ADULTBASICLIFESUPPORT THEORETICAL GUIDELINES FOR TRAINING AND ASSESSMENTOrganisational Learning Unit Northern Sector Office: Level 2, Campus Centre, Randwick Hospitals Campus. Phone:93825313 Fax:93825280
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 2
Version ControlReleased by Version Release Date Review Date
Organisational Learning Unit 1 September 2008. January 2009 Organisational Learning Unit 1.1 January 2009. June 2009
AcknowledgementsThe following people have contributed to the development of these learning resources:
SESIH Education Assessment and Training Subcommittee (EATS). Committee members as of
July 2008:
Michelle Brady The Sutherland Hospital Jenny Broe The Prince Of Wales Hospital David Collins The Prince of Wales Hospital Lynette Higgs Sydney/Sydney Eye Hospital Jon Magill Prince of Wales Hospital Catherine Molihan Royal Hospital for Women Kim O’Leary Shoalhaven Hospital Alex Pile St Vincent’s Hospital Suzanne Schacht SESIAH Garry Skinner War Memorial Hospital Carolyn Smith Sydney Children’s Hospital Jayne Tesch Organisational Learning Unit SESIAH Gai Vereker The Wollongong Hospital Bruce Way Prince of Wales Hospital Lis Woodhart The Sutherland Hospital Lian Zheng War Memorial Hospital
Published by the Organisational Learning Unit, SESIAHS
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 9
Basic Life Support Mandatory Training and AssessmentThese guidelines provide the foundation for the South East Sydney and Illawarra HealthService (SESIH) Basic Life Support Mandatory Training and Assessment Program whichconsists of:
1. A theoretical component
2. A practical component
3. An assessment component
Learning outcomes
The learning outcomes for the SESIH Basic Life Support (BLS) Mandatory Training and
assessment program are as follows:
1. Theoretical Foundations
Outline the responsibilities of the single rescuer in a Cardiac Arrest;
Outline each step in the ARC Adult Basic Life Support algorithm (DRABCD);
Identify the process for summoning assistance in a Cardiac Arrest;
Discuss the use of personal protective equipment during resuscitation.
2. Skills Assessment Identifies hazards to health and safety of self and others;
Minimises immediate risk to health and safety of self and others by isolatinghazards;
Assesses vital signs of collapsed person;
Recognises the need for CPR;
Summons assistance;
Performs CPR in accordance with ARC guidelines.
See Appendi x 1 f or t he SESIH Adult Basic Lif e Suppor t Assessment Cr it eri a
Skills assessment f requency: All staff for whom Basic Life Support is deemed a mandatory skill are required to havetheir Adult BLS skills assessed on a yearly basis.
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 11
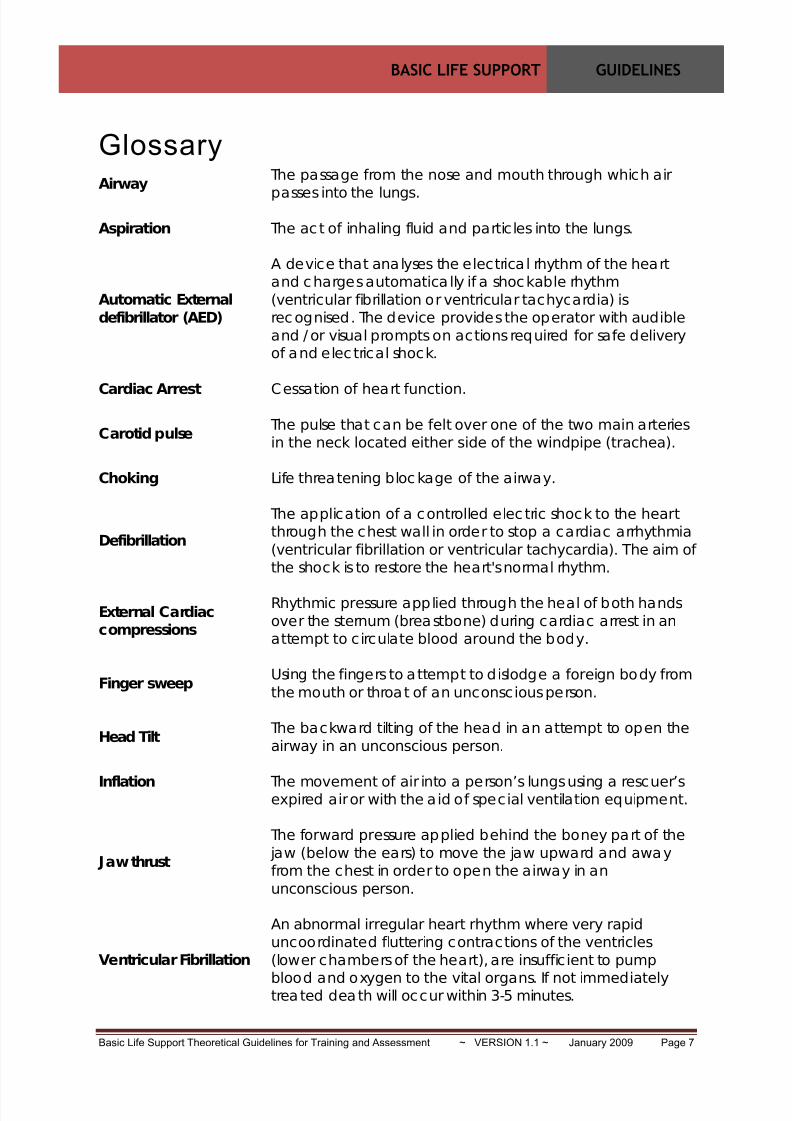
Foreword to GuidelinesBasic Life Support
Has been defined by the Australian Resuscitation Council (ARC) as “…the preservation oflife by the initial establishment of and /or maintenance of airway, breathing andcirculation, and related emergency care.” (ARC, 2006: Glossary of Terms: p2)
Cardiopulmonary Resuscitation
Cardiopulmonary resuscitation (CPR) includes the technique of combining rescue breathingwith chest compression. The aim of CPR is to maintain temporarily a critical amount ofcirculation to the heart and the brain (Handley et al, 2005:S7; ARC, 2006: Guideline 7)
About the Chain of Survival
The European Resuscitation Council (ERC) describes the steps involved in successfulresuscitation as the Chain of Survival (Nolan, 2005: S3). Each step is outlined below.
1. Early Recognition of Collapse/Emergency: Recognising those at risk of cardiacarrest and calling for help has the potential to avert a cardiac arrest.
2. Early Initiation of Cardiopulmonary Resuscitation: Effective CPR can dramaticallyincrease survival from ventricular fibrillation in sudden cardiac arrest by buying timeuntil successful defibrillation.
3. Early Defibrillation: Survival rates can be improved (49-75%) if CPR anddefibrillation are initiated within 3-5 minutes.
4. Early Advanced Life Support and Post Resuscitation Care: Effective postresuscitation care can preserve function particularly of the heart and brain.
Figure 1: ERC Chain of Survival (Nolan, 2005, S 5.)
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 15
Steps in Adult Basic Life Support
When a person collapses, his/her life may depend on the successful application of the
principles of the DRABCD of resuscitation:
D = DangerR = Response
= Airway= Breathing
C = Circulation D = Defibrillation with AED (in facilities where AED’s available)
(ARC, 2006, Guideline 7)
If someone collapses in your presence, or you find someone collapsed, take thefollowing steps:
DangerAssess for danger and remove the person and yourself to a safe environment if necessary(ARC, Guideline: 2.1 2002; Guideline 2.3 2005). Note: Do not attempt to move someoneby yourself, wait until help arrives to assist you.
ResponseDetermine responsiveness: Gently grasp and squeeze the person’s shoulders, speak to theperson by name if it is known. (ARC, 2006, Guideline: 3.1). Ask loudly “are you all right?”
If Responsive If Unresponsive
• Make the person comfortable and
observe airway breathing and
circulation (ABC);(ARC, 2004, Guideline: 3.1)
• Check Blood pressure and pulse;
• Call for nursing/medical help to
review person promptly.
• Summon HELP first
(ARC, 2006, Guideline: 2.1)
- Call/send for help; or
- If unlikely to get help easily, dialthe emergency number for your
fac ility or service (See Pa g e 5 );
- State the nature of the
emergency
- Give location
- Identify whether emergencyinvolves an adult or child
• Note the time;
• Assess Airway Breathing and
Circulation.
Ai rway
Open the airwayWhen a person is unconscious, all muscles are relaxed. If the person is lying on their backthe tongue falls against the back of the throat and obstructs the airway. To open theairway:
• Lay person flat on the back on firm surface (do not roll onto side);
• Apply head tilt /chin lift (see Figure 2) and/or jaw thrust (see Figure 3),
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 16
Ai rway (cont)
Manoeuvres to open Airway
Head Tilt/ Chin lift
The simplest way of ensuring an open
airway in an unconscious person is to
use a head tilt chin lift technique,
thereby lifting the tongue from the back
of the throat:
• Place your hand on the person’sforehead and gently tilt the headback.
• With your fingertips under thepoint of the persons chin, lift thechin to o en the airwa .
Figure 2: Head tilt chin lift
Jaw thrust
In the jaw thrust manoeuvre the jaw is
displaced forward, pulling the tongue
away from the back of the throat:
• Position yourself behind the headof the person;
• Place fingers behind the bonypart of the jaw (below the ears)and thrust the jaw upward and
away from the chest.
Figure 3: Jaw Thrust
Clearing the airway:
• Visually inspect airway;
• If safe to do so manually remove any visible solids or loose fitting dentures usinggloved hands. Note: Only perform a finger sweep if there is a visible obstruction.(Handley et al, 2005:s17).
• Use suction if available to clear secretions/vomitus from the airway. If suction notavailable roll person on side, if safe to do so, and drain fluid from the mouth.
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 17
Breathing
Once the airway is cleared and open, check for normal breathing for a period of up to 10seconds, using the following method. Not e t hat an occasional gasp or noisy br eat hing is
not consider ed normal br eat hing .
• Look and Feel for movement of lower chest or upper abdomen;
• Listen and Feel: for escape of air from nose and mouth.(ARC, 2008, Guideline: 5)
If Breathing NormallyIf Breathing Absent
or not normal • Place person in the recovery position
(see Figure 4):
Figure 4: Recovery position
• Check for continued breathing and
give oxygen flow rate to 15
litres/minute, if available;
• Note: Sta y w ith the p erson unt i l help
a rrive s .
(ARC, 2008, Guideline: 5)
• Ensure person is on a firm surface;
• Using mouth to mask resuscitation
method, give 2 rescue breaths each
of 1 second duration (See Figure 5;
See also Appendix 2);
Figure 5: Mouth to mask method
• If there is an oxygen source available
attach to the mask (flow rate to 15
litres/minute);
• Deliver a breath of sufficient volume
to see the chest rise;
• Note : If the c he st d o es no t riserec hec k hea d t ilt a nd c h in lif t ;
rec hec k m ask sea l; and d o no t
a t t emp t mo re t han tw o b rea t h s ea ch
t ime be fo re c om me nc ing o r re tu rn ing
to c hest co m p ression s ;
• Care should be taken not to use too
much force to inflate lungs. Ifexcessive force is used there is a risk
that air will inflate the stomachresulting in regurgitation of stomach
contents and aspiration into the lungs.ARC, 2008, Guideline: 5; Nolan et al, 2005)
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 18
KEY POINT: RESCUE BREATHING WITHOUT CHEST COMPRESSIONS
Information for Experienced Clinicians
In the event an experienced clinician determines that an adult person with palpable pulsesrequires support of ventilation:
• rescue breaths can be delivered at a rate of approximately 10 breaths per minute (onebreath every 5 to 7 seconds);
• each breath should be of sufficient volume to see the chest rise. If the chest does notrise, head tilt /chin lift and mask seal should be rechecked;
• Avoid inflating lungs with too much force as there is a risk that air will inflate thestomach resulting in regurgitation of stomach contents and aspiration into the lungs;
• Reassess for a pulse every 10 breaths but spend no more than 10 seconds doing so;
• Be prepared to commence compressions if a pulse is no longer palpable;
• If the person resumes breathing normally place in recovery position.
(ARC, 2006, Guideline 6; Nolan et al, 2005:S 44)
Circulation
Ensure person is on a firm surface. Keeping the airway open, check for signs of life. If nosigns of life present (i.e. person is unconsciousness, there is no movement and no normalbreathing or coughing) commence chest compressions immediately. Experienced cliniciansmay choose to check for a carotid pulse but are advised to spend no more than 10 seconds
doing so.
Performing Chest compressions
• Visualise and locate the centre of the persons chest (i.e. between the nipples);
• Kneel or stand vertically over the person so that your shoulders are over the sternumand your arms are straight;
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 19
Performing Chest compressions (cont)
• Place the heel of one hand in the middle of the sternum and place the other hand ontop for additional force;
Figure 6: Hand placement for compressions
• Do not apply pressure over the ribs;
• Compress the sternum, hard and fast, to at least 1/3 the depth of chest at a rate of100 per minute. Ratio of compressions to breaths should be 30:2;
Figure 7: Depth of compressions
• Compressions should be rhythmic with equal time for compression and relaxation.Note: Do not lift your hands from the sternum during compressions
(ARC, 2006, Guideline 6)
KEY POINT: RESUSCITATION IN LATE PREGNANCY
“In the obviously pregnant woman the pregnant uterus causes pressure on the majorabdominal vessels when she lies flat, reducing venous return to the heart. The pregnantwoman should be positioned on her back with her shoulders flat and sufficient padding(pillow or wedge) under the right buttock to give obvious pelvic tilt to the left.”
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 20
Additional Points on Compression
• Effective chest compressions generate a small, but critical amount of blood flow to themyocardium and brain and increases the likelihood of effective defibrillation;
• Both one operator and two operators should perform the same compression toventilation ratio of 30:2;
• Once an advanced airway has been secured (i.e. tracheal intubation) continuecompressions uninterrupted. Ventilations should be delivered at approximately 10breaths per minute or one breath every 5 to 7 seconds. Not e : Compr essions should
only be in te r rup t ed to per fo rm r hy thm ana lysis or t o def i b r i l l a t e ; (Nolan et al 2005:S 44).
• Performing chest compressions and rescue breaths at a ratio of 30:2 is tiring; it istherefore recommended that the person doing compressions be changed every 2minutes or when he/she becomes fatigued.
(ARC, 2006, Guideline 6)
Duration of CPR
Cardiopulmonary resuscitation should continue until:
• Signs of life return;
• Qualified help arrives;
• It is impossible to continue (e.g. exhaustion);
• An authorised person pronounces life extinct.(ARC, 2006, Guideline 7)
KEY POINT: PERFORMING CHEST COMPRESSIONS ONLY In cases where there is no barrier device or mask available for performing mouth to maskventilations, an acceptable alternative is to give uninterrupted chest compressions at arate of 100/minute (Koster et al, 2008) until qualified help arrives to secure an airwayand commence rescue breathing.
Note that the ARC states “Ventilation remains important in a significant proportion ofcardiac arrests. These include cardiac arrests … due to drowning or airway obstruction,in-hospital cardiac arrests and resuscitation attempts beyond the first 3 to 4 minutes.Compression-only CPR is insufficient in these circumstances”
(ARC Advisory Statement Compression only CPR: April 2008)
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 21
Automated External Defibr il lat ion (AED)
Note: The following section applies only to those facilities where AED’s are available andstaff have been trained in their use.
Introduction
Along with early initiation of cardiopulmonary resuscitation, early defibrillation is a keylink in the Chain of Survival’ following cardiac arrest (Nolan 2005:S4). VentricularFibrillation (VF) is the most frequent initial rhythm in sudden cardiac arrest withdefibrillation being the most effective treatment.
Survival rates following cardiac arrest can be improved provided CPR and defibrillation isinitiated early (within 3-5 minutes). Every minute a person remains in cardiac arrestrepresents a 10 % reduction in the likelihood of their survival to discharge from hospital(ARC, 2004: Guideline 10).
An Automated External Defibrillator (AED) is a portable automatic device that uses voiceand visual prompts to guide the lay rescuer or heath care professional in safely attemptingdefibrillation in cardiac arrest (ARC: 2004, Guideline 10; Hadley et al , 2005 )
Sequence for using an AED
• Verify that the person has no signs of life (i.e. unconsciousness, no movement, nonormal breathing or coughing)
• Initiate DRABC according to the guidelines outlined in pages 16 – 20 of this document;
•
As soon as the AED arrives the staff member operating the machine should switch it onand follow the spoken or visual prompts provided;
° Whilst continuing CPR, expose the patients’ chest and attach the electrode pads inthe following positions:
- Sternal Pad – Right Mid-clavicular line over 2nd intercostal space (See Figure 8);
- Apex Pad – Left Mid-axillary line over 6th intercostal space (See Figure 8).
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 23
Points on Defibri llation Safety
• Ensure defibrillator electrode pads are completely adhered to the skin. Air pocketsbetween the skin and the pads can result in burns to the skin during defibrillation or an
ineffective shock to be delivered. If the patient’s chest is excessively hairy it may benecessary to clip hair so the electrode pads will adhere to the chest. If the patient isdiaphoretic, wipe the chest carefully before attaching pads (AHA, 2005, Part 5).
• Avoid positioning defibrillator pads over any of the following:
° Any implanted medical device such as an implantable defibrillator orpacemaker.
Doing any of these things may cause electrical arching and/or burns duringdefibrillation and may also cause the defibrillation current to be diverted away fromthe heart (AHA, 2005, Part 5).
• Remove any free flowing oxygen from the vicinity of the defibrillator electrode pads,
as this presents a fire hazard during defibrillation (AHA, 2005, Part 5).
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 26
APPENDIX 3 Airway Management: Adul t foreign body obstruction
Foreign body airway obstruction (FBAO) is an uncommon but potentially treatable cause of
accidental death. The signs and symptoms of obstruction will depend on the cause and theseverity of the condition. For example, in the conscious person who has inhaled a foreignbody, there may be extreme anxiety, agitation, gasping, coughing or loss of voice.However in the unconscious person FBAO may not be apparent until rescue breathing isattempted.
The Adult FBAO sequence (see also Figure 10):
• If the person shows signs of mild airway obstruction, (i.e. they have an effectivecough), encourage him/her to cough but do nothing else;
• If the person shows signs of severe airway obstruction and is conscious apply up to
five back blows: stand to the side and slightly behind the person:
lean the person well forward, give up to 5 sharp blows between theshoulder blades with the heel of your hand;
check to see if each back blow has relieved the airway obstruction.
• If the person at any time becomes unconscious:
Support the person carefully to the ground – do not place yourself in dangerby ‘catching’ the person;
Summon HELP:- Call/send for help;
- Dial the facility emergency number state “Cardiac Arrest” and givelocation;
Begin CPR at a compression to ventilation ratio of 30:2
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 27
Adul t Basic Li fe Support Quiz Questions
The following Quiz in designed to assess the readers understanding of the Guidelinesoutlined in this document. The quiz can be undertaken as a self directed exercise or as
part of a facilitated question and answer session with other learners.
1. You find an adult person collapsed in a hospital corridor. What should you dofirst?
Determine responsivenessAssess for dangerCommence CPRCall for help(Need help? See Page 15)
2. What is your first priority after you determine the person is unresponsive?Make a note of the timeAssess airway and breathingCall for helpGive two breaths(Need help? See Page 15)
3. Of the options listed below indicate which one is recommended for opening theairway of a collapsed adult who isn’t breathing?
Roll person onto the left side and perform a backward head tilt
Perform a Heimlich manoeuvreUse Head tilt /chin lift or jaw thrust manoeuvreUse a finger sweep of the mouth to clear any obstruction(Need help? See Page 15, 16)
4. If the person does not commence breathing after you have opened the airway,what should you do?
Check the airway againPut the person in the coma positionStart chest compressions
Start rescue breathing(Need help? See Page 17)
5. When commencing rescue breathing, how many initial breaths do you give?2345(Need help? See Page 17)
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 28
6. A person with no ‘signs of life’ is:Unconsciousness/unresponsiveNot movingNot breathing normallyAll of the above(Need help? See Page 18)
7. You determine the collapsed person has no signs of life, what is itrecommended that you do now:
Call for HelpFeel for a pulseStart chest compressionsCheck their pupils(Need help? See Page 18)
8. When locating the site for chest compressions in an adult it is recommended tovisualise the centre of the chest.
TrueFalse(Need help? See Page 18)
9. When performing CPR the recommended ratio of compressions to breaths is?100 compressions to 2 breaths30 compressions to 2 breaths
15 compressions to 2 breaths5 compressions to 2 breaths(Need help? See Page 18)
10. It is recommended that CPR continue until:An authorised person pronounces life extinctQualified help arrives to assistExhaustion prevents you continuingSigns of life returnAll of the above
(Need help? See Page 19)
11. Basic Life support now includes defibrillation:TrueFalse(Need help? See Page 20)
12. What number do you call in your facility in the event of a Cardiac Arrest?
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 29
References:Anonymous (2000) “Part 4: The Automated External Defibrillator: Key Link in the Chain of Survival”,
Circulat ion, Vol. 108: (8) pp. 160-176.
American Heart Association (2005), ‘American Heart Association Guidelines for CardiopulmonaryResuscitation and Emergency Cardiovascular Care.’ Cir culat ion, Vol.112, (22): Supplement 1: 1-
136.
[http://circ.ahajournals.org/cgi/reprint/112/22_suppl/III-5] Accessed: March 5th 2008.
American Heart Association (2005), ‘Part 4: Adult Basic Life Support’ Cir culat ion, Vol.112, (24) :
Supplement 1:IV19-IV-34.
[http://circ.ahajournals.org/cgi/reprint/112/24_suppl/IV-19] Accessed: March 5th 2008.
Australian Resuscitation Council (2008). ‘Advisory Statement: Compression only CPR, The
Austr al i an Resuscit at ion Council Onli ne . [www.resus.org.au] Accessed July 9th 2008
Australian Resuscitation Council (2008). ‘Index of Guidelines’, The Aust ra l i an Resuscit at ion
Council Onli ne . [www.resus.org.au] Accessed July 9th 2008
Australian Resuscitation Council (2006). ‘Glossary of Terms’ Aust ra l i an Resuscit at ion Council
Online . [www.resus.org.au] Accessed July 9th 2008
Deakin, C.; Nolan, J. (2005), ‘European Resuscitation Council Guidelines for
cardioversion and pacing.’ Resuscitat ion (2005) 67S1, S25—S37
Handley, A.J.; Koster, R.; Monsieurs, K; Perkins, G. D.; Davies, S.; Bossaert, L. (2005) ‘European
Resuscitation Council Guidelines for Resuscitation: Section 2. Adult Basic Life support and use ofautomated external defibrillators.’ Resuscit at ion Vol . 67 (S1): S10.
[http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008.
Koster R.W. Bossaert, L.L.; Nolan, J.P. Zideman, D. (2008). ‘Advisory St at ement of t he European
Resuscit at ion Council on Basic Lif e Support . ’
[http://www.erc.edu/index.php/docLibrary/en/viewDoc/775/3/] Accessed, March 5th 2008.
Nolan, J. (2005). ‘European Resuscitation Council Guidelines for Resuscitation 2005: Section 1.Introduction.’ Resuscit at ion, Vol. 67: (S1)[http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed March 5th 2008.
Nolan, J. and Baskett, P. (2005), ‘European Resuscitation Council Guidelines for Resuscitation.’
Resuscit at ion, Vol. 67: (S1) [http://www.erc.edu/index.php/guidelines_download_2005/en/]Accessed March 5th 2008.
Nolan, J.; Deakin, C.D.; Soar, J.; Bottiger, B.W.; Smith, G. (2005) ‘European Resuscitation CouncilGuidelines for Resuscitation: Section 4. Adult Advanced Life Support.’ Resuscit at ion Vol . 67 (S1):
S51. [http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008.
Basic Life Support Theoretical Guidelines for Training and Assessment ~ VERSION 1.1 ~ January 2009 Page 30
Diagrams and Appendices:
Basic Life Support Flow Chart (Page 13)Australian Resuscitation Council (2006)[http://www.resus.org.au/public/arc_basic_life_support.pdf] Accessed March 5th 2008.
Figure 1: Chain of SurvivalNolan, J. (2005) ‘European Resuscitation Council Guidelines for Resuscitation: Section 1.Introduction.’ Resuscit at ion Vol . 67 (S1): S5.
[http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008.
Figure 2: Head Tilt Chin LiftNolan, J.; Deakin, C.D.; Soar, J.; Bottiger, B.W.; Smith, G. (2005) ‘European Resuscitation CouncilGuidelines for Resuscitation: Section 4. Adult Advanced Life Support.’ Resuscit at ion Vol . 67 (S1):
S51. [http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008.
Figure 3: Jaw ThrustNolan, J.; Deakin, C.D.; Soar, J.; Bottiger, B.W.; Smith, G. (2005) ‘European Resuscitation CouncilGuidelines for Resuscitation: Section 4. Adult Advanced Life Support.’ Resuscit at ion Vol . 67 (S1):
S51. [http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008. Figure 4: Recovery PositionHandley, A.J.; Koster, R.; Monsieurs, K; Perkins, G. D.; Davies, S.; Bossaert, L. (2005) ‘EuropeanResuscitation Council Guidelines for Resuscitation: Section 2. Adult Basic Life support and use ofautomated external defibrillators’ Resuscit at ion Vol . 67 (S1): S10. [http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008.
Figure 6: Hand Placement for Chest Compressions
Handley, A.J.; Koster, R.; Monsieurs, K; Perkins, G. D.; Davies, S.; Bossaert, L. (2005) ‘EuropeanResuscitation Council Guidelines for Resuscitation: Section 2. Adult Basic Life support and use ofautomated external defibrillators’ Resuscit at ion Vol . 67 (S1): S10.
[http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008.
Figure 7: Depth of CompressionsHandley, A.J.; Koster, R.; Monsieurs, K; Perkins, G. D.; Davies, S.; Bossaert, L. (2005) ‘EuropeanResuscitation Council Guidelines for Resuscitation: Section 2: Adult Basic Life support and use ofautomated external defibrillators.’ Resuscit at ion Vol . 67 (S1): S11.
[http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th, 2008.
Figure 8: Placement of Defibrillator electrodesPhillips Medical Systems (2004), ‘Heartstart Home Automated External Defibrillator: Instructions for
use.’ Edition 6. Phillips Electronics, North America.[http://www.heartstarthome.com/resources/HeartStart/docs/InstructionsForUse.pdf] Accessed,March 10th 2008.
Figure 10: Adult Forign Body Airway ObstructionNolan, J.; Deakin, C.D.; Soar, J.; Bottiger, B.W.; Smith, G. (2005) ‘European Resuscitation CouncilGuidelines for Resuscitation: Section 4. Adult Advanced Life Support.’ Resuscit at ion Vol . 67 (S1):
S53. [http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed, March 5th 2008.
Appendix 1: Adult Basic Life Support Assessment CriteriaSouth Eastern Sydney and Illawarra Area Health Service (2005) Adult Basic Life Support AssessmentCriteria, Incorporating the Automated External Defibrillator (AED).
Appendix 2: Mouth to Mask VentilationNolan, J.; Deakin, C.D.; Soar, J.; Bottiger, B.W.; Smith, G. (2005) ‘European Resuscitation CouncilGuidelines for Resuscitation: Section 4. Adult Advanced Life Support.’ Resuscit at ion Vol . 67 (S1):
S53. [http://www.erc.edu/index.php/guidelines_download_2005/en/] Accessed March 5th 2008.
Appendix 3: Adult Foreign Body Obstruction Management flow chartAfter: Australian Resuscitation Council (2006). ‘Management of Foreign Body Airway Obstruction
Choking: Guideline 6.’ Austr al i an Resuscit at ion Council Onli ne . [www.resus.org.au] Accessed