Chetan B. Patel, MD Assistant Professor of Medicine Duke Cardiac Transplantation and Mechanical Circulatory Support Program LVAD Complications: Bleeding and Clotting Duke Advanced Heart Failure Symposium October 5 th 2013
Transcript
Chetan B. Patel, MD
Assistant Professor of Medicine
Duke Cardiac Transplantation and Mechanical Circulatory Support Program
LVAD Complications: Bleeding and Clotting
Duke Advanced Heart Failure SymposiumOctober 5th 2013
Disclosures
• Consultant for Thoratec Corp and Heartware Inc.
* Off label use of eptifibitide, tissue-plasminogen activator
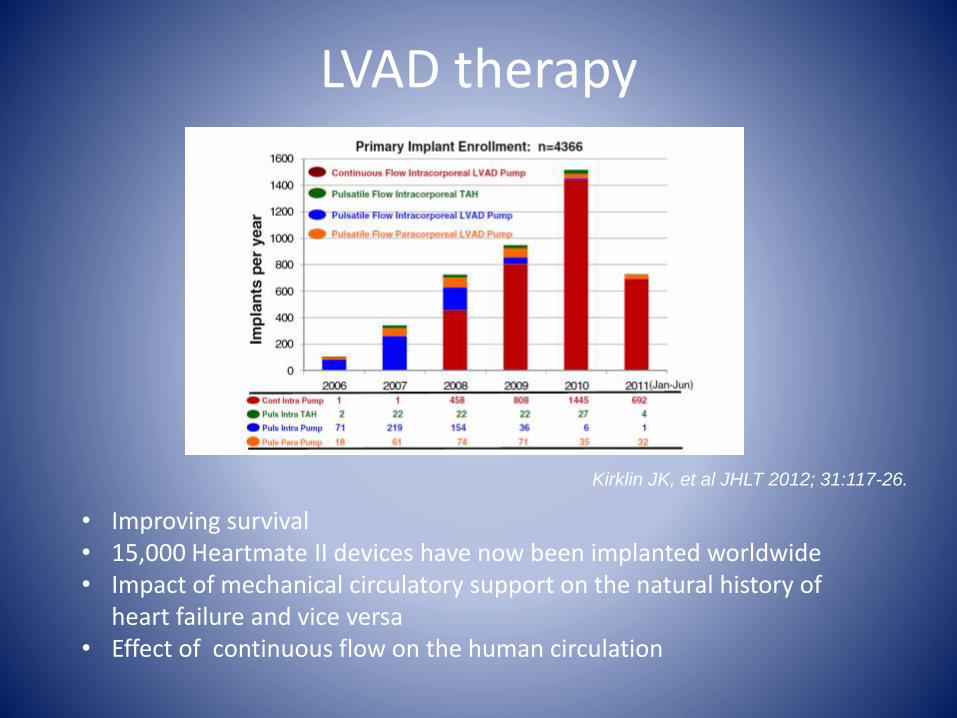
LVAD therapy
• Improving survival• 15,000 Heartmate II devices have now been implanted worldwide• Impact of mechanical circulatory support on the natural history of
heart failure and vice versa• Effect of continuous flow on the human circulation
Kirklin JK, et al JHLT 2012; 31:117-26.
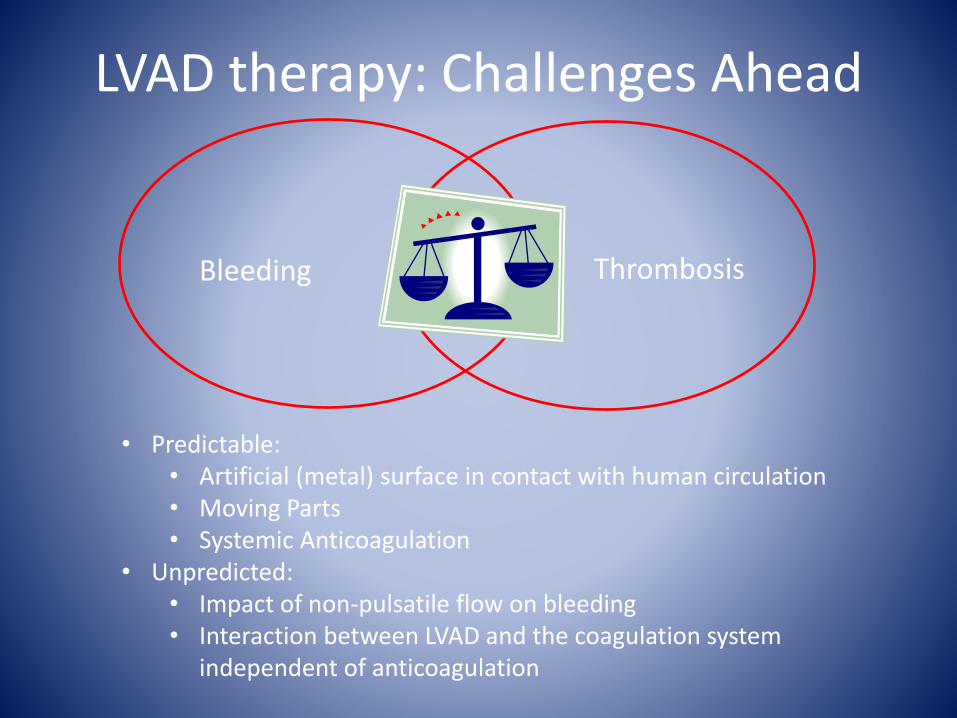
LVAD therapy: Challenges Ahead
Right Heart FailureTricuspid Regurgitation
Aortic Insufficiency
“Walking” Ventricular Tachycardia
Bleeding Thrombosis
LVAD therapy: Challenges Ahead
• Predictable: • Artificial (metal) surface in contact with human circulation• Moving Parts• Systemic Anticoagulation
• Unpredicted:• Impact of non-pulsatile flow on bleeding• Interaction between LVAD and the coagulation system
independent of anticoagulation
Anticoagulation Strategies for Continuous Flow LVADs
Historical Perspective
– Initial experience with early version of the HMII demonstrated high pump thrombosis rate (40%)
– Pump re-design and call for higher levels of anticoagulation (INR 2.5-3.5)
– Practice guidelines suggested INR 2.0-3.0
– Dual antiplatelet therapy
– Perioperative heparin
J Heart Lung Transplant 2010; 29:S1-S39
Early Bleeding/ThrombusHeartMate II Destination Therapy Trial
CF LVAD (n=133)
[211 pt-years] PF LVAD (n=59)
[41 pt-years]
Events/pt yr Events/pt yr Risk Ratio [95% Confidence
Interval] p-value
Pump Replacements 0.06 0.51
<0.001
Stroke 0.13 0.22 0.21
Ischemic 0.06 0.10 0.38
Hemorrhagic 0.07 0.12 0.33
Device-related infection 0.48 0.90 0.01
Local non-device infection 0.76 1.33 0.02
Sepsis 0.39 1.11 <0.001
Bleeding
Bleeding requiring PRBC 1.66 2.45 0.06
Bleeding requiring surgery 0.24 0.29 0.57
Other Neurological 0.17 0.29 0.14
Right Heart Failure
Extended Inotropes 0.14 0.46 <0.001
RVAD 0.02 0.07 0.12
Cardiac Arrhythmias 0.69 1.31 0.006
Respiratory Failure 0.31 0.80 <0.001
Renal Failure 0.10 0.34 <0.001
Hepatic Dysfunction 0.01 0.00
Device Thrombosis 0.02 0.00
Re-hospitalizations 2.64 4.25 0.02
0.0 0.5 1.0 1.5 2.0
Favors CF LVAD Favors PF LVAD
N Engl J Med 2009; 361: 2241-51
Early Bleeding/ThrombusHeartware HVAD Bridge to Transplant Study
Suarez J et al. Circ HF, 2011
Aaronson et al. Circulation, 2012
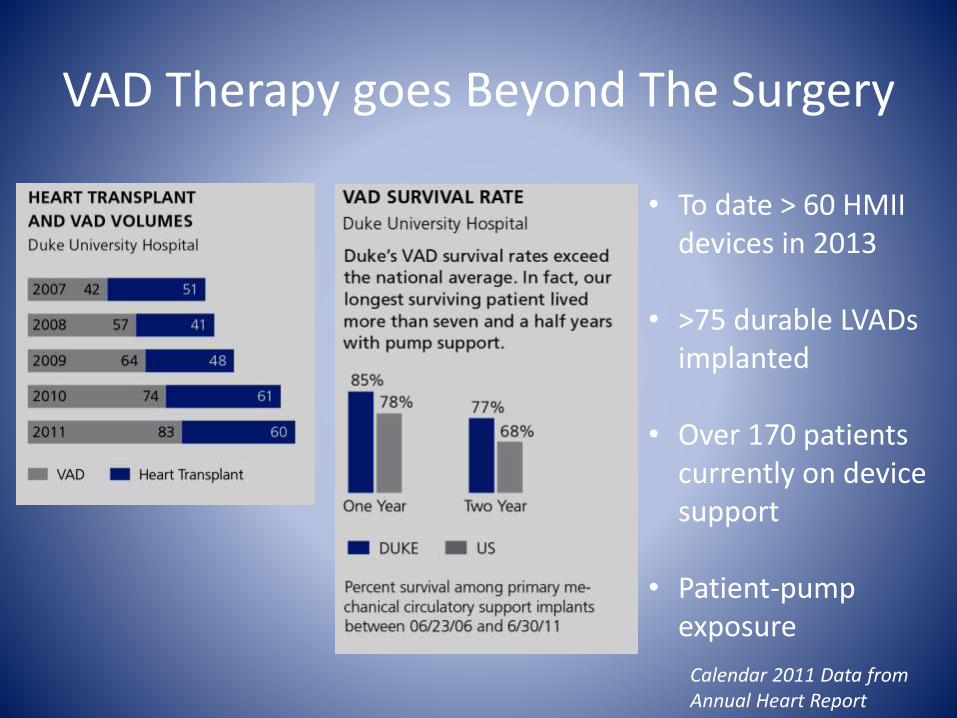
VAD Therapy goes Beyond The Surgery
• To date > 60 HMII devices in 2013
• >75 durable LVADs implanted
• Over 170 patients currently on device support
• Patient-pump exposure
Calendar 2011 Data from Annual Heart Report
Suarez J et al. Circ HF, 2011
Non-Surgical Bleeding after Continuous Flow Pump Support
Decrease in HMW multimers leading to impaired anticoagulation
Acquired vWD
vWF fragments Impaired platelet aggregation
Continuous Flow Device
Non-Surgical Bleeding after Continuous Flow Pump Support
N= 71 with 156 readmissions (4year) , 19% of all readmissions related to bleeding
N=83 with 224 readmissions ( 3 year) , 66 readmissions in 34 patients (30% overall) related to bleeding
Ann Thorac Surg 2013;95:1276–81)
J Am Coll Cardiol 2013;61:153–63
331 patients from a CF VAD BTT
trial
10 patients with thrombotic events
and 58 hemorrhagic events
Some centers reduced INR goal to
1.5-2.0 based on bleeding events
ASA 81 mg daily
No postoperative heparin
J Heart Lung Transplant 2009; 28:881-7
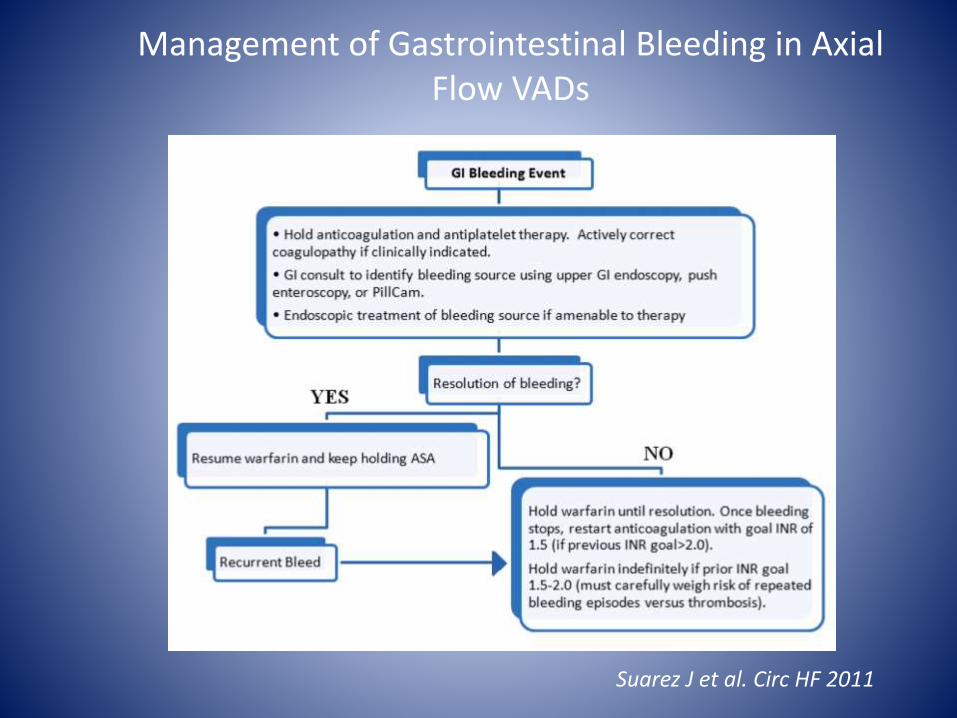
Suarez J et al. Circ HF 2011
Management of Gastrointestinal Bleeding in Axial Flow VADs
To do list:
Fix bleeding issues with LVAD therapy
The Other Side of the Bleeding-Clotting Quagmire
Romano et al. ISHLT 2011
• Event-free survival decreased with evidence of hemolysis
• Pump thrombus = Hemolysis?
What defines thrombosis?
Hemolysis DefinitionsINTERMACS: Plasma free Hgb > 40 mg/dl occurring > 72 hours post-implantHeartMate II DT Trial: 2 plasma free Hgb >40 mg/dl within 24 hours of each other and an LDH > 1000 mg/dl within the same 24-hour periodADVANCE: plasma free Hgb > 40 mg/dl
• Will add cine image of aortic outflow with possible thrombus at CT
Thrombosis is “invisible”
Managing Thrombotic Events
• Pump thrombosis may present with:
– Thromboembolism
– Hemolysis (LDH, haptoglobin, plasma free Hgb)
– Increasing power consumption with high flow rates
– Abrupt pump dysfunction (stoppage)
• Treatment will depend upon acuity, impact on patient, and pump performance
• Anticoagulation and antiplatelet therapy is device-specific
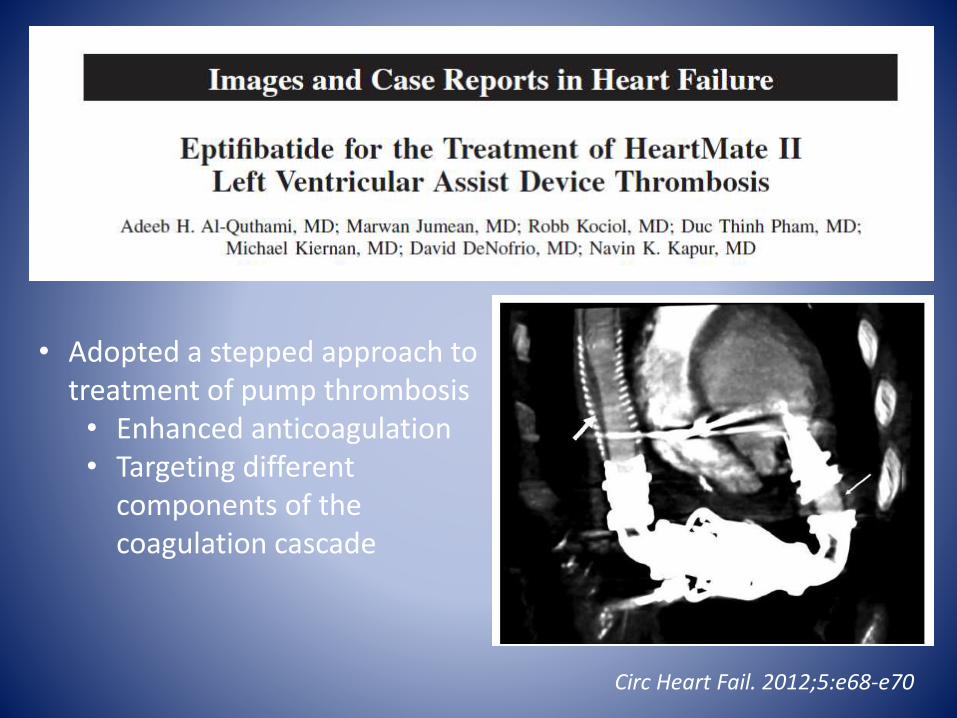
• Adopted a stepped approach to treatment of pump thrombosis• Enhanced anticoagulation• Targeting different