planned schedule until
discharge/discontinuation.
Rationale: Nutrition monitoring and evaluation is the fourth step in the Nutrition Care Process. Progress should be monitored, measured andevaluated on a timely, planned schedule. Alterations in outcome indicators (eg, undesired body weight changes, illness or injury, comprisedexercise recovery) require reevaluation of the nutrition care process. Monitoring specifically refers to the review and measurement of thepatient/client’s status at a scheduled (pre-planned) follow-up consultation. The follow-up would relate to the nutrition diagnosis, interventionplans/goals and outcomes, whereas evaluation is the systematic comparison of the most current findings with the previous status,intervention goals, or a reference standard.
Indicators for Standard 4: Nutrition Monitoring and EvaluationThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
4. Each RD:
4.1 Monitors progress X X X
4.1A Checks patient/client understanding and compliance with nutrition intervention X X X
4.1A4 When necessary, modifies nutrition intervention/care plan based onpatient/client tolerance, response, and outcome measures with regardto documented goals and objectives
X X X
4.1A5 Documents adherence to recommended timing of nutrient intake X X X
4.1B Determines if the intervention plan is being implemented as prescribed X X X
4.1B1 Evaluates intervention plan implementation in recreational andcompetitive athletes relative to general sports performance issues
X X X
4.1B2 Evaluates intervention plan implementation in competitive athletesbalancing multiple situations (eg, environmental extremes, rapid weightchanges, travel and events, and/or clinical complications)
X X
4.1B3 Develops appropriate outcomes and assessment plan to determine ifthe goals of the intervention are being met
Indicators for Standard 4: Nutrition Monitoring and EvaluationThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
4.1C Provides evidence of effectiveness of the plan/intervention strategy ininfluencing change in patient/client behavior or status
X X X
4.1C1 Uses multiple data sources to assess progress. Examples may include: X X X
- nutrition focused physical exam (including but not limited to signs offluid, energy, and/or nutrition depletion or excess)
X X X
- assesses adequacy of nutrient intake from all sources X X X
- evaluates changes in body weight, body composition X X X
- considers pertinent medications and sport/dietary supplements indevelopment and implementation of care plan
X X
- evaluates fluid and electrolyte balance X X
- evaluates effects of intervention on exercise/athletic training andperformance
X X
- evaluates effects of intervention on recovery following exercise/athletictraining and competition
X X
- evaluates effects of intervention on progress in rehabilitation X X
4.1C2 Monitors and interprets laboratory and other data X X X
4.1C3 Monitors factors (physical, social, cognitive, environmental) that mayinfluence response to nutrition intervention
X X X
4.1D Identifies positive or negative outcomes X X X
4.1D1 Demonstrates understanding of intended effects and potential adverseeffects of intervention
X X X
4.1D2 Anticipates and assesses intended effects and potential adverse effects
(eg, not meeting set weight class goal for competition) of intervention
X X
4.1E Gathers information to indicate progress or reasons for lack of progress X X X
4.1F Supports conclusions with evidence X X X
4.2 Measures outcomes X X X
4.2A Selects the nutrition care outcome indicator(s) to measure X X X
4.2A1 Impact on physical measures (eg, weight maintenance, body weightand body composition changes, laboratory values)
X X X
4.2A2 Impact on physical measures (eg, weight maintenance, body weightand body composition changes, laboratory values, fluid and electrolytebalance, bone density)
X X
4.2A3 Impact on treatment outcome (eg, minimize barriers, prevent treatmentdelays, reduce relapse and the need for more advanced/involvedtreatment options)
X X
4.2A4 Quality of life and athletic performance (eg, absence of fatigue,absence of muscle cramping, avoidance of gastrointestinal issues)
X X
4.2A5 Quality of life and athletic performance (eg, full sport participation,progress in rehabilitation, absence of fatigue, absence of musclecramping avoidance of gastrointestinal issues)
X
4.2B Uses standardized nutrition care outcome indicator(s) X X X
Figure 2. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e13
Indicators for Standard 4: Nutrition Monitoring and EvaluationThe “X” signifies the indicators forthe level of practice
Bold Font Indicators are ADA Core RD Standards of Practice Indicators Generalist Specialty Advanced
4.3 Evaluates outcomes X X X
4.3A Compares monitoring data with nutrition prescription/goals or reference standard X X X
4.3B Evaluates impact of the sum of all interventions on overall patient/client healthand exercise/athletic performance outcomes
X X
4.3C Establishes desired outcomes and develops evaluation plans to determine if goalsof program or facility are being met
X
4.4 Documents: X X X
4.4A Date and time X X X
4.4B Indicators measured, results, and the method for obtaining measurement X X X
4.4C Criteria to which the indicator is compared (eg, nutrition prescription/goal,evidence-based guidelines, reference standards, or national and internationalguidelines such as, ADA, Dietitians of Canada, ACSM, IOMs, IOC)
X X X
4.4D Factors facilitating or hampering progress X X X
4.4E Other positive or negative outcomes X X X
4.4F Future plans for nutrition care, nutrition monitoring, follow-up, discharge/discontinuation, or referral
X X X
Examples of OutcomesStandard 4: Nutrition Monitoring and Evaluation● The patient/client/community outcome(s) directly relate to the nutrition diagnosis and the goals established in the intervention plan.● Examples include, but are not limited to: Nutrition outcomes (eg, change in knowledge, behavior, food, or nutrient intake) Clinical and health status outcomes (eg, change in relevant laboratory values, body weight, body composition, hydration measures,
risk factors, signs and symptoms, clinical status, complications) Client-centered outcomes (eg, quality of life issues) and improvement in issues related to athletic performance (eg, fatigue,
dehydration, muscle cramping, inadequate recovery, injury), weight management, sports/dietary supplement use, disordered eatingand the female athlete triad, diarrhea and other gastrointestinal issues, illness, diabetes, dyslipidemia, or other clinical issues
Minimization of barriers (eg, patient/client compliance, timing of intervention relative to the annual athletic training/competition andtravel plan, food availability and preparation issues, schedule, living situation, mental health concerns, issues related to team-athlete-coach-parent dynamics, financial issues, and regulations imposed by sport governing bodies and associations regulations)
Health care utilization and cost effectiveness outcomes (eg, decreased need for medications (iron), shortened recovery time frominjuries, decreased incidence of injuries, few illnesses)
● Documentation of the monitoring and evaluation is: Comprehensive Specific Accurate Relevant
Evidence-based guidelines are determined by scientific evidence or, in the absence of scientific evidence, expert opinion or, in the absenceof expert opinion, professional standardst.
A multidisciplinary team within athletic performance/sports settings may include any or all of the following: physician, RD, physicaltherapist, physiologist, psychologist, athletic trainer, strength and conditioning coach, massage therapist, other coaches.
An ergogenic aid is a substance or agent that may have performance-enhancing effects.
The Female Athlete Triad refers to the inter-relationships among energy availability, menstrual function, and bone mineral density, whichmay have clinical manifestations including eating disorders, functional hypothalamic amenorrhea, and osteoporosis.
aRDregistered dietitian.b ADA American Dietetic Association (www.eatright.org).cBMIbody mass index.d VO2maxmaximal aerobic capacity, maximal rate of oxygen consumption, or maximal oxygen uptake.eNCAA National Collegiate Athletic Association (www.ncaa.org).fNFHSNational Federation of High School Associations (www.nfhs.org).gIOCInternational Olympic Committee (www.olympic.org).hUSADA US Anti-Doping Agency (www.usantidoping.org).iWADA World Anti-Doping Agency (www.wada-ama.org). jRMRresting metabolic rate.k
DXA
dual energy x-ray absorptiometry.lEEEexercise energy expenditure.mNEATnon-exercise activity thermogenesis.n ACSM American College of Sports Medicine.oNATA National Athletic Trainers’ Association (www.nata.org).pHIPPA Health Insurance Portability and Accountability Act of 1996 (http://www.hhs.gov/ocr/hipaa ).qDSM IVDiagnostic and Statistical Manual of Mental Disorders.rEALEvidence Analysis Library (www.eatright.org).sIOMInstitute of Medicine (www.iom.edu).tSource: National Committee for Quality Assurance. QI 9: Clinical Practice Guidelines, Element A: Evidence-based guidelines. 2009 Standards and Guidelines for Accreditation of Health
Plans. Washington, DC: National Committee for Quality Assurance; 2009.
Figure 2. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e15
Standards of Professional Performance for Registered Dietitians in Sports Dietetics
Standard 1: Provision of ServicesThe RD a in sports dietetics provides quality service based on customer expectations and needs
Rationale: Quality service is provided, facilitated, and promoted based on the sports dietitian’s knowledge, professional experience, andunderstanding of patient/client needs and expectations.
Indicators for Standard 1: Provision of ServicesThe “X” signifies the indicator forthe level of practice.
Bold Font Indicators are ADAb Core RD Standards of Professional Performance Generalist Specialty Advanced
1. Each RD:
1.1 Participates in the development of nutrition screening parameters for sports-relatedsettings
X X X
1.1A Uses an evidence-based review process to determine screening parameters X X X
1.1B Evaluates the effectiveness of general nutrition and sports nutrition screening tools X X X
1.1C Participates in content and process revisions of policies and protocols X X X
1.1D Directs development, management, and monitoring of nutrition screening policiesand protocols
X
1.2 Audits nutrition screening processes for efficiency and effectiveness X X X
1.3 Contributes to and designs referral process and systems to facilitate public accessto sports dietitians
X X X
1.3A Receives referrals for services from and makes referrals to sports medicine andother sports staff (ie, physician, psychologist, physical therapist, physiologist,athletic trainer, strength coach, other coaches)
X X X
1.3B Evaluates the effectiveness of sports dietetics referral tools (eg, “Find a SCANc
Dietitian” feature on SCAN’s Web site and state, local affiliate, and other referralmechanisms)
X X
1.3C Provides leadership in documenting, evaluating, and updating referral processes X X
1.3D Directs and manages referral processes and systems X
1.4 Collaborates with patient/client to assess needs, background, and resources and toset priorities, establish goals, and create individualized action plans
X X X
1.4A Demonstrates understanding of behavior change and counseling theories andapplies theories (eg, motivational interviewing, stages of change) in practice
X X X
1.4B Recognizes how the athletic environment, culture, health literacy, and socioeconomicstatus may influence exercise/athletic training and performance, health/wellness, andpatient/client use of health care services
X X
1.4C Adapts practice to meet the needs of ethnically and culturally diverse populations
(eg, uses interpreters, selects appropriate levels of interventions, adapts sportsnutrition education/counseling approaches and materials)
X X
1.4D Provides leadership in documenting and evaluating outcomes of using variousintervention models and techniques (eg, health belief model, social cognitivetheory/social learning theory, stages of change)
X X
1.4E Directs and manages systematic processes to identify, track, and update patient/ client resources; documents patient/client use of sports nutrition, and health careand services
X
1.5 Informs and involves patients/clients and their families, when appropriate, in decision-making
X X X
Figure 3. Standards of Professional Performance for Registered Dietitians in Sports Dietetics.
Indicators for Standard 1: Provision of ServicesThe “X” signifies the indicator forthe level of practice.
Bold Font Indicators are ADAb Core RD Standards of Professional Performance Generalist Specialty Advanced
1.6 Recognizes patient/client concepts of illness, injury, and rehabilitation and their culturalbeliefs
X X X
1.7 Applies principles of sports nutrition in relation to exercise training, performanceenhancement, health promotion, and behavior change appropriate for diversepopulations
X X X
1.8 Collaborates and coordinates with colleagues X X X
1.8A Collaborates within multidisciplinary medical teams to provide quality care X X X
1.8B Works in partnership with exercise/athletic performance professionals, otherhealth care providers, and ancillary referral sources
X X X
1.8C Serves as a consultant for medical management of nutrition-related illnesses andconditions
X X X
1.8D Develops and delivers nutrition education and services that integrate nutritionwith exercise/athletic performance, health promotion, and wellness
X X X
1.8E Develops and manages sports nutrition programs and educational materials based onpatient/client needs, culture, evidence-based guidelines, and available resources
X X
1.8F Plans, develops, and implements systems of sports dietetics care and servicesusing evidence-based guidelines and best practices
X X
1.8G Directs systems of sports dietetics care and services X
1.9 Applies knowledge and skills to determine appropriate action plans X X X
1.9A Applies general sports dietetics knowledge and skills to develop intervention andaction plans
X X X
1.9B Applies knowledge and skills at the specialty level (eg, functional workingknowledge of sports dietetics, evidence-based guidelines, best practices, and
clinical experience) to determine the most appropriate action plan
X X
1.9C Applies knowledge and skills at the advanced level (eg, advanced andcomprehensive knowledge of sports dietetics, evidence-based guidelines, bestpractices, and clinical experience) to determine the most appropriate action plan
X
1.10 Develops policies and procedures that reflect best evidence and applicable laws andregulations
X X X
1.10A Collects data and documents outcomes relative to evidence-based guidelines andbest practices
X X X
1.10B Participates in developing and updating policies and procedures and evidence-based sports dietetics practice tools in the work site.
X X X
1.10C Develops strategies for quality improvement tailored to the needs of theorganization and patient/client populations, (eg, identifies/adapts evidence-basedpractice guidelines/protocols/tools, skill training/reinforcement, and organizationalincentives and supports)
X X
1.10D Develops and manages sports dietetics education programs in compliance withevidence-based guidelines and national and international guidelines and standards(eg, ADA, Dietitians of Canada, ACSMd, NATA e, IOMf, IOCg)
X X
1.10E Leads the process of developing, monitoring, evaluating, and improvingprotocols, guidelines, and practice tools (eg, ADA, Dietitians of Canada);implements changes as appropriate
X
Figure 3. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e17
Standards of Professional Performance for Registered Dietitians in Sports Dietetics
Standard 2: Application of ResearchThe RD in sports dietetics applies, participates in, or generates research to enhance practice
Rationale: Application, participation, and generation of research promotes improved safety and quality of sports dietetic practice andservices.
Indicators for Standard 2: Application of ResearchThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
2. Each RD:
2.1 Accesses and reviews evidence-based guidelines for application to sports dieteticspractice
X X X
2.1A Demonstrates an understanding of research design and methodology, and use ofthe EALl
X X X
2.1B Demonstrates an understanding of data collection, interpretation of results, and
application
X X X
2.1C Identifies key health and performance questions and uses systematic methods toapply evidence-based guidelines to answer questions
X X
2.1D Utilizes the EAL as a resource in writing or reviewing research papers X X
2.1E Functions as a primary or senior author of research and organizational positionpapers.
X
2.2 Bases practice on significant scientific principles and evidence-based guidelines X X X
2.2A Utilizes the EAL as a resource for evidence-based guidelines X X X
2.2B Follows evidence-based practice guidelines to provide quality care for physicallyactive individuals
X X X
2.2C Follows evidence-based practice guidelines at the specialty level to provide safe,effective, sports dietetics care specific to age, sex, sport, training level, andenvironment
X X
2.2D Follows evidence-based practice guidelines at the advanced practice level (ie,considering the complexity of care for competitive athletes balancing multiplesituations and complications)
X
2.3 Integrates evidence-based guidelines and patient/client values into clinical andmanagerial practice
X X X
2.3A Identifies and utilizes evidence-based policies and procedures for sports dieteticspractice
X X X
2.3B Develops and implements evidence-based policies and procedures for sportsdietetics practice
X X
2.3C Directs the integration of evidence-based policies and procedures into sportsdietetics practice
X
Figure 3. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e19
Indicators for Standard 2: Application of ResearchThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
2.4 Promotes research through alliances and collaboration with food and nutrition andother professionals and organizations
X X X
2.4A Identifies research issues/questions X X X
2.4B Participates as a member/consultant to collaborative research teams thatexamine relationships among nutrition, exercise/athletic performance, and health
X X X
2.4C Serves as an investigator in collaborative research teams that examinerelationships among nutrition, exercise/athletic performance, and health
X X
2.4D Serves as a primary or senior investigator in collaborative research teams thatexamines relationships among nutrition, exercise/athletic performance, and health
X
2.5 Contributes to the development of new knowledge and research in sports dietetics X X X
2.5A Participates in practice-based research under the direction of a collaborativeresearch team
X X X
2.5B Participates in practice-based research networks (eg, ADA’s Dietetics PracticeResearch Network)
X X
2.5C Initiates research related to sports dietetics as the primary investigator or co-investigator with other members of the multidisciplinary research team
X
2.6 Collects measurable data and documents outcomes within practice setting X X X
2.6A Participates in research addressing outcomes of sports dietetics care X X X
2.6B Monitors and evaluates outcome data against expected results X X X
2.6C Uses data as part of a quality improvement process X X X
2.6D Develops systematic processes to collect data and to analyze, interpret, andevaluate outcomes
X X
2.7 Communicates research data and activities through publications and presentations X X X
2.7A Presents evidence-based sports nutrition research to community groups andcolleagues
X X X
2.7B Presents at professional meetings and conferences (local, regional, national,international)
X X
2.7C Authors articles in sports nutrition and related areas X X
2.7D Serves in a leadership role for sports nutrition related publications and programplanning at conferences (local, regional, national, international)
X X
2.7E Translates research findings for incorporation into the development of policies,procedures, and guidelines for sports dietetics practice at national andinternational levels
X
2.7F Directs collation of research data into publications and presentations X
Examples of OutcomesStandard 2: Application of Research● Patient/client receives appropriate services based on the application of evidence-based guidelines and best practices● A foundation for performance measurement and improvement is established● Evidence-based guidelines are used for the development and revision of resources used in practice● Benchmarking and knowledge of best practices is used to evaluate and improve performance
Standards of Professional Performance for Registered Dietitians in Sports Dietetics
Standard 3: Communication and Applications of KnowledgeThe RD in sports dietetics effectively applies knowledge and communicates with others
Rationale: RDs in sports dietetics work with and through others to achieve common goals by effective sharing and application of theirunique knowledge and skills in food, human nutrition, exercise science, and management services.
Indicators for Standard 3: Communication and Application of KnowledgeThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
Each RD:
3.1 Exhibits knowledge related to a particular aspect of the profession of dietetics X X X
3.1A Reads major peer-reviewed publications in sports dietetics and related areas;uses evidence-based guidelines and related resources
X X X
3.1B Demonstrates understanding of current research, trends, and epidemiological surveysin sports dietetics, sports nutrition education, and related areas of exercise science
X X X
3.1C Contributes to the body of knowledge for the profession X X X
3.1D Is familiar with regulatory, accreditation, and reimbursement programs andstandards that apply to sports dietetics care and sports/dietary supplements
X X X
3.1E Operates under regulatory, accreditation, and reimbursement programs andstandards that apply to sports dietetics care, including rules and regulations ofsports organizations and governing bodies (eg, NCAA, NFHS, IOC, USADA, WADA,professional sports) regarding sports/dietary supplements
X X
3.1F Interprets current research in sports dietetics and related areas and applies toprofessional practice as appropriate
X X
3.2 Communicates and applies scientific principles, research, and theory X X X
3.2A Demonstrates critical thinking, reflection, and problem-solving skills at thespecialty level (eg, uses evidence-based guidelines and selects best format forpresentation) in communications
X X
3.2B Demonstrates critical thinking, reflection, and problem-solving skills at theadvanced practice level (eg, uses a comprehensive approach to translateevidence-based guidelines into practical application) in communications
X
3.3 Selects appropriate information and best method or format in communications X X X
3.4 Integrates knowledge of food and human nutrition with knowledge ofexercise/athletic performance, exercise science, health, social sciences,communication, and management theory
X X X
3.4A Applies new scientific knowledge of sports dietetics care into practice X X X
3.4B Integrates new scientific knowledge and the collected knowledge from experience in
sports dietetics care into practice at the specialty level (eg, in new and varied contexts)
X X
3.4C Leads the integration of new scientific knowledge and the collected knowledge fromexperience in sports dietetics care into practice at the advanced practice level (ie, forthe most complex and exceptional problems) or in new research methodologies
X
Figure 3. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e21
Indicators for Standard 3: Communication and Application of KnowledgeThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
3.5 Shares knowledge and information with patients/clients, colleagues, and the public X X X
3.5A Presents to individuals and groups in local communities on topics related tohealth and wellness (eg, health fairs, wellness days)
X X X
3.5B Authors texts and authoritative articles for consumers and for sports- and healthcare professionals
X X
3.5C Serves as invited reviewer, author and/or presenter at local, regional, national,and/or international meetings and to the media
X X
3.5D Serves in leadership role for publications (eg, editor, editorial advisory board),review of textbooks and articles for journal publications; participates on programplanning committees
X X
3.5E Serves as local, regional, national, and international sports dietetics mediaspokesperson
X X
3.5F Functions as an opinion leader within the scope of sports dietetics practice X
3.6 Guides students, interns and patients/clients in the application of knowledge and skills X X X
3.6A Participates as a mentor or preceptor to dietetic students/interns X X X
3.6B Contributes to the education and professional development of dietitians, students,and sports- and health care professionals through formal and informal teaching andmentoring
X X
3.6C Mentors RDs interested in pursuing specialty certification in sports dietetics X X
3.6D Develops educational programs that promote safe, effective sports dietetics care X X
3.6E Develops mentor and preceptor programs in sports dietetics X X
3.7 Seeks current and relevant information related to practice X X X
3.7A Attends professional meetings and obtains continuing education in sports dietetics X X X
3.7B Builds relationships among researchers and decision-makers to influence policydevelopment and to translate evidence-based guidelines into sports dieteticspractice
X X
3.7C Demonstrates the experience and critical thinking skills required to review originalresearch and evidence-based guidelines relevant to sports dietetics practice
X
3.8 Contributes to the development of new knowledge X X X
3.8A Serves on planning committees/task forces to develop continuing education,activities, and programs in nutrition and/or sports dietetics for students andpractitioners
X X X
3.8B Serves as a consultant to organizations (eg, business, industry, government, health,
fitness, exercise/sports, sports dietetics) to address the needs of consumers, sportscare professionals, and health care providers for sports nutrition education
X X
3.8C Uses evidence-based guidelines, best practices, and clinical experience togenerate new knowledge and develop guidelines, programs, and policies inadvanced sports dietetics practice
3.9E Leads in the advancement of technology/informatics (eg, information technologyresearch, software program design) in sports dietetics
X
3.10 Contributes to the multidisciplinary approach by promoting food and nutritionstrategies that enhance exercise/athletic performance, health, and quality of lifeoutcomes of target populations
X X X
3.10A Communicates with the multidisciplinary team regarding nutritional strategies tooptimize exercise/athletic performance and health
X X X
3.10B Communicates with the multidisciplinary team to provide evidence-based guidelinesthat integrates food and nutrition with exercise/athletic performance and health
X X X
3.10C Consults with physicians and other health/sports professionals (eg, physician, physicaltherapist, psychologist, athletic trainer) on clinical and other health-related issues
X X X
3.10D Participates in multidisciplinary collaborations at a systems level (eg,incorporating sports dietetics within programs aimed at optimizingexercise/athletic performance)
X X
3.10E Contributes nutrition-related expertise to national projects and professionalorganizations as needed (eg, ACEm, ACSM, NATA, NCAA, NFHS, NSCA n, IOC,
USADA, WADA)
X
3.11 Establishes credibility as the sports nutrition resource within multidisciplinarysports/athletic, health care, or management teams
X X X
3.11A Educates members of multidisciplinary teams regarding the specializedknowledge and skills of the sports dietitian and the Board Certified Specialist inSports Dietetics
X X
Examples of OutcomesStandard 3: Communication and Application of Knowledge● Expertise in food, nutrition, and management is shared● Individuals and groups:
Receive current and appropriate information Understand information received Know how to obtain additional guidance
Figure 3. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e23
Standards of Professional Performance for Registered Dietitians in Sports Dietetics
Standard 4: Utilization and Management of ResourcesThe RD in sports dietetics uses resources effectively and efficiently
Rationale: Mindful, efficient, and effective management of time, money, facilities, and other resources demonstrates organizationalcitizenship.
Indicators for Standard 4: Utilization and Management of ResourcesThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
Each RD:
4.1 Uses a systematic approach to maintain and manage resources X X X
4.2 Quantifies management of resources in the provision of dietetic services X X X
4.2A Participates in operational planning of food and nutrition programs and services(eg, meals and menu planning, food service consultation, Nutrition Care Process,MNTo, nutrition education, program planning, and development)
X X X
4.2B Manages effective delivery of nutrition programs and services (eg, business andmarketing planning, program administration, Nutrition Care Process, delivery ofeducation programs, materials development) related to sports programs
X X
4.2C Directs or manages business and strategic planning for the design and deliveryof nutrition services in sports-related programs operating in various settings (eg,clinic, cafeteria, corporate, research)
X
4.3 Evaluates safety, effectiveness, and value while planning and delivering servicesand products
X X X
4.3A Participates in evaluations of services and products (eg, surveys, data collection) X X X
4.3B Manages the distribution/delivery of products (eg, food, team meals, sport/dietarysupplements, sports nutrition products) in a cost-effective manner
X X
4.3C Participates in management of budgeted funds for nutrition education services,foodservice, dietary/sports supplements, and sports nutrition products
X X
4.3D Evaluates the following at the systems level: safety, effectiveness, and cost inplanning and delivering nutrition services and products
Indicators for Standard 4: Utilization and Management of ResourcesThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
4.4 Participates in continuous quality improvement and documents outcomes relative toresource management
X X X
4.4A Practices in accordance with the goals and objectives of continuous qualityimprovement
X X X
4.4B Utilizes contemporary business skills relating to budget management, inventorytracking, ordering and distribution, negotiations for compensation and additionalresources
X X
4.4C Anticipates needs, identifies goals and objectives, and engages in long-termstrategic planning
X X
4.4D Anticipates outcomes and consequences of different approaches and makesnecessary modifications to achieve desired outcomes
X X
4.4E Directs the development and management of continuous quality improvementsystems
X
4.5 Assists individuals and groups to identify and secure appropriate and availableresources and services
X X X
4.5A Participates in programs that employ legal and sound business practices andensure goal-oriented outcomes
X X X
4.5B Establishes administratively sound programs (eg, Nutrition Care Processprotocols, MNT service delivery, sports and wellness counseling and education)
X X
4.5C Participates in achieving desired outcomes, securing resources and services, andcollaborating with medical, sports, administrative, and food service staffs
X X
4.5D Directs achieving desired outcomes, securing resources and services, andcollaborating with medical, sports, administrative, and food service staffs
X
Examples of OutcomesStandard 4: Utilization and Management of Resources● Documentation of resource use is consistent with plan● Data are recorded and used to promote and validate services● Desired outcomes are achieved and documented● Resources are effectively and efficiently managed
Figure 3. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e25
Standards of Professional Performance for Registered Dietitians in Sports Dietetics
Standard 5: Quality in PracticeThe RD in sports dietetics systematically evaluates the quality of services and improves practice based on evaluating clinical/dietary and physical performance outcomes
Rationale: Quality practice requires regular performance evaluation and continuous improvement.
Indicators for Standard 5: Quality in PracticeThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
Each RD:
5.1 Knows, understands and complies with federal, state, and local laws andregulations related to sports dietetics and nutrition care
X X X
5.1A Complies with HIPPA p regulations and standards X X X
5.2 Demonstrates understanding of pertinent national quality and safety initiatives (eg,ACSM, IOM, IHIq, NCQAr, NQFs)
X X X
5.3 Implements an Outcomes Management System to evaluate the effectiveness andefficiency of practice
X X X
5.3A Participates in and/or uses collected data as part of a quality improvementprocess relative to outcomes, quality of care, and services rendered
X X X
5.3B Advocates for and participates in developing clinical, operational, and financialdatabases upon which outcomes in sport dietetics care can be derived, reported,and used for improvement
X X
5.3C Directs the development, monitoring, and evaluation of practice-specific benchmarks(eg, appropriate hydration practices, weight management strategies) relevant tonational initiatives (eg, ADA, ACSM, Healthy People 2010, sports organizations andgoverning bodies) and to impact program planning and development
X
5.4 Understands and continuously measures quality of dietetic services in terms ofprocess and outcomes
X X X
5.5 Identifies performance improvement criteria to monitor effectiveness of services X X X
5.6 Designs and tests interventions to improve processes and services X X X
Indicators for Standard 5: Quality in PracticeThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
5.7 Identifies and addresses errors and hazards in dietetic services X X X
5.7A Identifies and addresses errors and potentials hazards as part of the evaluationprocess for quality sports dietetics care
X X X
5.7B Recognizes potential drug-nutrient interactions, drug-sport/dietary supplementinteractions, and potential interactions between scheduled interventions, othertherapies, and exercise training and competition; provides education andcounseling as appropriate
X X X
5.7C Recognizes problematic sports/dietary supplement products and manufacturingpractices, quality control, and error prevention recommendations (eg, as provided byISMPt, FDA u, USPv), and anti-doping rules and regulations of sports organizations andgoverning bodies (eg, NCAA, NFHS, IOC, USADA, WADA; provides education andcounseling as appropriate
X X
5.7D Develops protocols to identify, address, and prevent errors and hazards in thedelivery of sports dietetics services
X
5.8 Identifies expected outcomes X X X
5.9 Documents outcomes X X X
5.10 Compares actual workplace performance to expected outcomes X X X
5.11 Documents action taken when discrepancies exist between actual workplaceperformance and expected outcomes
X X X
5.12 Continuously evaluates and refines services based on measured outcomes related tosports dietetics practice
X X X
5.12A Evaluates and improves professional performance in relation to establishedoutcomes of quality sports dietetics care and services
X X X
5.12B Directs improvements in sports dietetics care and services X X
5.12C Directs the development and management of systems, processes, and programs thatadvance best practices and the core values and objectives of sports dietetics care
X
Examples of OutcomesStandard 5: Quality in Practice● Performance indicators are measured and evaluated● Results of quality improvement activities direct refinement of practice● Outcomes meet pre-established criteria (goals/objectives)
Figure 3. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e27
Standards of Professional Performance for Registered Dietitians in Sports Dietetics
Standard 6: Competence and AccountabilityThe RD in sports dietetics actively engages in lifelong learning
Rationale: Competent and accountable practice includes continuous acquisition of knowledge and skill development.
Indicators for Standard 6: Competence and AccountabilityThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
Each RD:
6.1 Conducts self-assessment at regular intervals X X X
6.1A Engages in self-assessment to ascertain progress in meeting desired performanceoutcomes
X X X
6.1B Evaluates professional practice consistent with evidence-based guidelines, bestpractices, and current research findings
X X X
6.2 Identifies needs for professional development from a variety of sources X X X
6.3 Participates in peer review X X X
6.3A Participates in peer evaluation, including but not limited to peer supervision,clinical chart review, professional practice, and performance evaluations, asapplicable
X X X
6.3B Participates in scholarly review including but not limited to professional articles,chapters, books
X X X
6.3C Serves as reviewer or editorial board associate for professional organizations, journals, and books
X X
6.3D Leads an editorial board for scholarly review including but not limited toprofessional articles, chapters, books
X
6.4 Mentors others X X X
6.4A Participates in mentoring dietetics professionals in sports dietetics practice X X X
6.4B Develops mentoring or internship opportunities for dietetics professionals andmentoring opportunities for sports- and health care professionals, as appropriate
X X
6.4C Directs and implements internships and mentoring programs X
6.5 Develops and implements a plan for professional growth X X X
6.5A Engages in continuing education opportunities in sports nutrition and relatedareas according to his or her professional development plan
X X X
6.5B Develops and implements a professional development plan for specialty practicespecific to employment/workplace setting
X X
6.5C Develops and implements a professional development plan for advanced practicespecific to employment/workplace setting
X
6.6 Documents professional development activities X X X
6.6A Documents, in professional development plan, activities that demonstrateprofessional responsibilities at the generalist level practice
X X X
6.6B Documents, in professional development plan, activities that demonstrate theprofessional responsibilities of specialty practice
X X
6.6C Documents, in professional development plan, activities that demonstrate theexpanded professional responsibilities of advanced practice
Indicators for Standard 6: Competence and AccountabilityThe “X” signifies the indicators forthe level of practice.
Bold Font Indicators are ADA Core RD Standards of Professional Performance Indicators Generalist Specialty Advanced
6.7 Adheres to the ADA Code of Ethics X X X
6.8 Assumes responsibility for actions and behaviors X X X
6.9 Integrates the ADA Standards of Practice and Standards of ProfessionalPerformance into self-assessment and development plans
X X X
6.9A Utilizes the ADA Standards to assess performance at the appropriate level of practice X X X
6.9B Utilizes the ADA Standards to develop and implement a professional developmentplan to enhance practice and performance
X X X
6.9C Utilizes the ADA Standards to develop and implement a professional developmentplan to advance practice and performance to a higher level
X X X
6.10 Integrates evidence-based guidelines into practice X X X
6.10A Reads and utilizes major peer reviewed sports nutrition and related publications X X X
6.10B Demonstrates skills in accessing and critically analyzing research X X X6.10C Uses evidence-based guidelines and best practices to provide quality care X X X
6.10D Serves as a presenter on sports nutrition topics for consumers, sports- andhealth care providers
X X X
6.10E Serves as a presenter for state/national professional organizations; authorssports nutrition and related publications for professionals
X X
6.10F Directs and manages professional meetings, workshops, and conferences X
6.11 Obtains occupational licensure and certifications in accordance with federal, state,and local laws and regulations and work-environment specific policies
X X X
6.11A Attains and maintains certifications accredited by the NCCA w, as appropriate topractice setting
X X X
6.11B Attains and maintains Board Certification as a Specialist in Sports Dietetics, asappropriate to practice setting
X X
6.12 Seeks leadership opportunities X X X
6.12A Exhibits effective interfacing (eg, communication, information gathering, rolemodeling) in sports dietetics practice, research, and/or education
X X X
6.12B Serves on sports nutrition or related committees/task forces (local, regional) forsports- and health care professionals and industry
X X X
6.12C Serves on sports nutrition or related committees/task forces (national,international) for sports- and health care professionals and industry
X X
6.12D Seeks and generates opportunities (local, regional, national, international levels)to integrate sports dietetics practices and programs within larger systems (eg,
ACSM, IOC, NCAA)
X X
6.12E Develops innovative approaches to complex practice issues X
6.12F Manages and directs the integration of sports dietetics principles within largersystems (eg, ACSM, IOC, NCAA)
X
Figure 3. Continued
March 2009 ● Journal of the AMERICAN DIETETIC ASSOCIATION 552.e29
Examples of OutcomesStandard 6: Competence and Accountability● Self-assessments are completed● Development needs are identified● Directed learning is demonstrated● Practice reflects the ADA Code of Ethics●
Practice reflects the ADA Standards of Practice and Standards of Professional Performance● Practice reflects evidence-based guidelines and professional standards● Relevant certifications are obtained and maintained● Commission on Dietetic Registration recertification requirements are met
Definitions
Evidence-based guidelines are determined by scientific evidence or, in the absence of scientific evidence, expert opinion or, in the absenceof expert opinion, professional standardsx.
The Female Athlete Triad refers to the inter-relationships among energy availability, menstrual function and bone mineral density, whichmay have clinical manifestations including eating disorders, functional hypothalamic amenorrhea and osteoporosis.
A multidisciplinary team within athletic performance/sports settings may include any or all of the following: physician, RD, physical
therapist, physiologist, psychologist, athletic trainer, strength and conditioning coach, massage therapist, other coaches.
A multidisciplinary research team within athletic performance/sports settings may include any or all of the following: principal investigator,co-principal investigators, project consultants, lab technicians, statisticians.
aRDregistered dietitian.b ADA American Dietetic Association (www.eatright.org).cSCANSports, Cardiovascular, and Wellness Nutrition (www.scandpg.org).d ACSM American College of Sports Medicine (www.acsm.org).eNATA National Athletic Trainers’ Association (www.nata.org).fIOMInstitute of Medicine (www.iom.edu).gIOCInternational Olympic Committee (www.olympic.org).hNCAA National Collegiate Athletic Association (www.ncaa.org).iNFHSNational Federation of High School Associations (www.nfhs.org). jUSADA US Anti-Doping Agency (www.usantidoping.org).k WADA World Anti-Doping Agency (www.wada-ama.org).
lEALEvidence Analysis Library (www.eatright.org).m ACE American Council on Exercise (www.acefitness.org).nNSCA National Strength and Conditioning Association (www.nsca-lift.org).oMNTmedical nutrition therapy.pHIPPA Health Insurance Portability and Accountability Act of 1996 (http://www.hhs.gov/ocr/hipaa ).qIHIInstitute for Healthcare Improvement (www.ihi.org).rNCQA National Center for Quality Assurance (www.ncqa.org).sNQFNational Quality Forum (www.qualityforum.org).tISMPThe Institute for Safe Medication Practices (www.ismp.org).uFDA Food and Drug Administration (www.fda.gov).vUSPUS Pharmacopeia (www.usp.org).wNCCA National Commission for Certifying Agencies (http://www.noca.org/Resources/NCCAAccreditation/tabid/82/Default.aspx ).xSource: National Committee for Quality Assurance. QI 9: Clinical Practice Guidelines, Element A: Evidence-based guidelines. 2009 Standards and Guidelines for Accreditation of Health
Plans. Washington, DC: National Committee for Quality Assurance; 2009.