57
Adult Language Disorders and Cognitive-Based Dysfunction
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| Upload: | dale-potter |
| View: | 216 times |
| Download: | 0 times |

Adult Language Disorders and Cognitive-Based
Dysfunction


Focus Questions
1. What is aphasia?
2. How is aphasia classified?
3. What are the defining characteristics of aphasia syndromes?
4. How is aphasia identified and treated?
5. What are right-hemisphere dysfunction, traumatic brain injury, and dementia?
Case Study 7.1: Ronnie Lamm 68-year-old retired insurance agent who resides with
his wife and family nearby. Ronnie experienced a left-hemisphere stroke approximately 10 years ago. At the time of his stoke, his medical evaluation revealed coronary artery disease, arteriosclerosis, hypertension , and three previous “ministrokes” from which he recovered fully. He actively participated in speech-language therapy. He now communicates effectively but does experience hesitations when talking and difficulty recalling words.

Case Study Questions
1. What are some reasons that survivors of stroke are at greater risk for depression?
2. How might family dynamics in this scenario influence Ronnie’s outcome?
3. Why do you think Ronnie did not recover fully from this stroke the way he did from the previous strokes?

Case Study 7.1: Thomas Driver A 61-year-old, right handed male who recently
suffered a left middle cerebral artery stroke. After Mr. Driver was initially stabilized he was transferred to the rehabilitation unit. His current problems include right hemiparesis of the face, arm, and leg; visual field deficits; and communication difficulties. His past medical history reveals hypertension, elevated cholesterol, and adult-onset diabetes and tobacco use. Mr. Driver is an architect who resides with his wife. They have 4 adult children, 2 of who live nearby. His goal is to return to his previous lifestyle at work and at home.

Case Study Questions
1. What psychological and social issues need to be considered by the rehabilitation team working with Thomas?
2. What factors in Thomas’s life support his recovery and ultimate return to work?

Overview of Aphasia? Define
• A language disorder that is acquired sometimes after an individual has developed language competence.
Literal definition• “absence of language” or “without language”
Comprehensive definition• A disturbance in the language system after language has
been established or learned.
• Results from neurological injury to the language-dominant hemisphere of the brain.
• Includes disturbances of receptive or expressive abilities for spoken and written language
On Broca’s Aphasia
https://www.youtube.com/watch?v=AFphjX8kBHg
https://www.youtube.com/watch?v=xIvM4qdHAro
https://www.youtube.com/watch?v=O3P6Tq6UatI
What Could the Role of an SLP Look Like?
https://www.youtube.com/watch?v=OGyOKItHS9Y

What is Aphasia?
Considerations• Aphasia is not a developmental disorder
• Aphasia is not a psychiatric problem
• Aphasia is not a motor speech disorder.
Additional terminology• Dysarthria
• Apraxia

More on Aphasia Aphasia is distinct from developmental disorders of language and from
dysfunction of the motor pathways and muscles that produce speech (dysarthria). It is broadly divided into receptive and expressive aphasia.
Receptive (sensory, fluent, or Wernicke's) aphasia: Patients cannot comprehend words or recognize auditory, visual, or tactile symbols. It is caused by a disorder of the posterosuperior temporal gyrus of the language-dominant hemisphere (Wernicke's area). Often, alexia (loss of the ability to read words) is also present.
Expressive (motor, nonfluent, or Broca's) aphasia: The ability to create words is impaired, but comprehension and ability to conceptualize are relatively preserved. It is due to a disorder that affects the dominant left frontal or frontoparietal area, including Broca's area. It often causes agraphia (loss of the ability to write) and impairs oral reading.
There are other types of aphasia (see Table 1: Function and Dysfunction of the Cerebral Lobes: Types of Aphasia ), which may overlap considerably. No aphasia classification system is ideal. Describing the types of deficits is often the most precise way to describe a particular aphasia.
Types of Strokes
Ischemic strokes• Happen when the blood supply to the brain is inhibited
because of an occlusion somewhere in the artery.
• Thrombosis
• Embolism
Hemorrhagic strokes• Result when a blood vessel or artery ruptures and
excessive amounts of blood enter the brain.


How is Aphasia Classified?
The classification system for the aphasias is known as taxonomy; it draws upon those characteristics of aphasia that most differentiate disorders from one another and is similar to the way we might classify automobiles.
The Behavioral Symptoms
Some persons with aphasia are unable to initiate speech at all; others can initiate speech well but produce extended, flowery monologues that seem void of content and contain odd names for things.
In general, the language deficits seen in aphasia are differentiated by their impact on: fluency, motor output, comprehension, repetition, naming, and reading and writing.

Fluency
Define• A qualitative aspect of communication and speech
that is used to describe its forward flow, including its phrasing, intonation, and rate.
• Fluent speech
• Non-fluent
• Short, choppy phrases
• Slow, labored production of speech
• Grammatical errors
• Telegraphic quality
• AKA Sensory Aphasia

Motor Output
For some people with aphasia, particularly those whose speech is nonfluent, motor systems involved with speech are compromised, resulting in a motor speech disorder. This occurs when the areas of the brain controlling motor planning and programming for speech are injured. These individuals may show slow and labored articulation of sounds, with some groping of the articulators as they seek accurate placement.

Language Comprehension
Also called auditory comprehension is the ability to understand spoken language; this is not acuity or the ability to hear the message but rather the interpretation of what is heard.
Aphasia characterized by comprehension problems is often referred to as receptive aphasia, to emphasize its impact on language reception.
Repetition
Define• The ability to accurately reproduce verbal
stimuli on demand
The ability to repeat verbal stimuli is a major factor in differentiating among the aphasias, and for many people with aphasia, it is an ability that is seriously compromised.

Naming Also known as word retrieval, is the ability to
retrieve and produce a targeted word during conversation or more structured tasks.• Anomia- which literally means “no name,” is the
term used to describe word-finding problems or the inability to retrieve a word.
• Paraphasia is a type of language output error characterized by the production of unintended syllables, words, or phrases during the effort to speak.
• Phonemic “literal” – sound substitiutions but language-like
• Semantic – spoken word is related to the intended word.
Reading and Writing
The language deficits of people with aphasia may extend to the domains of reading and writing, which involve the comprehension and expression of written language.
Often reading and writing deficits parallel the verbal language deficits.
What are the Defining Characteristics of Aphasia Syndromes?
Studying the language difficulties of people with aphasia provides information for classifying the types of aphasia into syndromes.
1. Broca’s Area2. Transcortical Motor Aphasia3. Global Area4. Wernicke’s Area5. Transcortical Sensory Aphasia6. Conduction Aphasia7. Anomica Aphasia

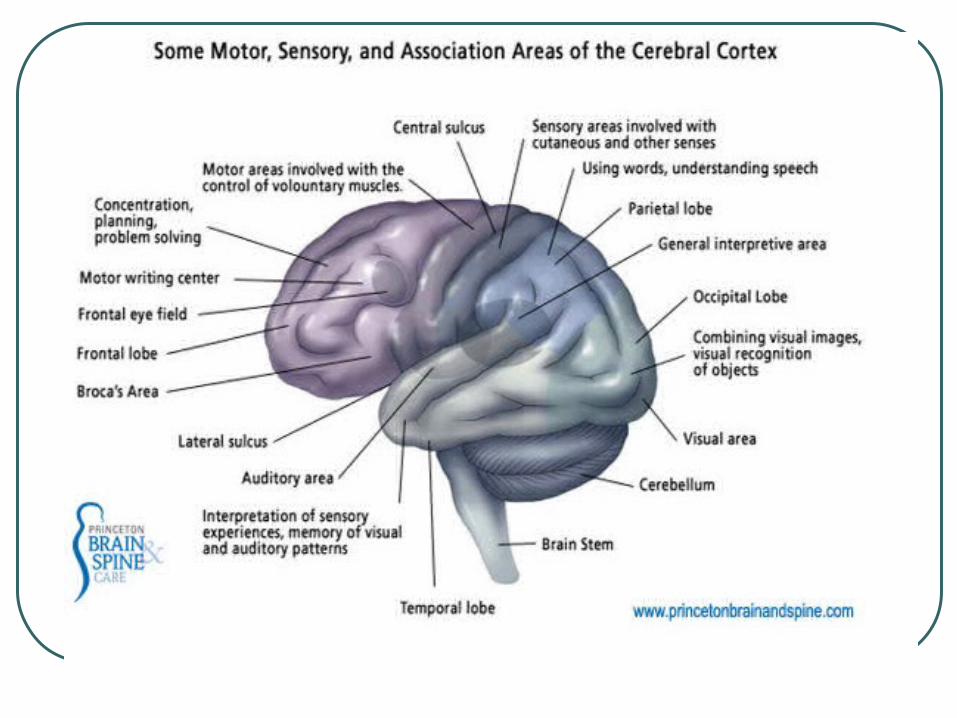
Broca’s Area
Broca’s Area aphasia results from damage to the frontal lobe of the brain.
Broca’s Area aphasia typically produces slowed, halting, and labored speech, yielding what some describe as a telegraphic or robot-like quality.
The person with Broca’s aphasia exhibits mild to moderate auditory comprehension problems, particularly when messages increase in length and complexity or when contextual cues are removed.
Transcortical Motor Aphasia
Transcortical motor aphasia results from damage to the frontal lobe, typically the superior and anterior portions.
The symptoms are similar to Broca’s aphasia except that these individuals have repetition skills that are far better than their spontaneous speech.
Most clients with this syndrome also demonstrate strong performance in oral reading.

Global Aphasia
“Global” aphasia occurs as a result of a large region of brain damage or multiple sites of brain injury in the language-dominant hemispheres.
Because this aphasia syndrome results in deficits across all language modalities, a person is likely to be non-fluent and have poor language comprehension.

Wernicke’s Aphasia Wernicke’s apasia results from brain injury to the
superior and posterior regions of the temporal lobe, possibly reaching to the parietal lobe of the language-dominant hemisphere.
The person with Wernicke’s aphasia produces spontaneous speech that flows well with normal prosody.• Prosody – patterns of stress and intonation• Logorrhea – extreme loquacity• Neologisms –creation of words that has meaning only to the
person who uses them• Jargon – speech incomprehensible but makes sense to the
person using it
http://www.youtube.com/watch?v=dKTdMV6cOZw

Transcortical Sensory Aphasia
Transcortical sensory aphasia results from injuries to the language-dominant hemisphere at the border of the temporal and occipital lobes or the superior region of the parietal lobe.
These clients have the classic symptoms of Wernicke’s profile except they have stellar repetition skills.
Echolalia
Conduction Aphasia
Conduction aphasia results from injury to the temporal-parietal region of the brain, typically a connecting pathway called the arcuate fasciculus.
Difficulties with repetition and reading aloud are the hallmark of conduction aphasia.
An inability to read aloud is a hallmark characteristic of this disorder.


Anomic Aphasia Anomic aphasia is not identified with a specific area
of the brain or a site of lesion. Anomic aphasia is fluent and expressive with
relatively few deficits in language expression and comprehension with the exception of naming.
This form of aphasia is the most pervasive type of chronic condition, even after treatment, and is the most common of aphasia profiles.

How is Aphasia Identified and Treated?
For the individual who has sustained neurological damage, the interdisciplinary rehabilitation team includes many people.
The speech-language pathologist’s assessment of speech and language functioning provides insight for the entire rehabilitation team.
Spontaneous recovery.

Assessment To diagnose aphasia and types of aphasia, a bedside evaluation either
by a speech-language pathologist or neuropsychologist is mandatory. He/she may conduct some tests and confirm the diagnosis of aphasia.
Some standardized tests for making aphasia diagnosis are Boston Diagnostic Aphasia Examination, Porch Index of Speech Ability, and Western Aphasia Battery. These examinations include testing the patient’s ability to speak, express ideas, understand language, read, and write. The above diagnostic tests indicate the severity and location of brain damage. Based on the test results, the aphasia type is determined, like fluent aphasia, nonfluent aphasia, or pure (specific selective deficit) aphasia.
MRI and CT scan also help ascertain the location and extent of brain damage. From this information, the aphasia type is established and prognosis of aphasia is made. Once aphasia type is diagnosed, specific aphasia treatments are started.

On Bedside Screening/EvaluationClinical bedside exploration of aphasia commonly includes: 1. Spontaneous, conversational speech. The clinician listens to andinteracts with the patient either during history taking or specifically toassess speech output. For example, "Tell me why you are in the hospital"can provide useful information on both fronts. "What did you eatfor breakfast (lunch) today?" is a reasonably good starting point, whena more neutral question is desired. Noting the fluency of output, effort,articulation, phrase length, dysprosody, paraphasic errors, and tendencyto omit words will help determine the presence of aphasic problems. 2. Repetition. Items here will usually begin with the repetition ofsingle digits and build up to the repetition of multisyllabic words,sentences, and verbal sequences.
More on Bedside Screening/Evaluations 3. Comprehension of spoken language. The clinician will attemptto determine whether the patient's ability to understand language is defectiveto a nature and degree that would suggest aphasia. If speaking is impaired, it maybe necessary to restrict the examination to questions that can be answered with"yes" or "no" responses or by having the patient point.
4. Word finding. Usually, the patient will be asked for the names ofcommon objects on the clinician's person (e.g., watch, pen) or in the patient's room (e.g., chair, telephone). Naming of object parts can occur along with naminggeneral objects, especially as this may elicit problems in persons with milder disorders (e.g., Albert et aI., 1981). This can be attempted first without and thenwith prompting. Frequently, the initial phoneme is offered as a cue, or an openended statement is provided to allow the word to be produced in an appropriate embedding or context. 5. Reading, usually from a newspaper or magazine or any item found in the patient's room (e.g., lunch menu). Unless the clinician car6

WAB Demonstration
https://www.youtube.com/watch?v=3s6afFPdRq0

Prognostic Indicator
Those variables that assist in predicting recovery: the site of the brain injury, the type and size of the injury, the type and severity of aphasia, handedness, age, preinjury health, and motivation for treatment.
Often, prognostic indicators are used to specify treatment.

Designing a Treatment Plans
The goal of aphasia treatment is to correct or compensate for speech language deficits so that individuals can communicate functionality in their daily routines.• Evidence-based practice – See the Practice
Portal!

An Example of Treatment
https://www.youtube.com/watch?v=B1SBFUgluK0

Working with Culturally and Linguistically Diverse Clients For individuals who speak multiple languages,
optimal testing procedures will evaluate them in all spoken languages.
Although there is still much to learn in this area of aphasia research, studies of bilingual persons with aphasia show several possible impacts:• Parallel impairments
• Differential impairment
• Differential aphasia
• Blended impairment
• Selective aphasia
Determining the Treatment Setting
Aphasia therapy is not limited to the speech-language pathologist and client working in a clinic or office setting. Therapies should encompass other environments to facilitate carryover and generalization of progress to different settings.
A group approach is another consideration for treating aphasia.

Measuring Outcomes
Effective language treatment for persons with aphasia should be measured based on their ability to communicate in real-world situations.• Real-world communication
• Functional outcomes
What are Right-Hemisphere Dysfunction, Traumatic Brain Injury, and Dementia?
Right-Hemisphere Dysfunction Traumatic Brain Injury Dementia
Right-Hemisphere Dysfunction
Define:• Results from neurological damage to the right
cerebral hemisphere Aphasia can result with left-hemisphere
damage; when damage affects the right hemisphere, language and cognition may be impacted, but the symptoms are quite different from those seen with aphasia.• Cognitive-linguistic disorder

Characteristics of RHD
1. Lack of awareness of cognitive-linguistic deficits and possible denial of problem areas.
2. Lack of awareness of the left side of the body and external stimuli to the left side.
3. Difficulty recognizing faces.4. Compromised pragmatics.5. A tendency toward using wordy expression providing
tangential information6. Difficulty understanding or using higher-level cognitive-
linguistic skills.7. Dysarthria or dysphagia when neuromuscular systems
are compromized.

Identification of RHD
Like left-hemisphere injury, right-hemisphere damage requires a comprehensive speech-language assessment as part of an interdisciplinary team assessment.
Specialized batteries are available specifically for the RHD population, such as the Mini Inventory of Right Brain Injury (MIRBI).
Treatment of RHD
Knowledge of treatments for RHD is more limited than that for left-hemisphere damage and aphasia. Initial therapy for RHD targets the management of attention and visual disruptions, since these impact productive treatment activities.
Therapy also targets higher-level cognitive-linguistic tasks, such as thinking through functional problems.
Traumatic Brain Injury
Define:• Refers to neurological damage to the brain resulting
from he impact of external forces. Epidemiology studies show that TBI is a
leading cause of death and disability in the United States.
Given the frequent long-term medical, vocational, and social needs of affected individuals, TBI represents a substantial health care issue in the United States.

Characteristics of TBI
Open-head• Occurs when the skull and the meninges
have been penetrated.
Closed-head injuries• The brain is jostled within the skull, yielding
diffuse to brain injury
Polytrauma
Identification of TBI The speech-language pathologist works as a
member of an of an interdisciplinary rehabilitation team to plan for treatment following a TBI.
The Glascow Coma Scale (GCS) rates the best-observed response for eye opening, verbal response, and motor response to characterize and individual’s functioning from severe TBI to mild TBI.


Treatment of TBI
Treatment interventions will vary according to an individual’s level of impairment as reflected by the Rancho scales.• Levels I to III: severe
• Level IV to VI: middle
• Level VII to X: mildhttp://tbims.org/combi/lcfs/lcfs.pdf
What is Dementia?
Define:• A chronic and progressive decline in memory,
cognition, language, and personality resulting from central nervous system dysfunction.
The diagnostic criteria of the American Psychiatric Association identify three defining traits of dementia:• Memory impairment
• Impairment in cognition skills
• Presence of aphasia, apraxia, or agnosia.
Identification of Dementia
A team of professionals evaluates suspected dementia to verify its presence, cause, and course of intervention. Medical testing will rule out other treatable illness that may appear like dementia.
More comprehensive testing by the speech-language pathologist typically involves the complete Arizona Battery for Communication Disorders of Dementia.

Treatment of Dementia
Research continue to develop more effective pharmacological treatments to combat degenerative changes associated with dementia. The majority of medications currently approved by the Food and Drug Administration for dementia target those individuals in mild to moderate stages.

On Alzheimer’s
https://www.youtube.com/watch?v=9Wv9jrk-gXc
Glen Campbell http://www.nbcnews.com/watch/nightly-news/
inside-country-legend-glen-campbells-battle-with-alzheimers-338802243712
https://www.youtube.com/watch?v=ED6upzp3reo
http://youtu.be/U8TsAh-zYFI












![Cognitive dysfunction in sleep disorders · COGNITIVE DYSFUNCTION IN SLEEP DISORDERS 425 Table 1 Neuropsychological tasks Perception (1–6) 1- Graphesthesia [12], 2- Hooper Visual](https://static.documents.pub/doc/80x56/5e0c9b08b929f624b50d2189/cognitive-dysfunction-in-sleep-disorders-cognitive-dysfunction-in-sleep-disorders.jpg)




