52
Wake County EMS System ADULT PROTOCOLS

Wake County EMS System
ADULT
PROTOCOLS

Wake County EMS System Protocols
Cardiac ArrestHistory:
Events leading to arrestEstimated downtimePast medical historyMedicationsExistence of terminal i llnessSigns of lividity, rigor mortisDNR
Signs and Symptoms:UnresponsiveApneicPulseless
Pearls:Exam: Mental Status
Success is based on proper planning and execution. Procedures require space and patient access. Make room towork.
If witnessed arrest - administer a precor dial thump. Reassess airway frequently and with every patient move. Maternal Arrest - Treat mother per appropriate protocol with immediate notification t o Medical Control and rapid
transport. Adequate compressions with timely defibrillation are the key s to success.
Go to appropriate protocol: Ventricular Fibrillation
Pulseless Ventricular TachycardiaPulseless Electrical Activity
AsystolePediatric Pulseless Arrest
Begin Continuous Compressions
Automated DefibrillationProcedure
Version 1.1
No
Withholdresuscitation Yes
Differential:Medical vs TraumaV. fib vs Pulseless V. tachAsystolePulseless electrical activity (PEA)
Universal Patient Care Protocol
Criteria for Death / No Resuscitation
Assess Rhythm
AT ANY TIMEReturn of
Spontaneous CirculationGo to
Post ResuscitationProtocol
I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
I
ALS Available?
No Yes
Airway Procedure
Interrupt Compressions Only as per AEDProcedure. Ventilate no more than 12breaths per minute (1 breath every 5
seconds)
CA-1
No
Yes
Wake EMS System
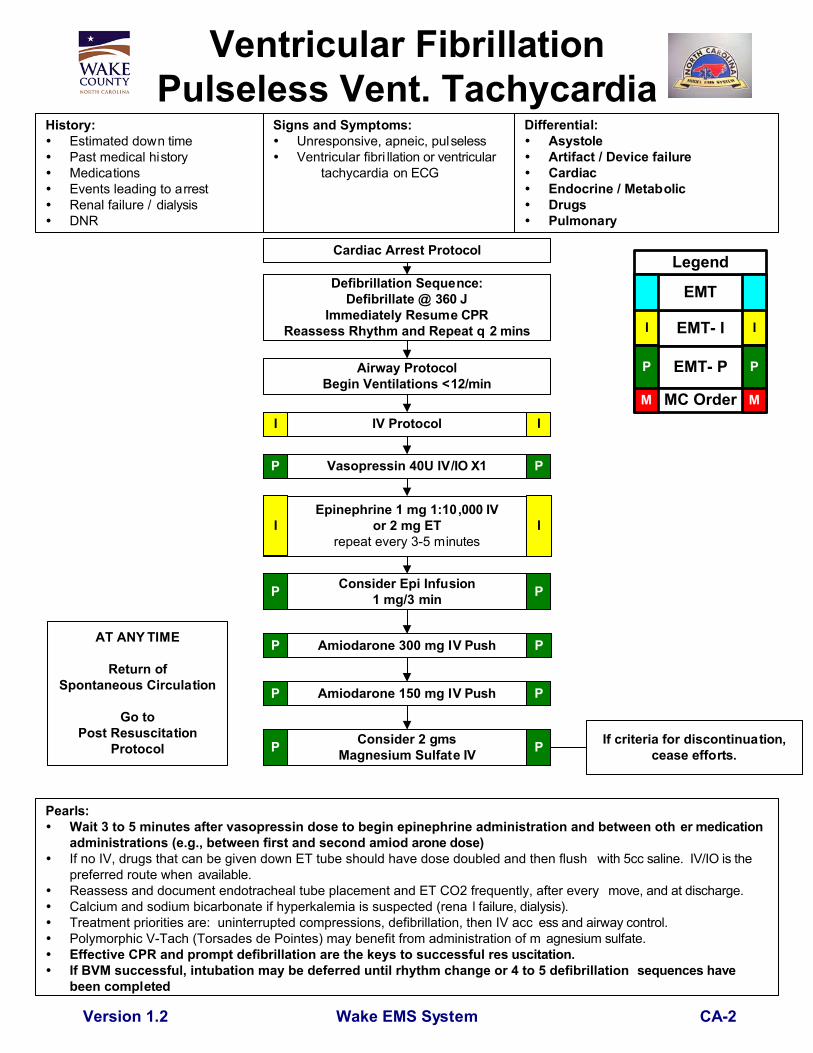
Ventricular FibrillationPulseless Vent. Tachycardia
Cardiac Arrest Protocol
Epinephrine 1 mg 1:10,000 IVor 2 mg ET
repeat every 3-5 minutes
Amiodarone 300 mg IV Push
Consider Epi Infusion1 mg/3 min
Consider 2 gmsMagnesium Sulfate IV
Airway ProtocolBegin Ventilations <12/min
History:Estimated down timePast medical historyMedicationsEvents leading to arrestRenal failure / dialysisDNR
Signs and Symptoms:Unresponsive, apneic, pulselessVentricular fibri llation or ventricular
tachycardia on ECG
IV Protocol
Pearls:Wait 3 to 5 minutes after vasopressin dose to begin epinephrine administration and between oth er medicationadministrations (e.g., between first and second amiod arone dose)If no IV, drugs that can be given down ET tube should have dose doubled and then flush with 5cc saline. IV/IO is thepreferred route when available.Reassess and document endotracheal tube placement and ET CO2 frequently, after every move, and at discharge.Calcium and sodium bicarbonate if hyperkalemia is suspected (rena l failure, dialysis).Treatment priorities are: uninterrupted compressions, defibrillation, then IV acc ess and airway control.Polymorphic V-Tach (Torsades de Pointes) may benefit from administration of m agnesium sulfate.Effective CPR and prompt defibrillation are the keys to successful res uscitation.If BVM successful, intubation may be deferred until rhythm change or 4 to 5 defibrillation sequences havebeen completed
Version 1.2
Differential:AsystoleArtifact / Device failureCardiacEndocrine / MetabolicDrugsPulmonary
AT ANY TIME
Return ofSpontaneous Circulation
Go toPost Resuscitation
Protocol
I I
I I
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Defibrillation Sequence:Defibrillate @ 360 J
Immediately Resume CPRReassess Rhythm and Repeat q 2 mins
PP
Vasopressin 40U IV/IO X1P P
Amiodarone 150 mg IV PushP P
P P
CA-2
If criteria for discontinuation,cease efforts.

Wake County EMS System Protocols
Epinephrine 1 mg 1:10,000 IV q 3 min
IV Protocol
AsystoleHistory:
Past medical historyMedicationsEvents leading to arrestEnd stage renal diseaseEstimated downtimeSuspected hypothermiaSuspected overdoseDNR
Signs and Symptoms:PulselessApneicNo electrical activit y on ECGNo auscultated heart tones
Version 1.2
Consider Correctable Causes
I
Criteria for DiscontinuationStopresuscitation
Pearls:Exam: Mental StatusAlways confirm asystole in more t han one lead.Correctable causes must be addre ssed.
Differential:Medical or TraumaHypoxiaPotassium (hypo / hyper)Drug overdoseAcidosisHypothermiaDevice (lead) errorDeath
Universal Patient Care Protocol
Cardiac Arrest Procedure
Atropine 1 mg IV up to 3 mg
AT ANY TIME
Return ofSpontaneous Circulation
Go toPost Resuscitation
Protocol
External Transcutaneous PacingP
I
P
I I
P P
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Vasopressin 40 IU IVP
Correctable Causes:AcidosisHypovolemiaHypothermiaHypoglycemiaHyperkalemiaOverdose (Narcotics,TricyclicAntidepressants,Calcium ChannelBlockers, BetaBlockers)TensionPneumothorax
If no IVEpi 1:10,000 2 mg ET q 3 minI I
Yes
Continue Epinephrine, Consideration ofCorrectable Causes
II
No
Yes
CA-3
II

Wake County EMS System Protocols
Pulseless Electrical Activity (PEA)
Signs and Symptoms:PulselessApneicElectrical activity on ECGNo heart tones on auscultation
Version 1.2
Consider early in all PEA pts:
No
Continue Resuscitation
Yes Stopresuscitation
Differential:Hypovolemia (Trauma, AAA, other)Cardiac tamponadeHypothermiaDrug overdose (Tricyclics, Digitalis,Beta blockers, Calcium channelblockers)Massive myocardial infarctionHypoxiaTension pneumothoraxPulmonary embolusAcidosisHyperkalemia
Cardiac Arrest Protocol
Airway and IVProtocols
History:Past medical historyMedicationsEvents leading to arrestEnd stage renal diseaseEstimated downtimeSuspected hypothermiaSuspected overdose
TricyclicsDigitalisBeta blockersCalcium channel b lockers
DNR
Epinephrine1mg 1:10,000 IV (2 mg ET)
q 2-5 min
Atropine (if rate < 60)1 mg q 5 min up to 3 mg
Criteria for Discontinuation
Pearls:Exam: Mental StatusConsider each possible cause listed in the differential: Survival is based on identify ing and correcting the cause!Discussion with Medical Control can be a valuable tool in developing a differentia l diagnosis and identifying possibletreatment options.
AT ANY TIME
Return ofSpontaneous Circulation
Go toPost Resuscitation
Protocol
I I
P P
P P
Fluid bolusD50 25 grams IVNarcan 2-4 mg IVCalcium 1 gram IV (hyperkalemia)Bicarbonate 1 meq/kg IV(tricyclic overdose, hyperkalemia,renal failure)Dopamine 2-20 mcg/kg/minPacingChest decompressionGlucagon 1 mg IV (Beta blocker)
I I
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
ConsiderEpinephrine Drip 1 mg/3 minP P
Vasopressin 40U IV
CA-4
II
Wake County EMS System Protocols
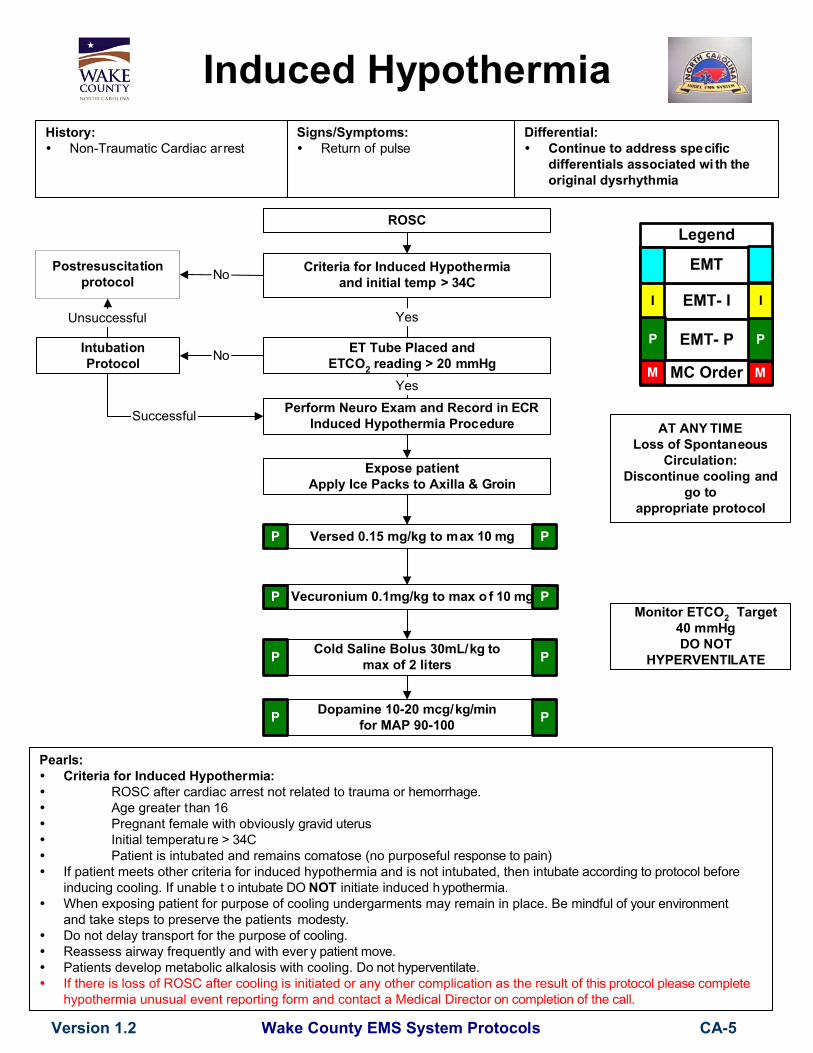
Induced Hypothermia
Pearls:Criteria for Induced Hypothermia:
ROSC after cardiac arrest not related to trauma or hemorrhage.Age greater than 16Pregnant female with obviously gravid uterusInitial temperature > 34CPatient is intubated and remains comatose (no purposeful response to pain)
If patient meets other criteria for induced hypothermia and is not intubated, then intubate according to protocol beforeinducing cooling. If unable t o intubate DO NOT initiate induced hypothermia.When exposing patient for purpose of cooling undergarments may remain in place. Be mindful of your environmentand take steps to preserve the patients modesty.Do not delay transport for the purpose of cooling.Reassess airway frequently and with ever y patient move.Patients develop metabolic alkalosis with cooling. Do not hyperventilate.If there is loss of ROSC after cooling is initiated or any other complication as the result of this protocol please completehypothermia unusual event reporting form and contact a Medical Director on completion of the call.
Expose patientApply Ice Packs to Axilla & Groin
Cold Saline Bolus 30mL/kg tomax of 2 liters
Version 1.2
Postresuscitationprotocol No
ROSC
Criteria for Induced Hypothermiaand initial temp > 34C
AT ANY TIMELoss of Spontaneous
Circulation:Discontinue cooling and
go toappropriate protocol
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Versed 0.15 mg/kg to max 10 mg
Dopamine 10-20 mcg/kg/minfor MAP 90-100
Monitor ETCO2 Target40 mmHgDO NOT
HYPERVENTILATE
CA-5
Vecuronium 0.1mg/kg to max o f 10 mg
P
PP
PP
P
PP
ET Tube Placed andETCO2 reading > 20 mmHg
Yes
IntubationProtocol No
History:Non-Traumatic Cardiac ar rest
Signs/Symptoms:Return of pulse
Differential:Continue to address specificdifferentials associated wi th theoriginal dysrhythmia
Perform Neuro Exam and Record in ECRInduced Hypothermia Procedure
Yes
Successful
Unsuccessful

Unattended Death: (Patient h as no knownprimary care physician). Contact State Medical
Examiner at 919-966-2253. Coordi nate with LawEnforcement. Leave all medical dev ices in place.
If devices have been removed, tape them across thechest of the patient. Do not place sha rps under tape
but rather note the devices in writi ng on the tape.
History:Patient encountered by EMSwho meets criteria forobvious deathPatient with DNR order inplace who is pulseless andapneicPatient for whomresuscitation effor ts areceased on-scene
Yes
Wake County EMS System Protocols
Deceased Persons
Version 1.2
No
Pearls:The body of a deceased person may be released to the funeral home if the death is attended (t he patient has aprimary care physician) and law enforcement confirms the death is non-suspicious. It is pre ferred (but notmandatory) to communicate directly with the primary care physician prior to releasing t he body. Allreasonable attempts should be made to contact the primary prior to releas ing the body.If there is no primary care physician, the Office of the State Medical Examiner mus t be contacted.If the death is traumatic in nature, the Office of the State Medical Examiner must be contacted.A patient has a primary care physician if there are in-date prescriptions from the physician, the family knowsthe name of the physician and can verify the patient still is seen by that physician, or o ther methods asapproved by medical control.
Key Information:Name of Primary CarePhysicianKnown medical conditionsLast time known to be alive
Differential:Attended Death (a patient with aprimary care physician who apparentlydied of medical causes (aka "naturaldeath")Unattended Death (a patient without aprimary care physician who apparentlydied of medical causes (aka " a naturaldeath")Suspicious Death (law enforcement)
Patient meets criteria forobvious death?
Patient Meets Criteriafor Discontinuation?
No
Attended Death? (Patient has pr imary carephysician who can be identified).
Attempt to contact primary care physician.
Contact made with primary ca re physicianand/or on-call physician?
Law Enforcment and/or EMSRecognize Suspicious Death?
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
CA-6
Continue with ResusciationPer Appropriate Protocol No
Coordinate with LawEnforcement
P P
Coordinate with LawEnforcement
Yes
Release of the body is appropri ate. Medicaldevices may be removed.
Describe case andobtain name of physicianto sign death certificate.Give information to law
enforcement
Confirm name ofprimary care physician
from family. Giveinformation to law
enforcement.
Yes
Yes
No Yes
No
Wake County EMS System ProtocolsVersion 1.2
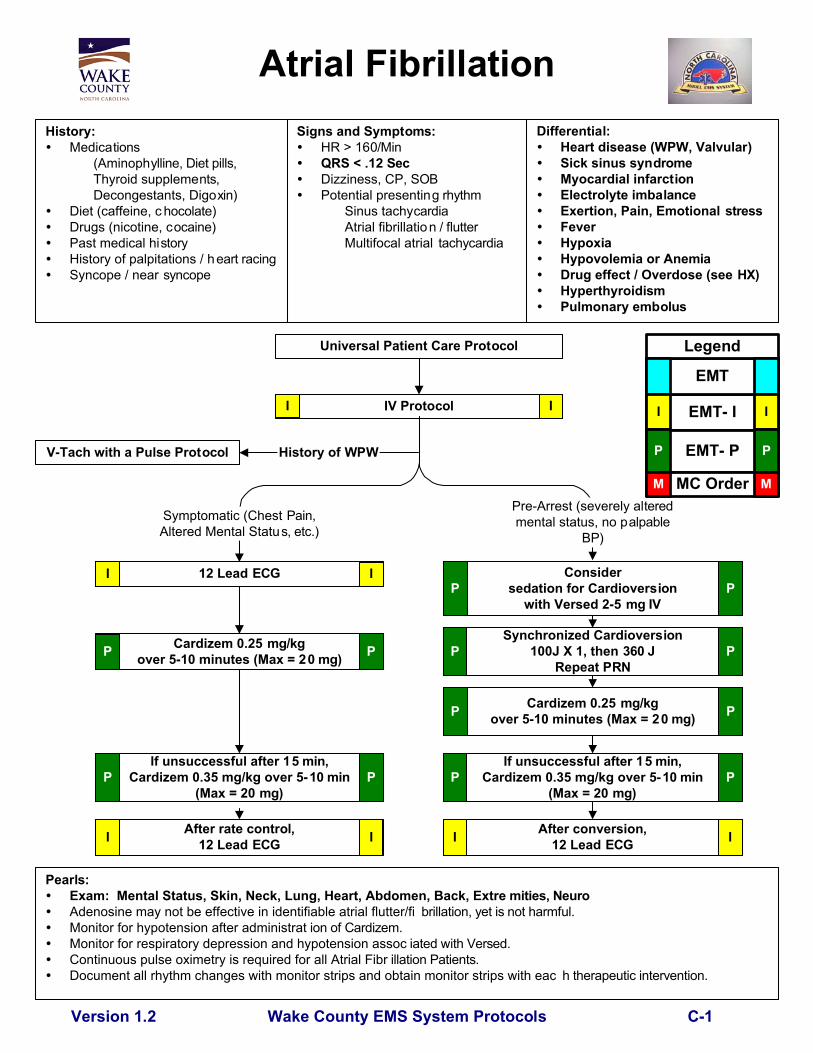
Atrial FibrillationHistory:
Medications(Aminophylline, Diet pills, Thyroid supplements,Decongestants, Digoxin)
Diet (caffeine, c hocolate)Drugs (nicotine, cocaine)Past medical historyHistory of palpitations / heart racingSyncope / near syncope
Signs and Symptoms:HR > 160/MinQRS < .12 SecDizziness, CP, SOBPotential presenting rhythm
Sinus tachycardiaAtrial fibrillation / flutterMultifocal atrial tachycardia
Pearls:Exam: Mental Status, Skin, Neck, Lung, Heart, Abdomen, Back, Extre mities, NeuroAdenosine may not be effective in identifiable atrial flutter/fi brillation, yet is not harmful.Monitor for hypotension after administrat ion of Cardizem.Monitor for respiratory depression and hypotension assoc iated with Versed.Continuous pulse oximetry is required for all Atrial Fibr illation Patients.Document all rhythm changes with monitor strips and obtain monitor strips with eac h therapeutic intervention.
If unsuccessful after 15 min,Cardizem 0.35 mg/kg over 5-10 min
(Max = 20 mg)
After rate control,12 Lead ECG
Considersedation for Cardioversion
with Versed 2-5 mg IV
Synchronized Cardioversion100J X 1, then 360 J
Repeat PRN
Cardizem 0.25 mg/kgover 5-10 minutes (Max = 20 mg)
Differential:Heart disease (WPW, Valvular)Sick sinus syndromeMyocardial infarctionElectrolyte imbalanceExertion, Pain, Emotional stressFeverHypoxiaHypovolemia or AnemiaDrug effect / Overdose (see HX)HyperthyroidismPulmonary embolus
Universal Patient Care Protocol
IV Protocol
12 Lead ECG
Symptomatic (Chest Pain,Altered Mental Status, etc.)
Pre-Arrest (severely alteredmental status, no palpable
BP)
I I
P P
P P
P
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
P
After conversion,12 Lead ECG
Cardizem 0.25 mg/kgover 5-10 minutes (Max = 20 mg)P P
V-Tach with a Pulse Protocol History of WPW
I I
I I II
C-1
If unsuccessful after 15 min,Cardizem 0.35 mg/kg over 5-10 min
(Max = 20 mg)P P

Wake County EMS System Protocols
BradycardiaHistory:
Past medical historyMedications
Beta-Blockers(Toprol, Atenolol)Calcium channel blockers(Verapamil, Calan)ClonidineDigitalis
Pacemaker
Signs and Symptoms:HR < 60/minChest painRespiratory distressHypotension or ShockAltered mental statusSyncope
Pearls:Exam: Mental Status, Neck, Heart, Lungs, Neuro
The use of lidocaine in heart block can worsen bradycardia and lead to asystole and death. Pharmacological treatment of Bradycardia is based upon the presence or absence of symptoms.
If symptomatic, treat. If asymptomatic, monitor only. Remember: The use of Atropine for PVC's in the presence of an MI may worsen heart damage. Consider treatable causes for bradycardia (Beta blocker OD, Calcium channel blocker OD, etc.) Be sure to aggressively oxygenate the patient and support respiratory effort.
HypotensionBlood Pressure <90 Systolic and/or
symptomatic
Differential:Acute myocardial infarctionHypoxiaHypothermiaSinus bradycardiaAthletes
Head injury (eleva ted ICP) orStrokeSpinal cord lesionSick sinus syndromeAV blocks (1°, 2°, or 3°)Overdose
Version 1.1
Universal Patient Care Protocol
IV Protocol / Fluid Bolus PRNI
Atropine 0.5-1 mg IV up to 3 mgP
External Transcutaneous PacingConsider sedation with Versed 2 mg IV
Consider Dopamine 2-20 mcg/kg/min
Monitor
12 Lead ECG
Not Second or ThirdDegree Heart Block
Second or ThirdDegree Heart Block
I
P
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
No
PP
External Transcutaneous PacingConsider sedation with Versed 2 mg IV
Atropine 0.5-1 mg up to 3 mg
Consider Dopamine 2-20 mcg/kg/min
ConsiderEpinepherine 0.2-0.3 mg 1:10,000 IV orEpinephrine Drip 1 mcg/min to HR >60
P P
PP
PP
PP
I I
ConsiderEpinepherine 0.2-0.3 mg 1:10,000 IV orEpinephrine Drip 1 mcg/min to HR >60
PP
C-2
No

Wake County EMS System Protocols
Continued pain?
Chest PainSuspected Cardiac Event
History:AgeMedicationsViagra, Levitra, CialisPast medical history (MI, Angina,Diabetes, Post Menopausal)Allergies (Morphine, Lidocaine)Recent physical exertionOnsetPalliation / ProvocationQuality (crampy, constant, sharp,dull, etc.)Region / Radiation / ReferredSeverity (1-10)Time (duration / repetition)
Signs and Symptoms:CP (pain, pressure, aching, vice-like tightness)Location (substernal, epigastric,arm, jaw, neck, shoulder)Radiation of painPale, diaphoresisShortness of breathNausea, vomiting, dizziness
Hypotension / DysrhythmiasTreat per Protocol
Version 1.2
Pearls:Exam: Mental Status, Skin, Neck, Lung, Heart, Abdomen, Back, Extremities, NeuroAvoid Nitroglycerin in any patient who has used Viagra or Levitra in the past 24 hours or Cialis in the past 36hours due to potential severe hypotension.If patient has taken nitroglycerin without relief, consider potency of the medication.If conditions prevent indicated doses of SL NTG from beng administered, move to NTG paste after 1st SL sprayIf positive ECG changes, establish a second IV while en route to the hospital.Monitor for hypotension after administration of nitroglycerin and morphine.Patients with chest pain but who do not have ST-segment elevation on their EKG should be transported to the hospitalof their choice. Only STEMI patients should be encouraged to go to Cath Lab Capable FacilityDiabetics and geriatric patients often have atypical pain, or only generalized complaints.Document 12-lead and transmission status using "12-lead EKG" procedure in the call reporting system
Differential:Trauma vs. MedicalAngina vs. Myocardial infarctionPericarditisPulmonary embolismAsthma / COPDPneumothoraxAortic dissection or aneurysmGE reflux or Hiatal herniaEsophageal spasmChest wall injury or painPleural painOverdose (Cocaine)
Universal Patient Care Protocol
12-Lead ECG
Nitroglycerin 0.4 mg SLq 5 minutesIf SBP > 90
IV Protocol
Aspirin 324 mg PO(Unless documented Aspirin allergy)
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M MI I
Morphine 2-5 mg slow IV up to 10 mg and / or
Nitroglycerin 0.4 mg SL q 5 minsIf SBP > 90
P P
Apply 1" Nitrogylcerin Paste to Chest Wall
If SBP > 90
Acute MI with STSegment Elevation
Transport within 15 minutesof arriving on scene to an
Interventional Cardiac CathLab Capable Facility.
Attempt to Transmit EKG.
For severe nausea or vomitingZofran 4 mg IV/IM
I I
I I
II
PP
II
Consider Fluid Bolus forInferior MIs
C-3

Pearls:Exam: Mental Status, Neck, Skin, Lungs, Heart, Abdomen, Extremit ies, NeuroHyperventilation is a significant cause of hypotension and recurrance of cardiac arrest in the post resuscitation phaseand must be avoided at al l costs.Most patients immediately post resuscitation will require vent ilatory assistance.The condition of post-resuscitation patients fluctuates rapidly and continuously, and they require close monitoring.Appropriate post-resuscitation management may be planned in consultat ion with medical control.Common causes of post-resuscitation hypotension include hyperventilation, hypovo lemia, pneumothorax, andmedication reaction to A LS drugs.Titrate Dopamine to maintain MAP >90. Ensure adequate fluid resu scitation is ongoing.
Wake County EMS System Protocols
Post Resuscitation
Repeat Primary Assessment
Patient potential candid ate for inducedhypothermia?
Monitor ECG
Consider 1000 ccNS fluid bolus
Treat perBradycardia Protocol
Go to AppropriateProtocol
If arrest reoccurs, revert to app ropriateprotocol and/or initial successfu l treatment
Version 1.2
History:Respiratory arrestCardiac arrest
Signs/Symptoms:Return of pulse
Differential:Continue to address specificdifferentials associated wi th theoriginal dysrhythmia
IV Protocol
Bradycardia
Dopamine 2-20 mcg/kg/minfor BP < 90
Hypotension
I I
I I
P PP P
Vital Signs
Pulse oximetry
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
12 Lead EKG II
Significant Ectopy
Monitor ETCO2 (ideal > 20 mmHg) with RR<12 unless otherwise indicated. D O NOT
HYPERVENTILATE.
No
I I
C-4
Go to Induced HypothermiaProtocol Yes

Wake County EMS System ProtocolsVersion 1.2
Supraventricular Tachycardia
History:Medications
(Aminophylline, Diet pills, Thyroid supplements,Decongestants, Digoxin)
Diet (caffeine, c hocolate)Drugs (nicotine, cocaine)Past medical historyHistory of palpitations / heart racingSyncope / near syncope
Signs and Symptoms:HR > 150/MinQRS < .12 Sec (QRS > .12 secgo to V-Tach Protocol)If history of WPW, go to V-Tach ProtocolDizziness, CP, SOBPotential presenting rhythm
Sinus tachycardiaAtrial fibrillation / flutterMultifocal atrial tachycardia
Pearls:Exam: Mental Status, Skin, Neck, Lung, Heart, Abdomen, Back, Extre mities, NeuroIf patient has history of or 12 Lead ECG reveals Wolfe Parkinson White (WPW), DO NOT administer Cardizem.Adenosine may not be effective in identifiable atrial flutter/fi brillation, yet is not harmful.Monitor for hypotension after administrat ion of Cardizem.Monitor for respiratory depression and hypotension assoc iated with Versed.Continuous pulse oximetry is required for all SV T Patients.Document all rhythm changes with monitor strips and obtain monitor strips with each therapeutic intervention.
May attemptValsalva's maneuver
initially and afte r each drugadministration if indicated.
Adenosine12 mg rapid IV
No change, 12 mg rapid IVuse 10 cc flush after each dose
Cardizem 0.25 mg/kg s low IV(Max = 20 mg)
Consider Adenosine12 mg rapid IV
with 10 cc flushSedate for Cardioversion
with Versed 2-5 mg IV
Synchronized Cardioverion100J X 1, then 360J
Repeat PRN
Cardizem 0.25 mg/kg s low IV(Max = 20 mg)
Differential:Heart disease (WPW, Valvular)Sick sinus syndromeMyocardial infarctionElectrolyte imbalanceExertion, Pain, Emotional stressFeverHypoxiaHypovolemia or AnemiaDrug effect / Overdose (see HX)HyperthyroidismPulmonary embolus
Universal Patient Care Protocol
IV Protocol
12 Lead ECG
StablePre-arrest
(No palpable BP, Alteredmental status)
I I
P P
P P
P
P P
P P
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
12 Lead ECG after conversionI
I I
IP
C-5

If No Response, RepeatAmiodarone 150 mg IV
Over 10 Minutes
Wake County EMS System Protocols
Ventricular Tachycardia/Wide Complex with Pulse
History:Past medical history /medications, diet, drugs.Syncope / near syncopePalpitationsPacemakerAllergies: lidocaine / novacaine
Signs and Symptoms:Ventricular tachycardia on ECG(Runs or sustained)Conscious, rapid pulseChest pain, shortness of breathDizzinessRate usually 150 - 180 bpm forsustained V-TachQRS > .12 Sec
Universal Patient Care Protocol
VentricularFibrillationProtocol
Palpable pulse ?
Yes
No
Pearls:Exam: Mental Status, Skin, Neck, Lung, Heart, Abdomen, Back, Extremities, NeuroFor witnessed / monitored ventricular tachycardia, try having patient cough or deliver a precordial thump.Polymorphic V-Tach (Torsades de Pointes) may benefit from the administration of magnesium sulfate 2 grams IV.If presumed hyperkalemia (end-stage renal disease, dialysis, etc), administered 1 to 2 amps of Sodium Bicarbonate
Version 1.3
Differential:Artifact / Device failureCardiacEndocrine / MetabolicHyperkalemiaDrugsPulmonary
Amiodarone 150 mg IVOver 10 minutes
Repeat Amiodarone150 mg IV
Over 10 minutes
Synchronized Cardioversion100 J
If No Response, thenSynchronized Cardioversion
360J (repeat prn)
IV Protocol
12-Lead ECG
Amiodarone 150 mg IVOver 10 Minutes
StablePre-arrest
(No palpable BP, Alteredmental status)
I I
P P
For sedation considerVersed 2.5-5 mg IV/IM/INP P
P P
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
No Response
PP
No Response
PPIf patient becomes unstable,consider move to pre-arrest
portion of protocolP P
P PAfter conversion12-Lead ECGI I
I I
C-6

Wake County EMS System Protocols
If equipment failure, utili ze equipment failureprocedure and complete the Wake EMSSystem Clinical Unusual Event Report
Patient Safety
Follow Universal Patient Care Protcol
Document at least once per shift the presence ofall equipment, medications, and supplies
listed on the Model System Ramp InspectionForm
If massive depletion of supplies (e.g, post-cardiac arrest) and/or contamination, remain
out-of-service until resupplied and clean
If supplies fall below required levels, restockat the nearest appropriate location. If
dispatched to a call that may require depletedsupplies, respond and call for next near unit.
If medication error, clinical misadventure, orother adverse patient outcome, contact
medical director via policy below.
Medical Director Notification Policy:If any events as listed in the Automatic Medical Director Notification section of the Foundations of Practice occur, notify themedical director immediately. If no answer with cell phone, call RWCC Rescom for further assistance.If any other adverse clinical outcome, notify the medical director as soon as possible via email and/or cell phone. Theprobability of utilization of the Disciplinary Procedure is greatly diminished if the provider with a misadventure contacts themedical director directly.If an error occurs without adverse patient outcome and/or a "near miss" occurs, complete the Wake County EMS SystemClinical Unusual Event Report.
Appropriate protocol Patient doesn't fit a protocol?Contact Medical Control
Version 1.1
M M
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Utilize Pre-printed Drug Dose CardsFor All Weight-Based Drug Administration
Verify correct drug and dose prior toadministration
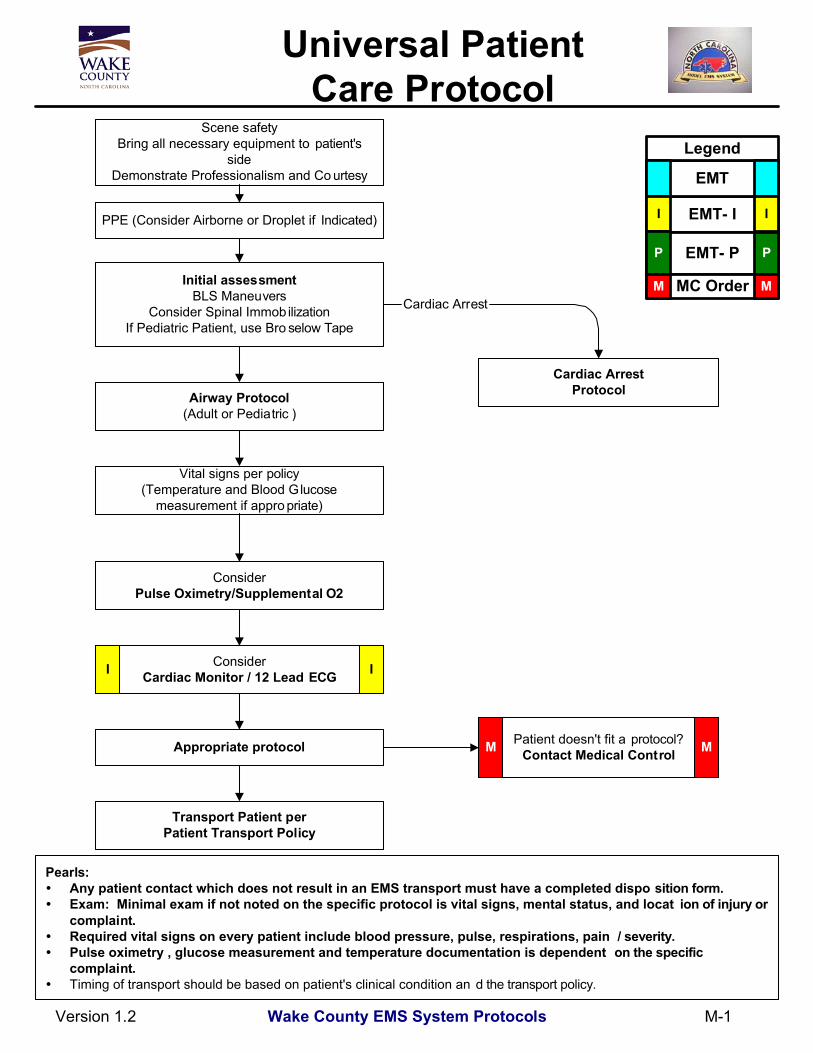
Transport Patient perPatient Transport Policy
M - 0
Wake County EMS System Protocols
ConsiderPulse Oximetry/Supplemental O2
Universal Patient Care Protocol
Scene safetyBring all necessary equipment to patient's
sideDemonstrate Professionalism and Co urtesy
Initial assessmentBLS Maneuvers
Consider Spinal ImmobilizationIf Pediatric Patient, use Bro selow Tape
Vital signs per policy(Temperature and Blood Glucose
measurement if appro priate)
Airway Protocol(Adult or Pediatric )
ConsiderCardiac Monitor / 12 Lead ECG
Pearls:Any patient contact which does not result in an EMS transport must have a completed dispo sition form.Exam: Minimal exam if not noted on the specific protocol is vital signs, mental status, and locat ion of injury orcomplaint.Required vital signs on every patient include blood pressure, pulse, respirations, pain / severity.Pulse oximetry , glucose measurement and temperature documentation is dependent on the specificcomplaint.Timing of transport should be based on patient's clinical condition an d the transport policy.
Appropriate protocol Patient doesn't fit a protocol?Contact Medical Control
Version 1.2
Cardiac Arrest
Cardiac ArrestProtocol
I I
M M
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
PPE (Consider Airborne or Droplet if Indicated)
Transport Patient perPatient Transport Policy
M-1
Wake County EMS System Protocols
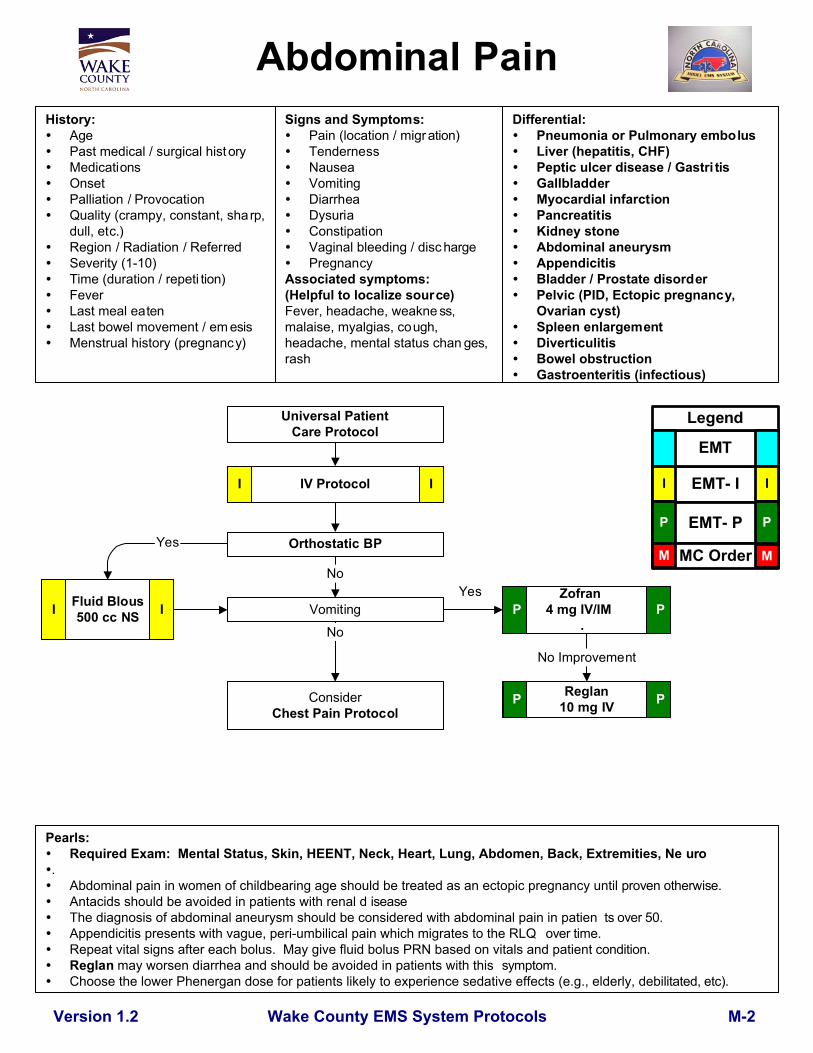
Abdominal PainHistory:
AgePast medical / surgical hist oryMedicationsOnsetPalliation / ProvocationQuality (crampy, constant, sharp,dull, etc.)Region / Radiation / ReferredSeverity (1-10)Time (duration / repeti tion)FeverLast meal eatenLast bowel movement / em esisMenstrual history (pregnancy)
Signs and Symptoms:Pain (location / migration)TendernessNauseaVomitingDiarrheaDysuriaConstipationVaginal bleeding / disc hargePregnancy
Associated symptoms:(Helpful to localize source)Fever, headache, weakne ss,malaise, myalgias, cough,headache, mental status chan ges,rash
Pearls:Required Exam: Mental Status, Skin, HEENT, Neck, Heart, Lung, Abdomen, Back, Extremities, Ne uro
.Abdominal pain in women of childbearing age should be treated as an ectopic pregnancy until proven otherwise.Antacids should be avoided in patients with renal d iseaseThe diagnosis of abdominal aneurysm should be considered with abdominal pain in patien ts over 50.Appendicitis presents with vague, peri-umbilical pain which migrates to the RLQ over time.Repeat vital signs after each bolus. May give fluid bolus PRN based on vitals and patient condition.Reglan may worsen diarrhea and should be avoided in patients with this symptom.Choose the lower Phenergan dose for patients likely to experience sedative effects (e.g., elderly, debilitated, etc).
Version 1.2
Differential:Pneumonia or Pulmonary embolusLiver (hepatitis, CHF)Peptic ulcer disease / Gastri tisGallbladderMyocardial infarctionPancreatitisKidney stoneAbdominal aneurysmAppendicitisBladder / Prostate disorderPelvic (PID, Ectopic pregnancy,Ovarian cyst)Spleen enlargementDiverticulitisBowel obstructionGastroenteritis (infectious)
Universal PatientCare Protocol
IV ProtocolI I
Orthostatic BP
Vomiting Zofran
4 mg IV/IM.
PP
ConsiderChest Pain Protocol
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Reglan10 mg IVP P
Yes
No
No Improvement
Fluid Blous500 cc NS
Yes
No
I I
M-2

Wake County EMS System Protocols
Epinephrine 0.3 mg 1:1000via Autojector
Allergic ReactionHistory
Onset and locationInsect sting or biteFood allergy / exposureMedication allergy / exposureNew clothing, soap, detergentPast history of reactionsPast medical historyMedication history
Signs and Symptoms:Itching or hivesCoughing / wheezing orrespiratory distressChest or throat constrictionDifficulty swallowingHypotension or shockEdema
Pearls:Exam: Mental Status, Skin, Heart , LungsContact Medical Control prior to administering epinephrine in patients who are >50 years of age, h ave a historyof cardiac disease, or if the patient's heart rate is >150. Epinephrine may precipitate card iac ischemia. Thesepatients should receive a 12 lead ECG.Any patient with respiratory symptoms or extensive reaction should receive IV or IM diphenhydramine.The shorter the onset from symptoms to contact, the more severe t he reaction.
IV / Cardiac Monitor
Hypotensionprotocol
Appropriateprotocol
Respiratorydistressprotocol
Dysrhythmia
II
Universal Patient Care Protocol
Differential:Urticaria (rash only)Anaphylaxis (systemic effect)Shock (vascular effect)Angioedema (drug induced)Aspiration / Airway obstructionVasovagal eventAsthma or COPDCHF
M-3
Respiratorydistress
Hypotension
If evidence of Ana phylaxisEpinephrine 0.3 mg 1:10,000 IV
Diphenhydramine25-50 mg IV/IM
Hives / Rash onlyNo respiratory component
Diphenhydramine25-50 mg PO/IV/IM
Reassess patient
II
Solumedrol 125 mg IV PP
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
IV / Cardiac monitorI I
II
I I
Impending Respiratory Arrest/Shock
Respiratory Distress notIn Arrest/Shock
Version 1.2
Epinephrine 0.5 mg IM II

Glucagon 1 mg IV/IM
Consider50% Dextrose 25 grams IV
Narcan 2-4 mg slow IV/ IN/IM12 Lead ECG
Wake County EMS System Protocols
Thiamine 100 mg IV50% Dextrose 25 grams IV
If no IV accessGlucagon 1 mg IM
Consider other causes:Head injuryOverdose
StrokeHypoxia
Normal Saline1000 cc bolus
IV Protocol
Altered Mental StatusHistory:
Known diabetic, medicalert tagDrugs, drug paraphernaliaReport of illicit dr ug use ortoxic ingestionPast medical historyMedicationsHistory of traumaChange in condition
Signs/Symptoms:Decreased mental statusChange in baseline menta l statusBizarre behaviorHypoglycemia (cool, diaphoreticskin)Hyperglycemia (warm, dry skin;fruity breath; Kussmal resps;signs of dehydration)
I
Return to baseline ?
Pearls:Exam: Mental Status, HEENT, Skin, Heart, Lungs, Abdomen, Back, Extremities, NeuroBe aware of AMS as presenting sign of an environmental toxin or Haz-Mat exposure and protect personal safety.It is safer to assume hypoglycemia than hyperglycemia if doubt exists. Recheck blood glucose after D50 or Glucagon.Do not let alcohol confuse the clinical picture. Alcoholics frequently develop hypoglycemia.Do not give oral glucose if patient canno t protect own airway.Consider restraints if necessary for patient's and/or personnel's protection per the restraint procedure.Thiamine may be omitted if the patient has no signs of malnutrition.If restraints are used, complete the "Restraint" procedure in the call reporting system.
Differential:Head traumaCNS (stroke, tumor, seizure, infection)Cardiac (MI, CHF)InfectionThyroid (hyper / hypo)Shock (septic, metabolic, traumatic)Diabetes (hyper / hypoglycemia)ToxicologicAcidosis / AlkalosisEnvironmental exposurePulmonary (Hypoxia)Electrolyte abnormatilityPsychiatric disorder
ConsiderSpinal Immobilization Protocol
Version 1.2
Universal Patient Care Protocol
Narcan 2-4 mg IV/IN/IMIf respirations depressed
Glucose < 60 Glucose > 350signs of dehydration
Glucose 60 - 350
Blood glucose
No
I
I I
I I I I
I
P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Patient may refuse transportwithout calling medical co ntrolif not taking oral diabetic meds
and:adult present with patient
Blood Sugar > 100Patient has ability to eat meal
now
I
P
Yes
M-4
Oral Glucose, 1 to 2 tubes

Wake County EMS System Protocols
Back PainHistory:
AgePast medical historyPast surgical historyMedicationsOnset of pain / injuryPrevious back injuryTraumatic mechanismLocation of painFeverImprovement or worseningwith activity
Signs and Symptoms:Pain (paraspinous, spinous
process)SwellingPain with range of motionExtremity weaknessExtremity numbnessShooting pain into an extremityBowel / bladder dysfunction
Pearls:Exam: Mental Status, HEENT, Neck, Chest, Lungs, Abdomen, Back, Extremit ies, Neuro
Abdominal aneurysms are a concern in patients ov er the age of 50 Kidney stones typically present with an acute onset of flank pain which ra diates around to the groin area. Patients with midline pain over the spinous processes should be spinally immobilized. Any bowel or bladder incontinence is a significant finding which requ ires immediate medical evaluation.
Version 1.1
Differential:Muscle spasm / strainHerniated disc with nerve compressionSciaticaSpine fractureKidney stonePyelonephritis (Kidney infection)AneurysmPneumoniaCardiac related
Universal Patient Care Protocol
SpinalImmobilization
Protocol
No
IV Protocol
Normal Saline Bolus
Positive
Orthostatic Blood Pressure
Pain Control Protocol
Injury or traumatic mechanism
Negative
No
Signs ofshock? Yes
Yes
I I
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
M-5

Wake County EMS System Protocols
Behavioral/Agitated Delirium
Version 1.2
Pearls:Exam: Mental Status, Skin, Heart, Lungs , NeuroConsider Haldol for patients with history of psychosis, Versed for patients with presumed s ubstance abuse.Be sure to consider all possible medical/trauma causes for behavior (hypoglycemia, over dose, substance abuse,hypoxia, head injury, etc.)Do not overlook the possibility of associated domestic viole nce or child abuse.If patient in agitated delirium suffers cardiac arrest, consider fluid bolus a nd sodium bicarbonate early.All patients who receive either physical or chemical restraint must be continuously o bserved by ALSpersonnel on scene or immediately upon their arrival.
History:Situational crisisPsychiatric illness/medicationsInjury to self or threats toothersMedic alert tagSubstance abuse / overdoseDiabetes
Signs and Symptoms:Anxiety, agitation, confusionAffect change, hal lucinationsDelusional thoughts, bizarrebehaviorCombative violentExpression of suicidal /homicidal thoughts
Differential:see Altered Mental Status differentialHypoxiaAlcohol IntoxicationMedication effect / overdoseWithdrawal syndromesDepressionBipolar (manic-depressive)Schizophrenia, anxiety disorders, etc
Scene Safety
Universal Patient Care Protocol
Treat suspected medical or trauma probl ems perappropriate protocol
Altered Mental StatusOverdose
Head Trauma
Remove patient from stressful envi ronment
Verbal techniques (reassurance, calm, establish ra pport)
Refusal of CareContact Medical ControlM M
Restraint Procedure
ConsiderHaldol 5mg IV or 5-10 mg IM
May repeat q 10 X 1P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
ConsiderVersed 2 mg IV or 4 mg IM
May repeat q 15 X 1P P
M-6
Wake County EMS System Protocols
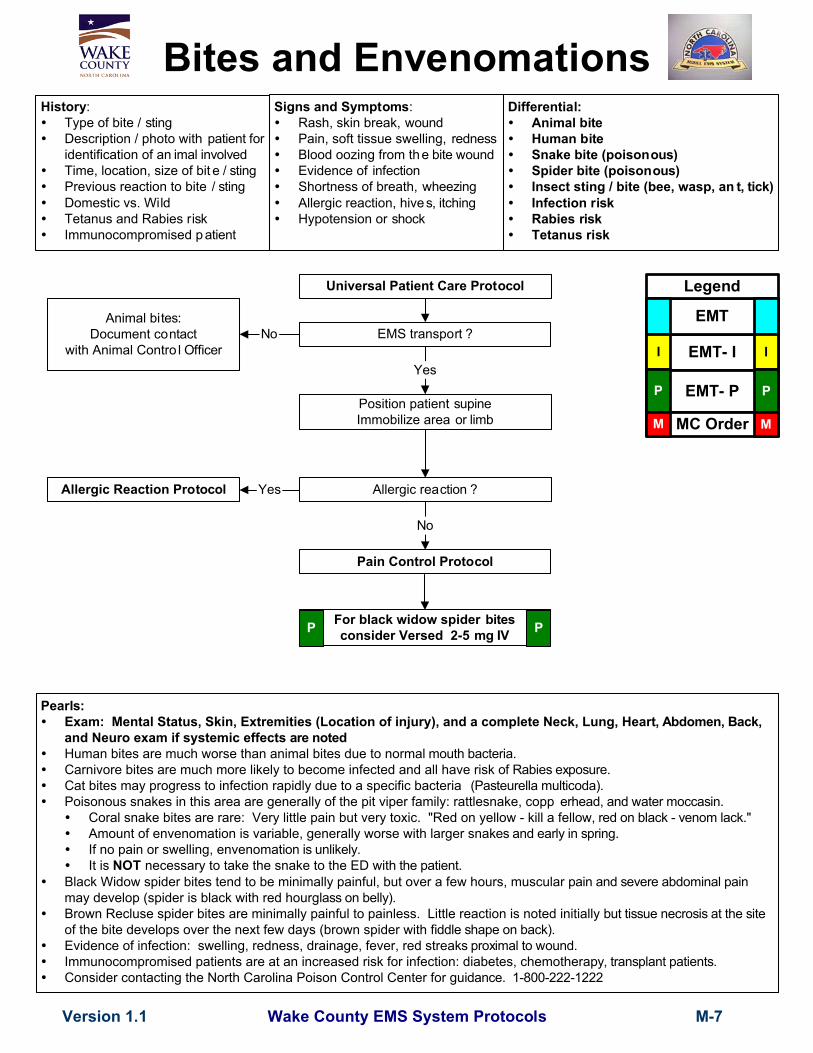
Bites and EnvenomationsHistory:
Type of bite / stingDescription / photo with patient foridentification of an imal involvedTime, location, size of bit e / stingPrevious reaction to bite / stingDomestic vs. WildTetanus and Rabies riskImmunocompromised p atient
Signs and Symptoms:Rash, skin break, woundPain, soft tissue swelling, rednessBlood oozing from the bite woundEvidence of infectionShortness of breath, wheezingAllergic reaction, hives, itchingHypotension or shock
Pearls: Exam: Mental Status, Skin, Extremities (Location of injury), and a complete Neck, Lung, Hear t, Abdomen, Back,
and Neuro exam if systemic effects are noted Human bites are much worse than animal bites due to norma l mouth bacteria. Carnivore bites are much more likely to become infected and all have risk of Rabies exposure.
Cat bites may progress to infection rapidly due to a specific bacteria (Pasteurella multicoda).Poisonous snakes in this area are generally of the pit viper family: rattlesnake, copp erhead, and water moccasin. Coral snake bites are rare: Very little pain but very toxic. "Red on yellow - kill a fell ow, red on black - venom lack." Amount of envenomation is variable, generally worse with larger sna kes and early in spring. If no pain or swelling, envenomat ion is unlikely. It is NOT necessary to take the snake to the ED wit h the patient.
Black Widow spider bites tend to be minimally painful, but over a few hours, muscular pain and severe abdominal painmay develop (spider is black with red hourg lass on belly).
Brown Recluse spider bites are minimally painful to painless. Little reaction is noted initially but tissue necrosis at the siteof the bite develops over the next few days (brown spider with fiddle shape on back).
Evidence of infection: swelling, redness, drainage, fever, red strea ks proximal to wound. Immunocompromised patients are at an increased risk for infection: diabetes, chemothera py, transplant patients. Consider contacting the North Carolina Poison Control Center for gu idance. 1-800-222-1222
Allergic reaction ?
No
Yes
Version 1.1
Differential:Animal biteHuman biteSnake bite (poisonous)Spider bite (poisonous)Insect sting / bite (bee, wasp, an t, tick)Infection riskRabies riskTetanus risk
Universal Patient Care Protocol
Position patient supineImmobilize area or limb
Allergic Reaction Protocol
EMS transport ?
Yes
No
Pain Control Protocol
Animal bites:Document contact
with Animal Contro l Officer EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
For black widow spider bitesconsider Versed 2-5 mg IVP P
M-7

Wake County EMS System Protocols
Childbirth / LaborHistory:
Due dateTime contractions started / how oftenRupture of membranesTime / amount of any vagin al bleedingSensation of feta l activityPast medical and delivery historyMedicationsDrug useGravida/Para statusHigh Risk pregnancy
Signs and Symptoms:Spasmotic painVaginal discharge orbleedingCrowning or urge to pushMeconium
Left lateral position
Visually inspect perineum forcrowning
(No digital vaginal exam)
Hypertension ?Abnormal vaginal bleeding ?
No
Crowning>36 weeks gestation
IV Protocol
Childbirth Procedure
Newly Born Protocol
ObstetricalEmergencies
ProtocolYes
No crowning
Monitor and reassessDocument frequency
and durationof contractions
Priority symptoms:Crowning
<36 weeks gestationAbnormal presentation
Severe vaginal bleedingMultiple gestation
If prolapsed cord,push up on head
Rapid transport
Pearls:Exam (of Mother): Mental Status, Heart, Lungs, Abdomen , Neuro
Document all times (delivery, contraction frequ ency, and length). If maternal seizures occur, refer to the Obstetrical Emerge ncies Protocol. After delivery, massaging the uterus (lower abdomen) will promote uterine contraction an d help to control post-partum
bleeding. Some perineal bleeding is normal with any childbirth. Large quantities of bl ood or free bleeding are abnormal. Record APGAR at 1 minute and 5 minutes a fter birth.
Version 1.1
Differential:Abnormal presentation
ButtockFootHand
Prolapsed cordPlacenta previaAbruptio placenta
Universal Patient Care Protocol
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
M-8

Wake County EMS System Protocols
History:AgePast medical historyMedicationsOnset of pain / injuryTrauma with "knocked ou t" toothLocation of toothWhole vs partial tooth injury
Signs and Symptoms:BleedingPainFeverSwellingTooth missing or fractured
Pearls:Exam: Mental Status, HEENT, Neck, Chest, Lungs, Neuro
Significant soft tissue swelling to the face or oral cavity can represent cellulitis or an abscess. Scene and transport times should be minimized in complete tooth avulsions. Reimplantation is possible within 4 hours
if the tooth is properly cared for. All tooth disorders typically need antibiotic coverage, i n addition to pain control Occasionally cardiac chest pain can ra diate to the jaw. All pain associated with teeth should be associated with a tooth which is tender to tappin g or touch (or sensitivity to cold
or hot).
Version 1.1
Differential:DecayInfectionFractureAvulsionAbscessFacial cellulitisImpacted tooth (wisdom)TMJ syndromeMyocardial infarction
Pain Control Protocol
No
Reassess and Monitor
Universal Patient Care Protocol
Tooth avulsion
Control bleeding with pressure
Place tooth inmilk or normal saline
Yes
Dental Problems
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
M-9
Wake County EMS System Protocols
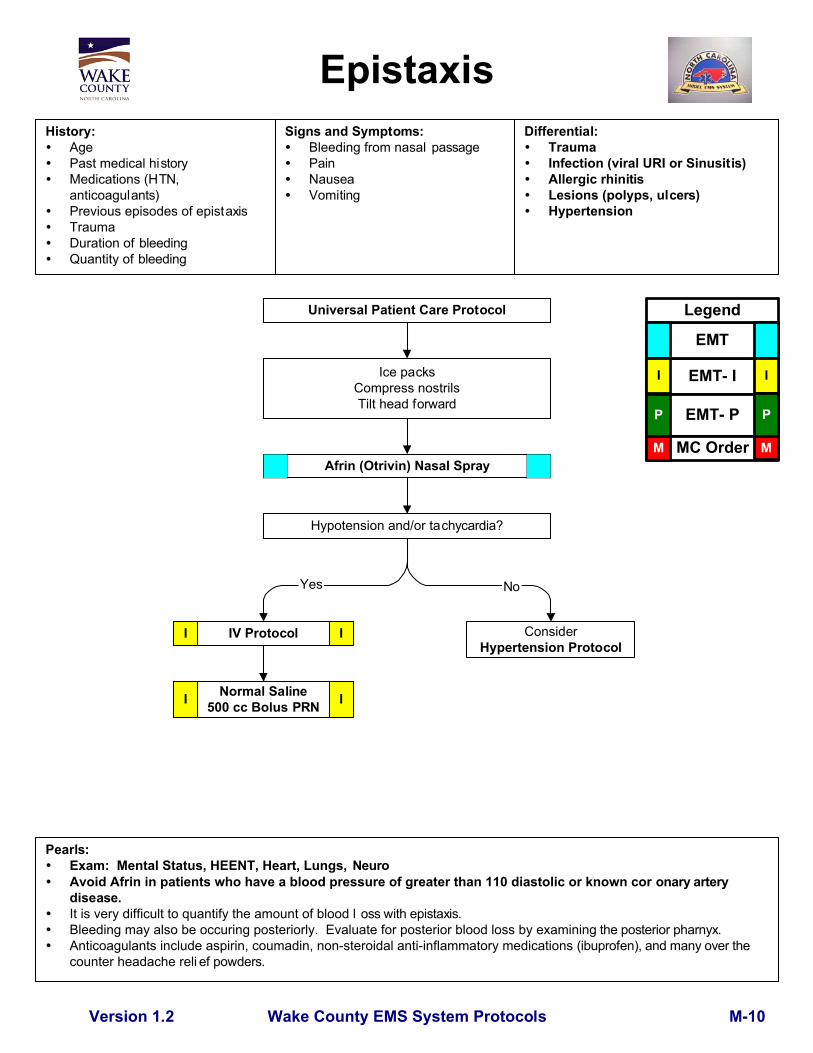
EpistaxisHistory:
AgePast medical historyMedications (HTN,anticoagulants)Previous episodes of epistaxisTraumaDuration of bleedingQuantity of bleeding
Signs and Symptoms:Bleeding from nasal passagePainNauseaVomiting
Pearls:Exam: Mental Status, HEENT, Heart, Lungs, NeuroAvoid Afrin in patients who have a blood pressure of greater than 110 diastolic or known cor onary arterydisease.It is very difficult to quantify the amount of blood l oss with epistaxis.Bleeding may also be occuring posteriorly. Evaluate for posterior blood loss by examining the posterior pharnyx.Anticoagulants include aspirin, coumadin, non-steroidal anti-inflammatory medications (ibuprofen), and many over thecounter headache reli ef powders.
Version 1.2
Differential:TraumaInfection (viral URI or Sinusitis)Allergic rhinitisLesions (polyps, ulcers)Hypertension
Normal Saline500 cc Bolus PRN
Universal Patient Care Protocol
Ice packsCompress nostrilsTilt head forward
ConsiderHypertension Protocol
I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M MAfrin (Otrivin) Nasal Spray
Hypotension and/or tachycardia?
IV ProtocolI I
I
Yes No
M-10

Wake County EMS System Protocols
IV Protocol
Temperature
Version 1.2
Normal Saline Bolus 500 cc
Universal Patient Care Protocol
Orthostatic Blood Pressure
Encourage po fluid intake andcooling measures
Appropriate Protocol by Complaint
Tylenol1 gram PO
Fever/Infection Control
Yes
> 100°F(38°C)
< 100°F(38°C)
No
Pearls:Exam: Mental Status, Skin, HEENT, Neck, Heart, Lungs, Abdomen, Back, Extrem ities, NeuroFebrile seizures are more likely in children with a history of febrile seizures and with a rapid elevation in temperature.Patients with history of Liver disease should not receive Ty lenol.Droplet precautions include standard PPE plus a standard surgical mask for providers who accompanypatients in the back of the ambulance and a surgical mask or NRB O2 mask for the patient. This level ofprecaution should be utilized when influenza, meningitis, mumps, streptococcoal pharyng itis, and otherillnesses spread via large particle droplets ar e suspected.Airborne precautions include standard PPE plus an N-95 mask for providers who accompany patients in theback of the ambulance and a surgical mask or NRB O2 mask for the patient. This level of pre caution shouldbe utilized when tubercuolosis, measles, varicella, or other infections that are spread by d roplet nuclei aresuspected.Contact precautions include standard PPE plus utilization of a gown, change of gloves after e very patientcontact, and strict handwashing precautions. This level of precaution is utilized when multi-d rug resistantorganisms (e.g., MRSA), scabies, or zoster (shingles), or other illnesses spread by cont act are suspected.All-hazards precautions include standard PPE plus airborne precautions plus contact precautio ns. This levelof precaution is utilized during the initial phases of an outbreak when the etiology of the infec tion is unknownor when the causative agent is found to be highly contagious (e.g ., SARS).
History:AgeDuration of feverSeverity of feverPast medical historyMedicationsImmunocompromised(transplant, HIV, diabetes,cancer)Environmental exposureLast acetaminophen or ibuprofen
Signs and Symptoms:WarmFlushedSweatyChills/Rigors
Associated Symptoms:(Helpful to localize source)
myalgias, cough, chest pain,headache, dysuria, abdominalpain, mental status changes,rash, stiff neck
Differential:Infections / SepsisCancer / Tumors / LymphomasMedication or durg reactionConnective tissue disease
ArthritisVasculitis
HyperthyroidHeat StrokeMeningitis
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Consider Droplet, Airborne, or ContactPrecautions
I I
M-11
Wake County EMS System Protocols
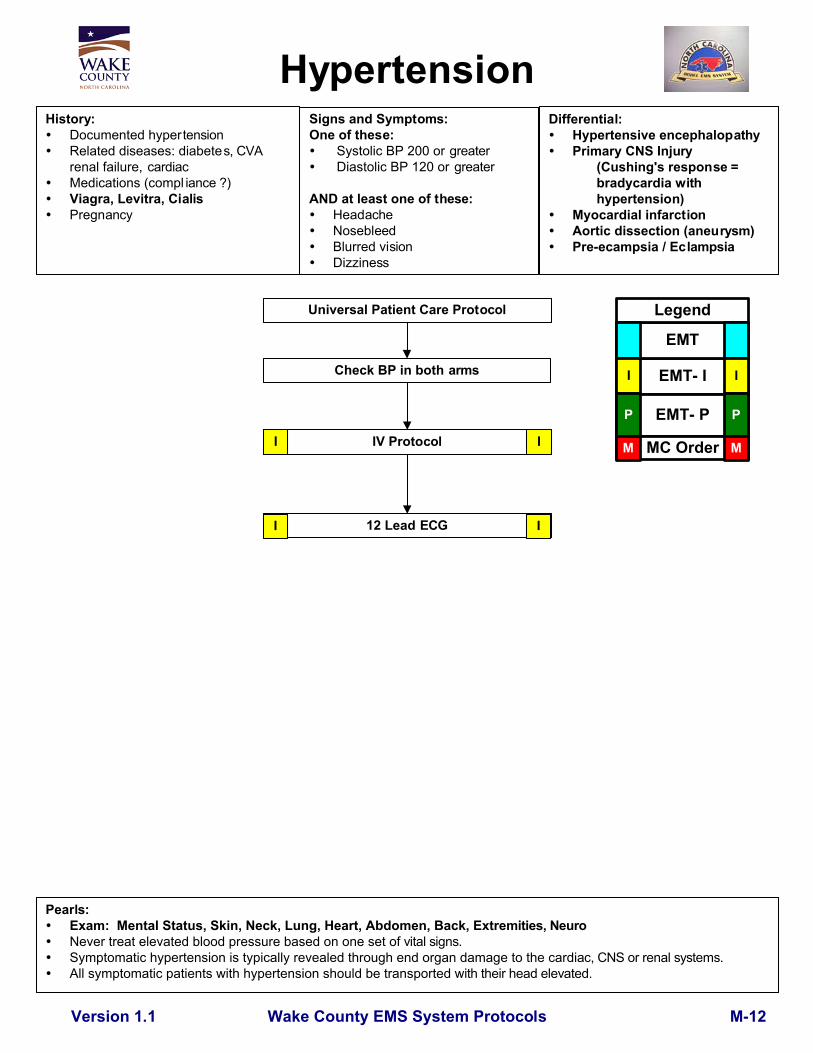
HypertensionSigns and Symptoms:One of these:
Systolic BP 200 or greater Diastolic BP 120 or greater
AND at least one of these:HeadacheNosebleedBlurred visionDizziness
History:Documented hypertensionRelated diseases: diabetes, CVArenal failure, cardiacMedications (compl iance ?)Viagra, Levitra, CialisPregnancy
Pearls: Exam: Mental Status, Skin, Neck, Lung, Heart, Abdomen, Back, Extre mities, Neuro Never treat elevated blood pressure based on one set o f vital signs. Symptomatic hypertension is typically revealed through end organ damage to the cardi ac, CNS or renal systems. All symptomatic patients with hypertension should be transported with their head elevated.
Differential:Hypertensive encephalopathyPrimary CNS Injury
(Cushing's response =bradycardia withhypertension)
Myocardial infarctionAortic dissection (aneurysm)Pre-ecampsia / Eclampsia
Version 1.1
Universal Patient Care Protocol
IV Protocol
12 Lead ECG
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Check BP in both arms
II
M-12
Wake County EMS System Protocols
IV Protocol500 cc Bolus
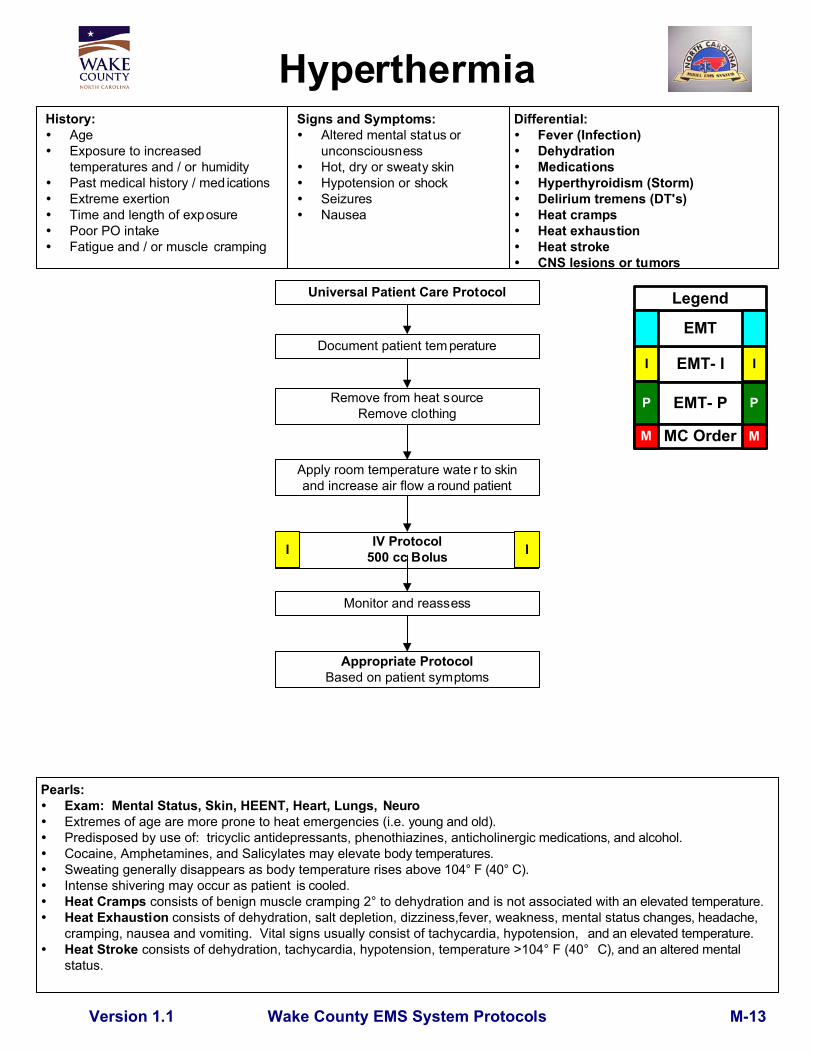
HyperthermiaHistory:
AgeExposure to increasedtemperatures and / or humidityPast medical history / med icationsExtreme exertionTime and length of exposurePoor PO intakeFatigue and / or muscle cramping
Signs and Symptoms:Altered mental status orunconsciousnessHot, dry or sweaty skinHypotension or shockSeizuresNausea
Document patient tem perature
Remove from heat sourceRemove clothing
Apply room temperature wate r to skinand increase air flow a round patient
Pearls:Exam: Mental Status, Skin, HEENT, Heart, Lungs, Neuro
Extremes of age are more prone to heat emergencies (i.e. young and old). Predisposed by use of: tricyclic antidepressants, phenothiazines, anticholinerg ic medications, and alcohol. Cocaine, Amphetamines, and Salicylates may elevate b ody temperatures. Sweating generally disappears as body temperature rises abo ve 104° F (40° C).
Intense shivering may occur as patient is cooled. Heat Cramps consists of benign muscle cramping 2° to dehydration and is not associated wit h an elevated temperature. Heat Exhaustion consists of dehydration, salt depletion, dizziness,fever, weakness, mental sta tus changes, headache,
cramping, nausea and vomiting. Vital signs usually consist of tachycardia, hypotension, and an elevated temperature.Heat Stroke consists of dehydration, tachycardia, hypotension, temperature >104° F (40° C), and an altered mentalstatus.
Monitor and reassess
Version 1.1
Differential:Fever (Infection)DehydrationMedicationsHyperthyroidism (Storm)Delirium tremens (DT's)Heat crampsHeat exhaustionHeat strokeCNS lesions or tumors
Appropriate ProtocolBased on patient symptoms
Universal Patient Care Protocol
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
M-13

Wake County EMS System Protocols
HypotensionShock (nontrauma)
Pearls: Exam: Mental Status, Skin, Heart, Lungs, Abdomen, Back, Extrem ities, Neuro Hypotension can be defined as a systolic blood pressure of less than 90. Consider performing orthostatic vital signs on patients in nontrauma situations if suspec ted blood or fluid loss. Consider all possible causes of shock and treat per appro priate protocol.
History:Blood loss - vaginal orgastrointestinal bleed ing, AAA,ectopicFluid loss - vomiting, d iarrhea,feverInfectionCardiac ischemia (MI, CHF)MedicationsAllergic reactionPregnancyHistory of poor oral intake
Signs and Symptoms:Restlessness, confusionWeakness, dizzinessWeak, rapid pulsePale, cool, clammy skinDelayed capillary refillHypotensionCoffee-ground emesisTarry stools
Version 1.1
Differential:Shock
HypovolemicCardiogenicSepticNeurogenicAnaphylactic
Ectopic pregnacyDysrhythmiasPulmonary embolusTension pneumothoraxMedication effect / overdoseVasovagalPhysiologic (pregnancy)
Universal Patient Care Protocol
IV Protocol
Treatment per appropriateTrauma Protocol
Normal Saline500 cc bolus
Consider Dopamine5-20 mcg/kg/min IV
Treatment per appropriateCardiac Protocol
No rales presentNormal Saline500 cc bolus
Consider Dopamine5-20 mcg/kg/min IV
Non-cardiacNon-trauma CardiacTrauma
I I
I I
I I
P PP P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
AdditionalNormal Saline500 cc bolus
I I
Symptomatic?Observe andReassess No
Yes
M-14

Wake County EMS System Protocols
HypothermiaHistory:
Past medical historyMedicationsExposure to environment even innormal temperaturesExposure to extreme coldExtremes of ageDrug use: Alcohol, barbituatesInfections / SepsisLength of exposure / Wetness
Signs and Symptoms:Cold, clammyShiveringMental status changesExtremity pain or sensoryabnormalityBradycardiaHypotension or shock
Universal Patient Care Protocol
Remove wet clothing
Handle very gently
IV ProtocolConsider using warm fluids
Blankets
Pearls: Exam: Mental Status, Heart, Lungs, Abdomen, Extremit ies, Neuro NO PATIENT IS DEAD UNTIL WARM AND DEAD.
Defined as core temperature < 35° C (95° F). Extremes of age are more susceptable (i.e. you ng and old). With temperature less than 31° C (88° F) ventricular fibrillation is common cause of deat h. Handling patients gently
may prevent this (rarely responds to defibrillation). If the temperature is unable to be measured, treat the patient based on the suspected temperature.
Hypothermia may produce severe b radycardia.Shivering stops below 32° C (90° F).
Version 1.1
Differential:SepsisEnvironmental exposureHypoglycemiaCNS dysfunction
StrokeHead injurySpinal cord injury
Temperature < 95° F (35° C)
Appropriate ProtocolBased on patient symptoms
No
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M MYes
M-15
Yes

Wake County EMS System Protocols
IV
Assess need for IVEmergent or potentially emergent
medical or trauma condition
Peripheral IV
Monitor Saline Lock
Intraosseous (ped or adult device)for life-threatening event
External Jugular IVfor life-threatening event
Pearls:Intraosseous with the appropriate adult or pediatric device.External jugular (> 12 years of age).Any prehospital fluids or medications approved for IV use, may be given through an intraosseous IV.All IV rates should be at KVO (minimal rate to keep vein open) unless administering fluid bolus.Use microdrips for all patients 6 years old or less.External jugular lines can be attempted initially in life-threatening events where no obvious peripheral site is noted.In the setting of cardiac arrest, any preexisting dialysis shunt or external central venous catheter may be used.In patients who are hemodynamically unstable or in extremis, contact medical control prior to accessing dialysisshunts or external central venous catheters.Any venous catheter which has already been accessed prior to EMS arrival may be used.Upper extremity IV sites are preferable to lower extremity sites.Lower extremity IV sites are contraindicated in patients with vascular disease or diabetes.In post-mastectomy patients, avoid IV, blood draw, injection, or blood pressure in arm on affected side.
Version 1.1
Universal Patient Care Protocol
UnsuccessfulSuccessful
Monitor infusion500 cc Fluid Bolus PRN
I I
P P
I
ContinuePeripheral IV
Intraosseous (ped or adult device)for life-threatening event
External Jugular IVfor life-threatening event
I I
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
I
M-16

Wake County EMS System Protocols
Obstetrical EmergencyHistory:
Past medical history Hypertension meds
Prenatal carePrior pregnancies / birthsGravida / Para
Signs and Symptoms:Vaginal bleedingAbdominal painSeizuresHypertensionSevere headacheVisual changesEdema of hands and face
Pearls:Exam: Mental Status, Abdomen, Heart, Lungs , Neuro
Severe headache, vision changes, or RUQ pain may indic ate preeclampsia. In the setting of pregnancy, hypertension is defined as a BP greater than 140 systolic or greater than 90 diastolic, or
a relative increase of 30 systolic and 20 diastolic from the patient's normal (pre-pr egnancy) blood pressure. Maintain patient in a left lateral position to minimize risk of sup ine hypotensive syndrome. Ask patient to quantify bleeding - number of pa ds used per hour. Any pregnant patient involved in a MVC should be seen immediately by a physician f or evaluation and fetal monitoring. Magnesium may cause hypotension and decreased respiratory drive . Use with caution.
Vaginal bleeding / Abdominal pain ?
Differential:Pre-eclampsia / EclampsiaPlacenta previaPlacenta abruptioSpontaneous abortion
Version 1.1
Universal Patient Care Protocol
Known pregnancy / Missed period?
Transport to Hospital
YesNo
Left lateral position
IV Protocol
Seizure or seizure-like activity?
Abdominal Pain Protocol
Complaint of Labor?
Normal Saline Bolus
Childbirth Protocol
NoYes
NoPlace Left Lateral Recumbant
No
Yes
I I
I I
Active seizure activity?Versed 2-5 mg slow IV
Blood Glucose Measurement
P P
Orthostatic BP
Yes
No
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Magnesium Sulfate 4 grams IVslow over 10-20 min PP
Known pregnancy / Missed period?
Yes
Hypertension?
Yes
No
M-17
Yes
No
Yes

Wake County EMS System Protocols
OverdoseToxic Ingestion
History:Ingestion or suspected ingestion ofa potentially toxic substanceSubstance ingested, route,quantityTime of ingestionReason (suicidal, accidental,criminal)Available medications in homePast medical history, medications
Signs and Symptoms:Mental status changesHypotension / hypertensionDecreased respiratory rateTachycardia, dysrhythmiasSeizures
Universal Patient Care Protocol
IV ProtocolConsider Charcoal 50 grams PO if alert
Tricyclic ingestion?Sodium Bicarbonate 1meq/kg
Narcan2-4 mg Slow IV/
4 mg IN
Atropine2 mg IV q 5 minNo Max Dose
Hypotension, Seizures,Ventricular dysrhythmias,or Mental status changes
Appropriate Protocol
Pearls:Exam: Mental Status, Skin, HEENT, Heart, Lungs, Abdomen, Extremities, NeuroDo not rely on patient history of ingestion, especially in suicide attempts.Bring bottles, contents, emesis to ED.Tricyclic: 4 major areas of toxicity: seizures, dysrhythmias, hypotension, decreased mental status or coma;
rapid progression from alert mental status to death.Acetaminophen: initially normal or nausea/vomiting. If not detected and treated, causes irreversible liver failureDepressants: decreased HR, decreased BP, decreased temperature, decreased respirations, non-specific pupilsStimulants: increased HR, increased BP, increased temperature, dilated pupils, seizuresAnticholinergic: increased HR, increased temperature, dilated pupils, mental status changesCardiac Meds: dysrhythmias and mental status changesSolvents: nausea, vomiting, and mental status changesInsecticides: increased or decreased HR, increased secretions, nausea, vomiting, diarrhea, pinpoint pupilsCharcoal may not be adminstered by NG tube. If the patient's mental status deteriorates after administration ofcharcoal, an NG tube may be placed to assist with airway management.Consider restraints if necessary for patient's and/or personnel's protection per the Restraint Procedure.MARK 1 kits contain 2 mg of Atropine and 600 mg of pralidoxime in an autoinjector for self administration or patientcare. These kits may be available as part of the domestic preparedness for Weapons of Mass Destruction.Consider contacting the North Carolina Poison Control Center for guidance.
M-18
Differential:Tricyclic antidepressants (TCAs)Acetaminophen (tylenol)DepressantsStimulantsAnticholinergicCardiac medicationsSolvents, Alcohols, Cleaning agentsInsecticides (organophosphates)
Respiratory depression Other
OrganophosphatesCarbamates
I I
I I
P P
P P
EMT- IEMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Version 1.2
Chest PainProtocolI I
Chest Pain

IV Protocol
Pain ControlHistory:
AgeLocationDurationSeverity (1 - 10)Past medical historyMedicationsDrug allergies
Signs and Symptoms:Severity (pain scale)Quality (sharp, dull, etc.)RadiationRelation to movement,respirationIncreased with palpation of area
Pearls:Patients with presumed kidney stone pain should first receive toradol. Morphine may then be considered.Pain severity (0-10) is a vital sign to be recorded pre and post IV or IM medication delivery and at disposition.Patient's initial and final pain levels are to be documented in the paramedic assessment procedure.Vital signs should be obtained pre, 15 minutes post, and at dispo sition with all pain medications.Contraindications to Morphine use include hypotension, altered mental status, head injury, respiratorydistress or severe COPD.Ketorolac (Toradol) should not be used in patients with known renal disease or renal transplant, in patientswho have known drug allergies to NSAID's (non-steroidal anti-inflammatory medications), or in patients whomay need surgical intervention such as open fractures or fracture deformities.All patients should have drug allergies documented prior to administering pain medications.All patients who receive IM or IV medications must be observed 15 minutes for drug reaction.No PO medications for patients who may need surgical intervention such as open fractures or fracture deformities.Do not administer Tylenol to patients with a history of liver disease.
Morphine 2-5 mg IVup to 20 mg
Monitor and reassess
Universal Patient Care Protocol
Differential:Per the specific protocolMusculoskeletalVisceral (abdominal)CardiacPleural / RespiratoryNeurogenicRenal (colic)
Contraindication to sedation?Abdominal pain?
Yes
Patient care according to Protocolbased on Specific Complaint
Tylenol1 gram PO
Morphine 2- 5 mg IVup to 20 mg
Pulse Oximetry
No
Pain Severity > 6 / 10or
Indication for IV / IM Medication
Yes
No
I I
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
For nausea/vomitingZofran
4 mg IV/IMP P
MM Toradol30 mg IV/IM
PresumedKidneyStone?
I I
Pulse Oximetry
Wake County EMS System Protocols M-19Version 1.2

Agitated Delirium?
Significant InjuryFrom Entry Point ofTaser or From FallAfter Taser Use?
Universal Patient CareProtocol
Police CustodyHistory:
Traumatic injuryDrug AbuseCardiac HistoryHistory of AsthmaPsychiatric History
Signs and Symptoms:
External signs of traumaPalpitationsShortness of breathWheezingAltered Mental StatusIntoxication/SubstanceAbuse
Pearls:Agitated delirium is characterized by marked restlessness, irritability, and/or high fever. Patients exhibit ing thesesigns are at high risk for sudden death and should be transported t o hospital by ALS personnel.Patients restrained by law enforcement devices cannot be transported in the ambulance without a law enforceme ntofficer in the patient compartment who is capable of removing the device s.If there is any doubt about the cause of a patient's alteration in mental status, transport the patien t to the hospital forevaluation.If an asthmatic patient is treated with pepper spray and released to law enforcment, all parties should be advised toimmediately recontact EMS if wheezing/difficulty breathing o ccurs.All patients in police custody retain the right to request transport. This should be coordinated wit h law enforcement.If extremity/chemical/law enforcement restraints are applied, complete "Restraint" procedure in call reporting syste m.
Differential:
Agitated Delirium Secondary toPsychiatric IllnessAgitated Delirium Secondary toSubstance AbuseTraumatic InjuryClosed Head InjuryAsthma ExacerbationCardiac Dysrhythmia
Wheezing?
Use of Pepper Spray or Taser?
Appropriate Protocol andTransport
Cardiac Historywith Pacemaker,
Chest Pain, orPalpitations?
Consider RestraintProcedure
and/or Chemical Restraint
No
EMT- IEMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Evidence of Traumatic Injuryor Medical Illness?
Irrigate face/eyesRemove
contaminatedclothing
BronchospasmProtocol and
Transport
No
Appropriate Protocol andTransport Yes
No
Pepper Spray
PP
P P
Coordinate dispostion withpatient and law enforcement
personnel
No
YesI
Taser
History ofAsthma?No
Yes
Observe 20 minWheezes?
Yes
I I
I
Yes
No
Yes
YesNo
Wake County EMS System ProtocolsVersion 1.2 M-20

Wake County EMS System Protocols
Thiamine 100 mg IV50% Dextrose 25 grams IVGlucagon 1 mg IM if no IV
Seizure
Pearls:Exam: Mental Status, HEENT, Heart, Lungs, Extremities, NeuroStatus epilepticus is defined as two or more successive seizures without a period of consciousness or recovery. This isa true emergency requiring rapid airway control, treatment, and transport.Grand mal seizures (generalized) are associated with loss of consciousness, incontinence, and tongue trauma.Focal seizures (petit mal) effect only a part of the body and are not usually associated with a loss of consciousnessJacksonian seizures are seizures which start as a focal seizure and become generalized.Be prepared for airway problems and continued seizures.Assess possibility of occult trauma and substance abuse.Be prepared to assist ventilations especially if Versed is used.For any seizure in a pregnant patient, follow the OB Emergencies Protocol.Thiamine may be omited in patients who do not appear malnourished.
History:Reported / witnessed seizureactivityPrevious seizure historyMedical alert tag informationSeizure medicationsHistory of traumaHistory of diabetesHistory of pregnancy
Signs and Symptoms:Decreased mental statusSleepinessIncontinenceObserved seizure activityEvidence of traumaUnconscious
Airway Protocol
Version 1.2
Universal Patient Care Protocol
Focused history /Physical exam
Consider Spinal Immobilization Protocol
IV Protocol
Versed 2.5-5 mg slow IVor Versed 5 mg IM/INMay be repeated X1
Blood Glucose
IV Protocol
Differential:CNS (Head) traumaTumorMetabolic, Hepatic, or Renal failureHypoxiaElectrolyte abnormality (Na, Ca, Mg)Drugs, Medications, Non-complianceInfection / FeverAlcohol withdrawalEclampsiaStrokeHyperthermiaHypoglycemia
Status / Seizure recurs?Versed 2.5-5 mg slow IV
or Versed 5 mg IM/INMay be repeated X1
Glucose < 60
Post-ictalStatus epilepticus
I I
P P
I I
P P
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
M-21

Pearls:Exam: Mental Status, HEENT, Heart, Lungs, Abdomen, Extremities, NeuroCincinnati Pre-Hospital Stroke Screen: Arm drift, leg drift, facial drooping, slurred speech.Thrombolytic Screening Checklist should be completed for any suspected stroke patient.With a duration of symptoms of less than 3 hours, scene times and transport times should be minimized. Considerdelay of procedures such as IV initiation until transport is under way.Onset of symptoms is defined as the last witnessed time the patient was symptom free (i.e. awakening with strokesymptoms would be defined as an onset time of the previous night when patient was symptom free).Whenever possible a family member should accompany patient to hospital to provide additional history and/or consent.The differential listed on the Altered Mental Status Protocol should also be considered.Be alert for airway problems (swallowing difficulty, vomiting).Hypoglycemia can present as a localized neurologic deficit, especially in the elderly.Patients who do not apprear malnourished do not require Thiamine.Document the Cincinnati evaluation using the "Stroke Screen" procedure in the call reporting system.Document the 12-lead using the "12-lead EKG" procedure in the call reporting system.
Wake County EMS System Protocols
If no IV accessGlucagon 1 mg IM
Thiamine 100 mg IV50% Dextrose25 grams IV
Suspected StrokeHistory:
Previous CVA, TIA'sPrevious cardiac / vascularsurgeryAssociated diseases: diabetes,hypertension, CADAtrial fibrillationMedications (blood thinners)History of trauma
Signs and Symptoms:Altered mental statusWeakness / ParalysisBlindness or other sensory lossAphasia / DysarthriaSyncopeVertigo / DizzynessVomitingHeadacheSeizuresRespiratory pattern changeHypertension / hypotension
Cincinnati Pre-Hospital Stroke Screen
Differential:See Altered Mental StatusTIA (Transient ischemic attack)SeizureHypoglycemiaStroke
ThromboticEmbolicHemorrhagic (~ 15%)
TumorTrauma
Version 1.2
Universal Patient Care Protocol
IV Protocol
Consider other protocols as indicatedAltered Mental Status
HypertensionSeizure
If Positive and Symptoms < 3 hours,transport to approved stroke facility.
Limit scene time to 10 minutes.
Blood Glucose
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
< 60
12 Lead EKG II
(~ 85%)
I I
M-22

IV Protocol
Wake County EMS System Protocols
Syncope
Pearls: Exam: Mental Status, Skin, HEENT, Heart, Lungs, Abdomen, Back, Extremi ties, Neuro Assess for signs and symptoms of trauma if associated or questionable f all with syncope. Consider dysrhythmias, GI bleed, ectopic pregnancy, and seizure as possible causes of syncope.
These patients should be transported. More than 25% of geriatric syncope is cardiac d ysrhythmia based. Thiamine may be omited in patients who do not ap pear malnourished.
History:Cardiac history, stroke, seizureOccult blood loss (GI, ectopic)Females: LMP, vaginalbleedingFluid loss: nausea, vomiting,diarrheaPast medical historyMedications
Signs and Symptoms:Loss of consciousness withrecoveryLightheadedness, dizzinessPalpitations, slow or rapid pulsePulse irregularityDecreased blood pressure
Orthostatic Vital Signs
Version 1.1
Blood Glucose
Consider Spinal Immobilization Protocol
Cardiac Monitor
AT ANY TIME
If relevant signs / symptoms foundgo to appropriate protocol:
DysrhythmiaAltered Mental Status
Hypotension
Differential:VasovagalOrthostatic hypotensionCardiac syncopeMicturation / Defecation syncopePsychiatricStrokeHypoglycemiaSeizureShock (see Shock Protocol)Toxicologic (Alcohol)Medication effect (hypertension)
Universal Patient Care Protocol
Thiamine 100 mg IV50% Dextrose 25 grams IV
If unable to establish IVGlucagon 1 mg IM
I I
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
II
12 Lead ECGI I
Blood Glucose< 60
M-23

Wake County EMS System Protocols
Vomiting and DiarrheaHistory:
AgeTime of last mealLast bowel movement/emesisImprovement or worseningwith food or activityDuration of problemOther sick contactsPast medical historyPast surgical historyMedicationsMenstrual history(pregnancy)Travel historyBloody emesis / diarrhea
Signs and Symptoms:PainCharacter of pain (c onstant,intermittent, sharp, dul l, etc.)DistentionConstipationDiarrheaAnorexiaRadiation
Associated symptoms:(Helpful to localize source)Fever, headache, blurred vision,weakness, malaise, myalgias,cough, headache, dysur ia, mentalstatus changes, rash
Pearls:Exam: Mental Status, Skin, HEENT, Neck, Heart, Lungs, Abdomen, Back, Extrem ities, NeuroReglan may worsen diarrhea and should be avoided in patien ts with this symptom.Maintain high suspiscion of a cardiac event for persons with dia betes or neuropathies.The list of differentials for N&V is long. Attempt to identif y underlying conditions.
Version 1.2
Universal Patient Care Protocol
Differential:CNS (increased pressure, headache,stroke, CNS lesions, trauma orhemorrhage, vestibular)Myocardial infarctionDrugs (NSAID's, antibiotics, narcotics,chemotherapy)GI or Renal disordersDiabetic ketoacidosisGynecologic disease (ovarian cyst, PID)Infections (pneumonia, influenza)Electrolyte abnormalitiesFood or toxin inducedMedication or Substance abusePregnancyPsychological
IV Protocol
Blood Glucose
Normal Saline Bolus500 cc bolusI I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
I I
Zofran 4 mg IV/IMP P
Reglan 10 mg IVP P
M-24
Orthostatic Blood Pressure
Vomiting/Severe Nausea?
Yes
OR
Monitor and Reassessthroughout transport
No

Wake County EMS System Protocols
Eye Injury/Complaint
Version 1.3
In socketOut of socket
Pearls:
Normal visual acuity can be present even with severe ey e injury
Remove contact lens whenever poss ible.
Any chemical or thermal burn to the face/eyes should raise suspicion of resp iratory insult
Orbital fractures raise concern of globe or nerve injury and need repeated assessments o f visual status
Always cover both eyes to prevent further injury.
Use shields, not pads, for physical trauma to eyes. Pads OK for una ffected eye.
Do not remove impaled objects
Suspected globe rupture or compartment syndromes require emergent in-facility in tervention.
History:
Time of injury/onset
Blunt/penetrating/chemical
Open vs. closed injury
Involved chemicals/MSDS
Wound Contamination
Medical History
Tetanus status
Normal visual acuity
Medications
Signs and Symptoms:
Pain, swelling, blood
Deformity, contusion
Visual deficit
Leaking aqueous/vitreous humor
Upwardly fixed eye
"Shooting" or "streaking" light
Visible contaminants
Rust ring
Lacrimation
Differential:
Abrasion/Laceration
Globe rupture
Retinal nerve damage/detachment
Chemical/thermal burn/agent of terror
Orbital fracture
Orbital compartment symdrome
Neurological event
Acute glaucoma
Retinal artery occlusion
Universal Patient Care Protocol
Nature?
Cover with saline-
moistened gauzeMechanism
Assess Orbital Stability
Assess visual acuity (when
feasible)
Penetrating Trauma/Rupture
of Globe?
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
M-25
Assess visual acuity
Evaluate pupils
Complete neuro exam
Screen for
unrecognized
chemical/agent
exposure
Cover both eyes
Pain Control Protocol
Isolated to eye(s)?Appropriate
Protocol
Immediate irrigation with
available saline or water
Tetracaine 2 gtt
Irrigate with Normal Saline
using Morgan Lens
Cover unaffected eye
No
InjuryPain/visual
Burn/Chemical Physical Trauma
Zofran 4 mg IV/IM
NoYes
P P
P P
Yes
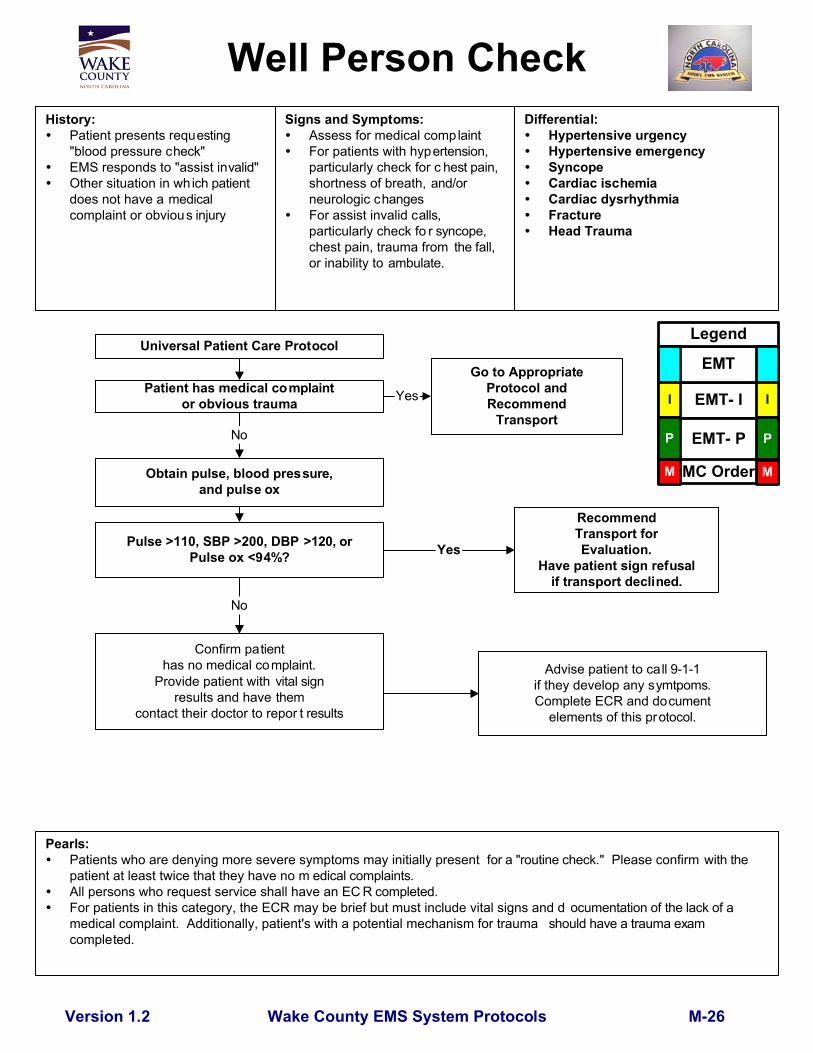
Pearls:Patients who are denying more severe symptoms may initially present for a "routine check." Please confirm with thepatient at least twice that they have no m edical complaints.All persons who request service shall have an EC R completed.For patients in this category, the ECR may be brief but must include vital signs and d ocumentation of the lack of amedical complaint. Additionally, patient's with a potential mechanism for trauma should have a trauma examcompleted.
Wake County EMS System Protocols
RecommendTransport forEvaluation.
Have patient sign refusalif transport declined.
Well Person CheckHistory:
Patient presents requesting"blood pressure check"EMS responds to "assist invalid"Other situation in which patientdoes not have a medicalcomplaint or obvious injury
Signs and Symptoms:Assess for medical complaintFor patients with hypertension,particularly check for c hest pain,shortness of breath, and/orneurologic changesFor assist invalid calls,particularly check fo r syncope,chest pain, trauma from the fall,or inability to ambulate.
Patient has medical complaintor obvious trauma
Differential:Hypertensive urgencyHypertensive emergencySyncopeCardiac ischemiaCardiac dysrhythmiaFractureHead Trauma
Version 1.2
Universal Patient Care Protocol
Advise patient to call 9-1-1if they develop any symtpoms.Complete ECR and document
elements of this protocol.
Obtain pulse, blood pressure,and pulse ox
Pulse >110, SBP >200, DBP >120, orPulse ox <94%?
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Confirm patienthas no medical complaint.
Provide patient with vital signresults and have them
contact their doctor to repor t results
M-26
No
Go to AppropriateProtocol andRecommend
Transport
Yes
No
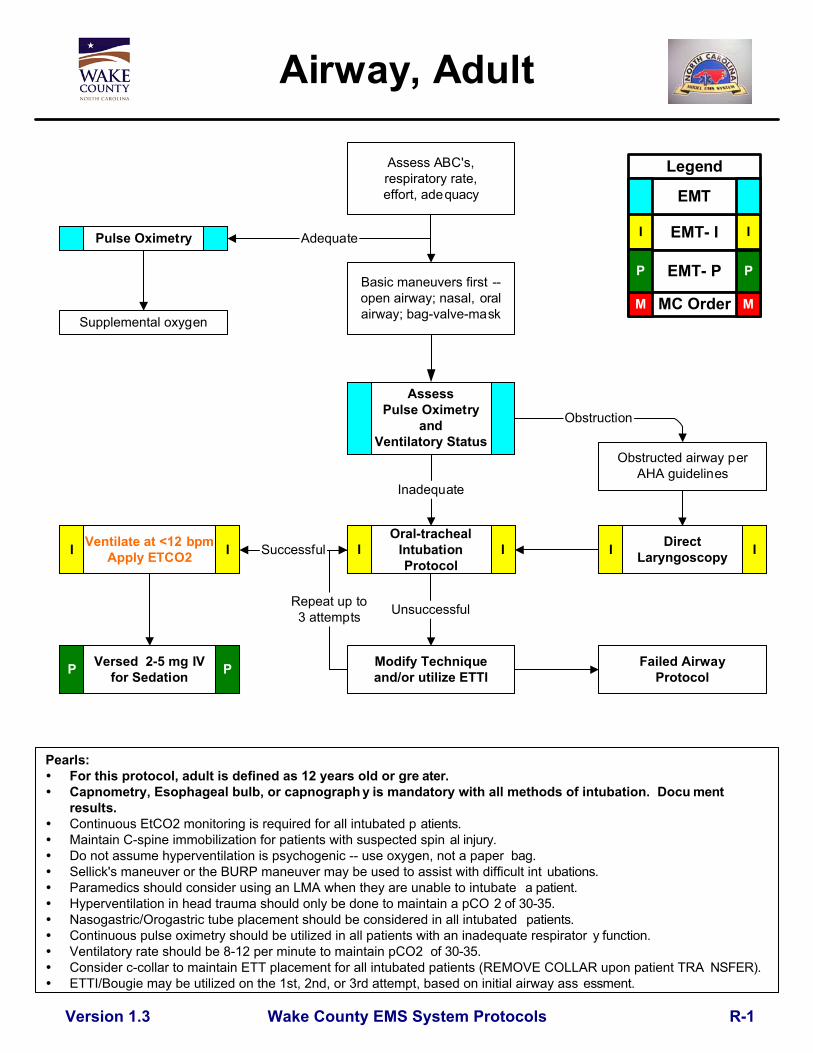
Pearls:For this protocol, adult is defined as 12 years old or gre ater.Capnometry, Esophageal bulb, or capnograph y is mandatory with all methods of intubation. Docu mentresults.Continuous EtCO2 monitoring is required for all intubated p atients.Maintain C-spine immobilization for patients with suspected spin al injury.Do not assume hyperventilation is psychogenic -- use oxygen, not a paper bag.Sellick's maneuver or the BURP maneuver may be used to assist with difficult int ubations.Paramedics should consider using an LMA when they are unable to intubate a patient.Hyperventilation in head trauma should only be done to maintain a pCO 2 of 30-35.Nasogastric/Orogastric tube placement should be considered in all intubated patients.Continuous pulse oximetry should be utilized in all patients with an inadequate respirator y function.Ventilatory rate should be 8-12 per minute to maintain pCO2 of 30-35.Consider c-collar to maintain ETT placement for all intubated patients (REMOVE COLLAR upon patient TRA NSFER).ETTI/Bougie may be utilized on the 1st, 2nd, or 3rd attempt, based on initial airway ass essment.
Wake County EMS System Protocols
Airway, Adult
Supplemental oxygen
Assess ABC's,respiratory rate,effort, adequacy
Basic maneuvers first --open airway; nasal, oralairway; bag-valve-mask
Obstructed airway perAHA guidelines
Oral-trachealIntubationProtocol
Version 1.3
Modify Techniqueand/or utilize ETTI
Pulse Oximetry
AssessPulse Oximetry
andVentilatory Status
DirectLaryngoscopy
Unsuccessful
I II I
Obstruction
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
SuccessfulVentilate at <12 bpmApply ETCO2
Versed 2-5 mg IVfor SedationP P
Inadequate
Adequate
I I
R-1
Failed AirwayProtocol
Repeat up to3 attempts

Pearls:Continuous pulse oximetry should be utilized in all patients with an inad equate respiratory function.Continuous EtCO2 should be applied to all patients with respiratory failure and to all intubated patients.Providers should consider using an LMA when they are unable to intubate a patient.EMT-Is and Basics may utilize the LMA only after attending approved Wake EMS System inser vice andcompleting practical examination.Nasogastric/Orogastric tube placement should be considered in all intubated patients.Notify Medical Control AS EARLY AS POSSIBLE about the patient's difficult / failed airway.Patient must have respiratory effort in order to place Nasotrach eal tube.
Wake County EMS System Protocols
Airway, Adult-Failed
If adequate oxygenation/ventilation, continue BVM.If inadquate, continue with
protocol
Good Air Movementwith BVM Ventilation ?Yes
No
Version 1.2
Continue BVM
Facial traumaor swelling ?
LMA Airway orNasotracheal
Intubation
Surgical Airway
YesNo
Adequate Airway? No
Yes
Continue ventilation
Three (3) failed intubation attemptsby most proficient technician on sc ene or anatomy
inconsistent with intubatio n attempts.
NO MORE THAN THREE (3) ATTEMPTS TOTAL
P P
P P
Ventilate at <12 bpmApply ETCO2
and Maintain EtCO2 above20 if possible
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
R-2
P

Pearls:Exam: Mental Status, Skin, Neck, Lung, Heart, Abdomen, Back, Extremities, NeuroAvoid Nitroglycerin in any patient who's used Viagra or Levitra in the past 24 hours o r Cialis in the past 36 hours due to possible severehypotension.If patient has taken nitrogl ycerin without relief, consider potency of the medication.Consider myocardial infarction in all these patients.Diabetics and geriatric patients often have atypical pain, or only generalized complaints.Careful monitoring of level of consciousness, BP, and respiratory status with above interventions is essential.Allow the patient to be in their position of comfort to maximize their breathing effort.If patient condition precludes us e of indicated NTG spray, proceed to NTG paste.If Nitro Paste is used, do not continue to use Nitro Spray.Document CPAP application using the "CPAP" proced ure in the call reporting system. Document 12-lead with "12-lead EKG" procedure
Wake County EMS System Protocols
Pulmonary EdemaHistory:
Congestive heart failurePast medical historyMedications (digoxin, lasix)Viagra, Levitra, CialisCardiac history --pastmyocardial infarction
Signs/Symptoms:Respiratory distress, bilateral ralesApprehension, orthopneaJugular vein distentionPink, frothy sputumPeripheral edema, diaphoresisHypotension, shockChest pain
Version 1.3
Differential:Myocardial infarctionCongestive heart failureAsthmaAnaphylaxisAspirationCOPDPleural effusionPneumoniaPulmonary embolusPericardial tamponadeToxic Exposure
Universal Patient Care Protocol
Nitroglycerin 0.4 mg SL q 2-3 minutesIf BP > 110 systolic
IV Protocol
Consider Morphine2 mg slow IV
12 Lead EKG
Consider Lasix 40 mg slow IV ordouble patient daily dose up to 80 mg
I I
I I
P P
1" Nitroglycerin Paste ifSBP > 110I I
PP
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Consider CPAPP P
Obtain and recordETCO2 and Pulse OximetryP P
II
Additional Morphine2 mg q 5 min up to 10 mg PP
R-3
Versed 1-2 mg IV or 2 mg IN ifSBP>110 and pt not tolerating mask

Respiratory DistressHistory:
Asthma; COPD -- chronicbronchitis, emphysema,congestive heart failureHome treatment (oxygen,nebulizer)Medications (theophylline,steroids, inhalers)Toxic exposure, smokeinhalation
Signs and Symptoms:Shortness of breathPursed lip breathingDecreased ability to speak
Increased respiratory rateand effortWheezing, rhonchi, rales,stridorUse of accessory musclesFever, coughTachycardia
Differential:AsthmaAnaphylaxisAspirationCOPD (Emphysema, Bronchitis)Pleural effusionPneumoniaPulmonary embolusPneumothoraxCardiac (MI or CHF)Pericardial tamponadeHyperventilationInhaled toxin (Carbon monoxide, etc.)
Wake County EMS System ProtocolsVersion 1.1
Universal Patient Care Protocol
IV ProtocolI I
Obtain and RecordETCO2 and Pulse Oximetry
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Pulmonary EdemaProtocol
3cc SalineNebulized
Respiratory Insuff iciency?Adult AirwayProtocol Yes Position to patient
comfortNo
WheezesStridor
Rales orSigns of CHF
II
No ImprovementEpi 0.3 mg 1:10,000 Neb
OrEpi 0.5 mg 1:1000 IM
I I
Solu Medrol 125 mg IVP P
For Severe CasesConsider Epi 1:10,000
0.3 mg IVP P
IV ProtocolI I
Albuterol 2.5 mg Neb
Albuterol 2.5 mg/Atrovent 500 mcg
NebI I
ConsiderSolu Medrol 125 mg IV
Magnesium Sulfate2 grams IV over 20 min
ConsiderContinuous Albuterol Neb
Pearls: EMT administration of albuterol is restricted only to patients who are under doctor's orders/presc ription for
albuterol. Any EMT wishing to provide albuterol must complete in-service training prior to admin istration. Pulse oximetry should be monitored continously if initial saturation is < or = 96%, or there is a decline in patient's
status despite normal pulse oximetry readings.Use of CPAP in Asthma patients is contrain dicated. Contact Medical Control prior to applying to asthma tic patient.Contact Medical Control prior to administering epinephrine in patients who are >50 years of age, have ahistory of cardiac disease, or if the patient's heart rate is >150. Epinephrine may precipita te cardiac ischemia.A 12-lead ECG should be performed on these p atients.A silent chest in respiratory distress is a pre-respiratory ar rest sign.
ETCO2 should be recorded for patients who require solumedrol, magnesium sulfate, or epinephrine.Xopenex may be substituted for Albuterol and mixed with Atrovent. Use patient current dose (0. 31-1.25 mg) and meds.
P PConsiderEpinepherine 0.3 mg
1:1,000 SQ / IMI I
Contact Medical Controlif patient does not meet
criteria for Epi(see Pearls below)
MM
R-4

Wake County EMS System Protocols
Differential:Superficial (1°) red and painfulPartial thickness (2°) blisteringFull thickness (3°) painless andcharred or leathery skinChemicalThermalElectricalRadiation
BurnsHistory:
Type of exposure (heat, gas,chemical)Inhalation injuryTime of injuryPast medical historyMedicationsOther traumaLoss of consciousnessTetanus/Immunization status
Signs and Symptoms:Burns, pain, swellingDizzinessLoss of consciousnessHypotension / shockAirway compromise / distressSinged facial or nasal hairHoarseness / wheezing
Universal Patient Care Protocol
Remove rings, bracelets, andother constricting items
Cover burn with a Dry sterile sheet or dressings
If burn < 10% body surface area(using rule of nines)
Cool down the wound with N ormal Saline andConsider Burn Gel (if available)
IV Protocol - Bolus
Consider Transport Directlyto UNC Burn Center if no Airway Involvment(Trasnsport to Nearest ED if Airway Involved)
For pain controlMorphine 5 mg IV q 5-10 min up to 50 mg
For Nausea, Zofran 4 mg IV
Eye involvement ?Continuous saline flush in affected eye(s)
Remove clothing or expose areaBrush off any visible dry chemicals or powder
Flush area with water or Normal Salinefor 10-15 minutes
Pearls:Exam: Mental Status, HEENT, Neck, Heart, Lungs, Abdomen, Extremities, Back, NeuroCritical Burns: >25% body surface area (BSA); 3° burns >10% BSA; 2° and 3° burns to face, eyes, hands or feet;electrical burns; respiratory burns; deep chemical burns; burns with extremes of age or chronic disease; and burns withassociated major traumatic injury. These burns may require hospital admission or transfer to a burn center.Early intubation is required in significant inhalation injuries.Potential CO exposure should be treated with 100% oxygen.Circumferential burns to extremities are dangerous due to potential vascular compromise 2° to soft tissue swelling.Burn patients are prone to hypothermia - Never apply ice or cool burns that involve >10% body surface area.Do not overlook the possibility of multiple system trauma.Do not overlook the possibility for child abuse with children and burn injuries.
Version 1.2
ChemicalThermal
I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
PP
I
T-1

Wake County EMS System Protocols
Pearls:Exam: Trauma Survey, Head, Neck, Chest, Abdomen, Pelvis, Back, Extremities, Skin, Neuro
With cold water no time limit -- resu scitate all. All victims should be transported for evaluation due to potential for worsening over the next several hours. Drowning is a leading cause of death among would-be rescuers. Allow appropriately trained and certified rescuers to remove victims from area s of danger. With pressure injuries (decompression / barotrauma), consider transport or availability of a hyperbaric
chamber (Duke University Medical Center).
Drowning / Near DrowningHistory:
Submersion in waterregardless of depthPossible history of trauma ie:diving boardDuration of immersionTemperature of waterFresh/Salt Water
Signs and Symptoms:UnresponsiveMental status changesDecreased or absent vital signsVomitingCoughing
Spinal Immobilization Protocol
IV Protocol
Cardiac monitorPulse Oximetry
ETCO2
Version 1.1
Differential:TraumaPre-existing medical problemPressure injury (diving)
BarotraumaDecompression sickness
Universal Patient Care Protocol
Adult Airway Protocolor
Respiratory Distress Protocolor
Other Appropriate Protocolbased on symptoms
Consider CPAP
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
P P
I I
T-2
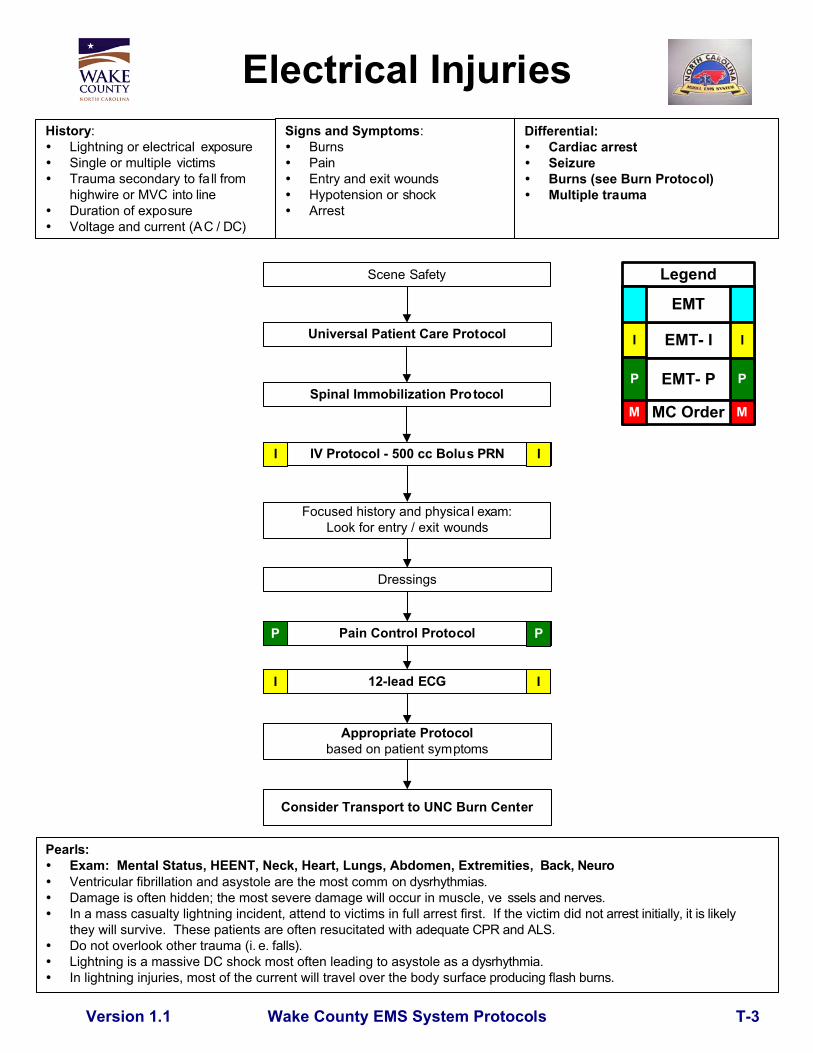
Wake County EMS System Protocols
Electrical InjuriesHistory:
Lightning or electrical exposureSingle or multiple victimsTrauma secondary to fa ll fromhighwire or MVC into lineDuration of exposureVoltage and current (AC / DC)
Signs and Symptoms:BurnsPainEntry and exit woundsHypotension or shockArrest
Pearls:Exam: Mental Status, HEENT, Neck, Heart, Lungs, Abdomen, Extremities, Back, NeuroVentricular fibrillation and asystole are the most comm on dysrhythmias.Damage is often hidden; the most severe damage will occur in muscle, ve ssels and nerves.
In a mass casualty lightning incident, attend to victims in full arrest first. If the victim did n ot arrest initially, it is likelythey will survive. These patients are often resucitated with adequate CPR and ALS.Do not overlook other trauma (i. e. falls).
Lightning is a massive DC shock most often leading to asystole as a dysrhythmia. In lightning injuries, most of the current will travel over the body surfa ce producing flash burns.
Universal Patient Care Protocol
Version 1.1
IV Protocol - 500 cc Bolus PRN
Focused history and physical exam:Look for entry / exit wounds
Dressings
Consider Transport to UNC Burn Center
Pain Control Protocol
Appropriate Protocolbased on patient symptoms
Differential:Cardiac arrestSeizureBurns (see Burn Protocol)Multiple trauma
12-lead ECG
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
Scene Safety
P P
I I
Spinal Immobilization Protocol
T-3

Wake County EMS System Protocols
Pearls:Exam: Mental Status, Extremity, NeuroIn amputations, time is critical. Transport to Trauma Center.Hip dislocations and knee and elbow fracture / dislocations have a high incidence of vascular compromise.Urgently transport any injury with vascular compromise.Blood loss may be concealed or not apparent with extremity injuries.Severe bleeding not rapidly controlled may necessitate application of a tourniquet.Lacerations must be evaluated for repair within 6 hours from the time of injury.
History:Type of injuryMechanism: crush / penetrating / amputationTime of injuryOpen vs. closed wound / fractureWound contaminationMedical historyMedications
Extremity TraumaSigns and Symptoms:
Pain, swellingDeformityAltered sensation / motor functionDiminished pulse / capillary refillDecreased extremity temperature
Wound care / hemorrhage control
Life or limb threatening event ?Pain medication needed ?
IV Protocol
Pain Control Protocol
Amputation ?Clean amputated part
Wrap part in sterile dressingsoaked in Normal Saline
Place in air tight containerPlace container on ice if available
Differential:AbrasionContusionLacerationSprainDislocationFractureAmputation
Universal Patient Care Protocol
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M MImmobolize extremity as indicated.Apply ice to reduce swelling.
Isolated extremity injury?
Yes
Multiple TraumaProtocol No
T-4Version 1.2

Wake County EMS System Protocols
History:Time of injuryMechanism: blunt / pe netratingLoss of consciousnessBleedingMedical historyMedicationsEvidence of multi -traumaHelmet use or damage to helmet
Head Trauma
Monitor and reassess
Spinal Immobilization Protocol
Isolated head trauma ?Multiple TraumaProtocol
Assist with basic airway maneuvers
No
If intubatedConsider Versed
2-5 mg IV for sedation
YesSeizure Protocol Seizure
Universal Care Protocol
Pearls: Exam: Mental Status, HEENT, Heart, Lungs, Abdomen, Extremities, B ack, Neuro
In absence of capnometer, hyperventilate the patient (adult: 20 breaths / min, chi ld: 30, infant: 35) only if ongoingevidence of brain herniation (blown pupil, decorticate or decerebrat e posturing, or bradycardia).
Increased intracranial pressure (ICP) may cause hypertension and bradycardia (Cus hing's Response). Hypotension usually indicates injury or shock unrelated to the head injury and sh ould be agressively treated. The most important item to monitor and document is a change in the level of con sciousness and GCS. Consider Restraints if necessary for patient's and/or personnel's protection per the Res traint Procedure. Concussions are periods of confusion or LOC associated with trauma which may have r esolved by the time EMS
arrives. Any prolonged confusion or mental status abnormality which does not return to normal within 15 minutes orany documented loss of consciousness should be evaluated by a physician ASAP.
Version 1.1
Signs and Symptoms:Pain, swelling, bleedingAltered mental statusUnconsciousRespiratory distress / failureVomitingSignificant mechanism of injury
Differential:Skull fractureBrain injury (concussion, contusion,hemorrhage, or laceration)Epidural hematomaSubdural hematomaSubarachnoid hemorrhageSpinal injuryAbuse
IV ProtocolNS Bolus to keep SBP > 100
Gag reflex present?
Yes
Lidocaine 100 mg IV
Intubate
Maintain ETCO2of 35 to 40 mmHg
Maintain Pulse Ox > 90%
I I
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
P P
Remove helmet ifindicated
Yes
II
Obtain GCS
GCS < 8
GCS > 8
Repeat every5-10 minutes
Do Not Give Haldol to Patient PP
No
If no facial trauma, Consider100 mg Lidocaine IV andNasotracheal Intubation
P P
P P
No
T-5

Wake County EMS System Protocols
Multiple TraumaHistory:
Time and mechanism of injuryDamage to structure or vehicleLocation in structure or vehicleOthers injured or deadSpeed and details of MVCRestraints / protective equipmentPast medical historyMedications
Signs and Symptoms:Pain, swellingDeformity, lesions, bleedingAltered mental status orunconsciousHypotension or shockArrest
Universal Patient Care Protocol
Spinal Immobilization Protocol
IV Protocol
Vital signs / perfusion ?
Ongoing assessmentNS Bolus to Maintain
SBP > 90
Consider rapid / air transport per air transportpolicy
Max 10 Min Scene Time
Pearls:Exam: Mental Status, Skin, HEENT, Heart, Lung, Abdomen, Extremities, Back, NeuroIn prolonged extrications/serious trauma consider air transport for transport speed and the ability to give blood.Severe bleeding from an extremity not rapidly controlled may necessitate the application of a tourniquetSee Trauma Procedure for criteria when notifying the ED of Trauma One or Trauma Alert.Record "Trauma Notification" procedure in electronic patient care reporting system.
Consider Pain Control ProtocolIf SBP >90 and GCS = 15
Differential (Life threatening):Chest Tension pneumothorax
Flail chestPericardial tamponadeOpen chest woundHemothorax
Intra-abdominal bleedingPelvis / Femur fractureSpine fracture / Cord injuryHead injury (see Head Trauma)Extremity fracture / DislocationHEENT (Airway obstruction)Hypothermia
NormalAbnormal
Rapid trauma assessment and GCS
I I
I
P P
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
I
Notify Trauma Center of Trauma Alert/One
Continued Hypotension(SBP < 90)?
Continue Fluid Bolus Consider: Reduction of Long Bone Fracture Reduction of Pelvic Fracture Control of External Hemorrhage
II
Consider Chest Decompression
T- 6Version 1.2

Wake County EMS System Protocols
Spinal ImmobilizationClearance
Neuro Exam: Any focal deficit?
Spinal Exam: Point tenderness orpain to ROM in spinal p rocess?
Distracting Injury: Any painful injurythat might distract the patient
from the pain of a c-spi ne injury?
Intoxication: Any evidence?
Pearls: Consider immbolization in any patient with arthritis, cancer, or other underl ying disease. Significant mechanism includes high-energy events such as ejection, high falls, and abr upt deceleration crashes and
may indicate the need for spinal immobilization in the absence of symptoms. Range of motion should NOT be assessed if patient has midline spinal tenderness. Patient's r ange of motion should
not be assisted. The patient should touch their chin to their chest, extend their neck (look up) , and turn their head fromside to side (shoulder to shoulder) without spinal process pain.
The acronym "NSAIDS" should be used to remember the steps in thi s protocol. "N" = Neurologic exam. Look for focal deficits such as tingling, reduced strength, on nu mbness in an extremity. "S" = Significant mechanisim in extre mes of age. "A" = Alertness. Is patient oriented to person, place, time, and situation? Any change to alertness with this incident?
"I" = Intoxication. Is there any indication that the person is intoxicated (impaired decision making ability)? "D" = Distracting injury. Is there any other injury which is capable of producing significant pain in this patient? "S" = Spinal exam. Look for point tenderness in any spinal process or spinal process tendernes s with range of motion. The decision to NOT implement spinal immobilization in a patient is the responsibility of t he paramedic. In very old and very young patients, a normal exam may not be sufficient to rule out spi nal injury.
Spinal ImmobilizationNot Required
No
No
No
No
No
Version 1.1
Spinal Immobilization Required
Alertness: Any alteration in patient?
Yes
Patient > 65 or < 5 withSIGNIFICANT mechanism?
Yes
Yes
Yes
Yes
Yes
No
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
II
II
II
II
II
II
II
T-7
No
Yes
Yes

Bilateral Chest Decompression
Return of Pulse?
Spinal Immobilization Protocol
Trauma ArrestHistory:
Patient who has sufferedtraumatic injury and is nowpulseless
Signs and Symptoms:
Evidence of penetratingtraumaEvidence of blunt trauma
Pearls:Injuries obviously incompatible with life include decapitation, massively deforming head or chest injuries, orother features of a particular patient encounter that would make resuscitation futile. If in doubt, place patienton the monitor.Consider using medical cardiac arrest protocols if uncertainty exists regarding medical or traumatic cause ofarrest.
Differential:
Medical condition precedingtraumatic event as cause of arrest.Tension PneumothoraxHypovolemic Shock
External hemorrhageUnstable pelvic fractureDisplaced long bone fracture(s)HemothoraxIntra-abdominal hemorrhageRetroperitoneal hemorrhage
Universal Patient Care Protocol
Do not attemptresusciation.Contact law
enforcment asappropriate.
Patient with injury obviouslyincompatible with life or traumatic
arrest in asystole?
Continue Fluid Bolus Consider: Reduction of Long Bone Fracture Reduction of Pelvic Fracture Control of External Hemorrhage
Go to AppropriateProtocol
IV Protocol withFluid Bolus
No
Yes
No
EMT- I
EMT
EMT- P
Legend
MC Order
I
P
I
P
M M
I
Yes
P
I
I I
P
Wake County EMS System ProtocolsVersion 1.2 T - 8

















