Page 1
Using evidence to develop services for children and families:some considerations and challenges for the Child & Family
Support Agency
Item type Article
Authors McKeown, Kieran
Publisher Journal of the Institute of Public Administration
Journal Journal of the Institute of Public Administration
Downloaded 17-May-2018 02:40:30
Link to item http://hdl.handle.net/10147/292543
Find this and similar works at - http://www.lenus.ie/hse
Page 2
Administration:
Journal of the Institute of Public Administration,
Volume 61, No 1, April 2013
Using Evidence to Develop Services for Children and Families:
Some Considerations and Challenges for the Child & Family Support Agency
by
Kieran McKeown, Social & Economic Research Consultant, Dublin
www.kieranmckeown.ie
ABSTRACT
The Child and Family Support Agency will be established by the Department of Children and
Youth Affairs in 2013. This is a significant undertaking and an opportunity to design and
deliver services for children and families that are ‘evidence-informed’ and ‘outcome-
focused’. This article summarises and reflects on six types of evidence that could contribute
to making services for children and families more effective thereby increasing the likelihood
of improved outcomes. Specifically, it suggests six types of evidence could add value to the
work of the new agency: evidence on matching needs to services; evidence on effectiveness
of different service systems for children and families; evidence on outcomes of services;
evidence on determinants of well-being; evidence on processes of helping; and evidence on
inter-agency working.
KEYWORDS
services for children and families; evidence; outcome; need; well-being.
Page 3
2
Introduction
The idea that public policy and services should be ‘evidence-based’, or at least ‘evidence-
informed’, and should also be ‘outcome-focused’, is now accepted as the basis for assessing
their performance and usefulness. It is not an entirely new idea but has gained particular
currency in Ireland since the OECD reviewed the public service in 2008 and called for a
greater focus on managing performance, improving dialogue on performance targets and:
‘Instead of focusing on inputs and processes, more information needs to be gathered on
outputs and outcomes and what has actually been achieved, so that this can better feed back
into measuring how the Public Service is meeting overarching targets and objectives.’
(OECD, 2008, p.13). In light of the OECD review and the collapse of the Celtic Tiger which
began around the same time, the programme of the current Government (2011-present) lays
particular emphasis on performance management and the use of performance information to
inform decisions about how resources are allocated to policies and services (Department of
Taoiseach, 2011, p.24). This is reflected in a new approach to public expenditure involving
‘performance-based budgeting’ which links the spending of each Government Department to
its strategic programmes and associated performance indicators rather than traditional
accounting ‘sub-heads’ (Department of Public Expenditure and Reform, 2012, p.74-75).
Reflecting these developments, the Statement of Strategy by the new Department of Children
and Youth Affairs (DCYA), which was set up in June 2011, places particular emphasis on
using evidence to improve performance: ‘Information is a key driver for improving the
delivery of services. In the current economic climate, with reducing resources, better analysis
of performance information will be essential in achieving the most value from use of these
resources.’ (Department of Children and Youth Affairs, 2012, p.11). Similarly, the report of
the Task Force which was set up to advice on the new Child and Family Support Agency
(CFSA) emphasises the importance of establishing a performance management framework
Page 4
3
for the new agency so that: ‘The Minister and the DCYA will have a key role in setting clear
objectives and raising the political dialogue from one that concentrates on inputs to one that
focuses on desired outcomes and realistic measurable targets.’ (Task Force on the Child and
Family Support Agency, 2012, p.16).
The fact that public policy and services are increasingly framed in terms of evidence about
performance on outputs and outcomes does not, of itself, generate new evidence much less
improve performance. New ways of talking are not the same as new ways of doing. Talking
about outcomes without corresponding evidence can have the effect of replacing evidence
with presumptions which is not a sound basis for assessing performance. Establishing a more
evidence-based approach to public policy and services constitutes a major undertaking
because it involves producing valid and reliable indicators of performance for the outcomes
of each programme funded by each Government Department, in addition to putting in place
IT systems to routinely collect and analyse the data. More fundamentally, it involves a new
way of thinking about public services which focuses more on whether it is making a
difference to those who receive it rather than just delivering a service. That is why setting up
the new CFSA provides an opportunity to explore what types of evidence might be helpful to
ensure it builds a strong foundation of knowledge about how to design and deliver services
for children and families. That is the purpose of this article.
The article summarises six types of evidence that could contribute to designing services that
are effective and increase the likelihood of improved outcomes. These are: (1) evidence on
matching needs to services; (2) evidence on effectiveness of different service systems for
children and families; (3) evidence on outcomes of services; (4) evidence on determinants of
Page 5
4
well-being; (5) evidence on evidence on processes of helping; and (6) evidence on inter-
agency working. Before doing so, we outline briefly the background to the new agency.
Child and Family Support Agency
The establishment of CFSA is part of the programme of the current Government which states:
‘We will fundamentally reform the delivery of child protection services by removing child
welfare and protection from the HSE and creating a dedicated Child Welfare and Protection
Agency, reforming the model of service delivery and improving accountability to the Dáil
(Department of Taoiseach, 2011, p. 56). This, in turn, is part of a wider reform of health
services and a commitment that: ‘The Health Services Executive will cease to exist over
time’ (Department of Taoiseach, 2011, p. 32).
The task of setting up CFSA is being carried out by DCYA which itself brings together the
main areas of policy and provision affecting children and young people. In September 2011
the Department appointed a Task Force to advise on setting up CFSA, including the
necessary legislation and the transition arrangements to full implementation. Its report was
published in July 2012 and it recommended that the new agency ‘should be operationally
separate from the DCYA and governed by a board’ (Task Force on Child and Family Support
Agency, 2012:vii).
The Task Force recommended that the new agency should directly provide or commission the
following core services: child protection, family support, public health nursing, speech and
language, child and adolescent mental health, psychology, educational welfare, children in
detention schools, domestic and sexual violence (Task Force on Child and Family Support
Agency, 2012, p.31). The vision informing this recommendation is that ‘the scope of services
Page 6
5
provided directly by the CFSA, or linked with it in a defined and structured way, should
range from support to families in the community to highly specialised interventions where
children have been identified as requiring out of home care.’ (Ibid, p.25). In addition, the
recommendation was informed by the practical consideration that ‘the demand for multi-
disciplinary integrated working will be almost impossible to achieve in the current fiscal and
organisational climate unless services for children are working in the context of a single
vision, leadership and governance structure.’ (Ibid, p. 30).
The establishment and running of CFSA will involve a budget of around €550 million and
approximately 4,000 staff. Its success will depend on many factors, one of which is the use of
appropriate, timely and good quality evidence. We now discuss some types of evidence that
could assist the new Agency in addressing acknowledged weaknesses in services for children
and families while also supporting DCYA’s mission ‘to lead the effort to improve the
outcomes for children and young people in Ireland’ (Department of Children & Youth
Affairs, 2012, p. iii).
Evidence on matching needs to services
The purpose of services is to meet needs. A precondition of meeting needs therefore is to
have evidence which shows that services, and the resources required to fund them, are
geographically distributed according to need. At present, the evidence suggests that many
public services are not distributed according to need; well-documented examples are health
services (Expert Group on Resource Allocation and Financing in the Health Sector, 2010;
Staines, et al, 2010a; 2010b) and social work services (PA Consulting Group, 2009).
Generally speaking, the main drivers of resource allocation to services in Ireland have been
precedent rather than population need, community need, individual need, or even policy need
Page 7
6
(Expert Group on Resource Allocation and Financing in the Health Sector, 2010; Staines, et
al, 2010a; 2010b). That is why any move to a more rational and managed system of resource
allocation – as envisaged by the programme of the current Government (Department of
Taoiseach, 2011; Department of Public Expenditure and Reform, 2012) - must be based on
evidence about how services match needs at national level. This is a significant challenge
because of deficiencies in the information systems used to make decisions about resource
allocation as well as manage services. Pending the development of information systems that
are fit for this purpose, there is an immediate requirement for evidence on the match of needs
to services in the new CFSA.
Beginning with the needs of children and families, information is available through data on
levels of deprivation in each part of the country, down to the level of ‘small areas’ (each
comprising an average of 100 households), using the Pobal HP Deprivation Index (details at
www.pobal.ie and www.trutzhaase.eu). It is true that deprivation is only a proxy indicator of
need since not every child or family who lives in a deprived area is necessarily in need of a
service apart from the universal services which all children and families need; nevertheless
they are more likely than those living in an affluent area. Similarly, disability is a source of
need which is separately measured by the National Disability Survey. Children and families
who are already in receipt of HSE services are also in need and this is an important source of
data, though incomplete since not every child and family in need is known to the HSE.
Combining these different sources of data and their geographical distribution is a significant
undertaking but a necessary one in order to estimate the scale and distribution of need for the
purpose of efficient and equitable resource allocation.
Page 8
7
Once the distribution of need is established, it is then necessary to examine where child and
family services are located, including the catchment areas which are served by those services.
This is also a substantial undertaking. Ideally, it requires a census of every child and family
service in order to bring each service within one comprehensive database to facilitate the
analysis of how needs are matched to services. Some of this information is already available,
particularly on the distribution of child protection services, but assembling data on the
distribution of the other services which will be part of CFSA is more challenging given the
diversity of providers and the diversity of their catchment areas. The Task Force drew
particular attention to the challenge that different services for children and families have
different catchment areas – such as health, education, income support, Gardaí, local
authorities – and these organisational boundaries need to be aligned in order to facilitate
closer working relationships between services, and ‘maximize co-terminosity’ (Task Force on
Child and Family Support Agency, 2012, pp.21-22).
It is clear from this that producing solid information on the actual distribution of needs and
services would be a major achievement. Once established, this would then enable more
informed decisions about the appropriate balance of services between child protection and
family support within each area. These decisions, as suggested in the next section, would also
benefit from consideration of relevant international evidence regarding the effectiveness of
different service systems for producing improved outcomes for children and their families.
Evidence on effectiveness of different service systems
In designing services for children and families – particularly finding the right balance
between child protection and family support services – it is worth considering the
international evidence on how different service systems produce different outcomes. This is a
Page 9
8
challenging area of research due to the complexity of comparing different systems and their
outcomes. The Task Force commissioned the Centre for Effective Services to undertake an
international review of governance arrangements for dealing with children’s services,
including an assessment of the balance between child protection and child welfare. The
review suggested that, in the jurisdictions analysed (England, Scotland, Northern Ireland,
Norway, Ontario and New South Wales), there has been a merging of these two orientations
(child protection and child welfare) but also emergence of ‘a third orientation, child focused,
which concentrates its focus on the child as an individual with an independent relation to the
state. The object of concern is the child’s overall development and well-being, rather than
narrow concerns about harm and abuse.’ (Task Force on Child and Family Support Agency,
2012, p.84).
In Ireland, a previous review of family support services considered these system-level issues
and, on the basis of evidence available at that time (2004), observed that: ‘the amount of
family support activity in the system seems to be inversely related to the amount of child
protection activity, including the rate of children in care. … . As a result, systems which have
high levels of child protection activity (such as the US), tend to have low levels of family
support activity while others (such as the UK) which have lower levels of child protection
activity tend to have higher levels of family support activity. Ireland, which holds a similar
position to the UK as measured by the rates of children in care, also fits this pattern … and
shows that those Health Boards with the highest levels of family support provision tend to
have the lowest rates of children in care while those Health Boards with the lowest levels of
family support provision tend to have the highest rates of children in care. Although it is not
possible to offer a definitive explanation for this association, it provides food for further
reflection and investigation as part of the context for developing and rebalancing services for
Page 10
9
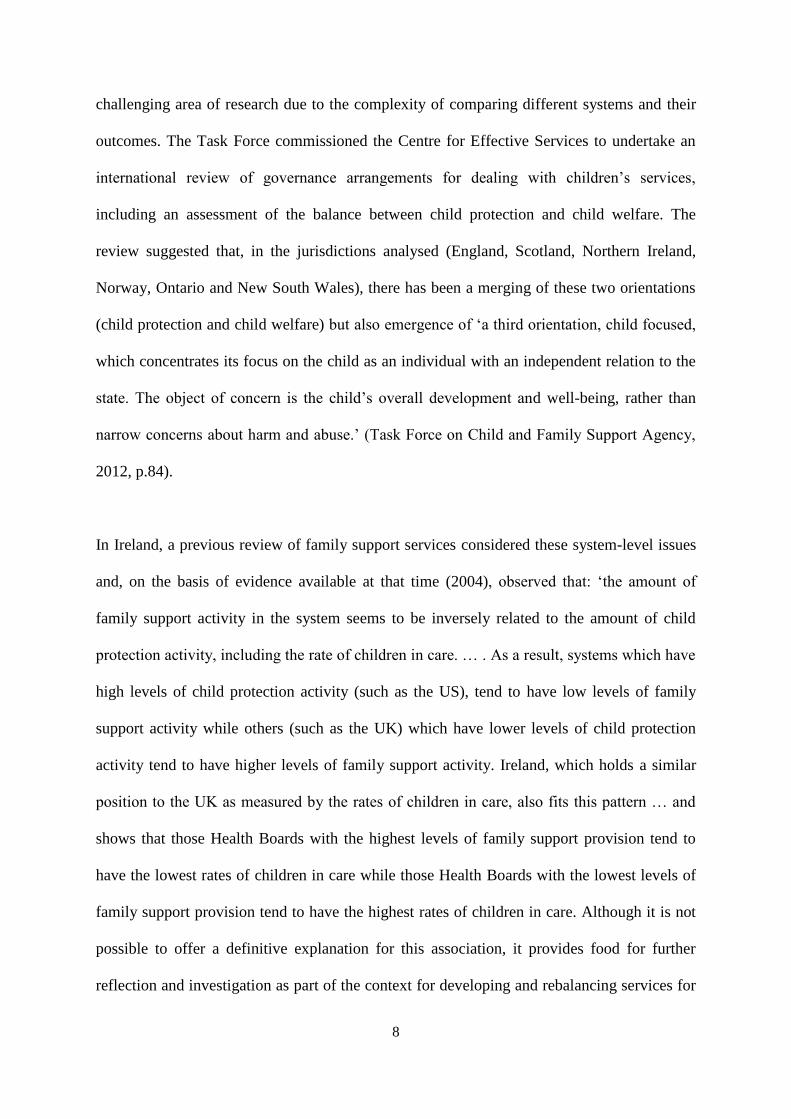
families and children in Ireland.’ (McKeown, Clarke and Little, 2004, p. 35; McKeown and
Haase, 2004). Building on this, Figure 1 graphically illustrates the hypothetical relationship
between child protection and family support and draws attention to the inverse relationship
just described.
Figure 1 Hypothetical Relationship Between Family Support & Child Protection
Of particular interest is whether the outcomes produced by different service systems are due
to differences in the needs of children in families or, as some evidence suggests, to the way
services respond to those needs. For example, some UK evidence suggests that when children
are classified as child protection cases, more effort is invested in finding out whether abuse or
neglect occurred than in responding to identified social needs (Farmer and Owen, 1995). As a
consequence, children allocated to family support are more likely to get support and to get it
rapidly than are child protection cases (Department of Health, 1995). This outcome is
contrary to the equitable and efficient use of resources but is also contrary to professionals’
perception of what happens, namely that the child protection label is needed to secure
resources (Schuerman, Rzepnicki and Littell, 1994; Hallett, 1995).
Family Support Activity
Child Protection Activity
UK
US
Ireland?
Page 11
10
The Task Force identified four levels of intervention for children and families, as summarised
in Figure 2, building on the ‘Hardiker model’ (2002).
Figure 2 Levels of Need and Services for Children and Families
Source: Adapted from Hardiker, (2002),
The Task Force recommended that CFSA ‘should provide services to and support families at
all levels’ adding that ‘The service model should focus on strengthening services at universal
level within the remit of the Agency, thereby preventing problems from arising in the first
place and managing such difficulties at the earliest opportunity by linking families to the
most appropriate family support service. Supporting families within the community and
working to prevent children from entering the child protection system is essential requiring
an emphasis on early intervention community based services.’ (Task Force on Child and
Family Support Agency, 2012, p.38).
Level 1: mainstream services for all
children with universal needs
Level 2: targeted services for children
with additional needs
Level 3: multiple services for children at
risk in families with serious or chronic
problems
Level 4: out-of-home services for
children because of family breakdown
Page 12
11
A graphic illustration of how these four levels are expected to form an integrated service in
CFSA is illustrated in Figure 3.
Figure 3 Integration of Services in Child and Family Support Agency
OtherCommunity &
Voluntary Services
Target Services
Early Intervention / Prevention
Universal ServicesE.g. Local Government, Education, Health
Local Area PathwaySupporting Children
and FamiliesSocial Work
Child in Care
Close
Child Protection
(CPNS)
Child Welfare re cases at risk of
formal intervention (DRM type response)
Formal Communication
Mechanism
Ava
ilabl
e Lo
cal
Com
mun
ity
Serv
ices
Community & Voluntary
Services (38 & 39)
Referral
Initial Assessment
Point of Entry ScreeningContact Concern Intake
Not open to social work Open to social work
Source: Jeyes, 2012.
The recommendations of the Task Force are consistent with available evidence about the
importance of prevention and early intervention (for recent reviews, see Allen, 2011; Field,
2010; Statham and Smith, 2010). However implementation of this service model will present
challenges given the tendency for urgent interventions at levels 3-4 to take precedence over
important interventions at levels 1-2. One way of strengthening implementation therefore is
to create robust information systems for tracking how resources are allocated at each level -
Page 13
12
including appropriate flexibility to reflect variations from one catchment area to another –
and to link this systematically to service outcomes.
Evidence on the outcomes of services
We have seen that the purpose of services is to meet needs. In the case of services for
children and families, this could be reframed by saying that services are useful and valuable
only if their outcome is improved well-being for children and families. This implies that the
usefulness of services, including their value-for-money, is determined by their outcomes.
National policy for children (Department of Health and Children, 2000; 2007) is committed
to five outcomes in the following domains:
Domain Outcomes for Children
1. Health Healthy physically, mentally and emotionally
2. Education Supported in active learning
3. Safety Safe from accidental and intentional harm; secure in the immediate and
wider physical environment
4. Income Economically secure
5. Participation Part of positive networks of family, friends, neighbours and the
community; included and participating in society
The Task Force recommend that this ‘outcomes framework’ should be adopted by the CFSA
and by all other services affecting children and families. ‘In other words, the service delivery
model should be focused on improving well-being and outcomes for children based on the
five national outcomes.’ (Task Force on the Child and Family Support Agency, 2012, p. xii;
and pp. 37-38).
Page 14
13
Implementation of this recommendation could improve the quality of services for children
and families provided it is accompanied by a shift in the focus of service providers from
delivering services to checking if the service is making a difference. This switch requires an
empathic relationship between the person giving the service and the person receiving it, and
is the difference between ‘delivering services’ and ‘delivering outcomes’. This switch is
known to improve outcomes: ‘monitoring client-based outcome, when combined with
feedback to the clinician, significantly increases the effectiveness’ (Lambert, 2010).
The focus on outcomes also requires an information system for monitoring, reviewing and
evaluating how services deliver these outcomes. This however will involve a radical
departure from current practice since most services for children and families are not
monitored or evaluated in terms of outcomes even though this framework has been in
existence since 2007. This applies to child protection services - despite the large number of
inquiries (Commission to Inquire into Child Abuse, 2009; Commission of Investigation,
2010; Roscommon Child Care Inquiry, 2010; Ombudsman for Children’s Office, 2010.),
reviews (PA Consulting Group, 2009) and audits (available at: www.hiqa.ie) - as well as
family support services. At the same time, it is acknowledged that substantial evaluations are
being undertaken of selected programmes and services, under the auspices of DCYA,
including Prevention and Early Intervention Programme (PEIP), National Early Years Access
Initiative (NEYAI) and National Framework for Early Childhood Education (Síolta).
Monitoring performance requires a minimum dataset which is prepared annually and
enumerates the activities, beneficiaries and resources in each outcome area. A minimum
dataset is the standard tool used to monitor the performance of public programmes and, as the
term suggests, is designed to collect the minimum data necessary to give a national overview
Page 15
14
of the programme while minimising the burden of data collection on those delivering it.
Minimum datasets also facilitate the setting of targets and assessing whether they are met,
including identification of sources of variation between areas in meeting them.
In addition to monitoring, it is also necessary to undertake periodic reviews and evaluations.
This is necessary in order to assess the impact of services. Unlike monitoring data which is
typically ‘cross-sectional’ in the sense that it provides an annual snap-shot, evaluation data is
typically ‘longitudinal’ in the sense that it measures change over time by reference to an
appropriate baseline or standard. Given that scientific evaluations are relatively infrequent
because they are also relatively complex and expensive undertakings, the need for service
reviews every 2-3 years is important to address questions such as the following:
What evidence is available to show that progress has been made in each of the five
outcome areas for children, parents, adults, and communities?
Can this evidence be corroborated from more than one source?
What changes are needed to improve size and sustainability of outcomes?
If evidence suggests that little or no progress has been made in some or all of the
outcome areas, what are the reasons for this and what are the reasons to justify
continuing the service?
What lessons have been learned about those services which children and families find
most helpful and most suited to their needs and preferences?
Evidence on determinants of well-being
Given that the raison d'être for services is to improve the well-being of children and their
families, it is appropriate to give further consideration to what well-being means. Well-being
is about the enjoyment of life. It is a way of describing the quality of life and happiness of
Page 16
15
individuals, families, communities and society itself. The concept has deep roots in almost
every philosophical and religious tradition, and has been revived in recent times as a way of
offering a more holistic understanding of what constitutes a full life. In the area of health, for
example, it has been used to promote an understanding of health as ‘more than the absence of
illness’ (Department of Health and Children, 2001:15), just as mental health is now seen as
‘broader than the absence of mental disorders’ (Expert Group on Mental Health Policy,
2006:16). Informed by this perspective, a new field of research has been created, called
positive psychology, in order to understand what makes people well instead of the more
traditional focus of psychology on pathologies (Seligman, 2002:xi). In the field of economics,
there has been a parallel realisation that the welfare of societies is not adequately measured
by its income and a broader understanding based on the concept of well-being is required
(Stiglitz, Sen and Fitoussi, 2009). In the area of philosophy, there are equally important
questions about the sources of well-being since the answers to these questions have relevance
for how one seeks it.
The most significant source of data on child and family well-being in Ireland is the national
longitudinal study of children, Growing Up in Ireland (GUI), funded by DCYA. A growing
body of statistical analysis is now being undertaken on this dataset (for example, Fahey,
Keilthy and Polek, 2013; McCrory and Layte, 2011; see also www.growingup.ie). One study,
based on the nine year-old cohort (8,570 nine-year old children with data collected between
September 2007 and June 2008), used structural equation modelling to estimate the strength
of parent-child relationships in in two-parent families by first defining the concept of parent
well-being (comprising depression, parent-child relationship, and parent-parent relationship)
and child well-being (comprising self-concept, strengths and difficulties, and scholastic
achievement) and then analysing the key influences on each
Page 18
Figure 4 shows that a one-unit change in well-being of a parent (in this case the mother since
the primary caregiver is usually the mother in GUI) is associated with a 0.41-unit change in
well-being of the child. In other words, when parental well-being improves the child’s well-
being is also likely to improve. The converse of this also applies: when parental well-being
deteriorates the child’s well-being is also likely to deteriorate. From an intergenerational
perspective, and taking a wider body of evidence into account, one could say that the parent-
child relationship is the main route by which the well-being of one generation is handed
down to the next, whatever the family type.
Figure 4 also shows how being healthy (based on the mother’s report of her own health and
her child’s health) is central to the experience of well-being for both parents and children. In
addition, socio-economic factors, particularly household deprivation and financial
difficulties, have a direct and adverse effect on parental well-being and, indirectly on child
well-being; however children are also directly and adversely affected by the level of
deprivation in the area where they live. Parental education is another route through which
socio-economic factors have an influence since lower levels of parental education are
associated with lower levels of child well-being. Also, children of younger parents tend to
have poorer well-being, probably because children benefit from the greater maturity of older
parents.
These finding are consistent with numerous studies on the factors which influence the well-
being of children and their parents (for recent reviews, see Allen, 2011; Field, 2010; Statham
and Smith, 2010;). They are particularly relevant to the design and delivery of services for
children and families because they provide a map of how services could align themselves
Page 19
18
with the generic processes of well-being in order to strengthen protective factors and mitigate
risk factors. The parent-child relationship is crucial to this but so too are the wider contextual
influences, since parents effectively act as a buffer between the child and these wider
influences. That is why a range of supports is required, but particularly targeted at parents in
adverse family and socio-economic circumstances and in early years of the child’s life when
adversity has its most negative consequences, since the evidence indicates that this is one of
the most effective ways of promoting the well-being of children.
These finding also draw attention to the relative importance of different influences on well-
being. The evidence in Figure 4 indicates that improving parental well-being is one of the
best ways to improve child well-being, though naturally not the only way. In fact there are
few services, if any, that produce an impact on children that is equivalent to parents. For
example, childcare programmes like High Scope (Barnett, 2011, p. 975), Early Head Start
(Mathematica Policy Research, 2002, p. xxv), Effective Pre-School and Primary Education
Project (Sammons, 2010, pp. 128-130), all have relatively small effects by comparison. The
same applies to family support programmes like Sure Start (National Evaluation of Sure Start
Team, 2010, p. 29) and Springboard (McKeown, Haase and Pratschke, 2006). None of this
implies that the relatively small effects of programmes and services are not worthwhile
(Heckman, Moon, Pinto, Savelyev and Yavitz, 2009); the point is that interventions which
are carefully designed and targeted at the processes of well-being are more likely to show a
measurable effect.
As theory and research has become more subtle and sophisticated, it is possible to separate
the inter-locking strands of child and parent well-being by distinguishing between immediate
and direct influences on the child (usually referred to as ‘proximal influences’) and those
Page 20
19
which have an indirect and more distant influence (usually referred to as ‘distal influences’)
(Bronrenbrenner and Morris, 2006). Proximal influences typically refer to characteristics
such as the personality traits and states of parents as well as the relationship of parents to
each other and their children, while distal influences include characteristics such as the socio-
economic characteristics of the household as well as the level of disadvantage and service
provision in the neighbourhood and wider community. Some variables – such as personality,
support networks, socio-economic status, local community – have been found to exercise a
direct as well as an indirect influence on child well-being, suggesting their pervasive
influence on the family system (NICHD Study of Early Child Care and Youth Development,
2006:23-25). This approach to understanding children and their parents is informed by the
‘ecological perspective’, associated with the name of Uri Bronfrenbrenner (1917-2005), and
is now the dominant paradigm in this field.
The significance of this evidence lies primarily in the fact that services to improve the well-
being of children need to take account of the fact that these are likely to have greater impact
when they simultaneously support and enhance the well-being of parents and children. In
other words, services are more likely to produce large and sustainable outcomes when they
adopt a holistic family approach rather than focusing solely on either the child or the parent.
To some extent, this evidence is already well known but its implications need to infuse the
vision of CFSA and inform its practice of how services are designed and delivered.
Page 21
20
Evidence on processes of helping
Helping is at the heart of all services and a normal and natural part of life, arising
spontaneously because people help, and are helped, all the time through family, friends, and
communities. Everyone is a natural helper and people seek professional help only when all
other sources have been exhausted. ‘Throughout human history, individuals with social and
emotional difficulties have benefited from talking with a sympathetic ‘other’ perceived as
being able to offer words of comfort and sound counsel either because of recognised
inherently helpful personal qualities, or by virtue of his or her role in the community. …
However, even in today’s world, the vast majority of individuals who are experiencing
psychological distress do not seek help from trained and credentialled professional
counsellors and therapists: they obtain relief by talking to individuals untrained in counselling
or psychotherapy’ (McLennan, 1999, p.169). Helping, in other words, could be described as a
naturally-occurring process and professional help works best when it draws from that source
to strengthen and support the experience of well-being.
This raises the question: what factors contribute to effective helping in order to produce
improved well-being? There is now a strong body of scientific evidence, particularly in the
field of psychotherapy and counselling, which focuses on the common factors shared by all
effective programmes and interventions. A number of meta-analytic reviews have been
undertaken of this work (Lambert, and Bergin, 1994; Dunn and Schwebel, 1995; Smith and
Glass, 1977; Hubble, Duncan and Miller, 1999; Duncan, Miller, Wampold and Hubble,
2010). These reviews confirm the effectiveness of therapeutic interventions generally but,
more importantly, confirm that therapeutic outcomes are more influenced by what
programmes have in common than by what differentiates them. These common factors, as
summarised in Figure 5, comprise client characteristics, therapist-client relationship,
Page 22
21
therapeutic technique and client hopefulness. Remarkably, ‘technique’ or intervention, about
which so much is written and claimed, contributes a relatively small part to the overall
outcome. The main influence comes from what the client brings to the service and the way
the therapist interacts with the client to create opportunities for change, triggering a sense of
hopefulness that change is possible and attainable.
Figure 5 Common Factors in Therapeutic Outcomes
Source: Asay and Lambert, 1999.
The significance of this work is recognised in the field of social work and family support,
particularly in the US, where there is increasing focus on ‘the common factors framework’
and a recognition of the need for a feed-back loop from clients to therapists in order to ensure
that interventions ‘engage clients, heighten hope for improvement, fit client preferences,
maximise therapist-client fit, and accelerate client change’ (Barth, Lee, Lindsey, Collins,
Strieder, Chorpita, Becker, and Sparks, 2012, p. 114).
Page 23
22
The focus on common factors is significant in the context of designing services for children
and families because it widens the conventional understanding of what is usually meant by
‘evidence-informed practice’ which has tended to focus on ‘proven programmes’ rather than
approaches which are effective and common across all programmes. It is also significant
because it addresses one of the challenges faced by practitioners that ‘evidence’ usually takes
the form of manuals with detailed instructions about how to implement a particular
programme, itself a reason why the uptake of evidence-based approaches tends to be
relatively limited in areas such as social work (Plath, 2006; 2009; Barth, Lee, Lindsey,
Collins, Strieder, Chorpita, Becker, and Sparks, 2012) and social care (Farrelly, 2009), but
probably also in family support. However a focus on evidence-based programmes is not the
only, or necessarily the best, way to think about evidence-informed practice since the focus
on common factors widens the possibilities for using evidence. Naturally, this does not
exclude using evidence-based programmes – since the value of these programmes is
undiminished - but it includes the option of using evidence not just with fidelity but also with
flexibility, taking into account the unique needs of each child and family and the relationship
qualities that are known to be associated with therapeutic effectiveness: emotionally warm,
responsive, problem-solving, collaborative, interested and engaged (see McKeown, 2013). As
a recent review observed: ‘Positive therapeutic outcomes are robustly predicted when
therapists are experienced as being personally engaged rather than detached, collaborative
rather than directive, empathic and warmly affirming’ (Duncan, 2011:23-24).
Page 24
23
Evidence on inter-agency working
The Task Force is unambiguous in its assessment, based on a review of published reports,
that ‘fragmentation and silos that exist in services is the systemic cause of the failure to meet
children’s needs’ (Task Force on the Child and Family Support Agency, 2012, p.iii).
Correspondingly, its recommendation on CFSA’s core services is designed to eliminate ‘the
current silo structure of services to children and families’ so that they ‘are working in the
context of a single vision, leadership and governance structure’ (Task Force on the Child and
Family Support Agency, 2012, p.iv and 30). In reaching this recommendation, the Task Force
formed the view that existing instruments for inter-agency working, such as ‘collaborative
arrangements’ and ‘service level agreements’ have proven inadequate (Ibid).
Against this background, it is useful to consider the evidence on inter-agency working and
how this could inform the work of CFSA. The policy consensus in Ireland for over two
decades is that inter-agency working is an important aspect of all public services but
particularly services for children and families. Ironically, and despite repeated affirmations of
this policy, there is just as much consensus that inter-agency collaboration is still poorly
developed. One of the challenges in finding evidence on inter-agency working is that there
are few well-designed studies which show that it improves outcomes for children and
families. For example, a recent review of international research on inter-agency working
commissioned by DCYA concluded that: ‘There is, as yet, limited evidence on improved
outcomes for children and families from this [inter-agency] way of working, but there is
promising evidence from many countries on the benefits of a more joined-up approach in
improving professional practice and providing better support at an earlier stage for children
and families who need it’ (Statham, 2011:4).
Page 25
24
In light of this, it is useful to consider some Irish evidence that emerged from an in-depth
evaluation of a five-year inter-agency initiative (2005-2010) designed to address the needs of
10-18 year old children and their families in the Ballymun area of Dublin (WRC Social and
Economic Consultants, 2010; McKeown, 2011; 2012). This initiative, called Ballymun
Network, was formed by managers of 17 local services (including almost all ‘core’ CFSA
services as well as additional ‘interface’ services) with the aim of improving inter-agency
responses for vulnerable young people. Around the same time as Ballymun Network was
being formed, the Prevention & Early Intervention Programme for Children (PEIP) was being
introduced through youngballymun in 2006 with substantial investment in a series of
integrated services for children, young people and families, these delivered through many of
the same agencies in Ballymun Network. Evaluation of these services is at various stages of
completion and a preliminary economic appraisal of results indicates that youngballymun is
delivering a ‘positive return to the State’ (Lawlor and Gilloway, 2012:726; see also Clarke,
2012).
Ballymun Network focused exclusively on improving inter-agency services for a well-
defined target group of 10-18 year olds and their families whose needs were not being met.
The results of an independent evaluation reached the conclusion that Ballymun Network had
created an excellent inter-agency process in terms of good inter-personal and inter-agency
relationships, a protocol for inter-agency case work, joint delivery of Strengthening Families
Programme, and joint training on legal aspects of care (notably Freedom of Information Acts
and Data Protection Acts). However the evaluation also found that outcomes of Ballymun
Network were disappointing since few young people or their families showed improvement
(WRC Social and Economic Consultants, 2010).
Page 26
25
Further analysis of why a good inter-agency process did not generate significant outcomes
pointed the following probable causes: (i) it was a difficult target group to work with since
some young people were already in the criminal justice system and did not want to engage
with any service; (ii) the quality of work by staff in some agencies was below standard as
evidenced by poor attendance at case meetings, incomplete minutes of meetings, minutes not
circulated, lack of follow-up on decisions made at meetings; (iii) managers appeared to
exercise little control over the quality of inter-agency work by front-line staff despite issues
about handling specific cases being raised at almost every meeting of Ballymun Network;
(iv) agencies did not seem to include inter-agency work in assessing individual or collective
performance; (v) most agencies seemed to view their work as delivering services rather than
outcomes as evidenced by the fact that they did not change or adapt their services despite the
fact that many young people and their families did not want what was offered.
These findings point to a simple but important conclusion of relevance to CFSA namely, that
the relatively poor outcomes of Ballymun Network are due mainly to intra-agency problems
rather than inter-agency problems. The evaluation suggests that the limits of inter-agency
effectiveness may be set by the poorest performing agencies, particularly where they have a
significant role to play in services for young people. Naturally, this conclusion does not imply
that the performance of every agency in Ballymun Network was poor or the same. Nor does it
imply that agencies in Ballymun are less effective than agencies elsewhere, or that
management and staff are not highly committed to giving the best possible service under the
circumstances. However it does imply that the case for continuing to deliver the same
services in the same way, irrespective of outcomes, is hard to justify, particularly where each
agency is an effective monopoly for its service.
Page 27
26
This draws attention to a diagnostic error that is commonly made in discussions about inter-
agency working. The error is that problems with services are often misdiagnosed as flaws in
the inter-agency process when in fact they may be problems of individual agency
performance and management, and the broader policy environment through which services
are commissioned which lacks instruments to promote quality standards for intra-agency as
well as inter-agency working. The observations of the former Director General in the Office
of the Minister for Children and Youth Affairs seem apposite in this context: ‘The Irish
Public Service has been relatively strong historically in the area of policy formulation. I have
come to the conclusion, however, that we are relatively weak when it comes to
implementation and many good policies fail due to a lack of appropriate structures and
processes to ensure their successful implementation from policy objectives to tangible
outcomes’ (Langford, 2007:250).
The findings of the evaluation of Ballymun Network may be expressed more formally in
terms of the necessary and sufficient conditions for inter-agency working. The necessary
condition is an effective and inclusive inter-agency process. The sufficient condition is that
each agency also has an effective intra-agency process which delivers services that children
and their families want to use and find helpful, and there is a policy environment which
supports and requires this. The findings of this evaluation suggest that Ballymun Network has
met the necessary conditions for effective inter-agency working but the sufficient conditions
have not been met. This is because the best inter-agency process in the world cannot
compensate for short-comings of individual agencies or weaknesses in the implementation of
policy.
Page 28
27
A further implication of this analysis merits attention: the promotion of inter-agency working
may actually serve to mask, however unintended or unwittingly, more fundamental problems
in the performance and management of individual agencies, including gaps in the broader
national context of policy implementation. It is not uncommon for Government Departments
and their agencies to frame issues as ‘inter-agency difficulties’ - to be solved by information-
sharing, procedures, protocols, capacity-building, committees, partnerships, consortiums -
when they are in fact ‘intra-agency difficulties’ of performance and management, or wider
difficulties in the way funders manage the performance of agencies. In other words, a good
inter-agency process can help correct relationship difficulties between agencies – and may
even magnify the performance of well-functioning agencies - but it cannot correct the
performance of poorly-functioning agencies, or weaknesses in policy implementation.
These findings are relevant to CFSA because, in bringing together previously separate
agencies into one core organisation, what was formerly an inter-agency challenge now
becomes an intra-agency challenge. Addressing this challenge will require a clear
understanding and commitment to ‘putting the child at the centre of policy and services’, as
the Task Force recommends (Task Force on Child and Family Support Agency, 2012:iii). In
practice this will mean designing and delivering services in light of the known needs and
preferences of children and families, especially those in adverse family and socio-economic
circumstances; it will mean shifting focus from delivering standardised services to constantly
checking if the service is helpful, making an improvement or at least preventing difficulties
getting worse; it will mean shifting from a ‘refer on culture’ as described by the Task Force
(Ibid:29), to a culture where CFSA acts as an advocate for children and families and ‘draws
in’ whatever services are required to meet needs in a timely fashion. In line with systems
thinking which has been used to bring about substantial and sustained improvements in
Page 29
28
education (Fullan, 2010; Mourshed, Chinezi and Barber, 2010) and the public sector
generally (Zokaei, Elias, O’Donovan, Samuel, Evans and Goodfellow, 2010), these changes
will require CFSA to see itself as a system from the perspective of service users – looking
from ‘outside-in’ rather than ‘top-down’ or ‘inside-out’ - and responding at each step of the
service user’s journey within the system, from entry to exit, in order to make sure that needs
are being met and well-being is improved. It may also require a new approach to
commissioning and funding services which puts children and families ‘first’ by giving them
greater choice about the services they wish to use and find useful. This approach and practice
is likely to improve outcomes for children and families but is also likely to improve the
quality of work for staff in CFSA because of the intrinsic and extrinsic job satisfaction that
comes from delivering the agency’s purpose and having relationships with service users that
are helpful, generate solutions to their difficulties, and result in improved well-being.
Concluding Comments
This article reviewed evidence that could assist the new CFSA. Specifically, it suggested that
six types of evidence could add value to its work: evidence on matching needs to services;
evidence on effectiveness of different service systems for children and families; evidence on
outcomes of services; evidence on determinants of well-being; evidence on processes of
helping; and evidence on inter-agency working.
The article builds on widespread consensus about the importance of using evidence to assess
how well public policies and services are performing relative to their expected outcomes.
However consensus about the importance of evidence does not, of itself, generate new
evidence much less improve performance. That is why the article draws attention to the
substantial implications of this way of talking about services since it implies a switch from
Page 30
29
simply delivering a service to checking if the service is needed, wanted and making a
difference. In addition, it involves creating information systems which give transparency to
the connection between services and outcomes.
There are high expectations of CFSA, reflected in the Task Force observation that ‘this is a
once in a generation opportunity to fundamentally reform children’s services in Ireland’
(Task Force on the Child and Family Support Agency, 2012, p.iii). This sense of optimism is
appropriate, even necessary, in order to sustain the vision and motivation that will be required
to withstand resistance to change which the new agency will inevitably encounter over the
next 5-10 years in particular. That is why optimism also needs to be tinged with realism and
an acknowledgement that CFSA could fail since ‘fear of failure’ may also strengthen resolve
to succeed.
The possibility of failure, or at least failure to achieve the full potential of CFSA, arises for
two main reasons. The first and most immediate reason is that CFSA is being established
because the previous seven-year attempt (2005-2012) to reform services for children and
families through the HSE largely failed. The planned abolition of HSE might also be seen as
the reason for the new health services reform plan (Department of Health, 2012a; 2012b). It
is salutary to remember that the optimism surrounding CFSA was also present at the
establishment of HSE, even to the point that its former CEO used the same formula of words:
‘The advent of the HSE was a once-in-a-lifetime opportunity’ (Drumm, 2010:50; 2011). The
second reason why failure is a possibility is that ‘only a relatively few structured change
efforts achieve great success - most just get by while the majority fail to reach predefined
performance goals and objectives’ (Owen and Dietz, 2012:1; see also Mansfield, 2010). This
generalisation applies particularly to healthcare systems which are recognised internationally
Page 31
30
as being the most resistant to change (see for example, Coiera, 2011; Hurst, 2010). At the
heart of these failed reform attempts is resistance to change, conscious as well as
unconscious, not just by those who work in the system but by the way its work is organised,
commissioned and funded. To some extent, this is part of the challenge of ‘operating within a
public-sector environment’ (Drumm, 2011: 52) but also, as the former CEO of HSE
observed, ‘From my perspective, the problem was that services were more often than not
provided in a way that primarily facilitated those of us professionals who provided the
services rather than the patient’ (Drumm, 2011:3).
It is beyond the scope of this article to outline the steps required to ensure the CFSA
succeeds. Studies of successful change processes underline the importance of having a clear
goal, implemented through a series of incremental steps which align individual and
organisational capacities to that goal, with regular evidence-based reviews to ensure change
is on target to reach the goal (Owen and Dietz, 2012:1; see also Mansfield, 2010; Coiera,
2011; Hurst, 2010). In the field of education, for example, successful change processes on
this scale normally take around six years, involve every level of the system both individual
and organisational, and have clear outcome measures to determine whether it is succeeding or
failing (OECD, 2010; Mourshed, Chinezi and Barber, 2010). It is also worth noting that since
capacity for system change diminishes as organisations become more complex, adding
‘reforms’ is more likely to be effective only if accompanied by removal of elements and
practices which are no longer a ‘good fit’ with the goals of CFSA; otherwise ‘reform’ simply
creates further complexity and inertia (Coiera, 2011).
In this wider perspective of system change, evidence is just part of a bigger picture, a means
to an end and not an end in itself. The purpose of CFSA and the services it provides is to
Page 32
31
meet needs and improve outcomes for children and families especially those in adverse
family and socio-economic circumstances; evidence is only useful to the extent it contributes
to that purpose. One of the known risks associated with inappropriate use of evidence is that,
when poorly designed indicators and targets are used to measure performance and outcomes,
they can have the effect of distorting or displacing service activity by creating an incentive to
meet targets rather than delivering change and genuine improvements. Documented examples
of this draw attention to the importance of devising measurement instruments which capture
the true impact of individual services, including wider system-level impacts, while also
encouraging continuous quality improvement (Zokaei, Elias, O’Donovan, Samuel, Evans and
Goodfellow, 2010).
Finally, it is worth recalling that evidence is a way of seeing (as its Latin root ‘evidens’
implies – to see out), just as knowledge is also a way of seeing (as its Greek root ‘gnosis’
implies – ‘to know by the senses’). This understanding of evidence draws attention to the
attitude which precedes knowledge which involves a disposition to question and a refusal to
adopt taken-for-granted, ‘business-as-usual’, views of the world. That attitude creates
openness and responsiveness, including flexibility to adapt and change as circumstances
require. That is why evidence, in this wider understanding, is a stepping stone to knowledge
as well as self-knowledge and, as Socrates recognised, to wisdom (Plato, 2003, p. 43-6).
That, in turn, affects how one gives service as recognised by Polish poet and Nobel laureate,
Czeslaw Milosz (2001):
‘Then he wants to use himself and things
So that they stand in the glow of ripeness.
It doesn't matter whether he knows what he serves:
Who serves best doesn't always understand.’
Page 33
32
References
Asay, TD., and Lambert, MJ., (1999). ‘The Empirical Case for the Common Factors in
Therapy’, in Hubble, M.A., Duncan, B.L., and Miller, S.D., (Editors), The Heart and Soul of
Change: What Works in Therapy, Washington DC: American Psychological Association.
Allen, G. (2011). Early Intervention: The Next Steps, An Independent Report to Her
Majesty’s Government. January, London: Cabinet Office.
Barnett, W.S. (2011). ‘Effectiveness of Early Educational Intervention’, Science, Vol 333, 19,
August, 975-977.
Barth, R.P., Lee, B.R., Lindsey, M.A., Collins, K.S., Strieder, F., Chorpita, B.F., Becker,
K.D. & Sparks, J.A. (2012). ‘Evidence-based practice at a crossroads: the timely emergence
of common elements and common factors’, Research on Social Work Practice 22 (1), 109-
119.
Bronfenbrenner, U., and Morris, P. (2006). ‘The Bioecological Model of Human
Development’, in Lerner, R.M.V., Damon, W., & Lerner, RMS., (Editors), Handbook of
Child Psychology, Vol. 1: Theoretical Models of Human Development, pp.793-828.
Hoboken, NJ: Wiley.
Clarke, C., (2012). Evaluation of Write-Minded: A shared area-based literacy strategy,
SQW. Available at: www.youngballymun.com
Page 34
33
Coiera, E., (2011). ‘Why System Inertia Makes Health Reform so Difficult’, British Medical
Journal, 342:d3696
Commission of Investigation. (2010). Report into Catholic Diocese of Cloyne. Available at:
www.justice.ie [8 May 2012].
Commission to Inquire into Child Abuse. (2009). Final Report (Ryan Report). Available at:
www.childabusecommission.ie
Department of Children & Youth Affairs. (2012). Statement of Strategy 2011-2014. Dublin:
Department of Children & Youth Affairs, 2011:35. Available at: www.dcya.gov.ie [8 Jan
2013].
Department of Health, (2012a). Statement of Strategy 2011-2014, March, Dublin: Department
of Health.
Department of Health, (2012b). Future Health: A Strategic Framework for Reform of the
Health Service 2012 – 2015, November, Dublin: Department of Health.
Department of Health, (1995). Child Protection: Messages from Research, London: HMSO.
Department of Health and Children, (2000). The National Children’s Strategy: Our Children
– Their Lives, November, Dublin: Stationery Office. Available at www.dohc.ie [8 May
2012].
Page 35
34
Department of Health and Children, (2001). Quality and Fairness: A Health System For You,
Health Strategy, Dublin: Stationery Office. Available at www.dohc.ie
Department of Health and Children, (2007). The Agenda for Children’s Services: A Policy
Handbook, Dublin: Office of the Minister for Children and Department of Health and
Children. Available at: www.dohc.gov.ie [8 May 2012].
Department of Public Expenditure and Reform, (2012). Comprehensive Expenditure Report
2012-14, Dublin: Department of Public Expenditure and Reform, Available at: www.
per.gov.ie [8 Jan 2012].
Department of Taoiseach, (2011). Government of National Recovery 2011-2016, Dublin:
Department of Taoiseach. Available at: www.taoiseach.gov.ie [8 May 2012].
Drumm, B., (2010). ‘Frontline lessons in health care transformation – An interview with
Brendan Drumm, MD’, Health International, Number 10, pp.42-49. Available at:
www.mckinseyquarterly.com
Drumm, B., (2011). The Challenge of Change: Putting Patients Before Providers, Dublin:
Open Press.
Duncan, B.L., Miller, S.D., Wampold, B.E., and Hubble, M.A. (Editors), (2010). The Heart
and Soul of Change: Delivering What Works, Second Edition, Washington DC: American
Psychological Association.
Page 36
35
Duncan, BL., (2011). On Becoming a Better Therapist, Washington DC: American
Psychological Association.
Dunn, R.L., and Schwebel, A.I., (1995). ‘Meta-Analytic Review of Marital Therapy Outcome
Research’, Journal of Family Psychology, Volume 9, Number 1, 58-68.
Expert Group on Mental Health Policy, (2006). A Vision for Change: Report of the Expert
Group on Mental Health Policy, Dublin: Stationery Office. Available at: www.doh.ie
Expert Group on Resource Allocation and Financing in the Health Sector, (2010). Report of
the Expert Group on Resource Allocation and Financing in the Health Sector, July, Dublin:
Government Publications.
Fahey, T., Keilthy, P., and Polek, E., (2013). Family Relationships and Family Well-Being: A
Study of Families of Nine Year-Olds in Ireland, January, Dublin: Family Support Agency.
Farmer, E. and Owen, M. (1995). Child Protection Practice, London: HMSO.
Farrelly, T. (2009). ‘Evidence-based Practice in Social Care’, Share P., and Lalor, K.,
(Editors), Applied Social Care: An Introduction for Students in Ireland, Second Edition,
(pp.150-162), Dublin: Gill & Macmillan.
Page 37
36
Field, F. (2010). The Foundation Years: Preventing poor children becoming poor adults: The
report of the Independent Review on Poverty and Life Chances, December, London: Cabinet
Office. Available at: www.frankfield.co.uk [8 May 2012].
Fullan, M., (2010). ‘The Big Ideas Behind Whole System Reform’, Education Canada,
Volume 50, Number 3, pp.24-27. Available at: www.cea-ace.ca
Hallett, C. (1995). Inter-Agency Co-operation and Child Protection, London: HMSO.
Hardiker, P., (2002), ‘A framework for conceptualising need and its application to planning
and providing services’, Ward, H., and Rose, W., (Editors), Approaches to needs assessment
in children’s services, (pp.49-70), London: Jessica Kingsley Publishers.
Heckman, J.J., Moon, S.H., Pinto, R., Savelyev, P.A., and Yavitz, A., (2009). ‘The Rate Of
Return To The High/Scope Perry Preschool Program’, The National Bureau of Economic
Research (NBER): NBER Working Paper Series, Working Paper 15471, Cambridge,
Massachusetts. Available at www.nber.org [8 May 2012].
Hubble, M.A., Duncan, B.L., and Miller, S.D., (Editors), (1999). The Heart and Soul of
Change: What Works in Therapy, Washington DC: American Psychological Association.
Hurst, J. (2010), “Effective Ways to Realise Policy Reforms in Health Systems”, OECD
Health Working Papers, No. 51, OECD Publishing. Available at: www.oecd.org
Page 38
37
Jeyes, G., (2012). ‘Once in a Generation, Presentation to Conference of National Forum of
Family Resource Centres, Navigating the Future’, Croke Park Conference Centre, Dublin, 7th
November.
Lambert, M.J., and Bergin, A.E. (1994). ‘The Effectiveness of Psychotherapy’, in Bergin
A.E., and Garfield, S.L., (Editors), Handbook of Psychotherapy and Behaviour Change,
(pp.143-189). Fourth Edition, New York: Wiley,
Lambert, MJ., (2010). Prevention of treatment failure: The use of measuring, monitoring,
and feedback in clinical practice. Washington, DC: American Psychological Association.
Langford, S., (2007). ‘Delivering Integrated Policy and Services for Children’, Journal of the
Statistical and Social Inquiry Society of Ireland, June, Vol XXXVI pp.205-260. Available at
www.omc.ie
Lawlor, E., and McGilloway, S., (2012). An Economic Appraisal of the youngballymun
Initiative. Just Economics. London. Available at: www.youngballymun.org
Mansfield, J., (2010). The nature of change or the law of unintended consequences. London,
England: Imperial College Press.
Mathematica Policy Research, (2002). Making a Difference in the Lives of Infants and
Toddlers and Their Families: The Impacts of Early Head Start, Volume 1: Final Technical
Report, Washington DC: US Department of Health and Human Services. Available at: www.
mathematica-mpr.com[8 May 2012].
Page 39
38
McCrory, C., and Layte, R., (2011). ‘The effect of breastfeeding on children’s educational
test scores at nine years of age: Results of an Irish cohort study’, Social Science and
Medicine, XXX, 1-7.
McKeown, K. (2013). Strategic Framework for Family Support within the Family and
Community Services Resource Centre Programme, January, Dublin: Family Support Agency.
McKeown, K., (2012). ‘Inter-agency cooperation between services for children and families
in Ireland: does it improve outcomes?’, Journal of Children’s Services, Volume 7, Issue 3, pp.
191 – 200.
McKeown, K., (2011). ‘Inter-Agency Cooperation in Services for Children and Families: On
why a good inter-agency process alone may not guarantee better outcomes’, Administration,
Vol. 59, No. 2 pp. 27–47.
McKeown, K., Haase, T., and Pratschke, J., (2006). ‘Evaluating Springboard: Impact of a
family support programme in Ireland’, Journal of Children’s Services, Volume 1, Issue 1,
April, 16-27.
McKeown, K., Clarke, M., and Little, M., (2004). Promoting the Well-Being of Families and
Children: A Study of Family Support Services in the Health Sector in Ireland, December,
Dublin: Stationery Office.
Page 40
39
McKeown, K., and Haase, T., (2004) A Census of Family Support Services in Ireland:
Results of a Census of Family Support Services which were funded by Health Boards in 2002,
December, Dublin: Stationery Office.
McKeown, K., (2000). Supporting Families: A Guide to What Works in Family Support
Services for Vulnerable Families, October, Dublin: Stationery Office. Available at:
www.doh.ie [8 May 2012].
McLennan, J., (1999). ‘Becoming an Effective Psychotherapist or Counsellor: Are Training
and Supervision Necessary?’, in Feltham, C., (Editor), Controversies in Psychotherapy and
Counselling, (pp.164-173). London: Sage Publications.
Miłosz, C., (2001). ‘Love’, New and Collected Poems 1931-2001. P.50, London: Penguin
Press.
Mourshed, M., Chinezi, C., & Barber, M., (2010). How the world’s most improved school
systems keep getting better. London: McKinsey & Company.
National Evaluation of Sure Start Team, (2010). The Impact of Sure Start Local Programmes
on Child Development and Family Functioning: Report of the Longitudinal Study of 5-year-
old Children and their Families. London: Department for Education. Available at:
www.ness.bbk.ac.uk [8 May 2012].
Page 41
40
NICHD Study of Early Child Care and Youth Development, (2006). Findings for Children
Up to Age 4.5 Years, Washington, DC: U.S. Government Printing Office. Avaialble at:
http://www.nichd.nih.gov/publications [8 May 2012].
OECD, (2008). Ireland: Towards an Integrated Public Service, OECD Public Management
Reviews, Paris: OECD. Available at: www.oecd.org [8 May 2012].
OECD, (2010). PISA 2009 Results: Overcoming Social Background – Equity in Learning
Opportunities and Outcomes (Volume II), Paris: OECD. Available at: www.oecd.org.
Ombudsman for Children’s Office, (2010). A report based on an investigation into the
implementation of Children First: National Guidelines for the Protection and Welfare of
Children, Dublin: Ombudsman for Children’s Office. Available at: www.oco.ie [8 May
2012].
Owen, KO., and Dietz, AS., (2012). ‘Understanding Organizational Reality: Concepts for the
Change Leader’, Sage Open, October-December, pp1-14.
PA Consulting Group, (2009). Strategic Review of Children and Family Services: Putting
Children first and meaning it’, October. Available at www.hse.ie [8 May 2012].
Plath, D., (2006). ‘Evidence-Based Practice: Current Issues and Future Directions’,
Australian Social Work, Vol. 59, No. 1, March, 56-72.
Page 42
41
Plath, D., (2009). ‘Evidence-Based Practice’, in Grey and Webb (Editors), Social Work:
Theories and Methods, SAGE, Thousand Oaks, pp. 172-183.
Plato, (2003). The Last Days of Socrates, London: Penguin Books.
Pratschke, J., Haase, T., and McKeown, K. (2011). ‘Well-being and the Family System: A
Structural Equation Model of Individual, Relational and Contextual Influences’, Growing Up
in Ireland Third Annual Research Conference, D4 Berkley Hotel, Dublin, 1 December.
Available at: www.trutzhaase.eu [8 May 2012].
Roscommon Child Care Inquiry, (2010). Report of the Inquiry Team to the Health Service
Executive. Available at: www.hse.ie
Sammons, P. (2010). ‘Do the benefits of pre-school last? Investigating pupil outcomes to the
end of Key State 2 (aged 11)’, in Sylva, K., Melhusih, E., Sammons, P., Siraj-Blatchford, I.,
Taggart, B., Early Childhood Matters: Evidence from the Effective Pre-School and Primary
Education Project, (pp. 114-148) Oxford: Routledge.
Schuerman, J., Rzepnicki, T., and Littell, J. (1994). Putting Families First: An Experiment in
Family Preservation, New York: Aldine de Gruyter.
Seligman, M., (2002). Authentic Happiness: Using the New Positive Psychology to Realise
Your Potential for Lasting Fulfilment, New York: The Free Press.
Senge, P., 1990. The Fifth Discipline, Random House Business Books.
Page 43
42
Smith, M., and Glass, C. (1977). ‘Meta-analysis of Psychotherapy Outcome Studies’,
American Psychologist, Volume 32, 752-760.
Staines, A., et al, (2010a). Towards the Development of a Resource Allocation Model for
Primary, Continuing and Community Care in the Health Services, Volume 1, Executive
Summary, Dublin: Dublin City University.
Staines, A., et al, (2010b). Towards the Development of a Resource Allocation Model for
Primary, Continuing and Community Care in the Health Services, Volume 2, Technical
Report, Dublin: Dublin City University.
Statham, J., (2011). A review of international evidence on interagency working to inform the
development of Children’s Services Committees in Ireland, August, Dublin: Department of
Children and Youth Affairs. Available at: www.dcya.gov.ie [8 May 2012].
Statham, J., and Smith, M. (2010). Issues in Earlier Intervention: Identifying and supporting
children with additional needs, March, London: Department for Children, Schools &
Families and Thomas Coram Research Unit, Institute of Education, University of London.
Available at: www.dcsf.uk [8 May 2012].
Stiglitz, J., Sen, A., and Fitoussi, JP., (2009). Report by the Commission on the Measurement
of Economic Performance and Social Progress. Available at: www.stiglitz-sen-fitousssi.fr [8
Jan 2013].
Page 44
43
Task Force on the Child and Family Support Agency, (2012). Report of the Task Force on the
Child and Family Support Agency, July, Dublin: Government Publications. Available at:
www.dcya.ie [8 Jan 2013].
WRC Social & Economic Consultants, (2010). More than the Sum of its Parts: An Evaluation
of Ballymun Network for Assisting Children and Young People (2005-2010). Available at:
www.youngballymun.org.
Zokaei, K., Elias, S., O’Donovan, B., Samuel, D., Evans, B., and Goodfellow, J., (2010).
Lean and Systems Thinking in the Public Sector in Wales, Report for the Wales Audit Office,
January, Cardiff University: Lean Enterprise Research Centre. Available at
www.leanenterprise.org.uk