18
Adenocarcinoma of Gastroesophageal Junction Joint Hospital Surgical Grand Round 8 th November, 2014 Prepared by Dr. Rain So Kwong Wah Hospital
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | mitchell-barnett |
| View: | 217 times |
| Download: | 1 times |

Adenocarcinoma of Gastroesophageal
Junction
Joint Hospital Surgical Grand Round 8th November, 2014
Prepared by Dr. Rain So
Kwong Wah Hospital
Outline of Presentation
• Definitions • Classification of adenocarcinoma of
OGJ • Surgical approach • Neoadjuvant therapy in locally
advanced disease
Definitions • Gastric cardia
• Zone of the stomach adjacent to the orifice of the tubular esophagus
• OGJ• Endoscopically: The proximal margin of longitudinal
gastric mucosal folds
• Anatomically: At the level of the angle of His
• The squamocolumnar junction (Z-line) • The visible line formed by the juxtaposition of squamous
and columnar epithelia, 3-10mm proximal to OGJ
Classification of OGJ tumour
• Described by Dr. Siewert • OGJ tumor: All tumours that have their center within
5 cm proximal or distal to the anatomical OGJ.• The classification was approved at the consensus
meetings of the 7th International Society of Diseases of the Esophagus in 1995 and the 2nd International Gastric Cancer Congress in Munich 1997

Classification
1cm to 5cm above OGJ
1cm above to 2 cm below OGJ
2cm to 5cm below OGJ

Lymphatic spread
• Later in type I than type II/III• Chronic inflammatory process leads to a
degeneration of lymphatic vessel
• Lymph node involvement• Type I: Upper mediastinum, the tracheal
bifurcation and above. • Type II/III: lower mediastinum, celiac
trunk.
P.M. Schneider (ed.), Adenocarcinoma of the Esophagogastric Junction,Recent Results in Cancer Research 182, DOI: 10.1007/978-3-540-70579-6_2,© Springer-Verlag Berlin Heidelberg 2010
Surgical treatment• Primary Aim: R0 resection
• Complete resection of primary tumour• Type I:
• Intramural spread, multiple satellite tumours• Reported incidence of residual tumour at the
resection margin: 5-35%*
• Adequate lymphadenectomy
Stipa S, Di Giorgio A, Ferri M. Surgical treatment of adenocarcinoma of the cardia.Surgery 1992; 111:386–93.Bozzetti F, Bignami P, Bertario L, Fissi S, Eboli M. Surgical treatment of gastric cancer invading the oesophagus. Eur J Surg Oncol 2000;26: 810–4.

Topic to be discussed• Optimal proximal resection and
surgical approach in esophagectomy for type I
• Surgical approach for Type II/III
• Optimal lymph node dissection in type II/III
Extent of oesophageal resection
• No infiltration was observed in patients whose proximal margin exceeded 7 cm.
• Median survival rate in PPRM 11.1 months Vs NPRM 36.3 months (p<0.02)
• No difference in postoperative mortality and morbidity rates, in anastomotic leakage or recurrence rates.
• Conclusion: 8cm proximal margin is considered to be adequate.
C. Mariette, et al (2003), Extent of oesophageal resection for adenocarcinoma of the oesophagogastric junction, EJSO 2003; 29: 588–593

Type I• Phase III trial in Netherlands (Dutch trial)
• Right thoracic approach Vs Transhiatal esophagectomy in type I
• More pulmonary complications and chylous leakage (57% vs 27%, P<0.001; 10% vs 2%, p=0.002)
• Longer ICU/Hospital stay (6 vs 2 days, p<0.01 and 19 vs 15 days, p<0.001)
• 14% survival benefit in RTA group in Type I patients (51% Vs 37%, p=0.33)
• 5 years locoreginal disease-free survival was better in RTA group (1-8 + nodal mets) (64% Vs 23%, p=0.02)
C. Mariette, et al (2003), Extent of oesophageal resection for adenocarcinoma of the oesophagogastric junction, EJSO 2003; 29: 588–593
Type II/III
• Phase III trial in Japan (JCOG 9502) • Type II/III tumour• Left thoracoabdominal Vs transhiatal extended
total gastrectomy • Total gastrectomy with D2 Lymphadenectomy
(including splenectomy) + para-aortic node dissection (lateral to aorta and above the left renal vein)
• TH: periesophageal lymph node dissection • LTA: mediastinal nodal dissection
Sasako M, et al; Japan Clinical Oncology Group (JCOG9502) (2006) Left thoracoabdominal approach versus abdominal-transhiatal approach for gastric cancer of the cardia or subcardia: a randomised controlled trial. Lancet Oncol 7:644–651
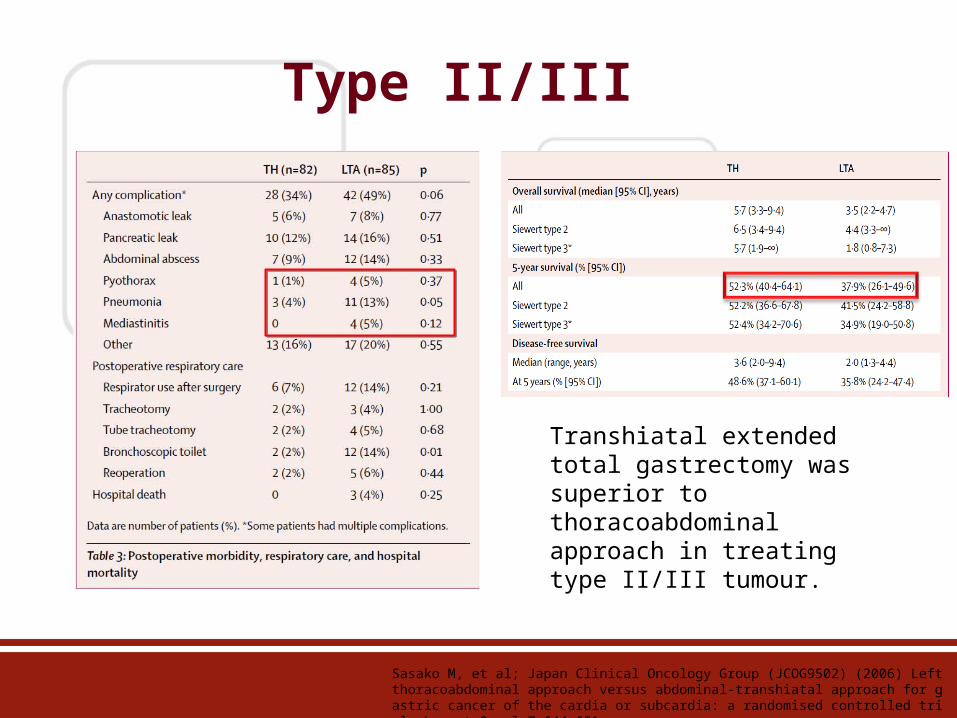
Type II/III
Sasako M, et al; Japan Clinical Oncology Group (JCOG9502) (2006) Left thoracoabdominal approach versus abdominal-transhiatal approach for gastric cancer of the cardia or subcardia: a randomised controlled trial. Lancet Oncol 7:644–651
Transhiatal extended total gastrectomy was superior to thoracoabdominal approach in treating type II/III tumour.
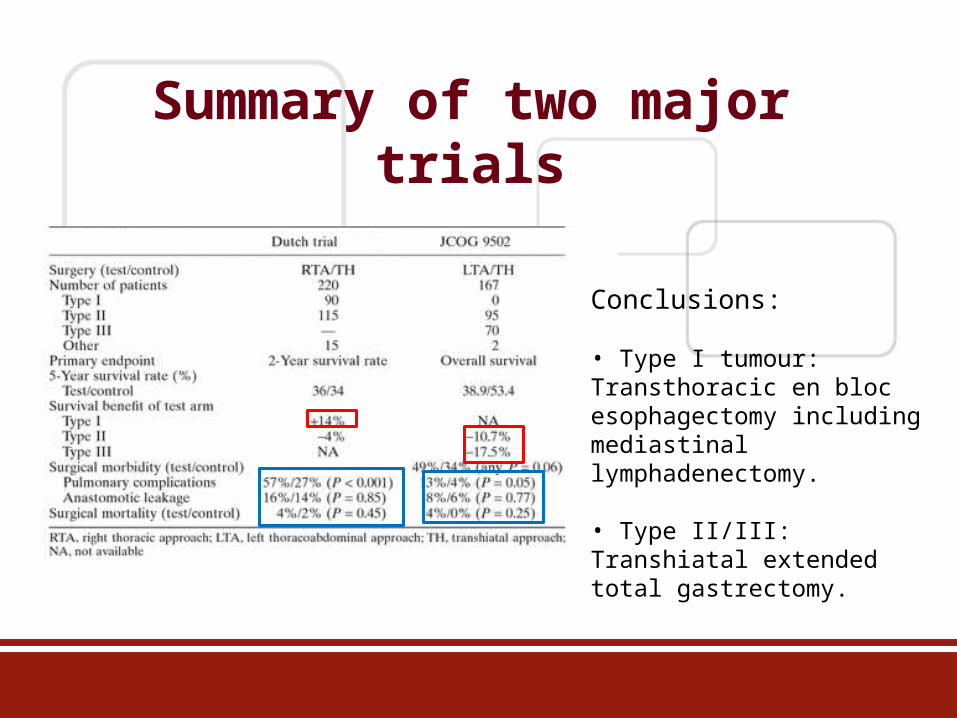
Summary of two major trials
Conclusions:
• Type I tumour: Transthoracic en bloc esophagectomy including mediastinal lymphadenectomy.
• Type II/III: Transhiatal extended total gastrectomy.

Type II/III
• IEBLD=index of estimated benefit of LN dissection•Frequency (+LNmet) x 5-year survival rate of pts with +LNs
• Type II: IEBLD =0 in distal perigastric LNs Proximal gastrectomy can be a feasible option for type II tumour
• Type III: IEBLD =2.6-3.8 in 4b, 4d, 5 Total gastrectomy
Difference in lymph node dissection?
H Goto et al, The optimal extent of lymph node dissection for adenocarcinoma of the oesophagogastric junction differs between siewert tyoe II and siewert type III patient, Gastric cancer, DOI 10.1007/S10120-014-0364-0
Locally advanced tumour
• T3/4, node-positive disease• Failure of surgery to obtain locoregional control
and early systemic dissemination of disease• 5-year survival after potentially curative
resection is only up to 20%
Hulscher JBF, van Sandick JW, de Boer AGEM, et al.: Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med 2002, 347:1662–1669. Kelsen DP, Ginsberg R, Pajak TF, et al.: Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med 1998, 339:1979–1984.
How about neoadjuvant therapy?
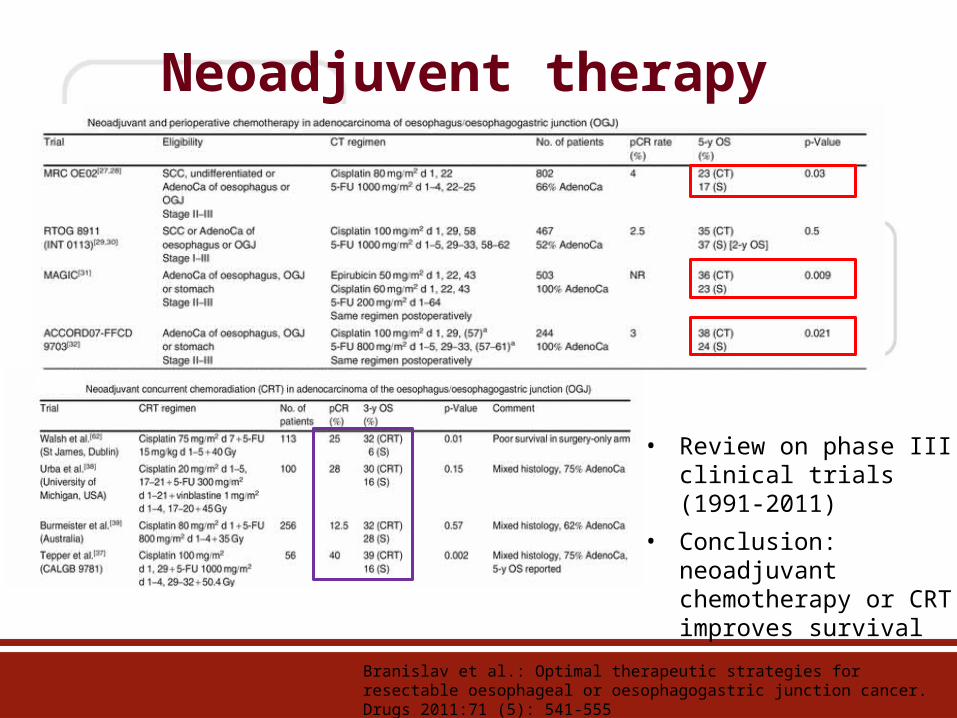
Neoadjuvent therapy
Branislav et al.: Optimal therapeutic strategies for resectable oesophageal or oesophagogastric junction cancer. Drugs 2011:71 (5): 541-555
• Review on phase III clinical trials (1991-2011)
• Conclusion: neoadjuvant chemotherapy or CRT improves survival
Summary• Siewert classification of OGJ tumour bears a good
correlation with lymphatic spread.
• Type I: Transthoracic en bloc esophagectomy including mediastinal lymphadenectomy.
• Type II/III: Transhiatal extended total gastrectomy.
• Proximal gastrectomy can be a feasible option for Type II.
• Results of neoadjuvant therapy in managing locally advanced cancer is promising and shown to improve survival.

~END~
All questions are welcome

















