60
Adjuvant systemic therapy Breast cancer
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | cbcfbcyukon |
| View: | 397 times |
| Download: | 1 times |

Adjuvant systemic therapy Breast cancer
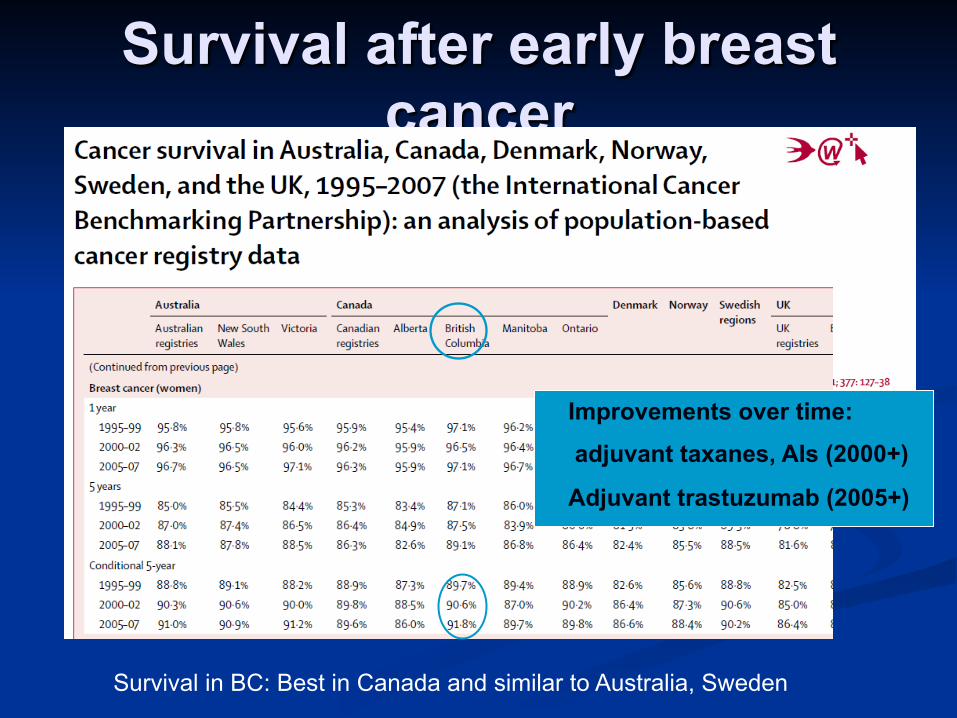
Survival after early breast cancer
Survival in BC: Best in Canada and similar to Australia, Sweden
Improvements over time:
adjuvant taxanes, AIs (2000+)
Adjuvant trastuzumab (2005+)
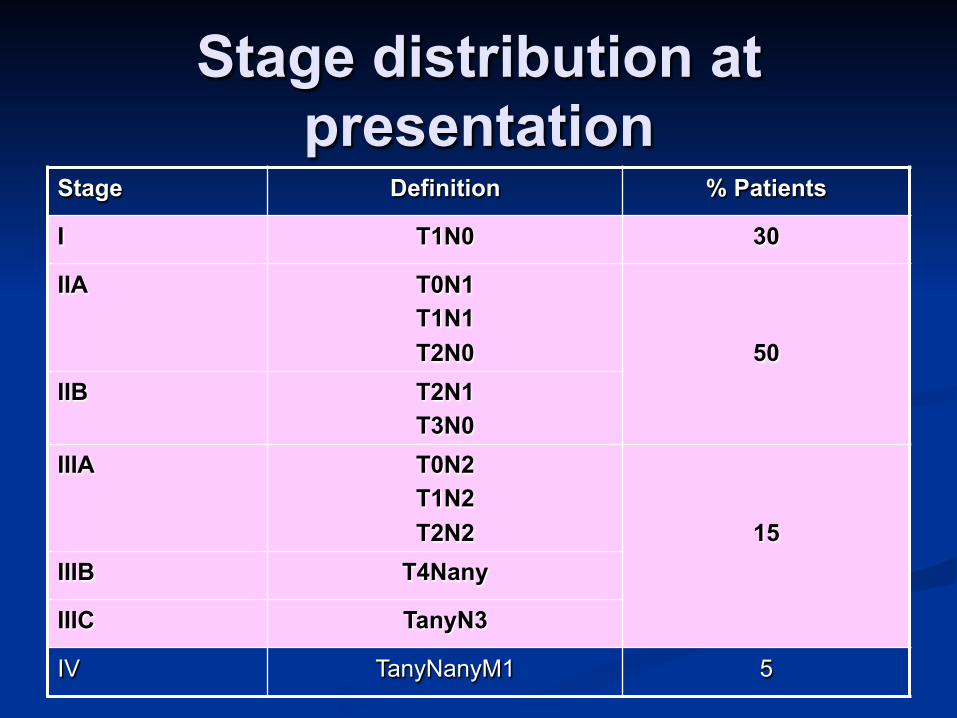
Stage distribution at presentation
Stage Definition % Patients
I T1N0 30
IIA T0N1 T1N1 T2N0
50 IIB T2N1
T3N0 IIIA T0N2
T1N2 T2N2
15 IIIB T4Nany
IIIC TanyN3
IV TanyNanyM1 5

Early BC treatment pples
Surgery: PM, M, AXND, SNB Radiation: Breast, loco-reg, chest wall Hormone Rx: what, how long, who Chemotherapy: what, how much, who Anti-HER2 therapy: who, how long

Local Therapy SURGERY
Breast: Partial mastectomy Mastectomy
Axilla: Sentinel node biopsy
Most cases
Axillary dissection May follow sentinel bx In clinically positive
nodes
RADIATION Breast:
After partial mastectomy
After mastectomy if Positive surgical
margins Lymphatic invasion If positive nodes
Nodes: if contain cancer Axilla, supraclavicular,
internal mammary

Systemic Therapy
Choice of treatment is based on Hormone therapy: expression of ER, PR Chemotherapy: absolute recurrence risk,
age, co-morbidity Anti-HER2 therapy: HER2 positivity,
indications for chemotherapy, adequate cardiac function
How to Assess risk and treatment benefit
Traditional: T, N, grade, ER, HER2, LVI
Enhanced pathology: Adjuvant! On line (adds age, co-morbidity, effect of adjuvant intervention)
Other prognostic tools: Oncotype Dx, mammaprint, PAM50, etc
The old paradigm High risk: chemo
Young Node positive Big cancer High grade ER – HER2+
Low risk: no chemo Older Node negative Small cancer Low grade ER+
The new paradigm
Size doesn’t matter Nodal status may or may not matter Phenotype (ER, PR, HER2) and biology
matter
These apply not only to natural history but to responsiveness to treatment
Prognostic/Predictive variables
Lower risk Older (menopausal) Small T NN Grade 1,2 ER 2-3+ Her2 negative
Higher risk Younger
(premenopausal) Larger T Node positive Grade 3 ER 1+ or ER negative Her2 positive LVI
Premenopausal ER+ breast cancer
38y premenopausal woman post partial mastectomy for 1.8cm, grade 3, ER 2+, PR-, HER2-, node negative ductal cancer with lymphatic invasion (LVI).
Hormone therapy: if ER and/or PR positive Chemotherapy: determined by recurrence risk Clinical predictors for recurrence: grade, LVI, young
age Clinical predictors for benefit from treatment: ER
(hormone therapy); ?age, grade (chemo)

Menopausal case: 68y menopausal woman post mastectomy for 2.7cm,
grade 1, ER3+, PR 3+, HER2-, 1 node positive ductal carcinoma.
Co-morbidities HTN, diabetes, high cholesterol, overweight
Medications: ramipril; metformin; lipitor
Grade, strong ER/PR, and node negative predict for low recurrence
Grade, strong ER/PR, age predict for low benefit from chemo
Age, comorbidities predict for lack of survival benefit from chemo
Molecular subtypes Luminal A: ER+, low Ki67, her2- Luminal B: ER+, high Ki67, her2- Normal: ER+, Her2+ Her2+: ER-, PgR- Basal: triple negative, EGFR+ Different gene exp’n, natural hx and response to Rx. Basal are chemo sensitive but have worst OS. Her2+ also have poor Px high prolif index (influence of Herceptin)
Tools to help us PROGNOSTIC, (estimate risk): clinical
experience; adjuvant online; Oncotype Dx Recurrence Score; intrinsic subtype (luminal A vs B); Mammaprint; UPA, PAI-1
PREDICTIVE, (estimate benefit): clinical experience; clinical trials; adjuvant online; Oncotype Dx; PEPI score (neoadjuvant hormone therapy)

Adjuvant online
Limitations:
• Her2 and LVI not adequately accounted for
• Less accurate for very small cancers, and for
very young pts

Microarray gene exp: Oncotype DX
21 gene expression panel (RNA expression using RT-PCR: 16 cancer genes, 5 reference genes NSABP B14: ER+, node
negative postmenopausal women with TAM
NSABP B20: ER+ node negative with TAM or CMF and TAM
INT100: ER+ postmenopausal node positive with TAM or TAM/CAF
Other markers: MammaPrint; uPA, PAI-1

Oncotype Dx Tissue based assay to assess risk in HR+ node
negative BC
Retrospective analyses suggest that for a low and intermediate score, there is NO additional benefit from chemotherapy
Oncotype Dx
Recurrence score (RS) depends heavily on ER and proliferation markers (grade and degree of ER positivity are the poor man’s Oncotype Dx)
Generally weak ER+ cancers and higher grade cancers will have a higher RS
<5% of grade 1 cancers will have high RS and 10% of grade 3 cancers will have a low RS
Not yet validated for NP premenopausal BC
Useful for clinically intermediate risk ER+, NN cancers as decision aid for chemo vs not

Hormone therapy

Hormone therapy options Premenopausal
Tamoxifen 5 years 10 years Switch to AI at 5y for
another 5y (menopausal)
Ovarian ablation + tam Ovarian ablation +
Aromatase Inhibitor (AI)
Menopausal Early switch AI x 5 years Tam x 5 years
Stop at 5 years Continue to 10 years Switch to AI at 5 years
for another 5 years
“Switch”: tamoxifen for 2-3 years followed by AI for balance of 5 years

Tamoxifen (T): mechanism of action
, cells die
located in cell nucleus
Effective in premenopausal and postmenopausal women with ER+ BC
Role in primary prevention; adjuvant therapy; metastatic disease
Partial agonist effects: bone; endometrium; CVS
T
Estrogen can’t bind
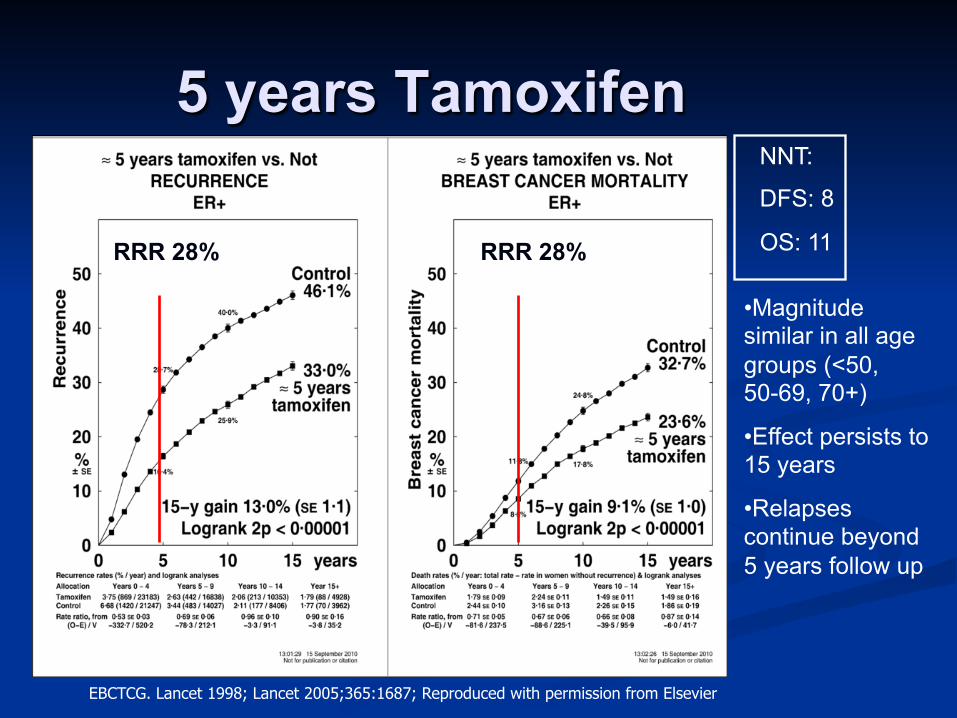
5 years Tamoxifen
EBCTCG. Lancet 1998; Lancet 2005;365:1687; Reproduced with permission from Elsevier
NNT:
DFS: 8
OS: 11
• Magnitude similar in all age groups (<50, 50-69, 70+)
• Effect persists to 15 years
• Relapses continue beyond 5 years follow up
RRR 28% RRR 28%
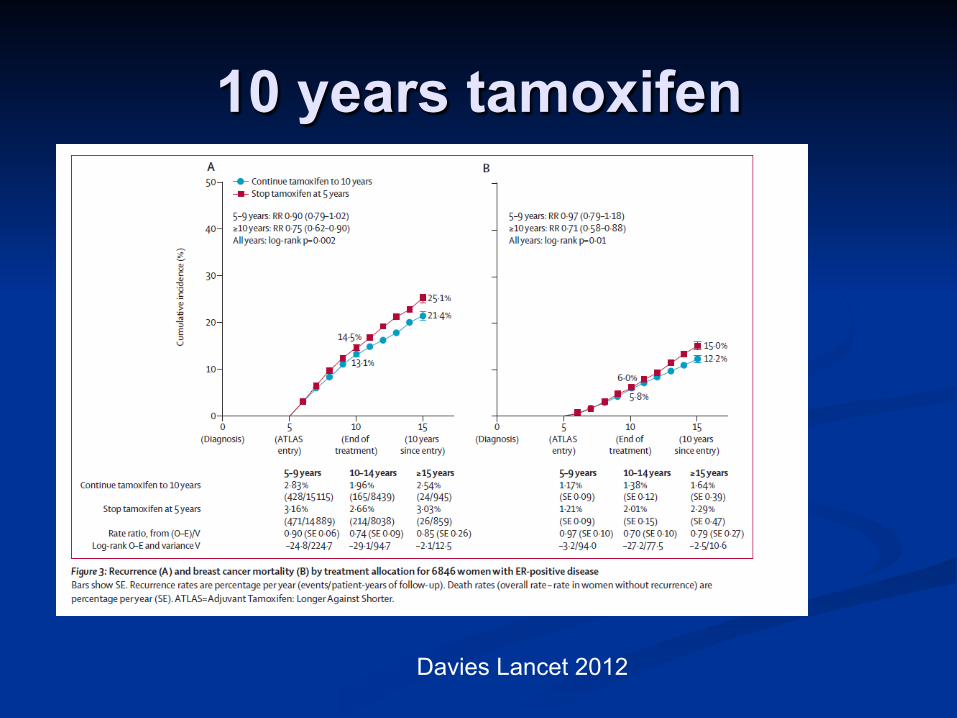
10 years tamoxifen
Davies Lancet 2012
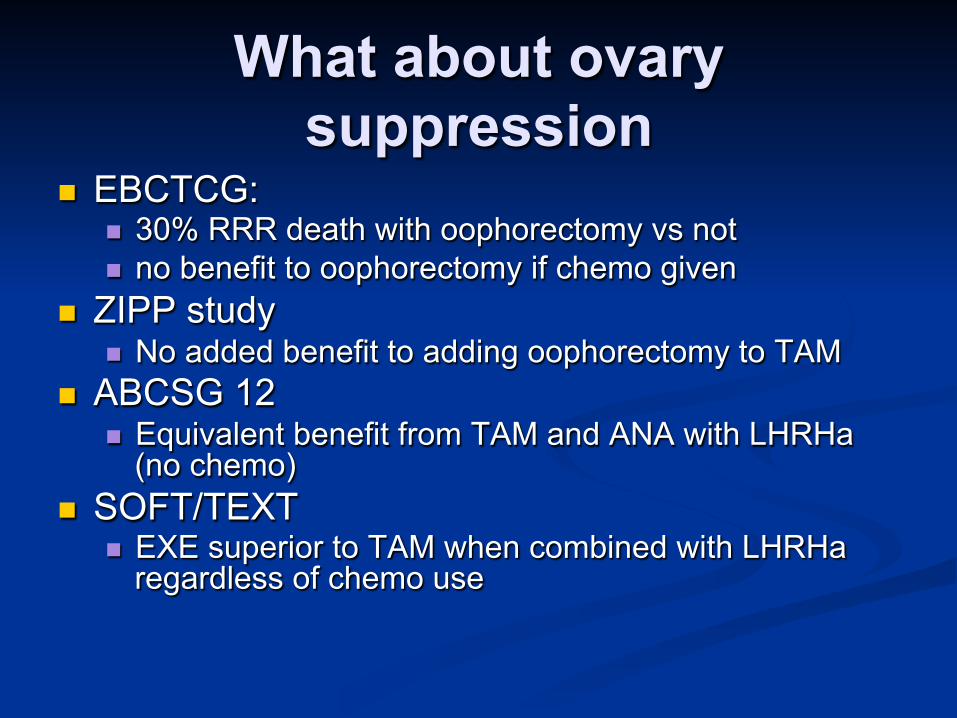
What about ovary suppression
EBCTCG: 30% RRR death with oophorectomy vs not no benefit to oophorectomy if chemo given
ZIPP study No added benefit to adding oophorectomy to TAM
ABCSG 12 Equivalent benefit from TAM and ANA with LHRHa
(no chemo) SOFT/TEXT
EXE superior to TAM when combined with LHRHa regardless of chemo use

Nuances…
If TAMOXIFEN x5y is the standard: Are tam and OA the same? Are two hormone therapies better than one? What about when there are contraindications
or harm from tamoxifen VTE Endometrial cancer Depression
Contribution of bisphosphonates to hormone therapy?
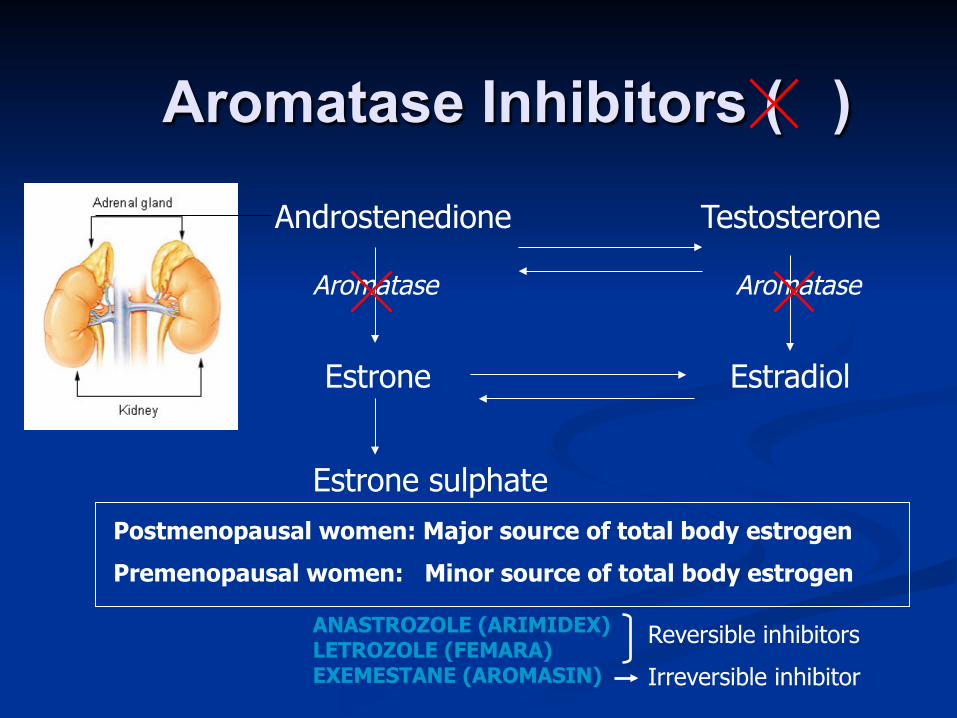
Aromatase Inhibitors ( )
Androstenedione Testosterone
Estrone Estradiol
Aromatase Aromatase
Estrone sulphate Postmenopausal women: Major source of total body estrogen
Premenopausal women: Minor source of total body estrogen
ANASTROZOLE (ARIMIDEX) LETROZOLE (FEMARA) EXEMESTANE (AROMASIN)
Reversible inhibitors
Irreversible inhibitor

Adjuvant AI meta-analysis
Compared with 5 years of tamoxifen: 3% improvement in DFS with AI x5y
1.1% NON-significant difference in BC-mortality
3% improvement in DFS with switch 0.7% improvement in BC-mortality
Dowset, JCO 2010
DFS = relapse, new CLBC, death from any cause
NNT = 33 (SWITCH or AI 5y instead of 5y TAM) NNT = 6 (SWITCH or AI 5y instead of No hormone therapy)
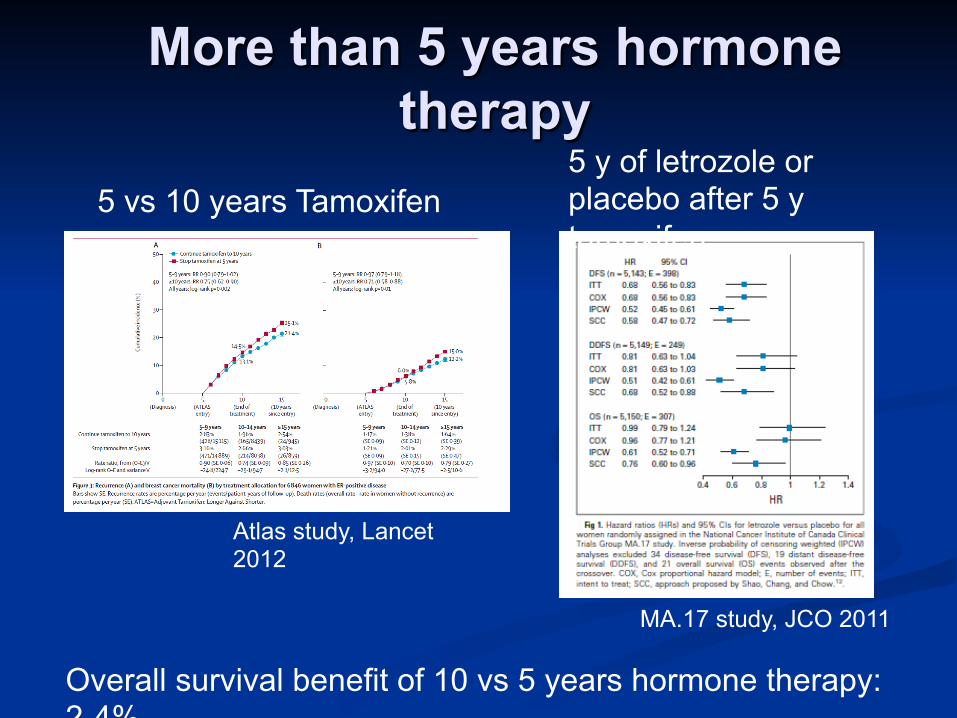
More than 5 years hormone therapy
5 vs 10 years Tamoxifen 5 y of letrozole or placebo after 5 y tamoxifen
Overall survival benefit of 10 vs 5 years hormone therapy: 2-4%
Atlas study, Lancet 2012
MA.17 study, JCO 2011

Extended Adjuvant: MA17
RESULTS DFS HR 95% CI or p value
OS HR
95% CI or p value
ALL* 60m 30m
0.68 0.58
P<0.00005 P<0.0004
0.88 0.82
P0.37 P0.3
Node Neg 0.45 (0.27-0.75) NS _
Node Pos
0.61 (0.45-0.84) 0.61 (0.38-0.98)
*Absolute difference in DFS 6%
Chemotherapy

Premenopausal ER+ breast cancer
38y premenopausal woman post partial mastectomy for 1.8cm, grade 3, ER 2+, PR-, her2-, LVI positive, NN ductal cancer
Chemotherapy: determined by recurrence risk Hormone therapy: if ER and/or PR positive Clinical predictors for recurrence: grade, LVI, young
age Clinical predictors for benefit from treatment: ER
(hormone therapy); ?age, grade (chemo)

Menopausal case: 68y menopausal woman post mastectomy for 2.7cm,
grade 2, ER3+, PR 3+, her2-, NN ductal carcinoma.
Co-morbidities HTN, NIDDM, high cholesterol, overweight
Medications: ramipril; metformin; lipitor
Grade, strong ER/PR, and node negative predict for low recurrence
Grade, strong ER/PR, age predict for low benefit from chemo
Age, comorbidities predict for lack of survival benefit from chemo

Consider chemo
~Always Triple negative (ER,
PR, HER2 negative) HER2+ Grade 3 <45y and T2+ >3 nodes positive
~Usually Weak ER positive Young and 1-3 node
pos Older, healthy, and 1-3
node pos and other worry (high grade, weak ER, LVI…)
Anti HER2 therapy HER2+ breast cancer: more aggressive, high
recurrence rates, very sensitive to chemo/antiHER2 antibodies
Normal cardiac function: small incidence of cardiac injury, often reversible
Chemotherapy planned: trivial benefit without chemo
Standard of care: 1 year of trastuzumab Future standard of care:
Low risk: 3 months chemo, 1 year trastuzumab Intermediate risk: 6 months chemo, 1 year
trastuzumab High risk: 6 months chemo, 1 year trastuzumab,
pertuzumab
Chemotherapy timing
Adjuvant = neoadjuvant Neoadjuvant advantages
Local downstaging (locally advanced) Tests in vivo sensitivity
Chemotherapy primer
Anthracycline based: AC, FEC, FAC BRAJAC; BRAJFEC; BRAJFAC
Anthracycline free: DC, CMF, TCH BRAJDC; BRAJCMF; BRAJDCARBT
Anthracycline + taxane: (AC-T), ddAC-T, AC-D, AC-wT, FEC-D (BRAJACT); BRAJACTG; BRAJACTW;
BRLAACD; BRAJFECD

Node negative DC or AC or FEC
ER+ Older (>65) Her2 negative grade 3 but T1 Cardiac risk (DC) LVI
Anthracycline + Taxane Triple negative Younger Her2 positive Grade 3 but T2+ LVI

Node positive Anthracycline-taxane
BRAJACT-G (needs GCSF) and BRAJACTW (no GCSF) have the lowest toxicity coupled with best efficacy
BRAJACT (q3weeks) is antiquated (lower efficacy) but often given in her2+ so trastuzumab can be conveniently added to every 3 weeks
BRAJFEC-D is an option, but D (docetaxel) has high haem toxicity and needs G-CSF
BRLAACD typically used for locally advanced (stage III) due to higher heam toxicity with D.

Node positive Coverage for GCSF
BRAJACT-G (q2w) BRAJFECD BRLAACD
No coverage for GCSF BRAJACTW (q1w T) BRAJACTT (if her2+) BRAJDCARBT (if
her2+ and cardiac worry)

Anti-her2 therapy
12 months trastuzumab standard of care Finher Phare
Addition of pertuzumab or lapatinib increases pCR in neoadjuvant therapy Pertuzumab/trastuzumab/chemo approved in
neoadjuvant therapy in US based on neosphere and gepartquinto studies
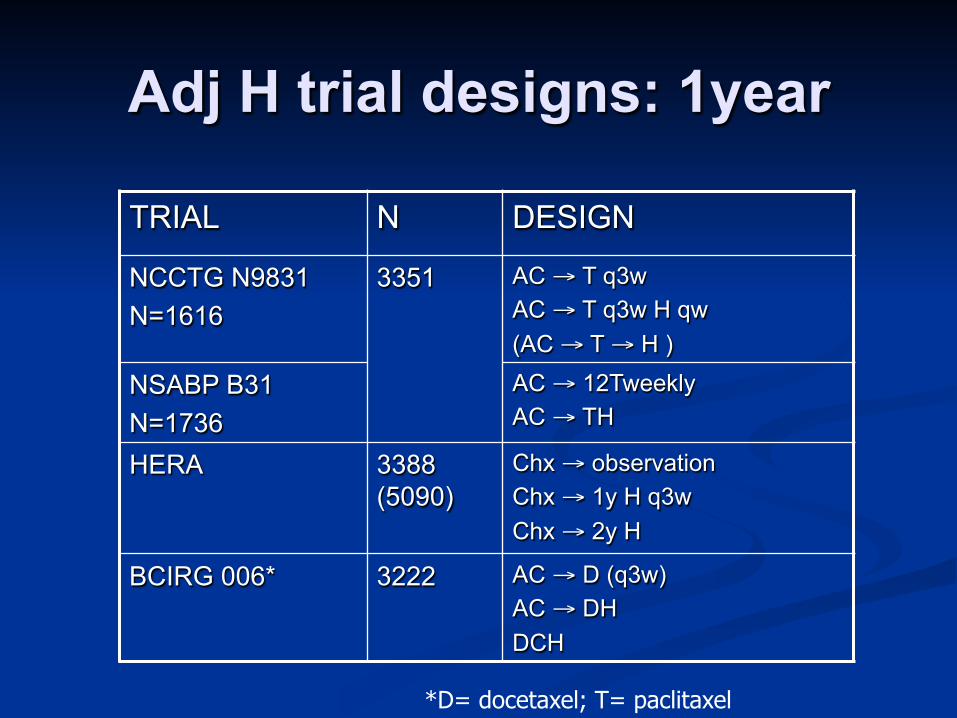
Adj H trial designs: 1year
TRIAL N DESIGN
NCCTG N9831 N=1616
3351
AC → T q3w AC → T q3w H qw (AC → T → H )
NSABP B31 N=1736
AC → 12Tweekly AC → TH
HERA 3388 (5090)
Chx → observation Chx → 1y H q3w Chx → 2y H
BCIRG 006* 3222 AC → D (q3w) AC → DH DCH
*D= docetaxel; T= paclitaxel
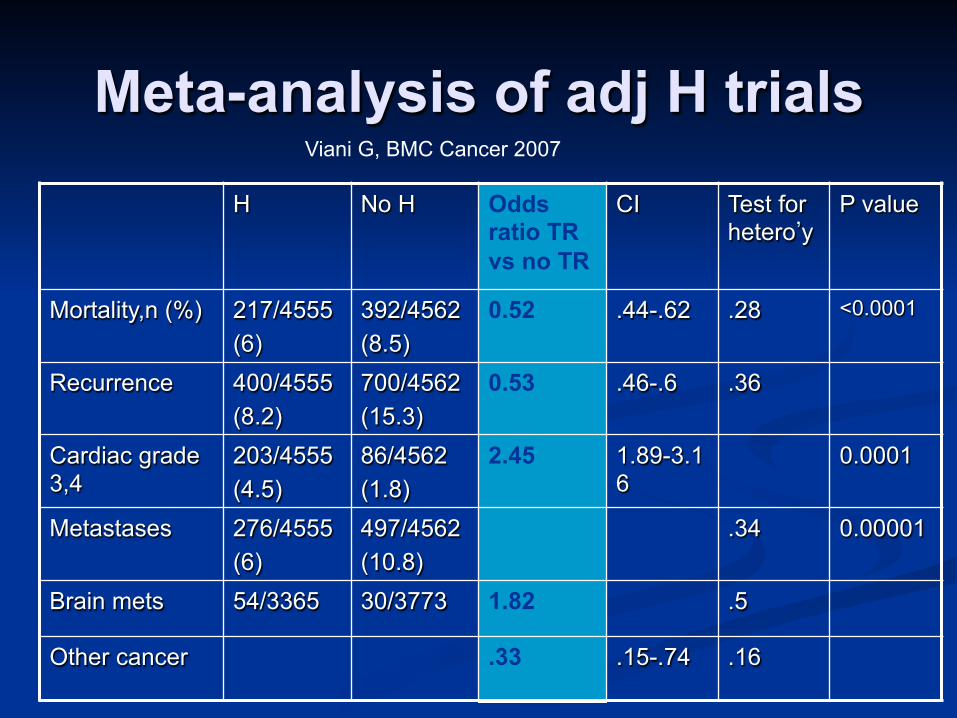
Meta-analysis of adj H trials H No H Odds
ratio TR vs no TR
CI Test for hetero’y
P value
Mortality,n (%) 217/4555 (6)
392/4562 (8.5)
0.52 .44-.62 .28 <0.0001
Recurrence 400/4555 (8.2)
700/4562 (15.3)
0.53 .46-.6 .36
Cardiac grade 3,4
203/4555 (4.5)
86/4562 (1.8)
2.45 1.89-3.16
0.0001
Metastases 276/4555 (6)
497/4562 (10.8)
.34 0.00001
Brain mets 54/3365 30/3773 1.82 .5
Other cancer .33 .15-.74 .16
Viani G, BMC Cancer 2007
When to start chemo
Wound healed, no ongoing infection 3-10 weeks post surgery is ideal Reduced benefit if >12 weeks from
surgery Can defer re-excision of margins,
completion axillary dissection until post chemo if high risk and result will not influence chemo choice

Venous Access Typically we avoid the affected arm Practically, for those with Sentinel node
biopsy, lymphedema risk is only 1-2%, so can use both arms
Consider port for multiple iv start regimens Weekly chemo: 16 IV starts over 6 months HER2+: 21 IV starts over 15 months Anyone with needle phobia or poor venous access
Epirubicin can sclerose veins; doxorubicin, cyclophopshamide, and taxanes typically do not
Chemotherapy Side Effects
Educate pts What to expect When to expect onset, peak, resolution When and who to call

Hair Loss Alopecia: all adjuvant chemo regimens for BC
Starts about 2 weeks after first dose Scalp: ~ 100% Eyelashes, eyebrows, body hair: Variable but frequent Most Extended Health Benefits will reimburse wig
Pt needs a signed prescription “for chemo induced alopecia” Prevention: ice cap and tourniquet
Used in Europe; impractical for infusions >1h (paclitaxel)
Regrowth: 6-8 months to a short crop No regrowth: subtotal alopecia in 3% of docetaxel
treated pts

Nausea and Vomiting Anthracyclines, iv cyclophosphamide, carboplatin Acute phase peaks and recedes within 3 days Often worse in younger pts, pts who have had
morning sickness, are prone to motion sickness Ondansetron, dexamethasone pre and post dose Nausea, vomiting despite premeds:
Ongoing: IV hydration and anti-emetics if needed Next cycle:
add Aprepitant (EMEND) 125mg pre, 80mg day 2, day 3 Ondansetron, dexamethasone IV, +/- ativan
Late nausea: >3 days Is it heartburn, malaise, constipation, intercurrent illness? Breakthrough meds: metoclopramide, prochlorperazine Continue dexamethasone 1-2 days longer
Heamatologic effects Heamatologic
WBC and neutrophils: Counts drop with all regimens Least impact with weekly dosing (paclitaxel) Highest impact with docetaxel Pt to be assessed for febrile neutropenia if T>38 Celcius
Hemoglobin Modest drops with anthracyclines, taxanes Can contribute to fatigue Transfusion rarely needed
Platelets Carboplatin Trastuzumab (rare) Concurrent G-CSF
G-CSF; dose reduction; delay
Replace iron if needed, monitor
Delay; dose reduce; monitor

Peripheral Neuropathy Numbness, tingling (+/-painful):
sensory (glove, stocking) and motor Cumulative dose related Taxanes, carboplatin
Paclitaxel worse than docetaxel Weekly worse than q3w or q2w dosing Often worse for several months after chemo ends Small % permanent
Monitor for function loss, or pain Dose reduce; stop; gabapentin
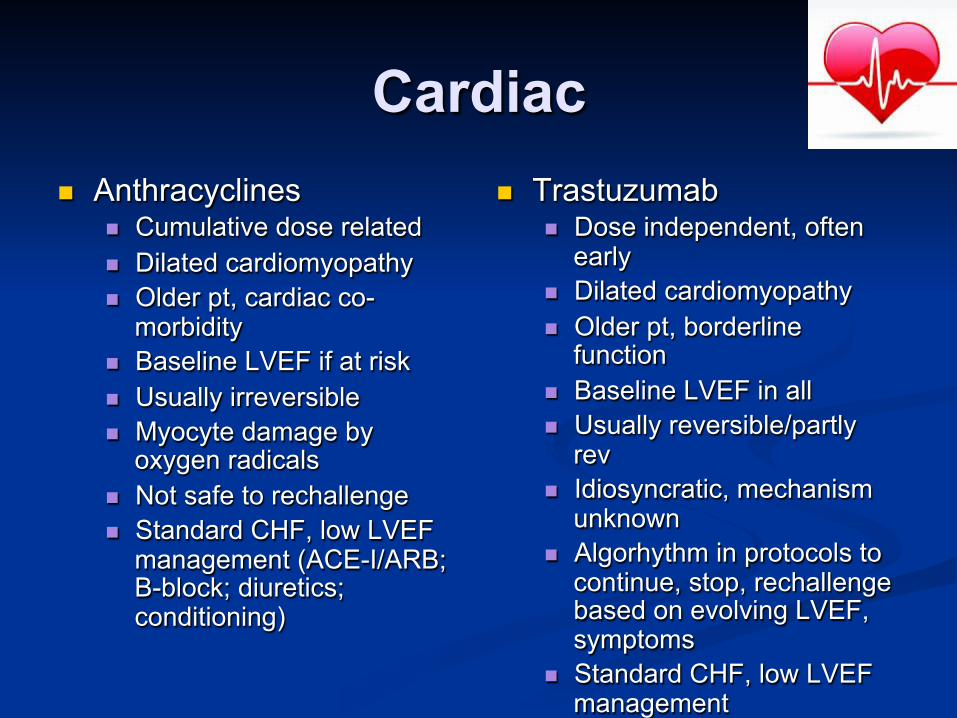
Cardiac Anthracyclines
Cumulative dose related Dilated cardiomyopathy Older pt, cardiac co-
morbidity Baseline LVEF if at risk Usually irreversible Myocyte damage by
oxygen radicals Not safe to rechallenge Standard CHF, low LVEF
management (ACE-I/ARB; B-block; diuretics; conditioning)
Trastuzumab Dose independent, often
early Dilated cardiomyopathy Older pt, borderline
function Baseline LVEF in all Usually reversible/partly
rev Idiosyncratic, mechanism
unknown Algorhythm in protocols to
continue, stop, rechallenge based on evolving LVEF, symptoms
Standard CHF, low LVEF management

Mucositis (mouth sores)
All drugs, worst with anthracyclines, cyclophosphamide
Any pt can get mouth sores Generally confined to mouth, but can get sore
throat Prophylactic baking soda mouth rinse bid Magic mouthwash Thrush overgrowth uncommon Lower incidence in pts on G-CSF
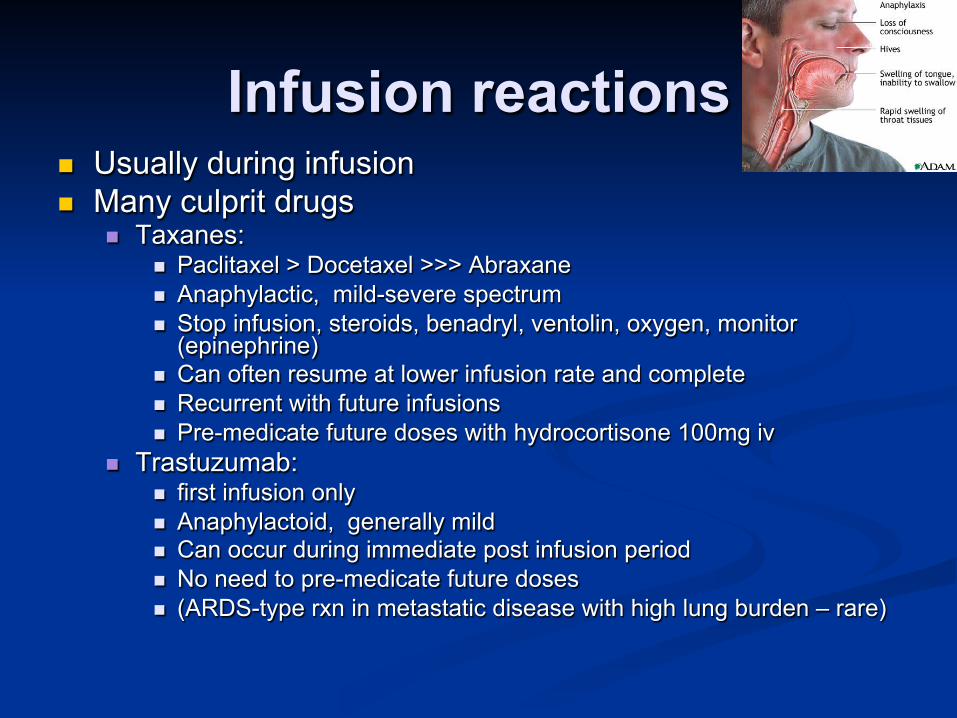
Infusion reactions Usually during infusion Many culprit drugs
Taxanes: Paclitaxel > Docetaxel >>> Abraxane Anaphylactic, mild-severe spectrum Stop infusion, steroids, benadryl, ventolin, oxygen, monitor
(epinephrine) Can often resume at lower infusion rate and complete Recurrent with future infusions Pre-medicate future doses with hydrocortisone 100mg iv
Trastuzumab: first infusion only Anaphylactoid, generally mild Can occur during immediate post infusion period No need to pre-medicate future doses (ARDS-type rxn in metastatic disease with high lung burden – rare)
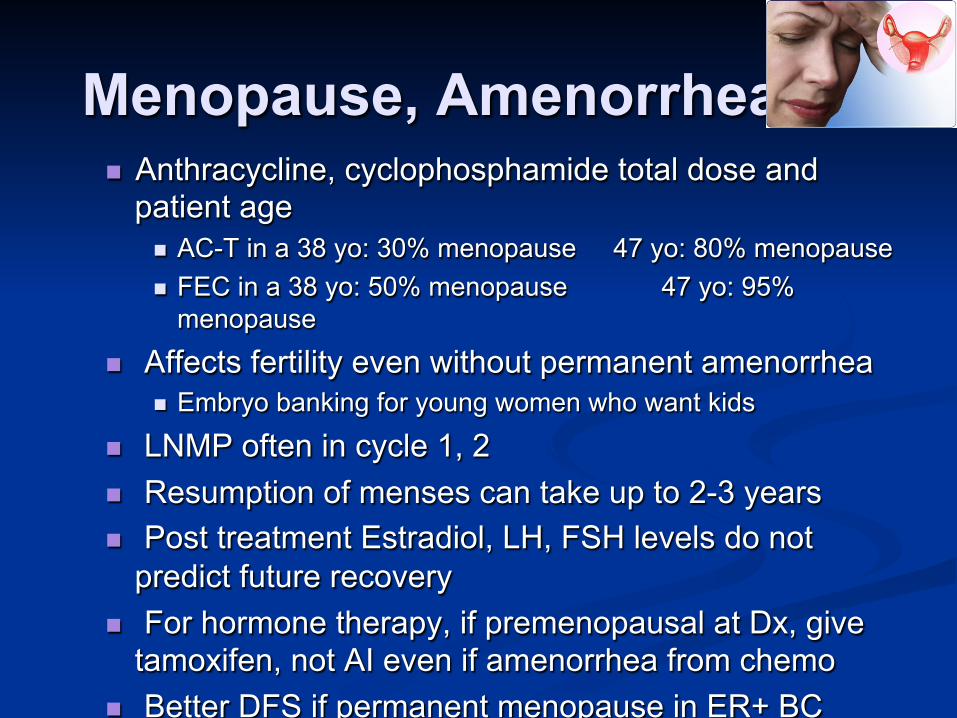
Menopause, Amenorrhea Anthracycline, cyclophosphamide total dose and
patient age AC-T in a 38 yo: 30% menopause 47 yo: 80% menopause FEC in a 38 yo: 50% menopause 47 yo: 95%
menopause
Affects fertility even without permanent amenorrhea Embryo banking for young women who want kids
LNMP often in cycle 1, 2 Resumption of menses can take up to 2-3 years Post treatment Estradiol, LH, FSH levels do not
predict future recovery For hormone therapy, if premenopausal at Dx, give
tamoxifen, not AI even if amenorrhea from chemo Better DFS if permanent menopause in ER+ BC
Chemo Brain Mechanism not well understood Not predictable by patient or regimen Multifactorial:
Menopause Fatigue Depression, worry, anxiety, pre-occupation Poor sleep Chemo
multi-tasking, short-term memory, concentration fatigue, processing speed
Variable resolution, frequently persistent

Nail Changes
Fingers/toes All drugs but worst with docetaxel, paclitaxel. Dark lines, splitting, lifting, oozing, loosing,
ridges Frozen gloves with docetaxel very effective Soak in warm salt water if oozing Changes resolve slowly (months)

Myalgias, Arthralgias During chemo:
Taxanes: paclitaxel q3w > weekly > docetaxel Days 3-7 Gapabentin; tylenol; opioids recurrent
G-CSF: usually lessens with subsequent dosing After chemo:
Aromatase inhibitor Rule out unmasked arthritis Autoimmune / rheumatoid type multi-joint pain
Infrequent ?3% Occasionally severe enough to need steroids Usually resolves gradually with no permanent changes to
joints
Taste and Weight Weight gain common:
Steroids Menopausal changes Change in routine (not working, less exercise, comfort
eating) Depression, anxiety alter metabolism Hormone therapy may alter metabolism
Taste: temporary “food tastes metallic” “everything is sweet” “things taste like wood” “my mouth is so dry I can’t swallow”

Work and Chemo
Is it safe to work? No significant risk to self, co-workers, family
Is it sensible to work? Multiple appointments Transient side effects at different times, cumulative Emotional roller coaster Decreased physical and mental stamina
When is return to work reasonable? 3-6 months post chemo or radiation (whichever is last) When hormone therapy side effects adjusted to Graduated hours return is optimal Some have lasting fatigue and cannot return to former work level

Summary Majority of women in BC have early stage
and highly curable breast cancer Treatment is multi-disciplinary (surgery,
radiation, hormone, chemo, antiHER2) A few side effects are permanent or long
lasting, most are temporary Women need support through treatment
(anxiety, menopausal symptoms, body image, depression, loss of control)

Questions?

















